THROMBOPLASTIN NEWLY RECOGNIZED COMPONENT OF … · by diluting the plasmatic reagent 1: 50 with...
13
THROMBOPLASTIN GENERATION ACCELERATOR, A NEWLY RECOGNIZED COMPONENT OF THE BLOOD COAGULA- TION MECHANISM PRESENT IN EXCESS IN CERTAIN THROMBOTIC STATES * By CHRIS A. PASCUZZI, JOHN A. SPITTEL, JR., JOHN H. THOMPSON, JR. AND CHARLES A. OWEN, JR. WITH THE TECHNICAL ASSISTANCE OF CHARLENE MATTHEES (From the Sections of Medicine and Clinical Pathology, Mayo Clinic and Mayo Foundation, Rochester, Minn.) (Submitted for publication October 31, 1960; accepted March 2, 1961) Recent years have witnessed an increasing in- terest in the study of the possible relationship of blood coagulation to intravascular thrombosis (1-4). In spite of numerous methods of investi- gation, a consistent means of demonstrating and defining a clotting abnormality in thromboembolic diseases has not emerged. By retarding artificially the thromboplastin gen- eration test (TGT) we have been able to show acceleration of thromboplastin generation in cer- tain patients with intravascular thrombosis (5, 6). Our experience to date indicates that 75 per cent of 52 patients who had arteriosclerosis obliterans with thrombosis demonstrated the acceleration, 50 per cent of 40 patients with "idiopathic" recurrent thrombophlebitis did likewise, but only 11 per cent of 35 patients who had arteriosclerosis obliterans without thrombosis exhibited acceleration of the TGT. Of several hundred "normal" plasmas, less than 1 per cent was abnormally rapid in the TGT. It became apparent that the cause of the rapid formation of thromboplastin in the blood of these patients was demonstrable only in the adsorbed plasma reagent of the TGT, not in the serum re- agent. Since the adsorption of plasma removes plasma thromboplastin component (PTC or fac- tor IX), stable factor (factor VII), and Stuart factor (factor X), as well as prothrombin, these substances are probably not directly involved in the clot acceleration. A number of other factors remains; these are considered in detail in the pres- ent report. We wish to present evidence that the abnormal clot acceleration results from the presence of an * This investigation was supported in part by research grant H-5008(Ri) from the National Institutes of Health. excessive amount of coagulative activity which resides with the globulins in normal human plasma. We have designated this protein "thromboplastin generation accelerator," or simply "TGA," be- cause its activity seems to lie in the thromboplastin generation phase of clotting. METHODS 1. One-stage prothrombin time of Quick (7). This test, as modified locally (8), gives a normal value of 17 to 19 seconds. For the determinations of "dilute pro- thrombin time," fresh plasma was diluted 1: 5 and 1: 10 with oxalated saline solution (1 part of 0.1 M sodium oxalate and 9 parts of 0.9 per cent sodium chloride), and the test was carried out in the usual manner. Nor- mal values are 30 to 49 seconds for the 1: 5 dilution of plasma, and 56 to 67 seconds for the 1: 10 dilution. 2. Plasma clotting (recalcification) time (9). The normal value is 90 to 110 seconds. 3. Thromboplastin generation test (TGT) of Biggs and Douglas (10), modified by Duckert and co-workers (11), with substitution of soybean phosphatides for platelets (12). Normal values are the shortest clotting times, 8 to 11 seconds, occurring at 7 to 11 minutes of incubation. Retardation of the TGT (6) is carried out by diluting the plasmatic reagent 1: 50 with buffered saline [1 part of imidazole buffer (13) and 9 parts of 0.9 per cent sodium chloride] instead of our usual 1: 25 dilu- tion [Duckert modification (11)]. Normal values for the "retarded TGT" are the shortest clotting times, 13 to 16 seconds, occurring at 11 to 13 minutes of incuba- tion. Since we have demonstrated excess TGA activity as well with soybean phosphatide as with platelets (5), the convenience of the former has led to its routine use. 4. Electrophoresis of plasmatic factors (14). The fresh plasma was first treated with barium sulfate (50 mg per ml, for 5 minutes at 240 C) to remove prothrombin and factors VII, IX and X; 0.15 ml was applied to strips of Whatman no. 2 filter paper, 4 cm wide. Electrophore- sis was carried out in a cold room (40 C) for a period of 16 hours at a constant current of 0.6 ma per cm width of paper strips; the buffer used was sodium barbital-bar- 1006
Transcript of THROMBOPLASTIN NEWLY RECOGNIZED COMPONENT OF … · by diluting the plasmatic reagent 1: 50 with...

THROMBOPLASTINGENERATIONACCELERATOR,A NEWLYRECOGNIZEDCOMPONENTOF THE BLOODCOAGULA-
TION MECHANISMPRESENTIN EXCESS INCERTAIN THROMBOTICSTATES*
By CHRIS A. PASCUZZI, JOHNA. SPITTEL, JR., JOHN H. THOMPSON,JR. ANDCHARLESA. OWEN,JR. WITH THE TECHNICAL ASSISTANCE OF
CHARLENEMATTHEES
(From the Sections of Medicine and Clinical Pathology, Mayo Clinic and MayoFoundation, Rochester, Minn.)
(Submitted for publication October 31, 1960; accepted March 2, 1961)
Recent years have witnessed an increasing in-terest in the study of the possible relationship ofblood coagulation to intravascular thrombosis(1-4). In spite of numerous methods of investi-gation, a consistent means of demonstrating anddefining a clotting abnormality in thromboembolicdiseases has not emerged.
By retarding artificially the thromboplastin gen-eration test (TGT) we have been able to showacceleration of thromboplastin generation in cer-tain patients with intravascular thrombosis (5, 6).Our experience to date indicates that 75 per centof 52 patients who had arteriosclerosis obliteranswith thrombosis demonstrated the acceleration, 50per cent of 40 patients with "idiopathic" recurrentthrombophlebitis did likewise, but only 11 per centof 35 patients who had arteriosclerosis obliteranswithout thrombosis exhibited acceleration of theTGT. Of several hundred "normal" plasmas, lessthan 1 per cent was abnormally rapid in the TGT.It became apparent that the cause of the rapidformation of thromboplastin in the blood of thesepatients was demonstrable only in the adsorbedplasma reagent of the TGT, not in the serum re-agent. Since the adsorption of plasma removesplasma thromboplastin component (PTC or fac-tor IX), stable factor (factor VII), and Stuartfactor (factor X), as well as prothrombin, thesesubstances are probably not directly involved inthe clot acceleration. A number of other factorsremains; these are considered in detail in the pres-ent report.
Wewish to present evidence that the abnormalclot acceleration results from the presence of an
* This investigation was supported in part by researchgrant H-5008(Ri) from the National Institutes ofHealth.
excessive amount of coagulative activity whichresides with the globulins in normal human plasma.Wehave designated this protein "thromboplastingeneration accelerator," or simply "TGA," be-cause its activity seems to lie in the thromboplastingeneration phase of clotting.
METHODS
1. One-stage prothrombin time of Quick (7). Thistest, as modified locally (8), gives a normal value of 17to 19 seconds. For the determinations of "dilute pro-thrombin time," fresh plasma was diluted 1: 5 and 1: 10with oxalated saline solution (1 part of 0.1 M sodiumoxalate and 9 parts of 0.9 per cent sodium chloride),and the test was carried out in the usual manner. Nor-mal values are 30 to 49 seconds for the 1: 5 dilution ofplasma, and 56 to 67 seconds for the 1: 10 dilution.
