Unit 3 Autoimmunity Part 4 Hashimoto’s Thyroiditis Part 5 Grave’s Disease

THYROID DISEASE
IN PREGNANCY
Grand Rounds
December 5, 2018
Maria Kolojeski, DO (PGY3)https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html

REVIEW OF THYROID HORMONES
Hypothalmus
Thyroid Releasing Hormone (TRH)
Anterior Pituitary
Thyroid-Stimulating Hormone (TSH)
Thyroid
Triiodothyronine (T3)
Thyroxine (T4)
Iodine

THYROID CHANGES IN PREGNANCY
Thyroid Volume: 30% larger in 3rd vs 1st trimester
Increased thyroid binding globulin
Increased in total T3 & T4 levels
Free T3 & T4 typically remain stable
Weak stimulation of TSH receptors by hCG (first 12 weeks)
Increases serum free T4
Thyrotropin (AKA: Thyroid Stimulating Hormone [TSH])
Decreases in early pregnancy
Transient subclinical hyperthyroidism, Gestational transient hyperthyroidism
Returns to baseline in second trimester
Increased in third trimester due to placental deiodinase

THYROID
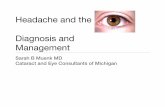
LABORATORY WORKUP
➢ First Trimester
➢ 0.1 - 2.5 mIU/L
➢ Second Trimester
➢ 0.2 - 3.0 mIU/L
➢ Third Trimester
➢ 0.3 - 3.0 mIU/L
➢ If TSH abnormal order free T4
➢ Rarely T3 toxicosis is the cause
➢ Consider antibody testing if
euthyroid but clinical signs presentWilliams Obstetrics 24ed. Ch. 58 – Fig.1.
❖ Universal screening not recommended

THYROID HORMONES & THE FETUS
Maternal T4 crosses the placenta
Fetal brain development
Provides thyroid hormone
before 12 weeks
Fetal thyroid begins to produce own
thyroid hormone & concentrate
iodine
30% of T4 at term is estimated
to be of maternal production

IODINE REQUREMENTS
Iodine deficiency in Pregnancy
Causes
Increased thyroid hormone production
Increased renal iodine loss
Fetal iodine requirement
Mild mental impairment to cretinism
Iodine Intake in Pregnancy
Reproductive age: 150mcg daily
Pregnant: 220mcg daily
Lactating: 290mcg daily
About 50% of PNV don’t contain iodine
Not to excess 500mcg daily
http://www.faqs.org/nutrition/images/nwaz_01_img0114.jpg

HYPERTHYROIDISM
Prevalence: 0.2 - 0.4% pregnancies (US); studies in UK (0.7 - 1.7%), China (1%)
Causes: Graves disease (95%), trophoblastic disease, toxic multinodular goiter, toxic adenoma, thyroiditis, exogenous thyroid hormone
Diagnosis: low TSH and high free T4
Symptoms: fatigue, nervousness, frequent stools, sweating, tachycardia, tremors, weight loss, heat intolerance, insomnia, palpitations, HTN, insomnia, +/- goiter
Additional symptoms associated with Grave’s Disease: ophthalmopathy, dermopathy
Complications: SAB, preeclampsia, heart failure, preterm birth, low birth weight, fetal thyroid disease, infection, anemia, hearing loss
SUBCLINICAL HYPERTHYROIDISM
Prevalence in pregnancy: 1.7%
No associations with adverse pregnancy outcomes
Antithyroid medications have can have adverse effects on the fetus

THYROID STIMULATING ANTIBODIES
Risk of immune-mediated fetal hypothyroidism and hyperthyroidism
Thyroid stimulating immunoglobulins (TSI) stimulate fetal thyroid
1-5% of neonates have hyperthyroidism or neonatal Grave’s disease
TSH-binding inhibitory immunoglobulins inhibit fetal thyroid
Decreased occurrence with maternal treatment during pregnancy
However – increased risk if previous maternal treatment via surgery or radioiodine ablation
Consider fetal thyrotoxicosis in all women with a history of Grave’s
American Thyroid Association and American Associate of Clinical Endocrinologists recommend antibody testing between 22-26wga in women with a history of Grave’s disease.
ACOG does not, due to no change in management.

