thy of Pre Maturity

of 18
Transcript of thy of Pre Maturity
-
8/3/2019 thy of Pre Maturity
1/18
Retinopathy of Prematurity
Mr Farrukh Ali
Department of Ophthalmology
Arrowe Park Hospital, Wirral UK
-
8/3/2019 thy of Pre Maturity
2/18
Introduction
Retinopathy of prematurity (ROP) is an abnormal growth of blood vesselsin the retina at the back of a premature babys eye. It primarily affectspremature infants weighing about 1500 grams or less and are born before
32 weeks of gestation (A full-term pregnancy has a gestation of 3842weeks).
Today, with advances in neonatal care, smaller and more premature
infants are being saved. These infants are at a much higher risk for ROP.Not all babies who are premature develop ROP. The disease improves
and leaves no permanent damage in milder cases of ROP. About 90percent of all infants with ROP are in the milder category and do not needtreatment. However, infants with more severe disease can developimpaired vision or even blindness.
ROP was first diagnosed in 1942.
-
8/3/2019 thy of Pre Maturity
3/18
Cause of ROP
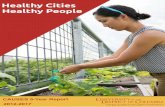
ROP occurs when abnormal blood vessels grow and spreadthroughout the retina, the tissue that lines the back of the eye.
These abnormal blood vessels are fragile and can leak, scarringthe retina and pulling it out of position. This causes retinaldetachment. Retinal detachment is the main cause of visual
impairment and blindness in ROP
Division of retina in zones to classify ROP
-
8/3/2019 thy of Pre Maturity
4/18
Several complex factors may be responsible for the development of ROP.
The eye starts to develop at about 16 weeks of pregnancy, when the
blood vessels of the retina begin to form at the optic nerve in the back ofthe eye. The blood vessels grow gradually toward the edges of thedeveloping retina, supplying oxygen and nutrients. During the last 12
weeks of a pregnancy, the eye develops rapidly. When a baby is born full-term, the retinal blood vessel growth is mostly complete (The retina
usually finishes growing a few weeks to a month after birth). But if a babyis born prematurely, before these blood vessels have reached the edges
of the retina, normal vessel growth may stop. The edges of the retinatheperipherymay not get enough oxygen and nutrients
-
8/3/2019 thy of Pre Maturity
5/18
Risk factors for ROPIn addition to birth weight and how early a baby is born, other factors
contributing to the risk of ROP include anaemia, blood transfusions,respiratory distress, heart anomalies, breathing difficulties, and theoverall health of the infant.
Scientists believe that the periphery of the retina then sends out signalsto other areas of the retina for nourishment. As a result, new abnormal
vessels begin to grow. These new blood vessels are fragile and weakand can bleed, leading to retinal scarring. When these scars shrink,they pull on the retina, causing it to detach from the back of the eye.
-
8/3/2019 thy of Pre Maturity
6/18
Stages of ROP
ROP is classified in five stages, ranging from mild (stage I) tosevere (stage V):
Stage I The outer aspect of the retina is affected by thediminished blood supply and is shown by a cleardemarcation line. About 80% of babies born more than 10
weeks early will suffer some degree of Stage 1 retinopathy.This usually resolves spontaneously without any significant
effect on vision.
Demarcation line as shown above
-
8/3/2019 thy of Pre Maturity
7/18
Stage II
In stage 2 demarcation line becomes thickened and ridged.
Ridge
-
8/3/2019 thy of Pre Maturity
8/18
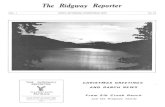
Stage III
In stage 3 abnormal blood vessels develop on the ridge. Theseabnormal vessels can loose there elasticity and begin to contract leading
to retinal detachment. Some infants who develop stage III improve withno treatment and eventually develop normal vision. However, when
infants have a certain degree of Stage III and "plus disease, treatment isconsidered. "Plus disease" means that the blood vessels of the retinahave become enlarged and twisted, indicating a worsening of thedisease. Treatment at this point has a good chance of preventing retinal
detachment.
Plus
Disease
Ridge with abnormal vessels
-
8/3/2019 thy of Pre Maturity
9/18
Stage IV
Partially detached retina. Traction from the scar produced by bleeding,
abnormal vessels pulls the retina away from the wall of the eye
Stage V
Completely detached retina and the end stage of the disease. If the eyeis left alone at this stage, the baby can have severe visual impairment
and even blindness.
-
8/3/2019 thy of Pre Maturity
10/18
What are the symptoms of retinopathy of prematurity
There are no symptoms of retinopathy, therefore all small babiesborn less than 32 weeks gestation are screened by specialist doctor
( Ophthalmologist ). Usually the screening begins when the baby iseither six weeks old or is 33 weeks gestation and usually takes place
fortnightly until the blood vessels in babys retina are mature.
Why is screening so important?
Screening is important for two reasons.
1. The seriousness of the condition is not apparent unless the retina isexamined. The baby can still see up to and including stage 3 disease.It is only when stage 4 or 5 has occurred and when there is retinaldetachment, that the baby stops being able to see.
2. Treatment is only successful at stage 3 disease.
Therefore, it is very important for the baby to attend regular check ups
by the ophthalmologist. ROP is a very progressive disease and evenone week can make a difference.
