Tickborne Diseases in Children in the United States
19
Tickborne Diseases in Children in the United States Jennifer S. Read, MD, MS, MPH, DTM&H* † *Department of Pediatrics, University of Vermont Medical Center, Burlington, VT † Infectious Disease Epidemiology, Vermont Department of Health, Burlington, VT Practice Gaps The most common tick-borne infections in the United States are Lyme disease, ehrlichiosis, anaplasmosis, Rocky Mountain spotted fever, and babesiosis. The epidemiology of these infections in the United States is integrally related to the geographic distribution and seasonality of the tick vector of each of the infections. Because these infections can be very serious and sometimes fatal, and because of the inherent delay in obtaining laboratory confirmation (especially with serologic assays requiring acute and convalescent titers), considering early implementation of empirical treatment based on the patient’s clinical presentation is extremely important. Prevention of acquisition of tick- borne diseases requires avoiding tick-infested areas or, if this is not possible or desired, implementing steps to decrease the likelihood of tick bites and the duration of tick attachment. Objectives After completing this article, readers should be able to: 1. Understand the etiologic organisms and the associated ticks responsible for transmission, the geographic distribution of and the reported infections associated with the ticks in the United States, and the seasonality and incubation periods of tick-borne infections in the United States. 2. Recognize the clinical manifestations and laboratory abnormalities associated with the infections, especially as they relate to children. 3. Plan for the diagnosis, treatment, and prevention of these infections. INTRODUCTION Vector-borne diseases, caused by microorganisms transmitted by insects and ticks, are major causes of morbidity and mortality globally. In the United States, vector-borne diseases are occurring more frequently and represent a significant public health concern. (1) The numbers of reported vector-borne disease cases in the United States (tick-borne, mosquito-borne, and flea-borne diseases) are AUTHOR DISCLOSURE Dr Read has disclosed no financial relationships relevant to this article. This commentary does not contain a discussion of an unapproved/investigative use of a commercial product/device. ABBREVIATIONS CSF cerebrospinal fluid EM erythema chronicum migrans IFA immunofluorescent antibody Ig immunoglobulin RMSF Rocky Mountain spotted fever PCR polymerase chain reaction Vol. 40 No. 8 AUGUST 2019 381 at Health Sciences Library, Stony Brook University on June 3, 2020 http://pedsinreview.aappublications.org/ Downloaded from
Transcript of Tickborne Diseases in Children in the United States

Tickborne Diseases in Childrenin the United States
Jennifer S. Read, MD, MS, MPH, DTM&H*†
*Department of Pediatrics, University of Vermont Medical Center, Burlington, VT†Infectious Disease Epidemiology, Vermont Department of Health, Burlington, VT
Practice Gaps
The most common tick-borne infections in the United States are Lyme
disease, ehrlichiosis, anaplasmosis, Rocky Mountain spotted fever, and
babesiosis. The epidemiology of these infections in the United States is
integrally related to the geographic distribution and seasonality of the tick
vector of each of the infections. Because these infections can be very
serious and sometimes fatal, and because of the inherent delay in
obtaining laboratory confirmation (especially with serologic assays
requiring acute and convalescent titers), considering early
implementation of empirical treatment based on the patient’s clinical
presentation is extremely important. Prevention of acquisition of tick-
borne diseases requires avoiding tick-infested areas or, if this is not
possible or desired, implementing steps to decrease the likelihood of tick
bites and the duration of tick attachment.
Objectives After completing this article, readers should be able to:
1. Understand the etiologic organisms and the associated ticks
responsible for transmission, the geographic distribution of and the
reported infections associated with the ticks in the United States, and
the seasonality and incubation periods of tick-borne infections in the
United States.
2. Recognize the clinical manifestations and laboratory abnormalities
associated with the infections, especially as they relate to children.
3. Plan for the diagnosis, treatment, and prevention of these infections.
INTRODUCTION
Vector-borne diseases, caused by microorganisms transmitted by insects and
ticks, are major causes of morbidity and mortality globally. In the United States,
vector-borne diseases are occurring more frequently and represent a significant
public health concern. (1) The numbers of reported vector-borne disease cases in
the United States (tick-borne, mosquito-borne, and flea-borne diseases) are
AUTHOR DISCLOSURE Dr Read has disclosedno financial relationships relevant to thisarticle. This commentary does not contain adiscussion of an unapproved/investigativeuse of a commercial product/device.
ABBREVIATIONS
CSF cerebrospinal fluid
EM erythema chronicum migrans
IFA immunofluorescent antibody
Ig immunoglobulin
RMSF Rocky Mountain spotted fever
PCR polymerase chain reaction
Vol. 40 No. 8 AUGUST 2019 381 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

shown in Table 1. (1) The reported incidence of vector-borne
diseases most likely significantly underestimates the actual
occurrence of these diseases; some individuals with vector-
borne infections may be asymptomatic or, if symptomatic,
may not seek medical care.
This review addresses the most common tick-borne
diseases reported in the United States, (1) specifically, Lyme
disease, ehrlichiosis and anaplasmosis, spotted fever rick-
ettsiosis, including Rocky Mountain spotted fever (RMSF),
and babesiosis. Specifically, the following are discussed: the
organisms and the associated ticks responsible for trans-
mission; the geographic distribution of and the reported
infections associated with the ticks in the United States;
the seasonality of tick-borne infections in the United States;
the infections’ incubation periods; the clinical manifes-
tations and laboratory abnormalities associated with the
infections, especially as they relate to children; and the
diagnosis, treatment, and prevention of these infections.
LYME DISEASE
Lyme disease is the most common tick-borne infection in
the United States. (2) Over a 12-year period ending in 2016,
402,502 cases of Lyme disease were reported in the United
States. (1) Table 2 summarizes characteristics of Borrelia
burgdorferi sensu stricto (B burgdorferi), the causative organ-
ism of Lyme disease in the United States. The first report in
the United States of the skin lesion characteristic of Lyme
disease, erythema chronicummigrans (EM), was published
in 1970. (3) Subsequently, the full spectrum of clini-
cal manifestations of Lyme disease, including EM, was
described in 1977. (4) B burgdorferi, a spirochete in the
family Spirochaetaceae, (5) was first isolated in 1982. (6)
Another Borrelia species (Borrelia miyamotoi) was first iden-
tified in Japan in the 1990s, (7) and subsequently the first
case in the United States was described. (8)
B burgdorferi infection is transmitted by the blacklegged
tick (Ixodes scapularis) (Fig 1) and the western blacklegged
tick (Ixodes pacificus). (2) B miyamotoi is transmitted by the
same tick vectors as B burgdorferi. (9)(10)(11)(12) The season-
ality of Lyme disease is summarized in Table 2. (5) In the
United States, most cases of Lyme disease are reported from
2 regions: 1) New England through the mid-Atlantic states
and 2) the upper Midwest states (Table 2, Fig 2). (5)(13) B
miyamotoi infections have similar seasonality and distribu-
tion as Lyme disease cases. (9)(10)(12)
The incubation period and clinical manifestations of, and
the laboratory abnormalities associated with, Lyme disease
are summarized in Table 3. (2)(5)(13) The clinical manifes-
tations of Lyme disease occur in 3 stages: early localized,
early disseminated, and late. (5) Early localized disease
(2)(5)(13) is characterized by EM at the site of the tick bite
and systemic manifestations. In children, EM is the most
commonmanifestation of Lyme disease. Some patients with
large EM lesions are misdiagnosed as having cellulitis. Only
a minority of patients have the classic bull’s-eye appearance
(concentric rings). Several weeks after the tick bite, the next
stage of Lyme disease (early disseminated disease) (2)(5),(13)
TABLE 1. Vector-borne Disease Cases Reportedto the National Notifiable DiseaseSurveillance System—US States andTerritories, 2004–2016
DISEASE NO. CASES
Tick-borne diseases
Lyme disease 402,502
Anaplasmosis/ehrlichiosis
39,959
Spotted feverrickettsiosis
37,376
Babesiosis 9,631
Tularemia 2,102
Powassan virus 101
Subtotal 491,671
Mosquito-borne diseases
Dengue viruses 46,692
Zika virus 41,680
West Nile virus 31,919
Malaria 20,167
Chikungunya virus 9,081
California serogroupviruses
1,063
St Louis encephalitisvirus
133
Eastern equineencephalitis virus
106
Yellow fever virus 1
Subtotal 150,842
Flea-borne disease(plague)
89
Total 642,602
Adapted from Rosenberg R, Lindsey NP, Fischer M, et al. Vital signs: trendsin reported vectorborne disease cases—United States and Territories,2004-2016. MMWR Morb Mortal Wkly Rep. 2018;67(17):496–501.
382 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

