Thesis written by · Web viewJ Orthop Sports Phys ical Ther apy. 25.3 (1997): 171–184. Peterson,...
40
Saint Xavier University A review of the anatomy and current research on the female predisposition to noncontact anterior cruciate ligament injuries Honors Project Submitted In Partial Fulfillment of the Requirements of HONOR 352/53 and for Graduation with Honors Spring 2015 By: Suzanne Broski Mentor: Dr. Rudyard Sadleir
-
Upload
duongkhanh -
Category
Documents
-
view
214 -
download
0
Transcript of Thesis written by · Web viewJ Orthop Sports Phys ical Ther apy. 25.3 (1997): 171–184. Peterson,...

Saint Xavier University
A review of the anatomy and current research on the female predisposition to noncontact anterior cruciate ligament injuries
Honors ProjectSubmitted
In Partial Fulfillment of theRequirements of HONOR 352/53and for Graduation with Honors
Spring 2015
By:Suzanne Broski
Mentor:Dr. Rudyard Sadleir

2
Thesis written by
Suzanne Broski
Approved by
________________________________________________, Mentor
Accepted by
__________________________________________, Honors Program Director
3
Abstract
Adolescent female athletes represent the population that is most likely to suffer from
noncontact anterior cruciate ligament (ACL) injuries, with a 4-6 times greater risk than their
male counterparts. Following an explanation of the normal anatomy and functioning of the ACL
and the mechanism of ACL injury, this paper explores possible causes of the gender disparity
surrounding ACL injury rates. Specifically, research studies regarding the differences between
male and female anatomical structure, biomechanics, neuromuscular functioning, genetics, and
hormones are considered. Despite attempts to conclude a singular cause of the increased risk of
noncontact ACL injury amongst female athletes, the gender disparity is likely multifactorial.
Therefore, prevention programs implemented to reduce the risk of female ACL injury should
target the modifiable risk factors which include biomechanical and neuromuscular functioning.
Ideally, these programs should be started as soon as a female begins participating in athletics in
order to avoid developing maladaptive techniques that may put her at risk of ACL injury.

4
INTRODUCTION
The anterior cruciate ligament (ACL) is a ligament in the knee that serves a stabilizing
function. In the United States, approximately 1 of every 3,500 individuals injures their ACL
annually, and an estimated 125,000-200,000 ACL reconstructions are performed each year.
Worldwide, an estimated one million ACL injuries occur every year (Noyes & Barber-Westin,
2012). ACL injury is very commonly suffered during athletic participation as a result of indirect
force to the knee, such as sudden changes in direction or speed. The consequences of injury to
the ACL are severe, especially for competitive athletes; these athletes may potentially miss an
entire season or more of their sport, lose scholarship funding or wages, suffer psychologically,
and/or experience future osteoarthritis. In addition to painful physical costs, the financial costs of
ACL reconstruction and rehabilitation are staggering for the patient and the broader community.
The average cost for ACL surgical repair is $38,121, which is independent of the expenses
incurred in physician evaluation, radiography of the knee, or postoperative rehabilitation
(Peterson & Krabak, 2014).
Studies suggest that most noncontact ACL injuries, or injuries that are not a result of a
direct external force to the knee such as a football tackle, occur between ages 16 to 18. Females
have a 4-6 times greater risk of ACL injury than their male counterparts participating in the same
sport (Hewett, Shultz, & Griffin, 2007). As the number of female athletes continues to rise, the
statistics regarding female ACL tears are especially alarming. Noncontact ACL injuries have
been reported to be as high as one out of every 100 high school female athletes and one out of
every 10 collegiate female athletes (Hewett, Shultz, & Griffin, 2007).
