
Hookah smoking and cancer: carcinoembryonic antigen (CEA ...
Upload
manuel-diezCategory
view
212download
0
Time-Dependency of the Prognostic Effect ofCarcinoembryonic Antigen and p53 Protein inColorectal Adenocarcinoma
Manuel Dıez, M.D.1
Marina Pollan, M.D.2
Jose M. Muguerza, M.D.1
Maria J. Gaspar, M.D.3
Antonio M. Duce, M.D.1
Marıa J. Alvarez, M.D.3
Tomas Ratia, M.D.1
Pilar Hernandez, M.D.1
Antonio Ruiz, M.D.4
Javier Granell, M.D.1
1 Department of General Surgery, Prıncipe de As-turias Hospital, Alcala de Henares University, Ma-drid, Spain.
2 Epidemiology Cancer Unit, National Centre forEpidemiology, Carlos III Institute of Public Health,Madrid, Spain.
3 Department of Clinical Biochemistry, Prıncipe deAsturias Hospital, Alcala de Henares University,Madrid, Spain.
4 Department of Pathology, Prıncipe de AsturiasHospital, Alcala de Henares University, Madrid,Spain.
Presented at the VII International Symposium onBiology and Clinical Usefulness on Tumor Markers,Barcelona, Spain, February 3–6, 1999.
Address for reprints: Manuel Dıez, M.D., CirugıaGeneral, Hospital Prıncipe de Asturias, Alcala deHenares, 28805 Madrid, Spain.
Received March 8, 1999; revision received July26, 1999; accepted August 12, 1999.
BACKGROUND. This study examined the prognostic information regarding the risk
of postoperative tumor recurrence obtained by simultaneous determination of
preoperative serum carcinoembryonic antigen (CEA) and immunohistochemical
expression of p53 protein in tumor tissue from patients with colorectal carcinoma.
METHODS. A retrospective study of 174 patients (AJCC/UICC Stages I, II and III) was
conducted. Serum CEA levels were determined by an enzyme-linked immunoad-
sorbent assay. Immunohistochemical expression of nuclear p53 protein was as-
sessed in formalin fixed, paraffin embedded archival tumor tissue. The results of
both factors were categorized by clinical and histopathologic variables. The relative
prognostic significance of all factors with regard to disease free survival was
assessed by Cox proportional hazards regression analysis. The stability of the
predictive value of both markers was assessed: 1) by splitting the follow-up into
three intervals and performing separate analyses for each period and 2) graphically
by plotting the corresponding cumulative hazards ratio along the follow-up.
RESULTS. Eighty-two (47%) tumors manifested overexpression of p53 protein and
60 tumors (34.4%) exhibited elevated serum CEA levels (cutoff value of 5 ng/mL).
p53 positive immunostaing and elevated CEA levels were associated with low
cumulative disease free survival at 60 months’ of follow-up, and proved to have
independent prognostic significance. Analysis performed in different time periods
of follow-up showed that the prognostic effect of both markers was not stable over
time. The predictive significance of CEA and p53 changed along the study periods.
An elevated preoperative CEA level was an indicator of a high risk of recurrence
only during the first 2 years after surgery (hazards ratio, 3.26; 95% confidence
interval [95% CI], 1.65– 6.42). The presence of p53 immunoreactivity in the primary
tumor was an indicator of a high risk of recurrence only after the first year of
follow-up (hazards ratio, 4.02; 95% CI, 1.68 –9.6).
CONCLUSIONS. The serum CEA level and expression of p53 protein provide com-
plementary prognostic information. Time-dependency of the prognostic influence
of both parameters should be taken into consideration when establishing postop-
erative predictive estimations. Cancer 2000;88:35– 41.
© 2000 American Cancer Society.
KEYWORDS: colorectal carcinoma, p53 protein, carcinoembryonic antigen, recur-rence, prognostic factors.
H istologic stage of spread at surgical diagnosis (Dukes-based orTNM classifications) is the most important prognostic variable in
patients with colorectal carcinoma.1 However, the predictive limita-tions of these staging systems are not only well known, but areparticularly noticeable at the intermediate stages in which the major-ity of patients are found.2 Colorectal carcinoma is a heterogeneous
35
© 2000 American Cancer Society

neoplasm comprised of different cell clones, with di-verse growth rates and metastatic potential.3 This mayexplain why its clinical behavior may be different evenamong patients classified as having the same stage ofdisease.