may manifest as multiple EM lesions. Other clinical man-
ifestations may occur (with or without multiple EM lesions),
including neurologic, cardiac, and systemic manifestations.
Late Lyme disease (2)(5)(13) occurs in individuals who were
not treated during the early localized or early disseminated
stages of infection. Several months may pass between a tick
bite and late Lyme disease manifestations. Children with
late Lyme disease usually present with arthritis. Because
some patients with Lyme disease do not report a history of
clinical features of early localized or early disseminated
TABLE 2. Tick-borne Diseases in Children in the United States:Organisms, Vectors, Seasonality, and Geographic Distribution
DISEASE ORGANISM VECTOR SEASONALITY GEOGRAPHIC DISTRIBUTION
Lyme disease Borrelia burgdorferi sensustricto (B burgdorferi)
Blacklegged tick (Ixodesscapularis) and the westernblacklegged tick (Ixodespacificus)
Most early localized, earlydisseminated disease: April–October
>50% during June and July
>90% of cases reported fromNew England (Maine, NewHampshire, Vermont,Connecticut, Rhode Island,Massachusetts) and thenortheastern and mid-Atlantic states (Delaware,Maryland, New Jersey, NewYork, Pennsylvania, Virginia)
Less frequently, Lyme disease isreported from the upperMidwest (especiallyMinnesota and Wisconsin)
Some cases have beenreported from northernCalifornia, Oregon, andWashington
Ehrlichiosis Ehrlichia chaffeensis Lone star tick (Amblyommaamericanum)
Most infections: April–September
Predominantly southeast,south central, east coaststates
Peak incidence: May–July Highest incidence in Arkansas,Delaware, Missouri,Oklahoma, Tennessee,Virginia
Ehrlichia ewingii Lone star tick (A americanum) Most infections: April–September
Mostly southeastern, southcentral, midwestern states
Peak incidence: May–JulyEhrlichia muris–likeorganism
Possibly blacklegged tick(I scapularis)
Highest incidence: April–September
Minnesota, Wisconsin
Can occur year-round in areaswith endemic disease
Anaplasmosis Anaplasmaphagocytophilum
Blacklegged tick (I scapularis) orwestern blacklegged tick(I pacificus)
Most infections: June–November
Most frequently reported fromnortheastern and uppermidwestern states
RMSF Rickettsia rickettsii American dog tick (eastern,central, western United States)
Highest incidence: April–September (but, in areas withendemic disease, can occuryear-round)
Throughout most of thecontinental United States
Rocky Mountain wood tick inRocky Mountain states
In 2002–2012, 5 statesaccounted for 63% of cases(Arkansas, Missouri, NorthCarolina, Oklahoma,Tennessee)
Brown dog tick in southwesternUnited States and along US-Mexico border
Has become more common inparts of Arizona
Babesiosis Babesia microti and otherBabesia species
Blacklegged tick (I scapularis) Most infections during latespring, summer, or fall
Northeast (especiallyConnecticut, Massachusetts,New Jersey, New York,Rhode Island; also, Maine,Pennsylvania)
Upper Midwest (Minnesota andWisconsin)
Vol. 40 No. 8 AUGUST 2019 383 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

Lyme disease, arthritis and other manifestations of late
Lyme disease may occur in patients without a history of
EM. Patients with B miyamotoi infections most commonly
report systemic manifestations (fatigue, headache, arthral-
gia, myalgia, nausea) as well as high fever (temperature
>104°F [>40°C]), which may be recurrent, and chills.
(14)(15)(16)(17)(18) Laboratory abnormalities observed in
patients with Lyme disease (13) include an elevated eryth-
rocyte sedimentation rate, elevated hepatic transaminase
concentrations, and microscopic hematuria or proteinuria.
With Lymemeningitis, the cerebrospinal fluid (CSF) usually
has a lymphocytic pleocytosis, a slightly elevated protein
concentration, and a normal glucose concentration. Leuko-
penia, thrombocytopenia, and elevated liver enzyme con-
centrations have been reported with B miyamotoi infection.
(19)
Diagnostic assays for Lyme disease are summarized in
Table 4. (2)(5)(13) Of note, the diagnosis of Lyme disease
depends heavily on a compatible clinical presentation along
with plausible geographic exposure to the tick vector.
Patients with early Lyme disease with EM may be treated
presumptively (and serologic testing is not recommended).
(5) The laboratory diagnosis of Lyme disease involves dem-
onstration of B burgdorferi antibodies in serum. A 2-step
laboratory testing protocol is recommended. First, an
enzyme-linked immunosorbent assay or an immunofluo-
rescent antibody (IFA) assay is performed. If the result of the
antibody assay is positive or equivocal, the second-tier
standardized Western immunoblot is necessary. If Lyme
meningitis is suspected, the CSF can be tested for immu-
noglobulin (Ig) M or IgG antibodies. There are several
important considerations for serologic testing for Lyme
disease. (13) First, antibody titers are often negative if the
serum specimen was obtained during the first few weeks of
infection. Second, in those with more than 1 month of
illness, only IgG testing should be performed (not IgM
testing). Third, because of antibody persistence, a single
positive serologic assay result cannot reliably distinguish
between previous and current infection. Fourth, serologic
assays cannot be used to assess response to treatment. Fifth,
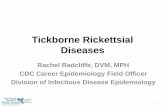
Figure 1. Ticks that commonly bite humans. (Reprinted with permission from Centers for Disease Control and Prevention. Tickborne Diseases of theUnited States. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2018.)
384 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