HYPERTHYROIDISM MANAGEMENT
Thioamides – decrease production of T3 & T4; cross the placenta
Proplthiouracil (PTU) – first trimester
Inhibits iodination of tyrosine and conversion of T4 to T3 in peripheral tissues
Hepatotoxicity (0.1-0.2%), ANCA (20%; rare for serious vasculitis)
Methimazole (MMI) – second & third trimesters
Inhibits iodination of tyrosine
Associated with esophageal and choanal atresia, fascial dysmorphism, aplasia cutis, omphalocele
Side effects: transient leukopenia (10%), agranulocytosis (0.3 - 0.4%)
Dosage: PTU 50-150mg PO TID; MMI 10-40mg PO divided into BID or TID dosing
Surveillance: measure T4 level q2-4 weeks
Beta blockers
Used for management of tachycardia and tremors
Avoid longer than 2-6 weeks due to increased risk of IUGR, bradycardia & hypoglycemia
Dosing
Metoprolol 25-50mg daily
Propranolol 20mg q6-8hr

HYPERTHYROIDISM MANAGEMENT
Thyroidectomy – rarely performed during pregnancy
Reserved for individuals with allergy to thioamides or agranulocytosis
Pretreatment with a beta-blocker and potassium iodine
Fetal Monitoring
Fetal heart rate monitoring, growth ultrasounds;
Consider fetal thyroid ultrasound if mother with Grave’s or TRAb 2-3x normal
Postpartum
Methimazole preferred due to PTU side effects
If dose >20mg daily, then infants should have thyroid function testing at 1 and 3 months of age
TSH and free T4 at 6 weeks
Not recommended
Routine thyroid antibody testing
Some recommend if require treatment with thioamides to test initially, at 18-22 and 30-34 wga
Routine fetal thyroid evaluation: fetal US, cord blood sampling
Consider in cases of IUGR, fetal tachycardia, fetal hydrops, goiter

HYPERTHYROID EMERGENCIES
Thyroid StormThyrotoxic Heart Failure & Pulmonary Hypertension
Incidence: 1-2% of pregnant patients with hyperthyroidism
High risk of maternal heart failure
Abrupt onset
Diagnosis: fever, tachycardia, cardiac dysrhythmia, CNS dysfunction
If suspect, order TSH & free T4, CBC, LFTs, Ca2+
Treat underlying cause
Avoid delivery
Incidence: 8% pregnant patients with uncontrolled hyperthyroidism
Excess T4 -> high-output cardiomyopathy that can develop into dilated cardiomyopathy
Precipitating conditions: preeclampsia, anemia, sepsis
Frequently these conditions are reversible

Inhibit release of T3 & T4
• PTU 1,000mg PO load, then 200mg PO q6hr
• Iodine (1-2hr after PTU)
• Sodium iodine 500-1,000mg IV q8hr OR
• Potassium iodide, 5 drops PO q8hr OR
• Lugol solution, 10 drops PO q8hr OR
• Lithium carbonate, 300mg PO q6hr (iodine allergy)
Block peripheral T4 -> T3
• Dexamethasone, 2mg IV q6hr x 4 OR
• Hydrocortisone, 100mg IV q8hr x 3
Consider beta-blocker
for tachycardia
• Caution in those with heart failure
• Propranolol, 10-40mg PO q4-6hr; (labetalol, esmolol)
MANAGEMENT of THYROID STORM or
THYROTOXIC HEART FAILURE in PREGNANCY
Don’t forget supportive care!
O2, IVF, telemetry, NG tube, cooling measure, avoid salicylates

HYPOTHYROIDISM
Complicates 2 – 10 per1,000 pregnancies
Causes: Iodine deficiency, chronic autoimmune thyroiditis (Hashimoto’s),
prior radioiodine ablation/surgery, pituitary/hypothalamic disorders
Diagnosis: high TSH and low free T4
Consider measurement of TPO antibodies if TSH≥2.5
Symptoms: fatigue, constipation, cold intolerance, muscle cramps, dry skin,
hair loss, prolonged relaxation of DTRs, weight gain, edema, +/- goiter
Paresthesias: early symptom present in 75% of hypothyroid patients
Other: large tongue, myxedema, hoarse voice
Complications: SAB, preeclampsia, preterm birth, low birth weigh, impaired
neuropsychologic development, placental abruption, fetal death

