
tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
5
Case Report E nd od ont ic r et r eatment of an autotran sp lan te d lower f ir st p remolar: a case r ep ort Transplantation is the transfer of a tooth from one alv eol ar soc ke t toanot her , ei ther in the sa me or di¡er - ent individual (1). If the transfer is from the alveolar socket to another in the same individual it is termed autotrans pla nta tion . The suc cess ra te of an au to trans - pla nted tooth di¡ers wid ely , and it has been repo rted from 0 to 100% (2, 3). The cause of failure may be beca use of a number of cond it ionssuch as roo t res orp - tion , api cal periodon titis, lac k of root formatio n, dis- place men t from the alv eolus , periodo ntal disease and failure in primary healing. Other factors such as do no r too th type, st ag e of eru pt ion , age of the pa tien t, bone type, periodon tal status, risk fac tors such as smo king , andthe sur gic altechniq ue andskill can con- trib ute to the prognosis (4 ,5 ) . Failure of conventional root-canal treatment com- monl y resul ts from intr aradi cular infectio n which may be because of numerous factors such as inade- qua te con trol andeliminationof infectio n, poor access cavity design, inadequa te canal instrumentation and obt uration , missed canals and c oronal le akage (6 ) . Additional causes of persistent periapical pathology after conventional root-canal treatment in well-trea- ted cases may be an extraradicular infection such as Actinomyces sp. and Arachnia propionica (7, 8), a foreign body reaction (9^12), or the presence of a true cyst ( 1 3, 1 4 ) . The t reatment alter natives f or an e ndodontic failur e are conventio nal endodontic retrea tmen t, end odo nti c surgery, a com bin a tio n of bot h, or ex trac- tio n of the toot h. This paper presents a clinical report of an auto- trans plan ted too th tha t req uired non -surgi cal and surgical interventions to treat the tooth subsequent to the dev elo pme nt of pro ced ural pr ob lems and asso- ciated periapical patho logy . Report A 24- year- old female was ref err ed to the disc ip line of End odo nt ics fro m the disc ip line of Or al andMaxill o- facial surgery for treatment of a recurrent periapical abscess associated with the upper left ¢rst premolar tooth. Her medic al histo ry was non-contrib ut ory. The pa tien t wasa reg ularvisito r to her gen era l dental pr ac tit ion er, and she wa s prepa redto und ergo furt her endodon tic treatment. On questioning the patient it became evident that the too th had a uniqu e histo ry. In Ma y 1 990 , the pa tientwas referredto an orthod on tist for ortho don tic treatment of a mild Clas s3 de nt al and sk ele tal mal oc- cl usio n. Sh e hadcong eni tal ly missi ng upper righ t ¢rs t premolar and upper left ¢rst and second premolar teeth with lower arch crowding. Orthodontic treat- ment planning was carried out in consultation with an or al and maxill ofa cial sur geo n reg ard ing themiss- ing upper left premo lar s. In ord er to esta blis h a Dental Traumatology 2003; 19: 228±232 Copyri ght # Blackwell Munksgaard 2003 Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY ISSN 1600±4469 228 Kosh y S, Lo ve RM. End odonti c retreatmen t of an aut otransplan ted lower ¢rst premolar: a case rep ort. Dental T raumatol 2003; 19: 228^232. # Blackw ell Munksga ard, 200 3 . Ab stract ^ A 24- year -old fema le with no con trib ut ory medica l his to ry had been treated by ort hod ontic ali gnme nt and transp lantation of the lo we r le ft ¢rst pr emol ar tothe up per lef t ¢rs t premolar site to correct for cong enita lly missing upper premo lars . Su bseq uen tly , the transp lan ted premo lar was treated by conven tional endodon tics and apical surgery for persistent periapi cal periodon titis ov er a span of 1 2 years . A combina tion of conven tional endodontic retrea tment and periapical surgery resul ted in periap ical healin g . This case ou tlines the need for careful preoperativ e case assessment. Sajeev Koshy, Robert Matthew Love Department of Stomatology , School of Dentistry, University of Otago, PO Box 647, Dunedin, New Zealand Key words: a utotransplantati on; endodontic retreatment; periapical surgery; periapical cyst Dr Robert M.Love, MDS , PhD , FRA CDS,Departmen t of Stomatology , University of Otago, School of Dentistry, PO Box 647, Dunedin,New Zealand Tel.: 64 347971 21 Fax: 64 347 9 7046 e-mail: robert.love@dent.otago.ac.nz Accepted 8 January, 2003
-
Upload
florin-ionescu -
Category
Documents
-
view
218 -
download
0
Transcript of tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report

8/3/2019 tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
http://slidepdf.com/reader/full/tic-re-treatment-of-an-auto-transplanted-lower-first-premolar-a-case-report 1/5
Case Report
Endodontic retreatment of an autotransplantedlower first premolar: a case report
Transplantation is the transfer of a tooth from onealveolar socket toanother, either in the same or di¡er-ent individual (1). If the transfer is from the alveolar
socket to another in the same individual it is termedautotransplantation.The success rate of an autotrans-planted tooth di¡ers widely, and it has been reportedfrom 0 to 100% (2, 3). The cause of failure may bebecause of a number of conditions such as root resorp-tion, apical periodontitis, lack of root formation, dis-placement from the alveolus, periodontal diseaseand failure in primary healing. Other factors such asdonor tooth type, stage of eruption, age of thepatient,bone type, periodontal status, risk factors such assmoking, andthe surgicaltechnique andskill cancon-tribute to the prognosis (4, 5).
