Thromboelastography and Thromboelastometry in Assessment ...
24
Review Article Thromboelastography and Thromboelastometry in Assessment of Fibrinogen Deficiency and Prediction for Transfusion Requirement: A Descriptive Review Henry T. Peng , 1,2 Bartolomeu Nascimento, 3 and Andrew Beckett 4 1 Defence Research and Development Canada, Toronto Research Centre, Toronto, Ontario, Canada 2 Research Institute of Xi’an Jiaotong University, Hangzhou, Zhejiang, China 3 Sunnybrook Health Sciences Centre, Department of Surgery, University of Toronto, Toronto, Canada 4 Royal Canadian Medical Services, Ottawa, Ontario, and McGill University, Montreal, Quebec, Canada Correspondence should be addressed to Henry T. Peng; [email protected] Received 28 May 2018; Revised 28 September 2018; Accepted 6 November 2018; Published 25 November 2018 Academic Editor: Franc ¸ois Berthiaume Copyright © 2018 Henry T. Peng et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Fibrinogen is crucial for the formation of blood clot and clinical outcomes in major bleeding. Both romboelastography (TEG) and Rotational romboelastometry (ROTEM) have been increasingly used to diagnose fibrinogen deficiency and guide fibrinogen transfusion in trauma and surgical bleeding patients. We conducted a comprehensive and comparative review on the technologies and clinical applications of two typical functional fibrinogen assays using TEG (FF TEG) and ROTEM (FIBTEM) for assessment of fibrinogen level and deficiency, and prediction of transfusion requirement. Clot strength and firmness of FF TEG and ROTEM FIBTEM were the most used parameters, and their associations with fibrinogen levels as measured by Clauss method ranged from 0 to 0.9 for FF TEG and 0.27 to 0.94 for FIBTEM. A comparison of the interchangeability and clinical performance of the functional fibrinogen assays using the two systems showed that the results were correlated, but are not interchangeable between the two systems. It appears that ROTEM FIBTEM showed better associations with the Clauss method and more clinical use for monitoring fibrinogen deficiency and predicting transfusion requirements including fibrinogen replacement than FF TEG. TEG and ROTEM functional fibrinogen tests play important roles in the diagnosis of fibrinogen-related coagulopathy and guidance of transfusion requirements. Despite the fact that high-quality evidence is still needed, the two systems are likely to remain popular for the hemostatic management of bleeding patients. 1. Introduction Fibrinogen is perhaps the most important protein in hemostasis, as the final stage of the coagulation cascade is converted to fibrin by thrombin and cross-linked by factor XIII. It also induces platelet activation and aggregation via binding to glycoprotein IIb/IIIa receptors on the surface of platelets, acting as the bridge for stable clot formation [1]. During major bleeding, fibrinogen is the first clotting factor to reach critically low levels below the normal physiological level of around 2 to 4 g/L, which is associated with increased bleeding, coagulopathy, and in turn worsened clinical out- comes [2–5]. Fibrinogen is an independent predictor of mortality in major trauma patients [6]. romboelastography (TEG; Haemonetics Corporation, Haemoscope Division, Nile, Illinois, USA) and Rotational romboelastometry (ROTEM; Tem Innovations GmbH, Munich, Germany; succeeded by Instrumentation Labora- tory, Bedford, MA, USA) are two point-of-care systems for hemostatic tests in whole blood [7]. Both have been increas- ingly used to diagnose fibrinogen deficiency [8], predict risk of bleeding and mortality, and guide fibrinogen transfusion in trauma [9], cardiac surgery [10], liver transplantation [11], and postpartum bleeding [12]. TEG- and ROTEM- based algorithms have been widely used to direct fibrinogen administration in different settings leading to reduction in transfusion needs, costs, adverse outcomes, and even mortality [13–16] although a recent review indicated that the
Transcript of Thromboelastography and Thromboelastometry in Assessment ...

Review ArticleThromboelastography and Thromboelastometry inAssessment of Fibrinogen Deficiency and Prediction forTransfusion Requirement: A Descriptive Review
Henry T. Peng ,1,2 Bartolomeu Nascimento,3 and Andrew Beckett4
1Defence Research and Development Canada, Toronto Research Centre, Toronto, Ontario, Canada2Research Institute of Xi’an Jiaotong University, Hangzhou, Zhejiang, China3Sunnybrook Health Sciences Centre, Department of Surgery, University of Toronto, Toronto, Canada4Royal Canadian Medical Services, Ottawa, Ontario, and McGill University, Montreal, Quebec, Canada
Correspondence should be addressed to Henry T. Peng; [email protected]
Received 28 May 2018; Revised 28 September 2018; Accepted 6 November 2018; Published 25 November 2018
Academic Editor: Francois Berthiaume
Copyright © 2018 Henry T. Peng et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Fibrinogen is crucial for the formation of blood clot and clinical outcomes in major bleeding. Both Thromboelastography (TEG)and RotationalThromboelastometry (ROTEM) have been increasingly used to diagnose fibrinogen deficiency and guide fibrinogentransfusion in trauma and surgical bleeding patients. We conducted a comprehensive and comparative review on the technologiesand clinical applications of two typical functional fibrinogen assays using TEG (FF TEG) and ROTEM (FIBTEM) for assessment offibrinogen level and deficiency, and prediction of transfusion requirement. Clot strength and firmness of FF TEG and ROTEMFIBTEM were the most used parameters, and their associations with fibrinogen levels as measured by Clauss method rangedfrom 0 to 0.9 for FF TEG and 0.27 to 0.94 for FIBTEM. A comparison of the interchangeability and clinical performance of thefunctional fibrinogen assays using the two systems showed that the results were correlated, but are not interchangeable betweenthe two systems. It appears that ROTEM FIBTEM showed better associations with the Clauss method and more clinical use formonitoring fibrinogen deficiency and predicting transfusion requirements including fibrinogen replacement than FF TEG. TEGand ROTEM functional fibrinogen tests play important roles in the diagnosis of fibrinogen-related coagulopathy and guidance oftransfusion requirements. Despite the fact that high-quality evidence is still needed, the two systems are likely to remain popularfor the hemostatic management of bleeding patients.
1. Introduction
Fibrinogen is perhaps the most important protein inhemostasis, as the final stage of the coagulation cascade isconverted to fibrin by thrombin and cross-linked by factorXIII. It also induces platelet activation and aggregation viabinding to glycoprotein IIb/IIIa receptors on the surface ofplatelets, acting as the bridge for stable clot formation [1].During major bleeding, fibrinogen is the first clotting factorto reach critically low levels below the normal physiologicallevel of around 2 to 4 g/L, which is associated with increasedbleeding, coagulopathy, and in turn worsened clinical out-comes [2–5]. Fibrinogen is an independent predictor ofmortality in major trauma patients [6].
Thromboelastography (TEG; Haemonetics Corporation,Haemoscope Division, Nile, Illinois, USA) and RotationalThromboelastometry (ROTEM; Tem Innovations GmbH,Munich, Germany; succeeded by Instrumentation Labora-tory, Bedford, MA, USA) are two point-of-care systems forhemostatic tests in whole blood [7]. Both have been increas-ingly used to diagnose fibrinogen deficiency [8], predict riskof bleeding and mortality, and guide fibrinogen transfusionin trauma [9], cardiac surgery [10], liver transplantation[11], and postpartum bleeding [12]. TEG- and ROTEM-based algorithms have been widely used to direct fibrinogenadministration in different settings leading to reductionin transfusion needs, costs, adverse outcomes, and evenmortality [13–16] although a recent review indicated that the

2 BioMed Research International
benefit of reduced blood products (red blood cells, freshfrozen plasma, and platelet) and improved morbidity inbleeding patients with the application of TEG- or ROTEM-guided transfusion strategies were primarily based on tri-als of elective cardiac surgery involving cardiopulmonarybypass, with low-quality evidence [17]. Similarly, a systematicreview and meta-analysis of the use of TEG and ROTEM ingoal-directing treatment with allogeneic blood products inbleeding patients found that the amount of transfused redblood cells, fresh frozen plasma, and bleeding volume wasreduced in the TEG- or ROTEM-guided groups compared tothe control groups either treated at the clinician’s discretionor based on conventional coagulation tests (CCTs), whereasthere were no differences in platelet transfusion andmortality[18]. Furthermore, a randomized clinical trial has concludedthat TEG-guided massive transfusion protocol for severetrauma improved survival compared with that guided byCCTs (i.e., prothrombin time [PT]/international normalizedratio [INR], fibrinogen, and D-dimer) and utilized lessplasma and platelet transfusion during the early phase ofresuscitation [19].
Nevertheless, another recent review on routine use ofviscoelastic blood tests for diagnosis and treatment of coag-ulopathic bleeding concluded that TEG and ROTEM testsonly reduced red blood cells and platelet transfusion in adultsundergoing cardiac surgery [20]. Meta-analyses across allindications (trauma, cardiac surgery, and liver transplan-tation) have shown that TEG and ROTEM tests are cost-saving and more effective than standard laboratory tests intrauma patients and patients undergoing cardiac surgery [21].Moreover, studies, including ours, have shown that TEG andROTEM provide different results for diagnosing coagulopa-thy and guiding transfusion [22–24]. Further evaluation ofTEG- or ROTEM-guided transfusion in prospective case-matched studies and different patient categories with low riskof bias is needed. Alternatively, TEG and ROTM have alsobeen used to study the effects of fibrinogen supplementationon hemostasis in an in vitromodel of dilutional coagulopathy[25], the correction of dilutional coagulopathy by fibrinogenconcentrate in orthopedic patients [26], and hypothermiccoagulopathy [27] as well as in patient blood [28].
Although the role of TEG and ROTEM in diagnosisof coagulopathy, prediction of transfusion and mortality inbleeding patients has been reviewed [12, 29]. This paperis focused on the studies on TEG and ROTEM functionalfibrinogen tests: FF TEG and ROTEM FIBTEM for the diag-nosis of fibrinogen deficiency and prediction of transfusionrequirements in bleeding patients. A follow-up paper will befocused on the use of FF TEG and ROTEM FIBTEM to guidefibrinogen replacement and monitor its hemostatic effects.
The paper is structured into four major sections. Thefirst session describes the principles of the two systems andvarious commercially available tests with an emphasis onfunctional fibrinogen tests. The second session reviews theuse of TEG and ROTEM for measurement of functional fib-rinogen levels in relation to fibrinogen concentration assays.The third session discusses the diagnosis of fibrinogen relatedcoagulopathy and prediction of transfusion requirements indifferent clinical settings. Finally, the review compares the
two systems in terms of reagents, parameter values, andclinical uses.
2. Principles of TEG and ROTEM FunctionalFibrinogen Tests
TEG 5000 (Haemonetics Corporation, Haemoscope Divi-sion, Niles, IL, USA) and ROTEM delta (InstrumentationLaboratory, Bedford, MA, USA) are the most used vis-coelastic hemostasis analyzers. Both systems measure theviscoelastic properties of blood as it clots under low shearstress based on pin-and-cup technology, but there are pri-mary hardware differences between the two [68]. The TEGanalyzer has a pin suspended by a torsion wire, wherein acup oscillates through 4.75 degree/5 seconds. In contrast, theROTEM analyzer has an immobile cup, wherein a pin/wiretransduction systemoscillates through 4.75 degree/6 seconds.It has been suggested that the ROTEM system uses a ball-bearing system for power transduction, which makes itless susceptible to movement and vibration [69] and thatthe automatic pipetting may ensure less variations amongoperations [70].
In addition to the differences in instrument, the twoviscoelastic point-of-care systems used different reagents forvarious tests and applications [68]. Specifically, the functionalfibrinogen reagent for TEG is composed of lyophilized tissuefactor and a platelet inhibitor (abciximab) that binds toglycoprotein IIb/IIIa receptors to inhibit platelet aggregationand exclude the platelet contribution to clot strength [71].However, it could contain kaolin or celite instead of tissuefactor [32, 43]. ROTEM fibrinogen assay uses two solutionscalled ex-tem andfib-tem [71].The ex-tem solution contains acombination of recombinant tissue factor and phospholipidsthat activates the extrinsic pathway of the coagulation system,while the fib-tem solution contains CaCl2 as a recalcificationreagent and a platelet inhibitor (cytochalasin D) that inhibitsactin/myosin-system. A new reagent called fib-tem pluscontains 2 platelet inhibitors, cytochalasin D, which inhibitsplatelet cytoskeletal reorganization, and tirofiban, which isa glycoprotein IIb/IIIa inhibitor similar to abciximab thatprevents fibrinogen from binding to glycoprotein IIb/IIIareceptors on the surface of platelets and platelet aggregation[48]. Furthermore, single portion reagents composed of alllyophilized reagents required for each ROTEM test have beendeveloped [72].
Although multiple parameters can bemeasured for bloodcoagulation and fibrinolysis, maximum amplitude MA inTEG and maximum clot strength MCF in ROTEM havebeen mostly used as a direct measure of fibrinogen functions.According to each manufacturer, the normal range of MAas measured by FF TEG using citrated blood is 11-24 mm(Guide to functional fibrinogen) and the normal range ofMCF as measured by ROTEM FIBTEM assay is 7-24 mm(Instructions for use of fib-tem). In addition, the clot firmnessat 5, 10, and 15 min after CT (A5, A10, and A15) has beenreported.
It should be noted that new and fully automated (nopipetting) TEG and ROTEM systems (TEG 6s and ROTEMsigma) are now commercially available. Both work with

BioMed Research International 3
4-channel cartridges based on different mechanisms. TEG6s uses a new technology called coagulation resonanceanalysis and works with two types of cartridges. One is aglobal hemostasis cartridge to perform four tests (kaolinTEG, kaolin TEG with heparinase, RapidTEG, and FF TEG)simultaneously and the other is a Platelet Mapping cartridgeto perform theTEGPlateMapping test (kaolinTEG, activatorF (ActF), adenosine diphosphate (ADP), and arachidonicacid (AA) [73, 74]. ROTEM sigma operates on the provenpin and cup technology as ROTEM delta, but uses two typesof cartridges containing lyophilized beads reagents insteadof liquid reagents for four tests per cartridge (cartridge 1:FIBTEM, EXTEM, INTEM, APTEM; cartridge 2: FIBTEM,EXTEM, INTEM, HEPTEM) [75].
3. Methods
A PubMed search was completed for the TEG and ROTEMstudies involving functional fibrinogen tests. The searchtermswere as follows: thrombelastogra∗ or thromboelastogra∗or TEG and fibrinogen, thromboelastomentr∗ orthrombelastromentr∗ or ROTEM and fibrinogen. Thespecific clinical use/interest of TEG and ROTEM (e.g.,trauma, cardiac surgery, transfusion, hypofibrinogenemia,hypo, and hyperfibrinolysis) was also used as keywords inthe search. Abstracts were used to determine the relevanceand when appropriate, further review of the original articleswas warranted. Additional publications were selected fromthe cross-references listed in the original papers and fromthe citing articles, and additional search was made throughMedline, Scopus, and Institute of Scientific Informationdatabases for those topicswith limited findings fromPubMed.The search was primarily focused on human studies.
We analyzed the correlations between functional fibrino-gen assays, i.e., Clauss method and FF TEG or ROTEMFIBTEM tests, and the accuracies (sensitivity, specificity, andarea under receiver operating characteristic (ROC) curve) ofFF TEG and ROTEM FIBTEM for the detection of hypofib-rinogenemia and prediction of bleeding and transfusion.Furthermore, data were extracted and pooled from differenttrials where FF TEG MA, ROTEM FIBTEM MCF versusplasma fibrinogen concentration data were reported. Linearregression with 95% confidence interval was then performedusing SigmaPlot Version 13.0 (Systat Software, Inc., San Jose,California, USA). We also calculated likelihood ratios of FFTEG and ROTEM FIBTEM for the diagnosis of hypofibrino-genemia defined as plasma fibrinogen level < 1.5 g/L usingthe following formula: sensitivity/(1-specificity) [76]. Meta-analysis of the clinical benefit of functional fibrinogen assaysusing TEG and ROTEM within their different uses could notbe conducted due to the small sample size and heterogeneityof studies.
4. Measurement of FibrinogenLevels and Functions
TEG has been used to study in vitro effects of fibrinogenon coagulation of plasma deficient in coagulation factors
and diluted by colloids [77, 78], and the effect of a car-diopulmonary bypass system with biocompatible coating onfibrinogen levels [38]. ROTEM has been used to determinethe usefulness of fibrinogen substitution to reverse dilutionalcoagulopathy in in vitro and in vivomodels [79–81]. All thesestudies showed that, to various extents, fibrinogen improvedclot strength (MA or MCF), clot formation (R or CT), andclot propagation (Alpha) as measured by TEG or ROTEM.
Clinical studies showed variable correlations betweenmaximum clot strength/firmness and fibrinogen levels assummarized in Table 1. The correlation coefficients rangefrom 0 (no significant correlation) [37] to 0.9 (strong cor-relation) [42] for FF TEG and 0.27 [3] to 0.94 [47] forROTEM FIBTEM. The correlations between A5, A10, or A15and fibrinogen levels have also been reported [34, 44, 45, 51,53, 57, 59]. These early values of clot firmness can providefast and reliable prediction of MCF to guide haemostatictherapy in severe bleeding [82]. Other ROTEM tests (e.g.,EXTEM) showed certain degrees of correlations with plasmafibrinogen concentrations as well [50, 55]. Both FF TEGand ROTEM FITBEM have been used in clinical settings oftrauma [30, 32–34, 46], cardiac surgery [36, 37, 39, 49, 52],liver transplantation [42, 54], and pregnancy [43, 59]with dif-ferent popularities. In addition, ROTEM FIBTEM has beenused for assessment of fibrinogen function in neurosurgery[60], burn injury [61], and cirrhosis [62].The variations in thecorrelations could be due to the differences in study popula-tion and range of fibrinogen concentrations as most TEG andROTEM tests were performed using TEG 5000 and ROTEMdelta with the same reagent and procedures as recommendedby their manufacturers. For example, one study reportedno significant correlations between either TEG functionalfibrinogen level (FLEV) or maximal amplitude (MA) andClauss fibrinogen level at baseline or 10min postprotamine incardiac surgery patients [37]. The different correlations werealso reported for children at different ages [40, 41].
Figure 1(a) shows the correlation between plasma fibrino-gen concentration measured by the Clauss method and FFTEG MA based on the data extracted from several studies.Overall correlation from pooled literature data was strong.Similarly, Figure 1(b) shows an overall strong correlationbetween the Clauss fibrinogen and FIBTEM MCF frompooled data extracted from the literature.
The Clauss assay is considered a standard functional testfor fibrinogen concentration by determination of the timein seconds to clot formation following addition of excessthrombin [83]. Other methods such as prothrombin time-derived method [56] and enzyme-linked immunosorbentassay (ELISA) [83] are also used. ELISAdoes not discriminatebetween functional and non-functional immunoreactive fib-rinogen protein, and even some degraded forms of fibrinogen[84].
The Clauss method is limited to only small concen-trations of heparin (which inactivates thrombin throughanti-thrombin III), which is a serious limitation in cardiacsurgery. It may be affected by fibrin degradation products,polymerization inhibitors as other inhibitors of fibrin for-mation [85]. Its turnaround time is approximately 40 min[86]. In comparison, TEG and ROTEM function fibrinogen