2. Plasma clotting (recalcification) time (9). Thenormal value is 90 to 110 seconds.
3. Thromboplastin generation test (TGT) of Biggsand Douglas (10), modified by Duckert and co-workers(11), with substitution of soybean phosphatides forplatelets (12). Normal values are the shortest clottingtimes, 8 to 11 seconds, occurring at 7 to 11 minutes ofincubation. Retardation of the TGT (6) is carried outby diluting the plasmatic reagent 1: 50 with bufferedsaline [1 part of imidazole buffer (13) and 9 parts of 0.9per cent sodium chloride] instead of our usual 1: 25 dilu-tion [Duckert modification (11)]. Normal values forthe "retarded TGT" are the shortest clotting times, 13to 16 seconds, occurring at 11 to 13 minutes of incuba-tion. Since we have demonstrated excess TGA activityas well with soybean phosphatide as with platelets (5),the convenience of the former has led to its routine use.
4. Electrophoresis of plasmatic factors (14). Thefresh plasma was first treated with barium sulfate (50 mgper ml, for 5 minutes at 240 C) to remove prothrombinand factors VII, IX and X; 0.15 ml was applied to stripsof Whatman no. 2 filter paper, 4 cm wide. Electrophore-sis was carried out in a cold room (40 C) for a periodof 16 hours at a constant current of 0.6 ma per cm widthof paper strips; the buffer used was sodium barbital-bar-
1006

THROMBOPLASTINGENERATIONACCELERATOR
bituric acid of pH 8.6 and 0.05 ionic strength. The vari-ous cut-paper fractions were eluted with 2.5 ml of buf-fered saline.
5. Precipitating with aninnoniun sulfate. At room tem-perature, 1 ml of fresh barium sulfate-adsorbed plasma,diluted to a total volume of 10 ml, was subjected to pro-gressively greater concentrations of saturated solution ofammonium sulfate after removal by centrifugation ofthe precipitate formed in each preceding step. The vari-ous precipitates were dissolved and subjected to dialysisagainst several changes of 0.9 per cent sodium chloridefor 16 hours at 40 C.
MATERIALS
1. Excess TGA plasma. This was obtained from pa-
tients with arteriosclerosis obliterans and associatedthrombosis. All of these samples of plasma exhibited in-creased thromboplastic activity in the thromboplastingeneration tests whether the plasma was diluted 1: 25 or1: 50. This increase in activity ranged from approxi-mately two to five times the normal rate of generationof thromboplastin. These values were estimated by com-
parison with the thromboplastin-generating activity ofnormal plasma. Essentially, the thromboplastin gener-
ated at various intermediate intervals of time is cal-culated from serial dilutions of the control and patientplasmas. If, for example, at the fifth minute of incu-bation twice as much thromboplastin has been generatedby the patient as by the control, the activity is recordedas two times normal.
On the other hand, in the studies of the properties ofTGA (electrophoretic mobility, precipitation, and heatstability) an attempt at more direct evaluation of TGAactivity was made by the degree of augmentation of thegeneration of thromboplastin by normal plasma to whichthe fraction was added.
2. AHG-deficient plasma. Fresh plasma was obtainedrepeatedly from 2 severely hemophilic patients. Thesesamples were cross checked with samples from 6 otherhemophilic patients and all 8 exhibited the same defect, a
lack of the antihemophilic globulin (AHG or factorVIII).
3. Aged normal plasma. Fresh normal plasma was
heated to 37.50 C for 24 to 30 hours until the prothrom-bin time exceeded 60 seconds and the plasma clotting timeexceeded 300 seconds. This plasma has been shown tobe deficient in both factor V and AHG when testedagainst plasmas of parahemophilic and hemophilic pa-
tients.All samples of plasma were oxalated by the addition
of 0.5 ml of 0.1 M sodium oxalate to 4.5 ml of freshlydrawn whole blood.
RESULTS
Certain known coagulation factors are presentin normal aged serum (factors VII, IX, X, Hage-man and PTA); others are active in fresh plasmathat has been treated with one of the various chem-
ical adsorbents, such as barium sulfate (factorsV, VIII, Hageman, PTA and fibrinogen). TheTGT is carried out by measuring the activity ofplasma thromboplastin formed from a mixturecontaining serum, adsorbed plasma, platelets orplatelet substitute, and calcium. Since thrombo-plastin generates only if all four reagents are pres-ent, replacement of the patient's serum or plasmawith normal serum or plasma can lead to a pre-liminary delineation of the patient's abnormality.
Wehave shown in previous reports (5, 6) thatacceleration of thromboplastin formation, whenpresent, has always been restricted to the plasmaticreagent. Serum activity in the thromboplastingeneration test in four representative cases inwhich accelerated thromboplastin formation wasexhibited is shown in Table I. Serums in Pa-tients 1, 2 and 3 were normal while the serum inPatient 4 was actually retarded because of the ad-ministration of coumarin drugs. The thrombo-plastin-generating activity of the plasmatic rea-gent in these patients ranged from two to five timesnormal. Because of this observation, it seemedunlikely that the serum factors could be responsiblefor the acceleration process.
Platelets likewise appear to bear no direct rela-tionship to the phenomenon of plasma acceleration,since we have observed it in thrombocytopenic
TABLE I
Serum activity in the TGTin patientswith excess TGA plasma *
Incuba- Typical Coagulation timetion controltime serum Pt. 1 Pt. 2 Pt. 3 Pt. 4
min sec sec1 65 90 93 78 523 47 66 68 72 485 45 42 47 41 457 32 30 478 21 16 26 159 12 14 15 12.5 39
10 10 12 12 1 1 3611 9.5 10 913 1 1 14 11.5 10.5 32
Plasma activ-ity in TGT,times normal 2 2 4 5
* Samples of serum (1: 10) from 4 patients with throm-boembolic disorders were combined with normal controlplasma (1:25) in the TGT. Patient 4 was being treatedwith coumarin drugs; prothrombin time was 35 seconds attime of test. His serum yielded reduced thromboplasticactivity; serum from the other three patients did not devi-ate significantly from normal.
1007

PASCUZZI, SPITTEL, THOMPSONAND OWEN
TABLE II
Stability of TGA at 56° C*
Excess Excess TGAplasma heatedNormal TGA at 560 Ctcontrol plasma
Incuba- plasma unheated 5 min 10 min 15 min 20 mintiontime Clotting time
min sec sec sec
1 81 56 48 76 70 1083 66 13 17 32 25 795 38 10.5 11 12 12 427 26 10.5 10.5 11.5 11.5 238 14 10.5 11 12 12 169 13.5 11.5 11.5 13 12.5 14
10 14 12 12.5 15
* Plasma containing excess of TGA was adsorbed withBaSO4 and diluted 1:50 in the TGT; normal serum wasdiluted 1:10. Increase in rate of generation and in amountof thromboplastin formed is evident.
t To maintain optimal AHGand factor V activity inheated samples, 1 vol fresh normal plasma (1: 25) wasmixed with 1 vol heated plasma (1:25); this mixture wasthen used as the plasmatic reagent in the TGT.
plasmas; and in our modification of the TGT,soybean phosphatide is used as a platelet substitute.