and most importantly, serologic assays may yield false-
positive results; there may be cross-reactivity with anti-
bodies to other spirochetes and to certain viruses (including
Epstein-Barr virus and varicella) and there may be false-
positive results in patients with certain autoimmune dis-
eases (eg, systemic lupus erythematosus). It is, therefore,
important to perform Lyme disease testing with an appro-
priate epidemiologic history of potential contact with tick
vectors associated with transmitting Lyme disease and
compatible clinicalmanifestations. The laboratory diagnosis
of B miyamotoi infection can be accomplished by identifi-
cation of the spirochetes on blood smears or CSF samples (if
neurologic manifestations), through polymerase chain reac-
tion (PCR) assays performed on blood or CSF samples, and
with serologic assays. (19)
Treatment of Lyme disease is summarized in Table 4.
(5)(13) Antibiotic therapy for patients who are asymptom-
atic (but seropositive) or who have nonspecific symptoms
is not recommended. As noted previously herein, patients
with EM can be treated presumptively. B miyamotoi in-
fections can be treated with doxycycline or amoxicillin.
(20)
EHRLICHIOSIS AND ANAPLASMOSIS
Between 2004 and 2016, 39,959 cases of ehrlichiosis and
anaplasmosis were reported in the United States (1) Table 2
summarizes characteristics of the causative organisms.
Ehrlichiosis and anaplasmosis are caused by infections
with Gram-negative cocci of the family Anaplasmataceae,
which are obligate intracellular bacteria. (21)(22)(23)(24)
In the United States, ehrlichiosis is caused by 1 of 3
different species of Ehrlichia (Ehrlichia chaffeensis, Ehrlichia
ewingii, and Ehrlichia muris eauclairensis). E chaffeensis, first
described in 1987, is the most common cause of human
ehrlichiosis in the United States. (25) The other species of
Ehrlichia were recognized in the 1990s. (26)(27) Anaplas-
mosis in the United States is caused by Anaplasma phag-
ocytophilum and was first described in humans in the
1990s. (28) These organisms have a tropism for leuko-
cytes (Ehrlichia species: usually monocytes or tissue mac-
rophages; A phagocytophilum: usually granulocytes). (21)(22)
(23)(24)
Both Ehrlichia species and A phagocytophilum are trans-
mitted by ticks, but A phagocytophilum also can be transmitted
Figure 2. Lyme disease cases reported to the Centers for Disease Control and Prevention, 2016. (Reprinted with permission from Centers for DiseaseControl and Prevention. Tickborne Diseases of the United States. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2018.)
Vol. 40 No. 8 AUGUST 2019 385 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

TABLE3. Tick-borne Diseases in Children in the United States: IncubationPeriod, Clinical Manifestations, and Laboratory Abnormalities
DISEASEINCUBATIONPERIOD CLINICAL MANIFESTATIONS LABORATORY ABNORMALITIES
Lyme disease 3–32 d (median,11 d)
Early localized stage:• EM rash:
o Begins with a red macule or papule, whichsubsequently (over a period of days to weeks)expands to form a large, erythematous, annularlesion, with or without central clearing
o Usually painless (but not always) and usuallynonpruritic
o Variable in terms of size and shape (size usually‡5 cm)
o May have a central vesicular component, pur-plish discoloration, or necrosis
• Systemic manifestations: fever (usually mild),malaise, headache, myalgia, arthralgia
Early disseminated stage:• Multiple EM lesions (similar to but smaller thanprimary lesion)
• Other manifestations (with or without EM lesions):o Cranial nerve palsies (usually cranial nerve VII)o Lymphocytic meningitis (oftenwith papilledemaor cranial neuropathy)
o RadiculitisoCarditis (atrioventricular block of varying degree)(occurs less commonly in children)
o Systemic manifestations: fever (usually mild),fatigue, headache, myalgia, arthralgia
Late disseminated stage:• Arthritis (usually monoarticular or pauciarticular;affecting large joints [especially knees])
• Other rare manifestations:o Pseudotumor cerebrio Encephalitiso Encephalopathyo Polyneuropathy
• Elevated erythrocyte sedimentation rate• Mildly elevated hepatic transaminaseconcentrations
• Microscopic hematuria or proteinuria• If Lyme meningitis: CSF typically shows lympho-cytic pleocytosis, slightly elevated protein, andnormal glucose
Ehrlichiosis 5–14 d • Systemic manifestations: fever, chills, malaise,headache, myalgia, nausea
• Gastrointestinal manifestations (abdominal pain,vomiting, diarrhea) (more common in children)
• Rash (petechial, maculopapular, or diffuseerythema, usually affecting the trunk andextremities) (more common in children)
• Severe manifestations: toxic shock– or septicshock–like syndromes, renal failure, hepatic failure,coagulopathies, hemophagocyticlymphohistiocytosis
• Leukopenia and thrombocytopenia• Anemia – occurs later than leukopenia orthrombocytopenia
• Hyponatremia• Elevated serum hepatic transaminaseconcentrations
• CSF abnormalities (pleocytosis with predominanceof lymphocytes, increased total proteinconcentration)
• Morulae may be visualized during acute illness
Anaplasmosis 5–14 d • Systemic manifestations: see ehrlichiosis• Gastrointestinal and CNS manifestations lessfrequent than in ehrlichiosis
• Rash in <10%• Severe manifestations (see ehrlichiosis), lesscommon than in ehrlichiosis
• Leukopenia and thrombocytopenia• Hyponatremia• Elevated serum hepatic transaminaseconcentrations
• Morulae may be visualized during acute illness
Continued
386 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

