Thrombolysis in acute pulmonary embolism - · PDF fileThrombolysis in acute pulmonary embolism...
42
Thrombolysis in acute pulmonary embolism Dr James Edwards Royal Prince Alfred Hospital Evidence Review in Emergency Medicine Wollongong March 3 rd 2016 Ma E
Transcript of Thrombolysis in acute pulmonary embolism - · PDF fileThrombolysis in acute pulmonary embolism...
Thrombolysis in acute pulmonary embolism
Dr James Edwards Royal Prince Alfred Hospital
Evidence Review in Emergency Medicine Wollongong March 3rd 2016 Ma
E
Case
A 66 yo male, previous well presents with SOB and pleuritic chest pain. Noted to have mild hypoxia, HR
110 and BP 100/70. Hs Troponin 30
CTPA shows a large saddle embolus. Bedside echo shows mod RV dilatation.
Management
a) Heparin b) Heparin and thrombolysis
c) Embolectomy d) Novel oral anticoagulant
e) Catheter directed fragmentation and/or thrombolysis
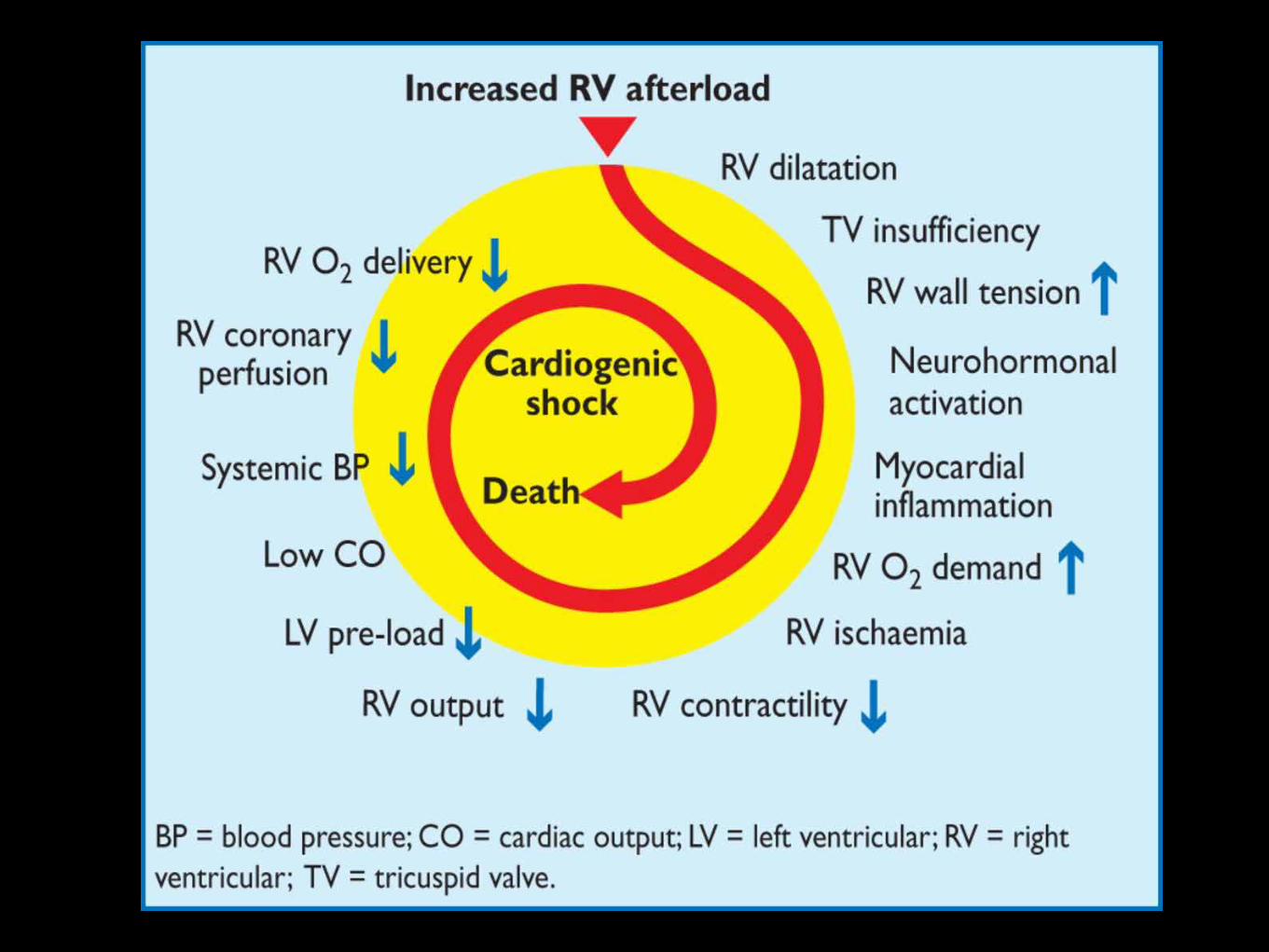
Pathophysiology

Rationale
Thrombolysis vs anticoagulation

Balance of risks
Bleeding
Recurrent PE
Death
Pulmonary hypertension
Risk stratification
High risk Low Intermediate
