Time-lapse cinefluorography in man
6
Time-Lapse Cincfluoro aphy in Man J.~'~r.s Rlrcnle, M.A., D.M. M LCH of the emphasis in motilitv studies of the colon has been on quanti- tative comparisons of intrahmfinal pressure records; efforts have been made to find increasingly sophisticated means of measuring experimental re- suits. This approach may be of great value in pharmacolo~c studies and in some clinical comparisons, but variation between individuals is so great that one can only draw conclusions from mean "motility indexes" derived from relatively large groups of subjects. Qualitative studies also may be useful in distinguishing between normal and abnormal bowel activity. At Oxford we have made studiest of coordi- nated propulsion in the normal colon with time-lapse cinelluorography at I-rnln_ intervals in subjects who had swallowed 100 ml. of Micropaque barium suffate dispersion 12 hr. previously. These show 2 forms of propulsive move- merit. One is based on a "systolic" action of the bowel wall, by which the contents of 3 or more haustra, contracting simultaneously as a coordinated unit, are displaced aborally into an adjoining section. The other is "peristal- tic," and arises essentially as a progressive contraction wave which advances along the colon, usually preceded by muscular relaxation. The systolic type of propulsion is chiefly seen in the first half of the colon and appears to be best adapted to transporting liquid contents. Peristalsis is most common in the transverse and ¢li~tal colon, and is much more. efficient in the propulsion of solids. One or the other of these propulsive movements is likely tO occur about once in 6 hr., and they are usually slow-moving; most of them take I0-20 min. to complete, and the bowel contents advance up to I in./min, over that period. When the movements are preceded or ac- companied by a tubular appearance of the bowel, they are given the name of mass propulsion; this may transport normal bowel contents at up to 6 int./rain. It is possible that some of the basic defects in 2 of the most important motor disorders of the colon, diverticular disease antl the irritable-colon syndrome, may be related to loc,d differences in the mechanism of propulsion. Figure I includes 9 frames from a cinefihu taken over 20 rain., which shows mass peristalsis in an ehlerlv man who had 1 normal daily bowel action. Diverticula were observed in the descending and pelvic colon. There was little interference From the Nulfieht Dvpartment of Medicine. Radcliffe h~firmar), and tile Nuffiehl Institute I't~r Medical Re.arch, Oxfgrd. England. .~u~plx~rltai hv a grant fr~rn the Medical Research Council. 488 Amer;.n Jo~nal of Dicjest;ve Diseases
-
Upload
james-ritchie -
Category
Documents
-
view
214 -
download
1
Transcript of Time-lapse cinefluorography in man

Time-Lapse Cincfluoro aphy in Man
J.~'~r.s Rl rcn le , M.A., D.M.
M LCH of the emphasis in motil i tv studies of the colon has been on quanti-
tative comparisons of intrahmfinal pressure records; efforts have been m a d e to find increasingly sophisticated means of measuring experimental re- suits. Th i s approach may be of great value in pha rmaco lo~c studies and in some clinical comparisons, but variat ion between individuals is so great that one can only draw conclusions from mean "moti l i ty indexes" derived from relat ively large groups of subjects.
Qual i ta t ive studies also may be useful in distinguishing between normal a n d abnormal bowel activity. At Oxford we have made studiest of coordi- n a t e d propulsion in the normal colon with time-lapse cinelluorography at I-rnln_ intervals in subjects who had swallowed 100 ml. of Micropaque bar ium suffate dispersion 12 hr. previously. These show 2 forms of propulsive move- merit . One is based on a "systolic" action of the bowel wall, by which the contents of 3 or more haustra, contracting simultaneously as a coordinated uni t , are displaced aborally into an adjoining section. T h e other is "peristal- t ic," and arises essentially as a progressive contract ion wave which advances a long the colon, usually preceded by muscular relaxation.
T h e systolic type of propulsion is chiefly seen in the first half of the colon a n d appears to be best adapted to transporting l iquid contents. Peristalsis is most common in the transverse and ¢li~tal colon, and is much more. efficient in the propulsion of solids. One or the other of these propulsive movements is l ikely tO occur about once in 6 hr., and they are usually slow-moving; mos t o f them take I0-20 min. to complete, and the bowel contents advance up t o I in . /min , over that period. When the movements are preceded or ac- companied by a tubular appearance of the bowel, they are given the name o f mass propulsion; this may transport normal bowel contents at up to 6 int./rain.
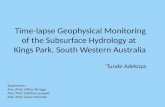
I t is possible that some of the basic defects in 2 of the most impor tant motor disorders of the colon, diverticular disease antl the irritable-colon syndrome, may be related to loc,d differences in the mechanism of propulsion. Figure I includes 9 frames from a cinefihu taken over 20 rain., which shows mass peristalsis in an ehlerlv man who had 1 normal daily bowel action. Diverticula w e r e observed in the descending and pelvic colon. T h e r e was little interference
F r o m the Nulfieht Dvpartment of Medicine. Radcliffe h~firmar), and tile Nuffiehl Institute I't~r Medical Re .a rch , Oxfgrd. England.
.~u~plx~rltai hv a grant fr~rn the Medical Research Council.
488 Amer;.n Jo~nal of Dicjest;ve Diseases