The series of experiments reported here werecarried out for the purpose of determining whichof the recognized factors present in adsorbedplasma and absent from serum, namely factors V,VIII and fibrinogen, might be responsible for theexcessive thromboplastin formation in certain pa-tients. Because we have not observed increasedconcentrations of fibrinogen in the plasma of thesepatients, our attack was directed primarily towardfactors V and VIII. As will be shown subse-
quently, fibrinogen appears to be excluded as thecause of increased formation of thromboplastin inthese cases.
Heat-stability studies. Wehave found that ex-
cess TGA activity persists after warming theplasma to 370 C for 30 minutes and to 240 C for24 hours, and after storage at - 200 C for as longas 1 year. A comparison of its lability at 560 Cwith factor V and AHGwas carried out.
The stability of factor V (labile factor) was
measured by determining the corrective effect ofnormal plasma (1 vol) on the prothrombin timeof aged normal plasma (9 vol), after the normalplasma had been exposed to a temperature of 560C for various lengths of time. Normal plasmathat had shortened the prothrombin time of theaged plasma from 85 to 30 seconds before heatingexerted no effect on the long prothrombin timeof the aged plasma after 1 minute at 560 C. Wefound that after 15 seconds at 560 C, 30 per cent offactor V activity remained; after 30 seconds, 12per cent; after 45 seconds, 5 per cent; and after60 seconds, 0 per cent. The thermolability offactor V in excess TGAplasma was indistinguish-able from normal.
Stability of AHGwas determined by heatingfresh normal plasma to 560 C for various periodsand then determining the effect of this plasma on
AHG-deficient plasma by means of plasma re-
calcification times and thromboplastin generationtests. By these methods, AHGactivity of nor-
TABLE III
Electrophoretic localization of TGA *
Normal plasma fractions Excess TGAplasma fractions
Control AlbuminIncuba- system +ai a2 a y1 s2 Albumin al I a2 a Y1+y2t
tiontime Clotting time
min sec sec sec sec sec sec
1 113 73 79 78 72 100 81 81 77 61 703 79 72 73 65 50 72 78 86 68 52 525 62 52 54 53 30 53 69 65 65 20 357 41 36 38 22 14 42 49 35 30 10 138 25 27 23 15 12 27 37 24 17 11 129 18 15 16 14 12 19 21 16 14 11 11
10 14 13.5 15 11 11.5 13 15 15 11 12 1111 13.5 13 14 11 13 13 15 15 10.5 12.5 1212 14 13.5 14 12 14 13 15 11 13
* Barium sulfate-adsorbed normal plasma and excess TGAplasma (Patient 1, Table IV) were electrophoresed onpaper strips (see Methods); zones were eluted with buffered saline and each was then used as diluent for normal plasmaticreagent in the TGT instead of the usual saline diluent. Accelerator activity was found in -y and 8 zones, the formerrelated to activity of AHGand factor V, the latter to TGA (see text).
t The 'yj and 72 zones were not clearly separable in this plasma and consequently were tested together.
1008

THROMIBOPLASTINGENERATIONACCELERATOR
TABLE IV
Summary of electrophoretic analyses of TGA activity (in s-globulin) and AHGactivity (in y-globulin)in the plasmas of seven patients with excess TGA activity *
,6-globulin (TGA) activity -yi-globulin (AHG) activity
Normal control plasma Excess TGAplasma Normal control plasma Excess TGAplasma
Shortest Shortest Shortest Shortestclotting at Incubation clotting at Incubation clotting at Incubation 'clotting at Incubation
Pt. time time time time time time time time
sec min sec min sec min sec min1 11 10 10 7 1 1.5 10 1 1 92 12 9 12 8 12 8 12.5 83 12.5 8 9.5 8 11.5 8 1 1 84 12.5 11 11 11 11 9 10 95 13.5 8 1 1 7 14 8 14 86 14 10 12 9 13 9 14 97 14.5 16 13 13 17 16 16.5 16
* The TGTwas performed as described in Table III. Only the shortest clotting times and the time of incubationrequired to reach these times are listed. The AHGactivity in all cases was comparable between the plasmas of patientsand controls. In every instance there was more accelerating activity in the ,8-globulin of the excess TGAplasma than inthe #-globulin of the control plasma subjected to electrophoresis concurrently.
mal plasma was found to be depressed about 70per cent in 1 minute and about 90 per cent in 5minutes, and was undetectable after 10 minutesof exposure to 560 C. The thermolability ofAHG in excess TGA plasma was indistinguish-able. from normal.
The effect of heating excess TGAplasma to 560C is shown in Table II. It can be seen that therate of thromboplastin generation was little af-fected for the first 15 minutes during which timeboth factor V and AHGactivities had completelydisappeared.
Electrophoretic identification. Fresh samplesof seven different barium sulfate-adsorbed ex-
cess TGA plasmas, along with seven samples ofnormal control plasma similarly treated, were sub-jected to paper electrophoresis. Eluates of variouszones on the paper strips were used as diluents forthe normal plasmatic reagent in the TGT. Ad-sorbed plasma was used for electrophoresis in or-
der to simplify the analyses by prior removal offactors VII, IX, X and prothrombin.
The complete TGT's of a typical case (Patient1, Table IV) are listed in Table III. All seven
cases are summarized in Table IV. Increasedthromboplastin formation was obtained when elu-ates from /8 and y, fractions of either the normalcontrol or excess TGA plasma were used as di-luents. The Y/ eluates of both the control and theexcess TGA plasma showed approximately thesame activity; however, the /8 fraction of the ex-
cess TGA plasma exhibited a greater degree of
thromboplastic activity than did the corresponding,8 fraction from normal plasma. Comparable re-sults were obtained invariably in each of the othersix studies (Table IV). It seems clear that TGAand AHGcan be differentiated electrophoretically.
Eluates from the various fractions of both nor-mal plasma and excess TGA plasma were testedfor AHGactivity (Table V). In every instancethe eluate from the Yi region decreased the re-calcification time of AHG-deficient plasma, whileeluates from the other fractions failed to influencesignificantly the clotting time of the hemophilicplasma. The apparent difference between ourfinding and that of Lewis, Walters, Didisheim andMerchant (15) may be technical, since this groupused continuous flow electrophoresis.
TABLE V
AHGactivity in electrophoretic fractionsof normal plasma *
ClottingPlasma time
sec
AHG-deficient plasma 440
AHG-deficient plasma plus:Albumin (fresh plasma) 450
(fresh plasma) 400ly (fresh plasma) 30071 (aged plasma) 410
* Eluates of paper electrophoretic fractions were addedto fresh AHG-deficient plasma in 1:10 ratio; plasma clot-ting times were determined on mixtures. Sample of agedplasma (free of AHG) was similarly treated as control.AHGactivity seemed to concentrate in ayl zone.
1009

PASCUZZI, SPITTEL, THOMPSONAND OWEN
Electrophoretic separation of coagulation factors
present in BaS04-adsorbed plasma
AHG TGA
Normal
I A.b' . ..
