Three dimensional conformal simultaneously integrated boost technique for
15
Three dimensional conformal simultaneously integrated boost technique for breast conserving radiotherapy Hans Paul van der Laan, Wil V. Dolsma, John H. Maduro, Erik W. Korevaar, Miranda Hollander, Johannes A. Langendijk International Journal of Radiation Oncology Biology Physics 2007; 68: 1018-1023 Presented by Sehrish Inam Trainee Medical Physicist
-
Upload
sehrish-inam -
Category
Healthcare
-
view
39 -
download
1
Transcript of Three dimensional conformal simultaneously integrated boost technique for
Three dimensional conformal simultaneously integrated boost technique for breast
conserving radiotherapy
Hans Paul van der Laan, Wil V. Dolsma, John H. Maduro, Erik W. Korevaar, Miranda Hollander, Johannes A. Langendijk
International Journal of Radiation Oncology Biology Physics 2007; 68: 1018-1023
Presented by Sehrish Inam Trainee Medical Physicist

Abstract To compare the target coverage and normal
tissue dose with the simultaneously integrated boost (SIB) and the sequential boost technique in
breast cancer, and to evaluate the incidence of acute skin toxicity in patients treated with the
SIB technique.

Introduction
• For early stage breast cancer RT, 50Gy is prescribed to
whole PTV while16 Gy to lumpectomy.
• Conventionally boost is delivered after RT of whole breast.
• In SIB greater dose per fraction is delivered to the boost
PTV and the no. of fractions is reduced.
• Study to compare conventional 3D-CRT with sequential
boost technique (SBT) vs 3D-CRT using SIB technique.

Materials & Methods• Patients and computed tomography
o 30 patients with left sided breast cancer schedule to
undergo RT after breast conserving surgery .
o CT was conducted along with patients were
positioned on a breast board with both arms
abducted alongside the head.
o Skin marks were placed to locate the boost volume
isocenter
Materials & Methods• Target volume and organs at risk
o The breast PTV was generated by adding a
3Dmargin of 5mm around CTV.
o The boost PTV was generated by adding a
5mm margin accordingly.
o Heart , both lungs and ipsilateral breast was
contoured as OAR.

Materials & Methods• Sequential boost treatment planning
o Two opposing tangential beams were constructed.
o Wedge & MLC were used in forward planning.
o Boost plan consists of 3 equally weighted photon beams.
o The isocenter and dose normalization point were placed
centrally in a slice representative of boost PTV.
o 50Gy /25 fr with boost of 16Gy boost, cumulative dose of
66Gy.

Materials & Methods• SIB fractionation schedule
o For SIB alternative fractionation schedule is necessary.
o Using the linear-quadratic cell survival model, we calculated
fraction sizes and total doses for the breast and boost PTVs that
were biologically equivalent to the total dose delivered to the
PTVs in 2-Gy fractions with the SBT.
o For this purpose, an α/β ratio of 10 Gy for tumour response and
an α/β ratio of 3 Gy for late-responding normal tissues were
used.

Materials & Methods• SIB treatment planning
o The SIB treatment plan was created by copying the sequentially planned breast and boost beams into an integrated treatment plan.
o Same isocenter and dose normalization points were used.
o Breast beams were set to contribute a daily dose of 1.81Gy to
PTV & 0.49Gy to boost PTV.
o Using wedge & MLC 95% isodose closely encompass the boost
PTV in 3 dimensional uniformly.o A cumulative dose plan was calculated, taking into account 28
fractions of 2.3 Gy for the SIB plan.

Materials & Methods• Analyses of target coverage and normal tissue dose
o Both PTV and boost covers 95% of their prescribed dose
o Heart mean dose < 30Gy.
o Volume of both lungs < 20Gy
o Right breast receiving < 10Gy.

Results
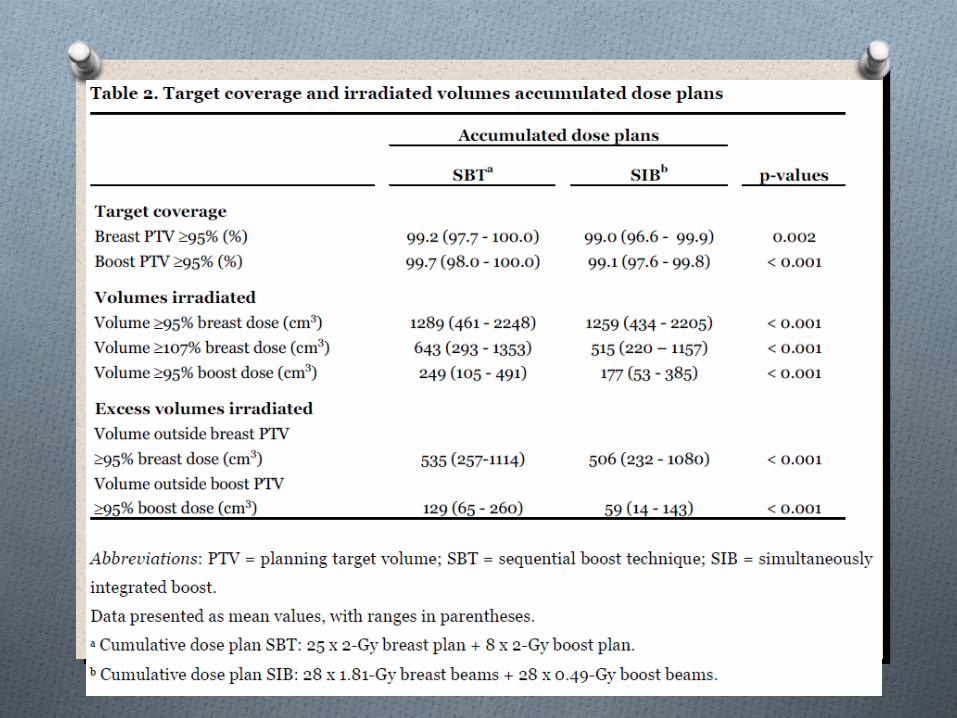
• PTV coverage and absolute volumes irradiated
o At least 95% of the prescribed dose was delivered to
99% of the breast and boost PTVs for the SBT and
SIB plans
o When the SBT beams were constructed, MLC
shielding was applied with a margin of 5–10 mm
outside the boost PTV to obtain adequate coverage.

SIB fractionation scheduleO With SIB technique PTV &boost PTV
combined into an integrated treatment plan.O Alternative fractionation needed.O For schedule we calculate α/β=10Gy for
tumor response & α/β=3Gy for late responding normal tissue.

Results • PTV coverage and absolute volumes irradiated
• Heart mean dose > 30Gy.• Volume of both lungs > 20Gy• Right breast receiving > 10Gy• Acute toxicity
o Grade 0 is 78%o Grade 1 is 60%o Grade 2 is 7.8%o Grade 3 is 31.1%

Disadvantage
• Currently investigating the incidence of late toxicity
because higher dose per fraction delivered to the boost
could cause increase the risk of late fibrosis.
• The lumpectomy cavity shrinks with the time elapsed
since surgery . Therefore, the position and shape of the
breast and boost PTVs should be monitored and
verified during the RT session.

Conclusion
The SIB technique is proposed for standard use in breast-
conserving RT
• reduce excess volumes of normal tissue irradiated
• shorten the treatment course,
• decrease the dose per fraction for the breast and
increase the dose per fraction for the boost
• low incidence of acute skin toxicity.