ANATOMY OF THE ACL
To better understand the causes of ACL injury, it is important to establish a full picture of
the anatomy of the human knee. The knee joint is the middle joint of the hind limb and is the

5
largest joint in the human body. It joins the femur (thigh bone) to the tibia (shin bone). The
patella, or knee cap, articulates with the femur and protects the knee joint in the front. The knee
has the ability to move with six degrees of freedom- three translations and three rotations. The
translations of the knee include proximal-distal (towards the body vs. away from the body),
anterior-posterior (front vs. back), and medial-lateral (side to side), and the rotations include
internal-external, varus-valgus (bow-legged vs. knock-kneed), and flexion-extension. The
muscles of the body pull on the bones of the skeleton to provide movement, and the primary
muscles that control the movement of the knee joint are the quadriceps, located on the anterior
surface of the thigh, and the hamstrings, located on the posterior surface of the thigh. In addition
to the bones and muscles of the knee, there are four ligaments that join the bones of the knee and
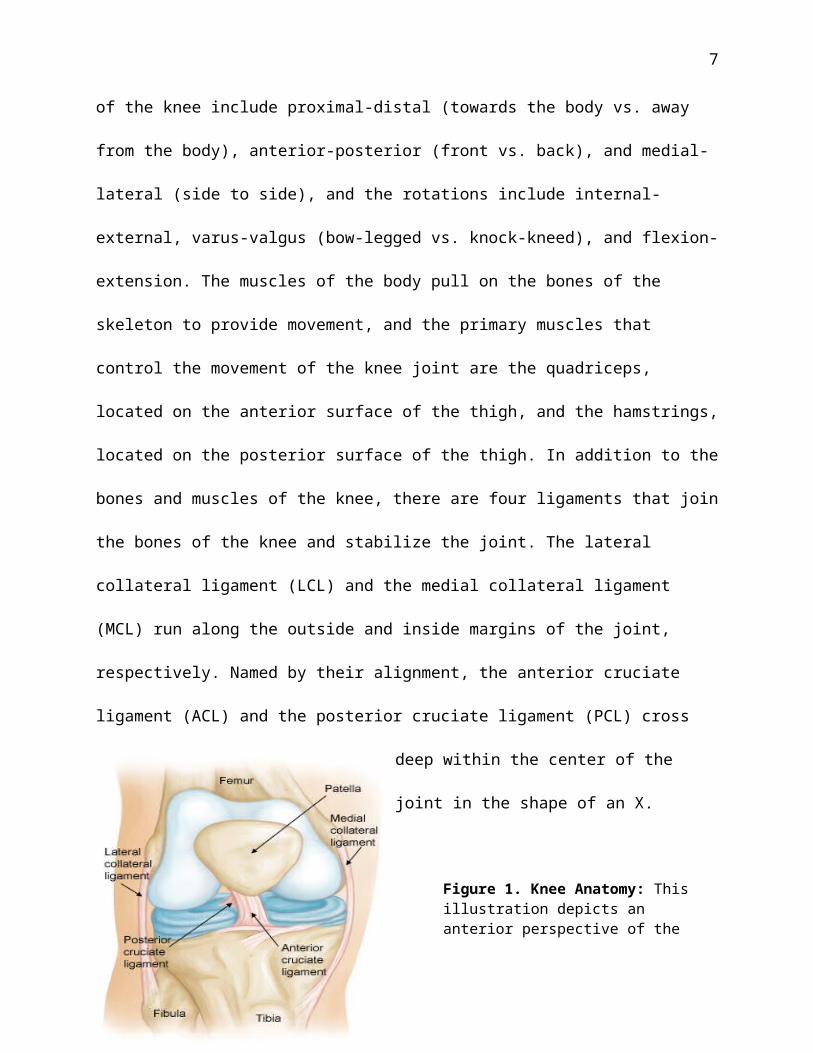
stabilize the joint. The lateral collateral ligament (LCL) and the medial collateral ligament
(MCL) run along the outside and inside margins of the joint, respectively. Named by their
alignment, the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL) cross
deep within the center of the joint in the shape of an X.
Figure 1. Knee Anatomy: This illustration depicts an anterior perspective of the right knee. The ACL is shown coursing anteriorly, medially, and distally from femur to tibia. Note the alignment in relation to the PCL (American Academy of Orthopedic Surgeons, 2009).
