Outpatient Physical Therapy Following Triple Arthrodesis ...

1 | P i c a d o
Three’s Company - The role of triple therapy in chronic obstructive pulmonary
disease (COPD) October 26th, 2018
Zahava Picado, PharmD PGY1 Pharmacy Resident
Central Texas Veterans Healthcare System [email protected]

2 | P i c a d o
Learning Objectives By the end of this session, the learner should be able to…
• Identify COPD patients who are potential candidates for triple therapy
• Compare the use of “fixed” triple therapy with “open” triple therapy
• Explain the role of using inhaled corticosteroids (ICS) in a COPD patient
Assessment Questions Patient HT is a 69-year-old male who presents to your clinic. His most recent pulmonary tests show an FEV1/FVC: 47%,
FEV1: 29% of expected, and 2 exacerbations in previous year, 1 requiring hospitalization. The patient reports that he had
to stop for breath several times to enter your office from the parking lot today (mMRC 3).
1. How would you classify this patient’s COPD?
a. GOLD 1, Group A
b. GOLD 2, Group B
c. GOLD 3, Group C
d. GOLD 4, Group D
2. Which of the following medication regimens would you recommend for HT? a. Albuterol + Tiotropium b. Albuterol + Salmeterol c. Albuterol + Umeclidinium + Vilanterol d. Albuterol + Fluticasone + Salmeterol + Tiotropium
Patient OP is a 71-year-old female who presents to your clinic. Her most recent PFTs show an FEV1/FVC: 45%, FEV1: 28%
of expected, and 1 exacerbation 8 months ago requiring a hospitalization. The patient is extremely upset that she is not
able to run around the backyard and play tag with her grandchildren like she used to (mMRC 2).
3. How would you classify this patient’s COPD?
a. GOLD 1, Group A
b. GOLD 2, Group B
c. GOLD 3, Group C
d. GOLD 4, Group D
4. Which of the following medication regimens would you recommend for HT?
a. Albuterol + Tiotropium b. Albuterol + Salmeterol c. Albuterol + Umeclidinium + Vilanterol d. Albuterol + Fluticasone + Salmeterol + Tiotropium
5. Which of these comorbidities is associated with an increased risk for pneumonia?
I. Morbid Obesity
II. Current Smoker
III. FEV1 30% of predicted
A. I only
B. I and II
C. II and III
D. I, II, and III
E. None of the above

3 | P i c a d o
Background - COPD Epidemiology
• COPD affects approximately 64 million people worldwide and is the 3rd leading cause of death.
• Chronic inflammatory disease with persistent airflow limitation
Classification of COPD
Classification of airflow limitation severity in COPD (based on post-bronchodilator FEV1) in patients with FEV1/FVC < 0.70
GOLD 1 Mild FEV1 > 80% of predicted
GOLD 2 Moderate FEV1 50-79% of predicted
GOLD 3 Severe FEV1 30-49% of predicted
GOLD 4 Very Severe FEV1 < 30% of predicted
Pharmacologic Options
• Beta Agonists o Short acting (SABA) and long acting (LABA)
• Muscarinic Antagonists o Short acting (SAMA) and long acting (LAMA)
• Inhaled Corticosteroids 2018 GOLD Guideline Recommendations
• SABA or SAMA: o Acceptable for occasional dyspnea only (Evidence A)
• LABA + LAMA: o Increases FEV1 and reduces symptoms compared to monotherapy (Evidence A) o Reduces exacerbations compared to monotherapy or ICS + LABA (Evidence B)
• ICS + LABA: o Improves lung function and health status, and reduces exacerbations compared to monotherapy
(Evidence A) • LABA + LAMA + ICS (AKA “triple therapy”):
o Improves lung function, symptoms and health status (Evidence A) and reduces exacerbations (Evidence B) compared to ICS/LABA and LAMA monotherapy
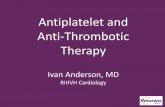
Noxious Air/Particle inhalation
Inflammatory cytokine release
Mucus hypersecretion
Airflow obstruction/air trapping
Gas exchange abnormalities
Pulmonary hypertension
Exacerbation History
> 2 or > 1 leading to hospitalization
GROUP C
GROUP D
0 or 1 (not leading to hospitalization)
GROUP A
GROUP B
mMRC 0-1 CAT < 10
mMRC > 2 CAT > 10
Symptom Severity

