Thyroid Disorders in Pregnancy 2012

of 80
-
Upload
kathleenzuniga -
Category
Documents
-
view
220 -
download
1
Transcript of Thyroid Disorders in Pregnancy 2012
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
1/80
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
2/80
1DEFINITION OF TERMS
2PHYSIOLOGIC CHANGES IN THYROID FUNCTION DURING
PREGNANCY
Thyroid Function and the Fetus
3HYPERTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
4HYPOTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
3/80
5
CLINICAL CONSIDERATIONS & RECOMMENDATIONS
What laboratory tests are used to diagnose and manage thyroid disorderduring pregnancy?
What medications can be used to treat hyperthyroidism and
hypothyroidism in pregnancy, and how should they be administered and
adjusted during pregnancy?
What changes in thyroid function occur with hyperemesis gravidarum, and
should TFTs be performed routinely in women with hyperemesis?How is thyroid storm diagnosed and treated in pregnancy?
How should a thyroid nodule or thyroid cancer should during pregnancy
be assessed?
How is postpartum thyroiditis diagnosed and treated?
Which pregnant patients should be screened for thyroid dysfunction?
6
SUMMARY OF RECOMMENDATIONS
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
4/80
Thyroid Gland:
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
5/80
Thyroid System:
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
6/80
Second most common endocrinedisease affecting women of
reproductive age
Both HYPERTHYROIDISMandHYPOTHYROIDISMmay INITIALLY
manifest during pregnancy
Obstetric conditions MAYaffectthyroid gland function
gestational trophoblastic disease
hyperemesis
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
7/80
Thyrotoxicosisa clinical and biochemical state
excess production of and exposure to thyroid hormone
Hyperthyroidismthyrotoxicosis caused by hyperfunctioning of the thyroid
gland
Gravesdiseaseautoimmune disease
production of (TSI) and (TBII) that act on (TSH) receptor
to mediate thyroid stimulation or inhibition respectively
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
8/80
Thyroid storm
severe, acute exacerbation of the signs and symptoms of
hyperthyroidism
Hypothyroidism
caused by inadequate thyroid hormone productionPostpartum thyroiditis
autoimmune inflammation of the thyroid gland
presents as new-onset, painless hypothyroidism,
transient thyrotoxicosis or thyrotoxicosis followed byhypothyroidism within 1 year postpartum
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
9/80
1DEFINITION OF TERMS
2PHYSIOLOGIC CHANGES IN THYROID FUNCTION DURING
PREGNANCY
Thyroid Function and the Fetus
3HYPERTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
4HYPOTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
10/80
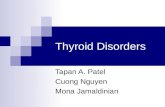
Thyroid function test results change in normal
pregnancy, hyperthyroidand hypothyroidstates as
depicted in TABLE 1
Thyroid binding globulin (TBG) concentrations INCREASESinpregnancy
reduced hepatic clearance
estrogenic stimulation of TBG synthesis
TransientINCREASEin (FT4) and (FTI) in 1sttrimesterNote: Elevations NOT beyond the normal non-pregnant range
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
11/80
Maternal status TSH FT4 FTI TT4 TT3 RT3U
Pregnancy Nochange
Nochange
No change Increase Increase Decrease
Hyperthyroidism Decrease Increase Increase Increase Increase or
no change
Increase
Hypothyroidism Increase Decrease Decrease Decrease Decrease or
no change
Decrease
Table 1. Changes in Thyroid Function Test Results in
Normal Pregnancy and in Thyroid Disease
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
12/80
Plasma iodide levels DECREASEduring
pregnancy
In 15% of women, associated with anINCREASEin thyroid gland size
Thyroid volume, by ultrasonography,
INCREASEDin pregnancy (mean increasesize of 18%)
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
13/80
At 10-12 weeks
fetal thyroid begins concentrating iodine
At 20 weeks
pituitary TSH controls the fetal thyroid
At 36 wks AOG
Mean adult levels of TSH, TBG, FT4 & FT3 are
reached TSH does NOT cross the placenta
Only small amounts of T4 and T3 cross the
placenta
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
14/80
Maternal thyroid hormone CROSSES
the placenta
Prevents overt stigmata of
hypothyroidism at birth
Maintain cord blood thyroid hormone
levels at 25-50% of normal
TRH, iodine and TSH receptor
immunoglobulins CROSS the placenta
as do PTU and methimazole
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
15/80
1DEFINITION OF TERMS
2PHYSIOLOGIC CHANGES IN THYROID FUNCTION DURING
PREGNANCY
Thyroid Function and the Fetus
3HYPERTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
4HYPOTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
16/80
Occurs in 0.2% of pregnancies
95% of cases are due to Gravesdisease
Distinctive symptoms of Gravesdisease: Ophthalmopathy (lid lag and lid retraction)
Dermopathy (localized or pretibial myxedema)
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
17/80
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
18/80
Some symptoms of hyperthyroidisimare SIMILAR
to symptoms ofpregnancyor nonthyroid disease,
SERUM TFTS differentiate thyroid disease from
nonthyroid disease.
