Thyroid functions & its disorders Dr. Shafali Singh.
87
Thyroid functions & its disorders Dr. Shafali Singh
-
Upload
wilfred-douglas -
Category
Documents
-
view
216 -
download
2
Transcript of Thyroid functions & its disorders Dr. Shafali Singh.

Thyroid functions &
its disorders
Dr. Shafali Singh

Objectives
• Describe briefly the synthesis of thyroid hormones
• Physiological actions of thyroid hormones• Regulation of thyroid hormone secretion• Explain the pathogenesis of common thyroid
disorders ( Grave’s Disease, Hypothyroidism and Hyperthyroidism)



Iodine Is Required for Formation of Thyroxine
• To form normal quantities of thyroxine, about 50 milligrams of ingested iodine in the form of iodides are required each year, or about 1 mg/week.
• To prevent iodine deficiency, common table salt is iodized with about 1 part sodium iodide to every 100,000 parts sodium chloride.


folliclecell
extracellular space
colloid space
Initial Steps in Thyroid Hormone Synthesis
I-
I-
thyroglobulin withmonoiodotyrosines and diiodotyrosines
iodination
Thyroglobulin
thyroglobulin
gene
I+ oxidation
I-Na+ 2Na+K+
ATPase
pendrin


Biosynthesis of thyroid hormones
• Iodide trapping : The follicular cells take up Iodides from plasma by active transport (Iodide pump); T.S.H. stimulates this process
• Oxidation of Iodide to Iodine: Iodide is oxidized to Iodine by the peroxidase enzyme system, to form nascent iodine or I3
- that is capable to bind with amino acid tyrosine.
• Iodination of Tyrosine: Iodine is bound to the tyrosine at the 3 position to form 3 monoiodotyrosine (MIT) & then 5position to form 3,5 Diiodotyrosine (DIT)

Iodination of Tyrosine- “Organification” of Thyroglobulin

Coupling of iodinated tyrosine






Overall Effects of Thyrotropin (TSH) on the Thyroid
Rapidly induced TSH effects
TSH tends to rapidly increase (within minutes or an hour) all steps in the syn-thesis and degradation of thyroid hormones, including:• Iodide trapping• Thyroglobulin synthesis and
exocytosis into the follicular lumen
• Pinocytotic reuptake of iodinated thyroglobulin back into the thyroid follicular cell
• Secretion of T4 into the blood
Slowly induced TSH effects
Changes that occur more slowly (hours or days) in response to TSH include:• Increased blood flow to the
thyroid gland• Increased hypertrophy or
hyperplasia of the thyroid cells, which initially leads to increased size of the gland or goiter

• Approximately 90% of the thyroid's output is (thyroxine, or T4). T4 is primarily a prohormone.
• About 10% is (T3), which is the active form of thyroid hormone.
• Less than 1% of thyroid output is (reverse T3, or rT3), which is inactive.

TRANSPORT AND METABOLISM OF THYROID HORMONES
• Secreted T4 and T3 circulate in the bloodstream almost entirely bound to proteins.
• The major binding protein is thyroxine-binding globulin (TBG). TBG is synthesized in the liver and binds one molecule of T4 or T3.
• Normally, only about 0.03% of total plasma T4 and 0.3% of total plasma T3 exist in the free state.
• Free T3 is biologically active and mediates the effects of thyroid hormone on peripheral tissues

TRANSPORT OF THYROID HORMONES IN BLOOD

The thyroid axis relies heavily on peripheral conversion through the action of thyronine-specific deiodinases
• Most conversion of T4 to T3 by type 1 deiodinase occurs in tissues with high blood flow and rapid exchanges with plasma, such as the liver, kidneys, and skeletal muscle.
• The brain maintains constant intracellular levels of T3 by a high-affinity deiodinase called type 2 deiodinase.
• There is also an "inactivating" deiodinase called type 3 deiodinase. Converts T4 to the inactive rT3. Type 3 deiodinase is increased during hyperthyroidism, which helps blunt the overproduction of T4

fasting, medical and surgical stresses, catabolic dis-eases, excess cortisol

• Certain clinical states are associated with a reduction in the conversion of T4 into T3, often with an enhanced conversion of T4 into rT3 (low T3 syndrome).
• Such states would include fasting, medical and surgical stresses, catabolic dis- eases.
• The result is a reduction in metabolic rate and a conservation of energy resources. In the early stages, the circulating T4 is normal but in many cases as the metabolic problem or stress becomes more severe, T4 can fall as well.

