Chapter 13 Child and Preadolescent Nutrition: Conditions and Interventions

ONLINE ONLY
Three-dimensional analysis of pharyngealairway in preadolescent children with differentanteroposterior skeletal patterns
Yoon-Ji Kim,a Ji-Suk Hong,a Yong-In Hwang,a and Yang-Ho Parkb
Seoul, Korea
Introduction: In growing patients with skeletal discrepancies, early diagnosis, evidence-based explanationsof etiology, and assessment of functional factors can be vital for the restoration of normal craniofacial growthand the stability of the treatment results. The aims of our study were to compare the 3-dimensional pharyngealairway volumes in healthy children with a retrognathic mandible and those with normal craniofacial growth,and to investigate possible significant relationships and correlations among the studied cephalometric vari-ables and the airway morphology in these children. Methods: Three-dimensional airway volume and cross-sectional areas of 27 healthy children (12 boys, 15 girls; mean age, 11 years) were measured by usingcone-beam computed tomography volume scans, and 2-dimensional lateral cephalograms were createdand analyzed. The subjects were divided into 2 groups based on their ANB angles (group I: 2� # ANB # 5�;group II: ANB .5�), and cephalometric variables, airway volumes, and cross-sectional measurements werecompared. Results: There were statistically significant differences in the following parameters: height ofthe posterior nasal plane (P \0.05), pogonion to nasion perpendicular distance (P \0.01), ANB angle(P \0.01), mandibular body length (P \0.01), facial convexity (P \0.01), and total airway volume (P \0.05).No statistically significant differences between the 2 groups were found in the cross-sectional area and thevolumetric measurements of the various sections of the airway except for total airway volume, which hadlarger values in group I (P \0.05). Conclusions: The mean total airway volume, extending from the anteriornasal cavity and the nasopharynx to the epiglottis, in retrognathic patients was significantly smaller thanthat of patients with a normal anteroposterior skeletal relationship. On the other hand, differences in volumemeasurements of the 4 subregions of the airway were not statistically significant between the 2 groups.(Am J Orthod Dentofacial Orthop 2010;137:306.e1-306.e11)
The effects of respiratory function on craniofacialgrowth have been studied for decades, and mostclinicians now understand that respiratory func-
tion is highly relevant to the orthodontic diagnosis andthe treatment plan. In 1907, Angle1 showed that hisClass II Division 1 malocclusion is associated with ob-struction of the upper pharyngeal airway and mouthbreathing. Clinical features related to impaired breath-ing have been observed by some authors, and Ricketts2
presented the main characteristics of the respiratory ob-struction syndrome as adenoid and tonsil hypertrophy,
From the Department of Orthodontics, Kangdong Sacred Heart Hospital,
Hallym University Medical Center, Seoul, Korea.aResident.bAssociate professor.
The authors report no commercial, proprietary, or financial interest in the prod-
ucts or companies described in this article.
Reprint requests to: Yang-Ho Park, Department of Orthodontics, Kangdong
Sacred Heart Hospital, 445 Gil-Dong, Gangdong-Gu, Seoul, Korea, 134-701.
e-mail, [email protected].
Submitted, May 2009; revised and accepted, October 2009.
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2009.10.025
crossbite, open bite, narrow external nares, and tonguethrusting.
Predisposing factors of nasal obstruction can in-clude adenoid and tonsil hypertrophy, polyps, allergies,infections, and nasal deformities. A common cause ofmouth breathing arises from the adenoids, which area conglomerate of lymphatic tissues located in the pos-terior pharyngeal airway. Infection and inflammation ofthe adenoids leads to upper airway obstruction, and theterm ‘‘adenoid facies’’ is often used to describe a possi-ble aberrant craniofacial growth pattern related tomouth breathing characterized by lip incompetency, un-derdeveloped nose, increased anterior facial height,constricted dental arches, and proclined maxillary inci-sors with a Class II occlusal relationship.3,4
In addition to studies that affirm nasal obstruction asthe major factor responsible for dentofacial anomalies,other studies refute a significant relationship betweenairway obstruction and the frequency of malocclusion.In a study of 500 patients with upper airway problems,Leech5 discovered that 60% of the mouth-breathing pa-tients were Class I and concluded that mouth breathing
306.e1

Table I. Sample characteristics
Group I Group II
Male Female Male Female Total
Subjects (n) 7 7 5 8 27
Age (y) (mean 6 SD) 11.46 6 0.69 11.71 6 0.86 10.23 6 0.73 11.09 6 1.03 11.19 6 1.28
Range (y) 10.50-12.58 10.67-12.92 9.42-12.33 9.08-12.17 9.08-12.92
306.e2 Kim et al American Journal of Orthodontics and Dentofacial Orthopedics
March 2010
has no influence on craniofacial growth. Similarly,Gwynne-Evans6 determined that facial growth is con-stant regardless of the mode of breathing. Additionally,Humphreys and Leighton7 found no significant differ-ence in the anteroposterior relationship of the jaws be-tween nose and mouth breathers.