sPESI score age > 80
history of cancer chronic cardiac or lung disease
HR >110 BP< 100 Sa02 <90
High risk (massive) PE
thrombolyse if shocked bedside echo if very unstable to rule in
no thrombolysis for undifferentiated shock
Intermediate risk (sub-massive) PE
Not shocked but presence of RV dysfunction
Does thrombolysis reduce mortality in intermediate
risk PE?
Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage. A Meta- analysis Chatterjee S et al.
JAMA. 2014 Jun 18;311(23):2414-21
16 trials 2115 patients
mortality benefit with thrombolytics (2.17% vs 3.89%)
NNT 59
increase in major bleeding with thrombolytics (9.24% vs 3.42%) NNH 11
increase in ICH with thrombolytics (1.46% vs 0.19%)
NNH 78
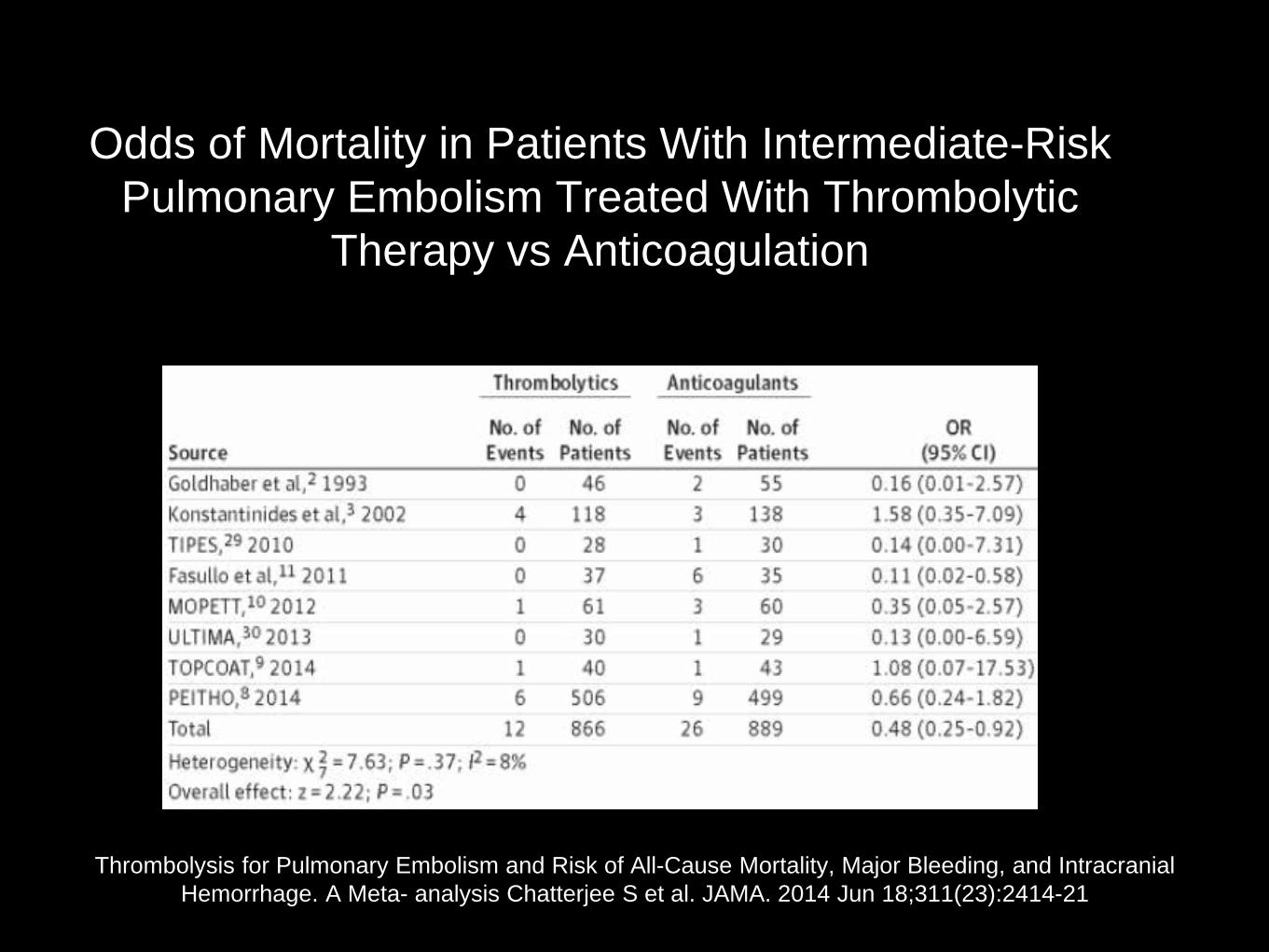
Odds of Mortality in Patients With Intermediate-Risk Pulmonary Embolism Treated With Thrombolytic
Therapy vs Anticoagulation
Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage. A Meta- analysis Chatterjee S et al. JAMA. 2014 Jun 18;311(23):2414-21
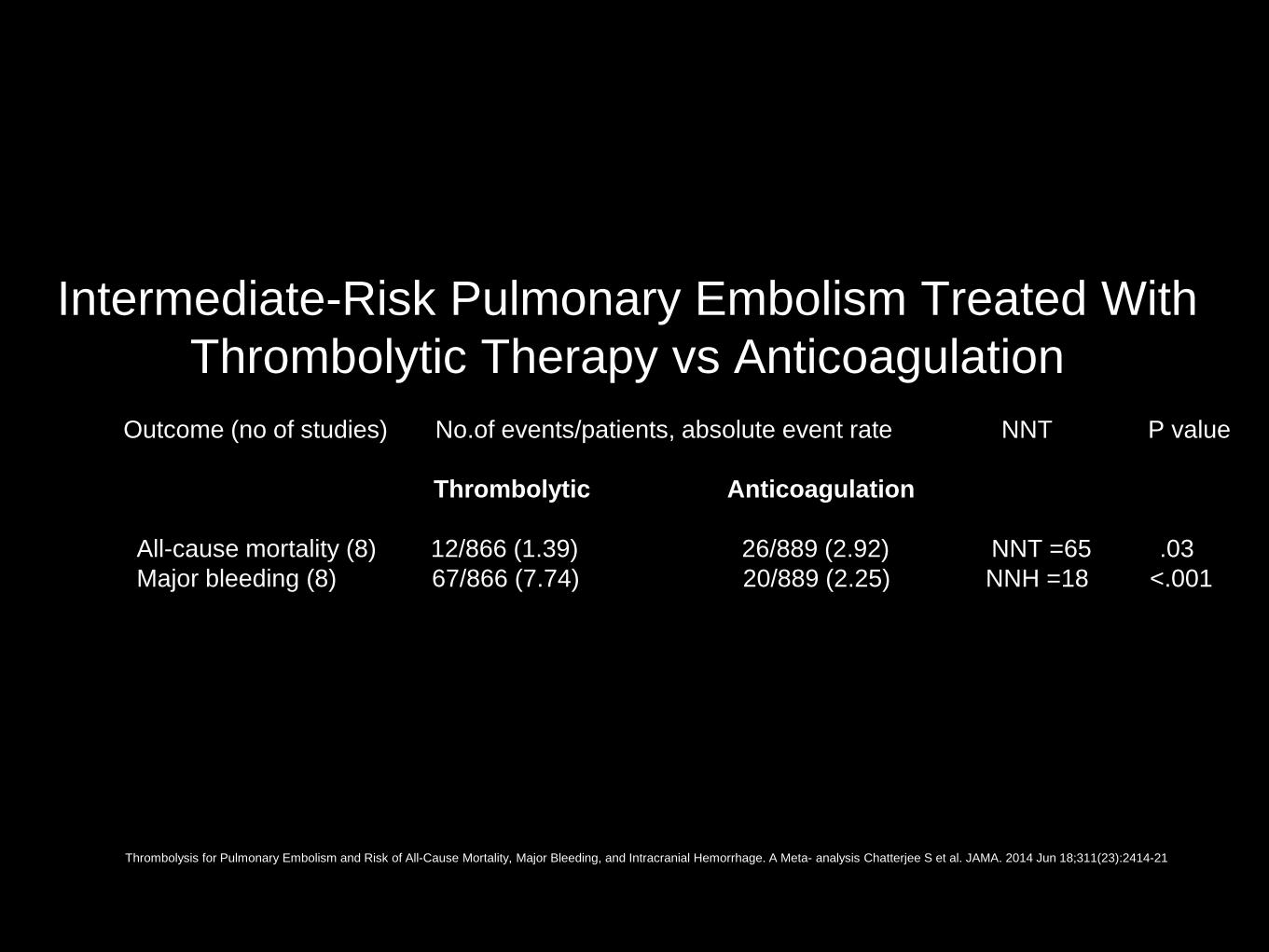
Intermediate-Risk Pulmonary Embolism Treated With Thrombolytic Therapy vs Anticoagulation