Intensive research has targeted the possibility thatsubgroups of patients with different risks of recur-rence can be identified by biologic factors. Carcino-embryonic antigen (CEA) and the p53 gene are someof the factors that have been studied most extensively.Although both have been analyzed separately, to ourknowledge they have not yet been examined simulta-neously. In addition, CEA and p53 are both closelyrelated to clinicopathologic variables, a factor thatfurther increases the difficulty of interpreting theirrespective clinical values. In principle, these are twodifferent parameters, structurally and functionally un-related. Yet hypothetically, each would be capable offurnishing different types of information in a multi-factorial prognostic model.4,5 It is possible that simul-taneous determination of parameters representativeof different aspects of tumor biology may yield a betterprognostic evaluation than that obtained by studyingeach factor in isolation. In this study, preoperativeserum CEA levels, immunohistochemical p53 expres-sion, and ten clinicopathologic variables were exam-ined in patients with colorectal carcinoma. Concor-dance between CEA levels and p53 expression wasevaluated. In addition, the relation between all factorsand the risk of tumor recurrence was examined simul-taneously. Special interest was devoted to exploringpossible changes in prognostic value during the post-operative course.
MATERIALS AND METHODSPatientsA retrospective review was conducted on data frompatients at our hospital who had undergone surgeryfor adenocarcinoma of the large bowel and had un-dergone curative surgical resection in the period be-tween January 1993 and July 1997. Cases were deemed“curative” if the surgeon and pathologist believed thatthe entire tumor had been removed. One hundredninety-seven patients operated on during this periodmet these criteria. Three patients who died of postop-erative complications and 20 patients with incompleteevaluation of all variables analyzed were excluded,leaving a final study group of 174 patients, none ofwhom had received anticancer therapy prior to sur-gery (78 males and 96 females) (mean age, 67 years;range, 30 –92 years). Postoperative TNM stage distri-bution was: 32 patients (18.4%) with Stage I disease(T2N0M0), 88 patients (50.6%) with Stage II disease(T3–T4N0M0), and 54 patients (31%) with Stage III
disease (T1–T4N1-2M0). At the time of surgery, indi-vidual patient profiles were drawn up and stored on acomputer file (Table 1). Patients were followed regu-larly according to a predetermined schedule. The me-dian follow-up time for the entire cohort was 28months (range, 4 – 81 months). During this time, 53patients developed tumor recurrence (locoregionaland/or metastases), with 36 dying as a result. Diseasefree survival for the entire series was 83% at 12months, 69% at 24 months, 61% at 36 months, and57% at 5 years.
CEA DeterminationPreoperative serum CEA levels were determined for allpatients immediately prior to surgery. CEA levels weremeasured by enzyme linked immunoassay using acommercially available kit (ES-300; Boehringer-Mann-heim, Indianapolis, IN). The cutoff level was 5 ng/mL.
HistologySurgically removed specimens were fixed in 4% buff-ered formaldehyde solution and embedded in paraf-fin. The time of formaldehyde fixation did not exceed48 hours. Sections were stained with hematoxylin andeosin. A mean of five tissue sections of each tumorwere examined. A single pathologist categorized alltumors. Variables analyzed included tumor site, his-tologic type, grade of differentiation, extent of bowelwall invasion, lymph node involvement, tumor growthpattern, peritumoral lymphocytic infiltration, and in-tramural venous invasion.