Inadequately treated maternal thyrotoxicosis is
associated with a GREATER RISK of preterm
delivery, severe preeclampsia and heart failure
UNTREATED hyperthyroidism is associated with
miscarriage
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
19/80
Inadequately treated hyperthyroidism is associatedwith an increase in medically indicated
preterm deliveries
low birth weight (LBW)
possible fetal loss
In one study, all of seven fetal losses occurred in
women with persistent hyperthyroidism
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
20/80
Fetal and neonatal risks associated with Gravesdisease are related to either to:
the disease itself
to thioamide treatment of the disease
The possibility of fetal thyrotoxicosis should beCONSIDERED in ALL WOMEN with a history ofGravesdisease
If FETAL THYROTOXICOSIS is diagnosed, consultationwith a clinician with expertise in such condition iswarranted.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
21/80
Thyroid dysfunction in women is mediated by
antibodies that cross the placenta
Gravesdisease
Chronic autoimmune thyroiditis
Risk of immune-mediated hypothyroidism and
hyperthyroidism to develop in the neonate.
In women with Gravesdisease:
TSI and TBII that can STIMULATEor INHIBITthe fetal thyroid
TBII may cause transient hypothyroidism in neonates of
women with Gravesdisease
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
22/80
1-5% of these neonates have hyperthyroidism or neonatal Graves
disease caused by the transplacental passage of maternal TSI
The incidence is low because of the balance of stimulatory and
inhibitory antibodies with thioamide treatment
Maternal antibodies are cleared less rapidly than thioamides in theneonate, resulting in a sometimes delayed presentation of neonatal
Gravesdisease
The incidence of neonatal Graves disease is unrelated to maternal
thyroid function.
The neonates of women who have been treated surgically or withradioactive iodine prior to pregnancy and require no thioamide
treatment are at higher risk for neonatal Gravesdisease because they
lack suppressive thioamide.14
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
23/80
The most common cause of hyperthyroidism is Graves
disease.
The other clinical characteristics of Graves disease
also are immune-mediated but they are lessunderstood.
The diagnosis of Gravesdisease is generally made by
documenting elevated levels of FT4 or an elevated FTI,
with suppressed TSH in the absence of a nodular
goiter or thyroid mass.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
24/80
Although most patients with Graves disease have
TSH receptor, antimicrosomial, or antithyroid
peroxidise antibodies, measurement of these is
neither required nor recommended to establish thediagnosis
Other etiologies of thyrotoxicosis are excess
production of TSH, gestational trophoblastic
neoplasia, hyperfunctioning thyroid adenoma, toxicmultinodular goiter, subacute thyroiditis, and
extrathyroid source of thyroid hormone.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
25/80
1DEFINITION OF TERMS
2PHYSIOLOGIC CHANGES IN THYROID FUNCTION DURING
PREGNANCY
Thyroid Function and the Fetus
3HYPERTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
4HYPOTHYROIDISM
Signs and Symptoms
Fetal and Neonatal Effects
Etiology and Differential Diagnosis
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
26/80
Having one autoimmune disease INCREASES
the likelihood of developing another;
5-8% incidence of hypothyroid disease in
patients with type 1 diabetes.
25 % risk of developing postpartum thyroid
dysfunction in women with type 1 DM
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
27/80
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
28/80
It is unusual for advanced hypothyroidism to
present in pregnancy
Subclinical hypothyroidism is defined as
elevated TSH with normal FTI in an
asymptomatic patient
Untreated hypothyroidism is associated with
an increased risk ofpreeclampsia
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
29/80
High incidence of LBWin neonates associated
with INADEQUATELY TREATED hypothyroidism
The etiology of LBW in these studies was
preterm delivery, preeclampsia or placental
abruption
Unclear if hypothyroidism is associated with
intrauterine growth restriction
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
30/80
Women with iodine-deficient hypothyroidism are at
significant risk of having babies with congenital
cretinism
growth failure mental retardation
neuropsychologic deficits
In an iodine deficient population, treatment with
iodine in the first and second trimesters of pregnancysignificantly reduces the incidence of the neurologic
abnormalities of cretinism
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
31/80
Untreated congenital hypothyroidism also results incretinism.