4 BioMed Research International
Table1:Summaryof
correlations
betweenfunctio
nalfi
brinogen
(FF)
TEG/ROTE
MFIBT
EMandfib
rinogen
levels.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
FFTE
G
Trauma
Arand
omized
controlledtrialoftraum
apatientsa
tris
kof
significanth
emorrhage(
n=45,ISS=18-29)
receivingeither
6gfib
rinogen
concentrate
(RiaSTAP�
)orp
lacebo
(normalsalin
e).C
itrated
who
lebloo
dwas
collected
from
ther
ando
mized
traumapatientsa
tadm
ission,
1-,3-,11-,
23-and
47-h
post-
infusio
ntim
e.
Standard
FFTE
Gwas
perfo
rmed
onac
ompu
teriz
edTE
GHem
ostasis
Syste
m5000
(Haemon
etics
Corpo
ratio
n,Haemoscope
Division
,Niles,IL,U
SA)
accordingto
manufacturer’s
protocol.Specifically,
500
𝜇Lof
theb
lood
samplew
aspipette
dinto
aFFvialwhich
contains
lyop
hilized
tissuefactorw
ithplateletinhibitor
(abcixim
ab)a
ndgentlymixed
byinversionfivetim
es,
andthen
340𝜇Lof
them
ixture
from
theFF
vialwas
addedinto
aTEG
cuppre-warmed
to37∘Ccontaining
20𝜇Lof
0.2M
calcium
chlorid
e.Plasmafib
rinogen
levelswe
remeasuredby
thes
tand
ardvonClauss
metho
d.
FFTE
GMAstr
onglycorrelated
with
Claussfib
rinogen
concentrationdeterm
ined
bySpearm
an’scorrelation(𝜌=0
.75,
p<0.00
1).FFTE
GK,A
lpha
show
edmod
eratec
orrelatio
nswith
fibrin
ogen
concentration(𝜌=-0.46
and0.40
,p<0.00
1),
whileTE
GFF
CL30
onlyshow
edwe
ekcorrelations
with
fibrin
ogen
concentration(𝜌=0
.21,p=
0.00
4).
[30,31]
Aprospectiveo
bservatio
nalstudy
oftraumapatients
(n=68),with
amedianISSof
23.5.C
itrated
who
le-blood
samples
were
obtained
from
the
patientso
narriv
alto
thee
mergencydepartmentand
with
inthefi
rst5
days
ofadmissionto
thes
urgical
intensivec
areu
nit.
TheF
Fandkaolin
TEGassays
were
perfo
rmed
onthe
TEG5000
device
inthetraum
aresearch
labo
ratory.Th
eFF
TEGassaymeasuresthe
FFlevel(FL
EV),which
isextrapolated
from
theM
Afib
rinogen
value.Plasma
fibrin
ogen
levelswe
remeasuredby
thesta
ndardvon
Claussmetho
d.
Sign
ificant
correlations
betweenTE
GFL
EVandClauss
fibrin
ogen
levels(R2=0.87,p<0.00
01)and
betweenTE
GFF
MAandClaussfib
rinogen
levels(R2=0.75,p<0.00
01).
Mod
erateinverse
correlationbetweenFL
EVandK(R2=0.35,
p<0.00
01),betweenFL
EVandalph
a(R2
=0.70,p<0.00
01).
[32]
Aprospectiveo
bservatio
nalstudy
of251critically
injuredtraumapatientsw
itham
edianISSof
9(1-19)
atas
ingleLevel1
traumac
enter.Citrated
who
lebloo
dwas
collected
from
thep
atientso
narriv
aland
at2,3,4,6,12,24,48,72,96,and
120haft
eradmission.
Forthe
kaolin
TEG,340𝜇Lkaolin-activated
bloo
dwas
transfe
rred
totheT
EGcup,pre-warmed
to37∘Cand
containing
20𝜇Lof
0.2M
CaC
l 2.For
theFF
TEG,500
𝜇Lof
citrated
bloo
dwas
addedto
theF
Fvial(kaolin
+glycop
rotein
IIb/IIIaantagonist)
andmixed;340𝜇Lwas
then
transfe
rred
totheTE
Gcup.Plasmafib
rinogen
concentrationwas
assayedby
thev
onClaussmetho
d.
FLEV
calculated
byanalyticalsoftw
arethrou
gha
transfo
rmationof
theF
FMAto
approxim
atethe
concentrationof
functio
nalfi
brinogen
correlates
with
stand
ardClaussfib
rinogen
(R2=0.57,p<0.00
1),sim
ilartoMA
(R2=0
.44-0.64
,p<0.00
1)bette
rthanthek
aolin
TEGmeasures
offib
rinogen
functio
n(kinetictim
eand
angle)
(R2=0
.01,
p=0.095;andR2
=0.03,p=
0.00
4)
[33]
Aprospectiveo
bservatio
nalstudy
of182trauma
patientsw
itham
edianISSof
17(9-26).C
itrated
bloo
dwas
sampled
immediatelyup
onarriv
al.
TheF
FTE
Gwith
tissuefactora
ctivator
andap
latelet
inhibitor(Re
oPro,a
GPIIb/IIIa
inhibitor)was
perfo
rmed
byaTE
G5000
Hem
ostasis
AnalyzerS
ystem
usingTE
GAnalyticalSoftw
areversion4.2.3
(Haemon
eticsC
orp.,B
raintre
e,MA),accordingto
the
manufacturer’s
recommendatio
ns.
FFTE
GMA,A
5,A10
hadmod
eratec
orrelatio
nwith
fibrin
ogen
concentrationdeterm
ined
bySpearm
an’s
correlation(𝜌=0
.64,0.68,0.68,p<
0.01).
[34,35]

BioMed Research International 5
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
Cardiac
surgery
Aprospectiveo
bservatio
nalstudy
of117
patients
operated
forischemicheartd
isease.Bloo
dwas
collected
before
cardiopu
lmon
arybypass
FFTE
Gtestwas
cond
uctedusingfunctio
nalfi
brinogen
reagent(lyop
hilized
tissuefactorw
ithplateletinhibitor-
glycop
rotein-IIb/IIIa
receptor
blocker).A
nalytical
softw
arec
alculatedthefun
ctionalfi
brinogen
level
(FLE
V)throu
ghthetransform
ationof
theM
Avalue.
Fibrinogen
levelswe
reassessed
bythev
onClauss
metho
d.
Amod
eratec
orrelatio
nwas
foun
dbetweenfib
rinogen
level
andFF
TEGFL
EVwith
aSpearman
correlationcoeffi
ciento
f0.476(p<0.00
01).
[36]
Aprospectives
tudy
of160cardiacs
urgery
patients.
Bloo
dwas
collected
atbaselin
e,priorto
heparin
isatio
nand10
min
postprotam
ine
administratio
n
TEG-fu
nctio
nalfi
brinogen
testwas
cond
uctedwith
nativ
eblood
usingthefun
ctionalfi
brinogen
reagent
(lyop
hilized
tissuefactorw
ithplateletinhibitor-
glycop
rotein
IIb/IIIareceptor
blocker).A
nalytical
softw
arec
alculatesthe
functio
nalfi
brinogen
level
(FLE
V)throu
ghthetransform
ationof
theM
Avalue.
Fibrinogen
levelswe
reassessed
with
citrated
bloo
dby
thevonClaussmetho
dusingFibrinogen-C
XL(H
emosiL;Instrum
entatio
nLabo
ratory,B
edford,M
A,
USA
)perform
edon
theA
CLTO
P300CT
Sanalyser
(Instr
umentatio
nLabo
ratory,B
edford,M
A,U
SA).
Nosig
nificantcorrelatio
nbetweentheT
EGFL
EVandthe
Claussfib
rinogen
levelatthe
baselin
e(R2
=0.10
6)and10
min
postprotam
ine(
R2=0
.025)and
betweentheT
EGFF
MAand
theC
laussfi
brinogen
concentrationattheb
aseline(R2
=0.061)
and10
min
postprotam
ine(R2=0
.26)
[37]
Aprospectives
tudy
of60
electiv
epatientso
perated
forischemicheartd
iseasew
ithCP
Bandrand
omly
assig
nedto
agroup
with
aheparin-coatedCP
Bsyste
mor
agroup
with
acon
ventional(no
n-coated)
circuit.Bloo
dwas
collected
from
right
after
indu
ctionof
generalanesth
esia,2-h
postop
eration,
andsecond
posto
perativ
eday.
FFTE
Gtestwas
cond
uctedby
mod
ified
TEGwith
plateletinhibitio
n(H
aemoscope
Corpo
ratio
n,Niles,IL,
USA
).Plasmafib
rinogen
levelswe
redeterm
ined
bya
Claussmetho
dno
tspecified.
Spearm
an’scorrelationanalysisshow
edam
oderatelyp
ositive
correlationbetweenperio
perativ
eClaussfi
brinogen
leveland
FFTE
GMA(n=6
0,r=0.40
8,p=
0.002)
[38]
Aprospectiven
on-rando
mized
study
of51
cardiac
surgerypatients.Citrated
(3.2%)b
lood
collection
tubesw
ereused
fora
llsamples
3tim
epoints:(1)
baselin
e;(2)rew
armingon
cardiopu
lmon
arybypass;
(3)p
ostb
ypass.
FLEV
assays
were
determ
ined
byTE
G5000
hemostasis
analyzersinaccordance
with
company’sprotocol
utilizing
thep
rovidedfunctio
nalfi
brinogen
reagentvials
(heparinasecups
were
used
fora
llbypasssamples).
Plasmafib
rinogen
levelswe
remeasuredusingthe
Claussmetho
d(Trin
iCLO
TFibrinogen
Kitwith
Destin
yMax
Coagulatio
nAnalyzer;Tcoag,Bray,Ireland
).
Asim
plelinearregressionmod
elshow
edas
trong
correlation
betweenthes
tand
ardlabo
ratory
assay(C
lauss)andthe
functio
nalfi
brinogen
level(FL
EV)assay
(r=0.76;p<0.00
01)
ofthefi
brinogen
values
attheb
aseline.Similarc
orrelatio
nwas
seen
atther
ewarmingandpo
stbypass.FLE
Vvalues
were
consistently
higher
than
thes
tand
ardlabo
ratory
assay.
[39]
Aprospectiveo
bservatio
nalstudy
of105child
renless
than
5yearso
fage
undergoing
congenitalh
eart
surgerywith
CPB.
Citrated
bloo
dwa
scollected
before
andaft
erbypass.
FFTE
Gwas
perfo
rmed
ontheT
EG5000
hemostasis
analyzersw
ithfunctio
nalfi
brinogen
reagentv
ialand
heparin
aseT
EGcup(H
aemon
etics,Niles,IL)b
yas
ingle
technician,w
ithin
20min
ofcollectionof
thes
amples.
Fibrinogen
levelswe
redeterm
ined
bytheC
lauss
metho
don
platelet-poo
r,centrifuged
bloo
dsamples
(STA
Fibrinogen,D
iagn
osticaStago).
Linear
correlationcoeffi
cientsbetweenFF
TEGMAand
fibrin
ogen
levelswe
re0.36
(p<0.00
1)before
and0.52
after
bypass(p=0
.02).
[40]
Aretro
spectiv
eand
observationalstudy
of119
child
renyoun
gerthan10
yearso
ldun
dergoing
congenitalcardiac
surgerywith
CPB.
Bloo
dwas
collected
twiced
uringsurgery,aft
eranesthesia
indu
ctionandCP
B.
ROTE
MFIBT
EMwas
perfo
rmed
accordingto
manufacturer’s
procedure.Fibrinogen
concentration
was
measuredby
afullyautomated
device
(Diagn
ostica
Stago,Asnieres,France).
Post-
CPBfib
rinogen
levelswe
reno
tcorrelatedwith
post-
CPB
FIBT
EMMCF
ininfants(r=0.155,p=
0.197,0.155),w
hereas
they
were
correlated
with
FIBT
EMMCF
inchild
renolderthan
12mon
ths(r=0.311,p=
0.031).
[41]

6 BioMed Research International
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
Livertransplantatio
n(LT)
Aprospectives
tudy
of27
consecutiveadultL
Tpatients.Bloo
dsamplew
astakenfrom
anarteria
llin
eatthe
timeo
fthe
skin
incisio
n(th
ebaseline)and
30min
after
graft
reperfusion
Thew
holebloo
dwas
analyzed
with
TEG5000
hemostasis
analyzer
accordingto
them
anufacturer’s
instr
uctio
ns.P
lasm
afibrinogen
levelw
eremeasured
with
amod
ified
Claussmetho
dusingac
oagulatio
nanalyzer
(STA
-REv
olutionEx
pertserie
shem
ostasis
syste
m,D
iagn
osticaStago,Parsippany,N
J,USA
)
FFTE
GMAcorrelated
stron
glywith
thep
lasm
afibrinogen
levelatthe
baselin
e(Spearm
an’scorrelationcoeffi
cient𝜌
=0.90,
p<0.01);ho
wever,thec
orrelatio
nredu
cedaft
ertheg
raft
reperfusion(𝜌=0
.58,p<
0.01).Th
esam
ecorrelations
were
seen
betweenFF
TEGFL
EVandthep
lasm
afibrinogen
level.
[42]
Pregnancy
Aprospectives
tudy
of21
healthy,term
parturients
schedu
ledfore
lectivecesarean
delivery.Freshwho
lebloo
dwas
draw
nfrom
each
patient.
Mod
ified
TEGwas
perfo
rmed
with
360mLof
1%celite-activ
ated
who
lebloo
dandwith
5mLof
(2mg/mL)
ReoP
ro�(plateletaggregatio
ninhibitor)addedto
355
mLof
1%celite-activ
ated
who
lebloo
dwith
in4min
ofbloo
dcollection.
Thep
lasm
afibrinogen
concentration
was
measuredby
theC
laussq
uantitativ
efib
rinogen
assayusingthrombinderiv
edfrom
bovine
plasma
(Ortho
Diagn
ostic
Syste
mInc.,
Raritan,N
J).
Linear
regressio
nanalysisrevealed
TEGMAas
asignificant
predictoro
fthe
plasmafi
brinogen
level,with
anadjuste
dR2
of0.49,and
aslope
offib
rinogen
level=
9.56×
MA+150.68
[43]

