[This handout is formatted for front-to-back printing] · [This handout is formatted for...
35
[This handout is formatted for front-to-back printing] Foundation Management Services, Inc. 2017 [Page 1 of 35]
-
Upload
vuongthien -
Category
Documents
-
view
217 -
download
0
Transcript of [This handout is formatted for front-to-back printing] · [This handout is formatted for...
![Page 1: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/1.jpg)
[This handout is formatted for front-to-back printing]
Foundation Management Services, Inc. 2017 [Page 1 of 35]
![Page 2: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/2.jpg)
Learning Outcome:2
�The learning outcome of this education activity is to enhance the knowledge of the home health Registered Nurse in the area of the OASIS-C2 dataset in the area of compliant data collection by addressing specific guidance and tools related to the new/changed OASIS items and significant changes in Integumentary guidance to ensure greater understanding of accurate OASIS-C2 data collection is achieved as evidenced by positive feedback from participants.
OASIS-C2 Dataset Changes
Why OASIS-C2?4
�“Improving Medicare Post-Acute Care Transformation Act of 2014” (IMPACT)� IMPACT is the driving force behind the OASIS-C2 revision� IMPACT requires post-acute care (PAC) providers to standardize patient assessment and quality data
�PAC providers affected by IMPACT & assessment instrument:� Long-term Care Hospitals – LTCH� Continuity Assessment Record and Evaluation (CARE)
� Inpatient Rehab Facilities – IRF� IRF-Patient Assessment Instrument (IRF-PAI)
� Skilled Nursing Facilities – SNF�Minimum Data Set (MDS)
� Home Health Agencies – HHA�Outcome and Assessment Information Set (OASIS)
Why OASIS-C2?5
� IMPACT requires PAC providers to begin reporting standardized assessment data for 5 quality measure domains according to these dates (with cross-setting standardization complete by 2019):
Quality Measure
Domain
LTCH IRF SNF HHA
Functional status & cognitive function
10/1/2018 10/1/2016 10/1/2016 1/1/2019
Skin integrity 10/1/2016 10/1/2016 10/1/2016 1/1/2017
Medication reconciliation 10/1/2018 10/1/2018 10/1/2018 1/1/2017
Incidence of major falls 10/1/2016 10/1/2016 10/1/2016 1/1/2019
Providing for transfer of health information and care preferences
10/1/2018 10/1/2018 10/1/2018 1/1/2019
Foundation Management Services, Inc. 2017 [Page 2 of 35]
![Page 3: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/3.jpg)
Which IMPACT measures?6
OASIS data collection for these two IMPACT measures began January 2017:�Percentage of Patients with Pressure Ulcers that are New or Worsened
�Drug Regimen Review Conducted with Follow-up for Identified Issues
Skin integrity 1/1/2017
Medication reconciliation 1/1/2017
Quality Measure
DomainHHA
Where does new risk for data inaccuracy exist in OASIS-C2?
7
�Three NEW standardized items�Renumbered items due to modification required to standardize with other PAC data collection
�Renumbered items due to the change to a uniform
“look-back” period
�Changes in guidance (OASIS Guidance Manual)�Chapter 1: NEW OASIS Convention regarding “dash value”
�Chapter 3: Includes several significant changes in guidance (specifically for this presentation, pressure ulcer guidance)� Review the entire Chapter 3 for changes not discussed today!
Items affected by “dash” guidance8
The dash ( – ) value indicates that no information is available, and/or an item could not be assessed (before the OASIS assessment was completed).
CMS expects dash
use to be a rare
occurrence.
� The dash is a valid response ONLY
for the following items:
� (M1028) Active Diagnoses
� (M1060) Height & Weight
� (M1313) Worsening in Pressure Ulcer Status since SOC/ROC
� (GG0170C) Mobility
� (M2001) Drug Regimen Review
� (M2003) Medication Follow-up
� (M2005) Medication Intervention
NEW items - added due to IMPACT
New standardized items10
�The three new items are risk-adjustment covariates for the “Percentage of Patients with Pressure Ulcers that are New or Worsened” outcome measure� (M1028) Active Diagnoses� (M1060) Height & Weight� (GG0170C) Mobility – Lying to sitting on side of bed
�Risk-Adjustment concepts for home care�Risk-adjustment is based on statistical models calculated using the national sample of HHA patients in order to predict the individual patient’s outcomes
� Information that contributes risk-adjustment potential is gathered at the SOC & ROC time points
� For each home health quality measure, an OASIS item that contributes to risk-adjustment potential is statistically meaningful as a predictor of whether a patient is “more likely” or “less likely” to achieve that outcome at Discharge
Foundation Management Services, Inc. 2017 [Page 3 of 35]
![Page 4: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/4.jpg)
(M1028) Active Diagnoses11
�Identifies whether two specific diagnosis categories
are present and active
�These diagnoses influence a patient’s functional
outcomes or increase a patient’s risk for
development or worsening of pressure ulcer
Foundation Management Services, Inc. 2017 [Page 4 of 35]
![Page 5: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/5.jpg)
(M1028) Active Diagnoses12
�Steps for Assessment�Identify diagnoses:
�Only diagnoses confirmed and documented in the medical record by a physician (or nurse practitioner, physician assistant, clinical nurse specialist) should be considered for this item
�Once a diagnosis has been identified, determine if the diagnosis is active
�Determine whether diagnoses are active:� Active diagnoses are diagnoses that have a direct
relationship to the patient’s current: � Functional, cognitive, mood or behavior status;�Medical treatments;�Nurse monitoring (examples include serial blood pressure evaluation, medication management); or
� Risk of death at the time of the assessment
(M1028) Active Diagnoses13
�Determine whether diagnoses are active, continued:�Do not include diseases or conditions that have been resolved or do not affect the patient’s current status, treatments, monitoring, or risk of death at the time of assessment
� If information regarding active diagnoses is learned after the (M0090) Assessment Completed Date, the OASIS should not be revised to reflect this new information� The OASIS should reflect what was known and documented at the time of the SOC or ROC assessment
�OASIS Q&A, Category 4b, Q46.3:� If the clinician confirmed the diagnosis during the completion timeframe, reporting the diagnosis in M1028 is appropriate
(M1028) Active Diagnoses14
�Active diagnoses include these ICD-10 codes
Response 1 – PVD/PAD Codes start with:
I70.2 Atherosclerosis of native arteries of the extremities
I70.3 Atherosclerosis of bypass graft(s) of the extremities
I70.4 Atherosclerosis of autologous vein bypass graft(s) of the extremities
I70.5 Atherosclerosis of non-autologous biological bypass graft(s) of extremities