Outcome (no of studies) No.of events/patients, absolute event rate NNT P value
Thrombolytic Anticoagulation
All-cause mortality (8) 12/866 (1.39) 26/889 (2.92) NNT =65 .03 Major bleeding (8) 67/866 (7.74) 20/889 (2.25) NNH =18 <.001
Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage. A Meta- analysis Chatterjee S et al. JAMA. 2014 Jun 18;311(23):2414-21
Impact of the efficacy of thrombolytic therapy on the mortality of patients with acute submassive
pulmonary embolism: a meta-analysis. Nakamura et al. J Thromb Haemost. 2014 Jul;12(7):1086-95
6 studies 1510 patients
no significant differences were found in all-cause death between the thrombolytic and heparin (2.3% vs. 3.7%)
30 day mortality 3%
Impact of the efficacy of thrombolytic therapy on the mortality of patients with acute submassive pulmonary embolism: a meta-analysis. Nakamura et al. J Thromb Haemost. 2014 Jul;12(7):1086-95
PEITHO study
Fibrinolysis for patients with intermediate-risk pulmonary embolism. Meyer G, et al. The New England Journal of
Medicine. 2014. 370(15):1402-1411
PEITHO
Double blind, RCT
76 centres/13 countries
Intermediate risk PE (RV dysfunction and trop rise)
N= 1005
tenecteplase (weight based) plus heparin (n=506) placebo plus heparin (n= 499)
Fibrinolysis for patients with intermediate-risk pulmonary embolism. Meyer G, et al. The New England Journal of Medicine. 2014. 370(15):1402-1411
Outcomes
Primary
All-cause mortality or haemodynamic decompensation at 7 days
Tenecteplase 2.6% vs. placebo 5.6% (OR 0.44; 95% CI 0.23-0.87; P=0.02; NNT 33)
All-cause mortality
At 7 days: tenecteplase 1.2% vs. placebo 1.8%
(OR 0.65; 95% CI 0.23-1.85; P=0.42)
At 30 days: tenecteplase 2.4% vs. placebo 3.2% (OR 0.73; 95% CI 0.34-1.57; P=0.42)
Fibrinolysis for patients with intermediate-risk pulmonary embolism. Meyer G, et al. The New England Journal of Medicine. 2014. 370(15):1402-1411
Bleeding risk
Extracranial bleeding occurred in 32 patients (6.3%) in the tenecteplase group and 6 patients (1.2%) in the placebo
group (P<0.001)
Stroke occurred in 12 patients (2.4%) in the tenecteplase group and was haemorrhagic in 10 patients; 1 patient (0.2%) in the placebo group had a stroke, which was
hemorrhagic (P=0.003).