In growing patients with skeletal discrepancies andclinical signs of adenoid facies, early diagnosis, evi-dence-based explanations of etiology, and assessmentof the functional factors might be vital for the restora-tion of normal craniofacial growth and the stability oftreatment results. Morphometric evaluation of the pha-ryngeal airway has been mostly performed on lateralcephalometric headfilms, by identifying specific land-marks and measuring various lengths and areas in thepharyngeal region.8-10
Despite the vast amount of research concerning air-way anatomy and its influence on craniofacial growthand development, most studies have been 2-dimen-sional (2D) and have used lateral or frontal cephalo-grams with limited evaluation of lengths and areas.New 3-dimensional (3D) technology of computed to-mography (CT) has expanded diagnostic capacities,making volumetric analysis and accurate visualizationof the airway possible. Most 3D studies of the airwayused multislice CT to evaluate the airway; this has theadvantage of high-quality images to discern hard- andsoft-tissue anatomies, but, because of the high radiationdose, it is restricted to patients with severe craniofacialdeformities and those undergoing orthognathic surger-ies.11,12 Recently, cone-beam CT (CBCT) systemshave been developed specifically for the maxillofacialregion. Because a CBCT scan uses a different type ofacquisition than traditional multislice CT, radiation isreduced and can be used in a wider range of patients,eg, those having maxillofacial surgery, implantology,and orthodontics.13 Cross-sectional and volumetric in-vestigations of the pharyngeal airway have been possi-ble by using CBCT scans to analyze the complexairway anatomy, and previous studies have confirmedthat volumetric measurements of airways with CBCTare accurate with minimal error.14
The aims of our retrospective, cross-sectional studywere (1) to compare the 3D pharyngeal airway volumes
in healthy children with a retrognathic mandible andthose with normal craniofacial growth and (2) to inves-tigate possible significant relationships and correlationsamong the studied cephalometric variables and the air-way morphology in these children.
MATERIAL AND METHODS
Pharyngeal airway structures were studied in 27healthy children (12 boys, 15 girls) with a mean ageof 11.19 6 1.28 years (Table I) who were referred tothe Department of Orthodontics of Kangdong SacredHeart Hospital, Hallym University Medical Center,Seoul, Korea, for treatment. Those who had symptomsof upper respiratory infection, pharyngeal pathologysuch as adenoid hypertrophy and tonsillitis or a historyof adenoidectomy or tonsillectomy were excluded.
The study protocol was approved by the EthicsReview Committee of the hospital (IRB 09-57).
CBCT volume scans of all subjects were obtainedby using the Master 3D dental-imaging system (Vatech,Seoul, Korea), and the imaging protocol used a 12-infield of view to include the entire craniofacial anatomy.The axial slice thickness was 0.3 mm, and the voxelswere isotropic.
Patients sat upright with natural head position, andtheir jaws were at maximum intercuspation with thelips and tongue in a resting position. The patientswere asked not to swallow and not to move their headsor tongues. Almost all 3D imaging modalities (eg, con-ventional CT or magnetic resonance imaging) requirepatients to be supine; this causes significant morpho-logic changes of the airway, since gravity affects thesoft tissues surrounding the oropharyngeal cavity.15 Itmight be reasonable to examine patients in the supineposition for diagnosing such disorders as obstructivesleep apnea. In most cases (including orthodontic diag-nosis and treatment planning), however, patients do notneed to be analyzed in the supine position. Recent ad-vances in CBCT permit the acquisition of axial CT im-ages in the upright sitting position, which is more validfor our study.
The axial images were imported to InVivoDentalsoftware (Anatomage, San Jose, Calif), and volumetric

Fig 1. A volumetric rendering of a subject’s craniofacial skeleton: A, lateral view right; B, frontal view;C, lateral view left.
Fig 2. For the horizontal reference plane, the FH planewas constructed from the right and left porions and theright orbitale, which was set as the origin.
American Journal of Orthodontics and Dentofacial Orthopedics Kim et al 306.e3Volume 137, Number 3
rendering was done for airway and cephalometric anal-ysis (Fig 1). To standardize the measurements and min-imize errors, the 3D image was reoriented, by using theFrankfort horizontal (FH) plane as its reference plane.The FH plane was constructed from the right and leftporions located in the most laterosuperior point of theexternal auditory meatus and the right orbitale (Fig 2).Cho16 proposed a 3D analysis system from a CBCT vol-umetric image with a set of landmarks, reference lines,and reference planes. In his system, the 3D image is re-oriented according to the nasofrontozygomatic planeand the FH plane. Lagravere et al17 designated referencepoints such as the midpoint between the foramen lac-
erum and the middorsum foramen magnum, since theyare easily viewed in the 3D images.
The 2D cephalometric images were derived fromthe 3D CT scans by creating an orthogonal projectionwith parallel rays, and the images were imported intoV-ceph software (Osstem Implant, Seoul, Korea) forconventional 2D analysis. Landmark identificationsand physical measurements were performed by thesame investigator (Y.J.K). For the cephalometric analy-sis, 13 conventional hard-tissue cephalometric land-marks were identified, and 5 anteroposterior and 5vertical measurements were calculated (Table II, Fig3). The subjects were assigned to 2 groups based ontheir ANB angles: 14 subjects (7 boys, 7 girls) whoseANB angles ranged from 2� to 5� were allocated togroup I, and 13 subjects (5 boys, 8 girls) who hadANB angles greater than 5� were allocated to group II(Table I).
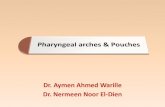
Five cross-sectional planes (2 frontal and 3 axialsections) and 5 volumes of the pharyngeal airwaywere developed in this study based on the FH planeand soft-tissue landmarks (Table III; Figs 4 and 5).Cross-sectional planes of the nasal cavity are perpendic-ular to the FH plane, whereas the pharyngeal cross-sec-tions are parallel to the FH plane. Although these cross-sections are not directly perpendicular to the long axisof the airway, the FH plane was used as a referenceplane to standardize the plane orientation and minimizeerror in identifying the studied cross-sectional planes ofthe subjects. Various dimensions of the airway were cal-culated by the same examiner. Cross-sectional measure-ments including width, length, and area were calculatedin the sectional views (frontal and axial) because theyprovide precise 2D visualization and linear accuracyof 2D measurements (Fig 5).

Fig 3. Landmarks, anteroposterior measurements, andvertical measurements used in this study.