I70.6 Atherosclerosis of non-biological bypass graft(s) of the extremities
I70.7 Atherosclerosis of other type of bypass graft(s) of the extremities
I70.91 Generalized atherosclerosis
I70.92 Chronic total occlusion of artery of the extremities
I73. Other peripheral vascular diseases
(M1028) Active Diagnoses15
Patient with BOTH Diabetes and PVD/PAD?�4th character “5” (E--.5-) Diabetes with circulatory complications
� .51 Diabetes with diabetic peripheral angiopathy w/o gangrene� .52 Diabetes with diabetic peripheral angiopathy with gangrene� .59 Diabetes with other circulatory complications
� This patient would not be coded with a listed PVD/PAD code (UNLESS the physician indicates the PVD/PAD is not due to DM)
� For M1028, select Response 2 & leave Response 1 unchecked
Response 2 – DM Codes start with:
E08. Diabetes mellitus due to underlying conditions
E09. Drug or chemical induced diabetes mellitus
E10. Type 1 diabetes mellitus
E11. Type 2 diabetes mellitus
E13. Other specific diabetes mellitus
(M1028) Active Diagnoses16
�OASIS Q&A, Category 4b, Q46.2.�If the assessment is completed and it is determined
that the patient does not have a diagnosis of
diabetes, PVD, or PAD, both boxes should be left
unchecked. Implementation of documentation or auditing strategies to ensure accurate completion of the comprehensive assessment are at the discretion of your organization.
Foundation Management Services, Inc. 2017 [Page 5 of 35]
![Page 6: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/6.jpg)
(M1060) Height and Weight17
�Diminished nutritional/hydration status can adversely affect wound healing & increase risk for new or worsened pressure ulcers
�These measures support calculation of the patient’s body mass index (BMI)
Foundation Management Services, Inc. 2017 [Page 6 of 35]
![Page 7: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/7.jpg)
(M1060) Height and Weight18
�Measure and record height in whole inches�When reporting height for a patient with bilateral
lower extremity amputation, measure and record the patient’s current height (that is, the patient’s height after bilateral amputation)
�Measure and record weight in whole pounds�If a patient cannot be weighed (for example, because
of extreme pain, immobility, or risk of pathological fractures), enter the dash value and document the rationale in the patient’s record
(M1060) Height and Weight19
�OASIS Q&A, Category 4b, Q62.9�The assessing clinician is expected to weigh and
measure the patient as part of the comprehensive assessment. Data collection for M1060 by self-report or from paperwork from another provider setting is not acceptable.
(M1060) Height and Weight20
From CMS’ PAC HHQRP Training (Nov 2016 – live Q&A session)� In response to a question asking for clarification of response
wording, trainer stated:� M1060, b-weight includes the phrase “Base weight on most
recent measure in last 30 days.” An example of when/how this would apply is a patient who is weighed at SOC by the home health clinician and the weight is entered in M1060b. On a subsequent date, the patient is transferred to the hospital and then returns home with a new cast, rendering the patient unable to be weighed accurately at ROC. A weight which was obtained at SOC (when the SOC is within the last 30 days prior to ROC) would meet criteria to be entered in M1060b at the ROC assessment. Weights obtained from another provider source (such as the hospital, in this example) would not be acceptable.
Foundation Management Services, Inc. 2017 [Page 7 of 35]
![Page 8: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/8.jpg)
Foundation Management Services, Inc. 2017 [Page 8 of 35]
![Page 9: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/9.jpg)
(GG0170C) Mobility22
�Clinician will enter a code based on a 6-point scale for BOTH columns 1 & 2:�1-SOC/ROC Performance – the patient’s current usual status in need for assistance while moving from lying on the back to sitting on the side of the bed with feet flat on the floor and with no back support
�2-Discharge Goal – in conjunction with patient & family input, determination of patient’s expectation to make functional progress
(GG0170C) Mobility23
�Steps for Assessment�Assess the patient’s functional status based on direct observation and/or on report by the patient, caregiver/family
�Patients should be allowed to perform activities as independently as possible, as long as they are safe
�If caregiver assistance is required because patient’s performance is unsafe or of poor quality, enter the response according to amount of assistance required to be safe
(GG0170C) Mobility24
�Steps for Assessment, continued�Activities may be completed with or without assistive device(s)�Use of assistive device(s) to complete this activity should not affect the scoring of the activity
�If the patient’s self-care performance varies during the assessment time frame, report the patient’s usual status, not the patient’s most independent status and not the patient’s most dependent status
(GG0170C) Mobility25
�Instructions for GG0170C1-SOC/ROC Performance, report the patient’s usual status at SOC/ROC using the 6-point scale or the 3 “activity not attempted” codes�06-Independent: Patient completes the activity by him/herself with no human assistance
�05-Setup or clean-up assistance: If caregiver sets up or cleans up, patient completes activity� Caregiver assists only prior to or following the activity, but not during the activity � For example, the patient only requires assist from a caregiver to remove bedding from lower body
Foundation Management Services, Inc. 2017 [Page 9 of 35]
![Page 10: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/10.jpg)
(GG0170C) Mobility26
�Instructions for GG0170C1-SOC/ROC Performance, continued�04-Supervision or touching assistance: Caregiver
must provide verbal cues or touching/steadying assistance as patient completes activity
�03-Partial/moderate assistance: Caregiver must provide less than half the effort� Caregiver lifts, holds, or supports trunk or limbs, but provides
less than half the effort�02-Substantial/maximal assistance: Caregiver must
provide more than half the effort� Caregiver lifts or hold trunk or limbs and provides more than
half the effort
(GG0170C) Mobility27
� Instructions for GG0170C1-SOC/ROC Performance, continued�01-Dependent: Caregiver must provide all of the effort
� Patient is unable to contribute any of the effort to complete the activity; <OR>
� The assistance of two or more caregivers is required for patient to complete the activity
�Compare/contrast this “01-Dependent” definition with OASIS Q&A, Category 4b, Q127.4 for M1800-M1900:� The response related to “assistance of another person” includes
those patients, actively participating in performing a task, but needing assistance of one or more person(s) to safely complete included tasks.
