
THIRD VISIT COMPETENCIES – QUESTIONS...
76
Pre-Registration Optometrist Learning Resource Page 1 Third Visit Competencies – Model Answers 2010/11 28/4/2010 THIRD VISIT COMPETENCIES – QUESTIONS 2010/11 Competency group 1: Communication and Professional conduct 1.8 An ability to understand the patient’s expectations and aspirations and manage empathetically situations where these cannot be met. 1.9 The ability to communicate with patients who have poor, or non-verbal, communication skills, or those who are confused, reticent or who might mislead. 1.10 The ability to communicate bad news to patients in an empathetic and understandable way. 2.4 The ability to make a judgement regarding referral and an understanding of referral pathways. 3.6 The ability to advise visually impaired patients about their impairment, disability or handicap. What aspects of non-verbal communication might you make use of in your examination to put a patient at ease or identify anxiety? What are closed questions? What are open questions? How would you explain that you were referring a patient to their GP? How might the AOP’s advice following the National Institute for Health and Clinical Excellence (NICE) guidelines on the diagnosis and management of chronic open angle glaucoma and ocular hypertension have changed your management of suspect OHT patients? Following the Nice Guidance which patients does the joint guidance from the College and the Royal College of Ophthalmologists say you now don’t have to refer and can monitor in your practice? What changes to non-contact tonometry readings does the joint guidance from the College and the Royal College of Ophthalmologists now indicate?
Transcript of THIRD VISIT COMPETENCIES – QUESTIONS...

Pre-Registration Optometrist Learning Resource
Page 1 Third Visit Competencies – Model Answers 2010/11 28/4/2010
THIRD VISIT COMPETENCIES – QUESTIONS 2010/11 Competency group 1: Communication and Professional conduct 1.8 An ability to understand the patient’s expectations and aspirations and manage empathetically situations where these cannot be met. 1.9 The ability to communicate with patients who have poor, or non-verbal, communication skills, or those who are confused, reticent or who might mislead. 1.10 The ability to communicate bad news to patients in an empathetic and understandable way. 2.4 The ability to make a judgement regarding referral and an understanding of referral pathways. 3.6 The ability to advise visually impaired patients about their impairment, disability or handicap. What aspects of non-verbal communication might you make use of in your examination to put a patient at ease or identify anxiety? What are closed questions? What are open questions? How would you explain that you were referring a patient to their GP? How might the AOP’s advice following the National Institute for Health and Clinical Excellence (NICE) guidelines on the diagnosis and management of chronic open angle glaucoma and ocular hypertension have changed your management of suspect OHT patients? Following the Nice Guidance which patients does the joint guidance from the College and the Royal College of Ophthalmologists say you now don’t have to refer and can monitor in your practice? What changes to non-contact tonometry readings does the joint guidance from the College and the Royal College of Ophthalmologists now indicate?

Pre-Registration Optometrist Learning Resource
Page 2 Third Visit Competencies – Model Answers 2010/11 28/4/2010
How would you manage this patient if you saw them in your practice? AGE AND GENDER Female Aged 31 years ETHNIC BACKGROUND Caucasian OCCUPATION AND HOBBIES Secondary school teacher (PE) reading, theatre, needlepoint PRESENTING SYMPTOMS AND HISTORY Aware of flashing lights and spots in front of eyes over the last month. Present distance spectacles worn constantly, 2 years old. DV & NV OK. No personal history of eye disease, Mother high blood pressure. Soft contact lens wearer. Dailies, CL AC 3/12 No problems GENERAL HEALTH AND MEDICATION Good PRESENT Rx, CENTRATION AND ACUITIES CR39 sv distance 2 years old Monoc cds RE: 30 LE: 30 RE: -10.00/+0.50 x 180 LE: -9.50 Distance RE: 6/5 LE: 6/5 Near RE: N4 LE: N4 PD/NCD 60/56 at 25 cms VISION RE: 1/60 LE: 1/60 PINHOLE VISION RE: 6/5 LE: 6/5 REFRACTION RE: -10.00/+0.50 x 180 LE: -9.50 VA Distance RE: 6/5 LE: 6/5
Near RE: N4 LE: N4
ACCOMMODATION RE: 10.00 LE: 10.00 Binoc: 15.00 BINOCULAR STATUS With Rx Distance Maddox Rod 2Δ
Near Maddox Wing 2 exophoria
Δ
Fixation Disparity mallet Unit: Distance no slip : Near no slip exophoria
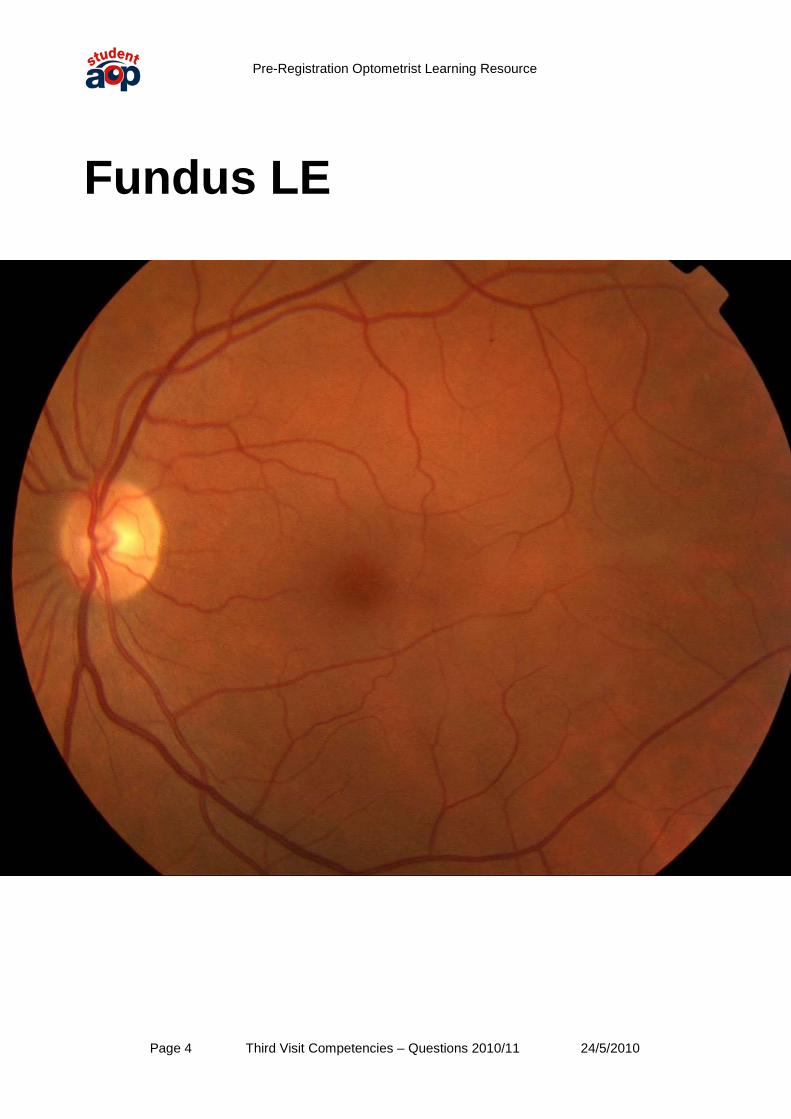
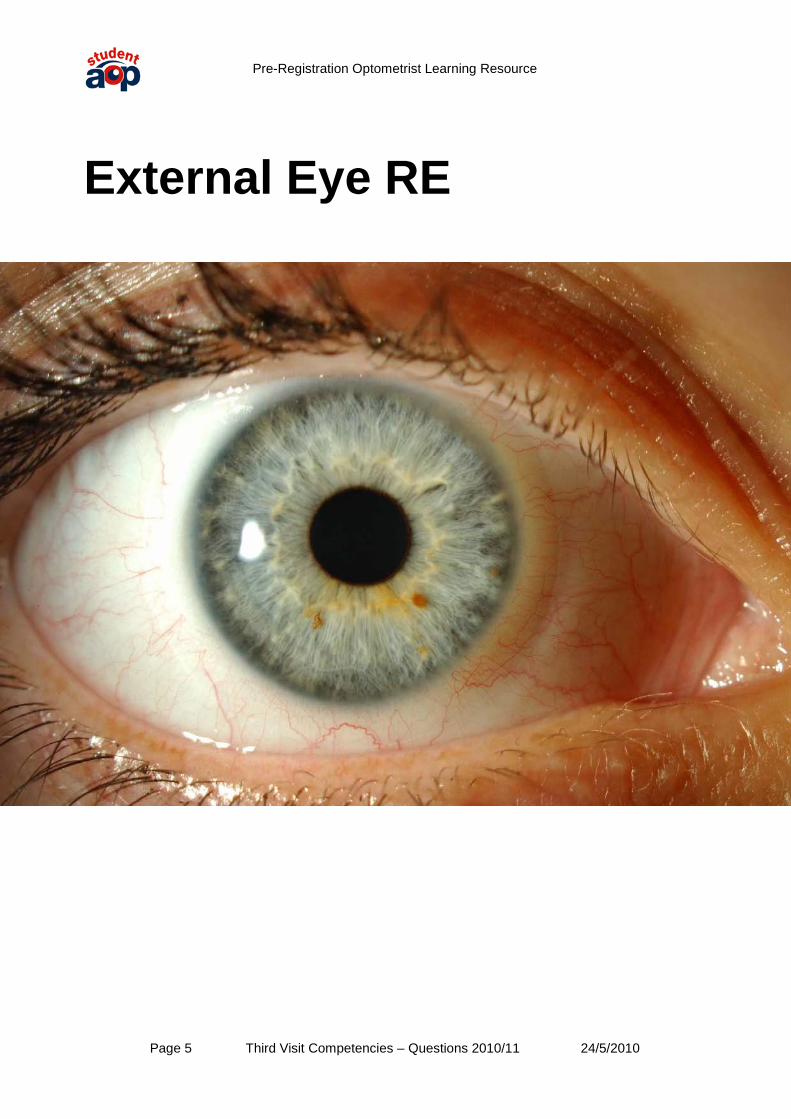
MOTILITY full, no diplopia CONVERGENCE NPC = 10cms PUPIL REACTIONS direct, consensual and near reflexes present FUNDUS EXAMINATION see attached FIELDS see attached IOP RE: 14 mmHg LE: 15 mmHg NCT 11.30am EXTERNAL EYE EXAMINATION see attached KERATOMETRY RE: 7.30 @ 180 7.35 @ 90 LE: 7.40 @ 180 7.40 @ 90 COLOUR VISION see attached

Pre-Registration Optometrist Learning Resource
Page 3 Third Visit Competencies – Questions 2010/11 24/5/2010
Fundus RE
Pre-Registration Optometrist Learning Resource
Page 4 Third Visit Competencies – Questions 2010/11 24/5/2010
Fundus LE
Pre-Registration Optometrist Learning Resource
Page 5 Third Visit Competencies – Questions 2010/11 24/5/2010
External Eye RE

Pre-Registration Optometrist Learning Resource
Page 6 Third Visit Competencies – Questions 2010/11 24/5/2010
External Eye LE

Pre-Registration Optometrist Learning Resource
Page 7 Third Visit Competencies – Questions 2010/11 24/5/2010
Field Plot RE

Pre-Registration Optometrist Learning Resource
Page 8 Third Visit Competencies – Questions 2010/11 24/5/2010
Field Plot LE

Pre-Registration Optometrist Learning Resource
Page 9 Third Visit Competencies – Questions 2010/11 24/5/2010
Colour Vision RE Number of plate
Score Normal Person with Red-Green Deficiencies
Person with Total colour blindness and weakness
1 12 12 12 12 2 8 8 3 X 3 6 6 5 X 4 27 29 70 X 5 57 57 35 X 6 5 5 2 X 7 3 3 5 X 8 15 15 17 X 9 71 74 21 X 10 2 2 X X 11 6 6 X X 12 97 97 X X 13 45 45 X X 14 5 5 X X 15 7 7 X X 16 16 16 X X 17 73 73 X X 18 X X 5 X 19 X X 2 X 20 X X 45 X 21 X X 73 X Protan Deutan
Strong Mild Strong Mild 22 26 6 (2)6 2 2(6) 23 42 2 (4)2 4 4(2) 24 35 5 (3)5 3 3(5) 25 96 6 (9)6 9 9(6)

Pre-Registration Optometrist Learning Resource
Page 10 Third Visit Competencies – Questions 2010/11 24/5/2010
Colour Vision LE Number of plate
Score Normal Person with Red-Green Deficiencies
Person with Total colour blindness and weakness
1 12 12 12 12 2 8 8 3 X 3 6 6 5 X 4 29 29 70 X 5 57 57 35 X 6 5 5 2 X 7 3 3 5 X 8 15 15 17 X 9 71 74 21 X 10 2 2 X X 11 6 6 X X 12 97 97 X X 13 45 45 X X 14 5 5 X X 15 7 7 X X 16 16 16 X X 17 73 73 X X 18 X X 5 X 19 X X 2 X 20 X X 45 X 21 X X 73 X Protan Deutan
Strong Mild Strong Mild 22 26 6 (2)6 2 2(6) 23 42 2 (4)2 4 4(2) 24 35 5 (3)5 3 3(5) 25 96 6 (9)6 9 9(6)