BioMed Research International 7
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
ROTE
MFIBT
EM
Trauma
Rand
omized
controlledtrialoftraum
apatientsa
tris
kof
significanth
emorrhage(
n=45,ISS=18-29)
receivingeither
6gfib
rinogen
concentrate
(RiaSTAP�
)orp
lacebo
(normalsalin
e).C
itrated
who
lebloo
dwas
collected
from
ther
ando
mized
traumapatientsa
tadm
ission,
1-,3-,11-,
23-and
47-h
post-
infusio
ntim
e.
Standard
ROTE
MFIBT
EMwas
perfo
rmed
ona
ROTE
Mdelta
syste
maccordingto
manufacturer’s
protocol.Specifically,
analyses
were
perfo
rmed
using300
𝜇Lof
citrated
who
lebloo
dand20𝜇Lof
ex-te
mtogether
with
20𝜇Lof
fib-te
mfollo
wingthep
rocedu
reas
recommendedby
thec
ompany.P
lasm
afibrinogen
levels
were
measuredby
thesta
ndardvonClaussmetho
d.
ROTE
MFIBT
EMMCF
stron
glycorrelated
with
Clauss
fibrin
ogen
concentrationdeterm
ined
bySpearm
an’s
correlation(𝜌=0
.87,p<
0.00
1).R
OTE
MFIBT
EMCF
T,Alpha
show
edmod
eratec
orrelatio
nswith
fibrin
ogen
concentration
(𝜌=-0.41
and0.54,p<0.00
1),w
hileCT
andLI30
weekly
correlated
with
fibrin
ogen
concentration(𝜌=-0.29,p<0.00
1and0.20,p=0
.003).
[30,31]
Aprospectives
tudy
of517adulttraum
apatientsw
ithas
ystolic
bloo
dpressure
(SBP
)of<
90mmHganda
medianISSof
14(8–27).C
itrated
bloo
dwas
collected
with
in20
min
ofarriv
alin
thee
mergency
department(ED
).
Bloo
dsamples
were
analyzed
with
in2hof
bloo
ddraw
,with
aRO
TEM
delta
instr
ument,at37∘C.
Twoseparate
ROTE
Massays
were
perfo
rmed
fore
achpatient,the
EXTE
M,m
easurin
gtissuefactor-initiated
clottin
g,and
theFIBT
EM,w
iththea
ddition
ofcytochalasin
D,a
plateletinhibitora
sper
manufacturer’s
protocols.
Fibrinogen
levelswe
redeterm
ined
with
theC
lauss
metho
dusingSTAFibrinogen
(Stago,A
snieressur
Seine,France)a
ndSiem
ensTh
rombin(Sysmex
UK,
Milton
Keynes,U
K)reagents.
EXTE
MandFIBT
EMmeasureso
fA5andmaxim
alclot
form
ation(M
CF)w
eres
ignificantly
correlated
with
Clauss
fibrin
ogen
levels,
andthec
orrelatio
nsbetweenFIBT
EMA5
andMCF
were
slightly
stron
gerthanEX
TEM
(r2=0.44
vs.
0.35
and0.27
vs.0.26).E
XTEM
andFIBT
EMA5gave
areceiver
operatingcharacteris
ticcurvea
reaof
0.8(95%
confi
denceinterval0.7–0
.9,p<
0.00
1)ford
iscrim
inating
patientsw
ithadmissionfib
rinogen
levelsbelow1.5
g/L.
[3]
Aretro
spectiv
estudy
of358traumapatientsw
itha
medianISSof
26(17–34).Citrated
bloo
dwas
collected
atadmissionanddu
ringthefi
rst12-hcare.
EXTE
MandFIBT
EMwe
reperfo
rmed
inasta
ndardized
fashionwith
in30
min
ofbloo
dcollection.
Fibrinogen
concentrationwas
measuredby
theC
lausstechn
ique,
STA-
Fibrinogen.
Correlatio
nsbetweenfib
rinogen
concentrationandFIBT
EMA5atadmission(Spearman
coeffi
cient𝜌
=0.858)and
durin
gcare
(𝜌=0
.824),no
bloo
dprod
uctg
roup
(𝜌=0
.772)and
bloo
dprod
uctg
roup
(𝜌=0
.823).
[44]
Aprospectiveo
bservatio
nalcoh
ortstudy
of182
traumapatientsw
itham
edianISSof
17(9
to26).
Bloo
dwas
sampled
immediatelyup
onarriv
alat
hospitaland
kept
atroom
temperature.
EXTE
M,INTE
MandFIBT
EMassays
were
perfo
rmed
with
citrated
bloo
daccordingto
them
anufacturer’s
recommendatio
ns1h
after
sampling.
Fibrinogen
concentrationhadmod
eratec
orrelatio
nswith
A5,
A10
andMCF
ofEX
TEM
(𝜌=0
.65-0.68),IN
TEM
(𝜌=0
.62-0.68)and
FIBT
EM(𝜌=0
.68).
[34]
Aprospectiveo
bservatio
nalstudy
of88
trauma
patientsw
ithan
ISSof22
(12-34).Bloo
dsamples
were
collected
immediatelyaft
erthep
atient’sarriv
alto
the
traumaroom
andat6,12
and24
haft
eradmission
EXTE
M,INTE
MandFIBT
EMwe
reperfo
rmed
at37∘C
inparallelw
iththec
itrated
bloo
dwith
in2handaft
er15
min
ofcollectionin
asta
ndardizedway.Fibrin
ogen
levelswe
reassayedaccordingto
Clausstechniqu
eusin
gFibriquick�reagent(Biom
erieux).
Asig
nificantcorrelatio
nwas
foun
dbetweenfib
rinogen
levels
andEX
TEM
CT(r=0.40
,p<0.00
1),A
15(r=0
.69,p<
0.00
1),
betweenfib
rinogen
levelsandIN
TEM
A15
(r=0
.66,p<
0.00
1),
andbetweenfib
rinogen
levelsandFIBT
EMA10
(r=0
.85,
p<0.00
1)
[45]
Aprospectivec
ohortstudy
of334blun
ttraum
apatients(ISS≥
15or
Glasgow
Com
aScore≤
14).
Citrated
bloo
dwas
collected
atho
spitaladm
ission.
ROTE
MEX
TEM
andFIBT
EMtests
were
perfo
rmed
accordingto
manufacturer’s
guides.P
lasm
afib
rinogen
concentrationwas
measuredusingtestkitsfrom
Siem
ensH
ealth
care
AG,E
rlangen,G
ermany.
EXTE
MandFIBT
EMMCF
show
edstr
ongcorrelations
with
fibrin
ogen
concentration(𝜌=0
.79and0.81,respectively,
p<0.00
1).
[46]

8 BioMed Research International
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
Cardiac
surgery
Aprospective,ob
servationalpilo
tstudy
of35
patientsu
ndergoingelectiv
ecardiacs
urgery
oncardiopu
lmon
arybypassforc
yano
ticcongenital
heartd
isease.Bloo
dsamples
were
collected
after
indu
ctionof
anesthesia.
EXTE
M,INTE
MandFIBT
EMwe
reperfo
rmed
with
citrated
bloo
daft
errecalcificationwith
20𝜇LCaC
l 2.
Fibrinogen
concentrationassaywas
notp
rovided.
Fibrinogen
concentrationshow
edas
ignificantcorrelatio
nwith
ROTE
MFIBT
EMMCF
(Pearson
coeffi
cientr=0
.94,p<
0.00
1),but
notw
ithEX
TEM
MCF
(r=0
.077,p=0
.67)
and
INTE
MMCF
(r=0
.162,p=
0.37).
[47]
Aprospectiveo
bservatio
nalstudy
of30
patients
undergoing
cardiacs
urgery
with
cardiopu
lmon
ary
bypass(C
PB).Citrated
bloo
dwas
draw
natthe
beginn
ingof
surgery(pre-C
PB),20
minutes
before
weaningfrom
CPBand5minutes
after
heparin
neutralization.
TEGwith
thefun
ctionalfi
brinogen
reagent(FF
TEG),
ROTE
Mwith
fib-te
m(FIBTE
M)and
fib-te
mplus
containing
twoplateletinhibitors:cytochalasin
Dand
tirofi
ban(FIBTE
MPL
US)
were
runfora
minim
umof
30min.Fibrin
ogen
concentrationwas
measuredusing
theClaussmetho
dandph
oto-op
ticaldeterm
inationon
theAC
LTo
p700(In
strum
entatio
nLabo
ratory,M
ilan,
Italy)a
ndQFA
thrombinreagent(Instr
umentatio
nLabo
ratory).
Sign
ificant
positivec
orrelatio
nswe
refoun
dbetweenMCF
orMAandfib
rinogen
concentration(allp<
0.00
1);the
highest
correlationwas
with
FIBT
EMPL
USMCF
(Spearman
coeffi
cient𝜌
=0.70),followe
dby
FIBT
EM(𝜌=0
.66)
andFF
TEG(𝜌=0
.56).
[48]
Aprospectives
tudy
of157patientsu
ndergoing
cardiacs
urgery
with
CPB.
Citrated
bloo
dwe
recollected
atbaselin
e(beforeindu
ctionof
anaesth
esia)
andatthee
ndof
CPB(afte
rprotamine
administratio
n).
Who
lebloo
dFIBT
EMwas
perfo
rmed
usingaR
OTE
Mdevice
accordingto
them
anufacturer's
instr
uctio
nsat
each
timep
oint.P
lasm
afib
rinogen
concentrationwas
measuredusingtheC
laussm
etho
dandwho
lebloo
dfib
rinogen
concentrationwas
calculated
asplasma
fibrin
ogen
concentration×(100−haem
atocrit)/100.
TheS
pearman
correlationcoeffi
cientb
etwe
enFIBT
EMMCF
andplasmafi
brinogen
concentrationwas
0.68
atbaselin
eand
0.70
after
protam
ine,whilethatbetweenFIBT
EMMCF
and
who
lebloo
dfib
rinogen
concentrationwas
0.74
atbaselin
eand
0.72
after
protam
ine(allp<
0.00
1).
[49]
Aprospectiveo
bservatio
nalstudy
of35
patients
undergoing
electiv
ecardiac
surgerywith
CPB.
Citrated
bloo
dwas
collected
from
atthreedifferent
timep
oints:preoperativ
ely(
immediatelybefore
anesthesiaindu
ction),and
at1-and24-h
post
operation.
Kaolin
TEGandRO
TEM
EXTE
M,INTE
M,FIBTE
Mwe
recond
uctedwith
thecitrated
bloo
dwith
in1h
after
thecollection,
accordingto
them
anufacturer’s
instr
uctio
ns.F
ibrin
ogen
concentrationwas
measuredby
asta
ndardmetho
d(not
specified).
Correlatio
nsbetweenfib
rinogen
concentrationandEX
TEM
MCF
(Pearson
coeffi
cientr=0
.71,p<
0.00
05),IN
TEM
MCF
(r=0
.53,p=0
.001),FIBT
EMMCF
(r=0
.79,p<
0.00
05)w
ere
foun
dat1-h
postop
erationandcorrelations
between
fibrin
ogen
concentrationandTE
GK(r=-0.52,p=0
.002),
Alpha
(r=0
.53,p=0
.001),TE
GMA(r=0
.63,p<
0.00
05),
EXTE
MMCF
(r=0
.58,p=
0.00
1),INTE
MMCF
(r=0
.63,
p<0.00
05),FIBT
EM(r=0
.50,p=
0.003)
at24-h
postop
eration.
[50]
Aretro
spectiv
eobservatio
nalstudy
of1077
patients
undergoing
cardiacs
urgery
with
CPB.
Citrated
bloo
dwas
collected
durin
gther
ewarmingph
ase(≥36∘ C).
EXTE
MandFIBT
EMwe
recond
uctedat37∘Cas
per
manufacturer’s
reagentsandprocedures.Fibrin
ogen
concentrationwas
measuredby
theC
laussm
etho
dusingSTAREv
olution(Stago,P
aris,
France).
Claussfib
rinogen
concentrationwas
correlated
stron
glywith
EXTE
MMCF
andA10
(Spearman
coeffi
cient𝜌
=0.68and0.70;
p<0.01)and
FIBT
EMMCF
andA10
(𝜌=0
.78and0.78;p<0.01).
Thec
orrelatio
nwas
relatedinverselyto
hemoglobin
concentration(p<0.01).
[51]
Arand
omized
controlledtrialof116
high-risk
patientsu
ndergoingcardiacs
urgery
with
CPB.
Bloo
dwas
collected
at20
min
beforeremovalof
theaortic
cross-clam
p(baseline)andaft
erplaceboor
fibrin
ogen
administratio
n.
FIBT
EMtestwas
cond
ucted.
Fibrinogen
concentrations
were
measuredaccordingto
apho
to-opticalClauss
metho
d,with
acoagulatio
nanalyser
(ACL
TOP700),a
calib
rator(Hem
osilNormalCon
trol),
andathrom
bin
reagent(Hem
osilQFA
thrombin).
Linear
regressio
nanalyses
show
edagood
associationbetween
FIBT
EMMCF
andClaussfib
rinogen
concentrationatthe
baselin
epop
ulation(R2=0
.66,p=
0.00
1),w
hich
redu
cedto
R2=0
.16(p=0
.003)infib
rinogen-sup
plem
entedsubjects.
[52]
Aprospectiveo
bservatio
nalstudy
of110
patients
undergoing
cardiacs
urgery
with
CPB.
Citrated
who
lebloo
dwas
sampled
from
acentralveno
uslin
eor
from
thee
xtracorporealcirc
uitatp
re-C
PB,
on-C
PB,post-C
PB.
ROTE
Massays
ofIN
TEM,E
XTEM
,FIBTE
Mand
HEP
TEM
were
perfo
rmed
at37∘Cby
certified
bioanalyticaltechnicians.
Plasmalevelsof
fibrin
ogen
were
measuredusingthe
Clausstechniqu
eon
acoagulationanalyzer
(BCS
,Dade
BehringInc.,
Germany)
usingtheM
ultifi
bren
U-Reagent
accordingto
manufacturer’s
specificatio
ns.
Thefi
brinogen
leveland
FIBT
EMA10
were
significantly
correlated
fora
lldatapo
ints(Pearson
coeffi
cientr=0
.81;
p<0.05).Th
eirc
orrelatio
nwas
stron
gero
n-CP
Batam
ean
hemoglobinof
83g/L(r=0.87)and
post-
CPB(m
ean
hemoglobin88
g/L;r=0.74)thanpre-CP
B(m
eanHem
oglobin
105g/L;r=0.66
).
[53]

BioMed Research International 9
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
Livertransplantatio
n(LT)
Aretro
spectiv
eobservatio
nalstudy
of282patients
receivingliver
transplantation.
Citrated
bloo
dwas
collected
at1h
after
indu
ctionof
generalanesth
esia,1
haft
erthefi
rstsurgicalincision
,30min
after
hepatectom
y,30
min
after
graft
reperfusion,
andaft
erhepatic
artery
anastomosis.
ROTE
Mtests
(EXT
EM,INTE
MandFIBT
EM)w
ere
routinelyperfo
rmed
accordingto
them
anufacturer’s
instr
uctio
ns.F
ibrin
ogen
concentrationwas
measured
usingtheD
adethrom
binreagent(Siem
ensH
ealth
care
Diagn
ostics,Erlangen,G
ermany)
andan
automatic
coagulationanalyzer
(Sysmex
CA-700
0,Siem
ens
Health
care
Diagn
ostics,Erlangen,G
ermany).
Fibrinogen
was
theprim
arydeterm
inanto
fFIBTE
MMCF
,accoun
tingfor7
3%of
thev
ariability.How
ever,insevere
hypo
fibrin
ogenem
ia(fibrinogen<1g
/L),fib
rinogen
accoun
ted
only22%
ofFIBT
EMMCF
varia
bility.Spearm
an’scorrelations
betweenfib
rinogen
concentrationandEX
TEM
MCF
(𝜌=0
.66,
p<0.00
1),INTE
MMCF
(𝜌=0
.65,p<
0.00
1),FIBTE
MMCF
(𝜌=0
.83,p<
0.00
1).
[54]
Aretro
spectiv
eobservatio
nalstudy
of295patients
(254
livingdo
norsand41
LTpatients).C
itrated
bloo
dwas
collected
from
1haft
erindu
ctionof
generalanesth
esia,1
haft
ersurgicalincisio
n,30
min
after
hepatectom
y,30
min
after
graft
reperfusion,and
after
hepatic
artery
anastomosis.
Thes
amea
sabo
ve
FIBT
EMMCF
significantly
correlated
with
fibrin
ogen
concentrationwith
ahighestSpearm
an’scoeffi
cient(𝜌=0.84,
p<0.00
1),followe
dby
EXTE
MMCF
(𝜌=0
.67,p<
0.00
1),
INTE
MMCF
(𝜌=0
.66,p<
0.00
1).
[55]
Aprospectives
tudy
of253patientsreceiving
orthotop
icliver
transplantation.
Citrated
bloo
dsamples
were
collected
after
indu
ctionof
general
anesthesia,atthe
endof
theh
epatectomy,20
minutes
after
graft
revascularization,
and90
minutes
after
graft
revascularization.
Theb
lood
samples
were
teste
djustaft
ercollectionby
ROTE
Mgammadevice
operated
accordingto
manufacturerinstructio
nsandwith
thetypea
ndconcentrationof
reagentsas
provided
byPentapharm
(Mun
ich,Germany).F
ibrin
ogen
concentrationwas
measuredby
prothrom
bintim
e-deriv
edmetho
d,with
values
below2g/Lbeingcheckedby
theC
laussm
etho
don
acoagulometer
(KC-
1A,A
melu
ng,L
emgo,G
ermany)
usingfib
rinogen
reagent(Diagn
osticaStago,Asnieres,
France)a
ccording
tothem
anufacturer’s
instr
uctio
ns.
FIBT
EMMCF
correlated
with
fibrin
ogen
level(Spearm
an’s
correlationcoeffi
cient𝜌
=0.70).
[56]
Aprospectiveo
bservatio
nalstudy
of20
patients
undergoing
orthotop
icliver
transplantation.
Bloo
dsamples
were
takenatthefollowingpo
intsdu
ring
OLT
:the
beginn
ingof
thed
issectio
nph
ase,thee
ndof
dissectio
nph
ase,10
min
into
thea
nhepaticph
ase,
10min
into
ther
eperfusio
nph
ase,and1h
after
dono
rgraft
reperfusion.
FIBT
EMwas
perfo
rmed
with
citrated
bloo
dwith
in4h
ofcollectionaccordingto
themanufacturer’s
instr
uctio
ns.C
laussfi
brinogen
assaywas
perfo
rmed
onaCA
-1500analyzer
(Sysmex,M
ilton
Keynes,U
K).
Therew
asas
ignificantcorrelatio
nbetweenFIBT
EMMCF
and
Claussfib
rinogen
concentration(Pearson’scorrelation
coeffi
cientr
=0.75,p≤
0.01).
[23]
Aprospectiveo
bservatio
nalstudy
of23
patients
undergoing
orthotop
icliver
transplantation.
Bloo
dsamples
were
collected
after
indu
ctionof
general
anaesth
esia,d
uringhepatectom
y,attheanhepatic
stage,30–
60min
after
graft
revascularization,
atthe
endof
surgery,and24
haft
ersurgery
ROTE
Mtests
(EXT
EM,INTE
M,FIBTE
MandAPT
EM)
were
perfo
rmed
intheo
peratin
gtheatre
andby
the
anaesth
esiologists
treatingthep
atientsa
ccording
tothe
manufacturer’s
instr
uctio
nsusingequipm
entand
test
reagentsprovided
byPentapharm
GmbH
.Plasm
afib
rinogen
concentrationwas
determ
ined
bytheC
lauss
metho
dperfo
rmed
onAC
LTo
pautomates
(Instr
umentatio
nLabo
ratory,Lexington
,MA,U
SA)
ROTE
MFIBT
EMA10
correlated
with
Claussfib
rinogen
(r=0
.74,p<0.00
01),on
lyslightly
stron
gerthanEX
TEM
A10
(r=0
.72,p<
0.00
01)
[57]