The incidence of congenital hypothyroidism is 1 in4,000 newborns and
only 5% of neonates are identified by clinicalsymptoms at birth, likely because of the ameliorativeeffects of maternal thyroid hormone.
If identified and treated within the first few weeks oflife, near-normal growth and intelligence can beexpected
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
32/80
IODINE DEFICIENCY
PRIMARY THYROID ABNORMALITY
HYPOTHALAMIC DYSFUNCTION HASHIMOTOSDISEASE
most common etiology
characterized by production of antithyroidantibodies (thyroid antimicrosomal and
antithyroglobulin antibodies)
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
33/80
IN PREGNANCY OR POSTPARTUM WOMEN,
Most common etiologies of hypothyroidism
Hashimotosdisease subacute thyroiditis
Thyroidectomy
Radioactive iodine treatment
Iodine deficiency
Associated with goiter Not associated with goiter
Hashimotos disease Subacute thyroiditis
Iodine deficiency
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
34/80
5
CLINICAL CONSIDERATIONS AND RECOMMENDATIONS
What laboratory tests are used to diagnose and manage thyroid disorderduring pregnancy?
What medications can be used to treat hyperthyroidism and
hypothyroidism in pregnancy, and how should they be administered and
adjusted during pregnancy?
What changes in thyroid function occur with hyperemesis gravidarum, and
should TFTs be performed routinely in women with hyperemesis?How is thyroid storm diagnosed and treated in pregnancy?
How should a thyroid nodule or thyroid cancer should during pregnancy
be assessed?
How is postpartum thyroiditis diagnosed and treated?
Which pregnant patients should be screened for thyroid dysfunction?
6
SUMMARY OF RECOMMENDATIONS
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
35/80
What laboratory tests are used to
diagnose and manage thyroid
disorder during pregnancy?
What laboratory tests are used to diagnose and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
36/80
Mainstay of thyroid function evaluation:
TSH testing
Now performed using monoclonal antibodies
making it more sensitive than the original
radioimmunoassay.
What laboratory tests are used to diagnose and
manage thyroid disorder during pregnancy?
What laboratory tests are used to diagnose and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
37/80
AACE and ATA, recommend TSHas the INITIAL TEST
for screening and evaluation of symptomatic disease
FREE COMPONENT
is the biologically active portion is not subject to change in conditions that alter TBG,
such as pregnancy.
In PREGNANT patients suspected of being
hyperthyroid or hypothyroid, TSH and FT4 or FTI
should be measured.
What laboratory tests are used to diagnose and
manage thyroid disorder during pregnancy?
What laboratory tests are used to diagnose and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
38/80
FREE THYROXINE assessment by either direct immunoradiometric or chemiluminescent
methods
preferred over the equilibrium dialysis method
FTI calculated as FTI = TT4 x RT3U
if FT4 is not available
FT3
only pursued in patients with thyrotoxicosis with
suppressed TSH but FT4 measurements.
If ELEVATED , T3 thyrotoxicosis (occur before excessive FT4
production develops
What laboratory tests are used to diagnose and
manage thyroid disorder during pregnancy?
What laboratory tests are used to diagnose and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
39/80
TRH STIMULATION TEST evaluates the secretory ability of the pituitary
ANTIBODY TESTS
TSH RECEPTOR ANTIBODIES either stimulatory (TSI) or inhibitory (TSII)
ANTIMICROSOMAL ANTIBODIES
TSI
Elevated in neonatal Gravesdisease
clinical usefulness is not clear
no practical use for measuring routinely
endocrinologists suggest that its measurement in the third trimester
What laboratory tests are used to diagnose and
manage thyroid disorder during pregnancy?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
40/80
What medications can be used to
treat hyperthyroidism and
hypothyroidism in pregnancy?