Pre-Registration Optometrist Learning Resource
Page 11 Third Visit Competencies – Questions 2010/11 24/5/2010
Indicate the conditions you feel would warrant referral -
Very urgently – Emergency same day
Urgent – without undue delay (1-14 days)
Routine – In turn What are the preferred new terms for Blind and partially sighted, from 2004? Under what circumstances (NHS terms of service) in the General Ophthalmic Service should a patient's Medical Practitioner be informed? What is the difference between "refer to" and "inform" a Medical Practitioner? Can an Optometrist supply spectacles if the patient has been referred to their Medical practitioner? What would you do if the person refuses to consult a Medical practitioner, following referral? Can an Optometrist use drugs to treat an eye injury? If when you are dispensing, as opposed to having undertaken the eye examination, you note that the patient has been referred to his GMP. Can you dispense spectacles to them? Does a Dispensing Optician have a duty to refer to a Medical Practitioner? What does a patient need to do to be registered as Blind or Partially Sighted? Who can be registered Blind (Severely Sight Impaired)? Who can be registered partially sighted (Sight Impaired)? What are the principal causes of visual handicap in children? What are the principal causes of visual handicap in young adults and the working population?
Pre-Registration Optometrist Learning Resource
Page 12 Third Visit Competencies – Questions 2010/11 24/5/2010
What are the principal causes of visual handicap in the elderly population? What are CVI, RVI and LVL? Who receives copies of the CVI forms? What additional information is provided to the patient with the CVI, RVI and LVL? What services might be available for a patient with visual impairment? How might these vary for a patient who is not registered compared to someone registered Partially sighted or Blind? These are some of the commonest problems talked about by clients/patients with a visual impairment, think of as many solutions to each problem, not necessarily optical. 1. Problems crossing the road 2. Problems watching TV 3. Walking past a friend without recognising them 4. Need a telephone but can not afford one 5. Problems reading the telephone directory 6. Problems dialling the correct number 7. Problems with dial settings on the gas/electric cooker, fire/central heating controls, tumble dryers, washing machines and television controls 8. Problems with tasks needing both hands free e.g. cutting toe nails, sewing, writing etc. 9. Problems finding a radio station 10. Problems with time on their hands 11. Poor mobility and life skills 12. Problems that you do not know the answer to Make an extensive list of non-optical aids to partial sight.
Pre-Registration Optometrist Learning Resource
Page 13 Third Visit Competencies – Questions 2010/11 24/5/2010
Competency group 2: Assessment of Visual function/Binocular Vision anomalies 3.3 The ability to use appropriate ocular diagnostic drugs to aid refraction. 3.4 The ability to assess children’s visual function using appropriate techniques. 3.5 The ability to assess patients with impaired visual function. 3.8 An understanding of the special examination needs of patients with learning and other disabilities. 3.9 An understanding of the special examination needs of patients with severe visual field defects 8.3 The ability to investigate and manage adult patients presenting with heterophoria. 8.5 The ability to manage children at risk of developing an anomaly of binocular vision. 8.6 The ability to manage children presenting with an anomaly of binocular vision. 8.7 The ability to manage a patient presenting with an incommitant deviation. How might you expand your routine to assess a visually impaired patient? What is nystagmus, what are the common types of nystagmus? What is a null position? How would you alter your routine for a patient with nystagmus? How would you expect your assessment of a patient’s vision to be affected by the following field defects? Glaucomatous loss? Age related macular degeneration? Homonymous Hemianopia?

Pre-Registration Optometrist Learning Resource
Page 14 Third Visit Competencies – Questions 2010/11 24/5/2010
What is your diagnosis and management plan for this patient?
Date of Exam 06.2.05 Optometrist Patient Alex Brown Age 3
CURRENT RX CONDITION None
VISION
SPH CYL AXIS PRISM BASE VA
CONTACT LENS USER Y/N TYPE NA
R 3/24
REASON FOR VISIT Mum feels RE turns in occ.
L 3/6
DATE OF LAST EXAM/LAST RX 1st
ADD
NEAR VA
DISTANCE/NEAR/BIF/VARIF
SYMPTOMS Mum feels RE turns in intermittently since birth, getting worse GH good BH FTND FH squints on M. side of family
OMB
DIST H R straight breaks to a R ESOT 45Δ
NEAR H
when concentrates
on small toy
R ESOT 45NPC
Δ 6cm
V NMD
V NMD
EXTERNAL R L Healthy LIDS/LASHES Healthy Clear and quiet CORNEA Clear and quiet Clear VH 4 A/C Clear VH 4 Clear LENS Clear
FIELDS R L
STEREO COLOUR
AMSLER
INTERNAL Clear MEDIA Clear Flat CD 0.2 DISCS:CUP Flat CD 0.2 healthy MARGIN healthy
Pink COLOUR pink A/V3:4 VESSELS A/V3:4 Reflex MAC Reflex Pink, flat PERIP Pink, flat
PD DIST 64mm
NEAR 58mm
ACCOMM R L BIN MOTILITY Full
PUPILS D 4 C 4 N 4 NO RAPD
RETINOSCOPY R +7.00 Cycloplegic L +7.00 R+L Cyclopentolate 1% 1) 9.45am
SUBJ SPH CYL AXIS VA PRISM BASE
BIN ADD BIN VA
ADD NEAR VA
R
L
SPH
CYL AXIS PRISM
BASE OMB DIST H NEAR H NPC
RX R L
V V
ADVICE RE PRESCRIPTION
ADVICE TO PATIENT NEAR ADD INTER ADD
BACK VERTEX WD 12mm

Pre-Registration Optometrist Learning Resource
Page 15 Third Visit Competencies – Questions 2010/11 24/5/2010
What would be your management of this patient and why?
Date of Exam 06.2.05 Optometrist Patient Alex Brown Age 27
CURRENT RX CONDITION Good, 2 years old
VISION
SPH CYL AXIS PRISM BASE VA
CONTACT LENS USER Y/N TYPE NA
R 6/9
-1.00 +0.50 180 6/6
REASON FOR VISIT Wants new glasses
L 6/6
-0.75 6/6
DATE OF LAST EXAM/LAST RX 2 years
ADD
NEAR VA N4.5
DISTANCE/NEAR/BIF/VARIF Distance
SYMPTOMS c/o occasional double vision when looking down ever since RTA six months ago.
OMB
DIST H Ortho
NEAR H Ortho
NPC 6cm
V L/R
V L/R
IOP R L TIME MEAN OF READINGS
EXTERNAL R L Healthy LIDS/LASHES Healthy Clear and quiet CORNEA Clear and quiet Clear VH 4 A/C Clear VH 4 Clear LENS Clear
FIELDS R L
STEREO COLOUR
AMSLER
INTERNAL Clear MEDIA Clear Flat CD 0.2 DISCS:CUP Flat CD 0.2 healthy MARGIN healthy
Pink COLOUR pink A/V3:4 VESSELS A/V3:4 Reflex MAC Reflex Pink, flat PERIP Pink, flat
PD DIST 64mm
NEAR 58mm
ACCOMM R L BIN MOTILITY left limitation of depression in adduction PUPILS D 4 C 4 N 4 NO RAPD
RETINOSCOPY R -1.00/+0.50 x 180 L -0.75
SUBJ SPH CYL AXIS VA PRISM BASE
BIN ADD
BIN VA ADD NEAR VA
R
-1.00 +0.50 180 6/6 6/6
N4.5
L
-0.75 6/6 N4.5
SPH
CYL AXIS PRISM
BASE OMB DIST H NEAR H NPC
RX R L
-1.00
+0.50 180 V V
-0.75
+0.25
180
ADVICE RE PRESCRIPTION
ADVICE TO PATIENT NEAR ADD INTER ADD
BACK VERTEX WD 12mm
Pre-Registration Optometrist Learning Resource
Page 16 Third Visit Competencies – Questions 2010/11 24/5/2010
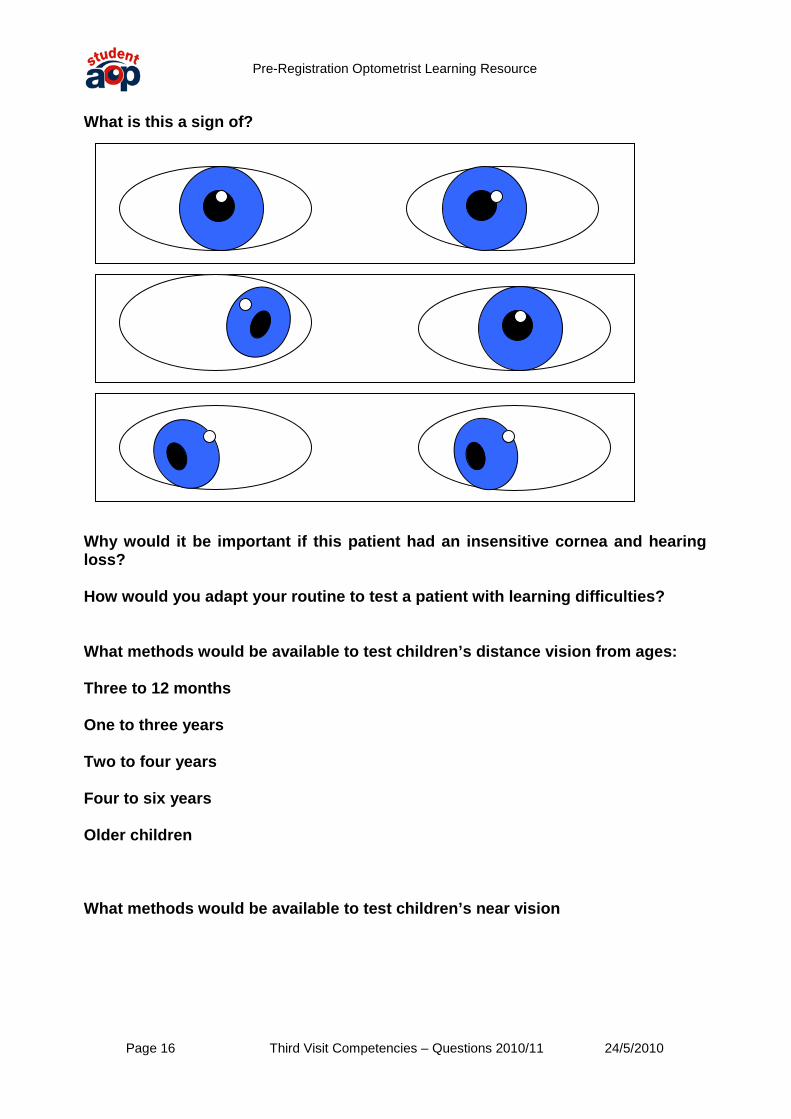
What is this a sign of?
Why would it be important if this patient had an insensitive cornea and hearing loss? How would you adapt your routine to test a patient with learning difficulties? What methods would be available to test children’s distance vision from ages: Three to 12 months One to three years Two to four years Four to six years Older children What methods would be available to test children’s near vision
Pre-Registration Optometrist Learning Resource
Page 17 Third Visit Competencies – Questions 2010/11 24/5/2010
What would be a normal refraction and expected corrected acuity for most children at age: One year Two years Three years Four years What spectacle correction would you prescribe for a patient under six years old? List the circumstances where a refractive correction might help in the management of a binocular vision problem in childhood?
Pre-Registration Optometrist Learning Resource
Page 18 Third Visit Competencies – Questions 2010/11 24/5/2010
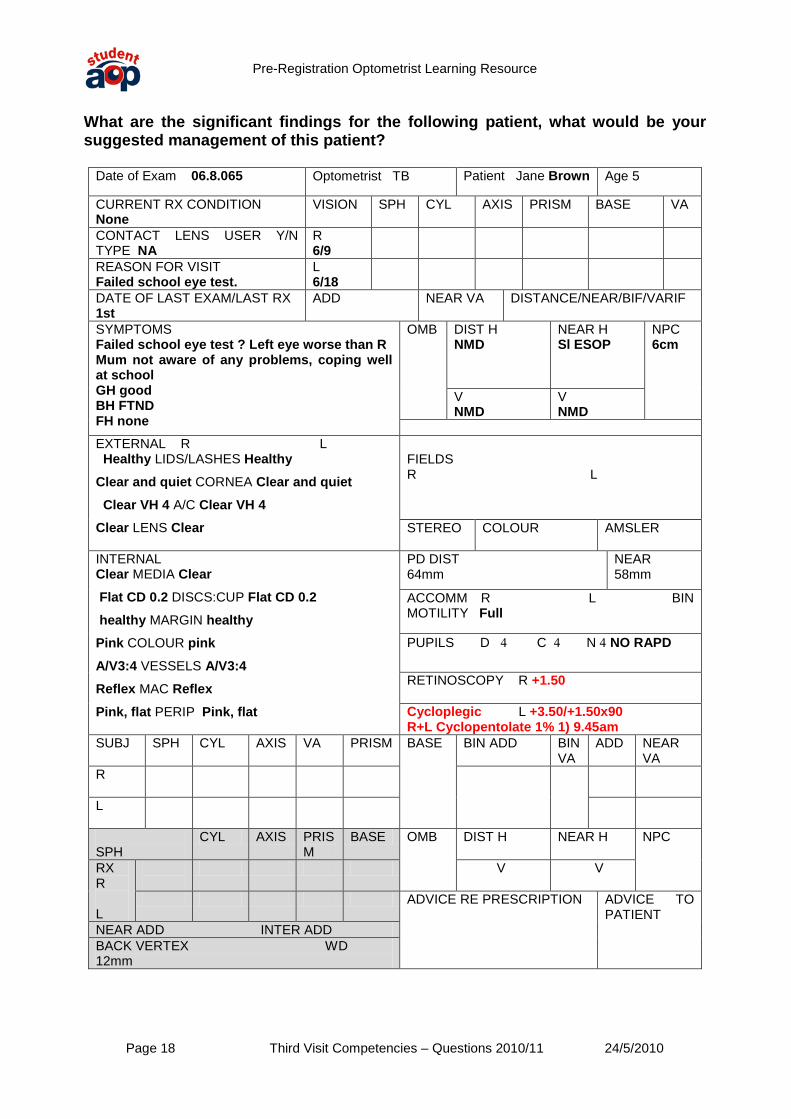
What are the significant findings for the following patient, what would be your suggested management of this patient?
Date of Exam 06.8.065 Optometrist TB Patient Jane Brown Age 5
CURRENT RX CONDITION None
VISION
SPH CYL AXIS PRISM BASE VA
CONTACT LENS USER Y/N TYPE NA
R 6/9
REASON FOR VISIT Failed school eye test.
L 6/18
DATE OF LAST EXAM/LAST RX 1st
ADD
NEAR VA
DISTANCE/NEAR/BIF/VARIF
SYMPTOMS Failed school eye test ? Left eye worse than R Mum not aware of any problems, coping well at school GH good BH FTND FH none
OMB
DIST H NMD
NEAR H Sl ESOP
NPC 6cm
V NMD
V NMD
EXTERNAL R L Healthy LIDS/LASHES Healthy Clear and quiet CORNEA Clear and quiet Clear VH 4 A/C Clear VH 4 Clear LENS Clear
FIELDS R L
STEREO COLOUR
AMSLER
INTERNAL Clear MEDIA Clear Flat CD 0.2 DISCS:CUP Flat CD 0.2 healthy MARGIN healthy
Pink COLOUR pink A/V3:4 VESSELS A/V3:4 Reflex MAC Reflex Pink, flat PERIP Pink, flat
PD DIST 64mm
NEAR 58mm
ACCOMM R L BIN MOTILITY Full
PUPILS D 4 C 4 N 4 NO RAPD
RETINOSCOPY R +1.50 Cycloplegic L +3.50/+1.50x90 R+L Cyclopentolate 1% 1) 9.45am
SUBJ SPH CYL AXIS VA PRISM BASE
BIN ADD BIN VA
ADD NEAR VA
R
L
SPH
CYL AXIS PRISM
BASE OMB DIST H NEAR H NPC
RX R L
V V
ADVICE RE PRESCRIPTION
ADVICE TO PATIENT NEAR ADD INTER ADD
BACK VERTEX WD 12mm