ImmunohistochemistryRepresentative blocks of formalin fixed, paraffin em-bedded tumor tissue were cut 4-mm thick, dewaxed inxylene, and then rinsed in alcohol and graded alcohol/water mixtures. For immunohistochemical staining ofp53, rabbit polyclonal antibody CM1 (Novocastra,Newcastle-upon-Tyne, UK) against both wild and mu-tated forms was used. The primary antibody, dilutedat 1:50 at room temperature, was applied for 60 min-utes. Subsequently, pretreatment in a microwave ovenacted as an antigen retrieval system. Immunohisto-chemical staining was performed using a standardavidin-biotin alkaline phosphatase-based complex(Ultraprobe™; (Biomeda Corporation, Foster City,CA). Antibody-bound activity was detected with Fas-tRed TT (Sigma, Deisenhofen, Germany). Sections of acolon tumor of known positive immunoreactivity wereused as positive control. Only nuclear staining wasinterpreted to indicate positive p53 immunoreactivity.Cases were deemed p53 positive when any percentageof tumor cells showed immunoreactivity.
36 CANCER January 1, 2000 / Volume 88 / Number 1

The proliferative cell nuclear antigen (PCNA) la-beling index was used to measure the proliferativerate. The sections were stained using the same avidin-biotin complex with the following incubation times:30 minutes at room temperature for the anti-PCNAantibody (PC10, dilution 1:20; Dakopatts, Glostrup,Denmark) and 45 minutes for the avidin-biotin com-plex. The percentages of nuclei stained across theentire tumor section were recorded subjectively inthree categories: , 10%, 10 –50%, and . 50%.
Statistical AnalysisDifferences in the relative frequency of the variablesanalyzed were compared by means of the chi-squaretest. Time was calculated from the date of surgery tothe date of recurrence or last follow-up visit. Concor-dance between p53 and CEA was analyzed using theKappa statistic, which compares observed concor-dance between the two markers against what wouldbe expected by chance. The likelihood of tumor recur-rence was studied using the Kaplan–Meier method.
The Mantel log rank test was used to compare differ-ences. The relative prognostic importance of CEA andp53 was assessed in a Cox proportional hazards re-gression analysis, with both markers included as in-dependent variables. The remaining variables wereincluded sequentially as possible confounders, andthose that were proven to have an independent effectwere retained in the final model. Adjusted and unad-justed hazard ratios and 95% confidence intervals(95% CI) were calculated for each variable as an esti-mate of relative risk. To increase the statistical power,categories of those variables that yielded similar haz-ard ratios in the univariate analysis were collapsed. Inthe last model, we tested whether any of the two terminteractions was statistically significant.
Implicit in the Cox model is the assumption ofproportional hazards, namely, a stable prognostic ef-fect over time. To determine whether this conditionwas indeed true for the variables of interest to us (CEAand p53), crude and adjusted analyses were per-formed for each variable in different time periods of
TABLE 1Clinicopathologic Characteristics and Predictors of Disease Free Survival According to Univariate Analysis
No. ofcases p531 (%) P value
CEA >5 ng/mL (%) P value
No. ofrecurrences (%)
Disease freesurvival at 5 yrs
Hazardsratio 95% CI
CEA, 5 ng/mL 114 43 (37%) ,0.01 — — 28 (24%) 63% 15 5 ng/mL 60 39 (65%) — 25 (41%) 48% 1.96 1.14–3.36
p53Negative 92 — — 21 (22%) ,0.01 20 (21%) 71% 1Positive 82 — 39 (47%) 33 (40%) 41% 2.38 1.36–4.17
pT categorypT2 37 10 (27%) ,0.01 7 (19%) 0.05 6 (16%) 72% 1pT3 121 61 (50%) 45 (37%) 36 (29%) 60% 1.90 0.80–4.51pT4 16 11 (68%) 8 (50%) 11 (68%) 22% 5.41 2.00–14.69
pN categorypN0 117 48 (40%) 0.04 37 (39%) 0.51 27 (23%) 65% 1pN1 43 24 (55%) 17 (39%) 18 (41%) 48% 1.65 0.91–3.00pN2 14 10 (71%) 6 (42%) 8 (57%) 38% 2.72 1.23–5.99
Tumor localizationRight colon 44 18 (41%) 0.10 16 (36%) 0.90 6 (13%) 83% 1Left colon 54 31 (57%) 19 (35%) 15 (27%) 56% 2.51 0.97–6.47Rectum 76 33 (43%) 25 (33%) 32 (42%) 46% 3.47 1.45–8.31
Peritumoral lymphocytic infiltrationAbsent 91 47 (51%) 0.20 35 (38%) 0.30 35 (38%) 46% 1Present 83 35 (60%) 25 (30%) 18 (21%) 71% 0.50 0.28–0.89
Vascular invasionAbsent 122 54 (44%) 0.30 43 (35%) 0.80 32 (26%) 62% 1Present 52 28 (53%) 17 (32%) 21 (40%) 49% 1.79 1.03–3.11
Histologic typeAdenocarcinoma 149 76 (51%) 0.02 52 (34%) 0.90 45 (30%) 57% 1Mucinous 25 6 (24%) 8 (32%) 8 (32%) 59% 0.96 0.45–2.04
PCNA indexLow 30 4 (13%) ,0.01 5 (16%) 0.04 14 (46%) 39% 1Moderate-high 144 78 (54%) 55 (38%) 39 (27%) 63% 0.58 0.32–1.07
1: positive; CEA: carcinoembryonic antigen; 95% CI: 95% confidence interval; PCNA: proliferating cell nuclear antigen.