X2 Ai 8 a. CV'1 Alb
TGA
AHG | 1
j'\ to I I1111
I IiExcess TGA I
!, ' L.' ,I 'X2 l a2 off Alb
FIG. 1. COAGULATION ACTIVITIES IN THE ,B AND ly
ZONES OF NORMALPLASMA AND EXCESS TGA PLASMA,
BOTH ADSORBED WITH BASO4 BEFORE PAPER ELECTRO-PHORESIS.
To exclude the effect of factor V, which usuallytravels with the yi plasma proteins (14), the elu-ates of the /8 fraction of both the control plasmaand the excess TGAplasma were heated to 56° Cfor 1 minute to inactivate completely any factorV that might have been present. These heatedsamples were then used as diluents for the plas-matic reagent in the TGT, as above. Neither theeluate from the control nor that from the excess
TGA plasma showed any loss of activity afterheating. It is assumed, therefore, that there was
virtually no factor V activity in the /8 fractions,and in turn that the /8-globulin clotting activitywas not attributable to factor V. In each electro-phoretic test, fibrinogen was heavily concentratedat the point of application of the plasma to thepaper strips in the y region, and far removed fromthe /8 fraction.
Hageman factor activity has been shown to
reside in the Yi fraction (16), and PTA activityin the 3,-y interspace (17); unlike TGA, how-ever, both are present in serum.
Electrophoretic analyses of barium sulfate-ad-sorbed serum (lacking prothrombin and factorsV, VII, VIII, IX, X and TGA, but containingPTA and Hageman factor) from normal controlsand from patients with accelerated clotting were
carried out and eluates from the various fractionswere studied in a manner similar to that used forthe plasma. No evidence of increased thrombo-plastic activity was found when these eluates were,
used as diluents in the TGT. It was assumed fromthis experiment that the presence of excessiveamounts of Hageman factor and PTA in the TGTdo not materially influence thromboplastin gen-eration. The electrophoretic zones of activity ofTGA, factor V, and AHGin normal and excess
TGAplasma are illustrated in Figure 1.Precipitating with ammonium sulfate. To cor-
roborate the findings obtained by electrophoresis,precipitation experiments with ammonium sulfate
TABLE VI
Localization of TGA by precipitation with ammonium sulfate *
Ammonium sulfate saturation
Fractions of normal plasma Excess TGAplasma fractionsControl
systemt 25% 25-35% 35-40% 40-45% 25% 25-35% 35-40% 40-45%Incuba-
tion time Clotting time
min sec sec sec sec sec
1 78 69 65 66 79 64 76 74 663 74 49 49 41 64 55 96 53 665 62 19 19 19 40 37 70 19 397 35 11 14 12 16 17 38 118 22 11 14 14 13.5 12.5 17 10 169 14 12 13 11.5 14.5 12 15 8.5 13
10 13 12 12 11.5 13 14 12.5 9.5 1411 13 12 12.5 13 14 14 1412 14 13.5 14 14 14 13.5
* Barium sulfate-adsorbed normal plasma and excess TGAplasma were fractionated with various concentrations ofsaturated ammonium sulfate. Precipitates were dissolved, freed of (NH4)2SO4 by dialysis, and used as diluents (1:50)for plasmatic reagent (normal plasma) in the TGT. AHGactivity is evident in 25% fractions, and TGAin 35 to 40%fractions, particularly in excess TGA plasma (see text). Reduced AHGactivity of excess TGA plasma is probablyrelated to 3-month storage of this plasma at -20° C.
t Buffered saline used as diluent.
1010

THROMBOPLASTINGENERATIONACCELERATOR
were performed. In these procedures, fresh nor-
mal plasma (control) and excess TGA plasmawere initially adsorbed with barium sulfate andthen subjected to fractionation with saturated am-
monium sulfate. The precipitates from the vari-ous concentrations were dissolved, dialyzed andthen used as diluents in the TGT. The influenceof these fractions on the retarded TGT is shownin Table VI.
Both the 25 per cent and the 35 to 40 per centammonium sulfate saturation fractions of normalplasma and the excess TGAplasma exhibited in-creased thromboplastic activity. When testedagainst AHG-deficient plasma, the 25 per centfractions were the most active in correcting thelong clotting time of the hemophilic plasma; therewas little difference between the 25 per centfraction derived from normal plasma and thatfrom excess TGA plasma (Table VII). On theother hand, the 35 to 40 per cent fraction fromexcess TGAplasma was significantly more activein accelerating normal thromboplastin generationin the TGT than was the same fraction from nor-
mal plasma. Neither 35 to 40 per cent fractionexhibited any AHGactivity.
Dialysis studies. Fresh excess TGA plasma,barium sulfate-adsorbed excess TGA plasma andthe 35 to 40 per cent ammonium sulfate saturationfraction of excess TGA plasma were dialyzed incellophane bags against 0.9 per cent sodium chlo-ride for 20 hours at 40 C. No reduction of TGAactivity was found in these plasmas; this is com-
patible with the concept that TGA is a protein.
TABLE VII
AHG activity in fractions obtained by precipitation fromnormal plasma with ammonium sulfate *
Clottingtime
sec
AHG-deficient plasma 209
AHG-deficient plasma plus fractionobtained at saturation of:
25% 15725-35% 19035-40% 20440-45% 21145-50% 196
* Influence of ammonium sulfate-precipitated fractionsof fresh normal plasma on prolonged recalcification time ofAHG-deficient plasma is shown. Percentages refer tostrength of saturated ammonium sulfate solution at whichprecipitation occurred. Precipitates were reconstitutedafter dialysis to equal plasma concentrations, then wereadded to AHG-deficient plasma in 1:9 ratio, and plasmaclotting times determined on mixtures. The 25 per centfractions presumably contained AHG(see text).
Effect of adsorbent chemicals. Each milliliterof plasma containing excess TGAwas treated withbarium sulfate (50 mg) for 5 minutes at 240 C,tricalcium phosphate (0.1 ml of a 0.2 M suspen-sion) for 5 minutes at 240 C, or aluminum hy-droxide (0.1 ml of a 6.1 per cent suspension) at0° C for varying periods of time and then testedin the TGT. Normal plasma similarly treatedwas used as the control. The results are shownin Table VIII. Accelerated generation of throm-boplastin was equally apparent after the bariumsulfate and tricalcium phosphate treatment. On
TABLE VIII
Action of adsorbing agents on TGA *
BaSO4-adsorbed Ca3 (P04)2-adsorbed Al (OH) 3-adsorbedt
Normal Excess TGA Normal Excess TGA Normal Excess TGAplasma plasma plasma plasma plasma plasma
Incubationtime Clotting time
min sec sec sec
1 73 83 63 63 70 773 69 50 59 62 71 695 42 45 49 47 50 527 32 26 37 31 35 369 19.5 13 21 16 21 22
10 16 12 17 14 17 191 1 14.5 11.5 16 12.5 15.5 1612 15 12 16 12.5 15.5 1613 17 13 16.5 17
* Normal plasma and excess TGAplasma were treated with BaSO4, Ca3(PO4)2 or Al(OH)3 and tested in the retardedTGT. Accelerated generation of thromboplastin was not evident after adsorption with Al(OH)3.
t Adsorbed for 5 minutes.