with the peristaltic movement as it l)a,~ed through tile diverticulum-bearing haustra in the descending colon, but in the Pelvic colon the peristaltic pro- gression was , topped; only when the haustrum proximal to those associated with diverticular disea.se was fur ther distended with contents from above, and responded with a systolic contraction, was the bar ium forced through the resistant section.
Williams -~ has recently shown that divertict, lar disease does not interfere with muscular relaxation ahead of a peristaltic type of propulsive movement, so that l iquid contents can be forced through divert icular segments of the bowel. Th is suggests that the obstruct ion to peristalsis of normal contents probably involves the propagation of the contraction wave itself.
T h e propulsion of solid contents against resistance by a systolic contraction of the bowel wall requires a greater mttsctdar effort than peristalsis; this causes a high local intraluminal pres, ure, and i~ may give rise to pain. An example of a painful systolic type of circular or combined muscular contraction is shown in Fig. 2.
This took place in the distal descending colon of a middle-aged patient with the irritable-colon syndrome, which had caused h im bouts of intermit tent abdomina l pain localized to this point over the previous 3-4 years. T h e figure illustrates 2 of many brief episodes of griping pain, about 15 min. apart; they represent instances in which the pain happened to coincide with a cinefluoro- gram, and in each case, the relevant frame is set between those taken 1 min. before and after it. T h e 2 series indicate that this patient 's pain was associated with a localized systolic contraction affecting 6 in. or so of the bowel, which displaced gas and l iquid contents but which failed to transport a small quant i ty of solid contents.
NuO~eld Department o[ Medicine Radcliffe lnllrmary
Oxford, England REFERENCES
1. Rrrcm~, J . .~ Colonic motor activity and bowel function. Gut In press. 2. WltuA~fS, 1. _Mass movements (mass peristalsis) and diverticular disease of the colon.
Brit ] Radiol 40:2, 1967.
[Illustrations follow]
New Ser|es, Vol. 13, No. 5, 1968 489

~IO
P
-u
uu
[~
=lu
!=u
uL
I ?
¢ =;.,-=
o,,
f t
P

\
•
~
.7
~
b \
b
16
"~ql
lg+
.,allF"
18
~ .
..
..
~
20
Fig
. 1.
P
eris
tals
is h
eld
up
at
dive
rtic
ular
ho
we!
seg
men
t.
Fra
mes
ar
e fr
om s
erie
s of
tim
e-la
pse
cinc
lhio
rogr
ams
at i
nter
vals
ind
icat
ed
(in
mim
ttes
),
Sub
ject
, w
ho
had
swal
low
ed
100
ml.
of
bar
ium
su
lfat
e 12
hr.
pr
evio
usly
, w
as p
ain-
free
an
d
had
norm
al
bow
el f
unct
ion,
but
di
scrt
ical
a w
ere
~isi
ble
in d
esce
ndin
g co
lon
at a
an
d in
pel
vic
colo
n at
b.
In
firs
t 3
fram
es p
eris
tals
is
adva
nced
sm
all
amo
tmt
of
bow
el
com
cnts
(y
) be
twc~
'n
~l
and
b;
haus
tra
in
regi
on o
f b
rela
xed
ahea
d of
y
and
beca
me
dist
ende
d w
ith
gas;
m
ore
soli
d co
mcm
s w
ere
unab
le
to
pass
th
rotl
gh.
Mas
s pe
risv
dsis
(c
) de
velo
ping
in
tr
ansv
erse
col
on,
prop
elle
d co
mcm
s in
to d
esce
ndin
g co
lon;
le
adin
g co
men
ts
(z)
pass
ed
a af
ter
abou
t I0
ra
in.
wit
h o~
dy
slig
ht
dela
y an
d so
me
e~id
ence
of
loca
l hy
perm
nus.
N
ot
unti
l ex
tra
volu
me
of c
onte
nts
was
add
ed
to y
, ca
usin
g ha
ustr
al d
iste
tlti
oll
and
sL'c
omla
t~ s
~sto
lic
type
ol
to
nltr
acti
on~
afte
r 18
ra
in.,
w
as
bari
um
forc
ed
thro
ugh
shor
t di
vcrt
icul
ar s
egm
ent
at
bl

: i ~
,i~ ¸
~: :
,E ~ :
~J
v
i
Min
s
Fig.
2.
(Con
tinu
ed o
n p.
49S
)

r..I
/ f.
/[
;~ ¢+
-,
Jr
L
'+'"+'+
$ I
'~';"
g
Fig
. 2.
ln
lcrm
itlc
nt
pain
il
l sp
asti
c co
lon.
T
wo
seri
es o
f 3
cons
ecut
ive
fram
es o
f ti
me-
laps
e ci
nefi
~lor
ogra
ph),
at
l-
rain
, il
|lcr
vals
are
sh
own:
ea
ch
illu
stra
lcs
deve
lopm
ent
of e
piso
de
of g
ripi
ng
pain
in
le
ft l
ilac
fos
sa
in
pati
ent
wit
h ir
rita
ble+
colo
n sy
mh'
o,ue
. In
bo
lh.
pain
co
inci
dt'd
w
ith
sl~c
oml
)1 t
he
~1 e
xpos
L,.,
'es
and
was
fel
t at
P
oint
P.
In
firs
t se
ries
, pa
in
was
ass
ocia
led
wit
h co
mbi
ned
circ
ular
and
lon
gitu
dina
l co
atra
ctio
n of
dis
tal
dt's
cend
ing
:olo
n,
whi
ch
caus
ed
rctr
opul
sion
of
gas
an
d so
me
liqu
id
bari
um
(a)
; so
lid
bari
um a
t b
was
not
dis
plac
oi,
so p
lopu
lsio
n m
ust
hax'
e Ix
'~n
s~st
olic
iat
ltct
ha
rt
peri
stal
tic.
In
se
cond
3
fram
es,
sim
ilar
sy
stol
ic c
ontr
acti
on
invo
lvin
g ci
rcul
ar
mus
cula
t~rc
of
abo
ut
4-6
in.
of
bo~
cl
disp
laoe
d ga
s di
stal
l)-
into
?c
ivic
col
on
(c)
at
tim
e w
hen
pain
w
as f
elt.
In
bo
th
inst
ance
s pa
in
was
id
ellt
ical
.


