Pre-Registration Optometrist Learning Resource
Page 19 Third Visit Competencies – Questions 2010/11 24/5/2010
What does a cycloplegic do? What are the advantages of a cycloplegic examination? How would you be sure that the cyclopentolate had caused adequate cycloplegia? What cycloplegics are available to the Optometrist, in what form, what onset and duration and what are their pharmacological principles? What are the contraindications for using a cycloplegic drug? Are there any disadvantages to the use and effects of cycloplegia? Cycloplegic examination can be indicated in patients with asthenopia. How would a patient usually describe symptoms of asthenopia? What refractive eye conditions may result in these symptoms? For each condition that you can think of, explain why - What would be the cycloplegic drug of choice in? a. An four year old Caucasian child? b. An adult? c. A pre-school child with dark irides? Which groups of children should always be considered for a cycloplegic refraction? What changes to legislation have affected the supply of Atropine? Could a child become overdosed on the normal amount of Atropine dispensed (one tube of ointment)? How would you recognise and deal with Atropine poisoning? Draw a diagrammatic representation of the visual pathways, Illustrate the field defects caused by lesions at A: The right optic nerve B: The right optic tract immediately post chiasmal C: The right optic tract just before the LGB D: The right optic radiations E: The right visual cortex F: The inferior chiasm G: The temporal chiasm A
Pre-Registration Optometrist Learning Resource
Page 20 Third Visit Competencies – Questions 2010/11 24/5/2010
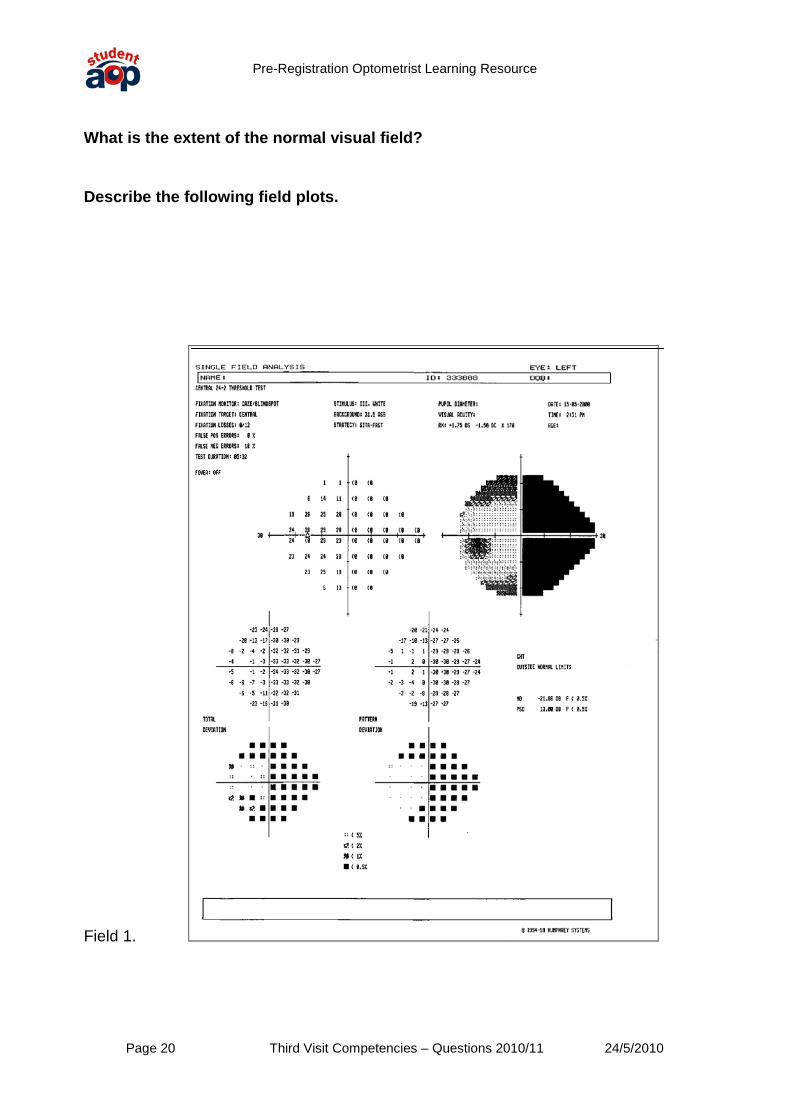
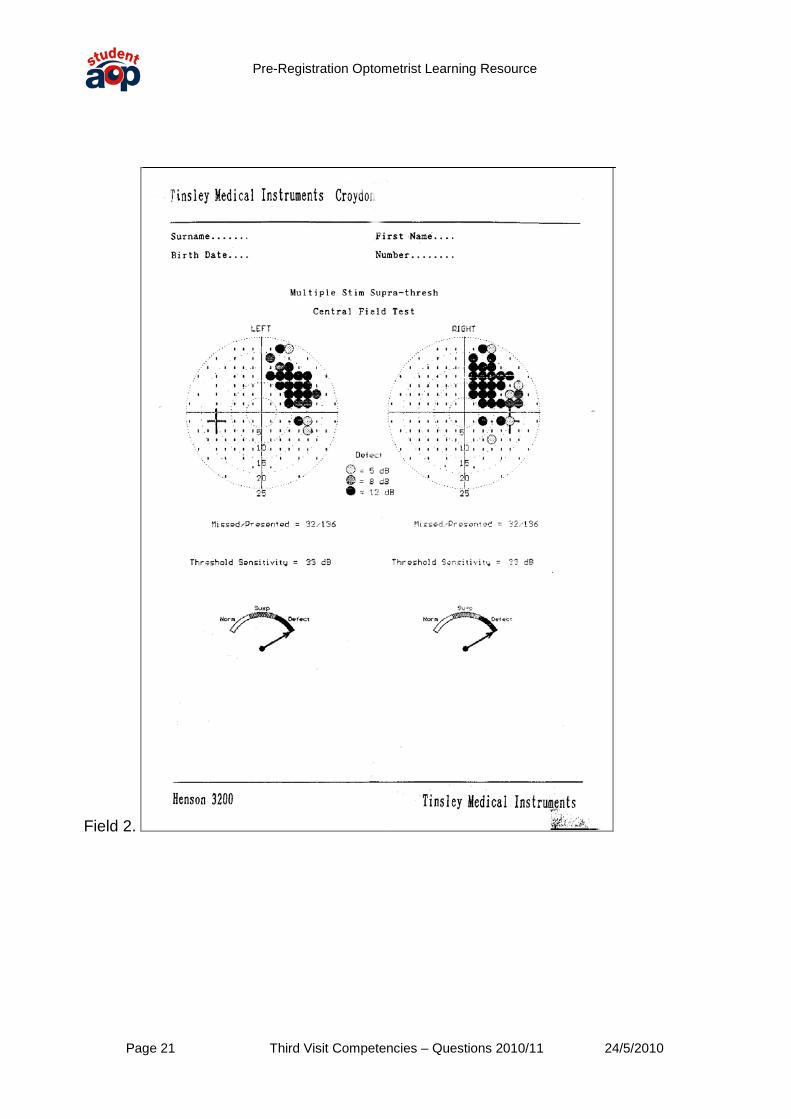
What is the extent of the normal visual field? Describe the following field plots.
Field 1.
Pre-Registration Optometrist Learning Resource
Page 21 Third Visit Competencies – Questions 2010/11 24/5/2010
Field 2.
Pre-Registration Optometrist Learning Resource
Page 22 Third Visit Competencies – Questions 2010/11 24/5/2010
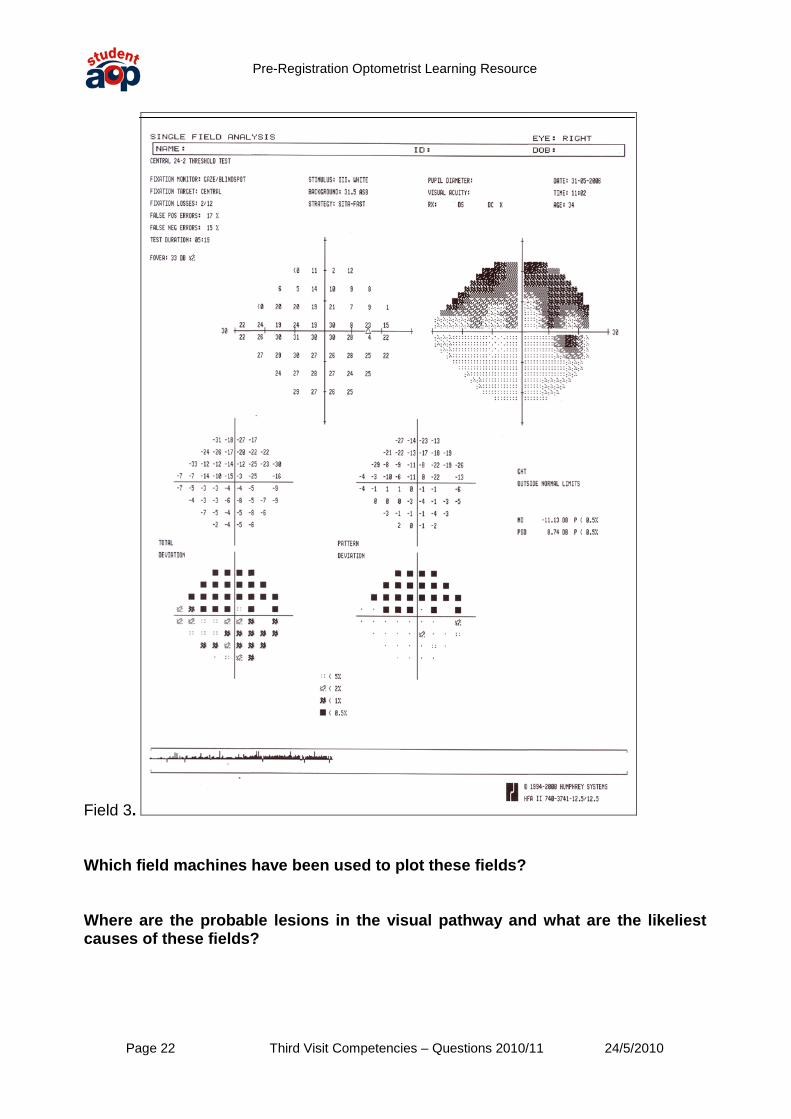
Field 3. Which field machines have been used to plot these fields? Where are the probable lesions in the visual pathway and what are the likeliest causes of these fields?

