Thyroid Disorders - cdn.ymaws.com · 1. (RX) Describe the signs and symptoms associated with...
12
3/14/19 1 Thyroid Disorders NGOC-YEN PHAM, PHARMD UNMH PGY-1 PHARMACY RESIDENT APRIL 1, 2019 Learning objectives 1. (RX) Describe the signs and symptoms associated with thyroid disorders 2. (RX) Identify the medications available for treatment of thyroid disorders 3. (RX) Describe the mechanism of action, drug-drug and drug-food interactions, contraindications, and adverse effects of pharmacological agents used in thyroid disorders 4. (RX) Given a case, formulate a treatment plan for the different thyroid disorders including medication selection and monitoring of therapy 3 Hypothyroidism Pathway Result: TSH: _____________ TH: ______________ How does this affect the body? DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e
Transcript of Thyroid Disorders - cdn.ymaws.com · 1. (RX) Describe the signs and symptoms associated with...

3/14/19
1
Thyroid DisordersNGOC-YEN PHAM, PHARMDUNMH PGY-1 PHARMACY RESIDENTAPRIL 1, 2019
Learning objectives 1. (RX) Describe the signs and symptoms associated with thyroid disorders
2. (RX) Identify the medications available for treatment of thyroid disorders
3. (RX) Describe the mechanism of action, drug-drug and drug-food interactions,
contraindications, and adverse effects of pharmacological agents used in thyroid
disorders
4. (RX) Given a case, formulate a treatment plan for the different thyroid disorders
including medication selection and monitoring of therapy
3
Hypothyroidism Pathway Result:
TSH: _____________
TH: ______________
How does this affect the body?
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e