through blood product transfusion. (21)(22)(23)(24) Tick vec-
tors in theUnited States for these organisms (Table 2) include
the lone star tick (Amblyomma americanum) (Fig 1), the
blacklegged tick (I scapularis) (Fig 1), and the western black-
legged tick (I pacificus). (21)(22)(23)(24) The seasonality
(21)(22)(23)(24) and geographic location (21)(22)(23)(24)(29)
of infections with Ehrlichia species andAphagocytophilum are
summarized in Table 2. In the United States, ehrlichiosis is
most often reported from southeastern and south-central
states (from the east coast to Texas) (Table 2, Fig 3), whereas
anaplasmosis is most often reported from the northeastern
and upper midwestern states (Table 2, Fig 4).
The incubation periods (21)(22)(23)(24) and clinical man-
ifestations (30)(31)(32)(32) of, and the laboratory abnor-
malities (30)(33)(34) associated with, ehrlichiosis and
anaplasmosis are summarized in Table 3. Many of the
clinical manifestations of ehrlichiosis and anaplasmosis
likely result from the body’s systemic inflammatory
response and not from direct effects of the bacteria. (24)
The estimated case fatality rates among those with ehrli-
chiosis and anaplasmosis seeking medical care are 3% and
less than 1%, respectively. (33)(35)(36)(37)(38) Although the
incidence of ehrlichiosis due to E chaffeensis generally
increases with increasing age, (29)(36)(39) the case fatality
TABLE 3. (Continued)
DISEASEINCUBATIONPERIOD CLINICAL MANIFESTATIONS LABORATORY ABNORMALITIES
RMSF 3–12 d Early (1–4 d):• Fever, chills, malaise• Severe headache (less common in young children)• Myalgia• Gastrointestinal symptoms (abdominal pain,nausea, vomiting, anorexia)
• Edema, periorbital or on the back of hands• PhotophobiaLate (5þ d):• Altered mental status, coma• Respiratory compromise (pulmonary edema, ARDS)• Necrosis (may require amputation)• Multiorgan system damage (eg, CNS, renal)Rash:• Early (2–5 d after onset of symptoms):maculopapular rash on wrists and ankles, oftenspreading within hours, both proximally to thetrunk and distally to the palms and soles (face isusually spared)
• Late (day 6 or later after onset of symptoms):petechial rash
• Thrombocytopenia• Hyponatremia• Elevated liver transaminase concentrations• Leukopenia• Anemia
Babesiosis 1–9 wk • Often asymptomatic or associated with only mild,nonspecific symptoms but can be a severe,potentially fatal disease
• Fever common• Gradual onset of symptoms such as fatigue,malaise, and anorexia
• Subsequently, influenzalike illness symptoms (fever,chills, arthralgia, myalgia, headache, nausea)
• Other, less common symptoms: conjunctivalinjection, photophobia, pharyngitis,nonproductive cough, abdominal pain, vomiting,weight loss, emotional lability
• Possible respiratory distress, hypotension, mildhepatosplenomegaly, jaundice, dark urine,depression
• Disseminated intravascular coagulation, renalfailure, hemodynamic instability, respiratorydistress, hepatic compromise, altered mentalstatus, and death may occur with severe infection
• Hemolytic anemia. elevated reticulocyte count• Thrombocytopenia• Proteinuria• Elevated concentrations of hepatic enzymes,creatinine, and blood urea nitrogen
ARDS¼acute respiratory distress syndrome, CNS¼central nervous system, CSF¼cerebrospinal fluid, EM¼erythema chronicum migrans.
Vol. 40 No. 8 AUGUST 2019 387 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

TABLE 4. Tick-borne Diseases in Children in the United States: Diagnosisand Treatment
DISEASE DIAGNOSIS TREATMENT
Lyme disease • Demonstration of diagnostic IgM or IgG antibodiesin serum. A 2-tiered testing protocol is recom-mended: enzyme-linked immunosorbent assay orIFA assay should be performed first; if positive orequivocal, Western blot should follow
• In suspected Lyme meningitis, testing for intra-thecal IgM or IgG antibodies
Early localized disease:• Doxycycline 4.4 mg/kg per day, PO, divided BID (maximum,200 mg/d) for 10 ds; OR
• Amoxicillin 50 mg/kg per day, PO, divided TID (maximum,1,500 mg/d) for 14 d; OR
• Cefuroxime 50 mg/kg per day, PO, divided BID (maximum,100 mg/d) for 14 d
For patients intolerant to the above:• Azithromycin 10 mg/kg per day, PO, once daily for 7 dExtracutaneous disease:• Isolated facial palsy: doxycycline 4.4 mg/kg per day, PO,divided BID (maximum, 200 mg/d) for 14 d
• Arthritis: an oral drug as for early localized disease, for 28 d• Persistent arthritis after first course of therapy: treat againusing an oral agent as for first-episode arthritis for 28 d; ORceftriaxone 50–75 mg/kg, IV, once daily (maximum, 2,000mg/d) for 14–28 d
• Atrioventricular heart block or carditis: an oral agent as forearly localized disease, for 14 d (range, 14–21 d); OR cef-triaxone 50–75 mg/kg, IV, once daily (maximum, 2,000 mg/d) for 14 d (range, 14–21 d if hospitalized; can be changed tooral therapy once stabilized/discharged)
• Meningitis: doxycycline 4.4 mg/kg per day, PO, divided intodoses (maximum, 200 mg/d) for 14 d; OR ceftriaxone 50–75mg/kg, IV, once daily (maximum, 2,000 mg/d) for 14 d
Ehrlichiosis • PCR assay to detect Ehrlichia DNA in whole blood• IFA assay: demonstration of a 4-fold rise in theEhrlichia IgG-specific antibody titer in a pair ofserum samplesa
• Immunohistochemical staining of skin, tissue, orbone marrow specimens to visualize Ehrlichiaspecies
Doxycycline (maximum, 100 mg per dose):• Children weighing <100 lb (<45.4 kg): 2.2 mg/kg per doseBID, PO or IV
• Larger children and adults: 100 mg BID, PO or IVDuration of therapy: minimum, 5–7 days; therapy should be
given until evidence of clinical improvement and at least 3d after fever resolves
Anaplasmosis • PCR assay to detect Anaplasma phagocytophilumDNA in bloodb
• IFA assay: demonstration of a 4-fold rise in the Aphagocytophilum IgG-specific antibody titer in apair of serum samplesa
• Immunohistochemical staining of skin, tissue, orbone marrow specimens to visualize Aphagocytophilum
Doxycycline (maximum, 100 mg per dose):• Children weighing less than 100 lb (45.4 kg): 2.2 mg/kg per
dose BID, PO or IV• Larger children and adults: 100 mg BID, PO or IVDuration of therapy: 10–14 d
RMSF • IFA assay: demonstration of a 4-fold change (usuallyan increase) in IgG-specific antibody titers in pairedserum samples (first sample obtained within firstweek of illness; second obtained 2–4 wk later)a
• PCR assay for detection of rickettsial DNA in abiopsy specimen (eg, skin biopsy of a rash lesion)
• Immunohistochemical staining of rickettsialorganisms from biopsy specimen (eg, skin or othertissue)
Doxycycline (maximum, 100 mg per dose):• Children weighing <100 lb (<45.4 kg): 2.2 mg/kg per doseBID, PO or IV
• Larger children and adults: 100 mg BID, PO or IVDuration of therapy: minimum, 5–7 d; therapy should be
given until evidence of clinical improvement and at least3 d after fever resolves
Continued
388 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