(The patient in this Q&A is NOT considered dependent when actively participating – despite the number of assisting persons required for safe completion of the activity. However, GG0170C guidance dictates that assistance of 2+ caregivers makes patient dependent.)
(GG0170C) Mobility28
�Instructions for GG0170C1-SOC/ROC Performance, continued�If the patient does not attempt the activity and the
caregiver does not complete the activity for the patient, report the reason the activity was not completed� 07-Patient refused
� 09-Not applicable: Patient did not perform this activity prior to the current illness, exacerbation, or injury
� 88-Not attempted due to medical condition or safety
concerns
(GG0170C) Mobility29
� Instructions for GG0170C2-Discharge Goal, report the discharge goal using the 6-point scale. �Do not enter 07, 09, or 88 to report the discharge goal�The assessing clinician, in conjunction with the patient and
family input, can establish the discharge goal� Patient is expected to make functional progress by discharge,
DC Goal response will be higher (more independent) than the SOC/ROC Performance score
� Patient is not expected to make progress during the episode, but is expected to be able to maintain SOC/ROC functional level, DC Goal response will be the same as the SOC/ROC Performance score
� Patient with a progressive neurological condition is expected to decline even though therapy services may slow the decline of function, the DC Goal response would be lower (more dependent) than the SOC/ROC Performance score
Renumbered – to standardize PAC data for IMPACT measures
Renumbered due to changes made to standardize with other PAC instruments
31
�(M1311) Current Number of Unhealed Pressure Ulcer�(M1313) Worsening in Pressure Ulcer Status�(M2001) Drug Regimen Review�(M2003) Medication Follow-up�(M2005) Medication Intervention
Foundation Management Services, Inc. 2017 [Page 10 of 35]
![Page 11: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/11.jpg)
Foundation Management Services, Inc. 2017 [Page 11 of 35]
![Page 12: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/12.jpg)
M1311 Guidance33
�(M1311) Current Number of Unhealed Pressure Ulcers at Each Stage�At SOC/ROC:� For each row, enter number currently present� (A1, B1, C1, D1, E1, F1)
�At Follow-up & Discharge:� For each row, enter number currently present� (A1, B1, C1, D1, E1, F1)
<AND>� For each row, enter the number of current pressure ulcers that were present at most recent SOC/ROC� (A2, B2, C2, D2, E2, F2)
M1311 Guidance34
�Determining “Present at most recent SOC/ROC”�For each pressure ulcer, determine whether the pressure ulcer was present at the time of the most recent SOC/ROC (did not form during the home health quality episode)
� If the ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge its “present at SOC/ROC” stage should be considered the stage at which it first became numerically stageable� If it subsequently increases in numerical stage, do not report
the higher stage ulcer as being “present at SOC/ROC” when competing the Discharge assessment
� EXAMPLE: Suspected DTI at SOC that opens to reveal full-thickness loss with exposed bone during week 2 (Stage 4).� At Discharge, C1 Stage 4 ulcers currently present = 1� C2 = 1 (ulcer was Stage 4 when it first became stageable)
M1311 Guidance35
�Determining “Present at most recent SOC/ROC”, continued�The general standard of practice in PAC settings is that patient assessments are completed as close to the actual time of the SOC/ROC as possible.� If a pressure ulcer that is identified on the SOC date increases in numerical stage (worsens) within the assessment time frame, the initial stage of the pressure ulcer would be reported in M1311 at the SOC
� EXAMPLE: Patient with one pressure ulcer (Stage 2) on left buttock identified on SOC Date. That ulcer worsened to Stage 3 on day 5 of the episode.� A1 Stage 2 ulcers currently present at SOC = 1� A2 Stage 3 ulcers currently present at SOC = 0
M1311 Guidance36
�NOTE: when completing A2, B2, C2, D2, E2, F2 at Follow-up & Discharge, the current ulcer must have been present at the most recent SOC/ROC at that same stage �EXAMPLE: A Stage 1 at SOC that progressed to Stage 2 by Discharge is NOT considered present at SOC/ROC on the Discharge assessment� A1 Stage 2 ulcers currently present at Discharge = 1� A2 = 0 (that Stage 2 ulcer was NOT present as a Stage 2 at SOC)
Foundation Management Services, Inc. 2017 [Page 12 of 35]
![Page 13: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/13.jpg)
OASIS-C2 (M1313)37
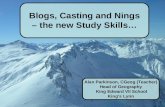
M1313 Guidance38
�(M1313) Worsening in Pressure Ulcer Status since SOC/ROC�At Discharge, enter number of ulcers present that were not present (are new) or have worsened (increased in numerical stage) since the most recent SOC/ROC:
�Reporting Algorithm for M1313 � EVERY clinician needs a copy of this tool!