Table II. Two-dimensional cephalometric variables used in this study
Variable Definition
Vertical skeletal pattern
Gonial angle The angle formed by the junction of the posterior and lower borders of the mandible
AFH Distance between nasion and menton
PFH Distance between sella and gonion
FMA The angle formed by the FH plane and the mandibular plane (Go-Me)
AFH/PFH Ratio of AFH to PFH
Anteroposterior skeletal pattern
A to N-perp The linear distance from Point A to nasion perpendicular
Pog to N-Perp The linear distance from pogonion to nasion perpendicular
ANB The difference between SNA and SNB
Mn body length The linear distance of the mandibular plane (Go-Me)
Facial convexity The angle fomed by nasion, Point A, and pogonion
306.e4 Kim et al American Journal of Orthodontics and Dentofacial Orthopedics
March 2010
Volumetric renderings of the subjects’ CT scanswere acquired with the InVivoDental software, and weproceeded with volumetric analysis of the defined air-ways. Since airway is void space surrounded by hardand soft tissues, inversion of the 3D-rendered image isrequired; this converts a negative value to a positivevalue, and vice versa. This process removes the hardand soft tissues of the image and embodies the airwayspaces of the craniofacial region including the paranasalsinuses and other empty spaces. Then sculpting wasdpme to isolate the desired airway section by removingunnecessary structures; subsequently, threshold valueswere adjusted to eliminate imaging artifacts and refine
the selected airway region. Finally, the volume of thedesignated airway was calculated in cubic millimeters.
Lateral cephalometric variables and airway dimen-sions of 15 randomly selected CT scans were remeas-ured by the same investigator 2 weeks after the firstmeasurements. A paired t test was used to estimate sys-temic error, and all measurements were free of systemicerror.18 Random error was estimated by using Dahl-berg’s formula19 (ME2 5 Sd2/2 n). Random errors var-ied from 0.49 to 2.24 mm in linear measurements, from11.33 to 36.12 mm2 in area measurements, and from57.36 to 91.37 mm3 in volume measurements.
Descriptive statistics including the mean and stan-dard deviation for each group were calculated by usingSPSS for Windows software (version 12.0, SPSS, Chi-cago, Ill). Differences between groups I and II, andbetween the sexes, were tested by using independentt tests. Pearson’s correlation coefficient test was usedto detect any relationship of different parts of the airwayand between airway volume and 2D cephalometricvariables.
RESULTS
Means and standard deviations for cephalometric,cross-sectional, and volumetric variables were com-pared by sex; since no sex differences were found inany measurement, the subjects were combined for sub-sequent analysis. Table IV gives the comparison resultsof groups I and II. There were statistically significantdifferences in the following parameters: height of theposterior nasal plane (P\0.05), pogonion to nasion per-pendicular distance (P \0.01), ANB (P \0.01), man-dibular body length (P \0.01), facial convexity(P\0.01), and total airway volume (P\0.05). Accord-ing to the lateral cephalometric analysis, group II hadretruded mandibles and a greater skeletal anteroposte-rior discrepancy, as evidenced by the pogonion to nasion

Table III. Cross-sectional planes and volumes of the 3D pharyngeal airway
Landmark Definition
Cross-sectional plane
Anterior nasal plane Ana plane A frontal plane perpendicular to the FH plane passing
through ANS
Posterior nasal plane Pna plane A frontal plane perpendicular to the FH plane passing
through PNS
Upper pharyngeal plane Uph plane An axial plane parallel to the FH plane passing
through PNS
Middle pharyngeal plane Mph plane An axial plane parallel to the FH plane passing
through the caudal margin of the soft palate
Lower pharyngeal plane Lph plane An axial plane parallel to the FH plane passing
through the superior margin of the epiglottis
Volume
Nasal airway Airway formed by the Ana and Pna planes
Superior pharyngeal airway Airway formed by the Pna and Uph planes
Middle pharyngeal airway Airway formed by the Uph and Mph planes
Inferior pharyngeal airway Airway formed by the Mph and Lph planes
Total airway Airway extending from Ana plane to Lph plane
American Journal of Orthodontics and Dentofacial Orthopedics Kim et al 306.e5Volume 137, Number 3
perpendicular distance, ANB, and facial convexityvalues. No statistically significant difference betweenthe 2 groups was found in the cross-sectional area andvolumetric measurements of the different parts of theairway. However, total airway volume, which is thesum of the 4 separate volumes of the airway, was signif-icantly greater in group I (P\0.05). The linear measure-ments of the cross sections indicated that the height ofthe posterior nasal plane was the only significant meanfound, with greater values in group I (P \0.05).
Tables V and VI show the correlations among thestudied variables. Table V shows the correlations of sec-tions of the airway with each other, and Table VI showscorrelations between the 2D cephalometric variablesand the 3D volumetric measurements of the airway.The nasal airway volume and the superior pharyngealairway volume had a positive correlation (P \0.01).Some analyses from the lateral cephalograms tendedto be correlated with airway volume. The anterior facialheights showed positive correlations to all volumetricmeasurements except the middle pharyngeal airwayvolume. Posterior facial height showed significant cor-relations with total airway volume and inferior pharyn-geal airway volume (P \0.05). Additionally, totalairway volume was significantly correlated with ANBangle and mandibular body length (P \0.05).