3/14/19
2
Alteration of thyroid labs TSH Thyroid Gland
Decrease - Glucocorticoids- Metformin- Opiates- Interleukin-6
Increase- Interleukin-2 - Amphetamine - Ritonavir - St. John’s wort
Iodine uptake - Amiodarone- Contrast - Iodine
Hormone production - Amiodarone - Sulfonylureas - Sulfonamides
Secretion - Lithium - Iodine- Amiodarone
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Thyroid Laboratory
Total T4Free T4 Total T3 TSH
Normal 4.5–10.9 mcg/dL 0.8–2.7 ng/dL 60–181 ng/dL 0.5–4.7 milli-international units/L
Hyperthyroid ↑↑ ↑↑ ↑↑↑ ↓↓
Hypothyroid ↓↓ ↓↓ ↓ ↑↑
Increased TBG ↑ Normal ↑ Normal
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e
Hypothyroidism
6
WHAT ARE YOU DOING MAGGOT! WE NEED MORE THYROID
HORMONE!
I’m s…s…sorry sir. There isn’t much out
there. This is all I could find
3/14/19
3
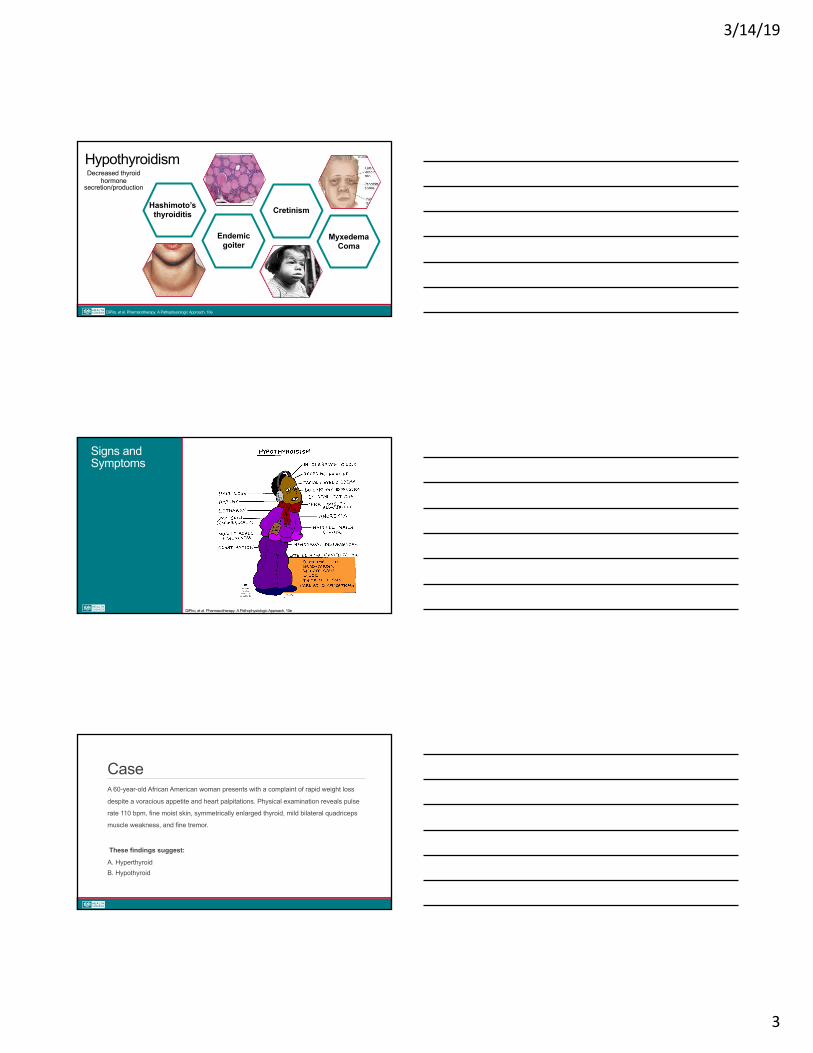
Severe long-standing
hypothyroidism
Congenital deficiency of
thyroid hormone
Hypertrophy of thyroid gland
Iodine deficiency
Autoimmune destruction of thyroid gland
HypothyroidDecreased thyroid hormone
secretion/production
Endemic goiter
Cretinism Hashimoto’s thyroiditis
Myxedema Coma
HypothyroidismDecreased thyroid
hormone secretion/production
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e
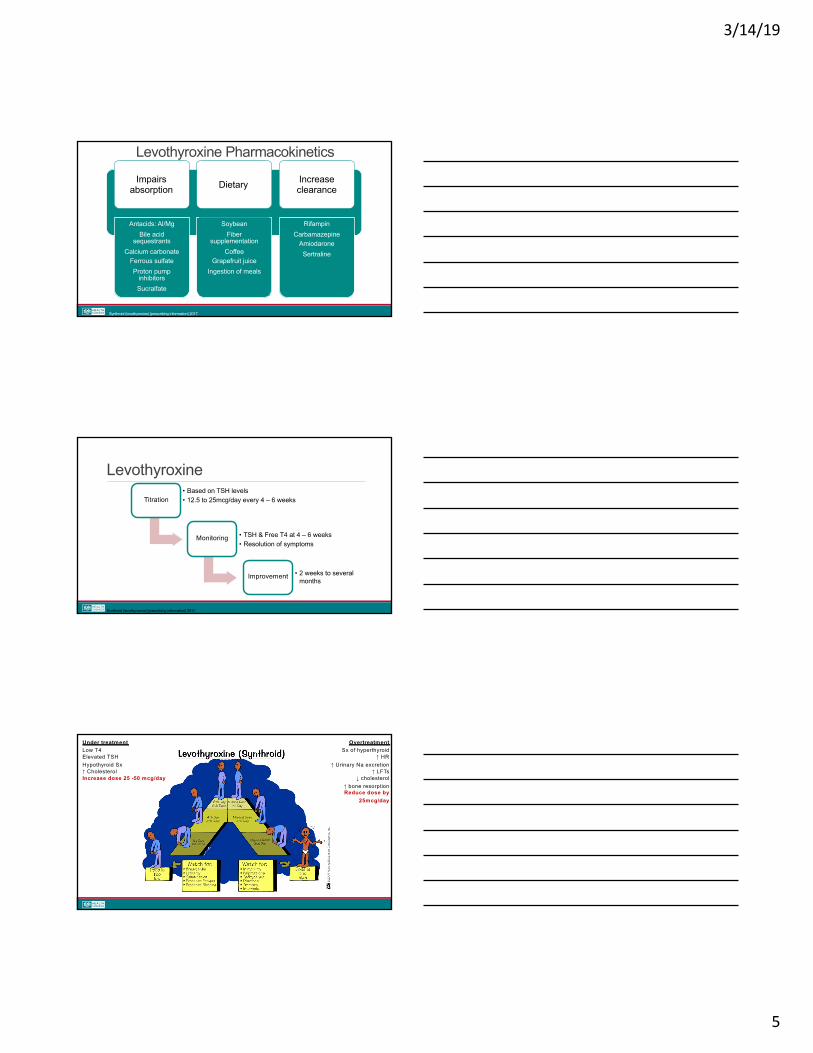
Signs and Symptoms
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e
CaseA 60-year-old African American woman presents with a complaint of rapid weight loss
despite a voracious appetite and heart palpitations. Physical examination reveals pulse
rate 110 bpm, fine moist skin, symmetrically enlarged thyroid, mild bilateral quadriceps
muscle weakness, and fine tremor.
