Timely Referral in CKD - FOMA District 2
34
Timely Referral in CKD Primary Care and Nephrology as a Team Jamal Salameh, M.D.
Transcript of Timely Referral in CKD - FOMA District 2
Timely Referral in CKD
Primary Care and Nephrology as a Team
Jamal Salameh, M.D.
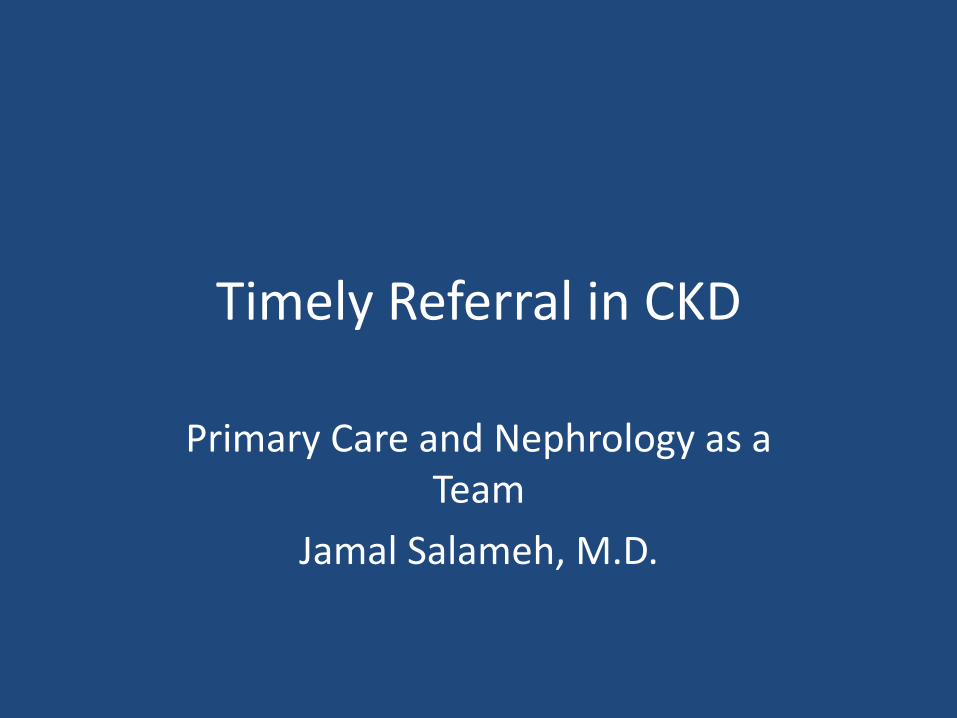
An Epidemic of Kidney Disease
Clinical Practice Guidelines for CKD Am J Kidney Dis. 2002;39(suppl 1):S17–S31.
GFR = glomerular filtration rate (mL/min/1.73 m2); *with kidney damage
Stage 1: GFR ≥90*
Stage 3: GFR 30–59
Stage 4: GFR 15–29
Stage 2: GFR 60–89*
Stage 5: GFR <15
n=5,900,000
n=5,300,000
n=7,600,000
n=400,000
n=300,000
Total=20 million USA
Prevalence CKD stages 1- 4
10% 1988-94
13% 1999-2004 Coresh, JAMA 298:2038, 2007
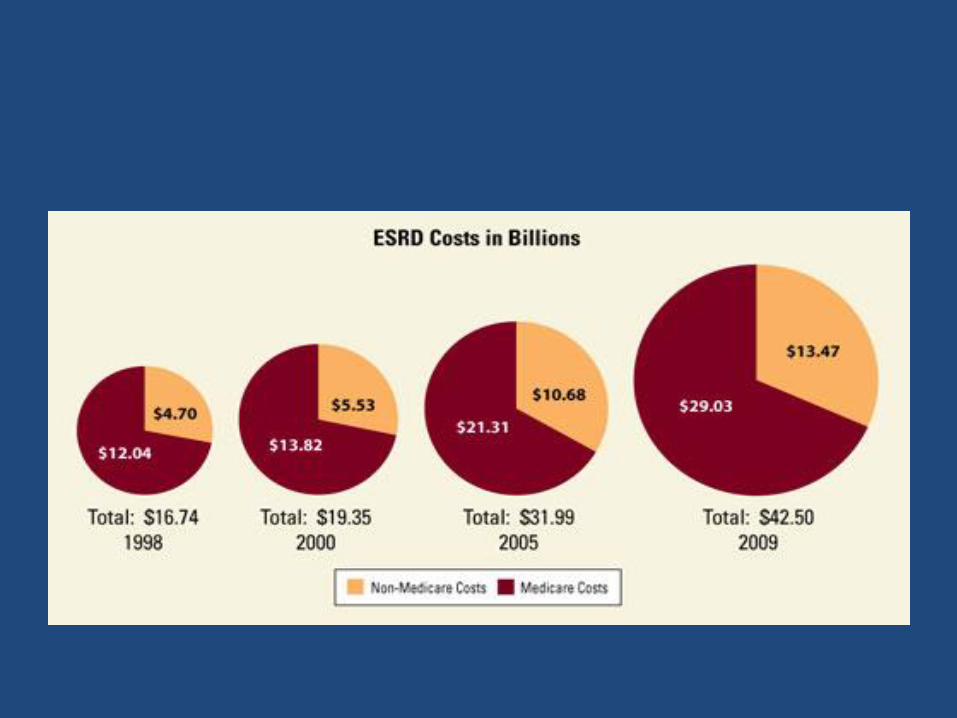
Treating ESRD patients cost the United States over $40 billion in public and private funds in 2009.
Scope of Chronic Kidney Disease (CKD) in the US
• There are over 8 million people in the US with advanced CKD
Stage 3 and 4 CKD 15-20 million people Stage 5 CKD 500,000 people
• There are over 360,000 patients currently on Renal Replacement Therapy
• 110,000 patients start Renal Replacement Therapy every year
• The cost of End Stage Renal Disease Care (ESRD) to Medicare exceeds $40 Billion per
year
5
Screening
• Screening Should Include: – Laboratory studies to include serum creatinine and
eGFR
– Urinalysis to determine the presence of proteinuria
– Imaging studies such as ultrasound
Screening recommendations are provided in KDOQI, Guideline 1
http://www.kidney.org/professionals/kdoqi/guidelines_ckd/toc.htm
ADD-CKD Study
• Over half of primary care clinicians recognize CKD diagnostic criteria yet only 12.1% of people with CKD with CKD were diagnosed.
• 84.8 % of individuals with type -2 diabetes had eGFR data in the past 15 months yet only 12.1% of people with CKD were diagnosed
Szczech LA, et al. PLoS One 9(11); 2014:e110535
6