4 | P i c a d o
• Role against LAMA/LABA still unclear o Recommended exclusively for patients with group D COPD who continue to have exacerbations despite
dual therapy. o Remains inappropriately prescribed to patients despite GOLD recommendations.
• Overuse of triple therapy results in a waste of limited health resources and increased risk of side effects
Question 1: Which patients will benefit the most from triple therapy?
Trial 1: TRILOGY
Treatment Arms • Beclomethasone + formoterol + glycopyrrolate (ICS/LABA/LAMA) • Beclomethasone + formoterol (ICS/LABA)
Primary Outcome • Change in pre-dose FEV1 and 2-hour post-dose FEV1 at 26 weeks
Select Secondary Outcomes
• COPD exacerbation frequency over 52 weeks
Inclusion Criteria • Age 40+ • Prebronchodilator FEV1 < 60% predicted • 1+ moderate/severe exacerbation within 12 months • Current or former smokers (10 pack-year history) • CAT > 10
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Asthma, allergic rhinitis or Non-COPD pulmonary condition • COPD exacerbation within last 4 weeks • Requiring long term oxygen • Already on ICS/LABA/LAMA regimen
Baseline Characteristics
• 1181 patients completed study • 602 in ICS/LABA/LAMA • 579 in ICS/LABA
• Average age: 63 years old • Average FEV1: ~36% of predicted – severe airflow limitation • Average CAT score 20.8 • 47% active smokers • 1.2 exacerbations in the previous year • COPD medication at study entry
• ICS/LABA or ICS/LAMA – 75% • LABA/LAMA – 14% • LAMA – 11%
Group DLAMA + LABA LABA + ICS LAMA + LABA + ICS
Group CLAMA LAMA + LABA LABA + ICS
Group BLong-acting bronchodilator (LAMA/LABA) LABA + LAMA
Group AShort acting bronchodilator (SABA/SAMA) as needed

5 | P i c a d o
Results Pre-dose FEV1 at 26 weeks • Triple therapy increased FEV1 82 ml; ICS/LABA, increased FEV1 by 1 ml • Adjusted mean difference: 81 ml (p<0.001, CI 52-109 ml)
Post-dose FEV1 at 26 weeks • Triple therapy increased FEV1 261 ml; ICS/LABA, increased FEV1 by 145 ml • Adjusted mean difference: 117 ml (p<0.001, CI 86-147 ml)
Exacerbation rate over 52 weeks • Triple therapy had a 23% lower incidence rate of exacerbations compared to
ICS/LABA (RR 0.77, p = 0.005, CI 0.65-0.92)
Trial 2: IMPACT
Treatment Arms • Fluticasone Furoate + Umeclidinium + Vilanterol (ICS/LAMA/LABA) • Fluticasone + Vilanterol (ICS/LABA) • Umeclidinium + Vilanterol (LAMA/LABA)
Primary Outcome • Moderate-severe exacerbation rate over 52 weeks
Select Secondary Outcomes
• Change in FEV1 over 52 weeks • Change in St Georges Respiratory Questionnaire (SGRQ) over 52 weeks
Inclusion Criteria • Age 40+ • Current or former smokers • COPD CAT Score > 10 • FEV1 <50% of expected AND 1 mod-severe exacerbation in previous year or • FEV1 50-70% of expected AND 2+ moderate exacerbations in previous year
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Severe cardiac dysfunction • Allergic rhinitis or non-COPD pulmonary condition • Requiring long-term oxygen • Chronic use of antibiotics or oral steroids
Baseline Characteristics
• 10,355 patients in study • 4151 in ICS/LABA/LAMA • 4134 in ICS/LABA • 2070 in LABA/LAMA
• Average age: 65 years old • Average CAT score of 20.1 • Average FEV1 ~45% of predicted – severe airflow limitation • 26%: 1 severe COPD exacerbation in previous year • 47%: 2+ moderate COPD exacerbations in previous year • 11%: 3+ moderate-severe exacerbations in previous year • 4%: 2+ Severe COPD exacerbations in previous year
Results Exacerbation rate over 52 weeks • Triple therapy had a 15% lower rate of mod-severe exacerbations compared to
ICS/LABA (RR 0.85, P< 0.001, CI 0.80-0.90), and a 25% lower rate of moderate-severe exacerbations compared to LAMA/LABA (RR 0.75, P <0.001, CI 0.70-0.81).
Change in FEV1 at 52 weeks • Triple therapy increased FEV1 94 ml vs ICS/LABA which decreased FEV1 by 3ml, and
LAMA/LABA, which increased FEV1 by 40 ml. • Adjusted mean difference: 97 ml (P<0.001, CI 85-109); 54 ml (P<0.001, 39-69)
Change in SGRQ Score at 52 weeks • Triple therapy decreased SGRQ score by 5.5 points vs ICS/LABA and LAMA/LABA,
which decreased SGRQ score by 3.7 points. • Adjusted mean difference: 1.8 points (–2.4 to –1.1)