HYPOTHYROIDISM
SUBCLINICAL HYPOTHYROIDISM
Prevalence in pregnancy: 2-5%
Approximately 1/3 have TPO antibodies
Possible increased risk of NICU admission, RDS, abruption, preterm birth, GDM
No evidence that treatment improves outcomes
ISOLATED MATERNAL HYPOTHYROXINEMIA
Prevalence in pregnancy: 1.3%
No increased rates of TPO antibodies
Inconsistent data on adverse pregnancy outcomes (neurodevelopment, macrosomia)
No evidence that treatment improves outcomes

ANTITHYROID ANTIBODIES
Hashimoto’s thyroiditis
glandular destruction via thyroid peroxidase (TPO) Ab & antithyroglobulin Ab (TG)
Euthyroid Autoimmune Thyroid Disease
TPO & TG antibodies are present in 6-20% of reproductive-aged women
Women with these antibodies are at an increased risk for
Early pregnancy loss (2-5 fold)
Placental abruption (3 fold)
Postpartum thyroid complications
Permanent thyroid failure
1 in 180,000 neonates will experience fetal hypothyroidism as a result of maternal TPO antibodies attacking the fetal thyroid

HYPOTHYROIDISM MANAGEMENT
T4 replacement recommended
Levothyroxine 1-2mcg/kg daily
Surveillance: measure TSH levels q4-6 weeks
If preexisting hypothyroidism, need for T4 increase in 1/3 of patients
Increased T4 needs can occur as early as week 5 of gestation
Anticipatory increase in dose by 25% at pregnancy confirmation (in those with no reserve)
Adjust dosages in 25-50mcg increments
Postpartum
Return to prepregnancy dose if preexisting condition
Measure TSH at 4-6 weeks after delivery
Safe to use in breastfeeding; can improve milk production
Not recommended
Routine thyroid antibody testing

MYXEDEMA COMA
Extreme/severe hypothyroidism
Mortality rate: 20%
Rare in pregnancy
Diagnosis: “think low”
Hypoventilation, hypothermia, hypotension, hyponatremia, and bradycardia
Treatment
Levothyroxine (IV/NG) 300-500mcg bolus IV, 75-100mcg IV daily
NG doses 30-50% higher than IV; PO 50-200mcg daily once stable
Liothyronine (T3 replacement) 10mcg q8hr
Hydroxycortison 100mg q8hr until cortisol level known, then titrate
Supportive: IVF, electrolyte replacement, telemetry, intubation, warming
Cardiac enzymes and cultures to further evaluate

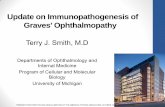
FETAL & NEONATAL EFFECTS Goitrous Thyrotoxicosis
Transfer of TSI across the placenta; increased risk if 3x normal limit
Nonimmune hydrops, heart failure, accelerated bone maturation, tachycardia, IUGR
Treatment: increase thioamide (regardless of maternal levels)
May need antithyroid drug during neonatal period
Fetal Thyrotoxicosis
Placental transfer of TSI s/p ablation or thyroidectomy
Goitrous Hypothyroidism
Due to maternal intake of thioamides
Delayed bone maturation, hydramnios, hyperextension
Treatment: decrease maternal thioamide dosage
Possible intramniotic thyroxine injection
Nongoitrous Hypothyroidism
Transfer of TSH receptor blocking antibodies
Williams Obstetrics 24ed. Ch. 58 – Fig.3.

FETAL & NEONATAL MANAGEMENT
Method of diagnosis: amniotic fluid or fetal cord blood sampling
Goiter complications
Compression of trachea and/or esophagus hydramnios and/or airway compromise
Fetal neck hyperextension labor dystocia
Fetal Thyrotoxicosis
Maternal thioamides; treat mother with levothyroxine supplementation if needed
Fetal Hypothyroidism
Discontinuation of maternal thioamide (if applicable and able)
Intraamniotic levothyroxine injections
50 - 800mg q1-4 weeks (no established protocol)

CONGENITAL HYPOTHYROIDISM
Prevalence: 1 in 2000 - 4000 births; female:male = 2:1
Causes
Iodine deficiency – most common
Developmental disorders – agenesis and hypoplasia
Hereditary defects in thyroid hormone production (dyshormonogenesis)
Failure of stimulation from pituitary
Complications: mental deficiencies/cognitive defects, limb length
Most treatable cause of mental deficiency
One study found that 8% of 1420 infants had other major congenital malformations
Universal newborn screening: TSH & free T4; required in US
Management: Thyroxine replacement (early & aggressive)