Failure of conventional root-canal treatment com-monly results from intraradicular infection whichmay be because of numerous factors such as inade-quate controlandeliminationof infection, pooraccesscavity design, inadequate canal instrumentation andobturation, missed canals and coronal leakage (6).Additional causes of persistent periapical pathologyafter conventional root-canal treatment in well-trea-ted cases may be an extraradicular infection such asActinomyces sp. and Arachnia propionica (7, 8), a foreignbody reaction (9^12), or the presence of a true cyst(13,14). The treatment alternatives for an endodonticfailure are conventional endodontic retreatment,
endodontic surgery, a combination of both, or extrac-tion of the tooth.
This paper presents a clinical report of an auto-
transplanted tooth that required non-surgical andsurgical interventions to treat the tooth subsequentto the development of procedural problems and asso-ciated periapical pathology.
Report
A 24-year-old female was referred to the discipline of Endodontics from the discipline of Oral andMaxillo-facial surgery for treatment of a recurrent periapicalabscess associated with the upper left ¢rst premolartooth. Her medical history was non-contributory.The patient wasa regular visitor tohergeneral dentalpractitioner, and shewas preparedto undergo furtherendodontic treatment.
On questioning the patient it became evident thatthe tooth had a unique history. In May 1990, thepatientwas referredto anorthodontist for orthodontictreatmentof a mild Class 3 dental and skeletalmaloc-clusion. She hadcongenitally missing upper right ¢rstpremolar and upper left ¢rst and second premolarteeth with lower arch crowding. Orthodontic treat-ment planning was carried out in consultation withan oral andmaxillofacialsurgeon regarding themiss-ing upper left premolars. In order to establish a
Dental Traumatology 2003; 19: 228±232 Copyright # Blackwell Munksgaard 2003
Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY
ISSN 1600±4469
228
Koshy S, Love RM. Endodontic retreatment of an autotransplantedlower ¢rst premolar: a case report. Dental Traumatol 2003;19:228^232.# Blackwell Munksgaard, 2003.
Abstract ^ A 24-year-old female with no contributory medical
history had been treated by orthodontic alignment andtransplantation of the lower left ¢rst premolar to the upper left ¢rstpremolar site to correct for congenitally missing upper premolars.Subsequently, the transplanted premolar was treated byconventional endodontics and apical surgery for persistentperiapical periodontitis over a span of 12 years. A combination of conventional endodontic retreatment and periapical surgeryresulted in periapical healing. This case outlines the need forcareful preoperative case assessment.
Sajeev Koshy, Robert Matthew Love
Department of Stomatology, School of Dentistry,
University of Otago, PO Box 647, Dunedin, New
Zealand
Key words: a utotransplantation; endodontic
retreatment; periapical surgery; periapical cyst
Dr Robert M.Love, MDS, PhD, FRACDS,Department of
Stomatology, University of Otago, School of Dentistry,
PO Box 647, Dunedin,New Zealand
Tel.:64 34797121
Fax:64 3479 7046
e-mail: [email protected]
Accepted 8 January, 2003

8/3/2019 tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
http://slidepdf.com/reader/full/tic-re-treatment-of-an-auto-transplanted-lower-first-premolar-a-case-report 2/5
balanced occlusion, the lower left ¢rst premolar wasextracted and transplanted to the upper left ¢rst pre-molarsiteby anoraland maxillofacial surgeon duringSeptember 1991. Subsequently, conventional endo-dontictreatmentwascarriedoutbya dentist. Areviewappointment in1993 revealedthat clinically thetrans-plantedtooth was symptomfree,had normal mobilityand no sign of periapical bone loss. The patientreported in May 1997 with an abscess in the regionof the upper left ¢rst premolar, and an apicectomyprocedure with a root-end ¢lling was performed in June 1997 by an oral and maxillofacial surgeon. Adiagnosis of periapicalgranulomawasestablishedhis-tologically. In January 2001, the patient was referredfor an endodontic opinion regarding the tooth thatwas painful and had a recent episode of swelling of the buccal gingiva.