6 | P i c a d o
Trial 3: SUNSET
Treatment Arms 3-week run-in period of Tiotropium + Salmeterol + Fluticasone, then: • Tiotropium + Salmeterol + Fluticasone (LAMA/LABA/ICS) • Indacaterol + glycopyrrolate (LABA/LAMA)
Primary Outcome • Change in FEV1 after 26 weeks of treatment
Select Secondary Outcomes
• Exacerbation rate over 26 weeks
Inclusion Criteria • Age 40+ • FEV1 40-80% predicted • No more than 1 moderate/severe exacerbation within 12 months • Current or former smokers (10 pack-year history) • Receiving ICS/LABA/LAMA for 6+ months
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Asthma, allergic rhinitis or Non-COPD pulmonary condition • Requiring long term oxygen • Blood eosinophil count > 600 cells/µl
Baseline Characteristics
• 1053 patients in study • 527 in ICS/LABA • 526 in ICS/LABA/LAMA
• Average age: 65 years old • Average FEV1 ~56.6% of predicted – moderate airflow limitation • 34.1% had one exacerbation in previous year
Results Difference in FEV1 (Non-inferiority margin: -50 ml) • ICS withdrawal led to a decrease in FEV1 of -26 ml (95% CI -53 to 1) compared to
patients who remained on triple therapy. • De-escalation with dual therapy is not non-inferior to triple therapy.
Exacerbation rate over 26 weeks • Withdrawal of ICS led to 8% higher rate of moderate-severe exacerbations compared
to patients left on triple therapy (RR 1.08, P = 0.58, CI 0.83-1.40)
Triple Therapy
• Class D COPD only
• Severe airflow restriction
• High eosinophil counts (300-600 cells/µL)
Dual Therapy
• Inappropriately escalated
• Stable on triple therapy for > 6 months.