Improved CKD diagnosis driven by the PC clinician…
• Studies demonstrate when a CKD diagnosis is identified by the PC clinician: – Significant improvements are shown in
• Increased urinary albumin testing
• Increased appropriate use of ACEi or ARB
• Avoidance of NSAIDs prescribing among patients with low eGFR
• Appropriate nephrology consultation
• Improved patient quality of life
• Decreased healthcare costs
Improved Diagnosis Improves Outcomes
• NSAID prescribing decreased after the implementation of eGFR reporting, and there were significant improvements in estimated renal function in patients who stopped taking NSAIDs. Hence eGFR reporting may result in safer prescribing.1
• There was significantly increased overall mortality in the late referral group as compared with the early referral group. The duration of hospital stay, at the time of initiation of renal replacement therapy, was greater in the late referred group by an average of 12 days.2
1. Wei, L., MacDonald, T.M., Jennings, C., Sheng, X., Flynn, R.W., & Murphy, M.J. (2013). Estimated GFR reporting is associated with decreased nonsteroidal anti-inflammatory drug prescribing and increased renal function. Kidney In,
84(1), 174-8. 2. Chan, M.R., Dall, A.T., Fletcher, K.E., Lu, N., & Trivedi, H. (2007). Outcomes in patients with chronic kidney disease
referred late to nephrologists: a meta-analysis. Am J Med, 120(12), 1063-1070.
9
KDOQI CKD Definition
• eGFR < 60 ml/min/1.73 m2 for 3 months or longer
OR
• Spot urine albumin/creatinine ratio of >30 mg/g in 2 of 3
urine samples