Fibrinolysis for patients with intermediate-risk pulmonary embolism. Meyer G, et al. The New England Journal of Medicine. 2014. 370(15):1402-1411
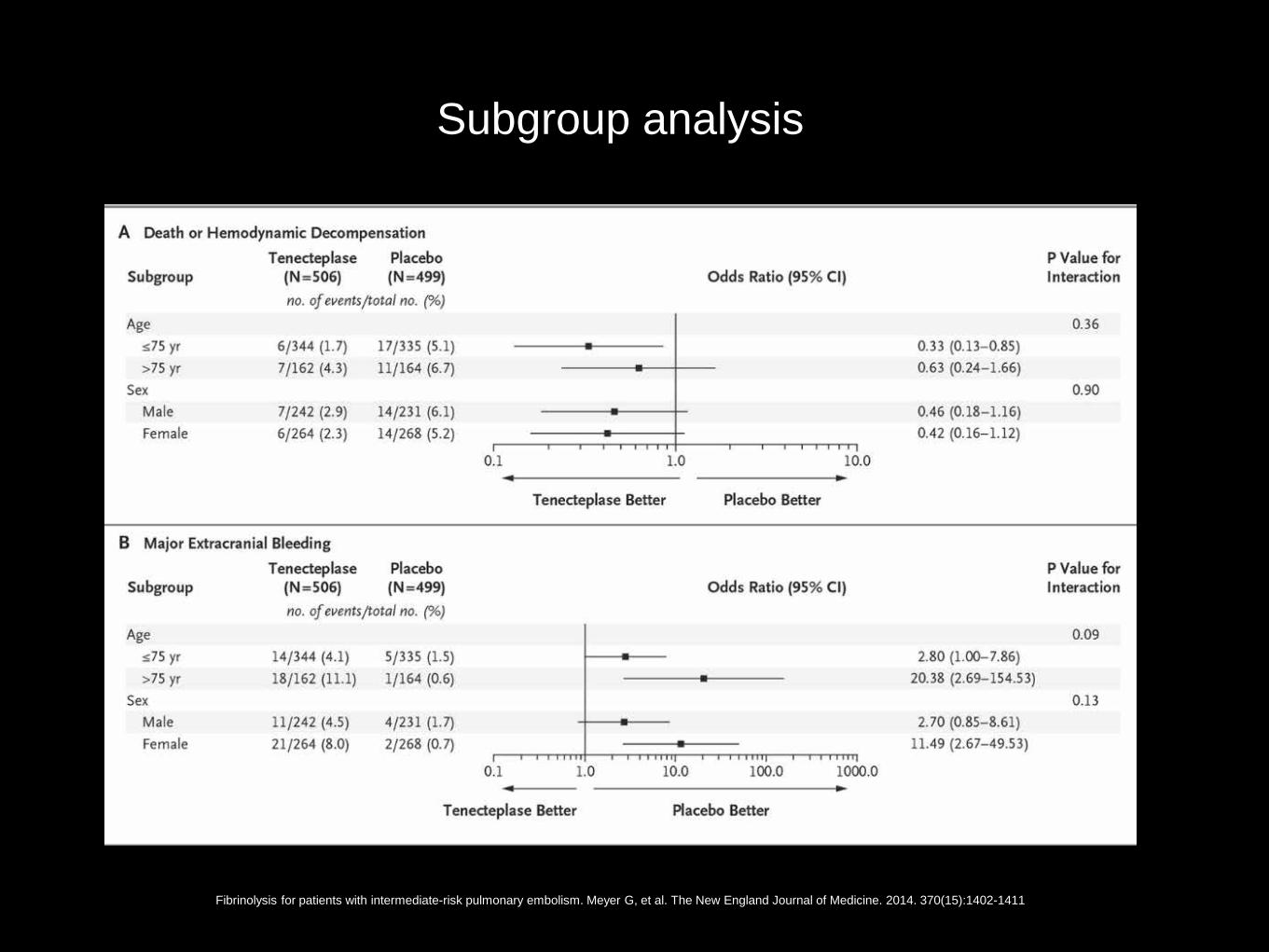
Subgroup analysis
Fibrinolysis for patients with intermediate-risk pulmonary embolism. Meyer G, et al. The New England Journal of Medicine. 2014. 370(15):1402-1411
Take home messages from PEITHO
No short term mortality benefit
Significant bleeding risk with thrombolysis especially age >75

TOPCOAT
Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3
months: multicenter double-blind, placebo- controlled randomized trial. Kline J. et al.. J Thromb Haemost. 2014.