DISCUSSION
Although the impact of respiratory function on cra-niofacial growth and its relevance in orthodontics haslong been a controversial issue, many clinical studieshave presented good evidence with sound data support-ing this hypothesis. To evaluate the airway, nasal resis-
tance and airflow tests, nasoendoscopy, and lateralcephalometry have been the primary means used forthe last few decades.20,21 As new-generation CBCT sup-plements the diagnosis and treatment planning of ortho-dontic patients, 3D analyses of the maxillofacialskeleton and the soft tissues are possible. Our study ofthe pharyngeal airway with CBCT produced anatomi-cally true images that are 3D reconstructed withoutmagnification or distortion, allowing accurate measure-ment in all 3 dimensions (sagittal, frontal, and trans-verse) to understand fully the pharyngeal morphologyin growing children.22-24
Because of the retrospective design of this study, di-rect examination of the patients’ nasopharyngeal func-tions was not possible; selection of subjects was basedon previous clinical chart information at their diagnosesfor orthodontic treatment, and CBCT images were usedadditionally to screen subjects with severe adenoid andtonsillar hypertrophy. Area measurements of adenoidsin lateral cephalograms have been reported to have clin-ically useful correlations with gold standards such as ac-tual tissue volumes obtained by adenoidectomy anddirect observations through endoscopy.25-27 However,Aboudara et al28 found that 2D measurements of the na-sopharyngeal airway area lacks much of the structuralinformation, since the 3D structure is compressed intoa 2D image. In our study, subjective grading of the ad-enoid and tonsil sizes in the 3D image was done, and pa-tients with severe adenoid or tonsillar hypertrophy wereconsidered as having infections or allergies, and theywere excluded in this study. As a result, we confirmedthat our patients were free of clinical signs and symp-toms related to pharyngeal pathology and had no historyof treatment intervention (eg, tonsillectomy or

Fig 4. Five cross-sectional planes of the pharyngeal airway used in this study: A, right lateral viewand B, frontal view of volume rendered images. a, Anterior nasal plane (Ana); b, posterior nasal plane(Pna); c, upper pharyngeal plane (Uph); d, middle pharyngeal plane (Mph); e, lower pharyngeal plane(Lph). C, The cross-sectional planes are shown in the lateral cephalogram.
306.e6 Kim et al American Journal of Orthodontics and Dentofacial Orthopedics
March 2010
adenoidectomy) in the pharyngeal area. Thus, we as-sumed that the subjects were relatively healthy andshowed normal patterns of nasorespiratory function.Obviously, this method of patient selection is not ideal,and we could have included patients with mild pharyn-geal diseases that could not be detected. According toa study by Laine-Alava and Minkkinen,29 however,a history or symptoms of upper respiratory diseaseshave no influence on variables related to nasorespiratoryfunction when the measurements are made during anasymptomatic period.
The nasopharyngeal airway is mainly influenced bythe adenoids, which are known to follow the lymphoidgrowth curve shown by Scammon et al.30 They increaserapidly from infancy, reach a peak before adolescence,and then gradually decrease to their adult sizes. Sub-telny and Baker31 concluded that the growth peak ofthe adenoids varies from 9 to 15 years of age. In ourstudy, children aged 9 to 12 years were selected. Ac-cording to the curves of general growth of Scammonet al,30 which the maxillomandibular growth is knownto follow, this period is the end of the second phase ofgrowth when the growth rate is steady and constant be-fore the adolescent growth spurt. Therefore, children atthese preadolescent ages can have adenoids that havereached their maximum size, and considerable facialgrowth has occurred to reflect functional influences be-cause they might be predisposed to the natural anatomicconditions of narrower nasopharyngeal airways.
The 2D lateral cephalometric images were createdfrom the CBCT scans primarily to assign the subjects
to the 2 groups and also to ascertain significant correla-tions among the cephalometric variables and the airwayvolumes. Linear accuracy of the CBCT-derived lateralcephalometric images has been studied.32-34 Moshiriet al35 compared linear measurements of lateral cepha-lograms derived from CBCT with those of conventionalcephalograms and direct measurements on a dry humanskull, which was considered to represent the anatomictruth. For most linear measurements calculated in thesagittal plane, they found that the CBCT-derived 2D lat-eral cephalograms were more accurate than conven-tional lateral cephalograms. Moreover, generation of2D cephalometric images from CBCT data prevents un-necessary irradiation of the patients. Regarding patientpositioning, Hassan et al33 compared linear measure-ments on 3D surface-rendered images, 2D tomographicmultiplanar reformatted slices, and 2D projection im-ages in both ideal and rotated positions of dry humanskulls. They concluded that linear measurements onall 3 images were accurate in the ideal skull position;however, the rotated skull provided linear accuracyonly for 3D surface-rendered images and 2D tomo-graphic slices.
To classify the subjects based on their anteroposte-rior skeletal relationships, Korean norms for the ANBangle were used.36 Several reports about the ANB anglehave indicated its lack of clinical significance and reli-ability in the determination of the anteroposterior jawposition. Hussels and Nanda37 showed that the ANB an-gle is influenced by rotation and vertical growth of thejaws, anteroposterior position of the nasion, and vertical

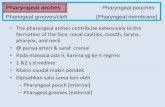
Fig 5. Cross-sectional views of the pharyngeal airway in the 5 planes: a represents the length (axialslice) or height (frontal slice) of the airway defined by the greatest distance in the anteroposterior orvertical direction of the airway cross section; b is the width of the airway defined by the greatest dis-tance in the right and left directions of the airway cross section. The colored region indicates thecross-sectional area of the airway.
American Journal of Orthodontics and Dentofacial Orthopedics Kim et al 306.e7Volume 137, Number 3
distance between Points A and B. Ferrario et al38 sug-gested that the orthodontic diagnosis should be basedon more than 1 anteroposterior appraisal. However,the ANB angle is a commonly used cephalometric pa-rameter in clinical orthodontics,39 and Ishikawa et al40
corroborated that it is reliable for determining the ante-roposterior relationship of the jaws. Additionally, theseauthors showed that the ANB angle and the angle ofconvexity in the prepubertal assessment have high pre-diction accuracy for postpubertal jaw relationships. Inour study, the anteroposterior analyses displayed statis-tically significant differences except Point A to nasionperpendicular distance, reaffirming the reliability ofthe ANB angle, which was used to classify our subjects.