Pre-Registration Optometrist Learning Resource
Page 23 Third Visit Competencies – Questions 2010/11 24/5/2010
Competency group 3: Methods of Ocular examination 5.10 The ability to use a contact tonometer to measure intraocular pressure and analyse and interpret the results. 5.12 The ability to use a slit lamp to detect anterior chamber signs of ocular inflammation. 5.14 Demonstrate an understanding of techniques for assessment of vision in infants. What is the principle behind the action of applanation tonometry? Why is the diameter of the applanation head important? What are some of the different types of tonometers available?
Why do we record the time of the IOP results?
What normal variations in IOP occur? What should you consider doing when using a contact applanation tonometer where there is corneal astigmatism above 3.00D? What are other possible sources of error when using a contact applanation tonometer? Is asymmetry in IOP results of any interest? What are the appearances of the flourescein picture when using a contact applanation tonometer with too little pressure, too much pressure and at the end point? Why is adapting the image of the NCT target to the patient's distance Rx important? What result from tonometry would you refer? What are the normal ranges of IOP? How do you check calibration on an AO NCT, a Goldmann and a Perkins Tonometer?

Pre-Registration Optometrist Learning Resource
Page 24 Third Visit Competencies – Questions 2010/11 24/5/2010
If out of calibration, can you proceed? How do the Pulsair and the AO NCT differ in the way they take their readings? Why is it necessary to take three readings with an NCT, but only one with a contact applanation technique? How would you set up to use a Volk lens? When would you use a Volk lens? How would you set up to use a Binocular Indirect ophthalmoscope? What are the advantages and disadvantages of the Binocular Indirect ophthalmoscope? What technique would you use to detect anterior chamber signs of ocular inflammation with your Slit lamp? How would you grade Cells and Flare? What tests are available for testing children’s distance vision? How might you adapt your routine to test a child? What are these children’s vision tests and how do they work?

Pre-Registration Optometrist Learning Resource
Page 25 Third Visit Competencies – Questions 2010/11 24/5/2010
What tests are available for testing children’s near vision?

Pre-Registration Optometrist Learning Resource
Page 26 Third Visit Competencies – Questions 2010/11 24/5/2010
Competency group 4: Dispensing and Optical appliances 4.3 The ability to advise on the use of, and to dispense simple low vision aids including: hand and stand magnifiers, typoscopes and hand held telescopes. 4.8 An understanding of the application of complex low vision aids e.g. spectacle-mounted telescopes, CCTV. 4.9 The ability to manage non-tolerance cases. What are the main advantages and disadvantages of hand magnifiers, stand magnifiers, high reading Adds, telescopes and closed circuit television. What are the differences between a Gallilean and an Astronomical telescope? How can you modify a distance telescope for near or intermediate use? Draw ray diagrams illustrating the optical principles of the following: i) A simple hand magnifier ii) A Gallilean telescope iii) An Astronomical telescope What do the markings on this telescope mean?
What kind of telescope is it likely to be?

Pre-Registration Optometrist Learning Resource
Page 27 Third Visit Competencies – Questions 2010/11 24/5/2010
What is this LVA?
What is this LVA? What is it used for?
Pre-Registration Optometrist Learning Resource
Page 28 Third Visit Competencies – Questions 2010/11 24/5/2010
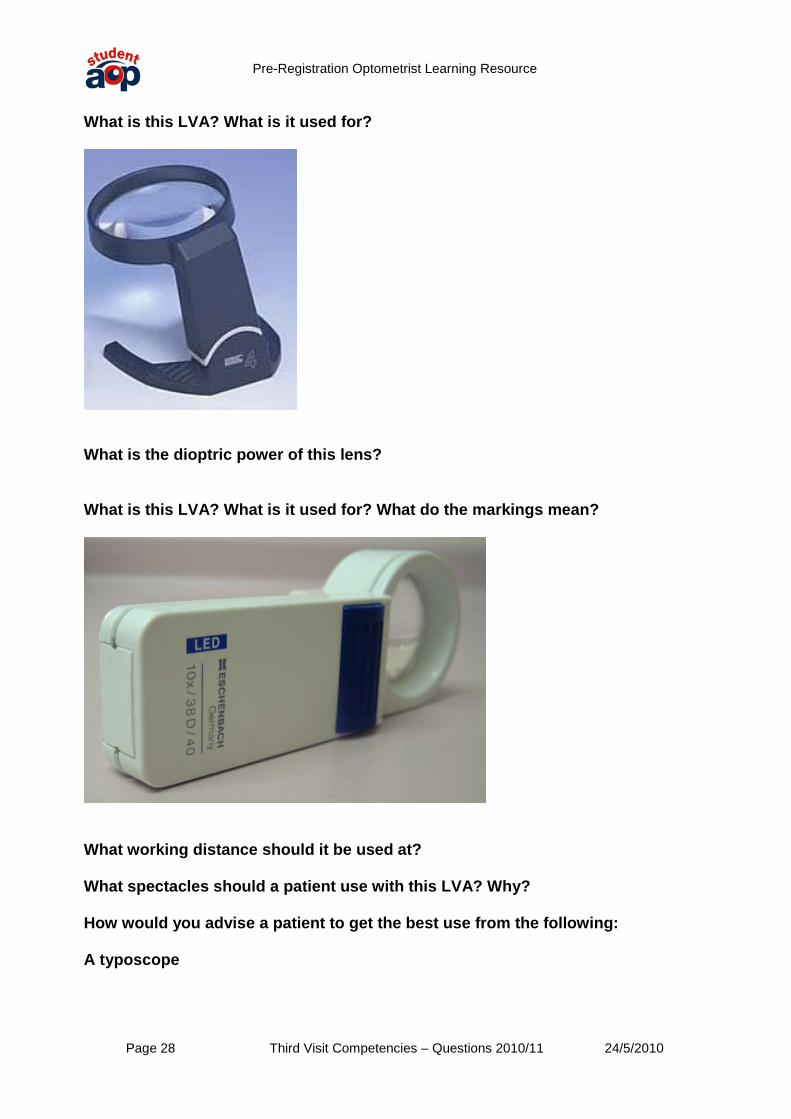
What is this LVA? What is it used for?
What is the dioptric power of this lens? What is this LVA? What is it used for? What do the markings mean?
What working distance should it be used at? What spectacles should a patient use with this LVA? Why? How would you advise a patient to get the best use from the following: A typoscope
Pre-Registration Optometrist Learning Resource
Page 29 Third Visit Competencies – Questions 2010/11 24/5/2010
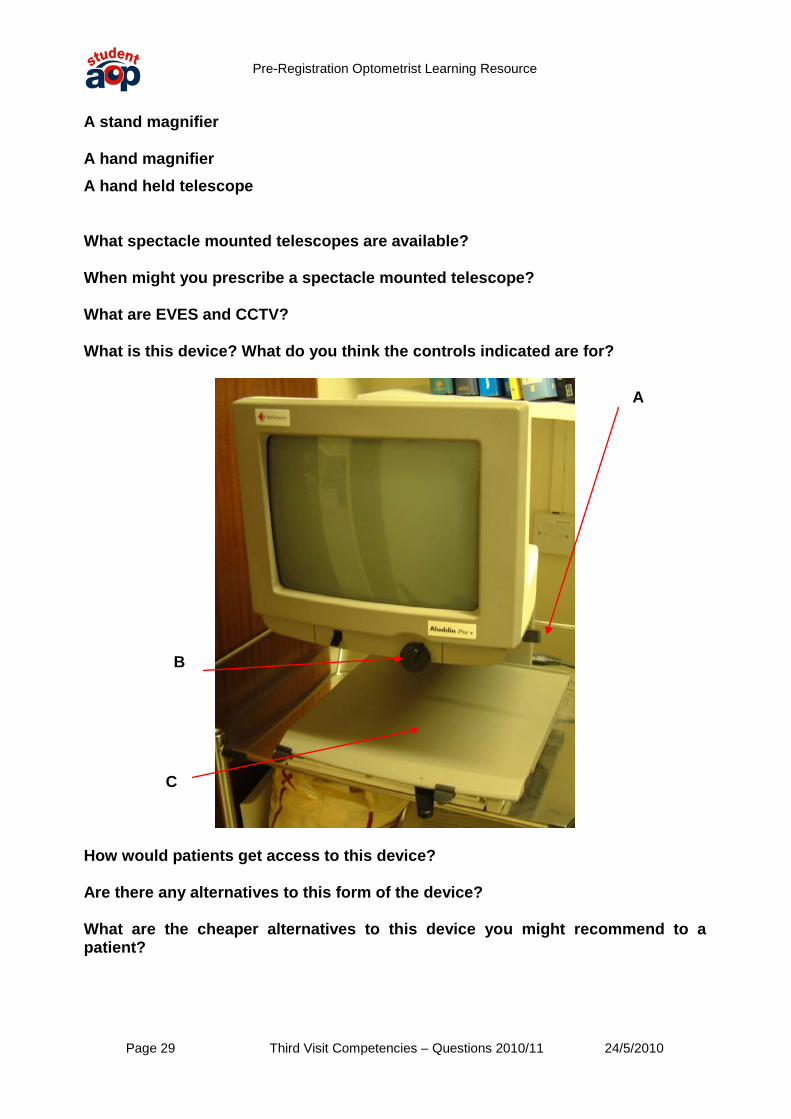
A stand magnifier A hand magnifier A hand held telescope What spectacle mounted telescopes are available? When might you prescribe a spectacle mounted telescope? What are EVES and CCTV? What is this device? What do you think the controls indicated are for?
How would patients get access to this device? Are there any alternatives to this form of the device? What are the cheaper alternatives to this device you might recommend to a patient?
A
B
C
Pre-Registration Optometrist Learning Resource
Page 30 Third Visit Competencies – Questions 2010/11 24/5/2010
Competency group 5: Contact lenses 7.2 The ability to fit soft lenses 7.5 The ability to manage the aftercare of patients wearing rigid gas permeable contact lens. 7.6 The ability to fit rigid gas permeable contact lenses. 7.8 An understanding of the techniques used in fitting contact lenses and to advise patients requiring complex visual correction. How would you expand your “history and symptoms” for a patient who wanted to be fitted for contact lenses? What should you discuss with the patient before fitting? What factors would influence your choice of lens? What factors would influence the patient’s choice? How does this tally with what is available? What are your “rules of thumb for choosing the parameters of a soft trial lens? What are your “rules of thumb for choosing the parameters of a rigid gas permeable trial lens? Give the clinical equivalents to 7.70 / 9.30 / -3.00 if: i) TD increased by 0.5mm. ii) BOZR flattened by 0.10mm Write out a full specification for a rigid corneal contact lens. Describe your initial slit lamp assessment of the patient prior to trial lens insertion. What ocular measurements do you require for all contact lenses and which only for soft or corneal lens fitting? Why? Draw a diagram indicating these additional measurements on the eye.
PAS

Pre-Registration Optometrist Learning Resource
Page 31 Third Visit Competencies – Questions 2010/11 24/5/2010
What might be the problems fitting this eye?
What instructions would you give a patient on how to insert and remove their rigid gas permeable contact lenses?
How would you describe the fluorescein fit of these RGP contact lenses?
Image 1. Image 2.

Pre-Registration Optometrist Learning Resource
Page 32 Third Visit Competencies – Questions 2010/11 24/5/2010
Image 3. Image 4. Image 5.
Image 6.
Image7. Image 8. Would you be happy with these fits?

Pre-Registration Optometrist Learning Resource
Page 33 Third Visit Competencies – Questions 2010/11 24/5/2010
What problems have occurred with these patient’s contact lenses? A.
B.

Pre-Registration Optometrist Learning Resource
Page 34 Third Visit Competencies – Questions 2010/11 24/5/2010
C.
D.

Pre-Registration Optometrist Learning Resource
Page 35 Third Visit Competencies – Questions 2010/11 24/5/2010
E.
F.