Foundation Management Services, Inc. 2017 [Page 13 of 35]
![Page 14: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/14.jpg)
OASIS-C2 Guidance Manual (Effective 1/1/2017)
Reporting Algorithm for M1313
CURRENT STAGE at Discharge
Look back to most recent SOC/ROC
PRIOR STAGE at most recent SOC/ROC
REPORT AS NEW OR WORSENED?
a. Stage 2 at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present
Stage 1
Covered with a non-removable dressing/device, then documented as a Stage 1 at any home visit or Follow-up assessment(s)
YES
Stage 2 NO
Stage 3
Stage 4
NA (Stage 3 or 4 could not become
a Stage 2)
Covered with a non-removable dressing/device and remains Unstageable until assessed as a Stage 2 at discharge
NO
b. Stage 3 at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present
Stage 1
Stage 2
Unstageable with documented Stage 1 and/or 2 at any home visit or Follow-up assessment(s)
YES
Stage 3 NO
Stage 4
NA (Stage 4 could not become a
Stage 3)
Unstageable until assessed as a Stage 3 at Discharge NO
c. Stage 4 at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present
Stage 1
Stage 2
Stage 3
Unstageable with documented Stage 1, 2, and/or 3 at any home visit or Follow-up assessment(s)
YES
Stage 4
Unstageable until assessed as a Stage 4 at Discharge
NO
d. Unstageable due to non-removable dressing at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present YES
Stage 1
Stage 2
Stage 3
Stage 4
Unstageable
NO
e. Unstageable due to slough and/or eschar at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present
Stage 1
Stage 2
YES
Stage 3
Stage 4
Unstageable
NO
f. Unstageable – suspected deep tissue injury at Discharge
If same pressure ulcer at most recent SOC/ROC was:
Not present
Stage 1
Stage 2
YES
Stage 3
Stage 4
Unstageable due to slough and/or eschar
NA (full thickness pressure ulcer
could not become a sDTI)
Unstageable – Suspected DTI or due to a non-removable dressing/device
NO
Foundation Management Services, Inc. 2017 [Page 14 of 35]
![Page 15: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/15.jpg)
OASIS-C2 (M2001)39
� (M2001) Drug Regimen Review�At SOC/ROC, document identification of potential clinically significant medication issues that in the clinician’s clinical judgment require physician notification by midnight of next calendar day (at the latest)
� In addition to “potential” issues, the item also includes the identification of an existing issue that in the care provider’s clinical judgment requires physician/physician-designee notification by midnight of the next calendar day
M2001 Guidance40
�(M2001) Drug Regimen Review, continued�Issues identified must reach a level of clinical significance that warrants notification of the physician/physician-designee for orders or recommendations (by midnight of the next calendar day)� Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medication issue
Foundation Management Services, Inc. 2017 [Page 15 of 35]
![Page 16: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/16.jpg)
OASIS-C2 (M2003)41
�At SOC/ROC, document whether the two-way communication to physician/physician-designee AND completion of the prescribed/recommended actions occurred by midnight of the next calendar day after the potential clinically significant medication issue was identified� When multiple potential clinically significant medication issues are identified at SOC/ROC, all must be communicated to the physician/physician-designee, with completion of all prescribed/recommended actions occurring by midnight of the next calendar day (for “Yes” response)
M2003 Guidance42
�(M2003) Medication Follow-up�If the physician/physician-designee recommends an action that will take longer than the allowed time to complete, “Yes” should be entered as long as by midnight of the next calendar day the agency has taken whatever actions are possible to comply with the recommended action� For example, physician orders agency to monitor the issue over the weekend and call if problem persists (or) instructs patient to address the concern with PCP on a visit scheduled in two days
�If the physician/physician-designee provides no new orders in response to timely communication, enter Response 1 – Yes
Foundation Management Services, Inc. 2017 [Page 16 of 35]
![Page 17: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/17.jpg)
OASIS-C2 (M2005)43
�At Transfer, Death at Home, & Discharge: Document whether physician/physician-designee was contacted AND prescribed/recommended actions were completed by midnight of the next calendar day for all significant issues identified at the time of or at any time since the SOC/ROC
� If a clinically significant medication issue was identified at the SOC or ROC visit, the issue (and related physician/physician-designee communication) would be reported at both the SOC/ROC (on M2003) and again at Transfer, Death at Home, or Discharge (on M2005)
Foundation Management Services, Inc. 2017 [Page 17 of 35]
![Page 18: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/18.jpg)
Renumbered – uniform “look-back”
Renumbered because of change to a uniform “look-back” period
45
In OASIS-C2, these items collected at Transfer & Discharge look back to “at the time of or at any time since the most recent SOC/ROC assessment”� In former OASIS versions, these items instructed a look-back
to “at the time of or at any time since the previous OASIS assessment” (the previous assessment would have included SOC, ROC, Recert, & Other Follow-up)
�This change in “look-back” requires an intentional change in assessment strategy for these items� (M1501) Symptoms in Heart Failure Patients� (M1511) Heart Failure Follow-up� (M2005) Medication Intervention� (M2016) Patient/Caregiver Education Intervention� (M2301) Emergent Care� (M2401) Intervention Synopsis
Significant Changes in Pressure Ulcer Item Guidance
Changes in pressure ulcer guidance47
�Terminology referring to “healed” versus “unhealed” pressure ulcers can refer to whether the ulcer is “closed” versus “open”�Recognize, however, that Stage 1 pressure ulcers
and suspected Deep Tissue Injury (sDTI), although closed (intact skin), would not be considered healed
�Unstageable pressure ulcers, whether covered with a non-removable dressing or eschar/slough, would not be considered healed
Foundation Management Services, Inc. 2017 [Page 18 of 35]
![Page 19: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/19.jpg)
Changes in pressure ulcer guidance48
�Stage 3 and 4 (full thickness) pressure ulcers heal through a process of:�Granulation (filling of the wound with connective/scar
tissue), �Contraction (wound margins contract and pull together), and �Re-epithelialization (covers with epithelial tissue from within
wound bed and/or from wound margins).�Once the Stage 3 or 4 pressure ulcer has fully
granulated and the wound surface is completely covered with new epithelial tissue, the wound is considered closed, and will continue to remodel and increase in tensile strength
�For the purposes of scoring, the (closed) wound is considered healed at this point, and should not be reported as an unhealed pressure ulcer
Changes in pressure ulcer guidance49
� A pressure ulcer treated with a skin graft (defined as transplantation of skin to another site) should not be reported as a pressure ulcer and until the graft edges completely heal, should be reported as a surgical wound on M1340
� Similarly, from (M1340) Surgical Wound guidance:� If a pressure ulcer is closed with a flap or a graft it is no longer
reported as a pressure ulcer� It should be reported as a surgical wound until healed� If the flap or graft fails, it should continue to be considered a
surgical wound until healedNOTE: The “success” of the flap or graft is not a factor – it is considered a surgical wound without consideration of the healing progress. The only way this area would return to pressure ulcer status is with new pressure injury in that area.