How should they be administeredand adjusted during pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
41/80
Thioamides (PTU and Methimazole)DECREASE thyroid hormone synthesis
by blocking the organification of iodide
PTU also reduces the peripheral
conversion of T4 to T3 quicker suppressant effect than methimazole
PTU is preferred in pregnancy crossed the placenta LESS WELL than methimazole
Methimazole associated with FETAL APLASIA CUTIS
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
42/80
NO SIGNIFICANT DIFFERENCE in mean FT4 or TSH
levels in newborn umbilical cord blood samples
between PTU and methimazole treated mothers
NO RELATIONSHIP between maternal dosage ofthioamide and umbilical cord blood levels of TSH or
FT4
NO SIGNIFICANT DIFFERENCE in incidence of aplasia
cutis between control women without thyroid
disease and women with hyperthyroidismwho were
treated with methimazole
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
43/80
can suppress Fetal and neonatal thyroid function Transient and rarely requires therapy
Fetal goiter
caused by drug-induced fetal hypothyroidism
Fetal thyrotoxicosis secondary to maternal antibodies (rare)
Monitor ALL fetuses for appropriate growth and normal
heart rate
routine screening for fetal goiter by ultrasonography isUNNECESSARY
Neonatal thyroid dysfunction
- All neonates of women with thyroid disease are at risk
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
44/80
PTU and Methimazole safe during BREASTFEEDING only small amounts cross into the breastmilk
GOAL OF MANAGEMENT:
To maintain the FT4 or FTI in the high normal range
To use the lowest possible dosage of thioamidestominimize fetal exposure to the drug
MONITORING:
FT4 or FTI every 2-4 weeks
titrate the thioamide until FT4 or FTI are consistently inthe high normal range
In more than 90% of patients, improvement is seenwithin 2-4 weeks after treatment begins
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
45/80
AGRANULOCYTOSIS Occurs in 0.1-0.4% - Fever and sore throat
CBC should be drawn - Discontinue medication
Cross reaction with other thioamides THROMBOCYTOPENIA
HEPATITIS
VASCULITIS- occur in less than 1% of patients Minor side effectsin 5% of patients
rash, nausea, arthritis, anorexia, fever and loss of taste or smell
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
46/80
BETA-BLOCKERS
may be used to ameliorate the symptoms of
thyrotoxicosis until thioamides decrease thyroid
hormone levels. Propranolol is the most common -blocker used
for this indication.
THYROIDECTOMY reserved for women in whom thioamide treatment
is unsuccessful.
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
47/80
IODINE 131
is CONTRAINDICATEDin pregnant womenrisk of fetal
thyroid ablation
Avoid pregnancy for 4 months after I-131 treatment.
IF at less than 10 weeks of gestation when exposed to I-
131, it is unlikely the fetal thyroid was ablated.
If exposure occurred at 10 weeks or later, the woman must
consider the risks of induced congenital hypothyroidism.
Breastfeeding should be avoided for at least 120 days after
treatment with I-131
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
What medications can be used to treat
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
48/80
SAME as for nonpregnantwomen LEVOTHYROXINE
at sufficient dosages to normalize TSH levels.
4 weeks for thyroxine to alter the TSH level
pregnancy increases maternal thyroid hormone
requirements
TSH levels INCREASED while FTI DECREASED during
pregnancy
INCREASE thyroxine dosage from 0.1mg/day to
0.148mg/day
check TSH levels every trimester
What medications can be used to treat
hyperthyroidism and hypothyroidism in pregnancy?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
49/80
What changes in thyroid function
occur with hyperemesis
gravidarum?
Should TFTs be performedroutinely in women with
hyperemesis?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
50/80
How is thyroid storm diagnosedand treated in pregnancy?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
51/80
What changes in thyroid function
occur with hyperemesis
gravidarum?
Should TFTs be performedroutinely in women with
hyperemesis?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
52/80
How is thyroid storm diagnosed
and treated in pregnancy?
Treatment of Thyroid Storm in
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
53/80
Treatment of Thyroid Storm in
Pregnant Women:
1 Propylthiouracil (PTU), 600-800 mg orally stat, then
150-200 mg orally every 4-6 hours. If oral
administration is not possible, use methimazole
rectal suppositories.2 Starting 1-2 hours after PTU administration, saturated solutionof potassium iodide (SSKI), 2-5 drops orally every 8 hours, or
Sodium iodide, 0.5 to 1.0 g/IV every 8 hours, or
Lugols solution, 8 drops every g hours, or Lithium carbonate, 300 mg orally every 6 hours.