These findings suggest:
A. HyperthyroidB. Hypothyroid

3/14/19
4
What laboratory abnormalitieswould be expected?A. High free T4 and high TSH
B. High free T4 and low TSH
C. Low free T4 and high TSH
D. Low free T4 and low TSH
Treatment Guidelines§Goals of therapy§ Eliminate symptoms
§ Normalize TSH & T4 levels
§ Shrink goiter (Hashimoto’s)
§Thyroid replacement therapy§ Natural hormones
§ Synthetic
§Available agents § Levothyroxine (T4)
§ Liothyronine (T3)
§ Desiccated thyroid (ArmourThyroid)
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Levothyroxine
Synthroid (levothyroxine) [prescribing information] 2017.
Patient Dose
Healthy adults 1.6mcg/kg/day
Adults >50 years w/o evidence of coronary heart disease
50mcg/day
Adults with cardiac disease 12.5 to 25 mcg/day
Pregnant patients 1.6 mcg/kg/day (severe) 1 mcg/kg/day (mild)
3/14/19
5
Antacids: Al/Mg Bile acid
sequestrantsCalcium carbonate
Ferrous sulfateProton pump
inhibitorsSucralfate
SoybeanFiber
supplementation Coffee
Grapefruit juice Ingestion of meals
RifampinCarbamazepine
AmiodaroneSertraline
Levothyroxine Pharmacokinetics
Synthroid (levothyroxine) [prescribing information] 2017.
Impairs absorption Dietary Increase
clearance
Levothyroxine
Synthroid (levothyroxine) [prescribing information] 2017.
Titration
• Based on TSH levels
• 12.5 to 25mcg/day every 4 – 6 weeks
Monitoring • TSH & Free T4 at 4 – 6 weeks
• Resolution of symptoms
Improvement • 2 weeks to several months
Under treatmentLow T4Elevated TSHHypothyroid Sx↑ CholesterolIncrease dose 25 -50 mcg/day
OvertreatmentSx of hyperthyroid
↑ HR↑ Urinary Na excretion
↑ LFTs↓ cholesterol
↑ bone resorptionReduce dose by
25mcg/day
3/14/19
6
Check-in QuestionWhat dose of Levothyroxine would you recommend for a 75 yo (50kg) women with no history of heart disease?
A. 88 mcg po daily
B. 25 mcg po daily C. 75 mcg po daily D. 12.5 mcg po daily
Case A 25-year-old African American woman presents with a complaint of rapid weight loss despite a voracious appetite and heart palpitations. Physical examination reveals pulse rate 110 bpm, fine moist skin, symmetrically enlarged thyroid, mild bilateral quadriceps muscle weakness, and fine tremor.
What pharmacological options should be used to manage this patient?
Myxedema Coma Hypothermia
Delirium/ComaAdvanced
hypothyroid symptoms
IV levothyroxine
IV hydrocortisone
Supportive therapy

3/14/19
7
HypothyroidDecreased thyroid hormone
secretion/production
Hyperthyroidism (thyrotoxicosis)
Increased thyroid hormone
secretion/production
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e
Thyroid Adenoma
Thyroid Storm
Grave’s Disease
Drug induced Hyperthyroidism
Amiodarone
Iodine induced
Inflammatory thyroiditis
ThionamidesRadioactive iodine
Prednisone 40mg daily for 6 to 12
weeks
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Signs and Symptoms

3/14/19
8
Signs and Symptoms
Onycholysis Exopthalmos
Pretibial myxedema Thyroid acropachy
Case A 23-year-old woman presents with palpitations. Over the past 6 months, she has reported loose stools, a 10-lb (4.5-kg) weight loss despite a good appetite and food intake, and increased irritability. She appears to be anxious.Thyroid gland is diffusely and symmetrically enlarged to twice the normal size, and it is firm and nontender; She has an eyelid lag, but no periorbital edema.