1011

PASCUZZI, SPITTEL, THOMPSONAND OWEN
TABLE IX
Effect of prolonged Al(OH)3 adsorption onTGA content of normal plasma *
BaSO4- Al (OH) :-treated plasmatreated
Incuba- plasma 15 min 30 min 45 mintiontime Clotting time
min sec sec
1 80 66 68 783 64 655 54 50 61 607 30 318 19 26 46 549 12 18 33 46
10 1011 9.5 15.5 21 2912 19 2113 10 15 16 1815 1 1 14.5 15.5 1717 16 16 18
* Samples of fresh normal plasma were adsorbed withBaSO4 (control) and with Al(OH)3 for 15, 30 and 45minutes. Activity of each treated sample was measuredin the TGT using normal serum diluted 1:10 in bufferedsaline. All samples were diluted 1:25 with bufferedsaline containing adsorbed normal serum as source ofoptimal PTA and Hageman factor. Generation of throm-boplastin diminished as exposure to Al(OH)3 increased.
the other hand, treatment with aluminum hy-droxide for 5 minutes sharply reduced the exces-sive TGAactivity.
In order to determine the effect of prolongedaluminum hydroxide adsorption on normal plasma,samples of plasma were exposed to aluminum hy-droxide for periods of 15, 30 and 45 minutes andwere then tested in the TGT (Table IX).Thromboplastin-generating activity diminished
steadily the longer the plasma remained in contact
with the aluminum hydroxide. In order to ruleout the possibility that the aluminum hydroxidewas adsorbing PTA or Hageman factor, bariumsulfate-adsorbed normal serum was added to theTGT. Since PTA and Hageman factors are
present in such serum, the diminished thrombo-plastin generation cannot be attributed to them.
Theoretically, the results of adsorption withaluminum hydroxide could be attributed to re-
moval of factor V, AHGor TGAfrom the plasma.To determine the effect of prolonged aluminumhydroxide adsorption on factor V activity, 1 volof normal plasma, treated for 15, 30 and 45 min-utes, was added to 9 vol of aged plasma, and one-
stage prothrombin times were determined on themixtures; the prothrombin time of the aged plasmaalone was 65 seconds. All of the samples short-ened the prothrombin time to 36 to 38 seconds.Since fresh, unadsorbed normal plasma shortenedthe prothrombin time of the aged plasma to thesame range, namely 37.5 seconds, it was con-
cluded that factor V activity was not affected byprolonged adsorption with aluminum hydroxide.
The effect of aluminum hydroxide on AHGac-
tivity of normal plasma was evaluated by measur-
ing the effect of such treated plasma on the pro-
longed clotting time of AHG-deficient plasma.Samples of the treated plasma were added to thehemophilic plasma in a 1:9 proportion. It was
found (Table X) that AHGactivity was not re-
TABLE X
Effect of prolonged Al(OH)3 adsorption on AHGactivity of normal plasma *
Estimated AHG,Plasma clotting Added AHG, % action, %
Sample time of normal of normal
sec
AHG-deficient plasma 480 0
AHG-deficient plasma plus:Normal plasma untreated 135 100Normal plasma treated for:
10 min 140 9030 min 142 8545 min 137 95
Normal plasma untreated anddiluted 1:4 in saline 170 25
Normal plasma treated for 45min and diluted 1:4 in saline 170 25
* Fresh normal plasma before and after adsorption with Al(OH)3 for 10, 30 and 45 minutes was mixed with AHG-deficient plasma and effect on clotting time noted. Plasmas were mixed in proportion of 9 parts AHG-deficient plasmato 1 part test plasma. There was no obvious effect of Al(OH)3 on AHGof normal plasma.
1012

THROMBOPLASTINGENERATIONACCELERATOR
TABLE XI
Influence of Al(OH)3 on normal plasma and excess TGA plasma in correction of defect of hemophilic plasma *
BaSO4-adsorbed Al (OH) a-adsorbedt
Fraction of Normal plasma Excess TGAplasmanormal or Normal plasma Excess TGA plasma
excess TGA Activityplasma in Clotting based on Clotting Rel. Clotting Clotting Rel.mixtures time dilution time Activityt act. time Activityt time Activityt act.
sec % sec % sec % sec %1/10 123 100 1041/20 139 50 110 143 45 123 100 2.21/40 155 25 127 90 3.6 151 30 142 45 1.51/80 165 12.5 144 45 3.6 162 14 156 25 1.81/160 184 6.3 150 30 4.81/320 210 3.1 170 10 3.3
* BaSO4 and Al(OH)3-adsorbed samples of normal and excess TGA plasma were added in various proportions toAHG-deficient plasma and clotting times were determined on mixtures. Clotting time of AHG-deficient plasma alonewas 390 seconds. Relative activity (Rel. act.) was calculated from: excess TGA%activity/normal %activity. AHGactivity of normal plasma was the same whether adsorbed in BaSO4or Al(OH)3. Apparent AHGactivity was 3.8 timesnormal when excess TGAplasma was adsorbed with BaSO4; half this increased activity disappeared after Al(OH)3 ad-sorption, suggesting TGArather than AHGeffect (see text).
t Plasma adsorbed for 10 minutes.t Compared with BaSO4-adsorbed normal plasma.
duced by 10, 30 or 45 minutes of exposure of nor-
mal plasma to aluminum hydroxide.Since aluminum hydroxide had no apparent ef-
fect on the AHGactivity of normal plasma, butdid on the TGA activity of excess TGA plasma,the effect of this adsorbent on the AHGactivity ofexcess TGA plasma was studied, barium sulfateadsorption being used as a control. Samples of ad-sorbed normal and excess TGAplasma were addedin decreasing concentrations to hemophilic plasma;plasma clotting times were determined on themixtures. These results are shown in Table XI.After barium sulfate adsorption the excess TGAplasma exerted about four times the activity ofnormal plasma in correcting the prolonged clottingtime of the AHG-deficient plasma. After adsorp-tion for 10 minutes with aluminum hydroxide, theactivity was reduced to about twice normal. Treat-ment with aluminum hydroxide did not apparentlyalter the corrective ability of the normal plasma,however. It was assumed from this and the previ-ous experiment (Table X) that the increased ac-
tivity of the excess TGAplasma in correcting the
clotting time of the hemophilic plasma was at-
tributable to the accelerator effect of TGA and
not to increased AHG, since AHGis apparentlynot adsorbed by aluminum hydroxide. The simi-
larity of action of TGA and AHGsuggests that
the positions of both factors in the scheme of blood
coagulation are closely allied.
Prothrombin time of diluted plasma. Thus far,the evidence places TGA activity early in theclotting reaction (prothromboplastic step), be-cause of acceleration in the TGT associated withnormal prothrombin times. In order to assessany possible second-stage activity of TGA, pro-thrombin times, which are independent of the firststage, were determined on diluted specimens of anumber of excess TGA plasmas (Table XII).The results tend to exclude any second-stage ac-tivity comparable to that exhibited by factors V,VII and X. The indirect implication is that ex-cess TGA activity is not the result of excessfactor V.
TABLE XII
Prothrombin time of undiluted and diluted normal plasmaand four samples of excess TGA plasma *
Prothrombin time
Excess TGAplasma samplesNormal
Plasma dilution plasma No. 1 No. 2 No. 3 No. 4
sec sec sec sec secUndiluted 17-19 19 17 18.8 181:5 30-49 37.5 37 35 411:10 56-67 58 49 57 61
Acceleration Normal 3 3 3 2of thrombo-plastin for-mation in TGTtimes normal
* There was no obvious effect of excessive TGA onsecond step of clotting (thromboplastin activation orcothromboplastic step).