Changes in pressure ulcer guidance50
�(M1307) Oldest Stage 2 Pressure Ulcer�Enter Response 1 (was present at the most recent
SOC/ROC) only if the oldest Stage 2 pressure ulcer that is present at discharge was already present as a Stage 2 pressure ulcer when first assessed at the SOC/ROC
�Enter Response 2 (developed since the most recent SOC/ROC) if the oldest Stage 2 pressure ulcer that is present at discharge was NOT a Stage 2 pressure ulcer at the most recent SOC/ROC� If Response 2 is entered, specify the date the Stage 2 pressure
ulcer was first identified
Significant changes in guidance51
� (M1307) Oldest Stage 2 Pressure ulcer, continued�OASIS Q&A, Category 4b, Q98.2.1
� This Q&A in OASIS-C1/ICD-10: “If a patient had a Stage 1 pressure ulcer at SOC/ROC and it advanced to a Stage 2 by discharge, Response 1 (was present at most recent SOC/ROC) would be appropriate due to the fact that the ulcer, caused by pressure, was present at the most recent SOC/ROC assessment, even though it was a Stage 1 at the time.”
� Current Q&A edited for OASIS-C2: “If a patient had a Stage 1 pressure ulcer at SOC/ROC and it advanced to a Stage 2 by
discharge, Response 2 (developed since the most recent
SOC/ROC assessment) would be appropriate due to the fact
that the ulcer, caused by pressure, was not present as a Stage 2
at the most recent SOC/ROC assessment.”
Foundation Management Services, Inc. 2017 [Page 19 of 35]
![Page 20: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/20.jpg)
Foundation Management Services, Inc. 2017 [Page 20 of 35]
![Page 21: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/21.jpg)
Foundation Management Services, Inc. 2017 [Page 21 of 35]
![Page 22: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/22.jpg)
Miss Jones – (M1028) Active Diagnoses)
Foundation Management Services, Inc. 2017 [Page 22 of 35]
![Page 23: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/23.jpg)
Ms. Maxey – (M1060) Height & Weight
Foundation Management Services, Inc. 2017 [Page 23 of 35]
![Page 24: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/24.jpg)
Mr. Black – Start of Care (Pressure Ulcers)
Foundation Management Services, Inc. 2017 [Page 24 of 35]
![Page 25: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/25.jpg)
(Mr. Black – SOC, continued)
Mr. Black – Discharge (Pressure Ulcers)
Foundation Management Services, Inc. 2017 [Page 25 of 35]
![Page 26: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/26.jpg)
(Mr. Black – DC, continued)
Foundation Management Services, Inc. 2017 [Page 26 of 35]
![Page 27: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/27.jpg)
Mrs. Moreno – (M1850) Transferring, (GG0170C) Mobility, (M1860) Ambulation/Locomotion
Foundation Management Services, Inc. 2017 [Page 27 of 35]
![Page 28: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/28.jpg)
Foundation Management Services, Inc. 2017 [Page 28 of 35]
![Page 29: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/29.jpg)
Mr. Featherston – Start of Care (M2001 & M2003)
Mr. Featherston – Discharge (M2005)
Foundation Management Services, Inc. 2017 [Page 29 of 35]
![Page 30: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/30.jpg)
Answer Key
1. Miss Jones – (M1028) Active Diagnoses Response 1 – PVD/PAD = blank; Response 2 – DM = checked
2. Ms. Maxey – (M1060) Height & Weight a. Height = 65; b. Weight = dash value
3. Mr. Black – Start of Care (M1311) Current Number of Unhealed Pressure Ulcers at Each Stage:
A1 Stage 2 = 0; A2 omitted at SOC
B1 Stage 3 = 1; B2 omitted at SOC
C1 Stage 4 = 0; C2 omitted at SOC
D1 dressing/device = 0; D2 omitted at SOC
E1 slough/eschar = 0; E2 omitted at SOC
F1 suspected DTI = 1; F2 omitted at SOC
(M1322) Current Number of Stage 1 Pressure Ulcers = 1
Mr. Black – Discharge (M1311) Current Number of Unhealed Pressure Ulcers at Each Stage:
A1 Stage 2 = 1; A2 = 0
B1 Stage 3 = 1; B2 = 0
C1 Stage 4 = 1; C2 = 1
D1 dressing/device = 0; D2 skipped
E1 slough/eschar = 0; E2 skipped
F1 suspected DTI = 0; F2 skipped
(M1307) Oldest Stage 2 Pressure Ulcer = Response 2
(M1313) Worsening in Pressure Ulcer Status since SOC/ROC
a. Stage 1 = 1
b. Stage 3 = 1
c. Stage 4 = 0
d. Dressing = 0
e. Slough/eschar = 0
f. Suspected DTI = 0
4. Mrs. Moreno (M1850) Transferring = Response 2
(GG0170C) Mobility
1. SOC/ROC Performance = 05
2. Discharge Goal = 06
(M1860) Ambulation/Locomotion = Response 2
5. Mr. Featherston – Start of Care (M2001) Drug Regimen Review = Response 1
(M2003) Medication Follow-up = Response 1
Mr. Featherston – Discharge (M2005) Medication Intervention = Response 0
Foundation Management Services, Inc. 2017 [Page 30 of 35]
![Page 31: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/31.jpg)
Foundation Management Services, Inc. 2017 [Page 31 of 35]
![Page 32: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/32.jpg)
Foundation Management Services, Inc. 2017 [Page 32 of 35]
![Page 33: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/33.jpg)
OASISOASISOASISOASIS----C2 Cheat Sheet:C2 Cheat Sheet:C2 Cheat Sheet:C2 Cheat Sheet: Obstacles to Data AccuracyObstacles to Data AccuracyObstacles to Data AccuracyObstacles to Data Accuracy
© Foundation Management Services, Inc. 2017 All rights reserved. Unauthorized reproduction is strictly prohibited. (02/17)
UUUUNIFORMNIFORMNIFORMNIFORM “L“L“L“LOOKOOKOOKOOK----BBBBACKACKACKACK” T” T” T” TIMEIMEIMEIME FFFFRAMERAMERAMERAME
ALLALLALLALL items collected at Transfer, Death, or Discharge that require a items collected at Transfer, Death, or Discharge that require a items collected at Transfer, Death, or Discharge that require a items collected at Transfer, Death, or Discharge that require a
“look back” to a prior assessment now reference back to “at the “look back” to a prior assessment now reference back to “at the “look back” to a prior assessment now reference back to “at the “look back” to a prior assessment now reference back to “at the