HR = 119 bpm, BP = 137/80 mmHg TSH = 0.02 microU/ml (0.5-5.0 microU/L)FT4 = 4.10 ng/dl (0.89 to 1.76ng/dl).
Treatment Goals
Relief of symptoms
Reduction of thyroid hormone
Reversing the cause of
thyrotoxicosis
Surgery
Radiation
Medications
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.

3/14/19
9
Pharmacological Agents
THIOUREAS (THIONAMIDES)
ADRENERGIC BLOCKERS
RADIOACTIVE IODINE
IODINE
DiPiro, et al. Pharmacotherapy: A Pathophysiologic Approach, 10e Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Thionamides : Methimazole (MMI)
Mechanism of action
• Inhibits thyroid peroxidase
Indications
• Thyroid storm • Preferred in
pregnancy
Dosing
• 10 – 40mg once daily
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Thionamides : Prophylthiouracil (PTU)
Mechanism of action
• Inhibits thyroid peroxidase and peripheral conversion of T4 to T3
Preference
• First trimester of pregnancy
• Thyroid storm
• Intolerance to methimazole
Dosing
• 150-600mg/day TID-QID
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.

3/14/19
10
Thionamides
Adverse effects
Common:
• Rash/urticaria
• Fever
• Arthralgia
Rare:
• Hepatitis
• SLE-like syndrome
• Agranulocytosis
• Cholestatic jaundice
Monitoring
• TSH, T3, T4, LFTS
• WBC + differential
• Repeat Q4-6 weeks after start
or change in doses
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Iodine Mechanism of
Action
• Blocks thyroid hormone release
Uses
• Grave’s disease • Severely
thyrotoxic• Post-radioactive
iodine therapy
Adverse effects
• Hypersensitivity reaction
• Salivary gland swelling
• “Iodism”
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Radioactive iodine (I131)
Indications
• Prior thyroid surgery
• Poor surgical risk
• Failed thionamide therapy
Details
• Contraindicated in pregnancy/breastfeeding
• Slow onset
• Preferred treatment for Graves’
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
3/14/19
11
Radioactive iodine (I131)
Considerations
• Pre-treatment with methimazole in older patients
• Acute hyperthyroid post-treatment • First line treatment in younger patients
Adverse Effects
• Carcinogenic • Leukemia • Genetic damage• Hypothyroidism
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
Beta-Blockers •Provide relief of increased sympathetic tone
• Palpitations, tachycardia, anxiety
•Beta-blockers can also reduce peripheral conversion of T4 à T3
•Propranolol IR may be preferred due to short half-life• Patient can self-titrate dose to ameliorate symptoms
•IV esmolol is used for symptomatic treatment of thyroid storm• Rapid onset, short half-life
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.