rates are highest in both adults 70 years or older and children
10 years or younger. (29)(36) Ehrlichiosis in immunocom-
promised individuals is associated with an increased risk of
death, (29)(36) but severe or fatal cases of ehrlichiosis have
occurred in previously healthy children and young adults.
(33)(40) Children with ehrlichiosis often are asymptomatic
or only mildly symptomatic. (33)(35)(41) With ehrlichiosis,
gastrointestinal manifestations and rash may be more com-
mon in children. (33)(41) More severe manifestations of
ehrlichiosis include toxic shock– or septic shock–like syn-
dromes, coagulopathies, renal failure, and hepatic failure.
(42) Rarely, E chaffeensis infection may result in hemophago-
cytic lymphohistiocytosis. (41)(43) Anaplasmosis is usually a
self-limiting illness. (24) Gastrointestinal manifestations and
central nervous system involvement occur less frequently in
patients with anaplasmosis than in those with ehrlichiosis,
(30)(44) and rash occurs in less than 10% of patients with
anaplasmosis. (30)(44) Severe or life-threatening manifes-
tations are less frequent with anaplasmosis than with
ehrlichiosis. Factors associated with a more severe clinical
course of ehrlichiosis or anaplasmosis include immunosup-
pression and delay in diagnosis or treatment. In cases of
anaplasmosis, laboratory abnormalities are usually observed
during the first week of clinical illness, and usually there are
no CSF abnormalities. (38) The organisms (Ehrlichia species
and A phagocytophilum) multiply within cytoplasmic vacuoles
of the target cells (monocytes or granulocytes), forming
clusters of bacteria called morulae. (45) Such morulae may
be visualized in the cytoplasm of these cells during the acute
stage of illness and are highly suggestive of the diagnosis (but
because examination of a blood smear is insensitive, finding
morulae should not be used alone to rule in or rule out the
diagnosis). Patients with anaplasmosis may have altered
neutrophil function, which could result in neutrophils having
ineffective microbicidal activity. (40)
Diagnostic assays for ehrlichiosis and anaplasmosis
are summarized in Table 4. For both diseases, laboratory
diagnosis can be accomplished in 3 different ways
(21)(22)(23)(24): PCR assays to detect the organism’s
DNA, IFA assays to detect antibodies against the organism,
and immunohistochemical staining to visualize the organ-
isms in tissue specimens.
Treatment of ehrlichiosis and anaplasmosis is summa-
rized in Table 4 (21)(22)(23)(24). The first-line treatment
for either disease is doxycycline. A clinical suspicion of
ehrlichiosis or anaplasmosis is sufficient to initiate treatment.
TABLE 4. (Continued)
DISEASE DIAGNOSIS TREATMENT
Babesiosis • Microscopic examination of Giemsa- or Wright-stained peripheral blood smears to identify intra-erythrocytic Babesia parasitesc
• PCR assay for detection of Babesia species DNA inbloodd
• IFA assay to detect Babesia-specific antibodies inbloode
Dosages for children:• Atovaquone 20 mg/kg every 12 h (maximum, 750 mg perdose); AND azithromycin 10 mg/kg (maximum, 500 mg perdose) on day 1 and 5 mg/kg every day (maximum, 250 mgper dose) subsequently
• Clindamycin 7–10 mg/kg, IV or PO, every 6–8 h (maximum,600 mg per dose); AND quinine 8 mg/kg PO every 8 h(maximum, 650 mg per dose)
Duration of therapy: 7–10 d
BID¼twice daily; IFA¼immunofluorescent antibody, Ig¼immunoglobulin, IV¼intravenous, PCR¼polymerase chain reaction, PO¼orally, TID¼three timesdaily.aAntibody titers are often negative if the serum specimen was obtained during the first 7 to 10 days of illness. Antibody results obtained in the first (acute)sample cannot be relied on alone for laboratory confirmation of the diagnosis. Because IgM antibodies are less specific than IgG antibodies (andmore likelyto generate false-positive results), IgM results should not be used alone for laboratory diagnosis.bPCR assays are most sensitive during the first week of illness, but the sensitivity may decrease after the administration of drugs in the tetracycline class.cMultiple smears may need to be examined, and if the diagnosis of babesiosis is being considered, the laboratory should be notified that a manual (not anautomated) review of blood smears for Babesia parasites is needed. It may be difficult to distinguish between Babesia organisms and Plasmodiumfalciparum or artifacts; examination of blood smears by a reference laboratory should be considered.dIn patients with low-grade B microti parasitemia (eg, early in the infection when parasites are more difficult to visualize on blood smear), PCR assays seemto have higher sensitivity than blood smear microscopy. Of note, PCR assays should be used with caution whenmonitoring a patient’s response to therapybecause B microti organisms can be detected for a long period (weeks to months) after the parasites can no longer be visualized on microscopicexamination of blood smears.eThis method is particularly useful for diagnosing babesiosis in individuals with very low levels of parasitemia and those in whom discrimination betweenbabesiosis and malaria is difficult because of inconclusive blood smear examination and/or a travel history that cannot exclude either parasite.
Vol. 40 No. 8 AUGUST 2019 389 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

Conversely, delaying initiation of treatment may result in
severe illness or death.
ROCKY MOUNTAIN SPOTTED FEVER
A total of 37,376 infections with spotted fever group
rickettsii (including Rickettsia rickettsii, Rickettsia parkeri,
and Rickettsia species 364D) were reported in the United
States from 2004 through 2016. (1) Table 2 summarizes
characteristics of R rickettsii, the causative organism of
RMSF, first described in 1906. (46) R rickettsii, a member
of the family Rickettsiaceae, is an obligate intracellular,
Gram-negative bacillus. (24)(47)(48) The organism primar-
ily targets endothelial cells of the vascular system, inducing
a diffuse vasculitis with resultant increased vascular per-
meability. (24)
The tick vector, (24)(47)(48) seasonality, (24)(47)(48) and
geographic distribution of reported cases (49)(50)(51)(52)
(53) are summarized in Table 2. R rickettsii is transmitted
by 3 different ticks (24)(47)(48): the American dog tick
(Dermacentor variabilis) (Fig 1), the Rocky Mountain wood
tick (Dermacentor andersoni), and the brown dog tick
(Rhipicephalus sanguineus). RMSF and related rickettsioses
have been reported throughout most of the continental
United States but are more common in certain south/south
central states (Table 2, Fig 5). (49)(50)(51)(52)(53)
The incubation period (54) and clinical manifestations
(24)(47)(48)(55)(56)(57)(58)(59) of, and laboratory abnormal-
ities associated with, RMSF are summarized in Table 3.
Patients with severe disease often have a shorter incubation
period (eg, £5 days) than those with milder disease. (60)
Symptoms associated with RMSF evolve during the illness.
(24)(47)(48) Early symptoms of RMSF (24)(47)(48) are
observed during the first 1 to 4 days of illness. (55)(56) A
rash usually appears a few days after the onset of symptoms,
but most patients seek medical attention before the rash
appears. (57)(58)(59) Most patients do not have the clas-
sic triad of a reported tick bite, fever, and rash at the time
they initially present for medical attention. (55)(57) The rash
associated with RMSF also evolves over time. (24)(47)(48)
Classically, the rash begins as small, pink, blanching
macules. Over the ensuing days, the rash usually becomes
maculopapular, and there may be central petechiae. A
petechial rash occurs relatively late (ie, at or after day 6
Figure 3. Ehrlichiosis cases reported to the Centers for Disease Control and Prevention, 2016. (Reprinted with permission from Centers for DiseaseControl and Prevention. Tickborne Diseases of the United States. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2018.)
390 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