CEA and p53 in Colorectal Carcinoma/Dıez et al. 37
the follow-up (first year, second year, and the remain-ing period).6 In addition, a graphic evaluation wasperformed by plotting the cumulative hazards ratioalong the follow-up period.7 This parameter is a rea-sonable estimate of the hazards ratio and, due to itsgreater stability, is easier to plot on a graph. Theresults confirmed that there had been a change in theeffect of both markers over time. The final modeltherefore was fitted again, with the difference thatboth markers were included as time-dependent vari-ables, yielding estimates of their effect at a specifictime during the follow-up.
A separate blind clinical follow-up for survivaldata, histopathologic evaluation, and statistical anal-ysis purposes was conducted by different authors, re-spectively.
RESULTSClinicopathologic Variables, p53, and CEAEighty-two tumors (47%) manifested nuclear overex-pression of p53 protein. As shown in Table 1, tumorcell staining was associated significantly with trans-mural tumoral infiltration into the bowel wall, positivelymph node status, histologic type, and high prolifer-ation rate. No correlation with tumor site, vascularinvasion, peritumoral lymphocytic infiltration, or tu-mor growth pattern was detected.
Sixty tumors (34.4%) exhibited elevated serumCEA levels. The presence of transmural infiltration ofthe neoplasms and a high proliferation rate were as-sociated significantly with elevated serum CEA con-centration (Table 1).
Relation between p53 and CEAResults of p53 staining and serum CEA showed agree-ment in 110 tumors (63.2%); 39 showed simulta-
neously elevated CEA and p53 positivity, whereas 71showed normal CEA and negative p53 (Table 1). Therewas a fair, yet statistically significant, concordancebetween p53 and CEA (kappa 5 0.25; P 5 0.0003).
Serum CEA concentration was higher in patientswith p53 positive tumors (mean, 15.8 ng/mL; standarddeviation [SD]: 39; median; 4.3) versus patients withp53 negative tumors (mean, 5.5 ng/mL; SD: 8.5; me-dian; 2.8) (P 5 0.02).
Disease Free Survival by Univariate Analysisp53 positive tumors showed a higher recurrence rate(33 cases; 40.2%) than p53 negative tumors (20 cases;21.7%) (P 5 0.01). Cumulative disease free survival at60-month follow-up was lower for p53 positive tumors(41% vs. 71%) (P 5 0.002) (Table 1).
The recurrence rate was higher among patientswith preoperative elevated serum CEA levels (25 cases;41.6%) than among patients with normal levels (28cases; 18.7%) (P 5 0.03). Cumulative disease free sur-vival at 60-month follow-up was significantly lower forpatients with high CEA levels (48% vs. 63%, respec-tively) (P 5 0.02) (Table 1).