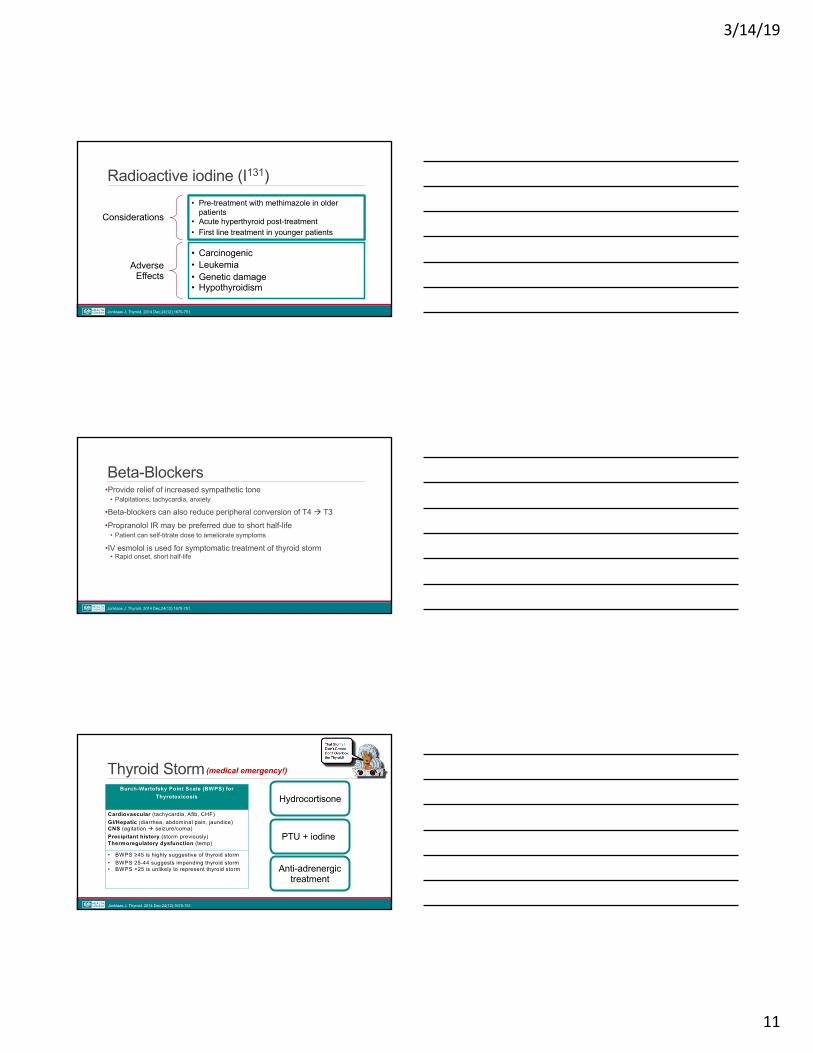
Thyroid Storm (medical emergency!)
Burch-Wartofsky Point Scale (BWPS) for Thyrotoxicosis
Cardiovascular (tachycardia, Afib, CHF) GI/Hepatic (diarrhea, abdominal pain, jaundice) CNS (agitation à seizure/coma) Precipitant history (storm previously) Thermoregulatory dysfunction (temp)
• BWPS ≥45 is highly suggestive of thyroid storm• BWPS 25-44 suggests impending thyroid storm• BWPS <25 is unlikely to represent thyroid storm
Hydrocortisone
PTU + iodine
Anti-adrenergic treatment
Jonklaas J. Thyroid. 2014 Dec;24(12):1670-751.

3/14/19
12
CaseMN, a 41-year-old male presented to the ED with confusion, rightsided numbness and tingling, slurred speech, dizziness, and facial edema. BP = 90/60 mm Hg, HR = 50 beats/min T = 95.7 degrees F Abnormal Labs: CK = 439 IU/L SCr = 1.6 mg/dLTSH = 126.4 microIU/mL ↑↑↑↑FT4 = 0.29 ng/dL ↓↓↓↓
Which of the following should be administered to MN immediately?A. Aspirin 325mg B. metoprolol + methimazoleC. 500mcg IV levothyroxine + hydrocortisone 100mg IV
CaseWhat is your medication recommendation for pharmacological treatment of AA’s hyperthyroidism?
A. Propranolol and MethimazoleB. Atenolol and Iodine
C. PTU and Atenolol
A 23-year-old woman presents with palpitations. Over the past 6 months, she has reported loose stools, a 10-lb (4.5-kg) weight loss despite a good appetite and food intake, and increased irritability. She appears to be anxious.Thyroid gland is diffusely and symmetrically enlarged to twice the normal size, and it is firm and nontender; She has an eyelid lag, but no periorbital edema.
HR = 119 bpm, BP = 137/80 mmHg TSH = 0.02 microU/ml ↓↓FT4 = 4.10 ng/dl ↑↑
Key Points 1) Thyroid hormone is essential in regulating cardiac function, bone growth, and
maintaining metabolism
2) The goal of treatment is to normalize TSH and eliminate symptoms
3) Levothyroxine is the mainstay of treatment in hypothyroidism
4) Thyroid storm is a medical emergency that requires prompt treatment