7 | P i c a d o
Question 2: Is “fixed” triple therapy better than “open” triple therapy?
Trial 4: TRINITY
Treatment Arms • Beclomethasone + formoterol + glycopyrrolate (FIXED) • Tiotropium alone • Beclomethasone + formoterol + tiotropium (OPEN)
Primary Outcome • COPD moderate-severe exacerbation rate
Select Secondary Outcomes
• Change in pre-dose FEV1 at week 52
Inclusion Criteria • Age 40-80 • Post-bronchodilator FEV1 <50% predicted • CAT > 10 • Current or former smokers (10 pack-year history) • 1+ moderate/severe exacerbation within 12 months
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Already receiving triple therapy • Asthma, allergic rhinitis or Non-COPD pulmonary condition • COPD exacerbation within last 4 weeks • Requiring long term oxygen
Baseline Characteristics
• 2691 patients • 1078 in fixed triple • 1075 in tiotropium • 538 in open triple
• Average age: 63 years old • Average FEV1 ~ 36.6% of predicted – Severe airflow limitation • Average CAT score 21 • 48% active smokers • COPD medication at study entry
• ICS/LABA or ICS/LAMA – 75% • LABA/LAMA – 12% • LAMA – 13%
Results Exacerbation Rate at 52 weeks • 20% lower exacerbation rate with fixed triple therapy compared to tiotropium
alone (RR 0.80, P = 0.0025, CI 0.69-0.92) • 21% lower exacerbation rate with open triple therapy compared to tiotropium
alone (RR = 0.79, P = 0.0095, CI 0.66-0.94) • 1% higher exacerbation rate with fixed triple therapy compared to open triple
therapy (RR = 1.01, P = 0.89, CI 0.85-1.21) Change in FEV1 at 52 weeks
• Fixed triple therapy increased FEV1 by 85 ml (65-100 ml) • Tiotropium therapy increased FEV1 by 21 ml (3-39 ml) • Open Triple therapy increased FEV1 by 85 ml (61-110 ml)
Study Conclusion: When compared to multiple inhalers, “fixed” triple therapy does not appear to have an impact on FEV1 or exacerbation rate.

8 | P i c a d o
Question 3: Which patients are at an increased risk for pneumonia with inhaled steroids? Role of ICS in COPD
• Historically, providers hypothesized that patients with COPD and inflammation would respond to inhaled steroids similar to patients with asthma.
• Data supporting the use of ICS is limited.
• There is evidence that ICS use leads to adverse reactions, such as candidiasis, bruising, and pneumonia.
Trial 5: TORCH
Treatment Arms • Fluticasone Propionate (ICS) • Salmeterol (LABA) • Fluticasone + Salmeterol (ICS/LABA) • Placebo
Primary Outcome • All-cause mortality at 3 years • COPD-related mortality at 3 years
Select Secondary Outcomes
• Rate of exacerbations • Change in FEV1
Inclusion Criteria • Age 40-80 • Prebronchodilator FEV1 <60% predicted • Poor reversibility of airflow obstruction • Current or former smokers (10 pack-year history)
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Asthma or Non-COPD pulmonary condition • COPD exacerbation within last 4 weeks
Baseline Characteristics
• 6112 patients included • 1500 in each treatment arm
• Average age: 65 years old • Average FEV1 ~ 44% of predicted – severe airflow limitation • Average pre-study exacerbation history:
• 1 ± 1.4 exacerbations/year requiring antibiotics/oral steroids • 43% active smokers, 48 pack-year history
Results All-cause mortality at 3 years • ICS/LABA did not significantly reduce risk of death compared to placebo (HR 0.825, CI
0.68-1.00, P=0.052) or salmeterol alone (HR 0.932, CI 0.765-1.134, P=0.48) • ICS/LABA was associated with a 23% reduction in risk of death compared to
fluticasone alone (HR 0.774, CI 0.641-0.934, P=0.007) COPD-related mortality at 3 years
• ICS/LABA was associated with a 22% reduction in risk of COPD-related death compared to placebo (HR 0.78, CI 0.57-1.06, P=0.011)
• ICS/LABA did not significantly reduce risk of COPD-related death compared to salmeterol (HR 0.77, CI 0.56-1.04, P=0.09)
• ICS/LABA was associated with a 33% reduction in risk of COPD-related death compared to fluticasone (HR 0.67, CI 0.50-0.90, P=0.008)
Pneumonia • ICS/LABA had 7.3% more pneumonia events compared to placebo (19.6% vs. 12.3%,
P<0.001) • Fluticasone alone had 6% more pneumonia events compared to placebo (18.3% vs.
12.3% P<0.001) • Salmeterol alone had 1% more pneumonia events compared to placebo (13.3% vs
12.3% P<0.001)