10 BioMed Research International
Table1:Con
tinued.
Clinicalsettings
Stud
ypo
pulatio
nandbloo
dsample
TEGandRO
TEM
metho
dsRe
sults
Ref.
Aretro
spectiv
estudy
of40
1patientsw
houn
derw
ent
liver
transplantation.
Bloo
dwas
sampled
at1h
after
indu
ctionof
generalanaesthesia,1
haft
ersurgical
incisio
n,30
min
after
hepatectom
y,and30
min
after
graft
reperfusionandaft
erhepatic
artery
anastomosis.
ROTE
Mtests
were
perfo
rmed
accordingto
the
manufacturer’s
instr
uctio
ns,u
singequipm
entand
test
reagents
provided
byTem
InternationalG
mbH
.Fibrin
ogen
level
was
measuredusingtheD
adeTh
rombinRe
agent
(SiemensH
ealth
care
Diagn
ostics)andan
automatic
coagulationanalyser
(Sysmex
CA-700
0,Siem
ens
Health
care
Diagn
ostics).
Thec
orrelations
ofFIBT
EMA5,A10,M
CFwith
fibrin
ogen
levelswe
redeterm
ined
usingSpearm
an’srank
correlation
coeffi
cients(𝜌=0.75,0.76
and0.75,respectively,p<
0.00
1).
[58]
Postp
artum
Aprospectiveo
bservatio
nalstudy
of91
women
atthe
third
trim
estero
fpregn
ancy:37with
postp
artum
haem
orrhage(stu
dygrou
p)and54
with
outabn
ormal
bleeding
(con
trolgroup
).Citrated
bloo
dwas
collected
from
women
atthethird
trim
estero
fpregnancy.
Standard
FIBT
EMwas
carriedou
tbyclinicians
with
the
bloo
dsamples
inthed
eliveryroom
.Fibrin
ogen
assay
was
forp
lasm
acon
centratio
nwith
in5min
after
samplingwith
aSTA
Rautomated
coagulationanalyser
(Diagn
osticaStagoInc.,
Franconville,France)
A5,A15
andMCF
were
significantly
lowe
rintheh
aemorrhage
grou
pthan
incontrol(p<
0.00
01)and
stron
glycorrelated
with
fibrin
ogen
levelsbo
thgrou
ps(Spearman’scorrelation
coeffi
cient𝜌
=0.84–0
.87,p<
0.00
01).
[59]
Neurosurgery
Aprospectiveo
bservatio
nalstudy
of92
patients
undergoing
emergent
neurosurgery
ROTE
Manalyses
were
perfo
rmed
with
inmin
ofbloo
dsamplingby
anesthesianu
rses
orph
ysicians
trainedto
perfo
rmtheR
OTE
Mtests
accordingto
the
manufacturer’s
instr
uctio
ns.P
lasm
afib
rinogen
concentrationwas
determ
ined
byClaussmetho
d(Siemens-DadeBe
hringHealth
care
Diagn
ostics,
Marbu
rg,G
ermany).
Therew
asas
trong
correlationbetweenPT
TandIN
TEM
CT(r=0
.76)asw
ellasb
etwe
enfib
rinogen
concentrations
and
FIBT
EMMCF
(r=0
.70).
[60]
Burn
injury
Aprospectiveo
bservatio
nalstudy
of20
consecutive
patients.Citrated
bloo
dwas
collected
immediately
after
admission,
12,24and48
haft
eradmission.
Four
ROTE
Mtests
(INTE
M,E
XTEM
,FIBTE
Mand
APT
EM)w
erep
erform
edsim
ultaneou
slyon
the
four-chann
elRO
TEM
intheICUwardlabateach
time
point.Plasmafib
rinogen
levelw
asdeterm
ined
byClauss
metho
dusingan
automated
coagulationanalyzer
(STA
-REv
olution,
Stago,Asnieres,France).
Fibrinogen
leveland
FIBT
EMMCF
were
with
inther
eference
rangeun
til24
haft
erbu
rninjury,but
increasedsig
nificantly
after
48h.Th
erew
asa
significantcorrelatio
nbetweenFIBT
EMMCF
andfib
rinogen
level(Spearm
an’scorrelationcoeffi
cient𝜌
=0.714,p<0.00
1).
[61]
Cirrho
sis
Across-sectionalsingle-centre
study
involving60
patientsw
ithalcoho
liccirrho
sis,24patientsw
ithcholestatic
cirrho
sisandac
ontro
lgroup
of50
healthy
volunteers.B
lood
samples
were
takenatadmission.
ROTE
MFIBT
EMassaywas
perfo
rmed
with
citrated
bloo
dwith
in1h
after
collectionusingas
etof
stand
ard
reagentsaccordingto
them
anufacturer’s
recommendatio
ns.C
laussfi
brinogen
assaywas
perfo
rmed
usingaBC
S�XP
automated
coagulation
analyzer
(SiemensH
ealth
care
Diagn
osticsG
mbH
,Marbu
rg,G
ermany).
Inallcirr
hosis
patients,FIBT
EMMCF
stron
glycorrelated
with
fibrin
ogen
concentration(r=0
.72-0.77,p<0.00
1).
[62]
CPB=
Cardiop
ulmon
aryBy
pass;ISS=InjurySeverityScore;Livertransplantatio
n=LT

BioMed Research International 11
Meyer 2015Peng 2018 Gottumukkala 1999
Lu 2014r=0.77, p<0.00195% Confidence Interval
4 6 8 102Clauss fibrinogen level (g/L)
0
10
20
30
40
50
60
70FF
TEG
MA
(mm
)
(a)
Blasi 2012Peng 2018
Meyer 2015Solomon 2013
Ranucci 2016 r=0.77, p<0.00195% Confidence Interval
0
10
20
30
40
50
ROTE
M F
IBTE
M M
CF (m
m)
2 4 6 80Clauss fibrinogen level (g/L)
(b)
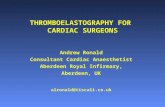
Figure 1: Correlations of Clauss fibrinogen level with FF TEGMA (a) and with ROTEM FIBTEMMCF (b).The correlation coefficients wereobtained through linear regression of all data extracted from the literature. The data were pooled from different clinical studies involving atotal of 275 patients for the correlation between Clauss fibrinogen level and FF TEG MA [30, 35, 42, 43] and a total of 626 patients for thecorrelation between Clauss fibrinogen level and ROTEM FIBTEM MCF [30, 35, 48, 52, 56]. The means ± standard deviations of FF TEGMA and Clauss fibrinogen level in (a) are 20.14±8.28 mm and 2.71±1.32 g/L. Themeans ± standard deviations of ROTEM FIBTEMMCF andClauss fibrinogen level in (b) are 15.40±7.86 mm and 2.74±1.22 g/L.
assays can be completed in 15 min and can provide rapidand accurate detection of hyperfibrinolysis [87]. Anotheradvantage of TEG and ROTEM is that they can be used forfully heparinised patients, e.g., when on cardiopulmonarybypass, with the use of a heparinase TEG cup or heparinase.In vitro studies showed that FF TEG MA was unaffected byheparin levels up to 2.8 IU/mL, but was reduced at 5.6 IU/mLof heparin in blood even performed in heparinase TEG cups[71], while ROTEM FIBTEMMCFwas insensitive to heparinup to a concentration of 4 IU/ml in whole blood, but thendeclined to values less than 50%of baseline at 8 IU/mL [88]. Aclinical study in pediatric cardiac surgery validated the use ofFIBTEM in the presence of very high heparin concentrations(400 IU/kg bodyweight) [89].
The correlations between Clauss fibrinogen concentra-tion and FF TEG MA or ROTEM FIBTEM MCF couldbe affected by a number of factors in addition to heparinconcentration. As elucidated in Table 1, different reagents andinstruments produced by Stago, Siemens, and Instrumenta-tion Laboratory are used to quantify fibrinogen concentra-tion. It is known that there can be systematic differencesbetween the fibrinogen concentrations obtained with variouscommercial kits [90]. The different detections used in theClauss method and resuscitation fluids administered mayaffect the correlation [91, 92].This is likely due to the fact thatFIBTEM test is more affected than fibrinogen concentrationassays by the fluids [93]. Solomon et al. examined correlationsbetween ROTEM FIBTEMMCF and Clauss fibrinogen con-centration as determined using photo-optical, mechanical,and electromechanical detections in cardiac surgery patients
[91]. The correlations obtained from the photo-optical andelectromechanical methods (r=0.82 and 0.81) were greaterthan the mechanical method (r=0.73 and 0.71). Fenger-Eriksen et al. assessed fibrinogen levels in plasma dilutedin vitro with different fluids (isotonic saline, hydroxyethylstarch, and human albumin) using an antigen determination,three photo-optical Clauss methods, one mechanical Claussmethod, a prothrombin-derived method, and viscoelasticmeasurement through ROTEM [92]. The fibrinogen levelswere overestimated using the photo-optical Clauss methodsas a result of the dilution with hydroxyethyl starch, whereasROTEM FIBTEM MCF was reduced by the dilution and toa lesser extent by human albumin. The former was ascribedto an unexplained interference with the optical source byhydroxyethyl starch and the latter was due to impairmentof fibrin polymerization induced by the fluid. In addition,the fibrinogen measurement by the Clauss method for thesame set of plasma samples can vary within and betweenlaboratories [94].
On the other hand, it was found that plasma fibrinogenlevel (FLEV) estimated by FF TEG was on average 1.0 g/Lhigher than that determined by the Clauss method in bothsurgical patients and healthy controls [95]. This is consistentwith other reports of higher TEGFLEVvalues than theClaussvalues in cardiac surgery [39] and overestimation of plasmafibrinogen level in liver transplantation when the plasmafibrinogen level becomes less than 1 g/L [42].
In our subgroup analysis of trauma patients who receivedfibrinogen concentrate versus placebo (i.e., normal saline),the correlation coefficients are not as significantly altered

12 BioMed Research International
between the two groups (0.68 versus 0.67 for FF TEG and0.88 versus 0.82 for ROTEM FIBTEM). This is in contrastwith patients undergoing liver transplantation [42, 54] andcardiac surgery [52, 91] where the correlation was impairedby severe hypofibrinogenemia and fibrinogen replacement.Specifically, the correlations between FIBTEM MCF andClauss fibrinogen concentration decreased from r=0.71-0.82to 0.33-0.59 after administration of fibrinogen concentratein patients undergoing complex cardiovascular surgery [91].In addition, hyperfibrinogenemia (>4 g/L) could impair thecorrelation between ROTEM FIBTEM MCF and fibrinogenlevels as reported in major upper gastrointestinal surgery[96].Therefore, the discrepancymay be due to the differencesin the range of plasmafibrinogen concentrations among thesestudies (e.g., interquartile range of 1.88-3.63 g/L in our studyvs. 0.77-1.38 g/L in the liver transplantation study). Similarcorrelations were reported between FIBTEM clot amplitudeand fibrinogen concentration (r=0.86) at admission and thendecreased correlations (r=0.43 and 0.63) after admission inthe trauma patients receiving fibrinogen concentrate [44].
It should be noted that the concentration measurementsby the Clauss method and other plasma fibrinogen assayscannot be the same as the clot strength of whole bloodmeasured by TEG and ROTEM. Apparently, fibrinogen is notthe only contributor to clot amplitude in these FF TEG andROTEM FIBTEM assays, which may impose some limita-tions on FF TEG and ROTEM FIBTEM for the assessmentof fibrinogen deficiency. Activated FXIII and hematocritcould have an impact on clot firmness as well and affect thecorrelations [49, 96–99]. Postoperative FXIII levels correlatedto FIBTEM MCF more significantly than fibrinogen levelsin patients undergoing major upper gastrointestinal surgery[96]. However, the same study also showed a significant cor-relation between platelet count and ROTEM FIBTEM MCF(r=0.55), which implied that the test might be profoundlyimpaired by incomplete inhibition of the platelet contributionto the clot strength. Furthermore, FXIII levels might affect FFTEG as well [98].
In addition, Ogawa et al. reported a higher correlationbetween ROTEM FIBTEM MCF and Clauss plasma fibrino-gen at lower hematocrit (<25%) than at higher hematocrit(>30%) (r =0.88 and 0.67, resp.) in cardiac surgery [99].In contrast, Solomon et al. found no significant differencesbetween the lowest haematocrit group (<25%) and the higherhaematocrit groups (25-27.9%, 28-29.9%, and >30%) forFIBTEM MCF or fibrinogen concentrations in whole bloodand plasma, and thus the hematocrit effect appeared to benegligible [49]. FF TEG has shown hypocoagulable states inpatients with cyanotic congenital heart disease mainly due toimpaired fibrinogen function negatively affected by elevatedhaematocrit [100].
In addition toMA, other TEG parameters, e.g., estimatedfunctional fibrinogen level (FLEV) and kinetic time K andAlpha, kaolin TEGK andAlpha, have shown different extentsof correlations with fibrinogen concentration [32, 33, 47].Kornblith et al. confirmed a significant correlation betweenFF TEG FLEV and the Clauss fibrinogen assay in traumapatients in agreement with the published findings from Harret al., but the correlation as assessed by linear regression was
weaker (R2= 0.57 vs. 0.87) [32, 33]. In addition, differentcorrelations of FLEV with kaolin TEG MA (R2= 0.44-0.64vs. 0.80), K (R2= 0.01 vs. 0.35), and Alpha (R2= 0.03 vs. 0.70)were reported in their studies likely due to different statisticalmethods (linear vs. polynomial regression). The correlationswere affected by fibrinogen concentration, decreases at lowand high ranges [32]. FF TEG FLEV was diminished andnegatively correlated to haematocrit [100].
We observed moderate correlations of Clauss fibrino-gen concentration with FF TEG K and Alpha (Spearman’scorrelation 𝜌=-0.46 and 0.40) and with ROTEM FIBTEMCFT and Alpha (𝜌=-0.41 and 0.54) in trauma patients [30].Furthermore, there were weak correlations of fibrinogenconcentration with ROTEM FIBTEM CT (𝜌=-0.29), andwith FF TEG CL30 and ROTEM FIBTEM LI30 (𝜌=0.21 and0.20).The correlations between K/CFT, Alpha and fibrinogenconcentration are consistent with their measurement of theactivity of clotting factors, in particular fibrinogen [101], andare comparable with or stronger than the reported correla-tions between FFTEGK/Alpha and fibrinogen concentration[32, 33]. A linear correlation was observed between the clotshear elasticity G calculated fromFFTEGMA and functionalfibrinogen levels measured by the Clauss method in bothwhole blood (R2=0.605) and platelet-poor plasma (R2=0.94)[102].
Among all the parameters, the strongest correlationsbetween FF TEG MA/ROTEM FIBTEM MCF and plasmafibrinogen concentration have been reported [32, 33, 103],suggesting these parameters are most useful for monitoringthe role of fibrinogen in hemostasis of bleeding patients.
Together with kaolin TEG, FF TEGhas been used to char-acterize functional fibrinogen to platelet ratio and was founduseful in preoperatively identifying thrombotic complicationin patients undergoing microvascular free tissue transferin head and neck surgery [104]. FF TEG MA correlatedwith a number of biomarkers of endothelial activation anddamages such as syndecan-1, thrombomodulin and proteinC, and plasminogen activator inhibitor-1 (r=-0.37, p<0.001)in patients with severe sepsis [105].
5. Diagnosis ofCoagulopathy/Hypofibrinogenemia andPrediction of Blood Transfusion
Table 2 summarizes the predictive accuracy of FF TEG andROTEM FIBTEM in various clinical settings. MA and MCFare the main parameters used for the predictions of hypofib-rinogenemia and blood transfusions.Theprediction accuracywas evaluated by sensitivity, specificity, and area under thereceiver operating characteristic curve (AUC) and variateregression analyses. Different cut-off values of fibrinogenconcentrations ranging from 1 to 1.8 g/L were used to definehypofibrinogenemia. Traditionally, a plasma fibrinogen levelof 1 g/L was established for fibrinogen replacement in patientswith congenital fibrinogen deficiency, whereas the thresholdvaried from 0.8 to 2.0 g/L in patients with acquired fibrinogendeficiency [14]. In contrast, a critical fibrinogen concentrationof 2.29 g/L was identified in trauma below which a significant

BioMed Research International 13
Table2:Clinicalevaluatio
nof
TEGandRO
TEM
functio
nalfi
brinogen
tests
ford
iagn
osisof
coagulop
athy
(hypofi
brinogenem
ia),predictio
nof
transfu
sionrequ
irementsandmortality.
Clinicalsettings
Stud
ydesig
nandpatients
Bloo
dcollectionandanalysis
Find
ings
Ref.
FFTE
G
Trauma
Rand
omized
controlledtrialoftraum
apatientsa
tris
kof
significanth
emorrhage(
n=45,ISS=18-29)
receivingeither
6gfib
rinogen
concentrate
(RiaSTAP�
)orp
lacebo
(normalsalin
e)
Citrated
who
lebloo
dwas
collected
from
the
rand
omized
traumap
atientsa
tadm
ission,
1-,3-,11-,
23-a
nd47-h
post-
infusio
ntim
e.Standard
FFTE
Gwas
perfo
rmed
onacompu
teriz
edTE
GHem
ostasis
Syste
m5000
(Haemon
eticsC
orpo
ratio
n,Haemoscope
Division
,Niles,IL,U
SA)a
ccording
tothemanufacturer’s
protocol.
FFTE
GMApredictedhypo
fibrin
ogenem
ia(fibrinogen
concentration<1g
/L)and
24-h
plasmatransfusio
nwith
high
accuracies
(AUC=
0.95,p=0
.002
andAU
C=0.70,p=0
.042).
[30,31]
Aprospectives
tudy
of182adulttraum
apatientsw
itham
edianISSof
17(9-26)
Bloo
dwas
sampled
immediatelyup
onarriv
alto
traumac
entre
andevaluatedin
tissuefactor-activ
ated
andplateletinhibitedTE
G(i.e.FF
TEG)p
recisely1h
after
samplingby
ahem
ostasis
analyzer
syste
m(TEG
5000
,Haemon
eticsC
orp.,B
raintre
e,MA)a
ccording
tothem
anufacturer’s
recommendatio
ns.A
llanalyses
were
cond
uctedat37∘C.
Sensitivity,specificity
andAU
Cof
FFTE
GMAford
etectio
nof
fibrin
ogen<1.5
g/Lwe
re77%,81%
and0.869,respectiv
ely.FF
TEGMAwas
also
aunivaria
tepredictorsof
massiv
etransfu
sion(>10
units
ofRB
Cs)at6
and24
hwith
oddratio
sof
0.79,0.82andmortalityat28
days
with
ahazardratio
of0.84.
[35,63]
Cardiac
surgery
Aprospectiveo
bservatio
nalstudy
of105child
renless
than
5yearso
fage
undergoing
congenitalh
eart
surgerywith
CPB
Who
lebloo
dsamples
were
collected
viaind
welling
arteria
lcathetersbefore
andaft
erCP
B.FF
TEGand
kaolin
heparin
aseT
EGwe
reperfo
rmed
ontheT
EG5000
with
company’sreagentsby
asingletechnician,
with
in20
min
ofcollectionof
thes
amples.P
lasm
afib
rinogen
levelswe
redeterm
ined
bytheC
lauss
metho
dusingthecommercialreagentsand
instr
ument(STAFibrinogen,D
iagn
osticaStago).
FFTE
GMApredictedhypo
fibrin
ogenem
ia(fibrinogen
concentration<2g/L)
with
AUCof
0.71
(95%
CI0.59-0.83)
[40]