Pre-Registration Optometrist Learning Resource
Page 36 Third Visit Competencies – Questions 2010/11 24/5/2010
How would you describe the fluorescein fit of these RGP contact lenses? A. B.
C. D.
Pre-Registration Optometrist Learning Resource
Page 37 Third Visit Competencies – Questions 2010/11 24/5/2010
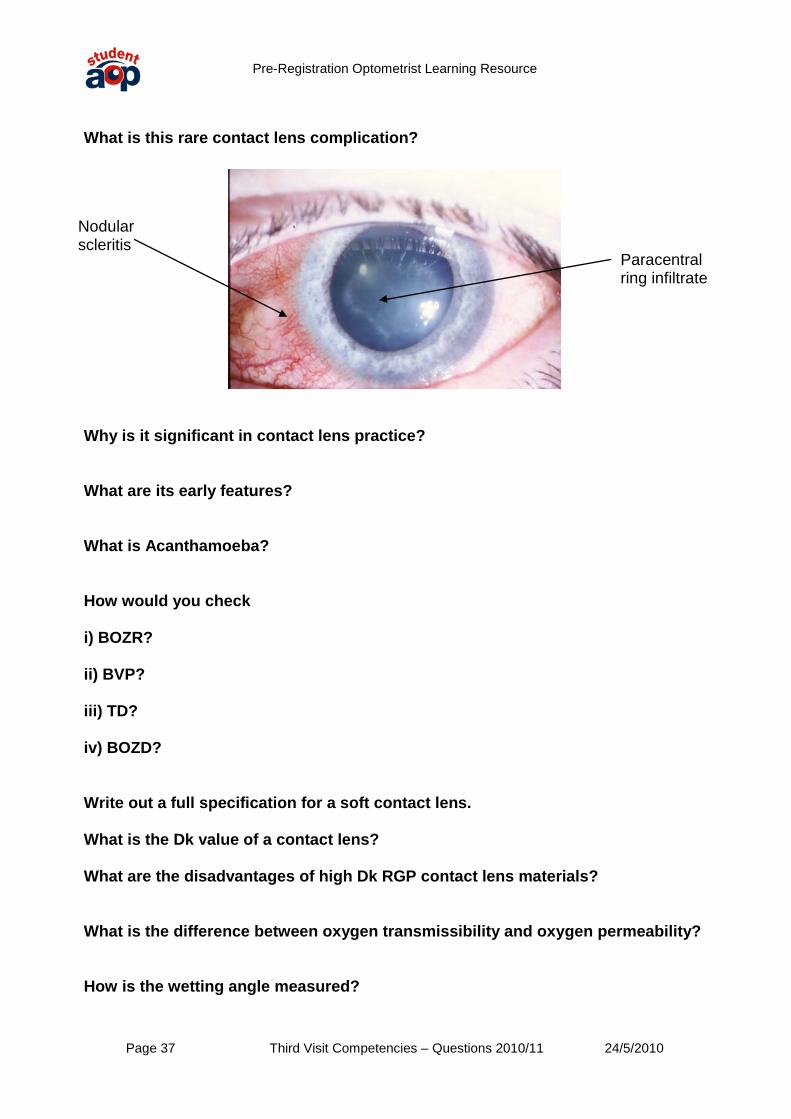
What is this rare contact lens complication?
Why is it significant in contact lens practice? What are its early features? What is Acanthamoeba? How would you check i) BOZR? ii) BVP? iii) TD? iv) BOZD? Write out a full specification for a soft contact lens. What is the Dk value of a contact lens? What are the disadvantages of high Dk RGP contact lens materials? What is the difference between oxygen transmissibility and oxygen permeability? How is the wetting angle measured?
Paracentral ring infiltrate
Nodular scleritis

Pre-Registration Optometrist Learning Resource
Page 38 Third Visit Competencies – Questions 2010/11 24/5/2010
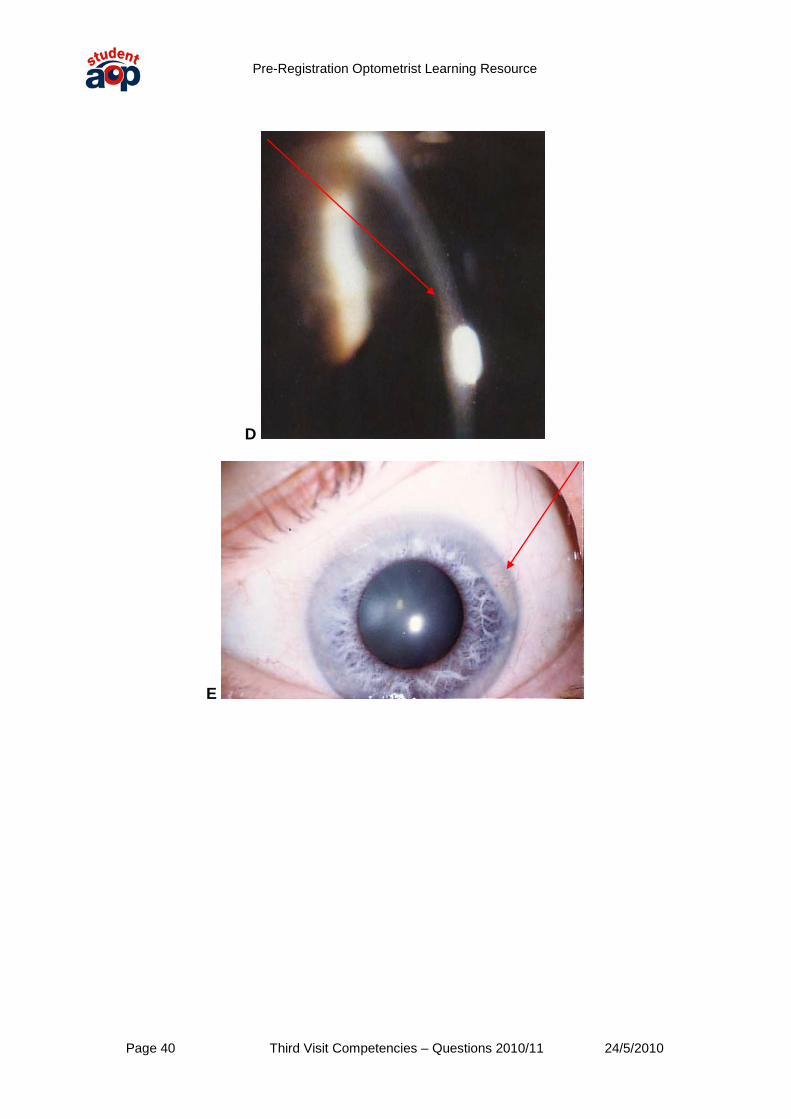
What is the six part classification for contact lens materials? Who may fit contact lenses in the UK? What changes to contact lens practice has the GOC’s Section 60 order caused? What is the difference between hypoxia and hypercapnia? What conditions do the following slides show? What are the cause, physiology and treatment of these conditions?
A

Pre-Registration Optometrist Learning Resource
Page 39 Third Visit Competencies – Questions 2010/11 24/5/2010
B
C
Pre-Registration Optometrist Learning Resource
Page 40 Third Visit Competencies – Questions 2010/11 24/5/2010
D
E

Pre-Registration Optometrist Learning Resource
Page 41 Third Visit Competencies – Questions 2010/11 24/5/2010
Identify the following conditions. What are the differences between them? A. B.
C.
What is the mechanism behind CLAPC? How would you grade CLAPC? What is your course of action in each of these situations? What is vCJD? Why is it of interest to contact lens practitioners? What does the General Optical Council statement of policy on the re-use of contact lenses have to say about trial contact lenses? What exceptions are there to this rule? What are the consequences for practitioners who do not follow this policy? What are Special complex diagnostic lenses?

Pre-Registration Optometrist Learning Resource
Page 42 Third Visit Competencies – Questions 2010/11 24/5/2010
How has the General Optical Council’s statement of policy altered the best practice for sterilising trial lenses? What contact lens options have you available for presbyopic patients? What would you need to be aware of in contact lens fitting in a patient with the following prescriptions? Patient 1: R -17.00 L -18.50/-0.50 x 180 Patient 2: R +17.00 L +18.50/-0.50 x 180 What does this corneal topography show?
Pre-Registration Optometrist Learning Resource
Page 43 Third Visit Competencies – Questions 2010/11 24/5/2010
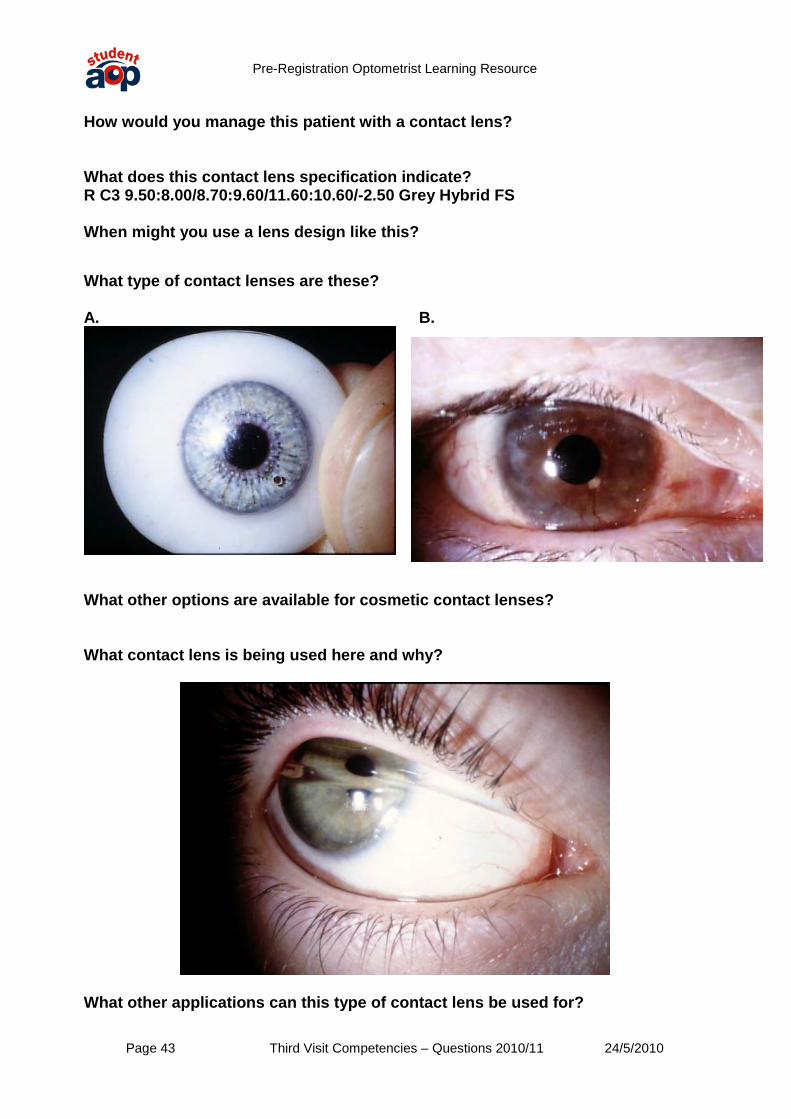
How would you manage this patient with a contact lens? What does this contact lens specification indicate? R C3 9.50:8.00/8.70:9.60/11.60:10.60/-2.50 Grey Hybrid FS When might you use a lens design like this? What type of contact lenses are these? A. B.
What other options are available for cosmetic contact lenses? What contact lens is being used here and why?
What other applications can this type of contact lens be used for?

Pre-Registration Optometrist Learning Resource
Page 44 Third Visit Competencies – Questions 2010/11 24/5/2010
Competency group 6: Ocular Disease 6.5 The ability to recognise common ocular abnormalities and to refer when appropriate. 6.6 The ability to manage a patient presenting with a red eye. 6.7 The ability to manage a patient presenting with reduced vision. 6.10 The ability to evaluate glaucoma risk factors, to detect glaucoma and refer accordingly. 6.11 The ability to manage a patient presenting with macular degeneration. 6.12 The ability to recognise, evaluate and manage diabetic eye disease and refer accordingly. 6.13 The ability to evaluate and manage a patient presenting with symptoms suggestive of retinal detachment. 6.15 The ability to recognise ocular manifestations of systemic disease. 6.17 The ability to assess symptoms and signs of neurological significance. 6.19 An ability to recognise adverse ocular reactions to medication. What is this condition? What is the appropriate action/possible treatment?

Pre-Registration Optometrist Learning Resource
Page 45 Third Visit Competencies – Questions 2010/11 24/5/2010
What signs can be identified on this patient’s fundus?
What condition is the patient likely to have? How is diabetic eye disease classified? What is its Epidemiology?
How does it affect the eye?
How is it detected? How can an optometrist investigate ARMD? What additional tests might an ophthalmologist use to investigate ARMD? Outline the aetiology, classification and treatment of ARMD. What is Avastin and why is relevant to optometric practice? What is CNV? How is it classified?

Pre-Registration Optometrist Learning Resource
Page 46 Third Visit Competencies – Questions 2010/11 24/5/2010
What do the following images show? How rapidly would you refer these patients and why?
1.

Pre-Registration Optometrist Learning Resource
Page 47 Third Visit Competencies – Questions 2010/11 24/5/2010
2.

Pre-Registration Optometrist Learning Resource
Page 48 Third Visit Competencies – Questions 2010/11 24/5/2010
3.

Pre-Registration Optometrist Learning Resource
Page 49 Third Visit Competencies – Questions 2010/11 24/5/2010
4.