On extra-and intraoral examination,noabnormal-ities were detected except that the upper left ¢rst pre-
molar was discoloured, slightly palatally placed andhada discharging sinus onthe buccal mucosaapprox-imating the position of the apex (Fig.1). The toothwasnot tender topercussion.The dentitionwas molarClass 1 occlusion with a skeletal Class 3. The overbiteandoverjet were within normal limits.The periodon-tium was generally pink and healthy except at themid-buccal of the tooth where there was pocketingof 3 mmbutnobleedingon probing. Sensibilitytestingwas carried out on the neighbouring teeth and allreacted within normal limits.
Radiographic examination revealed loss of laminadura and an area of periapical bone loss 6 mm in dia-
meter associated with the upper left ¢rst premolar(Fig.2). The root canal appeared to be well-obturatedand a root-end amalgam ¢lling was in place. A peria-pical radiograph taken in 1991revealed that the origi-nal root-canal system consisted of two canals (Fig.3).A radiograph taken in 1992 suggested that only onecanal was instrumented and obturated at that time(Fig.4).
Fig.1. Intraoral photograph demonstrating discloured upper
left first premolar with associated draining sinus in buccal
mucosa.
Fig. 2. Periapical radiographtakenat time of presentation. Peri-
apical pathology is evident.
Fig. 3. Periapical radiograph taken immediately after auto-transplantation of the lower left first premolar into the upper
left first premolar area. The reduction in size of the pulp space
in themidrootarea identifies that thecoronal canal separatedto
two apical canals.
Fig. 4. Radiograph taken after initial endodontic treatment.
The obturation pattern indicates that one canal was instrumen-
ted and obturated. The entrance to the second canal was obtu-
rated with sealer.
Endodontic retreatment of an autotransplanted lower premolar
229
8/3/2019 tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
http://slidepdf.com/reader/full/tic-re-treatment-of-an-auto-transplanted-lower-first-premolar-a-case-report 3/5
A diagnosis of chronic periapical periodontitis withdraining sinus was made, and it was decided to per-form orthograde endodontic retreatment in order tolocate the second canal, explore for root fracture,and evaluate healing of the sinus subsequent to clean-ing and shaping the root canal. If healing was evidentwithin 1^2 weeks then conventional retreatmentwould be completed and tooth 12 put under a reviewperiod. If no healing of the sinus took place, it wasplanned to perform conjunctive apical surgery andreview.
An access cavity was prepared, the gutta-perchaand sealer was removed with hand ¢les and chloro-form and the root explored for a palatal canal andforroot fractures. An entranceto a palatalcanalcouldnot be located and no fractures were detected. Thecanal was instrumented in conjunction with 2.5%sodium hypochlorite irrigation and an ethylenedia-minetetraacetic acid preparation (RC Prep, Premier
Dental Products Company, PA, USA), and thendressed with calcium hydroxide andtemporized witha resin reinforced zinc oxide eugenol material (IRM,Dentsply Caulk Milford, DE, USA). At 3 weeks, thedraining sinus was still present, the canal preparationwas optimized, dressed with calcium hydroxide andthe access temporized with IRM. On the next visit,the root canal was obturated by lateral condensationof gutta-percha and sealer(AH plus, DentsplyDetrey,Konstanz, GmbH, Germany) and the tooth tempor-ized with glass ionomer cement (Fuji IX, Shofu Cor-poration, CA, USA). Under local anaesthesia, a fullthickness mucoperiosteal triangular £ap from the
mesialoftheupperleft canineto thedistalof theupperleft ¢rst molar was raised for periradicular surgery.Soft tissue was curetted from the periapical area andsent for histopathological diagnosis. The retrogradeamalgam ¢lling was removed using ultrasonic instru-ments and the root face slightly bevelled to facilitatelocation of the palatal canal. Both the buccal andpalatal canals were prepared with an ultrasonicroot-end preparation tip (Satelac Inc., NJ, USA)and the retroprep ¢lled with mineral trioxide aggre-gate (ProRoot, Dentsply Maillefer, Ballaigues, Swit-zerland). The £ap was approximated and stabilizedwith three 4/0 black silk sutures. A postoperative peri-apical radiograph was taken (Fig.5), and the patientwas instructed on postoperative care.