1013

PASCUZZI, SPITTEL, THOMPSONAND OWEN
TABLE XIII
Estimation of factor V activity inexcess TGA plasma *
Prothrombin timeProportion of
normal plasma Normal Excess TGAplasmaof "excess TGA plasma samples
plasma" to values,aged plasma range No. 1 No. 2 No. 3 No. 4
sec sec sec1:10 38-46 40 30 40 431:20 48-56 49 43 48 50
Plasma acceleration 4 3 2 2in TGT, timesnormal
* Factor V activity in 4 samples of excess TGAplasmawas determined by adding this plasma to aged normalplasma in proportions of 1:10 and 1:20 and determiningone-stage prothrombin time on mixtures. Prothrombintime of aged plasma was 85 seconds. Only plasma no. 2exhibited any suggestion of excessive factor V activity.
Determination of factor V activity in excessTGA plasma. Factor V activity in excess TGAplasma was assessed directly by noting the degreeof correction of the prolonged prothrombin timeof aged plasma on mixing the two plasmas. Threeof the four studied showed no evidence of increasedactivity of factor V; in the fourth instance, therewas modest acceleration as compared to controlvalues (Table XIII).
Because of this one apparent exception to anotherwise sharp differentiation of TGA and fac-tor V, further discrimination was sought by wayof the TGT (Table XIV). Excess TGAplasma,which had approximately three times the normalthromboplastic activity in the TGT when meas-ured in the conventional manner, was heated for2 minutes at 56° C to inactivate factor V com-pletely. When tested in the TGT this plasma stillexhibited approximately the same degree of ex-cess activity as before heating. (A constant sourceof factor V was added in the form of fresh AHG-deficient plasma.) Since increased thromboplas-tic activity persisted in the excess TGA plasmadespite complete inactivation of its factor V con-tent, it was assumed that factor V was not re-sponsible for the increased activity of the unheatedplasma in the TGT.
Effect of coumarin drug therapy. Many of thepatients with thrombotic arterial and venous dis-ease whose plasma showed the phenomenon ofacceleration in the TGT were treated with oneor another coumarin drug. In spite of lengthened
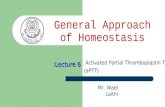
prothrombin time and retardation of the serumactivity in the TGT, their plasmas showed no re-duction in excessive TGAactivity. Results of theTGTof the plasma from one such patient on long-term anticoagulant therapy are illustrated in Fig-ure 2. This patient's prothrombin time was effec-tively prolonged by drug therapy, but the TGAactivity of his plasma remained persistently ele-vated. Wehave also observed excess TGAin theplasma of certain patients with thrombotic diseasein the presence of long-standing hepatic diseasewith demonstrable deficiencies of factors V, VII,X and prothrombin.
DISCUSSION
By retarding the conventional thromboplastingeneration test (retarded TGT), we have beenable to demonstrate an unusually rapid formationof plasmatic thromboplastin in 75 per cent of 52persons with acute peripheral arterial thrombosiscomplicating arteriosclerosis obliterans (18) andin 50 per cent of 40 patients with idiopathic throm-bophlebitis. The present study provides a de-tailed comparison of this accelerated clotting ac-tivity with each of the recognized blood clotting
TABLE XIV
Effect of heating excess TGA plasma for 2 minutes at 56° Con accelerated thromboplastin generation in TGT *
Incubation Control Excess TGAtime systemt systeml
min1 54 543 56 535 36 327 23 208 18.5 159 18 12
10 17 121 1 16 1112 16 10.514 1 7 1 1.5
* Factor V activity was removed from BaSO4-adsorbedexcessTGA plasma by heating at 56° C for 2 minutes.Mixture of equal parts of this plasma and fresh unheatedBaSO4-adsorbed AHG-deficient plasma (each diluted1: 25) constituted plasmatic reagent for TGT. Finalconcentration of factor V was 1:50 (all from AHG-de-ficient plasma), and of AHG1:50 (all from heated plasma).Normal plasma was similarly treated. TGAactivity wasnot appreciably reduced by heating despite complete de-struction of factor V.
t Normal plasma heated to 56° C for 2 minutes (1:25)plus fresh AHG-deficient plasma (1: 25).
1 Excess TGAplasma (exhibiting approximately 3 timesnormal activity in thromboplastin formation when testedin TGT prior to heating) heated to 560 C for 2 minutes(1: 25) plus fresh AHG-deficient plasma (1: 25).
1014

THROMBOPLASTINGENERATIONACCELERATOR
factors. This has led us to the conclusion that therapid generation of thromboplastin in these pa-tients cannot be satisfactorily explained on thebasis of any currently identified blood-clottingfactor. For clarification, we have applied tothe newly recognized hypercoagulable activity thename "thromboplastin generation accelerator"(TGA), since its function is thereby described.
TGA was found to migrate electrophoreticallywith the p-globulins of plasma, and in this regardis like factor VII (14) and factor IX (19). TGA,like AHG (factor VIII), labile factor (V),Hageman factor, PTA, and fibrinogen, was notadsorbed from plasma by barium sulfate. TGAdid not survive clotting, and is therefore absentfrom serum, like antihemophilic globulin (factorVIII), labile factor (V), prothrombin and fibrino-gen. On the basis of these simple experimentsalone, there can be only a few well authenticatedcoagulation factors that might have the TGA ac-tivity.
Factor V. TGA is considerably more heatstable than factor V. Within 1 minute at 560 C,factor V activity in human plasma was completelydissipated, while TGAremained active for at least15 minutes. When paper electrophoresis of freshplasma was carried out, factor V activity could bedemonstrated in the 8--y interspace (14), whileTGAactivity was confined to the ,8 fraction. Pro-longed contact with aluminum hydroxide decreasedTGA activity in direct proportion to the lengthof exposure. In contrast, factor V activity re-mained unaffected even after 45 minutes of ad-sorption. When assays of factor V were carriedout on plasmas containing excessive amounts ofTGA, a moderate increase was found in only oneof the four studied.
Antihemophilic globulin (AHG, factor VIII).TGA was found to be somewhat more stable at560 C than AHG, which was completely inacti-vated within 10 minutes. The stability of AHG,therefore, lies midway between that of factor Vand that of TGA.
After electrophoresis of fresh barium sulfate-adsorbed plasma, maximal AHGactivity could bedemonstrated in the y,-globulin fraction, but notin the /8-globulin zone of either normal plasma orplasma containing excess TGA. After precipi-tation with ammonium sulfate, AHGactivity wasconfined to the 25 per cent saturation fraction
70
50-
4040
30
20 \ \
10
1 2 3 4 5 6 7 8 9 10 11
Incubation time (minutes)
FIG. 2. EFFECT OF COUMARINANTICOAGULANTTHERAPYON TGA ACTIVITY. This 54 year old man had noted in-termittent claudication in right calf for 5 years. OnMarch 8, 1960, he sustained a sudden aortoiliac occlu-sion. An aortofemoral bypass graft (Teflon) insertedon April 1, 1960, resulted in return of normal arterialpulsations to both lower extremities. Anticoagulant ther-apy with Warfarin sodium was instituted on April 26,1960, with plans to continue it on long-term basis.TGA activity remained essentially unchanged during a3 month period, despite continuous and adequate therapywith Warfarin sodium.