14 BioMed Research International
Table2:Con
tinued.
Clinicalsettings
Stud
ydesig
nandpatients
Bloo
dcollectionandanalysis
Find
ings
Ref.
ROTE
MFIBT
EM
Trauma
Rand
omized
controlledtrialoftraum
apatientsa
tris
kof
significanth
emorrhage(
n=45,ISS=18-29)
receivingeither
6gfib
rinogen
concentrate
(RiaSTAP�
)orp
lacebo
(normalsalin
e)
Citrated
who
lebloo
dwas
collected
from
thetraum
apatientsa
tadm
ission,
1-,3-,11-,
23-a
nd47-h
post-
infusio
ntim
e.Standard
ROTE
MFIBT
EMwas
perfo
rmed
onaR
OTE
Mdelta
syste
m(Tem
Inno
vatio
nsGmbH
,Mun
ich,Germany;succeeded
byInstr
umentatio
nLabo
ratory,B
edford,M
A,U
SA)
accordingto
them
anufacturer’s
protocol.
ROTE
MFIBT
EMMCF
predictedhypo
fibrin
ogenem
ia(fibrinogen
concentration<1g
/L)and
24-h
plasma
transfu
sionwith
high
accuracies
(AUC=
0.96,p<0.00
1)and
AUC=
0.72,p=0
.023).
[30,31]
Aprospectiveo
bservatio
nalstudy
of88
trauma
patientsa
nmedianISSscoreo
f22(12-34)
Bloo
dsamples
were
collected
immediatelyaft
erthe
patient’sarriv
alto
thetraumar
oom
(H0)
andat6h
(H6),12h(H
12)a
nd24
h(H
24)afte
radm
ission,
representin
gatotalof
270samples.Th
eROTE
Mmeasurementsandsta
ndardcoagulationtests
were
perfo
rmed
with
in2hof
collectionof
bloo
dsamples.
Sensitivity,specificity
andAU
Cof
FIBT
EMA10
ford
etectio
nof
fibrin
ogen<1g
/Lwe
re91%,85%
and0.96,respectively.
[45]
Aretro
spectiv
eanalysis
ofdatafrom
323p
atients
with
aninjury
severityscore(
ISS)≥16
(20-50)
Bloo
dsamples
were
takenim
mediatelyup
onadmissionto
ER.R
OTE
Manalyses
(EXT
EM,
INTE
M,FIBTE
M)w
eretypicallyperfo
rmed
atthe
bedsidew
ithin
minutes
ofsamplec
ollection.
Fibrinogen
concentrationwas
measuredby
the
Claussmetho
d(STA
-Fib�assay(Roche
Diagn
ostics
GmbH
);op
ticalread-out),usingaS
TA-C
ompact�
machine
(Roche
Diagn
osticsG
mbH
,Vienn
a,Au
stria).
Sensitivity,specificity
andAU
Cof
FIBT
EMA10/M
CFfor
predictio
nof
massiv
etransfusio
n(≥10
units
RBCtransfu
sedin
24h)
63.3/77.5
%,83.2/74.9%,0.83/0.84
(95%
CI0.78-0.87/0.79-0.88),sim
ilartofib
rinogen
concentration
[64]
Aprospectivec
ohortstudy
of517traumap
atients
with
amedianISSof
14(8-27)
Bloo
dwas
draw
nfrom
either
thefem
oralvein
orantecubitalfossa
into
a2.7-mLcitrated
vacutainer
with
in20
min
ofarriv
alin
thee
mergency
department(ED
).RO
TEM
tests
were
perfo
rmed
with
in2hof
bloo
ddraw
with
aROTE
Mdelta
instr
ument,at37∘C.
Sensitivity,specificity
andAU
Cof
FIBT
EMA5ford
etectio
nof
fibrin
ogen<1.5
g/L87%,70%
and0.8(95%
CI0.7-0.9)
[3]
Aprospective,sin
gle-center,n
on-in
terventio
nal,
non-controlled,op
enclinicalstu
dyof
50tra
uma
patientsw
itham
edianISSof
13(4-66)
Bloo
dwas
collected
atho
spitaladm
ission,
3-and
24-h
after
admissionandanalyzed
byRO
TEM
assays
(EXT
EMandFIBT
EM).EX
TEM
was
considered
positiveifo
neof
thefou
rprin
ciplep
aram
eters(CT
,CF
T,MCF
,and
Maxim
umLysis)g
reater
than
20%
oftheexpected
highesto
rlow
estn
ormalvalueo
fthe
manufacturern
ormalvaluer
anges(CT≥94,C
FT≥
190,MCF≤40
,ML≤12).FIBT
EMwas
considered
positiveifM
CFwas
atleast2
0%sm
allerthanthe
expected
meanno
rmalvalue(MCF≤7).
Sensitivity,specificity
andAU
Cof
FIBT
EMMCF<7mm
with
inno
rmalEX
TEM
patientsa
re100%
,90.2%
,0.951
and
0%,87.5
%,0.563
forp
redictions
ofcoagulop
athy
(INR≥
1.3)
andmortalityat30
days
[65]
Aprospectives
tudy
of182adulttraum
apatientsw
itham
edianISSof
17(9-26)
Bloo
dwas
sampled
immediatelyon
hospitalarrival.
FIBT
EMassays
were
perfo
rmed
with
citrated
bloo
dprecise
ly1h
after
samplingaccordingto
the
manufacturer’s
recommendatio
ns.F
ibrin
ogen
level
was
determ
ined
byClaussmetho
d.
Sensitivity,specificity
andAU
Cof
FIBT
EMMCF<10
mm
were
80%,89%
and0.889ford
etectio
nof
fibrin
ogen<1.5
g/L.
[35]

BioMed Research International 15
Table2:Con
tinued.
Clinicalsettings
Stud
ydesig
nandpatients
Bloo
dcollectionandanalysis
Find
ings
Ref.
Aprospectivec
ohortstudy
of334blun
ttraum
apatients(ISS≥
15or
Glasgow
Com
aScore≤
14).
Citrated
bloo
dwas
collected
atho
spitaladm
ission.
ROTE
Mtests
were
perfo
rmed
accordingto
the
manufacturer’s
instr
uctio
ns,u
singequipm
entand
testreagentsprovided
byTem
InternationalG
mbH
.Lo
gisticr
egressionmod
elswe
reused
toevaluate
ROTE
Mtests
forp
redictionof
24-h
deathand6-h
transfu
sions.
FIBT
EMMCF
with
acut-offof
7mm
predictedtheneed
for
RBCtransfu
sionwith
anod
dratio
of0.92
(95%
CI0.87–0.98)
[46]
Cardiac
surgery
Aprospective,ob
servationalpilo
tstudy
of35
patientsu
ndergoingelectiv
ecardiacs
urgery
oncardiopu
lmon
arybypass(C
PB)for
cyanotic
congenitalh
eartdisease
Citrated
bloo
dwas
collected
after
indu
ctionof
anesthesiaandanalyzed
byRO
TEM.N
odetails
were
provided.Fibrin
ogen
concentrationassaywas
not
provided.
ROTE
MFIBT
EMMCF
ishighly
predictiv
eofh
ypofi
brinogenem
ia(fibrinogen<1.5
g/L)
(AUC=
0.99).
[47]
Arand
omized,placebo
-con
trolledtra
ilof
116high-risk
patientsu
ndergoingcardiacs
urgery
with
CPB
ROTE
MFIBT
EMwas
perfo
rmed
20min
before
removalof
thea
ortic
cross-cla
mp,aft
erfib
rinogen
supp
lementatio
n.Fibrinogen
concentrations
were
measuredup
onarriv
alin
ICUaccordingto
aph
oto-op
ticalClaussmetho
d.
FIBT
EMMCF
with
theb
estcut-offvalueo
f14mm
yieldeda
good
discrim
inativep
ower
forsevereb
leedingwith
anAU
Cof
0.721,sensitivity
of80%,specificity
of72%
[52]
Aretro
spectiv
eobservatio
nalstudy
of1077
patients
undergoing
cardiacs
urgery
with
CPB.
Citrated
bloo
dwas
collected
durin
gther
ewarming
phase(≥36∘C)
.EXT
EMandFIBT
EMwe
recond
uctedat37∘Cas
perm
anufacturer’s
reagentsand
procedures.Fibrin
ogen
concentrationwas
measured
bytheC
laussm
etho
dusingSTAREv
olution(Stago,
Paris
,France).
Theo
ptim
alFIBT
EMA10
cut-o
ffford
iagn
osisof
afibrinogen
concentration<1.5
g/Lwas≤8mm
with
anAU
Cof
0.95.
[51]
Aprospectiveo
bservatio
nalstudy
of110
patients
undergoing
cardiacs
urgery
with
CPB.
Citrated
who
lebloo
dwas
sampled
from
acentral
veno
uslin
eorfrom
thee
xtracorporealcirc
uitat
pre-CP
B,on
-CPB
,post-C
PB.R
OTE
Massays
ofIN
TEM,E
XTEM
,FIBTE
MandHEP
TEM
were
perfo
rmed
at37∘Cby
certified
bioanalytical
technicians.Plasmalevelsof
fibrin
ogen
were
measuredusingtheC
lausstechn
ique
ona
coagulationanalyzer
(BCS
,DadeB
ehrin
gInc.,
Germany)
usingtheM
ultifi
bren
U-Reagent
accordingto
manufacturer’s
specificatio
ns.
Anon
-CPB
FIBT
EMA10≤10
mm
identifi
edpatientsw
itha
post-
CPBClaussfib
rinogen
of≤1.5
g/Lwith
asensitivity
of0.99
andap
ositive
predictiv
evalueo
f0.60.
[53]
Aretro
spectiv
eand
observationalstudy
of119
child
ren<10
yearso
ldun
dergoing
congenitalcardiac
surgerywith
CPB.
Bloo
dwas
collected
twiced
uringsurgery,aft
eranesthesiaindu
ctionandCP
B.RO
TEM
EXTE
Mand
FIBT
EMwe
reperfo
rmed
with
citrated
bloo
daccordingto
them
anufacturer’s
recommendatio
ns.
Intraoperativ
eexcessiv
ebloo
dlosswas
defin
edas
estim
ated
bloo
dloss≥50%
ofestim
ated
bloo
dvolume.Lo
gisticr
egressionmod
elsw
ereu
sedto
identifypredictorsfore
xcessiv
eblood
loss.
Post-
CPBFIBT
EMCA
10<5m
mpredictedmassiv
eblood
loss
with
anod
dratio
of11.1(95%
CI2.6-47.3,p=0
.001)and
AUC
of0.83.
[41]

16 BioMed Research International
Table2:Con
tinued.
Clinicalsettings
Stud
ydesig
nandpatients
Bloo
dcollectionandanalysis
Find
ings
Ref.
Livertransplantatio
n(LT)
Aretro
spectiv
eobservatio
nalstudy
of295patients
(254
livingdo
norsand41
LTpatients).
Citrated
bloo
dwas
collected
from
1haft
erindu
ction
ofgeneralanesth
esia,1
haft
ersurgicalincisio
n,30
min
after
hepatectom
y,30
min
after
graft
reperfusion,
andaft
erhepatic
artery
anastomosis.
ROTE
M�tests
(EXT
EM,INTE
MandFIBT
EM)w
ere
routinelyperfo
rmed
accordingto
them
anufacturer’s
instr
uctio
ns.F
ibrin
ogen
concentrationwas
measured
usingtheD
adethrom
binreagent(Siem
ens
Health
care
Diagn
ostics,Erlangen,G
ermany)
andan
automaticcoagulationanalyzer
(Sysmex
CA-700
0,Siem
ensH
ealth
care
Diagn
ostics,Erlangen,
Germany).
FIBT
EMMCF<8m
mpredictedhypo
fibrin
ogenem
ia(fibrinogen<1.2
8g/L)
with
asensitivity
of82%,a
specificityof
90%
andAU
Cof
0.94.
[55]
Aprospectives
tudy
of253patientsreceiving
orthotop
icliver
transplantation.
Citrated
bloo
dsamples
were
collected
after
indu
ction
ofgeneralanesth
esia,atthe
endof
theh
epatectomy,
20min
after
graft
revascularization,
and90
min
after
graft
revascularization.
Theb
lood
samples
were
teste
djustaft
ercollectionby
ROTE
Mgammadevice
operated
accordingto
manufacturerinstructio
nsand
with
thetypea
ndconcentrationof
reagentsas
provided
byPentapharm
(Mun
ich,Germany).
Fibrinogen
concentrationwas
measuredby
the
PT-derived
metho
d,with
values
below2g/Lbeing
checkedby
theC
laussmetho
d.
Sensitivity,specificity
andAU
Cof
FIBT
EMA10
ford
etectio
nof
plasmafi
brinogen
level(<1.3
g/L)
86%,55%
and0.801
[56]
Aretro
spectiv
e,sin
gle-centre,observatio
nalstudy
of243a
dultliver
transplant
patients
Bloo
dsamples
were
collected
immediatelyup
onadmissionto
ICUandon
cedaily
until
thes
eventh
posto
perativ
eday.R
OTE
Mtests
inclu
ding
EXTE
M,
INTE
M,and
FIBT
EMwe
reperfo
rmed.Stand
ard
labo
ratory
tests
(PT,aPTT
,fibrinogen)w
ere
perfo
rmed
usingaBC
SAnalyzer(Siem
ens
Health
care
Diagn
osticsP
rodu
ctsG
mbH
,Erla
ngen,
Germany).
FIBT
EMA10/M
CFpredictedpo
stoperativ
ebleedingwith
asensitivity
of90/90%
,specificity
of33/32%
,AUCof
0.636/0.632,bette
rthanfib
rinogen
concentrationwith
74%,
39%
and0.531
[66]
Aprospectiveo
bservatio
nalstudy
of23
patients
undergoing
orthotop
icliver
transplantation.
Bloo
dsamples
were
collected
after
indu
ctionof
generalanaesthesia,d
uringhepatectom
y,atthe
anhepatic
stage,30–
60min
after
graft
revascularization,
atthee
ndof
surgery,and24
haft
ersurgery.RO
TEM
tests
(EXT
EM,INTE
M,FIBTE
MandAPT
EM)w
ereperfo
rmed
intheo
peratin
gtheatre
andby
theanaesth
esiologists
treatingthe
patientsa
ccording
tothem
anufacturer’s
instr
uctio
nsusingequipm
entand
testreagentsprovided
byPentapharm
GmbH
.Plasm
afib
rinogen
concentrationwas
determ
ined
bytheC
laussm
etho
dperfo
rmed
onAC
LTo
pautomates
(Instr
umentatio
nLabo
ratory,L
exington
,MA,U
SA).
ROTE
MFIBT
EMA10≤8mm
predictedhypo
fibrin
ogenem
ia(fibrinogen<1g
/L)w
ithas
ensitivity
of0.83,specificity
of0.35,and
AUCof
0.61,w
orse
than
EXTE
Mwith
correspo
nding
values
of0.83,0.75and0.84
[57]