IN THE CLINIC
• Because of its ability to trap and incorporate iodine into thyroglobulin (called organification), the activity of the thyroid can be assessed by radioactive iodine uptake (RAIU).

Subacute thyroiditis: overall a below-normal uptake of isotope Grave’s disease: increased tracer uptake that is distributed evenlythroughout the enlarged glandToxic adenomas: local areas of increased uptake with below-normal uptake in the remainder of the glandToxic multinodular goiter: enlarged gland that often has an abnormal architecture and with multiple areas of high and low uptake.


Regulation of thyroid hormone synthesis



Factors affecting thyroid hormone secretion
• Stimulatory factors:
1. TSH2. Thyroid stimulating immunoglobulins3. Increased TBG levels (pregnancy)

• the concentration of free thyroid hormones falls.
• decrease in the concentration of free thyroid hormones in the circulation stimulates TSH secretion,
• which in turn causes an increase in the production of free thyroid hormones.
• A new equilibrium is eventually reached at which the total quantity of thyroid hormones in the blood is elevated but the concentration of free hormones, the rate of their metabolism, and the rate of TSH secretion are normal.
• Corresponding changes in the opposite direction occur when the concentration of thyroid-binding protein is reduced. Consequently, patients with elevated or decreased concentrations of binding proteins, particularly TBG, are typically neither hyper- nor hypothyroid; that is, they are euthyroid
Increase in TBG Decrease in TBG

10 TSH; 100 Thyroid hor; 98 bound ; 2free
• Plasma pro inc (99)• Bound incr (99)• Free dec < 2 (1)• TSH inc ( 11)• Thyroid hr inc (101)• Bound 99 (inc)• Free 2• TSH dec to normal 10
• Plasma pro dec (97)• Bound dec (97)• Free dec > 2 (3)• TSH dec( 9)• Thyroid hr dec (99)• Bound 97 (dec)• Free 2• TSH inc to normal 10


A 33-year-old woman is noted by her physician to have some fatigue. She is three months in to her pregnancy. The following laboratories have been returned:TSH 1.0 mU/L (0.35-6.0 mU/L)Free thyroxine 1.0 ng/dL (0.8-2.7 ng/dL)Total thyroxine 13.0 μg/dL (4.5-12.0 μg/dL)Thyroid-binding globulin (TBG) 55 ng/mL (15-34 mg/L)Which of the following is the most likely diagnosis?a) Hyperthyroidismb) HypothyroidismC) Normal thyroid status

Mechanism of action of thyroid hormone
• Most of the Thyroxine Secreted by the Thyroid Is Converted to Triiodothyronine
• Thyroid Hormones Activate Nuclear Receptors.


• Physiologic Functions of theThyroid Hormones

Thyroid Hormones Increase Cellular Metabolic Activity
• metabolic rate can increase to 60 to 100 per cent above normal .
Mitochondria- increase in size & number - membrane surface area increases the rate of formation of adenosine
triphosphate (ATP) to energize cellular function. • Thyroid Hormones Increase Active Transport of Ions
Through Cell Membranes.• One of the enzymes that increases its activity in
response to thyroid hormone is Na+-K+ ATPase.

On carbohydrate metabolism
1. peripheral utilization of glucose (insulin like action)- hypoglycemia
2. Blood glucose (hyperglycemia) Intestinal absorption of glucose glycogenolysis Neoglucogenesis
Stimulation of Carbohydrate Metabolism.

• Protein turnover (release of muscle amino acids, protein degradation and, to a lesser extent, protein synthesis and urea formation) is also increased.
• T3 potentiates the respective stimulatory effects of epinephrine, norepinephrine, glucagon, cortisol, and growth hormone on gluconeogenesis, lipolysis, ketogenesis, and proteolysis of the labile protein pool.
• In addition, thyroid hormone stimulates the synthesis of cholesterol, but more so its oxidation and biliary secretion. The net effect is a decrease in the body pool and plasma levels of total and low-density lipoprotein cholesterol

• Increased O2 use ultimately depends on an increased supply of substrates for oxidation.
• T3 augments glucose absorption from the gastrointestinal tract and increases glucose turnover (glucose uptake, oxidation, and synthesis).
• In adipose tissue, thyroid hormone induces enzymes for the synthesis of fatty acids, acetyl-CoA carboxylase, and fatty acid synthase and enhances lipolysis by increasing the number of β-adrenergic receptors . Thyroid hormone also enhances the clearance of chylomicrons. Thus, lipid turnover (FFA release from adipose tissue and oxidation) is augmented

Respiratory Effects • Thyroid hormone stimulates O2 utilization and
also enhances O2 supply.
• Appropriately, T3 increases the resting respiratory rate, minute ventilation, and the ventilatory response to hypercapnia and hypoxia.
• Additionally, the hematocrit increases slightly and thereby enhances the O2-carrying capacity.