THYROID NODULES
Present in 1-2% of reproductive aged women
15% of Chinese women at nodules >2mm – 50% multiple; mostly nodular hyperplasia
Some studies have shown 40% malignancy rate of solitary nodules
Workup
TSH
Neck ultrasound (adequate for detecting nodules >0.5cm)
Malignant characteristics: irregular margins, microcalcifications, hypoechogenic pattern
FNA
Surgery: second trimester is optimal timing
Reserved for fast going masses, compression symptoms (recurrent laryngeal nerve)
Radioiodine scanning – contraindicated in pregnancy
Recommend waiting 6 months after ablation
Recommend waiting 3 months after delivery to undergo ablation due to storage of iodide in the breast tissue

THYROID CANCER
Requires multidisciplinary approach
Typically well differentiated and slow growing
Monitor with ultrasound every trimester
If discovered in 1st - 2nd trimesters, possible thyroidectomy in 3rd
trimester – otherwise delay surgery until after delivery.
Injury or inadvertent removal of parathyroid glands
Injury to recurrent laryngeal nerve
Persistent disease s/p radioiodine treatment
Pregnancy has does not lead to recurrence, however progression can occur
Follow with US and thyroglobulin levels
Continue levothyroxine

POSTPARTUM THYROIDITIS
➢ Thyroid dysfunction within 12 months of delivery
➢ Transient autoimmune thyroiditis account for 5-10% of cases
➢ Approximately 50% of women with TPO antibodies in first trimester developed
postpartum thyroiditis
➢ Most cases will resolve spontaneously➢ One third develop overt hypothyroidism
Thyrotoxicosis
Release of excess thyroid hormone
Abrupt onset
Small, painless goiter
Lasts a few months
Fatigue, irritability, weight loss,
palpitations, heat intolerance
Thioamides ineffective
Consider beta-blocker if severe
Hypothyroidism
Thyromegaly more common
Typically 4-8 months postpartum
Fatigue, cold intolerance, weight
gain, constipation, depression
T4 replacement for 6-12 months

REFERENCES1. American College of Obstetrics and Gynecology. “Practice Bulletin No. 148: Thyroid Disease in Pregnancy.” Obstetrics and
Gynecology. 2015;125:996-1005.
2. Cunningham, F. Gary,, et al. Williams Obstetrics. 24th edition. New York: McGraw-Hill Education, 2014.
3. Foley, F. Michael,, et al. Obstetric Intensive Care Manual. 5th edition. New York: McGraw-Hill Education, 2018.
4. Lafranchi, Stephen and Maynika Rastogi. “Familial Thyroid Dyshormonogenesis.” Orphanet Encyclopedia, August, 2010,https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=95716. Accessed 2 December 2018.
5. National Library of Medicine (US). Genetics Reference [Internet]. Bethesda, MD: The Library; 27 November 2018. Congenital Hypothyroidism; [reviewed 2015 September]. Available from: https://ghr.nlm.nih.gov/condition/congenital-hypothyroidism#inheritance. Accessed 2 December 2018.
6. Newborn screening for congenital hypothyroidism. Journal of Clinical Research in Pediatrtic Endocrinology vol. 5 Suppl 1,Suppl 1 (2013):8-12.
7. Ross, S. Douglas. (2018). Hyperthyroidism during pregnancy: treatment. In J. E. Mulder (Ed.), UpToDate. https://www-uptodate-com.proxy.kumc.edu/contents/hyperthyroidism-during-pregnancy-treatment?search=hyperthyroidism%20in%20pregnancy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H17 . Accessed 4 December 2018.
8. Ross, S. Douglas. (2018). Hypothyroidism during pregnancy: clinical manifestation, diagnosis, and treatment. In J. E. Mulder (Ed.), UpToDate. https://www-uptodate-com.proxy.kumc.edu/contents/hypothyroidism-during-pregnancy-clinical-manifestations-diagnosis-and-treatment?search=hypothyroid%20in%20pregnancy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed 4 December. 2018.
9. Ross, S. Douglas. (2018). Overview of Thyroid Disease in Pregnancy. In J. E. Mulder (Ed.), UpToDate. https://www-uptodate-com.proxy.kumc.edu/contents/overview-of-thyroid-disease-in-pregnancy?search=thyroid%20diseases%20and%20pregnancy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed 11 November 2018.

QUESTIONS?
THYROID DISEASE IN PREGNANCY