-
8/3/2019 thy of Pre Maturity
11/18
What happens during the screening checks?
Drops will be put into babys eyes to enlarge ( dilate ) pupils, this is
necessary for the doctor to see babys retina. Once pupils are dilated,anaesthetic drops will be put into the eyes so that baby does not feel any
pain during examination. The doctor will hold babys eyelids open, either byhand or with a small instrument, and look closely at the back of the eye witha special light. The doctor may need to gently press around babys eyes witha special probe, in order to get a better look. The examination only takes a
few minutes. The baby will not like the examination but should only feel slightpressure, but no pain.
Your babys nurse will keep you fully informed about the state of babys
retina and let you know if treatment is needed and the course of thetreatment will be discussed with you by the ophthalmologist.
-
8/3/2019 thy of Pre Maturity
12/18
How is retinopathy of prematurity treated?
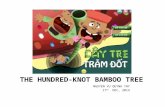
Stage 1 & 2:
Most babies who develop ROP stages I or II regresses without major
complications, as shown in the picture.
-
8/3/2019 thy of Pre Maturity
13/18
Stage 3:
If the baby has stage 3 retinopathy and fulfils the criteria fortreatment ( 5 contiguous or 8 non contiguous clock hours of stage 3
with plus disease in zone I or II. ), laser treatment will be given. Laseris a special piece of equipment that emits a very bright and fine beamof light. This laser light destroys non vascularised retina leading to
resolution of abnormal blood vessels causing haemorrhage, scarringfollowed by retinal detachment. Laser treatment involves baby havinga general anaesthetic and usually takes 2-3 hours. Normally only onelaser treatment session is necessary, but the doctors will continue to
check babys eyes on a regular basis. Laser treatment can causebabys eyes to become a little red and inflamed but this settle down
in a few days.
-
8/3/2019 thy of Pre Maturity
14/18
In the later stages of ROP ( stage 4 & 5 ), other treatment options include:
Scleral buckle. This involves placing a silicone band around the eye andtightening it. This keeps the vitreous gel from pulling on the scar tissue and allows
the retina to flatten back down onto the wall of the eye. Infants who have had asclera buckle need to have the band removed months or years later, since the eye
continues to grow; otherwise they will become nearsighted. Scleral buckles areusually performed on infants with stage IV or V.
Vitrectomy. Vitrectomy involves removing the vitreous and replacing it with a
saline solution. After the vitreous has been removed, the scar tissue on the retina
can be peeled back or cut away, allowing the retina to relax and lay back downagainst the eye wall. Vitrectomy is performed only at stage V.
The results of retinal surgery have been very disappointing. Regrettably,few, if any regain any useful sight.
Is this the end?No. There is much that can be done to help both you and your baby come to
terms with poor vision or blindness. There are all sorts of special services andteachers available to help blind children. Your doctor would be happy to discuss
this with you.
-
8/3/2019 thy of Pre Maturity
15/18
What is the long term outlook for babies with retinopathy?
Currently 80% of babies with stage 3 retinopathy do well and have good vision,
but will be regularly checked. Even with treatment, a small number of babieswith stage 3 retinopathy will have significant visual loss.
Most babies have an increased risk of developing eye problems as they grow
older. These problems may include:
Amblyopia ( Lazy eye ):
This can occur if the vision in one eye is better than in the other. The brain
learns to ignore the vision it receives from the weak eye, causing varyingdegrees of visual loss in that eye. Occlusion therapy ( Patching ) will be started
this involves your child wearing a patch over the strong eye to improvevision in the weak one.
Strabismus ( Squint ):
A squint ( eye turn ) may develop as a result of a lazy eye. Treatment of squintwill depend upon its severity and surgery may be required.
-
8/3/2019 thy of Pre Maturity
16/18
Myopia ( Short sightedness )
This is when the rays of light passing through the cornea are unable to focus
onto the retina, causing distant object to become blurry. This is usually
corrected by wearing appropriate glasses.
Glaucoma ( raised pressure within the eye )
Fluid in the eye is unable to drain away causing a build up of pressure. Thisincreased pressure can eventually cause some degree of visual loss. Often it
can be controlled with medicine and eye drops but, in some infants, mayrequire surgery.
All of these conditions, if they arise, will be discussed in much greater detailby babys eye doctor.
-
8/3/2019 thy of Pre Maturity
17/18
RISK OF EYE PROBLEMS IN PREMATURE VS TERM INFANTS
Myopia 6% vs. 2%
Amblyopia 4% vs. 0.1%
Strabismus 10% vs. 2%
Anisometropia (markedly different amount of nearsightedness orfarsightedness in the right and left eyes) 6% vs. 1.5%
Nystagmus (rapid "shaking" of the eyes) 2.5% vs. 0.1%
-
8/3/2019 thy of Pre Maturity
18/18
If you would like to know further and discuss your babys eyecondition, please contact me or the consultant on following
phone numbers:
Mrs P Pennefather: 0151 6785111 ext 2705
Mr F Ali: 0151 6785111 ext 2705
You may like to visit Royal College of Ophthalmologist website
( www. rcophth.ac.uk ) or other related websites for detailedinformation.