Pre-Registration Optometrist Learning Resource
Page 50 Third Visit Competencies – Questions 2010/11 24/5/2010
5.
Pre-Registration Optometrist Learning Resource
Page 51 Third Visit Competencies – Questions 2010/11 24/5/2010
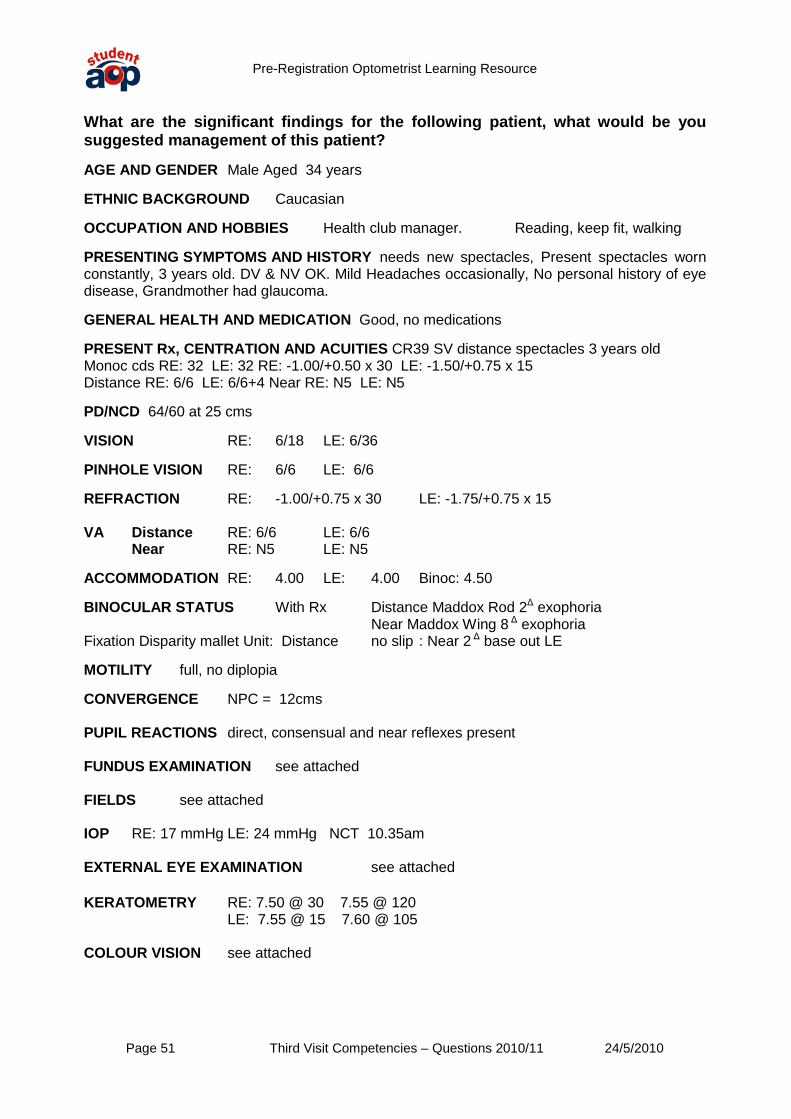
What are the significant findings for the following patient, what would be you suggested management of this patient? AGE AND GENDER Male Aged 34 years ETHNIC BACKGROUND Caucasian OCCUPATION AND HOBBIES Health club manager. Reading, keep fit, walking PRESENTING SYMPTOMS AND HISTORY needs new spectacles, Present spectacles worn constantly, 3 years old. DV & NV OK. Mild Headaches occasionally, No personal history of eye disease, Grandmother had glaucoma. GENERAL HEALTH AND MEDICATION Good, no medications PRESENT Rx, CENTRATION AND ACUITIES CR39 SV distance spectacles 3 years old Monoc cds RE: 32 LE: 32 RE: -1.00/+0.50 x 30 LE: -1.50/+0.75 x 15 Distance RE: 6/6 LE: 6/6+4 Near RE: N5 LE: N5 PD/NCD 64/60 at 25 cms VISION RE: 6/18 LE: 6/36 PINHOLE VISION RE: 6/6 LE: 6/6 REFRACTION RE: -1.00/+0.75 x 30 LE: -1.75/+0.75 x 15 VA Distance RE: 6/6 LE: 6/6
Near RE: N5 LE: N5
ACCOMMODATION RE: 4.00 LE: 4.00 Binoc: 4.50 BINOCULAR STATUS With Rx Distance Maddox Rod 2Δ
Near Maddox Wing 8 exophoria
Δ
Fixation Disparity mallet Unit: Distance no slip : Near 2 exophoria
Δ
base out LE
MOTILITY full, no diplopia CONVERGENCE NPC = 12cms PUPIL REACTIONS direct, consensual and near reflexes present FUNDUS EXAMINATION see attached FIELDS see attached IOP RE: 17 mmHg LE: 24 mmHg NCT 10.35am EXTERNAL EYE EXAMINATION see attached KERATOMETRY RE: 7.50 @ 30 7.55 @ 120 LE: 7.55 @ 15 7.60 @ 105 COLOUR VISION see attached

Pre-Registration Optometrist Learning Resource
Page 52 Third Visit Competencies – Questions 2010/11 24/5/2010
Fundus RE
Pre-Registration Optometrist Learning Resource
Page 53 Third Visit Competencies – Questions 2010/11 24/5/2010
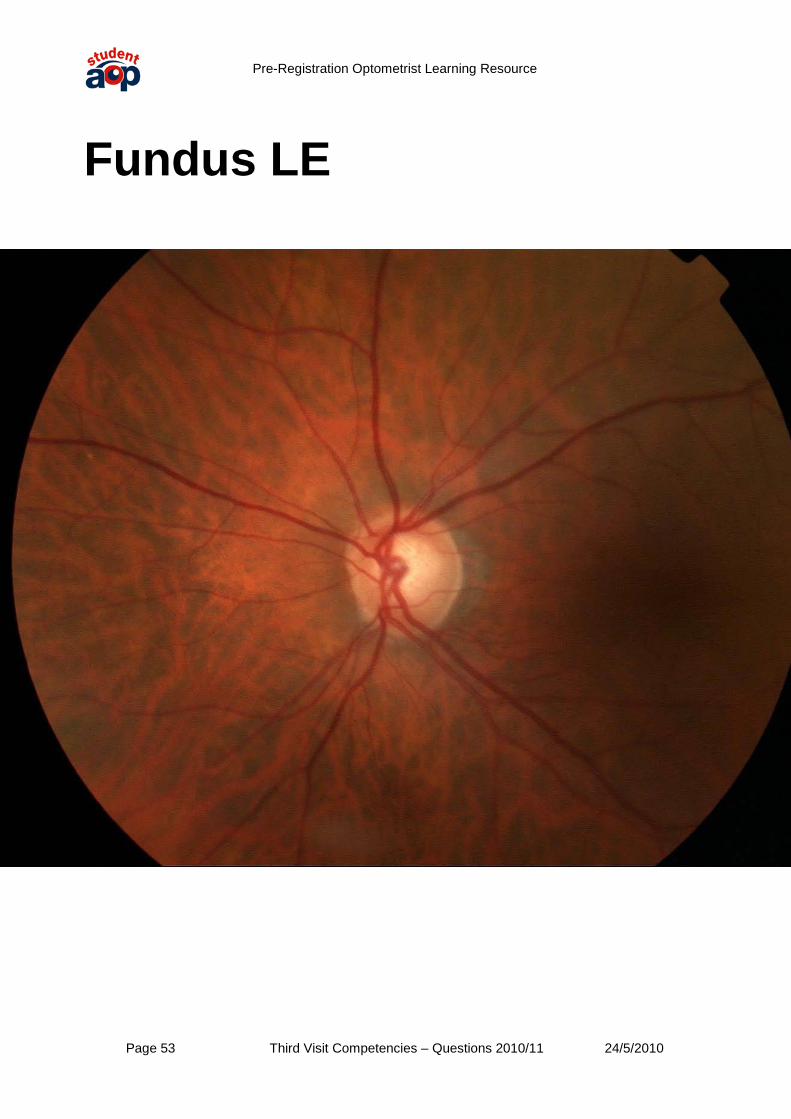
Fundus LE

Pre-Registration Optometrist Learning Resource
Page 54 Third Visit Competencies – Questions 2010/11 24/5/2010
External Eye RE

Pre-Registration Optometrist Learning Resource
Page 55 Third Visit Competencies – Questions 2010/11 24/5/2010
External Eye LE

Pre-Registration Optometrist Learning Resource
Page 56 Third Visit Competencies – Questions 2010/11 24/5/2010
Field plot RE

Pre-Registration Optometrist Learning Resource
Page 57 Third Visit Competencies – Questions 2010/11 24/5/2010
Field Plot LE
Pre-Registration Optometrist Learning Resource
Page 58 Third Visit Competencies – Questions 2010/11 24/5/2010
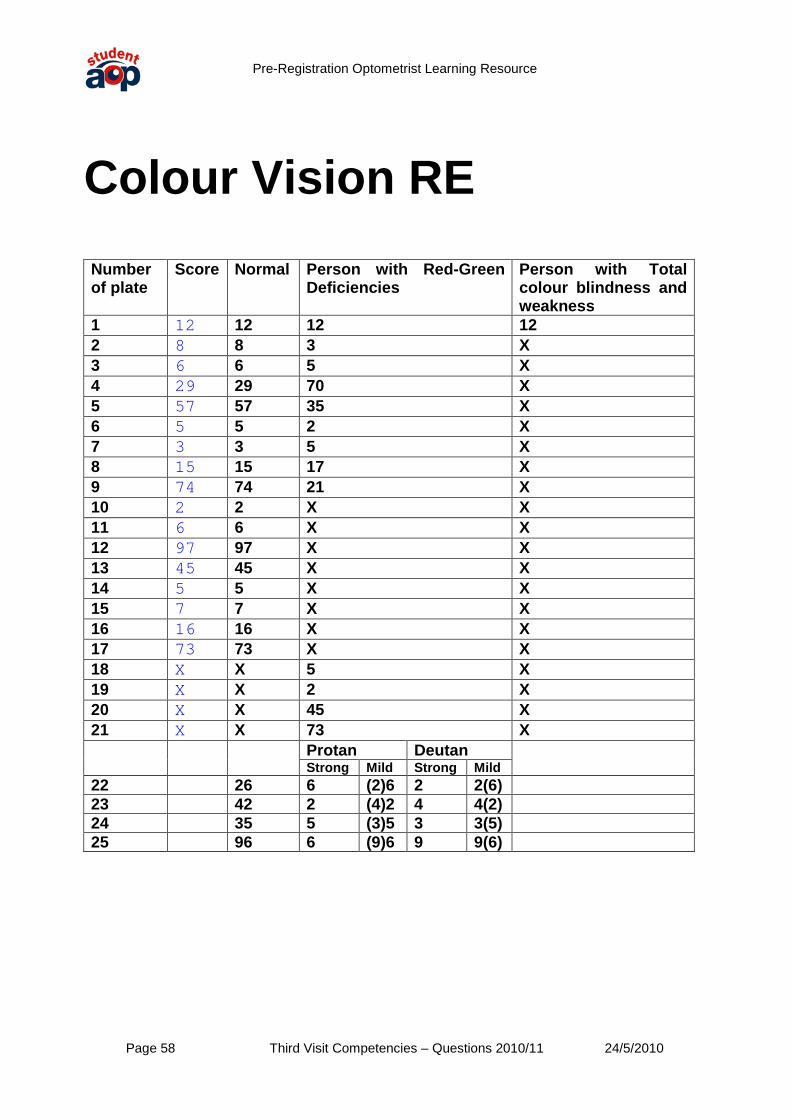
Colour Vision RE Number of plate
Score Normal Person with Red-Green Deficiencies
Person with Total colour blindness and weakness
1 12 12 12 12 2 8 8 3 X 3 6 6 5 X 4 29 29 70 X 5 57 57 35 X 6 5 5 2 X 7 3 3 5 X 8 15 15 17 X 9 74 74 21 X 10 2 2 X X 11 6 6 X X 12 97 97 X X 13 45 45 X X 14 5 5 X X 15 7 7 X X 16 16 16 X X 17 73 73 X X 18 X X 5 X 19 X X 2 X 20 X X 45 X 21 X X 73 X Protan Deutan
Strong Mild Strong Mild 22 26 6 (2)6 2 2(6) 23 42 2 (4)2 4 4(2) 24 35 5 (3)5 3 3(5) 25 96 6 (9)6 9 9(6)