The number of subjects in our study was limited and,therefore, this investigation should be considered a pilotstudy. Because of the small number of subjects, datafrom both sexes were collected, and, fortunately, no sex-ual dimorphism in any cross-sectional and volumetricmeasurements was observed. These findings agreewith those of Ceylan and Oktay41 and Freitas et al.42
Vertical cephalometric means of the 2 groups werewithin normal limits, and no statistically significant
differences in the vertical measurements betweengroups I and II were observed (Table IV), eliminatingthe possible effects of the vertical skeletal pattern thatmight have contributed to the variations of the airwaydimensions. In the longitudinal study of Akcam etal,43 upper and lower pharyngeal airways were mea-sured in preadolescents according to the different rota-tion types, and hyperdivergent subjects had narrowerlower pharyngeal airways.
All cross-sectional area and volumetric measure-ments of the subregions of the pharyngeal airwaywere greater in group I. However, they were not statis-tically significant, indicating that segmental airway ca-pacities are not related to mandibular deficiencies(Table IV). This agrees with previous 2D studies thatclaimed no association of airway dimensions with mal-occlusion types.12,41,42 Ceylan and Oktay41 assertedthat, as skeletal anteroposterior relationship changes,pharyngeal structures undergo postural modifications,and hence the size of the airway remains constant. Inter-estingly, total airway volume, the sum of the 4 subre-gions of the airway from the nasal cavity and thenasopharynx to the oropharyngeal region above the

Table IV. Descriptive statistics of groups I and II
Group I (n 5 14) Group II (n 5 13)Intergroup difference
Mean SD Mean SD P
Ana plane Height 44.62 6.03 40.32 8.67 0.16
Width 16.48 1.55 14.91 3.07 0.11
Cross-sectional area 263.51 71.47 216.92 95.07 0.17
Pna plane Height 22.15 1.17 19.42 2.01 0.03*
Width 25.85 2.14 25.40 2.25 0.61
Cross-sectional area 292.93 70.77 258.04 77.46 0.24
Uph plane Length 22.98 5.61 22.45 4.64 0.79
Width 29.72 5.55 28.63 5.12 0.61
Cross-sectional area 494.93 159.05 467.64 161.03 0.67
Mph plane Length 18.25 5.65 15.44 4.44 0.17
Width 25.38 5.68 23.57 4.11 0.36
Cross-sectional area 321.86 129.11 250.96 99.99 0.13
Lph plane Length 17.34 4.96 16.18 5.39 0.57
Width 29.63 3.12 28.72 4.14 0.53
Cross-sectional area 427.68 183.11 363.66 148.17 0.34
Cephalometric analysis Gonial angle 125.94 5.90 125.30 5.26 0.77
AFH 116.02 5.06 111.96 6.81 0.10
PFH 73.09 5.61 69.32 5.49 0.10
PFH/AFH 0.63 0.04 0.62 0.02 0.41
FMA 29.72 4.05 32.22 2.25 0.06
Point A to nasion perpendicular –1.15 2.87 –1.16 2.29 1.00
Pogonion to nasion perpendicular –6.84 5.05 –12.79 3.91 0.01*
ANB 2.42 1.10 5.85 1.15 \0.01†
Mandibular body length 68.22 4.99 63.10 3.03 \0.01†
Facial convexity 5.04 3.33 12.10 3.18 \0.01†
Airway volume Nasal airway 13479.62 2547.12 11124.00 3302.82 0.06
Superior pharyngeal airway 2620.77 899.23 2138.38 658.27 0.13
Middle pharyngeal airway 1581.23 509.83 1402.92 662.49 0.45
Inferior pharyngeal airway 3278.00 1101.55 2498.77 1095.03 0.08
Total airway 20959.62 3611.26 17164.08 4238.46 0.02*
Linear measurements (mm), area measurements (mm2), volumetric measurements (mm3), angular measurements (�).*P \0.05; †P \0.01.
306.e8 Kim et al American Journal of Orthodontics and Dentofacial Orthopedics
March 2010
epiglottis, appeared to be significantly greater in groupI. From these contrasting results, we inferred that eachsubregion of the upper airway does not specifically rep-resent a patient’s whole upper airway capacity, and,therefore, comprehensive assessment of the entire upperairway is needed in patients who require functional ex-amination. Further studies with larger samples areneeded to investigate certain airway subregions thatmight be significantly correlated to other skeletal pat-terns such as mandibular prognathism and verticalgrowth pattern. Additionally, evaluation of discriminat-ing capacities of airway parts limited by different ana-tomic landmarks might show specific regions of theairway that are responsible for significant relationshipsbetween the airway and the craniofacial structures.
Linear analysis of the cross-sections showed that thenasal airway dimension is influenced by skeletalpattern. The height of the posterior nasal cavity was sig-nificantly greater in group I, and the rest of the cross-sectional dimensions showed greater values in group I,
but they lacked statistical significance. Alves et al12
compared 3D airways of adult skeletal Class II andClass III patients, and concluded that nasal cavity widthhad statistical significance between the 2 groups,whereas the height of the nasal cavity did not. In con-trast, Kikuchi11 found in his 3D airway study that theoropharyngeal region of the airway was influenced bythe skeletal pattern. He maintained that airway mor-phology, rather than size, is influenced by the anteropos-terior position of the mandible and suggested thatairway volume remains constant by horizontal and ver-tical compensation mechanisms of the muscles adjacentto the pharynx.