time of or at any time since the most recent SOC/ROC” time of or at any time since the most recent SOC/ROC” time of or at any time since the most recent SOC/ROC” time of or at any time since the most recent SOC/ROC”
∗ (M1041/1046) Influenza Vaccine
∗ (M1051/1056) Pneumococcal Vaccine
∗ (M1307) Oldest Stage 2 Pressure Ulcer
∗ (M1311) Current Number of Unhealed Pressure Ulcer
∗ (M1313) Worsening in Pressure Ulcer Status
∗ (M1501) Symptoms in Heart Failure Patients————changed in C2changed in C2changed in C2changed in C2
∗ (M1511) Heart Failure Follow-up————changed in C2changed in C2changed in C2changed in C2
∗ (M2005) Medication Intervention
∗ (M2016) Patient/Caregiver Drug Education————changed in C2changed in C2changed in C2changed in C2
∗ (M2301) Emergent Care————changed in C2changed in C2changed in C2changed in C2
∗ (M2401) Intervention Synopsis————changed in C2changed in C2changed in C2changed in C2
Toll Free: 800.213.4732
Fax: 866.824.5119
www.askFMS.com
OASISOASISOASISOASIS----C2 C2 C2 C2 ANDANDANDAND THETHETHETHE “I“I“I“IMPROVINGMPROVINGMPROVINGMPROVING MMMMEDICAREEDICAREEDICAREEDICARE PPPPOSTOSTOSTOST----AAAACUTECUTECUTECUTE
CCCCAREAREAREARE TTTTRANSFORMATIONRANSFORMATIONRANSFORMATIONRANSFORMATION AAAACTCTCTCT OFOFOFOF 2014 (IMPACT)”2014 (IMPACT)”2014 (IMPACT)”2014 (IMPACT)” ♦ Requires post-acute providers (LTCHs, IRFs, SNFs, and HHAs) to
standardize patient assessment and quality data.
♦ IMPACT is a strong driving force for the OASIS-C2 version. ♦ January 2017, OASIS data collection for these quality measures
began in two of the five required IMPACT measure domains: ◊ For the Skin Integrity domain: “Percentage of Patients with
Pressure Ulcers that are New or Worsened” ◊ For the Medication Reconciliation domain: “Drug Regimen
Review Conducted with Follow-up for Identified Issues” ♦ Home Health will begin data collection in January 2019 for the
remaining three IMPACT quality measure domains—additional
revisions to the OASIS to accommodate this requirement are
expected. ◊ Functional Status & Cognitive Function domain ◊ Incidence of Major Falls domain ◊ Transfer of Health Information & Care Preferences domain
SSSSUMMARYUMMARYUMMARYUMMARY OFOFOFOF OASISOASISOASISOASIS----C2 AC2 AC2 AC2 ADDITIONSDDITIONSDDITIONSDDITIONS/C/C/C/CHANGESHANGESHANGESHANGES (areas at potential risk for data inaccuracies)(areas at potential risk for data inaccuracies)(areas at potential risk for data inaccuracies)(areas at potential risk for data inaccuracies)
♦ NEW NEW NEW NEW standardized items:
1. (M1028) Active Diagnoses
2. (M1060) Height and Weight
3. (GG0170C) Mobility—Lying to sitting on side of
bed
♦ Renumbered items due to modification to
standardize with other poststandardize with other poststandardize with other poststandardize with other post----acute data acute data acute data acute data collection:
1. (M1311) Current Number of Unhealed Pressure
Ulcer
2. (M1313) Worsening in Pressure Ulcer Status
3. (M2001) Drug Regimen Review
4. (M2003) Medication Follow-up
5. (M2005) Medication Intervention
♦ Renumbered items due to change to a uniform lookuniform lookuniform lookuniform look----
back periodback periodback periodback period:
1. (M1501) Symptoms in Heart Failure Patients
2. (M1511) Heart Failure Follow-up
3. (M2016) Pt/Cg Drug Education Intervention
4. (M2301) Emergent Care
5. (M2401) Intervention Synopsis
♦ Several changes in OASIS Guidance Manual
◊ Chapter 1: Conventions for Collecting OASIS (new “dash value” guidance)
◊ Chapter 3: Item-Specific Guidance (important changes in pressure ulcer guidance are detailed
in these tips; other chapter 3 changes are worthy of review)
‘R‘R‘R‘RISKISKISKISK----AAAADJUSTMENTDJUSTMENTDJUSTMENTDJUSTMENT” C” C” C” CONCEPTSONCEPTSONCEPTSONCEPTS FORFORFORFOR HHHHOMEOMEOMEOME CCCCAREAREAREARE
⇒ Risk-adjustment is based on statistical models
calculated using the national sample national sample national sample national sample of Home Health
patients in order to predict the individual patient’s predict the individual patient’s predict the individual patient’s predict the individual patient’s
outcomesoutcomesoutcomesoutcomes
⇒ Information that contributes risk-adjustment potential is
gathered at the SOC & ROC time points
⇒ For each home health quality measure, an OASIS item
that contributes risk-adjustment potential is statistically
meaningful as a predictor of whether a patient is “more predictor of whether a patient is “more predictor of whether a patient is “more predictor of whether a patient is “more
likely” or “less likely” to achieve the outcome likely” or “less likely” to achieve the outcome likely” or “less likely” to achieve the outcome likely” or “less likely” to achieve the outcome at
Discharge
Many OASIS responses collected at SOC/ROC serve no Many OASIS responses collected at SOC/ROC serve no Many OASIS responses collected at SOC/ROC serve no Many OASIS responses collected at SOC/ROC serve no
other purpose than to provide riskother purpose than to provide riskother purpose than to provide riskother purpose than to provide risk----adjustment potential adjustment potential adjustment potential adjustment potential
————accuracy in ALL items at ALL time points is ESSENTIALaccuracy in ALL items at ALL time points is ESSENTIALaccuracy in ALL items at ALL time points is ESSENTIALaccuracy in ALL items at ALL time points is ESSENTIAL
TTTTHEHEHEHE “D“D“D“DASHASHASHASH” R” R” R” RESPONSEESPONSEESPONSEESPONSE The dash ( The dash ( The dash ( The dash ( –––– ) value indicates that ) value indicates that ) value indicates that ) value indicates that no information is available, and/or no information is available, and/or no information is available, and/or no information is available, and/or an item could not be assessed an item could not be assessed an item could not be assessed an item could not be assessed (before the OASIS assessment was (before the OASIS assessment was (before the OASIS assessment was (before the OASIS assessment was completed). completed). completed). completed).