9 | P i c a d o
Trial 6: SUMMIT
Treatment Arms • Fluticasone Furoate • Vilanterol • Fluticasone + vilanterol • Placebo
Primary Outcome • Time to death from any cause
Select Secondary Outcomes
• Cardiovascular death, MI, stroke, UA, and TIA.
Inclusion Criteria • Age 40-80 • FEV1 ≥50 and ≤70% predicted • ≥2 on the mMRC dyspnea scale • History of cardiovascular disease or increased cardiovascular risk • Current or former smokers (10 pack-year history)
Exclusion Criteria • Alpha-1 antitrypsin deficiency • Asthma or Non-COPD pulmonary condition • COPD exacerbation within last 4 weeks • Requiring long term oxygen
Baseline Characteristics
• 16,568 patients included • 4100 in each treatment arm
• Average age: 65 years old • Average FEV1 ~ 59% of predicted – Moderate airflow limitation • Exacerbation History
• 61% patients had 0 exacerbations • 25% of patients had 1 exacerbation • 15% of patients had 2+ exacerbations
• 47% active smokers, 41 pack-year history
Results Time to death from any cause • ICS/LABA did not significantly reduce risk of death compared to placebo (HR 0·88, CI
0·74-1·04, p=0·137) • Fluticasone did not significantly reduce risk of death compared to placebo (HR 0·91,
CI 0·77-1·08, p=0·284) • Vilanterol did not significantly reduce risk of death compared to placebo (HR 0·96, CI
0·81-1·14, p=0·655) Pneumonia
• ICS/LABA had 0.5% more pneumonia events compared to placebo (5.7% vs 5.2%, P<0.001)
• Fluticasone did not have significantly higher pneumonia events compared to placebo (5.5% vs 5.2%, P = 0.716)
• Vilanterol had 1.3% less pneumonia events compared to placebo (3.9% vs 5.2%, P<0.001)
Study Conclusions: Patients at higher risk of pneumonia are:
• Current smokers • Age 55+ • BMI < 25 • Poor mMRC grade and/or severe airflow limitation (FEV1< 50%) • History of exacerbations and/or pneumonia

10 | P i c a d o
Presenter’s Conclusions
• Triple therapy o Recommended exclusively for patients with group D COPD who continue to have exacerbations despite
dual therapy. • Additional patients with high eosinophil counts may benefit from triple therapy.
o Consider de-escalating patients from triple therapy who are stable on their triple therapy for at least 6 months
• Open vs fixed triple therapy o When compared to multiple inhalers, “fixed” triple therapy does not appear to have an impact on FEV1
or exacerbation rate. • Role of ICS and pneumonia
o Use of ICS should be weighed strongly in patients who: are current smokers, age 55+, BMI < 25, are extremely symptomatic with significant airflow limitation, and who have a history of exacerbations and/or pneumonia
o ICS should never be used as monotherapy
Future Studies
1. INTREPID - Investigation of TRELEGY Effectiveness: Usual Practice Design (December 2019) a. Randomized, open-label, effectiveness, phase 4 study b. Fluticasone Furoate/Umeclidinium/Vilanterol single inhaler vs. multiple-inhaler triple therapy
2. TRIVOLVE - Fixed Dose Triple Therapy in Severe COPD in a Real-World Setting (August 2019) a. Prospective, non-interventional study b. Beclomethasone/Formoterol/Glycopyrrolate vs. multiple inhaler triple therapy
3. AIRWISE - Assessment in a Real-World Setting of the Effect of Inhaled Steroid-based Triple Therapy Versus the Combination of Tiotropium and Olodaterol on Reducing COPD Exacerbations (June 2020)
a. Randomized, open-label effectiveness phase 4 study b. Tiotropium/Olodaterol vs multiple inhaler triple therapy