Nasal airway volume and superior pharyngeal air-way volume were positively correlated (Table V), indi-cating a close relationship of the anterior and posteriorparts of the upper airway. Located above the hard palate,these 2 sections of the airway are not only anatomicallyadjacent, but also their volumetric dimensions havea direct relationship. Linder-Aronson3 studied the

Table V. Correlations among airway volumes
Nasalairway
Superior pharyngealairway
Middle pharyngealairway
Inferior pharyngealairway
Nasal airway Pearson correlation 1 0.542 0.343 0.159
P value ˙ 0.004* 0.086 0.437
Superior pharyngeal airway Pearson correlation 0.542 1 0.199 0.362
P value 0.004* ˙ 0.330 0.069
Middle pharyngeal airway Pearson correlation 0.343 0.199 1 0.375
P value 0.086 0.330 ˙ 0.059
Inferior pharyngeal airway Pearson correlation 0.159 0.362 0.375 1
P value 0.437 0.069 0.059 ˙
*P \0.01.
Table VI. Correlations between cephalometric variables and airway volumes
Gonial angle AFH PFH PFH/AFH FMA Pt A to N perp Pog to N perp ANB Mn body Facial conv
Nasal airway Pearson
correlation
0.01 0.57 0.37 0.00 0.00 –0.12 0.05 –0.36 0.33 –0.28
P value 0.95 \.01† 0.07 0.99 0.99 0.56 0.80 0.07 0.10 0.16
Superior pharyngeal
airway
Pearson
correlation
–0.13 0.51 0.39 0.07 –0.10 –0.09 –0.07 –0.14 0.33 –0.09
P value 0.53 \.01† 0.06 0.74 0.63 0.67 0.73 0.49 0.10 0.66
Middle pharyngeal
airway
Pearson
correlation
0.15 0.33 0.19 –0.04 –0.01 0.07 0.21 –0.31 0.22 –0.25
P value 0.46 0.10 0.36 0.83 0.95 0.73 0.31 0.13 0.27 0.23
Inferior pharyngeal
airway
Pearson
correlation
–0.33 0.41 0.39 0.18 –0.37 –0.15 0.06 –0.32 0.32 –0.34
P value 0.10 0.03* 0.04* 0.39 0.06 0.46 0.77 0.12 0.11 0.09
Total airway Pearson
correlation
–0.08 0.66 0.47 0.05 –0.12 –0.13 0.07 –0.42 0.42 –0.35
P value 0.70 \.01† 0.02* 0.80 0.57 0.52 0.74 0.03* 0.03* 0.08
Pt, Point; N, nasion; perp, perpendicular; Pog, pogonion; Mn, mandibular; conv, convexity.
*P \0.05; †P \0.01.
American Journal of Orthodontics and Dentofacial Orthopedics Kim et al 306.e9Volume 137, Number 3
relationship of the upper and lower parts of the airway,and reported that a smaller nasopharyngeal airway is ac-companied by a larger oropharyngeal airway. Ricketts2
and Dunn et al44 stated that oral breathing is related toa narrow nasopharyngeal airway width because it is eas-ily blocked by adenoid enlargement. In our study, nosignificant correlations were found among the rest ofthe airway volumes below the hard palate.
The relationship of conventional cephalometricanalyses and airway volumes were evaluated; anteriorand posterior facial heights were positively correlatedto nasal, superior pharyngeal, and inferior pharyngealairways, as well as to total airway volume (Table VI).This indicates that patients with vertical growth patternsare likely to have an expanded airway; this is inconsis-tent with studies that reported an inverse relationshipbetween pharyngeal volume and vertical facialheight.2,3,42,44,45 However, the variables used to assessvertical craniofacial patterns are different from thoseused in previous studies; this makes the comparison
less compatible. Interestingly, anterior facial heightshowed strong correlations (P \0.01) to the upperpart of the airway, and the nasal and superior pharyngealairway; this agrees with Freitas et al,42 who noted thatvertical growth patterns have significant correlationswith the upper part of pharyngeal airways.
Anteroposterior discriminants such as ANB angleand mandibular body length showed significant correla-tions with total airway volume, supporting the inter-group comparison of different anteroposterior skeletalpatterns in this study. The negative correlation of theANB angle and the total airway can be explained bygroup I (2�#ANB#5�) having significantly greater air-way volume than group II (ANB .5�). Mandibularbody length and total airway volume were both signifi-cantly greater in group I (Table IV), demonstratinga positive correlation. Hwang et al46 reported that a con-stricted nasopharyngeal airway is associated withretruded mandible and maxilla. On the other hand,Abu Allhaija and Al-Khateeb47 concluded that

306.e10 Kim et al American Journal of Orthodontics and Dentofacial Orthopedics
March 2010
anteroposterior pharyngeal airway dimensions were notaffected by changes of the ANB angle. Since these pre-vious studies were based on lateral cephalograms, more3D studies are needed to clarify this conflicting issue.
The standard deviations of the airway dimensionswere significantly large in cross-sectional area and vol-umetric measurements. This agreed with the findings ofOzbek et al,48 who analyzed airway dimensions includ-ing width, area, and angulation in lateral headfilms ofskeletal Class II growing children. The area measure-ment of the oropharnynx had large standard deviations,whereas the rest of the measurements such as airwaywidth and angulation showed narrow ranges. The wideranges of certain airway data were also evident in an-other study of airway morphology in skeletal Class IIand Class III adults.12 Whereas angular and linear mea-surements on the 3D airway model were typical of thedesignated lengths and angles, cross-sectional areasand volumes showed markedly large standard devia-tions in both skeletal types.