∗Items for which the dash is a valid response include ONLY:
(M1028) Active Diagnoses (M1060) Height & Weight (M1313) Worsening Pressure Ulcer (GG0170C) Mobility (M2001) Dreg Regimen Review (M2003) Medication Follow-up (M2005) Medication Intervention
CMS expects dash use to beCMS expects dash use to beCMS expects dash use to beCMS expects dash use to be aaaa rrrraaaarrrreeee ooooccccccccuuuurrrrrrrreeeennnncccceeee....
![Page 34: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/34.jpg)
(GG0170C) M(GG0170C) M(GG0170C) M(GG0170C) MOBILITYOBILITYOBILITYOBILITY————LLLLYINGYINGYINGYING TOTOTOTO SSSSITTINGITTINGITTINGITTING ONONONON EEEEDGEDGEDGEDGE OFOFOFOF BBBBEDEDEDED ♦ Contributes risk-adjustment for the “Percentage of Patients with
Pressure Ulcers that are New or Worsened” IMPACT measure.
♦ The patient’s use of assistive device(s) use of assistive device(s) use of assistive device(s) use of assistive device(s) to safely complete this
activity should NOT affect the scoring of this itemshould NOT affect the scoring of this itemshould NOT affect the scoring of this itemshould NOT affect the scoring of this item.
♦ 06-Independent (no human assistance, cuing, supervision)
♦ 05-Set-up or clean-up (needs assist before or after, not during)
♦ 04-Supervision or touching (verbal cues or steadying touch only)
♦ 03-Partial/moderate (caregiver provides less than half the effort)
♦ 02-Substantial/maximal (cg provides more than half the effort)
♦ 01-Dependent (caregiver provides all the effort <OR> assistance
of two or more caregivers is required to safely complete)
RRRREVISEDEVISEDEVISEDEVISED & R& R& R& RENUMBEREDENUMBEREDENUMBEREDENUMBERED IIIITEMSTEMSTEMSTEMS————DDDDRUGRUGRUGRUG RRRREGIMENEGIMENEGIMENEGIMEN & & & &
FFFFOLLOWOLLOWOLLOWOLLOW----UPUPUPUP FORFORFORFOR MMMMEDICATIONEDICATIONEDICATIONEDICATION IIIISSUESSSUESSSUESSSUES
♦ Items revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure cross----
setting standardization:setting standardization:setting standardization:setting standardization:
◊ (M2001) Drug Regimen Review: (M2001) Drug Regimen Review: (M2001) Drug Regimen Review: (M2001) Drug Regimen Review: at SOC/ROC, identification of potential and/or existing medication issues that in the clinician’s clinical judgment require physician notification by midnight of the next calendar day (at the latest).
◊ (M2003) Medication Follow(M2003) Medication Follow(M2003) Medication Follow(M2003) Medication Follow----up: up: up: up: at SOC/ROC, whether two-way communication to physician/designee AND completion of the prescribed actions occurred by midnight of the next calendar day after issue(s) identified.
◊ (M2005) Medication Intervention: (M2005) Medication Intervention: (M2005) Medication Intervention: (M2005) Medication Intervention: at Transfer/Death/Discharge, physician/designee was contacted AND prescribed actions were completed by midnight of next calendar day each time a potential and/or existing medication issue was identified at the time of or since the most recent SOC/ROC.
◊ If the prescribed action will take longer to complete than by midnight of next day, enter “Yes” for M2003 & M2005 if the agency has taken whatever actions are possible by midnight.
◊ Enter “Yes” for M2003 & M2005 if no new orders received.
(M1028) A(M1028) A(M1028) A(M1028) ACTIVECTIVECTIVECTIVE DDDDIAGNOSESIAGNOSESIAGNOSESIAGNOSES
♦ Contributes risk-adjustment for the “Percentage of Patients with
Pressure Ulcers that are New or Worsened” IMPACT measure.
♦ Identifies whether 2 specific diagnoses are present and active.
1. Peripheral Vascular Disease (PVD) or Peripheral Arterial
Disease (PAD); and/or
2. Diabetes Mellitus (DM)
♦ These diagnoses must be documented in medical record documented in medical record documented in medical record documented in medical record by the
physician (or NP, PA, CNS) and have a direct relationship direct relationship direct relationship direct relationship to the
patient’s current status, medical treatments, nurse monitoring,
or risk of death at the time of the assessment.