Pre-Registration Optometrist Learning Resource
Page 59 Third Visit Competencies – Questions 2010/11 24/5/2010
Colour Vision LE Number of plate
Score Normal Person with Red-Green Deficiencies
Person with Total colour blindness and weakness
1 12 12 12 12 2 8 8 3 X 3 6 6 5 X 4 29 29 70 X 5 57 57 35 X 6 5 5 2 X 7 3 3 5 X 8 15 15 17 X 9 74 74 21 X 10 2 2 X X 11 6 6 X X 12 97 97 X X 13 45 45 X X 14 5 5 X X 15 7 7 X X 16 16 16 X X 17 73 73 X X 18 X X 5 X 19 X X 2 X 20 X X 45 X 21 X X 73 X Protan Deutan
Strong Mild Strong Mild 22 26 6 (2)6 2 2(6) 23 42 2 (4)2 4 4(2) 24 35 5 (3)5 3 3(5) 25 96 6 (9)6 9 9(6)
Pre-Registration Optometrist Learning Resource
Page 60 Third Visit Competencies – Questions 2010/11 24/5/2010
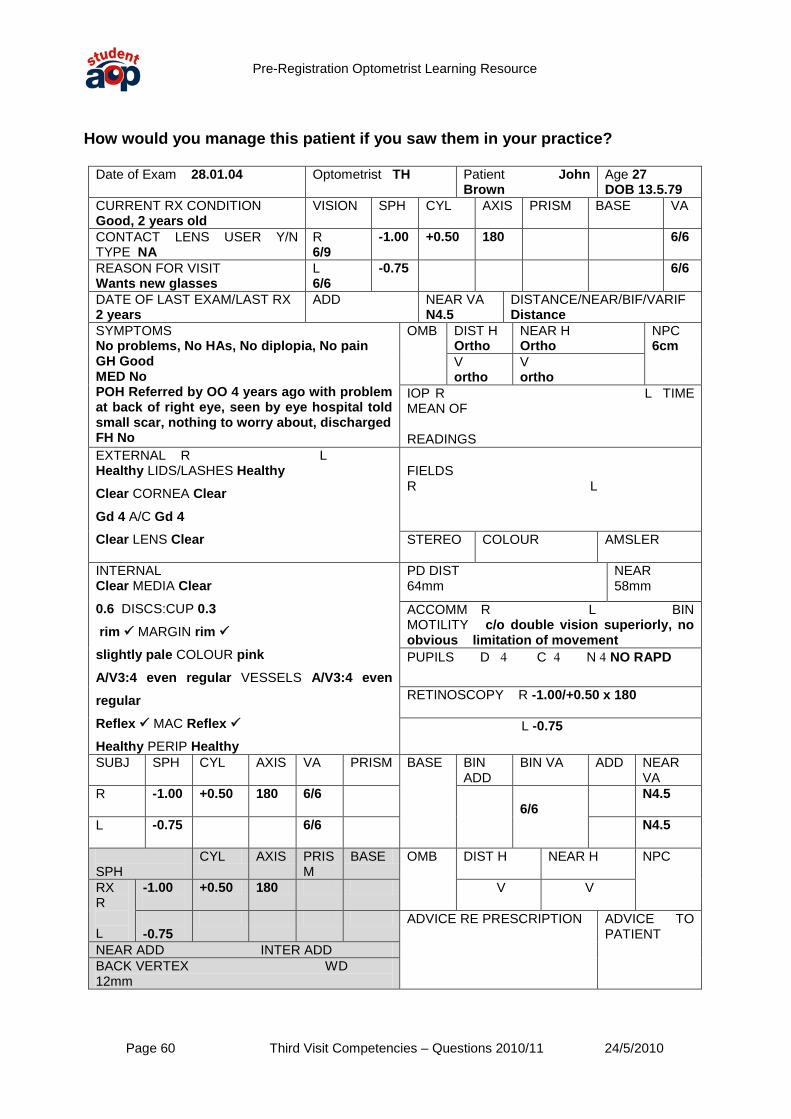
How would you manage this patient if you saw them in your practice?
Date of Exam 28.01.04 Optometrist TH Patient John Brown
Age 27 DOB 13.5.79
CURRENT RX CONDITION Good, 2 years old
VISION
SPH CYL AXIS PRISM BASE VA
CONTACT LENS USER Y/N TYPE NA
R 6/9
-1.00 +0.50 180 6/6
REASON FOR VISIT Wants new glasses
L 6/6
-0.75 6/6
DATE OF LAST EXAM/LAST RX 2 years
ADD
NEAR VA N4.5
DISTANCE/NEAR/BIF/VARIF Distance
SYMPTOMS No problems, No HAs, No diplopia, No pain GH Good MED No POH Referred by OO 4 years ago with problem at back of right eye, seen by eye hospital told small scar, nothing to worry about, discharged FH No
OMB
DIST H Ortho
NEAR H Ortho
NPC 6cm
V ortho
V ortho
IOP R L TIME MEAN OF READINGS
EXTERNAL R L Healthy LIDS/LASHES Healthy Clear CORNEA Clear Gd 4 A/C Gd 4 Clear LENS Clear
FIELDS R L
STEREO COLOUR
AMSLER
INTERNAL Clear MEDIA Clear 0.6 DISCS:CUP 0.3 rim MARGIN rim
slightly pale COLOUR pink A/V3:4 even regular VESSELS A/V3:4 even regular Reflex MAC Reflex
Healthy PERIP Healthy
PD DIST 64mm
NEAR 58mm
ACCOMM R L BIN MOTILITY c/o double vision superiorly, no obvious limitation of movement PUPILS D 4 C 4 N 4 NO RAPD
RETINOSCOPY R -1.00/+0.50 x 180 L -0.75
SUBJ SPH CYL AXIS VA PRISM BASE
BIN ADD
BIN VA ADD NEAR VA
R
-1.00 +0.50 180 6/6 6/6
N4.5
L
-0.75 6/6 N4.5
SPH
CYL AXIS PRISM
BASE OMB DIST H NEAR H NPC
RX R L
-1.00
+0.50 180 V V
-0.75
ADVICE RE PRESCRIPTION
ADVICE TO PATIENT NEAR ADD INTER ADD
BACK VERTEX WD 12mm
Pre-Registration Optometrist Learning Resource
Page 61 Third Visit Competencies – Questions 2010/11 24/5/2010
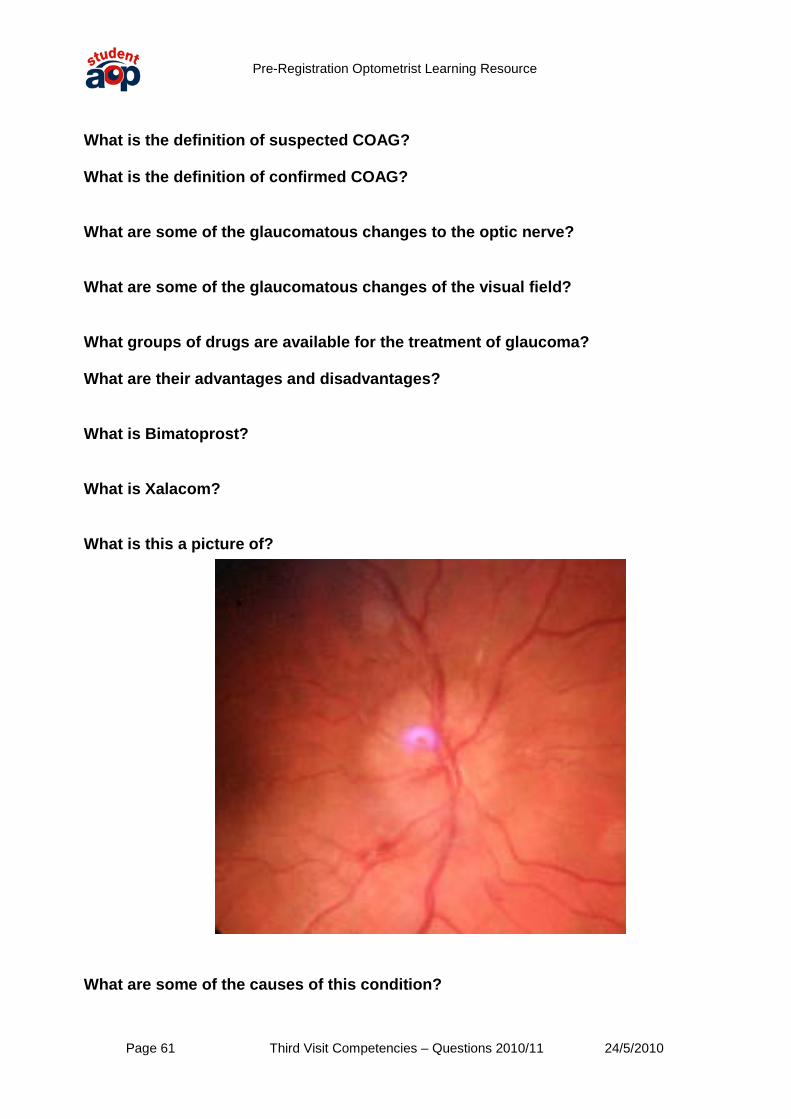
What is the definition of suspected COAG? What is the definition of confirmed COAG? What are some of the glaucomatous changes to the optic nerve? What are some of the glaucomatous changes of the visual field? What groups of drugs are available for the treatment of glaucoma? What are their advantages and disadvantages? What is Bimatoprost? What is Xalacom? What is this a picture of? What are some of the causes of this condition?

Pre-Registration Optometrist Learning Resource
Page 62 Third Visit Competencies – Questions 2010/11 24/5/2010
What solutions could you suggest for the difficulties faced by patients with: i) Central scotoma? ii) Gross peripheral field constriction? iii) Homonymous hemianopia? What antiseptic drugs are available to the optometrist? How do they work and what are they available as? What is the difference between antiseptic and anti-infective drugs? What would be your anti-infective drug of first choice? How does it work and what is it available as? Why are many GMPs reluctant to use Chloramphenicol? What other anti-infective drugs are available to the optometrist? What ophthalmic drugs can be prescribed by Level 2 optometric prescribers? What additional training is required for an optometrist to become a level 2 prescriber? How do corticosteroids work? What Corticosteroids are currently employed in ophthalmic treatment? What are the ocular side effects of steroid use? Which steroids may have fewer effects on IOP? What are NSAIDs? What NSAID is available for use (but not supply) by optometrists?
Pre-Registration Optometrist Learning Resource
Page 63 Third Visit Competencies – Questions 2010/11 24/5/2010
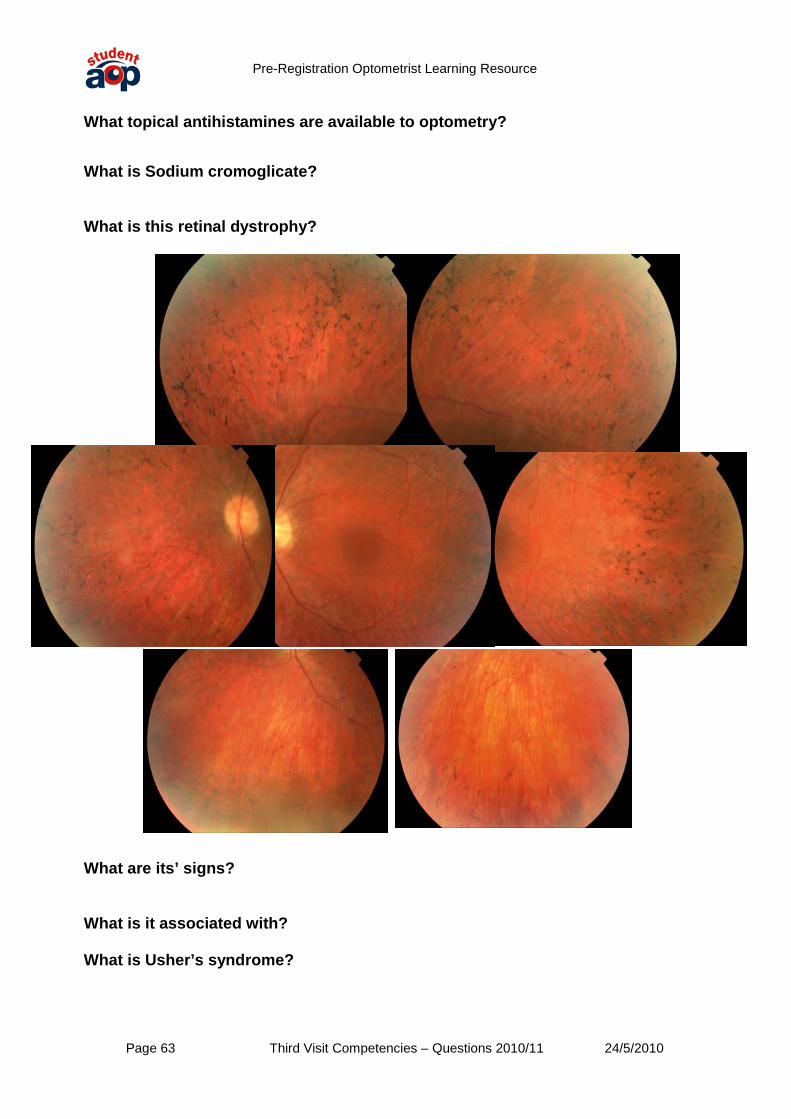
What topical antihistamines are available to optometry? What is Sodium cromoglicate? What is this retinal dystrophy?
What are its’ signs? What is it associated with? What is Usher’s syndrome?
Pre-Registration Optometrist Learning Resource
Page 64 Third Visit Competencies – Questions 2010/11 24/5/2010
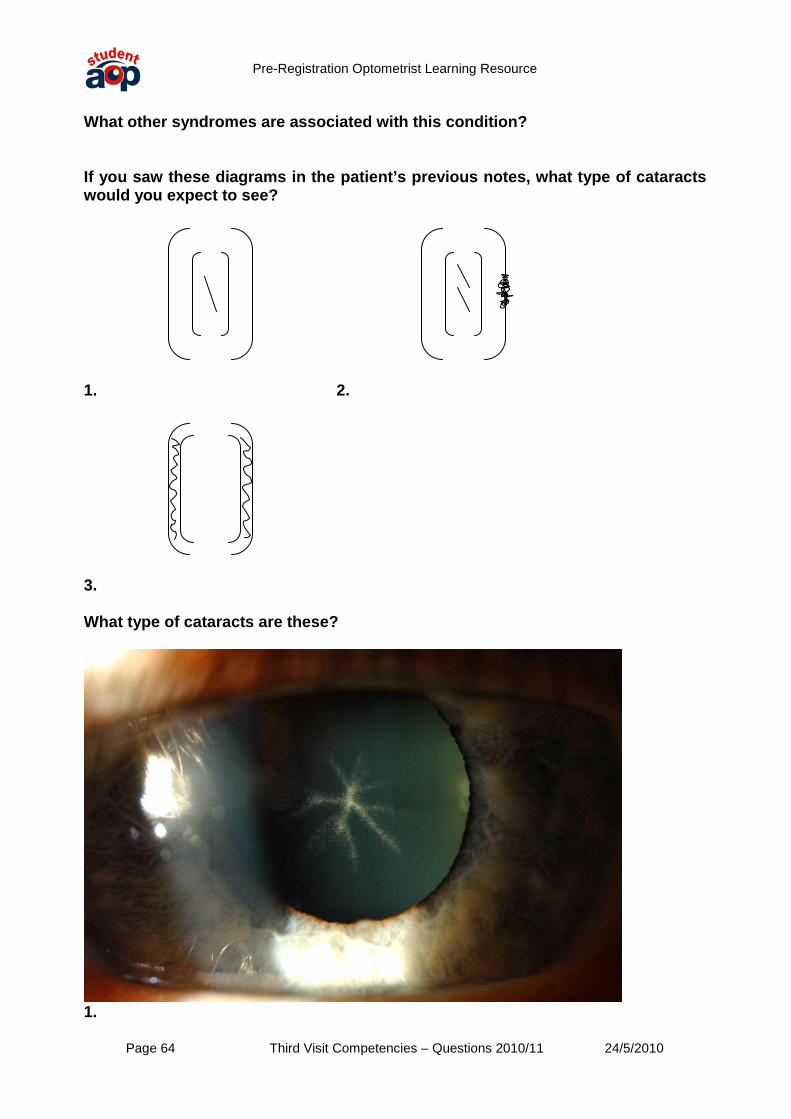
What other syndromes are associated with this condition? If you saw these diagrams in the patient’s previous notes, what type of cataracts would you expect to see?
1. 2.
3. What type of cataracts are these?
1.