of illness) and indicates an advanced infection. The
absence of a rash does not preclude the diagnosis of RMSF
(less than half of patients do not have a rash during the first
3 days of illness, and some patients do not ever develop a
rash). (55)(57) Children younger than 15 years are more
likely to have a rash and are more likely to develop a rash
sooner than are older individuals. (55)(61)(62) Untreated
RMSF can have severe clinical manifestations, and pro-
gression to severe disease can be rapid, even in previously
healthy individuals. Late clinical manifestations of RMSF
are more severe. (63)(64) Patients who are treated early in
the infection may have only mild disease with relatively
rapid resolution of symptoms. (24)(47)(48) The highest
incidence of RMSF is in older individuals (60–69 years of
age), although RMSF occurs in people of all ages. (49)
Children younger than 10 years have the highest RMSF
case fatality rate. (49) Significant long-term sequelae have
been described in patients with severe RMSF, including
cognitive impairment, blindness, and peripheral neuropa-
thy. (61)(65)(66)(67)(68)(69) Laboratory values in patients
with RMSF (57)(70)(71)(72) are often within normal limits
or only slightly abnormal early in the infection. Laboratory
abnormalities are more likely to be observed as the infec-
tion progresses. Damage to the vascular endothelium by R
rickettsii results in increased capillary permeability with
widespread microhemorrhage and platelet consumption.
(71) Hypovolemia leads to appropriate secretion of anti-
diuretic hormone with resultant hyponatremia. (72)
Diagnostic assays for RMSF are summarized in Table 4.
(24)(47)(48) The diagnosis of RMSF must be a clinical
diagnosis (based on the patient’s signs and symptoms)
because treatment of a patient with suspected RMSF should
be initiated as soon as the diagnosis is suspected; the
diagnosis can be confirmed through laboratory testing.
The gold standard for the laboratory diagnosis of RMSF
is the IFA assay. Other diagnostic assays used to confirm the
diagnosis of RMSF involve detection of the organism’s DNA
(through a PCR assay) or visualization of the organism
through immunohistochemical staining of a biopsy speci-
men (skin or other tissue). (24)
Treatment of RMSF is summarized in Table 4.
(24)(47)(48) As soon as RMSF is suspected, therapy with
Figure 4. Anaplasmosis cases reported to the Centers for Disease Control and Prevention, 2016. (Reprinted with permission from Centers for DiseaseControl and Prevention. Tickborne Diseases of the United States. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2018.)
Vol. 40 No. 8 AUGUST 2019 391 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

doxycycline should be initiated. Initiation of treatment
within the first few days of illness is associated with greater
effectiveness (in terms of preventing mortality and decreas-
ing morbidity) than if treatment does not begin until after
the fifth day of illness. Doxycycline is the antibiotic of choice
for all age groups for the treatment of RMSF.
BABESIOSIS
Between 2011 and 2016, 9,631 cases of babesiosis were
reported in the United States. (73) In 2015 alone, there were
1,804 confirmed cases of babesiosis in the United States,
primarily in New England and the mid-Atlantic area. (74)
Table 2 summarizes characteristics of the causative organ-
ism (Babesia microti is themost common cause of babesiosis
in the United States, but several other genetically distinct
Babesia species exist [2]). Babesia species belong to the
phylum Apicomplexa, which includes Plasmodium and
other species. (75) Themajor cell target of these intracellular
organisms is the red blood cell. (2)(73)(74)
Although Babesia infections can be transmitted through
blood transfusion and congenitally, (73)(74) babesiosis is a
primarily vector-borne disease. The vector for transmission
ofBmicroti is the blacklegged tick (I scapularis). (73)(74) Fig 1
shows the appearance of this tick. The white-footed mouse
(Peromyscus leucopus) is the primary reservoir host for B
microti in the United States. (74) Although not a reservoir
host for B microti, the white-tailed deer (Odocoileus virgin-
ianus) can serve as a host for blood meals by the tick. (74)
During the past several years, the increase in the deer
population in some regions, including suburban areas, is
likely related to the spread of the tick vector. (73) The
seasonality of vector-borne transmission of B microti is
summarized in Table 2 (73)(74). B microti infections have
been acquired in the northeast as well as in the upper
Midwest (76)(77)(78)(79) (Table 2, Fig 6). Occasionally,
cases of babesiosis caused by other Babesia species have
occurred in different parts of the United States, (80)(81) but
the tick vectors and the reservoir hosts for these organisms
are usually not known. (74)
Figure 5. Spotted fever rickettsiosis (including Rocky Mountain spotted fever) cases reported to the Centers for Disease Control and Prevention, 2016.(Reprinted with permission from Centers for Disease Control and Prevention. Tickborne Diseases of the United States. 5th ed. Atlanta, GA: Centers forDisease Control and Prevention; 2018.)
392 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

The incubation period and clinicalmanifestations of, and
laboratory abnormalities associated with, babesiosis are
summarized in Table 3. (2)(73)(74) In patients with symp-
tomatic babesiosis, clinical manifestations usually develop
within weeks of exposure, although manifestations may not
develop untilmonths after initial infection. (73) Parasitemiamay
persist, both in treated and untreated patients, and, especially in
immunocompromised individuals,may result in recrudescence
weeks or months later. (73)(82)(83) Even asymptomatic individ-
uals can have persistent (eg, for more than a year) parasitemia.
(74) Although babesiosis is often asymptomatic or associated
with mild and nonspecific symptoms, it can manifest as a
severe, potentially fatal disease. (73)(74) An estimated 50% of
children with babesiosis are asymptomatic or have only a mild
viral-like illness. (84)(85)(86)(87) Severe presentations are
more likely if the patient is elderly and/or immunocompro-
mised (eg, asplenic). (73)(74)(88)(89)(90) The first report of
a case of human babesiosis in 1957 was in an asplenic
patient. (91) The clinical manifestations of babesiosis
(2)(73)(74)(79)(80)(81)(85)(88)(89)–(90)(92)(93)(94)(95) may
resemble those of malaria. Although fever is common
in patients with babesiosis, individuals at the extremes of
age (eg, infants, the elderly) or those who are immuno-
compromised may be afebrile. (74) Organ failure and
death may occur with severe infection. (73)(74)(88)(93)
Hemolytic anemia and an elevated reticulocyte count are
the most prominent laboratory abnormalities with babe-
siosis. (2)(73)(88)(93)(95)
Because the clinical manifestations of babesiosis are
nonspecific, confirmation of the diagnosis requires labora-
tory testing. (2) The most reliable diagnosis of babesiosis is
made in patients with the following 3 characteristics: 1)
positive laboratory test results for Babesia, 2) residence in
or travel to an area where Babesia is endemic, and 3) a viral
infectionlike illness. (2) Diagnostic assays for babesiosis are
summarized in Table 4 (73)(74). The first method of diag-
nosis of babesiosis is the identification of intraerythrocytic
Babesia parasites by microscopic examination of Giemsa- or
Wright-stained peripheral blood smears (73)(74) in patients
with acute, symptomatic infection; the “tetrad” (Maltese
cross) form is pathognomonic. (73)(74) Other methods of
diagnosis of babesiosis are PCR analysis (73)(74)(96) and
Figure 6. Babesiosis cases reported to the Centers for Disease Control and Prevention, 2016. (Reprinted with permission from Centers for DiseaseControl and Prevention. Tickborne Diseases of the United States. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2018.)
Vol. 40 No. 8 AUGUST 2019 393 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