BioMed Research International 17
Table2:Con
tinued.
Clinicalsettings
Stud
ydesig
nandpatients
Bloo
dcollectionandanalysis
Find
ings
Ref.
Aretro
spectiv
eof4
01patientsw
houn
derw
entliver
transplantation.
Bloo
dwas
sampled
at1h
after
indu
ctionof
general
anaesth
esia,1
haft
ersurgicalincisio
n,30
min
after
hepatectom
y,and30
min
after
graft
reperfusionand
after
hepatic
artery
anastomosis.
Atotalof1125
FIBT
EMtests
were
perfo
rmed
accordingto
the
manufacturer’s
instr
uctio
ns.F
ibrin
ogen
levelw
asmeasuredusingtheD
adeTh
rombinRe
agent
(SiemensH
ealth
care
Diagn
ostics)andan
automatic
coagulationanalyser
(Sysmex
CA-700
0,Siem
ens
Health
care
Diagn
ostics).
ROCcurvea
nalysis
show
edthatac
ut-offvalueo
fFIBTE
MA5
at4mm
andA10
at5mm
predictedfib
rinogen<1g
/Lwith
asensitivity
of81%
and76%,specificity
of77%
and82%,A
UC
of0.86
and0.87
[58]
Postp
artum
hemorrhage
Aprospectiveo
bservatio
nalstudy
of91
women
atthe
third
trim
estero
fpregn
ancy:37with
postp
artum
haem
orrhage(stu
dygrou
p)and54
with
outabn
ormal
bleeding.
Standard
FIBT
EMwas
carriedou
tbyclinicians
with
citrated
bloo
dsamples
inthed
eliveryroom
.Plasm
afib
rinogen
was
assayedwith
in5min
after
sampling
with
aSTARautomated
coagulationanalyser
(Diagn
osticaStagoInc.,
Franconville,France)
accordingto
stand
ardprocedures.
Acut-o
ffvalueo
fA5andA15
at6mm
provided
ansensitivity
of100%
forb
othparameters,as
pecificity
of85
and88%,and
AUCof
0.96
and0.97,respectivelyto
detectafi
brinogen
level
<1.5
g/Lin
postp
artum
haem
orrhage.
[59]
Aprospectiveo
bservatio
nalpilo
tstudy
inclu
ding
217
healthypregnant
women
Bloo
dsamples
were
collected
upon
admissionto
the
deliveryroom
forlabor
andwith
in1h
after
vaginal
delivery.AllRO
TEM
tests
were
perfo
rmed
with
the
recommendedreagentsandin
accordance
with
the
manufacturer’s
procedures.Fibrin
ogen
levelswe
remeasuredwith
STA-
fibrin
ogen
reagent(Ro
che
Diagn
osticsG
mbH
,Mannh
eim,G
ermany)
using
Claussmetho
d.
TheA
UCof
ROTE
MFIBT
EMMCF
forp
redictionof
postp
artum
hemorrhaged
efinedas
bloo
dloss≥500mLwas
0.52
(95%
confi
denceinterval0.41–0.64
,p=0
.699),sim
ilarto
thep
redictivep
ower
offib
rinogen
levels(AUC=
0.53,95%
confi
denceinterval0.40–
0.65,p=0
.644
).
[67]
Neurosurgery
Aprospectiveo
bservatio
nalstudy
of92
patients
undergoing
emergent
neurosurgery
Bloo
dwas
sampled
intheop
eratingtheatero
ncitrated
tubesa
ndRO
TEM
analyses
were
perfo
rmed
with
inmin
ofbloo
dsamplingby
anesthesianu
rsesor
physicians
trainedto
perfo
rmtheR
OTE
Mtests
accordingto
them
anufacturer’s
instr
uctio
ns.P
lasm
afib
rinogen
concentrationwas
determ
ined
byClauss
metho
d(Siemens-DadeBe
hringHealth
care
Diagn
ostics,Marbu
rg,G
ermany).
Then
eedfortransfusio
n(≥
3PR
BCs)was
bestpredictedby
EXTE
MandFIBT
EMMCF
(AUCof
0.72
and0.71,
respectiv
ely)
andby
fibrin
ogen
concentration(AUCof
0.70),
with
asensitivity
of38.2,33.3
,25.6%
andspecificityof
85.1,
96.2and100%
.
[60]
AUC=
Areau
nder
thereceiver
operatingcharacteris
ticcurve;CI
=Con
fidence
Interval;C
PB=C
ardiop
ulmon
aryBy
pass;ICU
=Intensiv
eCareU
nit;ISS=
Injury
SeverityScore

18 BioMed Research International
increase inmortality occurred [106].The discrepancy impliesthat the negative impact of fibrinogen deficiency in traumamay have been underestimated. It should also be notedthat hypofibrinogenemia prevalence in major bleeding variesacross clinical contexts [107].
Most clinical studies are prospective observational, whilea few are retrospective and randomized controlled. Samplesize ranged from 23 to 1077 patients. In contrast withROTEM, FF TEG has been used less to detect hypofibrino-genemia and predict blood transfusion requirements with afocus on trauma patients. Among various clinical settings,ROTEM FIBTEM has been mostly used in trauma, cardiacsurgery, and liver transplantation with best predictive powerfor hypofibrinogenemia (fibrinogen <1.5 g/L) (AUC=0.99)in cardiac surgery [47]. Furthermore, several studies haveshown that FF TEG and ROTEM FIBTEM could predictbleeding and transfusion requirements in trauma [63, 64],cardiac surgery [52], and liver transplantation [58, 66] withvarious accuracies. It appeared that ROTEMwould have bet-ter predictive accuracy than TEG because it has greater speci-ficity for some common coagulopathies in cardiac surgery,such as fibrinogen deficiency. The averaged likelihood ratioof FF TEG MA for diagnosis of hypofibrinogenemia is4.71±2.18 based on a number of studies [30, 35, 40], while thecorresponding value of ROTEM FIBTEM MCF is 9.24±2.64calculated from the literature [30, 35, 55].
Two studies evaluated ROTEM devices in patients withpostpartum hemorrhage (PPH). One study provided data onthe ability of ROTEM FIBTEM to predict hypofibrinogene-mia (<1.5 g/L) [59]; the other evaluated the predictive powerof ROTEM FIBTEM and Clauss fibrinogen for PPH andfound no associations between the prepartum coagulationparameters and blood loss defined as blood loss ≥ 500 mL[67]. Alternatively, one study showed that FF TEG MAwith a cut-off value of 12.1 mm could predict obstetriccomplications in nonpregnant dysfibrinogenemia patientswith a sensitivity of 100%, specificity of 69.2%, and AUC of0.923, but could not distinguish patients with bleeding andnonbleeding symptoms [108].
Only a few studies demonstrated ROTEM FIBTEM pro-vided faster and better prediction than plasma fibrinogenconcentration formassive transfusion [64] and bleeding [66],respectively. ROTEM FIBTEM provided early prediction ofmassive transfusion in trauma similar to the most predic-tive laboratory parameters (e.g., fibrinogen and hemoglobinconcentrations) [64]. A separate study comparing standardfibrinogen measurement methods (i.e., Clauss method andthrombin clotting time) with ROTEM FIBTEM in patientswith cirrhosis suggested FIBTEM as a promising alternativeto standard plasma fibrinogen measurement in cirrhoticpatients, especially in evaluating fibrin polymerization disor-ders in these patients [62].
There is insufficient evidence or low-quality evidencefor the benefits of TEG and ROTEM for the prediction ofbleeding and adverse outcomes beyond that achieved usingroutinely measured baseline factors or conventional coag-ulation tests (CCTs) except for rapidity. ROTEM EXTEMand FIBTEM were no better than routine laboratory testsfor detecting differences between surviving and nonsurviving
critically ill patients [109]. ROTEM FIBTEM was unableto predict PPH and not superior to CCTs in a prospectiveobservational study of 217 healthy pregnant women [67].On the other hand, ROTEM FIBTEM was not a good testto predict the presence of acute coagulopathy of traumadefined as an international normalized ratio (INR) > 1.3 ora fibrinogen level < 1.5 g/L unless combined with EXTEM,and either of the tests could predict the need for emergentblood product transfusions (defined as ≥5 units of red bloodcells (RBC) and ≥3 units of plasma within the first 24 hof care) [65]. The use of CCTs such as INR in trauma hasbeen severely criticized due to the lack of association withbleeding and blood transfusion. It has been reported thatINR overestimated coagulopathy should not be used to guideblood transfusion in stable trauma and surgical patients [110].
Finally, if fibrinogen deficiency has a causal relationshipwith bleeding and adverse clinical outcomes, it is sensibleto suggest that TEG and ROTEM functional fibrinogen teststhat improve clinical prediction for fibrinogen-related bleed-ing may also have the potential to predict adverse clinicaloutcomes. However, randomized trials are needed to providehigh-quality evidence for the role of TEG and ROTEMin diagnosis, management, and monitoring of fibrinogenfunction and replacement in bleeding patients.
It is noteworthy that recently two large randomized trials,CRASH-2 (Clinical Randomisation of an Antifibrinolyticin Significant Haemorrhage 2) [111] and WOMAN (WorldMaternal Antifibrinolytic) [112], provide high-quality evi-dence for the early use of tranexamic acid for a survivaladvantage to many bleeding patients. An in vitro studyshowed that the antifibrinolytic reduced fibrinogenolysis inaddition to the correction of fibrinolytic effects on TEG (MA,LY) values in the presence of tissue plasminogen activator[113].
6. Comparison between TEG and ROTEM forFunctional Fibrinogen Assays
A number of studies compared the reagents and devicesbetween FF TEG and ROTEM FIBTEM. Solomon et al.showed that FF TEG MA was larger than FIBTEM MCFwhen performed with either their standard assay reagents(lyophilized tissue factor and abciximab on TEG and acombination of ex-tem and fib-tem on ROTEM) or the sameassay reagent [71]. In addition, the FF TEG reagent producedhigher values than the FIBTEM reagent on both TEG andROTEM. Schlimp et al. compared different fibrinogen assaysin eliminating platelet effects on TEG MA and ROTEMMCF. It was found that abciximab based on glycoproteinIIb/IIIa inhibition was less effective at inhibiting the plateletcontribution to clot strength than cytochalasin D based onprevention of platelet cytoskeletal reorganization, resulting inlarger FF TEGMA compared to ROTEM FIBTEMMCF andaffecting their correlations and changes with fibrinogen con-centration. In addition, the combination of both inhibitionsprovided the most accurate assessment of the clot strengthand fibrinogen function [114]. It has been speculated that theROTEM FIBTEM reagent might contain stabilizing agents(e.g., dimethyl sulfoxide) and more tissue factors than the

BioMed Research International 19
FF TEG reagent [115]. These results are consistent with otherstudies comparing TEG and ROTEM functional fibrinogenassays forwhole blood from surgical patients [48, 116], traumapatients, and healthy volunteers [91, 114].
However, the differences between FF TEG MA andROTEMFIBTEMMCFobtained using the same reagents [71,115] imply that TEG system itself may also be a contributingfactor. The hardware differences between the two systemsinclude the mechanisms for cup/pin rotation, detection ofthe rotation, cup materials, and interior surface properties[117, 118].
Meyer et al. compared different TEG and ROTEMtests including FF TEG and FIBTEM, and Clauss methodfor detection of trauma-induced coagulopathy and goal-directed transfusion therapy [34]. Specifically, FF TEG andROTEM FIBTEM early amplitudes (A5, 10) and MA/MCFhad similar correlations with Clauss fibrinogen level andcould differentiate coagulopathic and transfused patientsfrom noncoagulopathic and nontransfused patients.
Pruller et al. compared fibrinogen assays using FF TEGand ROTEM FIBTEM in surgical patients in terms oftheir MA and MCF values, and correlations with Claussfibrinogen level [116]. It was found that FF TEG MA washigher than ROTEM FIBTEMMCF and their MA and MCFcorresponded to different Clauss fibrinogen levels. The FFTEGMA showed a weaker correlation with Clauss fibrinogenthan ROTEM FIBTEMMCF (R2=0.542 vs. 0.671).
Different TEG (Rapid, Kaolin, and FF) and ROTEMtests (EXTEM, INTEM, and FIBTEM) were compared fortheir sensitivity to detect fibrinolysis induced by tissue plas-minogen activator in whole blood [119]. Compared to othertests, FF TEG and ROTEM FIBREM provided more rapiddetection of fibrinolysis, but FF TEG detected changes inclot strength as well. Comparison of tissue factor-triggeredROTEM FIBTEM and EXTEMwith contact-activated kaolinTEG in patients undergoing liver transplantation showedthe highest and lowest hyperfibrinolysis detection rates byFIBTEM and kaolin TEG, respectively, suggesting the effectsof coagulation activators and platelet inhibitors on sensitivityto identifying hyperfibrinolysis [120].
In contrast with hyperfibrinolysis detection, we foundonly kaolin TEG and ROTEM EXTEM as the methodsof measuring hypofibrinolysis (also called fibrinolysis shut-down) instead of FF TEG and ROTEM FIBTEM. In onestudy of 914 trauma patients (ISS≥15), the threshold forhypofibrinolysis was determined for EXTEM ML at 5.5%with a sensitivity of 61.6% and specificity of 58.4% [121]. Thestudy reported 29.9% hypofibrinolysis. In another study of550 severe trauma patients with a median ISS of 19, EXTEMML<3.5% was selected to define hypofibrinolysis with asensitivity 42.5% and specificity 76.5% [122]. The methodidentified 25.6% hypofibrinolysis. A number of studies haveused TEG in particular kaolin TEG LY30<0.81% to detecthypofibrinolysis in trauma patients with a median ISS of25 [123, 124]. These studies reported fibrinolysis phenotypeswith different prevalence: hypofibrinolysis at 29.9%, 25.6%,and 46%; physiologic fibrinolysis at 63.0%, 70.7%, and 36%.The ROTEM method indicated physiologic fibrinolysis as
the predominant phenotype with 63% [121] and 71% [122]followed by hypofibrinolysis, while the TEG method showedhypofibrinolysis as the most common phenotype with 46%followed by physiologic fibrinolysis with 36% [124]. Thediscrepancy could be the difference in patients’ characteristics(e.g., ISS) and the method itself (tissue factor-activatedROTEMEXTEM vs. contact-activated kaolin TEG). A recentretrospective analysis of the Pragmatic, Randomized Opti-mal Platelet and Plasma Ratios (PROPPR) trial found 61%of hypofibrinolytic patients as determined by kaolin TEGLY30<0.9%, followed by 22% of hyperfibrinolytic patientsbased on LY30≥3% [125]. The study also suggested thathypofibrinolysis did not reflect shutdown of enzymaticfibrinolysis with hypercoagulability, but rather a type ofcoagulopathy characterized by fibrinolytic activation withconcurrent fibrinogen consumption and platelet dysfunction.
There is a lack of studies to compare the utilities ofTEG and ROTEM for diagnosis of coagulopathy, predictionof mortality, and the requirement for massive transfusion,although both have been reported useful [45, 126]. Weconducted a comparative study of functional fibrinogenassays using TEG and ROTEM in trauma patients [30] todetermine (1) their interchangeability of the key parametervalues obtained by the two systems in all trauma patientsas well as severe trauma patients randomized to receivetheir fibrinogen concentrate or placebo (normal saline), and(2) utility of each system for predicting clinical outcomesand monitoring any changes in coagulation profiles in thetrauma patients randomized for treatment with fibrinogenconcentrate or placebo. In addition, a crossover analysis(ex-tem and fib-tem on TEG) was conducted to confirmwhether the assay reagents or the device could contribute tothe observed differences. Overall, we found that TEG andROTEM parameter values were correlated, being strongestbetween MA and MCF, but were significantly different, andtheir agreement fell outside acceptable limits and thus theirvalues were not interchangeable, arguably due to differencesin both devices and assay reagents used. Specifically, ROTEMFIBTEM MCF had a higher correlation with Clauss fibrino-gen (𝜌=0.87 vs. 0.75) and lower value than FF TEG MA(17.1±8.0 mm vs. 22.4±7.5 mm). Clinically, TEG MA andROTEM MCF showed reasonable predictive accuracy forplasma transfusion, but poor accuracy for any red bloodcells and cryoprecipitate transfusions. Both well predictedhypofibrinogenemia (fibrinogen concentration < 1 g/L) withAUC of 0.95 and 0.96. ROTEM FIBTEM MCF seems to bemore consistent with the duration of the between-group dif-ference as indicated by fibrinogen levels than FF TEGMA. Inaddition, ROTEM FIBTEM detected changes in coagulationtime (CT) and clot lysis (LI30) over hospitalization time as aresult of fibrinogen treatment.
In a study similar to ours, TEG and ROTEM werecompared for functional fibrinogen assays in trauma todetermine specific cut-offs of TEGMAand ROTEMMCF foran increased risk of receiving a transfusion [35]. It was foundthat FF TEGMA and ROTEM FIBTEMMCF correlated well(𝜌=0.71, p<0.001) and had the same correlation coefficientwith Clauss fibrinogen level (𝜌=0.64, p<0.001). Figure 2shows a strong correlation between FFTEGMAand ROTEM