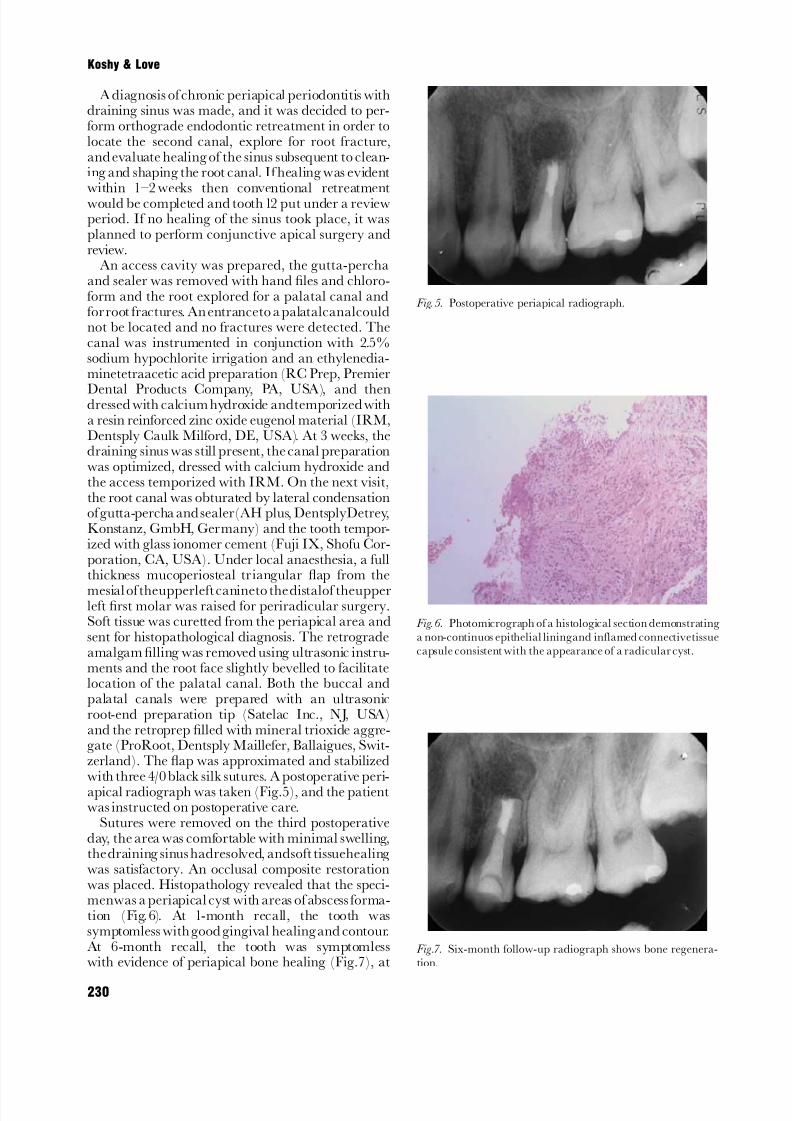
Sutures were removed on the third postoperativeday, the area was comfortable with minimal swelling,thedraining sinus hadresolved, andsoft tissuehealingwas satisfactory. An occlusal composite restorationwas placed. Histopathology revealed that the speci-menwas a periapical cyst with areas of abscess forma-tion (Fig.6). At 1-month recall, the tooth wassymptomless with good gingival healingand contour.At 6-month recall, the tooth was symptomlesswith evidence of periapical bone healing (Fig.7), at
Fig. 5. Postoperative periapical radiograph.
Fig. 6. Photomicrograph of a histological section demonstrating
a non-continuos epithelial liningand inflamed connectivetissue
capsule consistent with the appearance of a radicular cyst.
Fig.7. Six-month follow-up radiograph shows bone regenera-
tion.