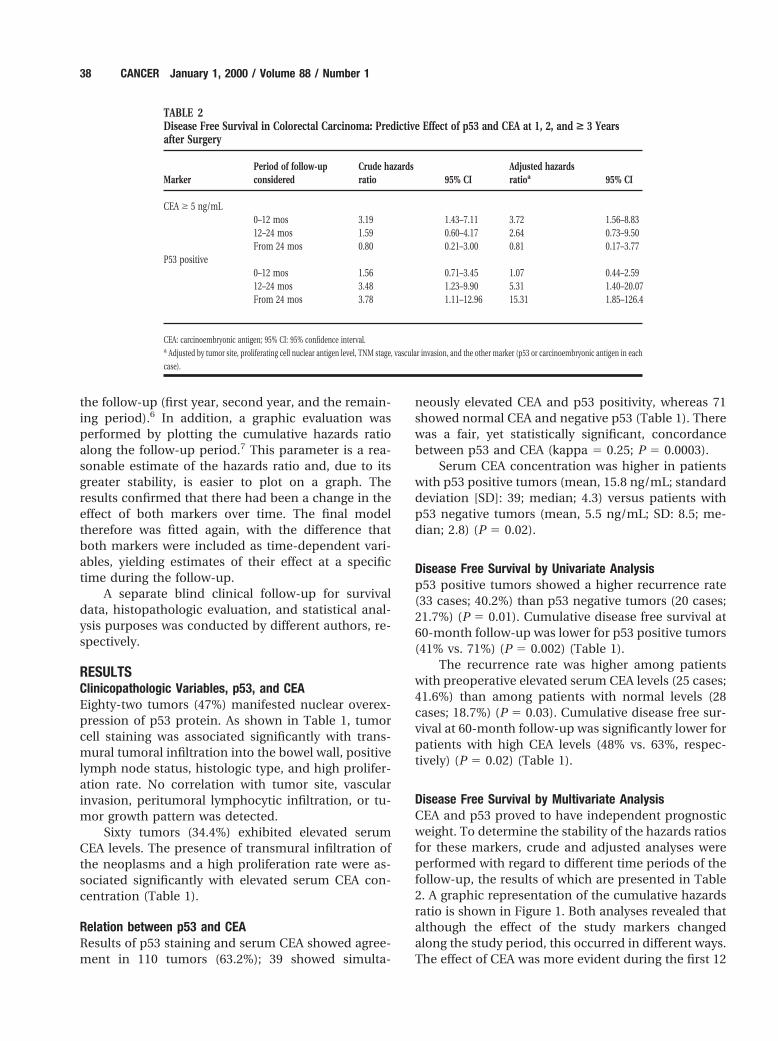
Disease Free Survival by Multivariate AnalysisCEA and p53 proved to have independent prognosticweight. To determine the stability of the hazards ratiosfor these markers, crude and adjusted analyses wereperformed with regard to different time periods of thefollow-up, the results of which are presented in Table2. A graphic representation of the cumulative hazardsratio is shown in Figure 1. Both analyses revealed thatalthough the effect of the study markers changedalong the study period, this occurred in different ways.The effect of CEA was more evident during the first 12
TABLE 2Disease Free Survival in Colorectal Carcinoma: Predictive Effect of p53 and CEA at 1, 2, and > 3 Yearsafter Surgery
MarkerPeriod of follow-upconsidered
Crude hazardsratio 95% CI
Adjusted hazardsratioa 95% CI
CEA $ 5 ng/mL0–12 mos 3.19 1.43–7.11 3.72 1.56–8.8312–24 mos 1.59 0.60–4.17 2.64 0.73–9.50From 24 mos 0.80 0.21–3.00 0.81 0.17–3.77
P53 positive0–12 mos 1.56 0.71–3.45 1.07 0.44–2.5912–24 mos 3.48 1.23–9.90 5.31 1.40–20.07From 24 mos 3.78 1.11–12.96 15.31 1.85–126.4
CEA: carcinoembryonic antigen; 95% CI: 95% confidence interval.a Adjusted by tumor site, proliferating cell nuclear antigen level, TNM stage, vascular invasion, and the other marker (p53 or carcinoembryonic antigen in each
case).
38 CANCER January 1, 2000 / Volume 88 / Number 1

months after surgery, after which time it decreasedand subsequently fell to nil after 2 years. In contrast,the effect of p53 was not evident during the first yearof the study, yet its importance increased thereafter.