Babesia-specific antibody detection through indirect fluo-
rescent antibody assay. (73)(74)(97)(98)
Treatment of babesiosis is summarized in Table 4.
(73)(74) Treatment for asymptomatic individuals is not rec-
ommended, irrespective of laboratory assays positive for
Babesia. (2) If an asymptomatic individual has 1 or more
positive Babesia assays, the assays should be repeated, and
treatment should be considered if parasitemia continues for
more than 3 months. (2)(73) Treatment is recommended for
active babesiosis (viral infection–like symptoms with either
visualization of Babesia parasites on a blood smear or a
positive PCR assay forBabesia). (2) Symptomatic individuals
with positive Babesia serology assays but no parasites
observed on blood smears and no positive PCR assays for
Babesia should not be treated. (2) Treatment for patients
with active babesiosis usually entails combination therapy
for 7 to 10 days with either atovaquone plus azithromycin or
clindamycin with quinine. (2)(73)(74)(75) A longer duration
of therapy may be necessary in patients with severe disease
or those who are persistently symptomatic until parasitemia
resolves. (2) The regimen of choice for the treatment ofmild
babesiosis in children is oral atovaquone with azithromycin.
(73)(74) Severe babesiosis (eg, with parasitemia greater than
10%, or those with severe hemolysis, or hepatic, renal, or
pulmonary compromise) is usually treated with intravenous
clindamycin with quinine. (2)(73)(74) Severely ill patients
may require or benefit from other concomitant interven-
tions, such asmechanical ventilation, dialysis, and exchange
transfusion. (73)(74)(99) With mild-moderate babesiosis,
clinical improvement within 48 hours and complete reso-
lution of symptoms within 3 months of initiation of therapy
should occur. (2) Patients withmoderate to severe babesiosis
should be monitored carefully during treatment for
improvement in clinical and laboratory parameters and
decrease in parasitemia. (2) For example, with severe bab-
esiosis, daily or every-other-day monitoring of the hemato-
crit value and the percentage of parasitemia until the patient
has improved and the parasitemia has decreased to less than
5% is recommended. (2) Persistent low-grade parasitemia
may occur for months after initiation of antimicrobial
therapy. (2) If blood smears or PCR assays for Babesia
remain positive for 3 months or more after initial treatment,
repeated treatment should be considered. (2) For patients
with especially severe or persistent symptoms despite appro-
priate treatment, the possibility of co-infection with other
organisms with the same tick vector (B burgdorferi and/or
A phagocytophilum) should be considered. (2) Special
treatment considerations for severely immunocompro-
mised patients (74) include 1) a duration of therapy of at
least 6 weeks, with negative blood smears for at least 2
weeks before treatment discontinuation, and 2) treatment
with higher doses of oral azithromycin.
PREVENTION
Prevention of acquisition of tick-borne diseases entails
primarily preventing tick bites and removing ticks as
quickly as possible if attachment has occurred. (100)
To prevent tick bites, the following practices can be
instituted: use of an Environmental Protection Agency–
registered insect repellent (http://www.epa.gov/insect-
repellents), treating cats and dogs for ticks, checking
for ticks daily, and showering or bathing soon after out-
door exposure. Environmental Protection Agency–regis-
tered insect repellents contain compounds such as DEET
(N,N-diethyl-meta-toluamide). In addition to applying
such an insect repellent to the skin, clothing and gear
(eg, boots) can be treated with products containing per-
methrin. Treatment of household pets (dogs and cats) for
ticks should be performed under the guidance of a
veterinarian. When checking for ticks, it is espe-
cially important to check in the following areas: around
the hairline and scalp, in and around the ears, behind the
knees, between the legs, around the waist, and inside the
umbilicus. Any tick found attached to the skin should be
removed as soon as possible and, after removing the tick, the
skin should be cleaned.
In general, antibiotic drug prophylaxis after a tick bite to
prevent tick-borne diseases is not recommended. However,
for one tick-borne disease, Lyme disease, antibiotic drug
prophylaxis can be implemented if a tick bite has occurred.
(100) A single dose of doxycycline for the prevention of
Lyme disease could be administered to children (5): 200-mg
dose (or 4.4 mg/kg for children weighing <100 lb [<45.4
kg]), if the following conditions are met (100): 1) the patient
resides in or has traveled to a state highly endemic for Lyme
disease (Connecticut, Delaware, Maine, Maryland, Mas-
sachusetts, Minnesota, New Hampshire, New Jersey, New
York, Pennsylvania, Rhode Island, Vermont, Virginia, Wis-
consin); 2) the attached tick is an adult or nymph stage I
scapularis tick; 3) the estimated duration of attachment is at
least 36 hours; 4) prophylaxis can be initiated within 72
hours of tick removal; and 5) the patient has no contrain-
dication to doxycycline.
394 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

References for this article are at http://pedsinreview.aappubli-
cations.org/content/40/8/381.
Summary• In general, the epidemiology of tick-borne diseases reflects thecharacteristics of the specific tick vector, including the tick’sknown geographic distribution and seasonality. However,some tick-borne diseases are transmitted through othermechanisms (eg, congenital). Because of this, and in areaswith high endemicity, there may be year-round incident“tick-borne” diseases.
• However, the epidemiology of tick-borne diseases in the UnitedStates is evolving, with new species being identified and therange of the tick vectors expanding. Although the most commonclinical manifestations of and laboratory abnormalities associatedwith each tick-borne disease are known, not every infectedindividual has all such clinical manifestations or laboratoryabnormalities with a given tick-borne disease, and the numberand combination of clinical and laboratory findings experiencedvaries fromone patient to the next. The possibility of concomitanttick-borne diseases (eg, I scapularis ticks transmit Lyme disease,B miyamotoi infections, anaplasmosis, and babesiosis) should be
suspected if a patient’s clinical or laboratory features are moresevere than usually observed with a given tick-borne disease.Because tick-borne diseases can be fatal, and because a delayin the initiation of treatment can be associated with a poorerprognosis, the diagnosis may be based on clinical suspicion alone(while confirmatory laboratory studies are pending). Diagnosticlaboratory testing for tick-borne diseases is evolving towardassays with faster turnaround times and less dependence onacute and convalescent serology samples. Prevention of tick-borne diseases primarily involves avoiding exposure to ticks andtick bites, checking for attached ticks, and prompt removal ofticks if found attached to the skin. Lyme disease remains theonly tick-borne disease for which antibiotic drug prophylaxisis recommended for certain patients known to have anattached tick.
Vol. 40 No. 8 AUGUST 2019 395 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