20 BioMed Research International
Peng 2018Meyer 2015
r=0.77, p<0.00195% Confidence Interval
0
10
20
30
40
50
ROTE
M F
IBTE
M M
CF (m
m)
10 20 30 40 500FF TEG MA (mm)
Figure 2: Comparison of FF TEGMA values and ROTEM FIBTEMMCF values.The correlation coefficientwas obtained through linearregression of pooled data from Peng 2018 [30] and Meyer 2015[35]. MCF=0.8384MA-1.065 (R2=0.5938). The means ± standarddeviations of FF TEGMAandROTEMFIBTEMMCF are 20.63±7.11mm and 16.23±7.73 mm (n=363).
FIBTEMMCF (r=0.77, p<0.001) based on the pooled data ofour study [30] and Meyer et al. [35], but a larger FF TEGMAthan ROTEM FIBTEM MCF on average (20.63±7.11 mm vs.16.23±7.73mm, n=363, p<0.001).
7. Conclusions
TEG and ROTEM functional fibrinogen tests play importantroles in diagnosis of fibrinogen-related coagulopathy andtransfusion requirements including fibrinogen replacement.The clot strength of FFTEGandROTEMFIBTEM is themostused parameter for discrimination of fibrinogen deficienciesand their correlations with Clauss fibrinogen levels are varieddepending on patient population and range of fibrinogenconcentrations. When using FF TEG and ROTEM FIBTEMto diagnose fibrinogen deficiency and predict transfusionrequirements other variables such as hematocrits, factorXIII levels and fibrinogen concentrate ranges should betaken into consideration. Both TEG and ROTEM have beenused to detect systemic fibrinolysis (physiologic, hypo, andhyperfibrinolysis). Studies comparing FF TEG and ROTEMFIBTEM suggest a stronger correlation of the latter withplasma fibrinogen concentration, likely due to its moreeffective elimination of platelet contribution to clot strength.We should be aware that the studies supporting the use TEGand ROTEM are limited for trauma and surgical bleedingpatients. Even without robust clinical data, TEG and ROTEMare likely to remain popular for the hemostatic managementof bleeding patients.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
References
[1] J. H. Levy, F. Szlam, K. A. Tanaka, and R. M. Sniecienski,“Fibrinogen and hemostasis: A primary hemostatic target forthe management of acquired bleeding,” Anesthesia & Analgesia,vol. 114, no. 2, pp. 261–274, 2012.
[2] D. Fries and W. Z. Martini, “Role of fibrinogen in trauma-induced coagulopathy,” British Journal of Anaesthesia, vol. 105,no. 2, pp. 116–121, 2010.
[3] C. Rourke, N. Curry, S. Khan et al., “Fibrinogen levels duringtrauma hemorrhage, response to replacement therapy, andassociation with patient outcomes,” Journal of Thrombosis andHaemostasis, vol. 10, no. 7, pp. 1342–1351, 2012.
[4] Y. Kimura, S. Kimura, S. Sumita, andM. Yamakage, “Predictorsof hypofibrinogenemia in blunt trauma patients on admission,”Journal of Anesthesia & Clinical Research, vol. 29, no. 2, pp. 242–248, 2015.
[5] K. Inaba, E. Karamanos, T. Lustenberger et al., “Impact offibrinogen levels on outcomes after acute injury in patientsrequiring a massive transfusion,” Journal of the AmericanCollege of Surgeons, vol. 216, no. 2, pp. 290–297, 2013.
[6] Z. K. McQuilten, E. M.Wood,M. Bailey, P. A. Cameron, and D.J. Cooper, “Fibrinogen is an independent predictor of mortalityin major trauma patients: A five-year statewide cohort study,”Injury, vol. 48, no. 5, pp. 1074–1081, 2017.
[7] D. Whiting and J. A. Dinardo, “TEG and ROTEM: technologyand clinical applications,” American Journal of Hematology, vol.89, no. 2, pp. 228–232, 2014.
[8] C. J. Schlimp andH. Schochl, “The role of fibrinogen in trauma-induced coagulopathy,” Hamostaseologie, vol. 34, no. 1, pp. 29–39, 2014.
[9] S. Figueiredo, A. Tantot, and J. Duranteau, “Targeting bloodproducts transfusion in trauma: What is the role of thromboe-lastography?”Minerva Anestesiologica, vol. 82, no. 11, pp. 1214–1229, 2016.
[10] K.Gorlinger, L. Shore-Lesserson,D.Dirkmann,A.A.Hanke,N.Rahe-Meyer, andK. A. Tanaka, “Managementof hemorrhage incardiothoracic surgery,” Journal of Cardiothoracic and VascularAnesthesia, vol. 27, no. 4, pp. S20–S34, 2013.
[11] K. Goerlinger, “Coagulation management during liver trans-plantation,”Hamostaseologie, vol. 26, no. 3, pp. S64–S75, 2006.
[12] M. Ranucci, B. Martinez, D. Colella, and D. Haxhiademi, Point-of-care tests for severe hemorrhage: A manual for diagnosis andtreatment, Cham: Springer International Publishing, 2016.
[13] D. Spahn, G. Spahn, and P. Stein, “Indications and Risks ofFibrinogen in Surgery and Trauma,” Seminars in Thrombosisand Hemostasis, vol. 42, no. 02, pp. 147–154, 2016.
[14] J. H. Levy, I. Welsby, and L. T. Goodnough, “Fibrinogen as atherapeutic target for bleeding: A review of critical levels andreplacement therapy,” Transfusion, vol. 54, no. 5, pp. 1389–1405,2014.
[15] J. H. Levy and L. T. Goodnough, “How I use fibrinogenreplacement therapy in acquired bleeding,” Blood, vol. 125, no.9, pp. 1387–1393, 2015.
[16] J. Stensballe, S. R. Ostrowski, and P. I. Johansson, “Viscoelasticguidance of resuscitation,” Current Opinion in Anaesthesiology,vol. 27, no. 2, pp. 212–218, 2014.
[17] A. Wikkelsø, J. Wetterslev, A. M. Møller, and A. Afshari,“Thromboelastography (TEG) or rotational thromboelastom-etry (ROTEM) to monitor haemostatic treatment in bleedingpatients: a systematic review with meta-analysis and trialsequential analysis,”Anaesthesia, vol. 72, no. 4, pp. 519–531, 2017.

BioMed Research International 21
[18] M. Fahrendorff, R. S. Oliveri, and P. I. Johansson, “The useof viscoelastic haemostatic assays in goal-directing treatmentwith allogeneic blood products - A systematic review andmeta-analysis,” Scandinavian Journal of Trauma, Resuscitation andEmergency Medicine , vol. 25, no. 1, article no. 39, 2017.
[19] E. Gonzalez, E. E. Moore, H. B. Moore et al., “Goal-directedhemostatic resuscitation of trauma-induced coagulopathy apragmatic randomized clinical trial comparing a viscoelasticassay to conventional coagulation assays,”Annals of Surgery, vol.263, no. 6, pp. 1051–1059, 2016.
[20] G. F. Serraino and G. J. Murphy, “Routine use of viscoelasticblood tests for diagnosis and treatment of coagulopathic bleed-ing in cardiac surgery: Updated systematic review and meta-analysis,” British Journal of Anaesthesia, vol. 118, no. 6, pp. 823–833, 2017.
[21] P. Whiting, M. Al, M. Westwood et al., “Viscoelastic point-of-care testing to assist with the diagnosis, management andmonitoring of haemostasis: A systematic review and cost-effectiveness analysis,”Health TechnologyAssessment, vol. 19, no.58, pp. 1–228, 2015.
[22] A. Sankarankutty, B. Nascimento, L. T. da Luz, and S. Rizoli,“TEG� and ROTEM� in trauma: Similar test but differentresults?”World Journal of Emergency Surgery, vol. 7, 2012.
[23] M. Coakley, K. Reddy, I. Mackie, and S. Mallett, “TransfusionTriggers in Orthotopic Liver Transplantation: A Comparisonof theThromboelastometry Analyzer, theThromboelastogram,and Conventional Coagulation Tests,” Journal of Cardiothoracicand Vascular Anesthesia, vol. 20, no. 4, pp. 548–553, 2006.
[24] S. Rizoli, A. Min, A. P. Sanchez et al., “In trauma, conventionalROTEMandTEG results are not interchangeable but are similarin clinical applicability,” Military Medicine, vol. 181, no. 5, pp.117–126, 2016.
[25] N. Schafer, A. Driessen, U. Bauerfeind et al., “In vitro effectsof different sources of fibrinogen supplementation on clotinitiation and stability in a model of dilutional coagulopathy,”Transfusion Medicine, vol. 26, no. 5, pp. 373–380, 2016.
[26] M. Mittermayr, W. Streif, T. Haas et al., “Hemostatic changesafter crystalloid or colloid fluid administration during majororthopedic surgery: The role of fibrinogen administration,”Anesthesia & Analgesia, vol. 105, no. 4, pp. 905–917, 2007.
[27] M. Durila, P. Lukas, M. Astraverkhava, and T. Vymazal, “Eval-uation of fibrinogen concentrates and prothrombin complexconcentrates on coagulation changes in a hypothermic in vitromodel using thromboelastometry and thromboelastography,”Scandinavian Journal of Clinical & Laboratory Investigation, vol.75, no. 5, pp. 407–414, 2015.
[28] B. Schenk, A. K. Lindner, B. Treichl et al., “Fibrinogen sup-plementation ex vivo increasesclot firmness comparable toplatelet transfusion in thrombocytopenia,” British Journal ofAnaesthesia, vol. 117, no. 5, pp. 576–582, 2016.
[29] L. T. Da Luz, B. Nascimento, A. K. Shankarakutty, S. Rizoli,and N. K. J. Adhikari, “Effect of thromboelastography (TEG�)and rotational thromboelastometry (ROTEM�) on diagnosis ofcoagulopathy, transfusion guidance and mortality in trauma:Descriptive systematic review,”Critical Care, vol. 18, no. 5, 2014.
[30] H. T. Peng, B. Nascimento, andH. Tien, “A comparative analysisof functional fibrinogen assays using teg and rotem in traumapatients enrolled in the fiirst trial,” Panamerican Journal ofTrauma, Critical Care & Emergency Surgery, vol. 7, pp. 143–157,2018.
[31] B. Nascimento, J. Callum, H. Tien et al., “Fibrinogen in theinitial resuscitation of severe trauma (FiiRST): a randomized
feasibility trial,” British Journal of Anaesthesia, vol. 117, no. 6, pp.775–782, 2016.
[32] J. N. Harr, E. E. Moore, A. Ghasabyan et al., “Functionalfibrinogen assay indicates that fibrinogen is critical in correctingabnormal clot strength following trauma,” Shock, vol. 39, no. 1,pp. 45–49, 2013.
[33] L. Z. Kornblith, M. E. Kutcher, B. J. Redick, C. S. Calfee, R. F.Vilardi, and M. J. Cohen, “Fibrinogen and platelet contribu-tions to clot formation: Implications for trauma resuscitationand thromboprophylaxis,” Journal of Trauma and Acute CareSurgery, vol. 76, no. 2, pp. 255–263, 2014.
[34] A. S. P. Meyer, M. A. S. Meyer, A. M. Sørensen et al.,“Thrombelastography and rotational thromboelastometry earlyamplitudes in 182 trauma patients with clinical suspicion ofsevere injury,” Journal of Trauma and Acute Care Surgery, vol.76, pp. 682–690, 2014.
[35] M. A. S. Meyer, S. R. Ostrowski, A. M. Sørensen et al.,“Fibrinogen in trauma, an evaluation of thrombelastographyand rotational thromboelastometry fibrinogen assays,” Journalof Surgical Research, vol. 194, no. 2, pp. 581–590, 2015.
[36] I. Fluger, K. Maderova, M. Simek, R. Hajek, J. Zapletalova,and V. Lonsky, “Comparison of functional fibrinogen assess-ment using thromboelastography with the standard von claussmethod,” Biomedical Papers, vol. 156, no. 3, pp. 260-261, 2012.
[37] S. Agarwal, R. I. Johnson, and M. Shaw, “A comparison offibrinogenmeasurement using TEG� functional fibrinogen andClauss in cardiac surgery patients,” International Journal ofLaboratory Hematology, vol. 37, no. 4, pp. 459–465, 2015.
[38] I. Fluger, K. Maderova, M. Simek, R. Hajek, J. Zapletalova,and V. Lonsky, “The effect of a cardiopulmonary bypass systemwith biocompatible coating on fibrinogen levels determined bythe TEG-functional fibrinogen method: Preliminary results,”Perfusion, vol. 26, no. 6, pp. 503–509, 2011.
[39] M. Fabbro, J. T. Gutsche, T. A. Miano, J. G. Augoustides, andP. A. Patel, “Comparison of Thrombelastography-Derived Fib-rinogen Values at Rewarming and Following CardiopulmonaryBypass inCardiac SurgeryPatients,”Anesthesia& Analgesia, vol.123, no. 3, pp. 570–577, 2016.
[40] N. K. Gautam, C. Cai, O. Pawelek, M. B. Rafique, D. Cattano,and E. G. Pivalizza, “Performance of functional fibrinogenthromboelastography in children undergoing congenital heartsurgery,” Pediatric Anesthesia, vol. 27, no. 2, pp. 181–189, 2017.
[41] E. Kim, H. S. Shim, W. H. Kim et al., “Predictive Value ofIntraoperative Thromboelastometry for the Risk of Periopera-tive Excessive Blood Loss in Infants and Children UndergoingCongenital Cardiac Surgery,” Survey of Anesthesiology, vol. 61,no. 1, p. 17, 2017.
[42] S. Yang Lu, K. A. Tanaka, E. Abuelkasem, R. M. Planinsic, andT. Sakai, “Clinical applicability of rapid thrombelastographyand functional fibrinogen thrombelastography to adult livertransplantation,” Liver Transplantation, vol. 20, no. 9, pp. 1097–1105, 2014.
[43] V. N. R. Gottumukkala, S. K. Sharma, and J. Philip, “Assessingplatelet and fibrinogen contribution to clot strength usingmodified thromboelastography in pregnantwomen,”Anesthesia& Analgesia, vol. 89, no. 6, pp. 1453–1455, 1999.
[44] J.-S. David, M. Durand, A. Levrat et al., “Correlation betweenlaboratory coagulation testing and thromboelastometry ismod-ified duringmanagement of trauma patients,” Journal of Traumaand Acute Care Surgery, vol. 81, no. 2, pp. 319–327, 2016.

22 BioMed Research International
[45] L. Rugeri, A. Levrat, J. S. David et al., “Diagnosis of early coag-ulation abnormalities in trauma patients by rotation thrombe-lastography,” Journal of Thrombosis and Haemostasis, vol. 5, no.2, pp. 289–295, 2007.
[46] H. Tauber, P. Innerhofer, R. Breitkopf et al., “Prevalence andimpact of abnormal ROTEM� assays in severe blunt trauma:Results of the ’Diagnosis and Treatment of Trauma-InducedCoagulopathy (DIA-TRE-TIC) study’,” British Journal of Anaes-thesia, vol. 107, no. 3, pp. 378–387, 2011.
[47] V. Bhardwaj, P. Malhotra, S. Hasija, U. K. Chowdury, andN. Pangasa, “Coagulopathies in cyanotic cardiac patients: Ananalysis with three point - Of - care testing devices (Throm-boelastography, rotational thromboelastometry, and sonoclotanalyzer),”Annals of Cardiac Anaesthesia, vol. 20, no. 2, pp. 212–218, 2017.
[48] C. Solomon, E. Baryshnikova, C. J. Schlimp, H. Schochl, L. M.Asmis, and M. Ranucci, “Fibtem plus provides an improvedthromboelastometry test for measurement of fibrin-based clotquality in cardiac surgery patients,”Anesthesia & Analgesia, vol.117, no. 5, pp. 1054–1062, 2013.
[49] C. Solomon, N. Rahe-Meyer, H. Schochl, M. Ranucci, and K.Gorlinger, “Effect of haematocrit on fibrin-based clot firmnessin the FIBTEM test,” Blood Transfusion, vol. 11, no. 3, pp. 412–418, 2013.
[50] A. Espinosa, R. Stenseth, V.Videm, andH. Pleym, “Comparisonof three point-of-care testing devices to detect hemostaticchanges in adult elective cardiac surgery: A prospective obser-vational study,” BMC Anesthesiology, vol. 14, no. 1, 2014.
[51] H. S. Mace, N. Lightfoot, S. McCluskey et al., “Validityof Thromboelastometry for Rapid Assessment of FibrinogenLevels in Heparinized Samples during Cardiac Surgery: ARetrospective, Single-center, Observational Study,” Journal ofCardiothoracic and Vascular Anesthesia, vol. 30, no. 1, pp. 90–95, 2016.
[52] M. Ranucci and E. Baryshnikova, “Fibrinogen supplementationafter cardiac surgery: Insights from the Zero-Plasma trial(ZEPLAST),” British Journal of Anaesthesia, vol. 116, no. 5, pp.618–623, 2016.
[53] G. Erdoes, G. Gerster, G. Colucci, H. Kaiser, L. Alberio,and B. Eberle, “Prediction of post-weaning fibrinogen statusduring cardiopulmonary bypass: An observational study in 110patients,” PLoS ONE, vol. 10, no. 5, 2015.
[54] H. Seo, J.-H. Choi, Y.-J. Moon, and S.-M. Jeong, “FIBTEM ofthromboelastometry does not accurately represent fibrinogenconcentration in patients with severe hypofibrinogenemia dur-ing liver transplantation,” Annals of Transplantation, vol. 20, pp.342–350, 2015.
[55] S.-M. Jeong, J.-G. Song, H. Seo, J.-H. Choi, D.-M. Jang, andG.-S. Hwang, “Quantification of Both Platelet Count andFibrinogen Concentration Using Maximal Clot Firmness ofThromboelastometry during Liver Transplantation,”Transplan-tation Proceedings, vol. 47, no. 6, pp. 1890–1895, 2015.
[56] A. Blasi, J. Beltran, A. Pereira et al., “An assessment ofthromboelastometry to monitor blood coagulation and guidetransfusion support in liver transplantation,” Transfusion, vol.52, no. 9, pp. 1989–1998, 2012.
[57] S. Roullet, J. Pillot, G. Freyburger et al., “Rotation thromboelas-tometry detects thrombocytopenia and hypofibrinogenaemiaduring orthotopic liver transplantation,” British Journal ofAnaesthesia, vol. 104, no. 4, pp. 422–428, 2010.
[58] J.-G. Song, S.-M. Jeong, I.-G. Jun, H.-M. Lee, and G.-S. Hwang,“Five-minute parameter of thromboelastometry is sufficient to
detect thrombocytopenia and hypofibrinogenaemia in patientsundergoing liver transplantation,”British Journal ofAnaesthesia,vol. 112, no. 2, pp. 290–297, 2014.
[59] C. Huissoud, N. Carrabin, F. Audibert et al., “Bedside assess-ment of fibrinogen level in postpartum haemorrhage bythrombelastometry,” BJOG: An International Journal of Obstet-rics & Gynaecology, vol. 116, no. 8, pp. 1097–1102, 2009.
[60] C. Ellenberger, N. Garofano, G. Barcelos, J. Diaper, G. Pavlovic,and M. Licker, “Assessment of Haemostasis in patients under-going emergent neurosurgery by rotational Elastometry andstandard coagulation tests: a prospective observational study,”BMC Anesthesiology, vol. 17, no. 1, 2017.
[61] E. Schaden,D. Hoerburger, S. Hacker, P. Kraincuk,D.M. Baron,and S. Kozek-Langenecker, “Fibrinogen function after severeburn injury,” Burns, vol. 38, no. 1, pp. 77–82, 2012.
[62] D. Vucelic, R. Jesic, S. Jovicic et al., “Comparison of standardfibrinogen measurement methods with fibrin clot firmnessassessed by thromboelastometry in patients with cirrhosis,”Thrombosis Research, vol. 135, no. 6, pp. 1124–1130, 2015.
[63] P. I. Johansson, A. M. Sørensen, C. F. Larsen et al., “Lowhemorrhage-related mortality in trauma patients in a Leveli trauma center employing transfusion packages and earlythromboelastography-directed hemostatic resuscitation withplasma andplatelets,”Transfusion, vol. 53, no. 12, pp. 3088–3099,2013.
[64] H. Schochl, B. Cotton, K. Inaba et al., “FIBTEM provides earlyprediction of massive transfusion in trauma,” Critical Care, vol.15, no. 6, 2011.
[65] M. L. Tonglet, J.-L. Poplavsky, L. Seidel, J. M. Minon, V. D’Orio,and A. Ghuysen, “Thromboelastometry in trauma care: a placein the 2018 Belgian health care system?” Acta Clinica Belgica:International Journal of Clinical and Laboratory Medicine, pp.1–7, 2018.
[66] T. M. Dotsch, D. Dirkmann, D. Bezinover et al., “Assessmentof standard laboratory tests and rotational thromboelastometryfor the prediction of postoperative bleeding in liver transplanta-tion,” British Journal of Anaesthesia, vol. 119, no. 3, pp. 402–410,2017.
[67] L. Kaufner, A. Henkelmann, C. Von Heymann et al., “Canprepartum thromboelastometry-derived parameters and fib-rinogen levels really predict postpartum hemorrhage?” Journalof Perinatal Medicine, vol. 45, no. 4, pp. 427–435, 2017.
[68] H. Schochl, W. Voelckel, A. Grassetto, and C. J. Schlimp,“Practical application of point-of-care coagulation testing toguide treatment decisions in trauma,” Journal of Trauma andAcute Care Surgery, vol. 74, no. 6, pp. 1587–1598, 2013.
[69] W. Schobersberger, D. Fries, M. Mittermayr et al., “Changesof biochemical markers and functional tests for clot formationduring long-haul flights,” Thrombosis Research, vol. 108, no. 1,pp. 19–24, 2002.
[70] L. Anderson, I. Quasim, M. Steven et al., “Interoperator andintraoperator variability of whole blood coagulation assays: Acomparison of thromboelastography and rotational thromboe-lastometry,” Journal of Cardiothoracic and Vascular Anesthesia,vol. 28, no. 6, pp. 1550–1557, 2014.
[71] C. Solomon, B. Sørensen, G. Hochleitner, J. Kashuk, M.Ranucci, and H. Schochl, “Comparison of whole blood fibrin-based clot tests in thrombelastography and thromboelastome-try,” Anesthesia & Analgesia, vol. 114, no. 4, pp. 721–730, 2012.
[72] N. Rahe-Meyer, C. Solomon, M. Vorweg et al., “Multicentriccomparison of single portion reagents and liquid reagents for