(euglobulin) while TGAwas present in the 35 to40 per cent fraction (pseudoglobulin). Anotherdistinction was the inability of aluminum hydrox-ide to adsorb AHG; after prolonged exposure,most or all of the TGAwas adsorbed.
Fibrinogen. Fibrinogen is closely associatedwith AHG in the y' electrophoretic and 25 percent ammonium sulfate saturation fractions; likeAHGit was cleanly separated from the zone oc-cupied by TGA.
PTA and Hageman factor. Since both PTAand Hageman factor were present in barium sul-fate-adsorbed plasma, the question might ariseconcerning the part played by these substances inthe hypercoagulable state. The fact that bothPTA and Hageman factor are present in an ac-tive state in serum (16, 17) would seem to dis-tinguish them from TGA, since the thromboplas-
1015

PASCUZZI, SPITTEL, THOMPSONANDOWEN
tin-generating activity of serum from none of ourpatients with thromboembolism has been hyper-active. Furthermore, eluates of electrophoreticallyprocessed normal, barium sulfate-adsorbed serum,containing only PTA and Hageman factor as faras is known, did not enhance thromboplastin for-mation in a TGT of normal plasma and serum.
Both PTA, in the 18-y interspace, and Hagemanfactor, in the Yi zone, were effectively separatedfrom TGA, in the 8 zone, by electrophoresis(16, 17).
Does TGA activity correspond to previouslydescribed blood coagulation factors? Increase inconcentrations of factor VII (20)) factor V (21),and AHG (22) in certain clinical states has beenreported but does not seem pertinent in this dis-cussion because of the significant differences be-tween these clotting factors and TGA.
Wessler, Reimer and Deykin (4, 23) have de-scribed a serum activity capable of inducing throm-bosis. They have entitled it serum thromboticaccelerator (STA). Since STA is present inserum and is readily adsorbed by barium sulfate,it cannot be reconciled with the properties ofTGA.
The absence of TGA in serum, its resistance tobarium sulfate adsorption, and its greater heatstability separate it from the prephase acceleratordescribed by Fisch (24).
Waaler (25) has reported that there is an"activation product" resulting from the interac-tion of PTA and Hageman factor. Certain prop-erties of activation product and TGAare similar:electrophoretic mobility, property of being unaf-fected by coumarin drugs, and susceptibility to am-monium sulfate precipitation. However, Waalerfound activation product reduced four-fifths byheating plasma for 30 minutes at 370 C, whereasTGA is unaltered by this same treatment. Fur-thermore, Waaler states that "activation productwas unstable when in plasma" and "in serum agreat amount of activation product was found."Neither of these descriptions is compatible withour observations of TGA activity. We are un-able to find in the literature any description of acoagulation activity like that of TGA.
Function of TGA. TGA appeared to influ-ence primarily the rate of formation, and possiblythe yield, of plasma thromboplastin. In the TGT,peak thromboplastic activity was reached in one-
half to two-thirds the time required by normalplasma. In addition, the activity of the thrombo-plastin produced was usually greater than thatof the control, as evidenced by shorter clottingtimes in the substrate plasma. When TGA waspartially removed from excess TGAplasma by ad-sorption with aluminum hydroxide, both the rateof formation and the amount of thromboplastinformed were reduced.
If TGA's function lies in the generation ofthromboplastin, it might act in the initial pro-thromboplastic step, in the second or activationstep, or both. These two steps can be distinguishedby the prothrombin time test of Quick (7), sincethe addition of an extract of brain to plasma ap-parently results in complete bypass of the pro-thromboplastic step with all the factors involved.Prothrombin times were determined in the usualmanner, as well as with five- and tenfold dilutionsof plasma in order to detect any minute shorteningof the prothrombin times. In both undiluted anddiluted plasmas, prothrombin times of excessTGAplasmas were uniformly within normal lim-its. This would seem to isolate TGA's positionin the scheme of clotting to the initial step, in as-sociation with platelets, Hageman factor, AHG,PTCand PTA.
Routine detection of excess plasmatic TGA.The original description of the TGT by Biggsand Douglas included adsorption of.the plasmaticreagent with aluminum hydroxide (10); sincethis reagent adsorbs TGA, it is possible that thosewho use this technic may be unable to detect allof the TGA activity. Furthermore, the Biggs-Douglas test is carried out with the adsorbedplasma diluted only fivefold, so that the normalendpoint is reached in 2 or 3 minutes. In theDuckert modification (11) of the TGT, plasma isadsorbed with barium sulfate and is then diluted25-fold. TGA is not adsorbed and excessiveamounts may be detected because slight accelera-tion over the normal reaction rate may be per-ceptible. In our experience, an even greaterdilution of the plasma ( 1: 50) is needed to recog-nize accelerated thromboplastin generation un-
equivocally.To date, our studies have been carried out
largely in patients with arteriosclerosis obliteransor idiopathic thrombophlebitis. Because of thenature of our selection of patients, excess TGA
1016

THROMBOPLASTINGENERATIONACCELERATOR
TABLE XV
Distinguishing properties of TGA
Present in:*Effect of
BaSO4- Al (OH) 3- Lability coumarinadsorbed adsorbed at 560 C, Electrophoretic drug
Coagulation factor Plasma plasma plasma Serum gradet localization therapy:
TGA + + 0 0 2 d 0AHG + + + 0 3 0l °FactorV + + + 0 4 A-e (14) 0PTC (IX) + 0 0 + 1 (3(19) +Factor VII + 0 0 + 1 d3(14) +Factor X + 0 0 + 3 (27) a (26) +Prothrombin + 0 0 0 a 2 (14) +PTA + + + + 1(28) #-y(I7) 0Hageman factor + + + + 1 (28) al (16) 0Fibrinogen + + + 0 Point of
appl. (14) 0Platelets + 0 0 0 Point of appl. 0
* Key: + = present; 0 = absent.t Graded on a basis of 0 to 4, 0 representing nonlability, and 4 greatest lability.I Key: + = depressed; 0 = no depression.
activity was usually found to be associated withrecent thrombosis. Before it is concluded that theexcess TGA activity is simply the result of thethrombosis, it may be recalled that normal plasmaexhibits a modest coagulative activity in the,8-globulin zone indistinguishable from TGA.Furthermore, in one patient studied serially for 3years and in whom there was no further clinicalevidence of thrombosis, excess TGA activity per-sisted unaltered. It should be stated that in onepatient the excess TGA activity disappearedwithin 3 weeks.
Additional evidence that TGA is not prothrom-bin, or factor VII, IX or X, all of which tend tobe depressed by coumarin-type therapy, is the factthat excess TGA activity is unaltered by suchtherapy. Since thrombi tend to disappear duringanticoagulant therapy, the persistence of excessTGA activity again raises the question of any di-rect relationship between excessive TGA andthrombosis. The distinguishing properties ofTGA are summarized in Table XV.