The final model was adapted to include a time-dependent effect for p53 and CEA (Table 3). TNMstage, tumor localization, and vascular invasion (asnegative risk factors) and PCNA (as a protective factor)attained statistically significant independent prognos-tic value. The two study markers had prognostic val-ues that changed in opposite directions with time. Anincreased CEA level implied a 3.26-fold higher risk ofrecurrence (95% CI, 1.65– 6.42) during the first andsecond years of follow-up (CEA level being no longerimportant after this period). Conversely, the presenceof p53 immunoreactivity indicated a 4.02-fold higherrisk of recurrence after the first year (95% CI, 1.68 –9.6)as compared with nonimmunoreactive tumors. Noneof the interaction terms between the variables provedto be statistically significant. Analysis performed onpatients with Stage II tumors and on patients withStage III tumors, separately, confirmed that the time-dependency of the predictions of CEA and p53 waspresent in both populations (Table 4).
DISCUSSIONAlthough tumor stage can furnish overall predictions,it is rather limited with regard to predicting diseaseprogression in an individual patient. It is indicative ofthe anatomic level reached by a tumor. Evidence ofthe dependence of tumor behavior on biologic char-acteristics (modification of antigen expression, prolif-eration kinetics, or genetic alterations) has been re-ported.3,5 Important data for understanding the
oncogenic process have been forthcoming. Hypothet-ically, a score derived using a multiple regression ap-proach that combined anatomic description of tumorspread and assessment of tumor aggressiveness mightgenerate a patient specific prognostic index in thefuture. However, prior to this an important step wouldbe to ascertain the relation between prognostic fac-tors, something that to our knowledge until now hasbeen analyzed inadequately.8,9 Reports generally donot take into account biomarkers, which other studiesclaim to be dominant.
Serum CEA assay is a common preoperative andfollow-up practice in colorectal carcinoma patients.CEA is a glycoprotein member of the immunoglobulingene family. As such, it functions as a homotypicalintercellular adhesion molecule that promotes cell ag-gregation.10 Adenocarcinomas overexpress CEA, andCEA may facilitate metastasis of colorectal carcinoma.Elevated preoperative serum levels are associated withhigh rates of recurrence and cancer mortality. Persis-tently elevated postoperative levels may indicate in-complete surgical resection or metastatic disease.11–13
CEA is the serum tumor marker prototype: cheap,simple, and informative, with a technique that is easy
FIGURE 1. Ratio between cumulative risk of recurrence according to carci-
noembryonic antigen (CEA) (left) and p53 levels (right). Point estimators are
shown as dots and smoothed trend is shown as a solid line.
TABLE 3Prognostic Factors for Disease Free Survival in Colorectal CarcinomaAccording to the Multivariate Model
VariableHazardsratio 95% CI P value
CEA, 5 ng/mL 1$ 5 ng/mL
0–24 mos 3.26 1.65–6.42 0.001. 24 mos 1.13 0.28–4.47 0.866
p53Negative 1Positive
0–12 mos 1.50 0.63–3.56 0.358. 12 mos 4.02 1.68–9.60 0.002
Tumor siteColon 1Rectum 2.22 1.27–3.89 0.005
TNM StageI 1II 1.54 1.02–2.34 0.042III 2.37 1.03–5.46 0.042
Vascular invasionNo 1Yes 2.18 1.20–3.98 0.011
PCNA indexLow 1Moderate-high 0.22 0.10–0.46 0.001
95% CI: 95% confidence interval; CEA: carcinoembryonic antigen; PCNA: proliferating cell nuclear
antigen.
CEA and p53 in Colorectal Carcinoma/Dıez et al. 39

to standardize. We believe that it should not be dis-carded in light of the current array of prognostic fac-tors. p53 is a tumor suppressor gene that plays a keyrole in the control of the cell cycle. Alteration of thisgene is a common event in colorectal carcinoma andhas been associated with adverse postoperative out-come and poor survival.14 –16 This may be due to theloss of wild-type p53 tumor suppressor function, ra-dioresistance or chemoresistance, or acquisition ofoncogenic properties.17,18
The results of our study indicate that althoughconcordance between CEA and p53 may be low, itnonetheless is statistically greater than what would beexpected by chance. However, it appears evident that,given the dispersion of results, knowledge of a CEAresult would not enable one to forecast the result ofp53. The greater coincidence of negative results, with40.8% of patients simultaneously showing a normalserum CEA concentration and absence of p53 immu-noreactivity, simply could be due to the low relativeincidence rate of positivity in both factors.