The Early NHANES III Study Analysis of Prevalence of CKD by Stage
Stage Description eGFR Range (ml/min/ 1.73 m2)
Population (1,000’s)
Population (%)
1 Kidney damage with
normal or increase GFR
≥ 90 5,900 3.3 %
2 Mildly decreased
GFR
60-89 5,300 3.0 %
3 Moderately decreased
GFR
30-59 7,600 4.3 %
4 Severely decreased
GFR
15-29 400 0.2 %
5 Kidney Failure < 15 300 0.1%
10 - Adapted from NHANES III (2000)
11
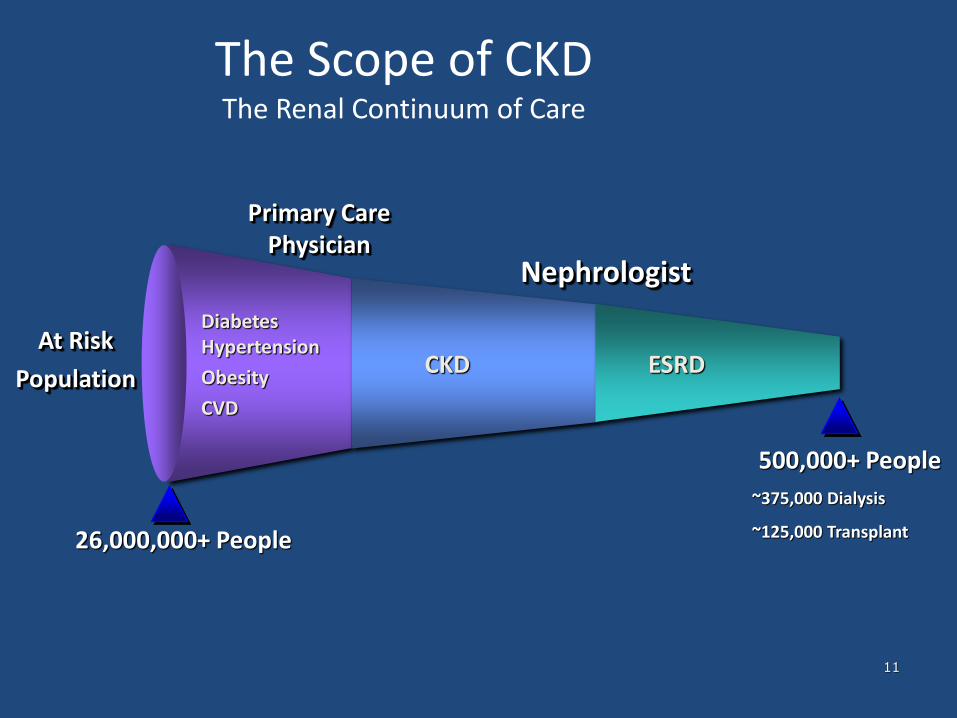
The Scope of CKD The Renal Continuum of Care
Nephrologist
Primary Care Physician
ESRD CKD At Risk
Population
Diabetes Hypertension
Obesity
CVD
26,000,000+ People
500,000+ People
~375,000 Dialysis
~125,000 Transplant

Primary & Secondary Prevention for CKD
Patients
• The 2006 CDC expert panel on CKD identified 3 Prevention Strategies:
– Primary Prevention-aimed at preventing and treating CKD risk factors
– Secondary Prevention-begins with the diagnosis of CKD
• CKD stages 1 & 2 (eGFR >60) attention to guidelines for good management of DM and HTN and CKD education
• CKD stage 3 (eGFR 30-59) attention to therapy for CKD related complications such as anemia and hyperparathyroidism and CV disease
• CKD stage 4 (eGFR 15-29) preparation for Renal Replacement Therapy with education about treatment choices and preparation for chronic access
– Tertiary Prevention- adequate renal replacement therapy
12
13
Do CKD patients need special care?
• CKD Prevalence – A worldwide public health condition
– Poor outcomes
– High cost of care
• Morbidity and Mortality – CKD Stage 3 (eGFR of 30-59)
• 1.1% risk of progression to ESRD
• 24.3% mortality risk before ESRD
– CKD stage 4 (eGFR of 15-29) • 17.6% risk of progression to ESRD
• 45.7% mortality risk before ESRD
14
CKD Care: Co-morbidities and Complications
• Establish CKD diagnosis and Details: – Make a specific renal disease diagnosis if possible – Identify co-morbidities
• Hypertension • Diabetes • Cardiovascular Disease
– Determine the severity of CKD (know the eGFR) – Identify CKD Complications
• Anemia (know the Hgb) • Secondary Hyperparathyroidism (know the Ca and Phos and PTH) • Malnutrition (know the albumin) • Metabolic Acidosis • Fluid Overload
– Assess stability of Kidney Function and CKD Stage
Recommendations for further evaluation are outlined in KDOQI Guideline 2 http://www.kidney.org/professionals/kdoqi/guidelines_ckd/toc.htm
CKD and Cardiovascular disease
• Framingham Heart Study:
-Prevalence of CVD 18% in Males and 21% in Females with CKD
-In Males Cr 1.5-3 and Females Cr 1.4-3
-Compared to 14% in M and 9% in F with Normal Serum
Creatinine levels
-CVD Mortality in CKD patients is More Likely than the Development of ESRD (198 DIED, 10 ESRD)
-Timely Referral for Cardiovascular disease screening
decreases Morbidity and Mortality.