• Thermogenesis must also increase concomitantly with O2 use. Thus, changes in body temperature parallel fluctuations in availability of thyroid hormone.
• The potential increase in body temperature, however, is moderated by a compensatory increase in heat loss through appropriate thyroid hormone-mediated increases in blood flow, sweating, and ventilation.

Effect of Thyroid Hormones on the Cardiovascular System

Skeletal Muscle Effects • Glycolysis and glycogenolysis are increased and
glycogen and creatine phosphate are reduced by an excess of T4 and T3..
• Slight increase in thyroid hormone usually makes the muscles react with vigor,
• but when the quantity of hormone becomes excessive, the muscles become weakened because of excess protein catabolism.
• Conversely, lack of thyroid hormone causes the muscles to become sluggish, and they relax slowly after a contraction.

Muscle Tremor
• increased reactivity of the neuronal synapses in the areas of the spinal cord that control muscle tone.
• occurs at the rapid frequency of 10 to 15 times per second.

Effects on the Autonomic Nervous System and Catecholamine Action
• There is synergism between catecholamines and thyroid hormones.
• Thyroid hormones are synergistic with catecholamines in increasing the metabolic rate, heat production, heart rate, motor activity, and excitation of the central nervous system.
• T3 may enhance sympathetic nervous system activity by increasing the number of β-adrenergic receptors in heart muscle and the generation of intracellular second messengers, such as cAMP.

Effects on Growth and Maturation
• A small but crucial amount of thyroid hormone crosses the placenta, and the fetal thyroid axis becomes functional at midgestation.
• Thyroid hormone is extremely important for normal neurological development and proper bone formation in the fetus.
• In infants, insufficient fetal thyroid hormone causes cretinism, characterized by irreversible mental retardation and short stature

Effects on Bone, Hard Tissue, and Dermis
• Thyroid hormone stimulates endochondral ossification, linear growth of bone, and maturation of the epiphyseal bone centers.
• T3 also stimulates adult bone remodeling. The progression of tooth development and eruption depends on thyroid hormone, as does the normal cycle of growth and maturation of the epidermis, its hair follicles, and nails.
• The normal degradative processes in these structural and integumentary tissues are also stimulated by thyroid hormone.

Effects on the Nervous System
• Thyroid hormone regulates the timing and pace of development of the central nervous system.
• Thyroid hormone deficiency in utero and in early infancy decreases growth of the cerebral and cerebellar cortex, proliferation of axons and branching of dendrites, synaptogenesis, myelinization, and cell migration.
• Irreversible brain damage results when thyroid hormone deficiency is not recognized and treated promptly after birth

Effects on the Nervous System • Thyroid hormone also enhances wakefulness,
alertness, responsiveness to various stimuli, auditory sense, awareness of hunger, memory, and learning capacity.
• In addition, normal emotional tone depends on proper thyroid hormone availability.
• Speed and amplitude of peripheral nerve reflexes are increased by thyroid hormone, as is motility of the gastrointestinal tract.

Effects on Reproductive Organs and Endocrine Glands
• In both women and men, thyroid hormone plays an important, permissive role in the regulation of reproductive function.
• The ratio of estrogens to androgens is increased in men (in whom breast enlargement may occur with hyperthyroidism

Physiologic Effects of Thyroid Hormones.
Target Tissue Effect Mechanism
Heart Chronotropic Inotropic Increased number of -adrenergic receptors
Enhanced responses to circulating catecholamines
Increased proportion of -myosin heavy chain (with higher ATPase activity)
Adipose tissue Catabolic Stimulated lipolysis
Muscle Catabolic Increased protein breakdown
Bone Developmental Promote normal growth and skeletal development
Nervous system Developmental Promote normal brain development
Gut Metabolic Increased rate of carbohydrate absorption
Lipoprotein Metabolic Formation of LDL receptors
Other Calorigenic Stimulated oxygen consumption by metabolically active tissues (exceptions: testes, uterus, lymph nodes, spleen, anterior pituitary)
Increased metabolic rate

Diseases of the Thyroid

TESTS OF THYROID FUNCTION• Determining the serum TSH is the first step in evaluating thyroid
function.• Secondly, free T4 (FT4) measurements are now readily available
and would confirm an initial conclusion based on the TSH measurement.
• An alternative test would be an index of the free T4 via resin uptake.
• Thirdly, a TRH stimulation is not usually necessary, but would differentiate secondary from tertiary hypofunction.
• Autoimmune thyroid disease is easily detected by measuring circulating antibodies. Most notably are the TPO antibodies, which are elevated in Hashimoto’s thyroiditis (hypothyroidism) and Grave’s disease (hyperthyroidism).
• Additional antibodies are those against thyroglobulin and the TSI antibodies that stimulate the TSH receptor in Grave’s disease.