♦ PVD/PAD and DM diagnoses may be present and active
(reported in M1028) even if they are not sequenced into the top
six diagnoses (recorded in M1021/M1023).
RRRREVISEDEVISEDEVISEDEVISED & R& R& R& RENUMBEREDENUMBEREDENUMBEREDENUMBERED IIIITEMSTEMSTEMSTEMS————PPPPRESSURERESSURERESSURERESSURE UUUULCERLCERLCERLCER
♦ Items revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure crossItems revised & renumbered to facilitate IMPACT measure cross
----setting standardization:setting standardization:setting standardization:setting standardization:
◊ (M1311) Current Number of Unhealed Pressure Ulcers at (M1311) Current Number of Unhealed Pressure Ulcers at (M1311) Current Number of Unhealed Pressure Ulcers at (M1311) Current Number of Unhealed Pressure Ulcers at
Each StageEach StageEach StageEach Stage
∗ “Present at most recent SOC/ROC” for an ulcer that is
stageable at Follow-up or Discharge, but was unstageable
at SOC/ROC should be considered the stage at which it first stage at which it first stage at which it first stage at which it first
became numerically stageable became numerically stageable became numerically stageable became numerically stageable after SOC/ROC.
∗ When completing A2, B2, C2, D2, E2, F2 at Follow-up &
Discharge, the current ulcer must have been “present at “present at “present at “present at
most recent SOC/ROC” most recent SOC/ROC” most recent SOC/ROC” most recent SOC/ROC” at that same stage.at that same stage.at that same stage.at that same stage.
◊ (M1313) Worsening in Pressure Ulcer Status since SOC/ROC(M1313) Worsening in Pressure Ulcer Status since SOC/ROC(M1313) Worsening in Pressure Ulcer Status since SOC/ROC(M1313) Worsening in Pressure Ulcer Status since SOC/ROC
Refer to the “Reporting Algorithm for M1313” from chapter 3
guidance to ensure accuracy when completing this item at
Discharge
The OASIS-C2 dataset & OASIS Guidance Manual can be downloaded from
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/OASIS/index.html
(M1060) H(M1060) H(M1060) H(M1060) HEIGHTEIGHTEIGHTEIGHT ANDANDANDAND WWWWEIGHTEIGHTEIGHTEIGHT
♦ Contributes risk-adjustment for the “Percentage of Patients with
Pressure Ulcers that are New or Worsened” IMPACT measure.
♦ These measurements must be assessed by the home health
clinician—data by selfdata by selfdata by selfdata by self----report or from another provider setting is report or from another provider setting is report or from another provider setting is report or from another provider setting is
not acceptable.not acceptable.not acceptable.not acceptable. ♦ If patient cannot be weighed, enter dash & document rationale.
© Foundation Management Services, Inc. 2017 All rights reserved. Unauthorized reproduction is strictly prohibited. (02/17)
Compare/Contrast GG0170C with other OASIS ADL GuidanceCompare/Contrast GG0170C with other OASIS ADL GuidanceCompare/Contrast GG0170C with other OASIS ADL GuidanceCompare/Contrast GG0170C with other OASIS ADL Guidance
∗ OASIS Q&A 127.4 for M1800-M1900: The response related to “assistance of another person” includes those patients, actively participating in performing a task, but needing assistance of one or more person(s) to safely complete included tasks.
⇒The patient in this Q&A is NOT considered “dependent” NOT considered “dependent” NOT considered “dependent” NOT considered “dependent” when actively participating—despite the number of assisting persons required for safe completion of the activity. (Applies to M1800s)
⇒BUT, the guidance for GG0170C defines that assistance of 2+ persons renders the patient “dependent” renders the patient “dependent” renders the patient “dependent” renders the patient “dependent” when scoring this item.
∗ Use of device does not impact scoring of GGO170C, but assistive devices do factor into response selection for several other ADL items (for example in M1850 Transferring, the patient who requires BOTH assistance AND device moves to a more dependent response than if the patient requires EITHER assistance OR device, but not both). Additional Changes in Pressure Ulcer GuidanceAdditional Changes in Pressure Ulcer GuidanceAdditional Changes in Pressure Ulcer GuidanceAdditional Changes in Pressure Ulcer Guidance
⇒ If pressure is not the primary cause of the lesion, do not
report the wound as a pressure ulcer.
⇒ Stage 3 & 4 pressure ulcers that have fully granulated and
are completely covered with new epithelial tissue are
considered closed closed closed closed andandandand HEALEDHEALEDHEALEDHEALED—no longer reported as a
current ulcer.
⇒ PRESSURE ULCER BECOMES SURGICAL WOUND:
∗ A pressure ulcer treated with a skin graftskin graftskin graftskin graft is no longer
reported as a pressure ulcer and until the graft edges
completely heal is reported as a surgical wound until the
graft edges completely heal.
∗ A pressure ulcer that has been replaced by a muscle flap muscle flap muscle flap muscle flap
is reported as a surgical wound until the wound edges
completely heal.
∗ NOTE: If the flap or graft fails, the wound is still
considered a surgical wound. The only way this area
would return to pressure ulcer status is with new pressure
injury in that area.
⇒ When differences exist, OASIS pressure ulcer guidance and
instructions take precedence over NPUAP definitions.
![Page 35: [This handout is formatted for front-to-back printing] · [This handout is formatted for front-to-back printing] ... enhance the knowledge of the home health ... Diabetes mellitus](https://reader042.fdocuments.us/reader042/viewer/2022022523/5b38f9ed7f8b9a4b0a8c484c/html5/page/35.jpg)



![[This handout is formatted for front-to-back printing] · Skilled Nursing Facilities –SNF Minimum Data Set (MDS) ... If the assessment is completed and it is determined that the](https://static.fdocuments.us/doc/165x107/5b5229927f8b9ac4368d305c/this-handout-is-formatted-for-front-to-back-printing-skilled-nursing-facilities.jpg)