12(4):459-468
TOPCOAT trial
multicentre, RCT83 pat 83 patients
placebo vs tenecteplase intermediate risk as determined by echo/biomarkers
LMWH rather than unfractionated in placebo
Primary outcome
Composite adverse outcome
Within 5 days PE related -death, haemodynamic compromise
Treatment complication
At 90 days pulmonary hypertension, poor quality of life, exercise intolerance
Improvement in tenecteplase group vs placebo
15% vs. 37% had at least 1 adverse outcome (P=0.017, NNT 5)

Take Home message
complicated composite outcome Is an improvement in self reported exercise
tolerance enough of a reason to give thrombolytics? Probably not
What dose of thrombolytic?
MOPETT study
Moderate pulmonary embolism treated with thrombolysis.
Sharifi M. Am J Cardiol. 2013 Jan 15;111(2):273-7
MOPETT trial
Single centre study, RCT Low dose thrombolysis n=61 and heparin n= 60
Alteplase 0.5mg/kg (max 50mg) with 10mg bolus and then
rest over 2 hour
Moderate (?Intermediate) risk
>70% involvement of thrombus in ≥ 2 lobar or either the left or right main pulmonary arteries
High probability V/Q scan with V/Q mismatch in ≥2 lobes
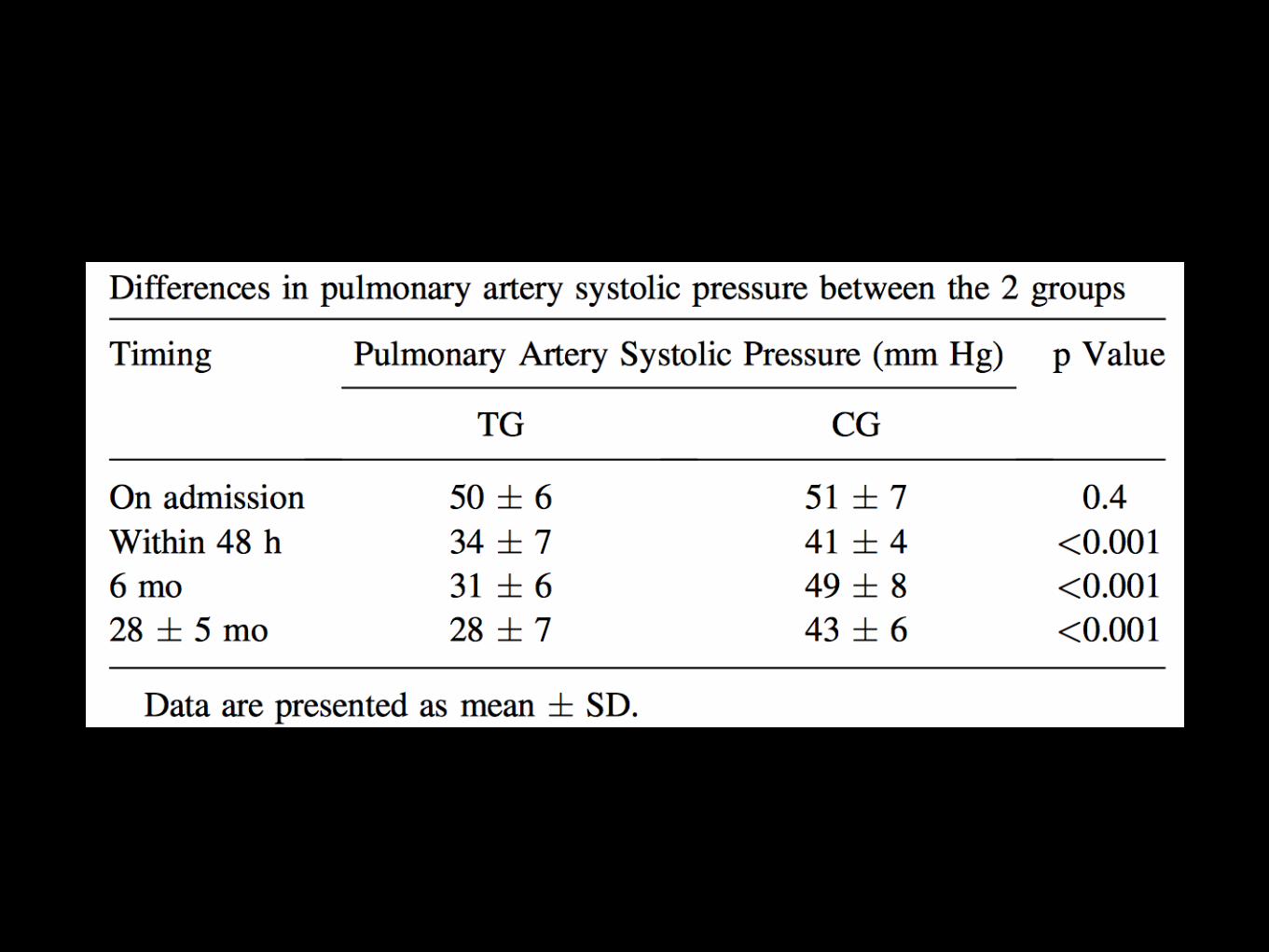
Primary outcomes
Pulmonary hypertension at 28 months thrombolysis16% (9/58) vs. heparin 57% (32/56)
(P<0.001; NNT 2)
Pulmonary hypertension or recurrent PE at 28 months tthrombolysis 16% (9/58) vs. heparin 63% (35/56)
(P<0.001; NNT 2)

Secondary outcomes
No difference in mortality No bleeding occurred in either group!
Take Home messages
Thrombolysis reduces the pulmonary arterial systolic pressure and this persisted for 2
years but is it clinically significant?
Less bleeding than other studies ? safer dose
PERFECT trial
Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis
(PERFECT): Initial Results From a Prospective Multicenter Registry Chest. 2015;148(3):667-673
PERFECT Trial
multi-centre registry of 101 consecutive patients
not randomised
high (n=28) and intermediate (n=73) risk
low dose tPA or urokinase for intermediate risk