Deficiency of TGA. As with all of the otherknown coagulation factors, it is to be expectedthat deficiency states of TGA will be discovered.Unfortunately, it is not possible to distinguish adeficiency of TGA from a deficiency of AHGbyany currently available TGT. Deficiency of eitherTGAor AHGis to be suspected when the genera-tion of thromboplastin from the patient's plasmais limited, but is normal from the patient's serum.Deficiency of AHGcould be distinguished from
that of TGA by adding aluminum hydroxide-ad-sorbed normal plasma to the TGT, since this wouldcontain AHGbut not TGA; if such a mixtureshould lead to a normal generation of thrombo-plastin, deficiency of AHGwould be confirmed.Since such a distinction has not been made in thepast, it is possible that certain patients believed tohave "classic hemophilia" may indeed suffer fromdeficiency of TGA. Perhaps with a differentiatingtest available, a re-evaluation of women with ap-parent AHGdeficiency, as in vascular hemophiliaor thrombasthenic hemophilia (12), should be car-ried out.
SUMMARY
Wehave described a new component of the co-
agulation mechanism. This substance, which wehave named thromboplastin generation accelerator,or TGA, appears to be responsible for the acceler-ated formation of plasma thromboplastin observedin certain patients with intravascular thrombosis.It is a moderately heat-labile protein associatedwith the 8-globulins. It is present in fresh plasmabut not in serum. Its site of action seems to bethe initial stage of clotting, where it appears to in-fluience primarily the rate of formation, and pos-sibly the yield, of plasma thromboplastin. It is un-
affected by therapy with coumarin drugs.
REFERENCES
1. Mustard, J. F. Blood coagulation in subjects withand without clinical evidence of atheroscleroticvessel disease. Canad. med. Ass. J. 1958, 79,554.
1017

PASCUZZI, SPITTEL, THOMPSONAND OWEN
2. Sharnoff, J. G. Increased pulmonary megakaryocytes-probable role in postoperative thromboembolism.J. Amer. med. Ass. 1959, 169, 688.
3. McDonald, L., and Edgill, M. Changes in coagu-lability of the blood during various phases ofischaemic heart-disease. Lancet 1959, 1, 1115.
4. Wessler, S., and Reimer, S. M. The role of humancoagulation factors in serum-induced thrombosis.J. clin. Invest. 1960, 39, 262.
5. Owen, C. A., Jr., and Thompson, J. H., Jr. Throm-bosis from the viewpoint of a blood coagulationistin Pathogenesis and Treatment of Cerebrovascu-lar Disease, W. S. Fields, Ed. Springfield, Ill.,Charles C Thomas, 1961, pp. 105-125.
6. Spittel, J. A., Jr., Pascuzzi, C. A., Thompson, J. H.,Jr., and Owen, C. A., Jr. Acceleration of earlystages of coagulation in certain patients with oc-clusive arterial or venous diseases: Use of a modi-fied thromboplastin generation test to evaluateclot acceleration. Proc. Mayo Clin. 1960, 35, 37.
7. Quick, A. J. On the quantitative estimation of pro-thrombin. Amer. J. clin. Path. 1945, 15, 560.
8. Hurn, M., Barker, N. W., and Magath, T. B. Thedetermination of prothrombin time following theadministration of Dicumarol, 3,3'-methylenebis(4-hydroxycoumarin), with special reference tothromboplastin. J. Lab. clin. Med. 1945, 30, 432.
9. Owen, C. A., Jr., Mann, F. D., Hurn, M. M., andStickney, J. M. Evaluation of disorders of bloodcoagulation in the clinical laboratory. Amer. J.clin. Path. 1955, 25, 1417.
10. Biggs, R., and Douglas, A. S. The thromboplastingeneration test. J. clin. Path. 1953, 6, 23.
11. Duckert, F., Flfickiger, P., Isenschmid, H., Matter,M., Vogel-Meng, J., and Koller, F. A modifica-tion of the thromboplastin generation test: Roleof calcium, factor V and factor VII in prothrombinconversion initiated by active blood thrombo-plastin. Acta haemat. (Basel) 1954, 12, 197.
12. Owen, C. A., Jr., and Thompson, J. H., Jr. Soy-bean phosphatides in prothrombin-consumption andthlronmboplastin-generation tests: Their use inrecognizing "thrombasthenic hemophilia." Amer.J. clin. Path. 1960, 33, 197.
13. Mertz, E. T., and Owen, C. A. Imidazole buffer:Its use in blood clotting studies. Proc. Soc.exp. Biol. (N. Y.) 1940, 43, 204.
14. Owen, C. A., Jr., and McKenzie, B. F. Applicationof paper electrophoresis to separation of blood-clotting factors. J. appl. Physiol. 1954, 6, 696.
15. Lewis, J. H., Walters, D., Didisheim, P., and M.er-
chant, W. R. Application of continuous flow elec-trophoresis to the study of the blood coagulationproteins and the fibrinolytic enzyme system. 1.Normal human materials. J. clin. Invest. 1958, 37,1323.
16. Thompson, J. H., Jr., Spittel, J. A., Jr., Pascuzzi,C. A., and Owen, C. A., Jr. Laboratory andgenetic observations in another family with theHageman trait. Proc. Mayo Clin. 1960, 35, 421.
17. Rosenthal, R. L. Properties of plasma thrombo-plastin antecedent (PTA) in relation to bloodcoagulation. J. Lab. clin. Med. 1955, 45, 123.
18. Spittel, J. A., Jr., Pascuzzi, C. A., Thompson, J. H.,Jr., and Owen, C. A., Jr. Accelerated thrombo-plastin generation in patients with acute periph-eral arterial occlusion complicating arteriosclero-sis obliterans. Unpublished data.
19. Aggeler, P. M., Spaet, T. H., and Emery, B. E.Purification of plasma thromboplastin factor B(plasma thromboplastin component) and its iden-tification as a beta. globulin. Science 1954, 119,806.
20. Loeliger, A., and Koller, F. Behaviour of factor VIIand prothrombin in late pregnancy and in thenewborn. Acta haemat. (Basel) 1952, 7, 157.
21. Forwell, G. D., and Ingram, G. I. C. The effect ofadrenaline infusion on human blood coagulation.J. Physiol. (Lond.) 1957, 135, 371.
22. Pitney, W. R., and Elliott, M. H. Plasma anti-haemophilic-factor concentrations in the Australianaborigine and in conditions associated with hyper-globulinaemia. Nature (Lond.) 1960, 185, 397.
23. Reimer, S. M., Wessler, S., and Deykin, D. Serumthrombotic accelerator (STA) activity: Its rela-tion to the first phase of clotting. Proc. Soc. exp.Biol. (N. Y.) 1960, 105, 438.
24. Fisch, U. Uber einen neuen Accelerator der Blut-thrombokinasebildung. Thromb. Diath. haemor.1958, 2, 60.
25. Waaler, B. A. Contact activation in the intrinsicblood clotting system. Scand. J. clin. Lab. Invest.1959, 11, suppl. 37.
26. Duckert, F. On the properties of the Stuart-Prower factor in New Blood Clotting Factors,I. S. Wright, F. Koller and F. Streuli, Eds. Stutt-gart, Friedrich-Karl Schattauer-Verlag, 1959, pp.32-36.
27. Graham, J. B. Stuart clotting defect and Stuartfactor. Ibid., pp. 22-31.
28. Soulier, J. P. Our present knowledge on PTA fac-tor. Ibid., pp. 123-131.
1018