On the basis of the multivariate analysis, CEA andp53 furnish independent and mutually complemen-tary prognostic information regarding risk of recur-rence, ancillary to that yielded by the histopathologicfactors on which tumor stage is based. This findingsupports the usefulness of simultaneous determina-tion of parameters that are representative of different
aspects of tumor biology. However we believe that thesingle finding of most relevance in our study is the factthat CEA and p53 display a changing influence onrecurrence with time (i.e., a time-dependency). Theeffect of CEA is evident only during the first 2 yearsafter surgery. In contrast, the effect of p53 is not evi-dent during the first postoperative year; its impor-tance increases thereafter. The results do indeed allowa trend to be discerned. Marker values at the com-mencement of treatment indicate a different risk ofrecurrence for each period of postoperative follow-up.Although to our knowledge the precise mechanismsare not known, each marker’s biologic properties maybe reflected in this phenomenon. Serum CEA concen-tration is related to tumor mass. It would appear log-ical that preoperative CEA determination in the typeof patient under study might have short term prog-nostic value, linked to the likelihood of performingcomplete surgical resection in the absence of localand/or distal microscopic residual disease. In con-trast, p53 is a medium term prognostic parameter andappears to act much like a factor linked to tumoraggressiveness and progression.
Time-dependency may have important implica-tions for the analysis of prognostic factors. Short termpostoperative predictions do not necessarily coincidewith those reported for a more prolonged time. To ourknowledge this observation has not previously been
TABLE 4Prognostic Factors for Disease Free Survival in Colorectal Carcinoma According to the Multivariate ModelCategorized by Stage
Variable
Stage II Stage III
HR 95% CI P value HR 95% CI P value
CEA, 5 ng/mL 1 1$ 5 ng/mL
0–24 mos 2.74 0.85–8.83 0.092 5.31 1.83–15.4 0.001. 24 mos 0.59 0.05–6.57 0.664 1.39 0.12–15.6 0.789
p53Negative 1 1Positive
0–12 mos 1.77 0.48–6.51 0.393 0.91 0.28–3.01 0.880. 12 mos 3.34 0.82–13.7 0.093 7.13 1.46–34.8 0.015
Tumor siteColon 1 1Rectum 2.97 1.18–7.49 0.021 1.51 0.65–3.50 0.337
Vascular invasionNo 1 1Yes 2.43 0.89–6.65 0.084 3.38 1.23–9.29 0.018
PCNA indexLow 1 1Moderate-high 0.35 0.11–1.13 0.079 0.18 0.05–0.65 0.008
HR: hazards ratio; 95% CI: 95% confidence interval; CEA: carcinoembryonic antigen; PCNA: proliferating cell nuclear antigen.
40 CANCER January 1, 2000 / Volume 88 / Number 1

made in connection with colorectal carcinoma, al-though similar findings have been reported in patientswith breast carcinoma.19 It is feasible that differencesin the duration of the observation period may explainin part discrepancies regarding the prognostic value ofp53 immunohistochemistry.20 –22
The combination of prognostic factors represen-tative of different aspects of tumor biology (such asCEA and p53 immunostaining) furnishes a greater de-gree of prognostic information in the case of patientswho undergo surgery for colorectal carcinoma thanthat obtained through examining the respective fac-tors in isolation. CEA and p53 have a changing influ-ence on recurrence with time. In the future, statisticalanalysis of survival time data that take time-depen-dency into consideration might become an increas-ingly acknowledged means of evaluating the effects ofprognostic factors.
REFERENCES1. Abulafi AM, Williams NS. Local recurrence of colorectal
cancer: the problem, mechanism, management and adju-vant therapy. Br J Surg 1994;81:7–19.