Causes of HyperthyroidismPrimary • Toxic multinodular goiter,• (Graves disease); accounts for 60–80% of the cases• Solitary toxic adenoma • Subacute and silent thyroiditis
Secondary• TSH-secreting pituitary tumor • Administration of T3 or T4 (factitious or iatrogenic hyperthyroidism)
• Ectopic thyroid tissue

Hyperthyroidism
• Causes of Hyperthyroidism (Toxic Goiter, Thyrotoxicosis, Graves’ Disease)
• Antibodies that cause hyperthyroidism occur as the result of autoimmunity that has developed against thyroid tissue
• These antibodies are called thyroid-stimulating immunoglobulinand (TSI ).

Primary Hyperthyroidism (Grave’s Disease)
• Thyrotoxicosis by definition is the clinical syndrome whereby tissues are exposed to high levels of thyroid hormone (= hyperthyroidism)
• The most common cause of thyrotoxicosis is Grave’s disease, a primary hyperthyroidism.
• Grave’s disease is an autoimmune problem in which one antibody is directed against the thyroid receptor. It is referred to as the thyroid stimulating antibody (TSI or TSH-R).
• In addition TPO antibodies and those against thyroglobulin are also found in Grave’s disease.
• ↑ FT4, ↓ TSH; it is the TSI stimulating the TSH receptor on the thyroid that is driving the hyperthyroidism.
• In Grave’s disease the thyroid is symmetrically enlarged.• Additional laboratory findings would be increased radioiodine uptake by
the thyroid and decreased serum cholesterol.

Signs and Symptoms of Thyrotoxicosis (Descending Order of Frequency)
Symptoms• Hyperactivity, irritability,
dysphoria• Heat intolerance and
sweating• Palpitations• Fatigue and weakness• Weight loss with
increased appetite• Diarrhea
Signs• Tachycardia• Tremor• Goiter• Warm, moist skin• Muscle weakness,
proximal myopathy• Lid retraction or lag

Signs of ophthalmopathy and dermopathy specific for Graves‘ disease



Causes of HypothyroidismPrimary• Autoimmune hypothyroidism: Hashimoto's thyroiditis (an
autoimmune destruction of the thyroid with lymphocytic infiltration; ↑ TPO antibodies; earlystages have a diffusely enlarged thyroid progressing in the later stages to a smaller atrophic and fibrotic gland.)
Iatrogenic: 131I treatment, subtotal or total thyroidectomy, external irradiation of neck ; Lithium
Severe Iodine deficiency Secondary Hypopituitarism: tumors, pituitary surgery or irradiation,
infiltrative disorders,

Signs and Symptoms of Hypothyroidism (Descending Order of Frequency)
Symptoms• Tiredness, weakness• Dry skin• Feeling cold• Hair loss• Difficulty concentrating
and poor memory• Constipation• Weight gain with poor
appetite• Dyspnea• Hoarse voice
Signs• Dry coarse skin; cool
peripheral extremities• Puffy face, hands, and
feet (myxedema)• Diffuse alopecia• Bradycardia• Peripheral edema• Delayed tendon reflex
relaxation


Myxedema.
• Increased quantities of hyaluronic acid and chondroitin sulfate bound with protein form excessive tissue gel in the interstitial spaces, and this causes the total quantity of interstitial fluid to increase.
• Because of the gel nature of the excess fluid, it is mainly immobile, and the edema is the non pitting type

Accumulation of subcutaneous mucopolysaccharides that give rise to a nonpitting edema (myxedema)Myxedema coma is the end stage of untreated hypothyroidism. Themajor features are hypoventilation, fluid and electrolyte imbalances, andhypothermia and ultimately shock and death.

Treatment
• Replacement doses of T4. The goal is to give enough T4 to normalize serum TSH.
• Because metabolism of T4 decreases and the plasma half-life increases with age, higher doses of T4 are required in younger individuals.
• Overall levels of TSH must be checked on occasion to make sure of the proper dosage of T4.
• In women beyond menopause, overdosing with T4 can contribute to the development of osteoporosis.