3 Dexamethasone, 2mg/IV or IM every 6 hours for 4
doses
Treatment of Thyroid Storm in
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
54/80
4 Propranolol, 20-80 mg orally every 4-6 hours, or
propranolol, 1-2 mg IV every 5 minutes for a total of 6
mg, then 1-10 mg IV every 4 hours.
If the patient has a history of severe
bronchospasm:
Reserpine, 1-5 mg IM every 4-6 hours
Guanethidine, 1mg/kg orally every 12 hours
Diltiazem, 60 mg orally every 6-8 hours5 Phenobarbital, 30-60 mg orally every 6-8 hours as
needed for extreme restlessness
Treatment of Thyroid Storm in
Pregnant Women:
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
55/80
How should a thyroid nodule or thyroidcancer during pregnancy be assessed?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
56/80
How is postpartum thyroiditis
diagnosed and treated?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
57/80
Which pregnant patients
should be screened for thyroid
dysfunction?
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
58/80
.
Level A Recommendation
Levels of TSH or FT4/FTI should be
monitored to manage thyroid
disease in pregnancy
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
59/80
.
Level B Recommendation
The following recommendations arebased on limited or inconsistentscientific evidence
Either PTU or Methimazole can be usedto treat pregnant women withhyperthyroidism
Thyroid function tests are not indicatedin asymptomatic pregnant women withslightly enlarged thyroid glands.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
60/80
.
Level C Recommendation
There is no need to measure TFTs
routinely in women with
hyperemesis.
There are insufficient data to
warrant routine screening of
asymptomatic pregnant women for
hypothyroidism.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
61/80
.
Level C Recommendation
Indicated testing of thyroid functionmay be performed in women with apersonal history of thyroid disease or
symptoms of thyroid disease. The presence of maternal thyroid
disease is important information to thepaediatrician to have at the time ofdelivery.
Thyroid nodules should be investigatedto rule out malignancy
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
62/80
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
63/80
What changes in thyroid function occur with hyperemesis gravidarum
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
64/80
What changes in thyroid function occur with hyperemesis gravidarum,
and should TFTs be performed routinely in women with
hyperemesis?
Nausea and vomiting of pregnancy have been attributed to thehigh HCG levels in the first trimester, and women with hyperemesis
gravidarum have been assumed to have particularly high HCG levels
and to be at risk for hyperthyroidism. Complete resolution of
biochemical and clinical hyperthyroidism also has been reported in
other studies. 37,38 These studies have reported that some
women with hyperemesis gravidarum required a short course of
thioamides; however, most had resolution of their signs and
symptoms without treatment. 38,39 Women who required
treatment throughout pregnancy had other symptoms of thyroiddisease, including thyroid enlargement, persistent tachycardia
despite fluid replacement and abnormal response to TRH
stimulation. 39
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
65/80
In a study comparing pregnant women with hyperemesis andthose without hyperemesis, there was no difference in mean
TSH or FT3 levels. 40 Levels of FT4 and HCG were significantly
higher in women with hyperemesis but HCG levels correlated
significantly and positively with FT4 levels and negatively withTSH levels only in the hyperemesis group. Hyperemesis
gravidarum is associated with biochemical hyperthyroidism
but rarely with clinical hyperthyroidism and is largely
transitory, requiring no treatment. Routine measurements of
thyroid function are not recommended in patients with
hyperemesis gravidarum unless other overt signs of
hyperthyroidism are evident.
How is thyroid storm diagnosed and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
66/80
How is thyroid storm diagnosed and
treated in pregnancy?
Thyroid storm is a medical emergency characterized byan extreme hypermetabolic state. It is rare, about 1%, but has
a high risk of maternal heart failure. 9 Older literature
described a maternal mortality of 25% but this has not been
substantiated by more recent data. 9,41 It is diagnosed by acombination of the following: fever, tachycardia out of
proportion to the fever, changed mental status, vomiting,
diarrhea and cardiac arrhythmia. 42 Often there is an inciting
event such as infection, surgery, labor or delivery. Diagnosis
can be difficult to make and requires expedient treatment to
avoid the severe consequences of untreated thyroid storm,
which include shock, stupor and coma
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
67/80
. If thyroid storm is suspected, serum FT4, FT3 and TSH levelsshould be evaluated to help confirm the diagnosis, buttherapy should not be withheld pending the results.