PIR QuizThere are two ways to access the journal CME quizzes:
1. Individual CME quizzes are available via the blue CME link under the article title in the Table of Contents of any issue.
2. To access all CME articles, click “Journal CME” from Gateway’s main menu or go directly to: http://www.aappublications.org/
content/journal-cme.
3. To learn how to claim MOC points, go to: http://www.aappublications.org/content/moc-credit.
REQUIREMENTS: Learnerscan take Pediatrics in Reviewquizzes and claim creditonline only at: http://pedsinreview.org.
To successfully complete2019 Pediatrics in Reviewarticles for AMA PRACategory 1 CreditTM, learnersmustdemonstrate aminimumperformance level of 60% orhigher on this assessment.If you score less than 60%on the assessment, youwill be given additionalopportunities to answerquestions until an overall 60%or greater score is achieved.
This journal-based CMEactivity is available throughDec. 31, 2021, however, creditwill be recorded in the year inwhich the learner completesthe quiz.
2019 Pediatrics in Reviewnow is approved for a totalof 30 Maintenance ofCertification (MOC) Part 2credits by the AmericanBoard of Pediatrics throughthe AAP MOC PortfolioProgram. Complete the first10 issues or a total of 30quizzes of journal CMEcredits, achieve a 60%passing score on each, andstart claiming MOC creditsas early as October 2019. Tolearn how to claim MOCpoints, go to: http://www.aappublications.org/content/moc-credit.
1. A previously healthy 9-year-old girl presents to the office in July with an enlarging, red,nontender, and nonpruritic rash of her left thigh for the past 3 days. She has felt warm, andher mom noted an oral temperature of 100.8°F (38.2°C) today. She has also complained ofbeing achy and having a headache. A tick was removed from the site of the rash 14 daysago. The family lives in rural Maine. She and her family traveled to Tennessee for 1 week 6weeks ago. On examination she is afebrile and her vital signs are normal. There is anannular, 8-cm-diameter erythematous macular lesion on her left thigh without centralclearing, eschar, or drainage. Her mother states that she is allergic to amoxicillin becauseshe had a rash when shewas an infant. Which of the following is most likely responsible forthe transmission of her illness?
A. Amblyomma americanum.B. Dermacentor andersoni.C. Dermacentor variabilis.D. Ixodes scapularis.E. Rhipicephalus sanguineus.
2. For the patient in question #1, which of the following is the most appropriate next step inmanagement?
A. Begin cephalexin therapy.B. Begin doxycycline therapy.C. Obtain a blood sample for Borrelia burgdorferi polymerase chain reaction (PCR).D. Obtain a serum sample for enzyme-linked immunosorbent assay B burgdorferi
antibodies.E. Obtain a serum sample for Western blot B burgdorferi immunoglobulin (Ig) G and
IgM antibodies.
3. A 17-year-old boy is seen in the office for follow-up of 2 months of fatigue that started inNovember. He also complains of headache 1 to 2 times per week. He has not had weightloss, arthritis, arthralgias, or rash. He states that he feels warm occasionally but when hechecks his temperature it is normal. He removed a tick from his inguinal region 7 monthsago and did not develop a rash at the site. He lives in Oklahomawith his family, and his onlytravel was a Caribbean cruise the previous summer. His mother is concerned that he hasLyme disease or some other tick-borne illness. His vital signs and physical examinationfindings are normal. A complete blood cell count, erythrocyte sedimentation rate, andhepatic transaminase levels are within normal limits. Which of the following is the mostappropriate diagnostic test for tick-borne disease?
A. Anaplasma phagocytophilum PCR on blood.B. A phagocytophilum IgG antibody on serum.C. B burgdorferi antigen assay on urine.D. B burgdorferi Western blot IgG and IgM on serum.E. No tick-borne disease testing is recommended.
396 Pediatrics in Review at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

4. A previously healthy 6-year-old girl presents to the office in June with a 3-day history offever to a temperature of 103°F (39.4°C) and increasing malaise. She also complained of aheadache the past day. Last night the parents noted a red rash on her arms and legs, whichthen spread to her trunk. The parents have not removed any ticks from the girl, but themom removed a tick from her brother 2 weeks ago. The family lives on a farm in Arkansasand has 2 pet dogs. In the office her temperature is 102.3°F (39.1°C), heart rate is 124 beats/min, respiratory rate is 22 breaths/min, blood pressure is 98/60 mm Hg, and oxygensaturation is 97%. She is moderately ill appearing but not lethargic. Her examination isremarkable for a generalized erythematous, blanching macular exanthem that is moreprominent on her hands, arms, feet, and legs and involves her palms and soles. There is nomeningismus. A complete blood cell count, blood culture, comprehensive metabolicprofile, urinalysis, and Rickettsia rickettsii IgG and IgM immunofluorescent antibody assayare pending. She is started on empirical intravenous ceftriaxone therapy. Which of thefollowing is the most appropriate additional antimicrobial therapy?
A. Atovaquone and azithromycin.B. Chloramphenicol.C. Ciprofloxacin.D. Doxycycline.E. No additional antimicrobial therapy is needed pending laboratory results.
5. A 12-year-old boy presents to the office in August with a 2-day history of low-grade fever,headache, and generalized myalgia. Three days before the onset of fever he had anorexiaand increasing fatigue. He lives in New York City. Hewent to upstate New York 3weeks agofor a 3-day camping trip and removed a tick from behind his right ear. He never developeda rash at that site. Laboratory testing is remarkable for hemolytic anemia, an elevatedreticulocyte count, mild thrombocytopenia, and elevated hepatic transaminase levels.Which of the following is most likely to confirm the diagnosis?
A. Acute and convalescent R rickettsii immunofluorescent antibody assay IgG serumantibody.
B. Blood for B burgdorferi PCR.C. Blood for Ehrlichia chaffeensis PCR.D. Manual review of Wright-stained peripheral blood smear.E. Urine for B burgdorferi antigen.
Vol. 40 No. 8 AUGUST 2019 397 at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.2018-03042019;40;381Pediatrics in Review
Jennifer S. ReadTickborne Diseases in Children in the United States
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/40/8/381including high resolution figures, can be found at:
Supplementary Material
.8.381.DC1http://pedsinreview.aappublications.org/content/suppl/2019/07/31/40Supplementary material can be found at:
References
-1http://pedsinreview.aappublications.org/content/40/8/381.full#ref-listThis article cites 86 articles, 16 of which you can access for free at:
Subspecialty Collections
iology_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/epidemEpidemiologyous_diseases_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/infectiInfectious Diseasefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pedsinreview.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.2018-03042019;40;381Pediatrics in Review
Jennifer S. ReadTickborne Diseases in Children in the United States
http://pedsinreview.aappublications.org/content/40/8/381located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0191-9601. Illinois, 60143. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Health Sciences Library, Stony Brook University on June 3, 2020http://pedsinreview.aappublications.org/Downloaded from