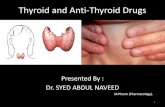
Cretinism
• Caused by extreme hypothyroidism during fetal life, infancy, or childhood. • failure of body growth and mental retardation. • Cause: congenital lack of thyroid gland (congenital
cretinism) genetic defect of the gland severe iodine lack in the diet (endemic cretinism).

• , Normal 6-year-old child (left) and a congenitally hypothyroid 17-year-old child (right) from the same village in an area of endemic cretinism.
• Short stature, obesity, malformed legs, and dull expression of the mentally retarded hypothyroid child. Other features are a prominent abdomen, a flat broad nose, a hypoplastic mandible, dry scaly skin, delayed puberty, and muscle weakness

• Skeletal growth more inhibited than soft tissue growth.
• soft tissues enlarge excessively, giving the child with cretinism an obese, stocky, and short appearance.
• Occasionally the tongue becomes so large that it obstructs swallowing and breathing.

CRETINISM

Goiter
• A goiter is simply an enlarged thyroid and does not designate functional status.
• A goiter can be present in hypo-, hyper-, and euthyroid states.
• There is no correlation between thyroid size and function.• A generalized enlargement of the thyroid is considered a
“diffuse goiter.”• Diffuse enlargement often results from prolonged
stimulation by TSHor TSH-like factor; e.g., Hashimoto’s thyroiditis, Grave’s disease, diet deficient in iodine

• How could an iodine-deficient diet lead to goiter, which is an enlargement of the thyroid gland?




• An irregular or lumpy enlargement of the thyroid is considered a “nodular goiter.”
• With time, excessive stimulation by TSH can result in a multinodular goiter
• e.g. iodine deficiency initially produces a diffuse nontoxic goiter.
• Long term however, focal hyperplasia with necrosis and hemorrhage results in the formation of nodules. Nodules vary from “hot nodules” that can trap iodine to “cold nodules “ that cannot trap iodine.


A 41-year-old woman presents to her primary care physician with weight and hair loss, diarrhea, nervousness, and eye pressure. She has no medical problems,but some of her family members have similar symptoms and require medication. On examination, she is noted to have exophthalmos, an enlarged nontender goiter, hyperreflexia, and a tremor when her arms are outstretched.The patient has a decreased thyroid-stimulating hormone (TSH) level and an increased free thyroxine (T4) level and is diagnosed with ? Graves disease (hyperthyroidism).
◆ What is the mechanism by which high levels of iodine inhibit thyroid production?
◆ How does propylthiouracil (PTU) inhibit thyroid synthesis?
◆ What affect does pregnancy have on the free thyroid hormone level?


A young lady is presenting to your office. She complains of heat intolerance, difficulty sleeping, anxiety, palpitations, and losing weight despite increased appetite. On physical examination you notice a stare in this patient, hypereflexia and bruit heard other the thyroid. Which of the lab test will you expect to find in this patient:
A) HIGH TSH, T4 and T3B) Low TSH, High T4 and T3C) Normal TSH, T4 and T3D) High TSH, Normal T3 and High T4E) Low TSH, T4 and T3


Which of the following is inconsistent with the diagnosis of Graves’ disease?
A) Increased heart rateB) ExophthalmosC) Increased plasma levels of triiodothyronine
(T3)D) Increased plasma levels of thyroxine (T4)E) Increased plasma levels of thyroid-stimulatinghormone

A patient has an elevated plasma thyroxine (T4) concentration,a low plasma thyroid-stimulating hormone (TSH) concentration, and a thyroid gland that is smaller than normal. Which of the following is the most likely explanation for these findings?
A) Patient has a lesion in the anterior pituitary thatprevents TSH secretionB) Patient is taking propylthiouracilC) Patient is taking thyroid extractD) Patient is consuming large amounts of iodineE) Patient has Graves disease

A 46-year-old man has “puffy” skin and is lethargic.His plasma thyroid-stimulating hormone concentrationis low and increases markedly when he is giventhyrotropin-releasing hormone. Which of the followingis the most likely diagnosis?A) Hyperthyroidism due to a thyroid tumorB) Hyperthyroidism due to an abnormality in thehypothalamusC) Hypothyroidism due to an abnormality in thethyroidD) Hypothyroidism due to an abnormality in the
hypothalamusE) Hypothyroidism due to an abnormality in thepituitary