Therapy for thyroid storm consists of a standard series ofdrugs (see Box). PTU or methimazole blocks additionalsynthesis of thyroid hormone, and PTU also inhibits peripheralconversion of T4 to T3. Saturated solution of potassiumiodide and sodium iodide block the release of thyroidhormone from the gland. Dexamethasone decreases thyroid
hormone release and peripheral conversion of T4 to T3, andpropranolol inhibits the adrenergic effects of excessive thyroidhormone.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
68/80
Finally, Phenobarbital can be used to reduce extreme agitation orrestlessness and may increase the catabolism of thyroid hormone. 42
General supportive measures should also be undertaken, including
administration of oxygen, maintenance of intravascular volume and
electrolytes, use of antipyretics, use of a cooling blanket, and appropriate
maternal and fetal monitoring; invasive central monitoring and continuousmaternal cardiac monitoring in an ICU setting may be indicated. The
perceived underlying cause of the storm should also be treated. As with
other acute maternal illnesses, fetal well-being should be appropriately
evaluated with ultrasonography, biophysical profile or non-stress test
depending on the gestational age of the fetus. In general, it is prudent toavoid delivery in the presence thyroid storm unless fetal indications for
delivery outweigh the risks to the woman.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
69/80
Treatment of Thyroid Storm in Pregnant Women:
1Propylthiouracil (PTU), 600-800 mg orally stat, then 150-200 mg orally every 4-6 hours. If oral
administration is not possible, use methimazole rectal suppositories.
2Starting 1-2 hours after PTU administration, saturated solution of potassium iodide (SSKI), 2-5 drops orally
every 8 hours, orSodium iodide, 0.5 to 1.0 g/IV every 8 hours, or
Lugols solution, 8 drops every g hours, or
Lithium carbonate, 300 mg orally every 6 hours.
3Dexamethasone, 2mg/IV or IM every 6 hours for 4 doses
4Propranolol, 20-80 mg orally every 4-6 hours, or propranolol, 1-2 mg IV every 5 minutes for a total of 6
mg, then 1-10 mg IV every 4 hours.
If the patient has a history of severe bronchospasm:
Reserpine, 1-5 mg IM every 4-6 hours
Guanethidine, 1mg/kg orally every 12 hours
Diltiazem, 60 mg orally every 6-8 hours5Phenobarbital, 30-60 mg orally every 6-8 hours as needed for extreme restlessness
H h ld th id d l th id h ld
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
70/80
How should a thyroid nodule or thyroid cancer should
during pregnancy be assessed?
The incidence of thyroid cancer in pregnancy is 1 per1,000. 43 Any thyroid nodule discovered during
pregnancy should be diagnostically evaluated,
because malignancy will be found in up to 40% of
these nodules. 34,44 Pregnancy itself does not
appear to alter the course of thyroid cancer. 43,45
Whether pregnancy increases the risk that a thyroid
nodule becomes cancerous is less clear. 34
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
71/80
In a cohort study comparing thyroid cancer in pregnant orpostpartum women with nonpregnant women, there were no
differences in the presenting physical findings, tumor type, rumor
size, presence of metastases, time between diagnosis and
treatment, recurrence rates of death rates. 43 Women in this study
were monitored for a median of 20 years. These data strongly
suggest that pregnancy does not affect the outcome of thyroid
cancer. In addition, except for the time between diagnosis and
surgery, there was no difference in outcome between those women
who had thyroidectomy during pregnancy and those who had theprocedure after pregnancy. Significantly more pregnant women
had no symptoms, emphasizing the importance of the physical
examination during pregnancy.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
72/80
Another study compared pregnancy outcomes among womenwith thyoid cancer who fell into 1 of 3 categories: a.) before
treatment b.) after thyroidectomy but before I-131 treatment
c.) after treatment with both thyroidectomy and I-131. 46
The study found no differences in stillbirths, LBW, ormalformations among the three groups. The incidence of
spontaneous abortion was significantly higher in women who
had any treatment for thyoid cancer but was not different
between those women who had surgery only and those who
had surgery an I-131 treatment.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
73/80
If the diagnosis of cancer is made, a multidisciplinarytreatement plan should be determined. The options are
pregnancy termination, treatment during pregnacy and
preterm or term delivery with treatment after pregnancy.
This decision will be affected by the gestational age atdaignosis and the tumor characteristics. Definitive treatment
for thyroid cancer is thyroidectomy and radiation.