Benefits of Early Identification and Treatment
• Renal Function Preservation
• Decline in Morbidity and Mortality
• Decline in Number of Hospitalizations
• Decline in Duration of Hospitalizations
• Increase in Access placement
• Appropriate Anemia Management
• Improves Quality of Life
Renal Function Preservation
• In one study 726 patients newly referred to Nephrology saw the rate of decline in GFR drop from 5.4 ml/min per year from the 5 years prior to 0.35 ml/min/year during the 5 years post referral
• The Protective Effect of Therapy has greatest impact if initiated before Creatinine exceeds 1.5 to 2 mg/dl or a GFR of < 60 ml/min per 1.73 m2

18
Timely Referral to Nephrology
• 30-40% of referrals to nephrologists occur less than 120 days prior to starting dialysis
• Referral to nephrology <4 months before starting dialysis is considered a “Late Referral” by Medicare and other Payers
• Timely Referral to Nephrology creates the opportunity for Modality Education, creation of a permanent dialysis access, and management of CKD complications like Anemia, Malnutrition, sHPT, Fluid overload, Metabolic Acidosis, etc…
19
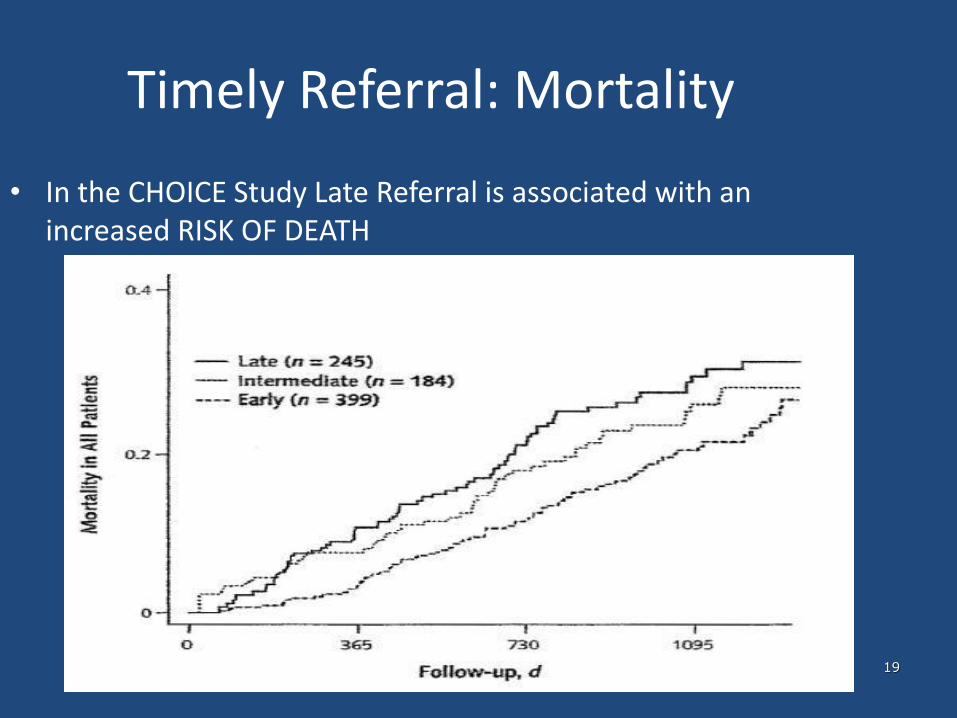
Timely Referral: Mortality
• In the CHOICE Study Late Referral is associated with an increased RISK OF DEATH
20
Timely Referral: Long-lasting benefits
• “Late Referral” patients have a 44% higher risk of mortality in the first year of dialysis compared to “Early Referral” patients
Timing of Nephrologist Referral and AV Access Use: CHOICE Study
• Cohort of 356 Dialysis patients in CHOICE
• Patients seeing Nephrologist at least 1 month prior to start of dialysis 39% AVF/G vs 10%
• At 6 month mark on HD this effect as 74% vs 56%
• Patients referred w/in 1 month of dialysis had a median of 202 days compared with 19 days of Catheter use for patients referred > 12 months prior
•