2. Casillas S, Pelley RJ, Milsom JW. Adjuvant therapy for colo-rectal cancer. Dis Colon Rectum 1997;40:977–92.
3. Johnson PG, Allegra CJ. Colorectal cancer biology: clinicalimplications. Semin Oncol 1995;22:418 –32.
4. Strauss G, Kwiatkowski D, Harpole D, Lynch T, Skarin A,Sugarbaker D. Molecular and pathological markers in stageI non-small cell lung cancer. J Clin Oncol 1995;13:1265–79.
5. Bosman F. Prognostic value of pathological characteristicsof colorectal cancer. Eur J Cancer 1995;31A:1216 –21.
6. Breslow NE, Day EN. Statistical methods in cancer research.Volume II. The analysis of cohort studies. Lyon, France:IARC Scientific Publications, 1987.
7. Hess KR. Graphical methods for assessing violations of theproportional hazards assumption in Cox regression. StatMed 1995;14:1707–23.
8. Nakamura T, Tabuchi Y, Nakae S, Ohno M, Saitoh Y. Serumcarcinoembryonic antigen levels and proliferating cell nu-clear antigen labelling index for patients with colorectalcarcinoma. Cancer 1996;77:1741– 6.
9. Bhatavdekar J, Patel D, Ghosh N, Chikhlikar P, Trivedi T,Suthar T, et al. Coexpression of bcl-2, c-myc, and p53 on-
coproteins as prognostic discriminants in patients withcolorectal carcinoma. Dis Colon Rectum 1997;40:785–90.
10. Pignatelli M, Vessey C. Adhesion molecules. Novel molecu-lar tools in tumor pathology. Hum Pathol 1994;25:849 –56.
11. Wang JY, Reiping T, Ming J. Value of carcinoembryonicantigen in the management of colorectal cancer. Dis ColonRectum 1994;37:272–7.
12. McCall J, Black R, Rich C, Harvey J, Baker R, Watts J, et al.The value of serum carcinoembryonic antigen in predictingrecurrent disease following curative resection of colorectalcancer. Dis Colon Rectum 1994;37:875– 81.
13. American Society of Clinical Oncology Tumor Marker ExpertPanel. Clinical practice guidelines for the use of tumormarkers in breast and colorectal cancer. J Clin Oncol 1996;14:2843–77.
14. Pricolo VE, Finkelstein SD, Hansen K, Cole BF, Kirby IB.Mutated p53 gene is an independent adverse predictor ofsurvival on colon carcinoma. Arch Surg 1997;132:371–5.
15. Remvikos Y, Tominaga O, Hammel P, Laurent-Puig P,Salmon RJ, Dutrillaux B, et al. Increased p53 protein contentof colorectal tumors correlates with poor survival. Br J Can-cer 1992;66:758 – 64.
16. Dıez M, Enriquez JM, Camunas J, Gonzalez A, Gutıerrez A,Muguerza JM, et al. Prediction of recurrence in B-C stages ofcolorectal cancer by p53 protein nuclear expression in com-parison with standard pathological features. Eur J Surg On-col 1995;21:635–9.
17. Velculescu V, El-Deiry W. Biological and clinical importanceof the p53 tumor suppressor gene. Clin Chem 1996;42:858 –68.
18. Chang F, Syrjanen S, Syrjanen K. Implications of the p53tumor-suppressor gene in clinical oncology. J Clin Oncol1995;13:1009 –22.
19. Yoshimoto M, Sakamoto G, Ohasshi Y. Time dependency ofthe influence of prognostic factors on relapse in breastcancer. Cancer 1993;72:2993–3001.
20. Smith DR, Yi C, Goh HS. Prognostic significance of p53overexpression and mutation in colorectal adenocarcino-mas. Br J Cancer 1996;74:216 –23.
21. Mulder J, Baas IO, Polak MM, Goodman SN, Offerhaus GJA.Evaluation of p53 protein expression as a marker for long-term prognosis in colorectal carcinoma. Br J Cancer 1995;71:1257– 62.
22. Poller DN, Baxter KJ, Shepherd NA. P53 and Rb1 proteinexpression: are they prognostically useful in colorectal can-cer? Br J Cancer 1997;75:87–93.
CEA and p53 in Colorectal Carcinoma/Dıez et al. 41


