Thyroidectomy can be performed during pregnancy,
preferably in the second trimester, but radiation should be
deferred until after pregnancy. Breastfeeidng should be
avoided for at least 120 days after I-131 treatment. 34
How is postpartum thyroiditis diagnosed and
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
74/80
How is postpartum thyroiditis diagnosed and
treated?
Postpartum thyroiditis occus in 5% of womenwho do not have a history of thyroid disease. 47Studies have found that approximately 44% ofwomen with postpartum thyroiditis have
hypothyroidism, while the remaining women areevenly split between thyrotoxicosis andthyrotoxicosis followed by hypothyroidism. 47,48 Inone study, goiter was present in 51% of women with
postpartum thyroiditis. 48 Postpartum thyroiditisalso may occur after pregnancy loss and has a 70%risk of recurrence. 49,50
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
75/80
The diagnosis of postpartum thyroiditis is made by documentingnew-onset abnormal levels of TSH or FT$ or both. If the diagnosis isin doubt, measuring antimicrosomal or thyroperoxidase antithyroidperoxidase antibodies may be useful to confirm the diagnosis.
The need for treatment in women with postpartum thyroiditis
is less clear. In a prospective study of 605 asymptomatic pregnantand postpartum women, only 5 or 11% diagnosed with postpatumthyroiditis developed permanent hypothyroidism. 48 Furthermore,none of the women with thyrotoxicosis required treatment. 48Those who were treated received T4 for extremely high levels of
TSH with suppressed T4 or increasing goiter size. Because of thelow incidence postpartum thyroiditis and the low likelihood ofrequireing treatment, screening with TFTs and antimicrosomalantibodies in asymptomatic women is not warranted.47,51
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
76/80
Women who develop a goiter in pregnancy or postpartum orwho developed postpartum hypothyroid or hyperthyroid
symptoms (including excessive fatigue, weight gain, dry skin,
dry hair, cold intolerance, persistent amenorrhea, difficulty
concentrating, depression, nervousness or palpitations)should have their TSH and FT4 levels evaluated. 47,48,51 As
noted previously, thyroid antimicrosomal or antithyroid
peroxidase antibodies may also be useful. If the patient has
hypothyroidism the decision to treat depends on the serverity
of abnormality and symptoms. Women with the highest
levels of TSH and antithyroid peroxidase antibodies have the
highest risk for developing permanent hypothyroidism. 48
Which pregnant patients should be screened for
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
77/80
Which pregnant patients should be screened for
thyroid dysfunction?
It is appropriate to perform indicatedtesting of thyroid function in women with a
personal history of thyroid disease or
symptoms of thyroid disease. Theperformance of TFTs in asymptomatic
pregnant nwomen who have a mildly enlarged
thyroid is not warranted. Development of asignificant goiter or distinct nodules should be
evaluated as in any patient.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
78/80
An observational study has drawn considerable attention to the suject ofmaternal subclinical hypothyroidism and resulte in calls from someprofessional organizations for universal screening for maternalhypothyroidism. 20 Investigators screened maternalserum samplesobtained in the second trimester for purposes of maternal sermalphafetoprotein screening for neural tube defectsfor elevated TSHlevels. 20 Out of 25,216 samples, only 75 had TSH levels above the 99.7thpercentile. The investigators then compared the results ofneuropsychologic testing for 62 children of hypothyroid women with thoseof 124 children of matched women with normal thyroid glands when thechildren were approximately 8 years of age. They found no significantdifference in mean IQ scores between the chidlren of hypothyroid womenand controls (p = 0.06). There was a significant difference in mean IQ
scores when the children of untreated hypothyroid women werecompared with controls but not between children of ountreated andtreated hypothyroid women, Among the children of the untreatedwomen, 19% had full scale IQ scores of 85% or lower, compared with only5% of the children of women with normal thyroid glands.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
79/80
It is important to achknowledge the lmitations of the currentunderstanding of this issue. The datea availabot areobservational. There have been no interveition trials todemonstrate the efficacy of screening and treatement toimprove neuropsychologic performance in the offspring of
hypothyroid women. The avilable data are consitetn with thepossibilit that maternal hypothyroidism is associated with adecrement in some neuropsychologic testing. However, theassociateion needs furhter testing to document its validityand, if confirmed, evidence that treatment ameliorates theeffect. For all of these reasons, it would be premature torecommend universal screening for hypothyroidism duringpregnancy.
-
8/21/2019 Thyroid Disorders in Pregnancy 2012
80/80