In a comparative study of the nasopharyngeal air-way size using a lateral cephalometric headfilm anda CBCT scan, Aboudara et al14 found that volume hasa much wider range than area of the same region ofthe airway, asserting that determination of airway vol-ume from 2D lateral cephalograms is inaccurate be-cause of inconsistencies of the 3D airway anatomy.Determined as percentages of the means, the standarddeviations of the area and volume in our study rangedfrom 24% to 43% and 17% to 47%, respectively, indi-cating great variability in both parameters. Sincea CBCT scan provides the most accurate dimensionalanalysis, it could be interpreted that much anatomic in-formation is lost when the imaging modalities are 2D,and linear and angular measurements do not giveenough information about the targeted structure.14,22-24
We showed that healthy preadolescent children withretruded mandibles have decreased total pharyngeal air-way volumes. Therefore, orthodontists should be awareof the pharyngeal morphologies that might predisposethese children to impaired craniofacial growth. Futureinvestigations of longitudinal airway changes in patientswith different skeletal patterns and assessment of theircraniofacial growth with 3D superimpositions willallow better understanding of the relationship betweenrespiratory function and craniofacial morphology.
CONCLUSIONS
The number of subjects available for this investiga-tion was small; therefore, it should be considered a pilotstudy. It was conducted to examine a possible signifi-cant relationship between airway size and maxillom-
andibular growth patterns in healthy preadolescentchildren without evident pharyngeal pathology. Accord-ing to our results, we can conclude the following.
1. Accurate volumetric determination of 3D pharyn-geal airway is possible in preadolescents by usingCBCT scans.
2. There is no sexual dimorphism in the 2D lateralcephalometric analysis or the 3D airway measure-ments of preadolescents.
3. The mean total airway volume, extending from theanterior nasal cavity and the nasopharynx to theepiglottis, of retrognathic patients was significantlysmaller than that of patients with a normal antero-posterior skeletal relationship. On the other hand,differences in volume measurements of the 4 subre-gions of the airway were not found to be signifi-cantly different between the 2 groups.
4. In preadolescents, volumetric measurements of theairway are significanlty correlated to anteroposte-rior and vertical cephalometric variables, mainlyanterior facial height and ANB angle.
We thank Kyung-Min Oh for her contributions todata collection for this study.
REFERENCES
1. Angle E. Treatment of malocclusion of the teeth. Philadelphia: SS
White Manufacturing Company; 1907.
2. Ricketts RM. Respiratory obstruction syndrome. Am J Orthod
1968;54:495-507.
3. Linder-Aronson Adenoids S. Their effect on mode of breathing
and nasal airflow and their relationship to characteristics of the fa-
cial skeleton and the denition. A biometric, rhino-manometric and
cephalometro-radiographic study on children with and without
adenoids. Acta Otolaryngol Suppl 1970;265:1-132.
4. Moore A. Observations on mouth breathing. Bull N Z Soc Perio-
dontol 1972;9-11.
5. Leech H. A clinical analysis of orofacial morphology and behav-
ior of 500 patients attending an upper respiratory research clinic.
Dent Pract 1958;9:57-68.
6. Gwynne-Evans E. Discussion on the mouth-breather. Proc R Soc
Med 1958;51:279-82.
7. Humphreys HF, Leighton BC. A survey of antero-posterior abnor-
malities of the jaws in children between the ages of 2 and 5 1/2
years of age. Br Dent J 1950;88:3-15.
8. Arun T, Isik F, Sayinsu K. Vertical growth changes after adenoi-
dectomy. Angle Orthod 2003;73:146-50.
9. Kirjavainen M, Kirjavainen T. Upper airway dimensions in Class
II malocclusion. Effects of headgear treatment. Angle Orthod
2007;77:1046-53.
10. Martin O, Muelas L, Vinas MJ. Nasopharyngeal cephalometric
study of ideal occlusions. Am J Orthod Dentofacial Orthop
2006;130:436.e1-9.
11. Kikuchi Y. Three-dimensional relationship between pharyngeal
airway and maxillo-facial morphology. Bull Tokyo Dent Coll
2008;49:65-75.
12. Alves PV, Zhao L, O’Gara M, Patel PK, Bolognese AM. Three-di-
mensional cephalometric study of upper airway space in skeletal

American Journal of Orthodontics and Dentofacial Orthopedics Kim et al 306.e11Volume 137, Number 3
Class II and III healthy patients. J Craniofac Surg 2008;19:
1497-507.
13. Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Do-
simetry of 3 CBCT devices for oral and maxillofacial radiology:
CB Mercuray, NewTom 3 G and i-CAT. Dentomaxillofac Radiol
2006;35:219-26.
14. Aboudara C, Nielsen I, Huang JC, Maki K, Miller AJ, Hatcher D.
Comparison of airway space with conventional lateral headfilms
and 3-dimensional reconstruction from cone-beam computed
tomography. Am J Orthod Dentofacial Orthop 2009;135:468-79.
15. Battagel JM, Johal A, Smith AM, Kotecha B. Postural variation in
oropharyngeal dimensions in subjects with sleep disordered
breathing: a cephalometric study. Eur J Orthod 2002;24:263-76.
16. Cho HJ. A three-dimensional cephalometric analysis. J Clin
Orthod 2009;43:235-52.
17. Lagravere MO, Hansen L, Harzer W, Major PW. Plane orientation
for standardization in 3-dimensional cephalometric analysis with
computerized tomography imaging. Am J Orthod Dentofacial
Orthop 2006;129:601-4.
18. Houston WJ. The analysis of errors in orthodontic measurements.
Am J Orthod 1983;83:382-90.
19. Dahlberg G. Statistical methods for medical and biological stu-
dents. London, United Kingdom: G: Allen & Unwin; 1940.