high risk PE were treated with catheter-directed mechanical or pharmacomechanical thrombectomy
Outcomes
6/101 deaths (4/28 high and 2/73 intermediate risk)
no major procedure-related complications,
major haemorrhages, or strokes
8/9 patients with absolute contraindications to systemic tPA survived
The future?
A 46 yo male, previous well presents with SOB and pleuritic chest pain. Noted to have mild hypoxia, HR 110
and BP 100/70. Hs Troponin 30
CTPA shows a large saddle embolus. Bedside echo shows mod RV dilatation.
Management a) Heparin
b) Heparin and thrombolysis c) Embolectomy
d) Novel oral anticoagulant e) Catheter directed fragmentation and/or thrombolysis

A 76 yo male, previous well presents with SOB and pleuritic chest pain. Noted to have mild hypoxia, HR 110
and BP 100/70. Hs Troponin 30
CTPA shows a large saddle embolus. Bedside echo shows mod RV dilatation.
Management a) Heparin
b) Heparin and thrombolysis c) Embolectomy
d) Novel oral anticoagulant e) Catheter directed fragmentation and/or thrombolysis
A 66 yo male, previous well presents with SOB and pleuritic chest pain. Noted to have mild hypoxia, HR 110
and BP 100/70. Hs Troponin 30
CTPA shows a large saddle embolus. Bedside echo shows mod RV dilatation.
Management a) Heparin
b) Heparin and thrombolysis c) Embolectomy
d) Novel oral anticoagulant e) Catheter directed fragmentation and/or thrombolysis
Take home messages
PE risk is a spectrum
In regards to thrombolysis in intermediate PE;
Age over 75, the risks probably outweigh the benefits
Under 75 (especially under 65), thrombolysis should be
considered within the context of bleeding risk
Ideal dose and role for catheter directed thrombolysis not clear
Shared decision making process with your colleagues (respiratory, haematology, ICU) and the patient prior to
decision to thrombolyse















![Acute Pulmonary Embolism [Radiology North Amer Clinics 2010]](https://static.fdocuments.us/doc/165x107/577d35bd1a28ab3a6b91457c/acute-pulmonary-embolism-radiology-north-amer-clinics-2010.jpg)