Pre-Registration Optometrist Learning Resource
Page 65 Third Visit Competencies – Questions 2010/11 24/5/2010
2. What are the following drugs used for and what are there possible ocular side effects? Hydroxychloroquine Ethambutol Desferal (Desferrioxamine mesilate) What might cause a bilateral light –near dissociation of the pupil reactions? What is the most common phakomatosis? What are its’ possible ocular features? What are alexia, agraphia, and agnosia? Why are they significant for the optometrist?
Pre-Registration Optometrist Learning Resource
Page 66 Third Visit Competencies – Questions 2010/11 24/5/2010
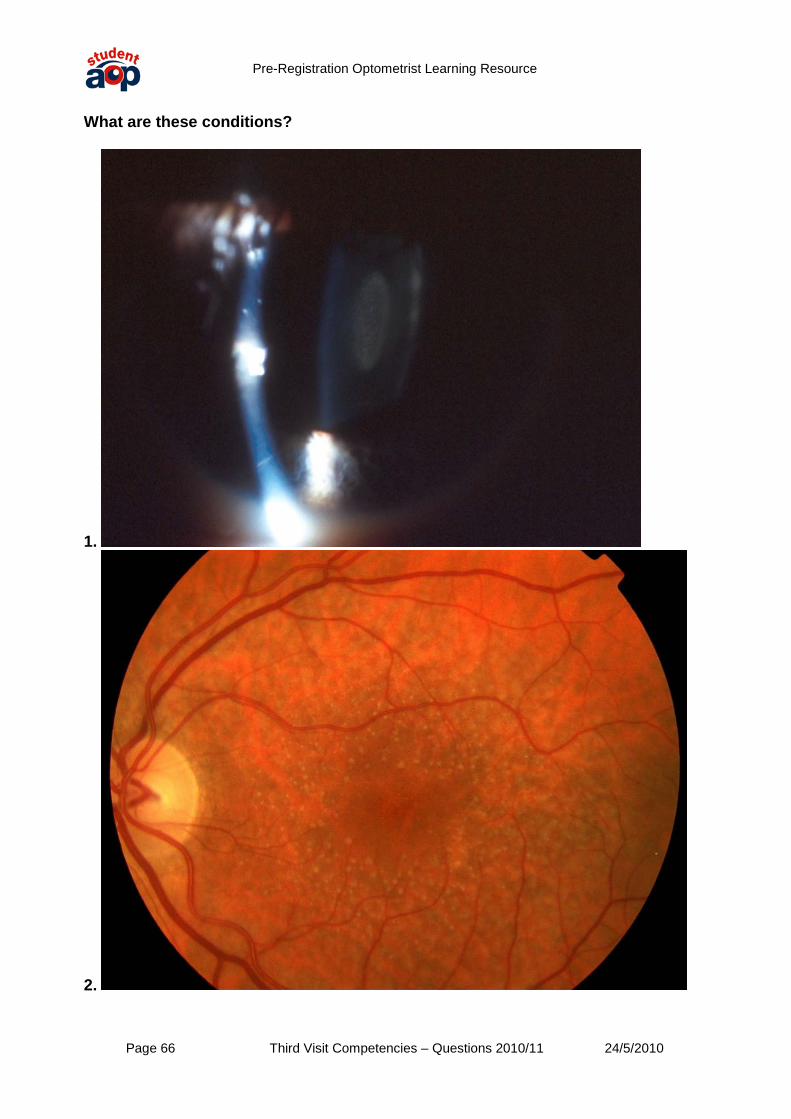
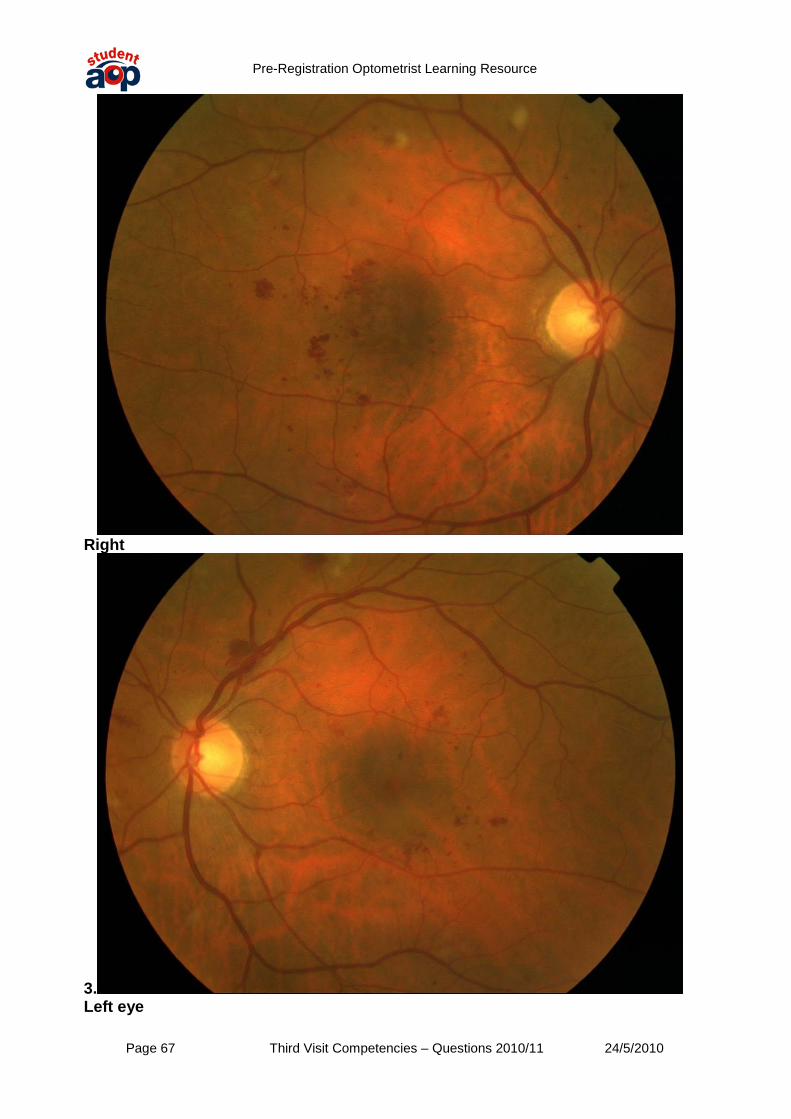
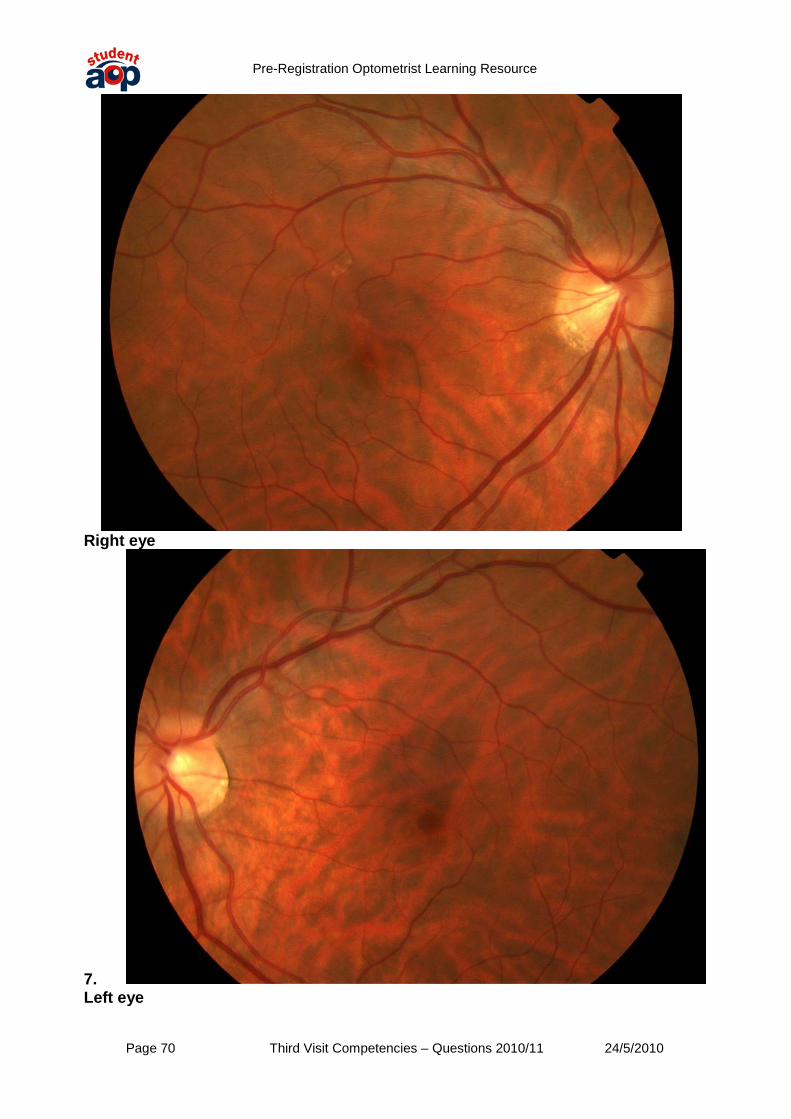
What are these conditions?
1.
2.
Pre-Registration Optometrist Learning Resource
Page 67 Third Visit Competencies – Questions 2010/11 24/5/2010
Right
3. Left eye

Pre-Registration Optometrist Learning Resource
Page 68 Third Visit Competencies – Questions 2010/11 24/5/2010
4.
5.

Pre-Registration Optometrist Learning Resource
Page 69 Third Visit Competencies – Questions 2010/11 24/5/2010
Right eye
6. Left eye
Pre-Registration Optometrist Learning Resource
Page 70 Third Visit Competencies – Questions 2010/11 24/5/2010
Right eye
7. Left eye

Pre-Registration Optometrist Learning Resource
Page 71 Third Visit Competencies – Questions 2010/11 24/5/2010
8.
9.

Pre-Registration Optometrist Learning Resource
Page 72 Third Visit Competencies – Questions 2010/11 24/5/2010
Right eye
10. Left eye

Pre-Registration Optometrist Learning Resource
Page 73 Third Visit Competencies – Questions 2010/11 24/5/2010
11.
12.

Pre-Registration Optometrist Learning Resource
Page 74 Third Visit Competencies – Questions 2010/11 24/5/2010
13.
14.

Pre-Registration Optometrist Learning Resource
Page 75 Third Visit Competencies – Questions 2010/11 24/5/2010
15.
16.

Pre-Registration Optometrist Learning Resource
Page 76 Third Visit Competencies – Questions 2010/11 24/5/2010
How would you manage them? What is the BNF? Why is it useful for an optometrist? What adverse ocular reactions to drugs would it be appropriate to report using the MRHA Yellow Card scheme? What should you not report?


