20. Major MP, Flores-Mir C, Major PW. Assessment of lateral ceph-
alometric diagnosis of adenoid hypertrophy and posterior upper
airway obstruction: a systematic review. Am J Orthod Dentofacial
Orthop 2006;130:700-8.
21. Vig KW. Nasal obstruction and facial growth: the strength of ev-
idence for clinical assumptions. Am J Orthod Dentofacial Orthop
1998;113:603-11.
22. Parks ET. Computed tomography applications for dentistry. Dent
Clin North Am 2000;44:371-94.
23. Mah J, Hatcher D. Three-dimensional craniofacial imaging. Am
J Orthod Dentofacial Orthop 2004;126:308-9.
24. Ziegler CM, Woertche R, Brief J, Hassfeld S. Clinical indications
for digital volume tomography in oral and maxillofacial surgery.
Dentomaxillofac Radiol 2002;31:126-30.
25. Maw AR, Jeans WD, Fernando DCJ. Inter-observer variability in
the clinical and radiological assessment of adenoid size, and the
correlation with adenoid volume. Clin Otolaryngol Allied Sci
1981;6:317-22.
26. Holmberg H, Linder-Aronson S. Cephalometric radiographs as
a means of evaluating the capacity of the nasal and nasopharyn-
geal airway. Am J Orthod 1979;76:479-90.
27. Jeans WD, Fernando DC, Maw AR. How should adenoidal en-
largement be measured? A radiological study based on interob-
server agreement. Clin Radiol 1981;32:337-40.
28. Aboudara CA, Hatcher D, Nielsen IL, Miller A. A three-dimen-
sional evaluation of the upper airway in adolescents. Orthod Cra-
niofac Res 2003;6:173-5.
29. Laine-Alava MT, Minkkinen UK. Should a history of nasal symp-
toms be considered when estimating nasal patency? Angle Orthod
1999;69:126-32.
30. Scammon RE, Harris JA, Jackson CM. The measurement of man.
Minneapolis: University of Minnesota Press; 1930.
31. Subtelny JD, Baker HK. The significance of adenoid tissue in
velopharyngeal function. Plast Reconstr Surg 1956;17:235-50.
32. Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG.
Linear accuracy of cone beam CT derived 3D images. Angle
Orthod 2009;79:150-7.
33. Hassan B, van der Stelt P, Sanderink G. Accuracy of three-dimen-
sional measurements obtained from cone beam computed tomog-
raphy surface-rendered images for cephalometric analysis:
influence of patient scanning position. Eur J Orthod 2009;31:
129-34.
34. Kumar V, Ludlow J, Soares Cevidanes LH, Mol A. In vivo com-
parison of conventional and cone beam CT synthesized cephalo-
grams. Angle Orthod 2008;78:873-9.
35. Moshiri M, Scarfe WC, Hilgers ML, Scheetz JP, Silveira AM,
Farman AG. Accuracy of linear measurements from imaging plate
and lateral cephalometric images derived from cone-beam com-
puted tomography. Am J Orthod Dentofacial Orthop 2007;132:
550-60.
36. Joo MJ. Analysis of the dento-facial complex in Koreans. Korean
J Orthod 1970;1:21-7.
37. Hussels W, Nanda RS. Analysis of factors affecting angle ANB.
Am J Orthod 1984;85:411-23.
38. Ferrario VF, Sforza C, Miani A Jr, Tartaglia GM. The use of linear
and angular measurements of maxillo-mandibular anteroposterior
discrepancies. Clin Orthod Res 1999;2:34-41.
39. Del Santo M Jr. Influence of occlusal plane inclination on ANB
and Wits assessments of anteroposterior jaw relationships. Am
J Orthod Dentofacial Orthop 2006;129:641-8.
40. Ishikawa H, Nakamura S, Iwasaki H, Kitazawa S. Seven parame-
ters describing anteroposterior jaw relationships: postpubertal
prediction accuracy and interchangeability. Am J Orthod Dentofa-
cial Orthop 2000;117:714-20.
41. Ceylan I, Oktay H. A study on the pharyngeal size in different
skeletal patterns. Am J Orthod Dentofacial Orthop 1995;108:
69-75.
42. de Freitas MR, Alcazar NM, Janson G, de Freitas KM,
Henriques JF. Upper and lower pharyngeal airways in subjects
with Class I and Class II malocclusions and different growth pat-
terns. Am J Orthod Dentofacial Orthop 2006;130:742-5.
43. Akcam MO, Toygar TU, Wada T. Longitudinal investigation of
soft palate and nasopharyngeal airway relations in different rota-
tion types. Angle Orthod 2002;72:521-6.
44. Dunn GF, Green LJ, Cunat JJ. Relationships between variation
of mandibular morphology and variation of nasopharyngeal
airway size in monozygotic twins. Angle Orthod 1973;43:
129-35.
45. Behlfelt K, Linder-Aronson S, McWilliam J, Neander P, Laage-
Hellman J. Cranio-facial morphology in children with and without
enlarged tonsils. Eur J Orthod 1990;12:233-43.
46. Hwang YI, Lee KH, Lee KJ, Kim SC, Cho HJ, Cheon SH, et al.
Effect of airway and tongue in facial morphology of prepubertal
Class I, II children. Korean J Orthod 2008;38:74-82.
47. Abu Allhaija ES, Al-Khateeb SN. Uvulo-glosso-pharyngeal
dimensions in different anteroposterior skeletal patterns. Angle
Orthod 2005;75:1012-8.
48. Ozbek MM, Memikoglu TU, Gogen H, Lowe AA, Baspinar E.
Oropharyngeal airway dimensions and functional-orthopedic
treatment in skeletal Class II cases. Angle Orthod 1998;68:
327-36.