11 | P i c a d o
References
1. Global Initiative for Chonic Obstructive Lung Disease. The Global Strategy for the Diagnosis, Management and Prevention of COPD. 2018 [accessed 2018 August]. Available from: http://goldcopd.org
2. Hatipoglu U, Aboussquan L. Chronic obstructive pulmonary disease: An update for the primary physician. Clev Clin J Med 2014;81(6):373–383.
3. Singh, D., Papi, A., et al. (2016). Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): A double-blind, parallel group, randomised controlled trial. The Lancet, 388(10048), 963-973. doi:10.1016/s0140-6736(16)31354-x
4. Chapman, K. R., Hurst, J. R., Frent, S., et al. (2018). Long-Term Triple Therapy De-escalation to Indacaterol/Glycopyrronium in Patients with Chronic Obstructive Pulmonary Disease (SUNSET): A Randomized, Double-Blind, Triple-Dummy Clinical Trial. American Journal of Respiratory and Critical Care Medicine, 198(3), 329-339. doi:10.1164/rccm.201803-0405oc
5. Vestbo, J., Papi, A., Corradi, M., et al. (2017). Single inhaler extra fine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): A double-blind, parallel group, randomized controlled trial. The Lancet, 389(10082), 1919-1929. doi:10.1016/s0140-6736(17)30188-5
6. Calverley PM, Anderson JA, Celli B, et al. Salmteterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007; 356(8): 775-89.
7. Vestbo J, Anderson JA, Brook RD et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomized controlled trial. Lance 2016; 387(10030): 1817-26
8. https://clinicaltrials.gov/ct2/show/NCT03467425?term=intrepid&cond=copd&rank=1 9. https://clinicaltrials.gov/ct2/show/NCT03627858?term=trivolve&rank=1 10. https://clinicaltrials.gov/ct2/show/NCT03265145?term=airwise&rank=1

12 | P i c a d o
Supplementary Material
Table 2: Modified Medical Research Council (mMRC) Questionnaire for categorizing COPD severity
Severity Score Level of breathlessness
None 0 Only breathless with strenuous exercise
Mild 1 Shortness of breath hurrying or walking up a slight hill
Moderate 2 Walks slower than age group or must stop for breath when walking on level ground at own pace
Severe 3 Stops for breath after walking 100 meters or a few minutes on level ground
Very Severe 4 Breathless when dressing/too breathless to leave the house
Adapted from: Global Initiative for Chronic Obstructive Lung Disease. 2018
Table 3: Common inhaler formulations/combinations
ICS/LABA LABA/LAMA ICS
Budesonide/Formoterol (Symbicort) Fluticasone/Salmeterol (Advair)
Fluticasone/Vilanterol (Breo) Mometasone/Formoterol (Dulera)
Olodaterol/Tiotropium (Stiolto) Umeclidinium/Vilanterol (Anoro)
Indacterol/Glycopyrrolate (Utibron) Formoterol/Glycopyrrolate (Bevespi)
Fluticasone (Flovent) Flunisolide (Aerospan)
Mometasone (Asmanex) QVAR (Beclomethasone) Budesonide (Pulmicort)
LABA LAMA SABA
Olodaterol (Striverdi) Indacterol (Arcapta)
Salmeterol (Serevent) Formoterol (Foradil, Perforomist)
Tiotropium (Spiriva) Glycopyrrolate (Seebri)
Aclidinium (Tudorza) Umeclidinium (Incruse)
Albuterol (Proair, Ventolin, Proventil)
Levalbuterol (Xopenex)
ICS/LAMA/LABA
Fluticasone/Umeclidinium/Vilanterol (Trelegy)
Table 1: Terms and Abbreviations
COPD – Chronic Obstructive Pulmonary Disease
LABA – Long Acting Beta Agonist
LAMA – Long Acting Muscarinic Antagonist
ICS – Inhaled Corticosteroid
GOLD – Global Initiative for Obstructive Lung Disease
SGRQ – St Georges Respiratory Questionnaire
mMRC – Modified Medical Research Council Dyspnea Scale
CAT – COPD Assessment Test
FEV1 - Volume of air expired in the 1st second during maximal respiratory effort
FVC - total volume of air expired after full inspiration

13 | P i c a d o
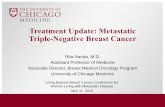
Figure 1. COPD Assessment Test