230
Koshy & Love

8/3/2019 tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
http://slidepdf.com/reader/full/tic-re-treatment-of-an-auto-transplanted-lower-first-premolar-a-case-report 4/5

8/3/2019 tic Re Treatment of an Auto Transplanted Lower First Premolar_ a Case Report
http://slidepdf.com/reader/full/tic-re-treatment-of-an-auto-transplanted-lower-first-premolar-a-case-report 5/5
Conclusion
This case highlights the importance of conducting adetailed clinical and radiographic examination andthe adherence to evidence-based dentistry prior totreatment planning.
References
1. American Association of Endodontists. Glossary: Contem-poraryTerminology for Endodontics, 6th edn. Chicago, IL:American Association of Endodontists;1998, p. 55.
2. Hovinga J. Autotransplantation of maxillary canines: along-term evaluation. J Oral Surg1969;27:701^8.
3. Slagsvold O, Bjerke B. Applicability of autotransplantationin cases of missing upper anterior teeth. Am J Orthod1978;74:410^21.
4. Schwartz O, Bergmann P, Klausen B. Autotransplantationof human teeth. A life-table analysis of prognostic factors.IntJ Oral Surg1985;14:245^58.
5. Lundberg T, Isaksson S. A clinical follow-up study of 278autotransplanted teeth. Br J Oral Maxillofac Surg1996;34:181^5.
6. Nair PNR, Sjo « gren U, Figdor D, Sundqvist G. Persistentperiapical radiolucencies of root-filled human teeth, failedendodontic treatments, and periapical scars. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1999;87:617^27.
7. Happonen R-P. Periapicalactinomycosis. A follow-up studyof 16 surgically treated cases. Endod Dent Traumatol1986;2:205^9.
8. Sjo « gren U, Happonen R-P, Kahnberg KE, Sundqvist G.Survival of Arachnia propionica in periapical tissue. IntEndodJ 1988;21:277^82.
9. Simon JHS, Chimenti Z, Mintz G. Clinical significance of the pulse granuloma. J Endod 1982;8:116^9.
10. Koppang HS, Koppang R, Solheim T, Aarneals H, StÖlenSÒ. Cellulose fibers from endodontic paper points as anetiologic factor in postendodontic periapical granulomasand cysts. J Endod 1989;15:369^72.
11. Sedgley CM, Messer H. Long-term retention of a paperpoint in the periapical tissues: a case report. Endod DentTraumatol 1993;9:120^3.
12. Sjo « gren U, Sundqvist G, Nair PNR. Tissue reaction togutta-percha particles of various sizes when implantedsubcutaneously in guinea pigs. Eur J Oral Sci 1995;103:313^21.
13. Simon JHS. Incidence of periapical cysts in relation to theroot canal. J Endod 1980;6:845^8.
14. Nair PNR, Sjo « gren U, Schumacher E, Sundqvist G. Radi-cular cyst affecting a root-filled human tooth: a long-term
post treatment follow-up. Int Endod J 1993;26:225^33.15. Tskiboshi M. Autotransplantation of teeth: requirements forpredictable success. Dent Traumatol 2002;18:157^80.
16. Pineda F, Kuttler Y. Mesiodistal and buccolingual roent-genographic investigation of 7275 root canals. Oral Surg1972;33:101^10.
17. Zillich P, Dowson J. Root canal morphology of mandibularfirst and second premolars. Oral Surg Oral Med OralPathol 1973;36:738^44.
18. Sundqvist G, Figdor D, Sjo « gren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcomeof conservative re-treatment. Oral Surg Oral Med OralPathol Oral Radiol Endod 1998;85:86^93.
19. Chong BS, Pitt Ford TR. Endodontic retreatment. Part 1.Indications and case selection. Dent Update 1996;23:320^8.
20. Rud J, Andreasen JO, Jensen JE. A follow-up of study of 1,000 cases treated by endodontic surgery. Int J Oral Surg1972;1:215^28.
21. Allen RK, Newton CW, Brown CE. A statistical analysisof surgical and non-surgical endodontic retreatment cases.
J Endod 1989;5:261^6.22. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjo «
B, Engstro « m B. Retreatment of endodontic fillings. Scand J Dent Res 1979;87:217^24.
23. Molven O.The frequency, technical standard and results of endodontic therapy. Thesis. University of Bergen, Bergen;1974.
24. Sjo « gren U, Hagglund B, Sundqvist G, Wing K. Factorsaffecting the long-term results of endodontic treatment.
J Endod 1990;16:498^504.25. Nair PNR, Pajarola G, Schroeder HE.Types and incidence
of human periapical lesions obtained with extracted teeth.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1996;81:93^102.
232
Koshy & Love


