Prospective Study of ESRD patients in Korea
• 1028 patients with ESRD comparing ER vs LR
• Survival was increased by 240 % (Hazard Ratio 2.4)
• Time to incident dialysis ER 62 mos vs 3 mos for LR
• Catheter use in 44% ER vs 52% LR
23
Timely Referral: Quality of Life
• Timely Referral improves Quality of Life in CKD patients – First dialysis is a planned event avoiding a “Crash” into Dialysis
– Dialysis Access is established
– Families and Patients are prepared
– Appropriate use of Erythropoeisis-Stimulating Agent (ESA) therapy for treating anemia
– Modality of Dialysis can be tailored to the patient’s needs
24
Timely Referral: Healthcare Costs
• Timely Referral Lowers Healthcare Costs
– Reduced Hospitalizations
– Improved management of co-morbidities
– Reduced complications from cardiovascular disease
– Delayed deterioration of residual renal function and the need to start Renal Replacement Therapy
– Enhances patient choices for treatment modalities

Improved Diagnosis Improves Population Health
• CKD patients & their co-morbid conditions drive significant healthcare costs across the board.
• HHS goal to have 85% of all Medicare fee-for-service payments tied to quality or value by 2016, and 90% by 2018.
Burwell, S. Setting Value-Based Payment Goals – HHS Efforts to Improve U.S. Health Care. New England Journal of
Medicine. (2015);DOI:10. 1056/NEJMp1500445

26
Benefits of Timely Referral in CKD Care
• Slower progression to ESRD
• Increased functional status
• Decreased Morbidity and Mortality from fewer
– Hospitalizations
– CVD events
– Urgent Care & Emergency Visits
– Medication Management complications
• Decreased costs from fewer urgent complications
27
Benefits of Timely Referral in Preparation for Renal Replacement Therapy
• Patient Education and Preparation associated with Timely Referral are critical for:
– Timely vascular access placement
– Reduced use of dialysis catheters
– Modality Choice for Patients • Home Therapies
– Peritoneal Dialysis
– Home Hemodialysis
• Transplantation
• In-Center Hemodialysis
• Palliative or End of Life Care
28
Coordinated Roles in the care of the CKD Patient
• Primary Care Provider – Early identification of CKD patients
– Focused & Structured evaluation and management
– Referral and co-management with nephrologist
– Co-Management of Co-Morbid Diseases
• Nephrologist and the Renal Care Team – Focused assistance in management of co-morbidities
• Diabetes, Hypertension, Cardiovascular disease
• Anemia, Mineral Metabolism, Nutrition & Volume management
• Vascular Access Preparation & Management
• Education on ESRD treatment options & modality selection
– Co-management of Medications, Family and Social Issues of Renal Disease

Rethinking the CKD Clinic
• Second Tier components of CKD Care 1. Protocols and tools for Anemia, Mineral
Metabolism and Nutrition Management (sharing best practices)
2. Communication tools for Co-management of Co-morbidities (DM, HTN, CVD)
3. Communication tools for exchanging Problem Lists, Medication Lists and Plan of Care with all Providers
4. Best Resources allocations based on Best Practices
30
CKD Care: PCP & Nephrology Team
• Various Descriptors of the PCP / Nephrology Team Relationship in CKD care
– “Joint Care” between PCP and Nephrology Team
– “Co-Management” as shared care with defined roles between PCP and Nephrology Team
– “Combicare” as care from an informed PCP working with support from the Nephrology team
– “Right Care” denoting jointly working together to provide the Right Care for the CKD patient
Treatment Options/Kidney Smart
• This multidisciplinary education improves patient and family understanding of CKD and treatment options including transplantation and dialysis
• Treatment Options education has been proven to increase the percentage of patients who chose Home Therapies and who start dialysis with a permanent access
• Treatment Options education may best be provided by a variety of encounters including clinic encounters & Nephrology Practice Educational programs
• CKD Coordinated Care should track and coordinate all Treatment Options Education encounters for every appropriate patient
32
Timely Referral Decision Making
• Timely Referral Guidance:
– Rapidly decreasing renal function REFER
– Abnormal eGFR AND proteinuria REFER
– eGFR ≤ 30 ml/min/ 1.73 m2 REFER
– eGFR <60 ml/min/1.73 m2 and Cardiovascular Disease Present REFER
– Uncontrolled Hypertension Present REFER

“Improving the way care is delivered is central to our reform efforts. We have put into place policies to encourage greater integration within practice sites, greater coordination among providers, and greater attention to population health.” - HHS
Burwell, S. Setting Value-Based Payment Goals – HHS Efforts to Improve U.S. Health Care. New England Journal of Medicine. (2015);DOI:10. 1056/NEJMp1500445

Jamal Salameh, M.D.
First Coast Nephrology