BioMed Research International 23
thromboelastometry,” Blood Coagulation & Fibrinolysis, vol. 20,no. 3, pp. 218–222, 2009.
[73] P. A. Gurbel, K. P. Bliden, U. S. Tantry et al., “First report of thepoint-of-care TEG: A technical validation study of the TEG-6Ssystem,” Platelets, vol. 27, no. 7, pp. 642–649, 2016.
[74] J. D. Dias, E. I. Haney, B. A. Mathew, C. G. Lopez-Espina,A. W. Orr, and M. A. Popovsky, “New-Generation Throm-boelastography: Comprehensive Evaluation of Citrated andHeparinized Blood Sample Storage Effect on Clot-FormingVariables,”Archives of Pathology& LaboratoryMedicine, vol. 141,no. 4, pp. 569–577, 2017.
[75] K. Gorlinger, J. Iqbal, D. Dirkmann, and K. A. Tanaka, “Wholeblood assay: Thromboelastometry,” Management of BleedingPatients, pp. 37–64, 2016.
[76] D. A. Grimes and K. F. Schulz, “Refining clinical diagnosis withlikelihood ratios,”The Lancet, vol. 365, no. 9469, pp. 1500–1505,2005.
[77] V. G. Nielsen, B. M. Cohen, and E. Cohen, “Effects of coagu-lation factor deficiency on plasma coagulation kinetics deter-mined via thrombelastography�: Critical roles of fibrinogen andfactors II, VII, X and XII,” Acta Anaesthesiologica Scandinavica,vol. 49, no. 2, pp. 222–231, 2005.
[78] V. G. Nielsen, “Colloids decrease clot propagation and strength:Role of factor XIII-fibrin polymer and thrombin-fibrinogeninteractions,” Acta Anaesthesiologica Scandinavica, vol. 49, no.8, pp. 1163–1171, 2005.
[79] D. Fries, P. Innerhofer, C. Reif et al., “The effect of fibrinogensubstitution on reversal of dilutional coagulopathy: An in vitromodel,” Anesthesia & Analgesia, vol. 102, no. 2, pp. 347–351,2006.
[80] D. Fries, A. Krismer, A. Klingler et al., “Effect of fibrinogen onreversal of dilutional coagulopathy: A porcine model,” BritishJournal of Anaesthesia, vol. 95, no. 2, pp. 172–177, 2005.
[81] C. Fenger-Eriksen, E. Anker-Møller, J. Heslop, J. Ingerslev, andB. Sørensen, “Thrombelastographic whole blood clot formationafter ex vivo addition of plasma substitutes: Improvements ofthe induced coagulopathy with fibrinogen concentrate,” BritishJournal of Anaesthesia, vol. 94, no. 3, pp. 324–329, 2005.
[82] K. Gorlinger, D. Dirkmann, C. Solomon, andA. A. Hanke, “Fastinterpretation of thromboelastometry in non-cardiac surgery:Reliability in patients with hypo-, normo-, and hypercoagula-bility,” British Journal of Anaesthesia, vol. 110, no. 2, pp. 222–230,2013.
[83] U. Kalina, H.-A. Stohr, H. Bickhard et al., “Rotational throm-boelastography for monitoring of fibrinogen concentrate ther-apy in fibrinogen deficiency,” Blood Coagulation & Fibrinolysis,vol. 19, no. 8, pp. 777–783, 2008.
[84] I. J. Mackie, A. S. Lawrie, S. Kitchen et al., “A performanceevaluation of commercial fibrinogen reference preparations andassays for clauss and PT-derived fibrinogen,” Thrombosis andHaemostasis, vol. 87, no. 6, pp. 997–1005, 2002.
[85] S. C. Koh, C. Y. Chew, O. A. Viegas, M. Choo, and S. S. Ratnam,“Influence of circulatingD-dimer levels on assays of fibrinogen,”ANNALS Academy of Medicine Singapore, vol. 23, pp. 856–860,1994.
[86] L. M. Asmis, “Coagulation factor concentrates,” in Perioperativehemostasis: Coagulation for anesthesiologists, C. E.Marcucci andP. Schoettker, Eds., pp. 177–204, Springer, Berlin, Heidelberg,2015.
[87] H. Schochl, W. Voelckel, and C. Solomon, “Detection andimpact of hyperfibrinolysis in trauma,” Wiener KlinischeWochenschrift, vol. 122, no. 5, pp. S11–S13, 2010.
[88] R. Gertler, G. Wiesner, P. Tassani-Prell, S.-L. Braun, and K.Martin, “Are the point-of-care diagnostics MULTIPLATE andROTEM valid in the setting of high concentrations of heparinand its reversal with protamine?” Journal of Cardiothoracic andVascular Anesthesia, vol. 25, no. 6, pp. 981–986, 2011.
[89] B. S. Romlin, H. Wahlander, M. Synnergren, F. Baghaei, andA. Jeppsson, “Earlier detection of coagulopathy with throm-boelastometry during pediatric cardiac surgery: A prospectiveobservational study,”Pediatric Anesthesia, vol. 23, no. 3, pp. 222–227, 2013.
[90] A. M. H. P. Van Den Besselaar, C. J. J. Van Rijn, C. M.Cobbaert et al., “Fibrinogen determination according to Clauss:Commutability assessment of International and commercialstandards and quality control samples,” Clinical Chemistry andLaboratory Medicine, vol. 55, no. 11, pp. 1761–1769, 2017.
[91] C. Solomon, J. Cadamuro, B. Ziegler et al., “A comparisonof fibrinogen measurement methods with fibrin clot elasticityassessed by thromboelastometry, before and after administra-tion of fibrinogen concentrate in cardiac surgery patients,”Transfusion, vol. 51, no. 8, pp. 1695–1706, 2011.
[92] C. Fenger-Eriksen, G. W. Moore, S. Rangarajan, J. Ingerslev,and B. Sørensen, “Fibrinogen estimates are influenced bymeth-ods of measurement and hemodilution with colloid plasmaexpanders,” Transfusion, vol. 50, no. 12, pp. 2571–2576, 2010.
[93] D. Winstedt, C. Solomon, A. Hillarp, T. Lundahl, and U.Schott, “Intraoperative Hydroxyethyl Starch and its Effectson Different Fibrinogen Measurements,” Clinical and AppliedThrombosis/Hemostasis, vol. 22, no. 7, pp. 641–647, 2016.
[94] C. Solomon, E. Baryshnikova, A. Tripodi et al., “Fibrinogenmeasurement in cardiac surgery with cardiopulmonary bypass:Analysis of repeatability and agreement of Clauss methodwithin and between six different laboratories,” Thrombosis andHaemostasis, vol. 112, no. 1, pp. 109–117, 2014.
[95] A. Agren, A. T. Wikman, A. Ostlund, and G. Edgren, “TEG�functional fibrinogen analysis may overestimate fibrinogenlevels,”Anesthesia & Analgesia, vol. 118, no. 5, pp. 933–935, 2014.
[96] O.Thomas, H. Rein, K. Strandberg, and U. Schott, “Coagulativesafety of epidural catheters after major upper gastrointestinalsurgery: advanced and routine coagulation analysis in 38patients,” Perioperative Medicine, vol. 5, no. 1, 2016.
[97] C. J. Schlimp, J. Cadamuro, C. Solomon, H. Redl, and H.Schochl, “The effect of fibrinogen concentrate and factor XIII onthromboelastometry in 33% diluted blood with albumin, gela-tine, hydroxyethyl starch or saline in vitro,” Blood Transfusion,vol. 11, no. 4, pp. 510–517, 2013.
[98] V. G. Nielsen, W. Q. Gurley, and T. M. Burch, “The Impactof Factor XIII on Coagulation Kinetics and Clot StrengthDetermined by Thrombelastography,” Anesthesia & Analgesia,vol. 99, no. 1, pp. 120–123, 2004.
[99] S. Ogawa, F. Szlam, D. Bolliger, T. Nishimura, E. P. Chen,and K. A. Tanaka, “The Impact of Hematocrit on FibrinClot Formation Assessed by Rotational Thromboelastometry,”Anesthesia & Analgesia, vol. 115, no. 1, pp. 16–21, 2012.
[100] A. S. Jensen, P. I. Johansson, L. Bochsen et al., “Fibrinogenfunction is impaired inwhole blood frompatientswith cyanoticcongenital heart disease,” International Journal of Cardiology,vol. 167, no. 5, pp. 2210–2214, 2013.
[101] H. T. Peng and S. G. Rhind, “Thromboelastographic Studyof Psychophysiological Stress,” Clinical and Applied Thrombo-sis/Hemostasis, vol. 21, no. 6, pp. 497–512, 2015.
[102] R. C. Carroll, R. M. Craft, J. J. Chavez, C. C. Snider, R. K. Kirby,and E. Cohen, “Measurement of functional fibrinogen levels

24 BioMed Research International
using the Thrombelastograph,” Journal of Clinical Anesthesia,vol. 20, no. 3, pp. 186–190, 2008.
[103] A. Rizza, Z. Ricci, C. Pezzella et al., “Kaolin-activated throm-boelastography and standard coagulation assays in cyanoticand acyanotic infants undergoing complex cardiac surgery: aprospective cohort study,” Pediatric Anesthesia, vol. 27, no. 2, pp.170–180, 2017.
[104] R. J. Parker, K. A. Eley, S. Von Kier, O. Pearson, and S.R. Watt-Smith, “Functional fibrinogen to platelet ratio usingthromboelastography as a predictive parameter for thromboticcomplications following free tissue transfer surgery: A prelimi-nary study,”Microsurgery, vol. 32, no. 7, pp. 512–519, 2012.
[105] S. R. Ostrowski, N. Haase, R. B. Muller et al., “Associationbetween biomarkers of endothelial injury and hypocoagulabil-ity in patients with severe sepsis: A prospective study,” CriticalCare, vol. 19, no. 1, 2015.
[106] J. S. Hagemo, S. Stanworth, N. P. Juffermans et al., “Prevalence,predictors and outcome of hypofibrinogenaemia in trauma: Amulticentre observational study,” Critical Care, vol. 18, no. 2,2014.
[107] Z. K. McQuilten, M. Bailey, P. A. Cameron et al., “Fibrinogenconcentration and use of fibrinogen supplementation withcryoprecipitate in patients with critical bleeding receivingmassive transfusion: a bi-national cohort study,” British Journalof Haematology, vol. 179, no. 1, pp. 131–141, 2017.
[108] J. Zhou, Y. Xin, Q. Ding et al., “Thromboelastographypredicts risks of obstetric complication occurrence in(hypo)dysfibrinogenemia patients under non-pregnantstate,” Clinical and Experimental Pharmacology and Physiology,vol. 43, no. 2, pp. 149–156, 2016.
[109] A. Larsson, N. Tynngard, T. Kander, J. Bonnevier, andU. Schott,“Comparison of point-of-care hemostatic assays, routine coag-ulation tests, and outcome scores in critically ill patients,”Journal of Critical Care, vol. 30, no. 5, pp. 1032–1038, 2015.
[110] S. P. McCully, L. J. Fabricant, N. R. Kunio et al., “The inter-national normalized ratio overestimates coagulopathy in stabletrauma and surgical patients,” Journal of Trauma andAcute CareSurgery, vol. 75, no. 6, pp. 947–953, 2013.
[111] H. Shakur, I. Roberts, and R. Bautista, “Effects of tranexamicacid on death, vascular occlusive events, and blood transfusionin trauma patients with significant haemorrhage (CRASH-2): arandomised, placebo-controlled trial,” The Lancet, vol. 376, no.9734, pp. 23–32, 2010.
[112] H. Shakur, I. Roberts, B. Fawole et al., “Effect of earlytranexamic acid administration on mortality, hysterectomy,and other morbidities in women with post-partum haemor-rhage (woman): An international, randomised, double-blind,placebo-controlled trial,” The Lancet, vol. 389, pp. 2105–2116,2017.
[113] A.Godier, K. Parmar, K.Manandhar, andB. J. Hunt, “An in vitrostudy of the effects of t-PA and tranexamic acid on whole bloodcoagulation and fibrinolysis,” Journal of Clinical Pathology, vol.70, no. 2, pp. 154–161, 2017.
[114] C. J. Schlimp, C. Solomon, M. Ranucci, G. Hochleitner, H.Redl, and H. Schochl, “The effectiveness of different functionalfibrinogen polymerization assays in eliminating platelet contri-bution to clot strength in thromboelastometry,” Anesthesia &Analgesia, vol. 118, no. 2, pp. 269–276, 2014.
[115] C. J. Schlimp, C. Solomon, G. Hochleitner, J. Zipperle, H.Redl, and H. Schochl, “Thromboelastometric maximum clotfirmness in platelet-free plasma is influenced by the assay used,”Anesthesia & Analgesia, vol. 117, no. 1, pp. 23–29, 2013.
[116] F. Pruller, A. Munch, A. Preininger et al., “Comparison of func-tional fibrinogen (FF/CFF) and FIBTEM in surgical patients– a retrospective study,” Clinical Chemistry and LaboratoryMedicine (CCLM), vol. 54, no. 3, 2016.
[117] V. G. Nielsen, “A comparison of theThrombelastograph and theROTEM,” Blood Coagulation & Fibrinolysis, vol. 18, no. 3, pp.247–252, 2007.
[118] T. Tomori, D. Hupalo, K. Teranishi et al., “Evaluation of coagu-lation stages of hemorrhaged swine: Comparison of thromboe-lastography and rotational elastometry,” Blood Coagulation &Fibrinolysis, vol. 21, no. 1, pp. 20–27, 2010.
[119] J. N. Harr, E. E.Moore, T. L. Chin et al., “Viscoelastic hemostaticfibrinogen assays detect fibrinolysis early,” European Journal ofTrauma and Emergency Surgery, vol. 41, no. 1, pp. 49–56, 2014.
[120] E. Abuelkasem, S. Lu, K. Tanaka, R. Planinsic, and T. Sakai,“Comparison between thrombelastography and thromboelas-tometry in hyperfibrinolysis detection during adult liver trans-plantation,” British Journal of Anaesthesia, vol. 116, no. 4, pp.507–512, 2016.
[121] L. S. Gall, P. Vulliamy, S. Gillespie et al., “The S100A10 Path-way Mediates an Occult Hyperfibrinolytic Subtype in TraumaPatients,” Annals of Surgery, p. 1, 2018.
[122] J. C.Gomez-Builes, S. A. Acuna, B.Nascimento, F.Madotto, andS. B. Rizoli, “Harmful or Physiologic,” Anesthesia & Analgesia,vol. 127, no. 4, pp. 840–849, 2018.
[123] H. B.Moore, E. E. Moore, E. Gonzalez et al., “Hyperfibrinolysis,physiologic fibrinolysis, and fibrinolysis shutdown: the spec-trum of postinjury fibrinolysis and relevance to antifibrinolytictherapy,”The Journal of Trauma and Acute Care Surgery, vol. 77,no. 6, pp. 811–817, 2014.
[124] H. B. Moore, E. E. Moore, I. N. Liras et al., “Acute FibrinolysisShutdown after InjuryOccurs Frequently and IncreasesMortal-ity: AMulticenter Evaluation of 2,540 Severely InjuredPatients,”Journal of the American College of Surgeons, vol. 222, no. 4, pp.347–355, 2016.
[125] J. C. Cardenas, C. E. Wade, B. A. Cotton et al., “Teg Lysis Shut-down Represents Coagulopathy in Bleeding Trauma Patients,”Shock, p. 1, 2018.
[126] R. Carroll, R. Craft, and R. Langdon, “Early Evaluation of AcuteTraumatic Coagulopathy by Thrombelastography,” Journal ofVascular Surgery, vol. 51, no. 1, p. 280, 2010.