6
The ACL, the primary focus of this paper, is a band of dense regular connective tissue
that connects the femur to the tibia. Specifically, the ligament originates at the medial side of the
lateral femoral condyle and crosses obliquely through the intercondylar fossa to the medial tibial
eminence where it is inserted. The tibial attachment is somewhat broader than the femoral
attachment, with the ACL beginning to “fan out” in the proximal one-third of the ligament. As
the ACL courses anteriorly, medially, and distally from femur to tibia, it turns in a slight lateral
spiral giving it a twisting appearance (Jackson, 1993).
The ACL primarily resists anterior displacement of the tibia with respect to the femur and
secondarily resists tibial rotation. However, the ACL does not function as a singular cord, but
rather as two major fiber bundles, named according to the insertion sites on the tibia: the
anteromedial (AM) bundle and the posterolateral (PL) bundle. The AM bundle acts as the
primary tissue restraining anterior tibial translation; in other words, the AM bundle prevents the
tibia from displacing anterior to the femur. The PL bundle stabilizes the knee at full extension to
prevent internal and external rotation of the tibia. The difference in functionality between the two
bundles results from varied tensions throughout the knee joint’s range of motion. With the knee
extended, the AM bundle is moderately loose, and the PL bundle is tight. When the knee is
flexed, the femoral attachment of the ACL has a horizontal orientation that causes the AM
bundle to tighten and the PL bundle to relax (Petersen & Zantop, 2006).
BIOMECHANICS OF THE ACL: the pathway to INJURY
The ACL limits the anterior tibial translation, axial tibial rotation, and varus or valgus
knee angulation. The ACL provides 87% of the total restraining force to anterior tibial
translation when the knee is flexed at a 30° angle and 85% at a 90° angle (Noyes & Barber
Westin, 2012). Without an intact ACL, stabilization of the knee is greatly reduced. Varying
7
angles of knee flexion, knee constraint, and the magnitude and direction of the applied load can
produce different forces in the ACL. Studies done by Berns et al. (1992), Markolf et al. (1995),
and Fleming et al. (2001) all demonstrate that anterior shear force on the proximal end of the
tibia increases ACL loading. Additionally, the studies show that knee valgus angulation and
internal rotation of the tibia, in combination with anterior shear force at the proximal end of the
tibia, increase the strain on the ACL. The quadriceps muscles are the primary contributors of
anterior shear force on the proximal end of the tibia, while the hamstrings reduce ACL loading
during contraction. Finally, the studies show that a decreasing knee flexion angle increases ACL
loading (Hewett, Shultz, & Griffin, 2007).
An ACL injury can be categorized as a partial tear, a complete tear, or a bone avulsion.
Partial tears are characterized as such when only a portion of the ACL fibers are damaged. A
complete tear is defined by both the AM and PL bundles being completely severed. A bone
avulsion occurs when the bony attachment area of the ACL gets pulled away from the rest of the
bone. 70% of ACL tears are a result of noncontact forces such as cutting, pivoting, accelerating,
decelerating, or landing from a jump. The forces that cause noncontact ACL injuries are a
product of ground reaction forces and internal soft-tissue and muscles forces. The other 30% of
ACL injuries are termed contact injuries, which result from a direct blow to the knee joint.
Contact ACL injuries are commonly seen in football. Kiapour et al. (2014) identified a multi-
planar mechanism of non-contact ACL injuries. Using human cadaveric tissue, the study
indicated that a combination of anterior tibial translation, knee abduction (valgus moment), and
internal tibial rotation leads to greater strain on ACL, and therefore, increases the risk for injury.
The results also emphasized the significant role of anterior tibial translation and knee abduction
8
as primary contributors and internal tibial rotation as a secondary contributor to the risk of ACL
injury.
THE GENDER DISPARITY IN ACL INJURY RATES
The female athlete has a 4-6 times greater risk of injuring her ACL in comparison to the
male athlete playing a sport with similar landing and cutting movements. The gender disparity
associated with ACL injury is speculated to be multifactorial in nature. Proposed causes of
gender differences in ACL injury rates include the effects of anatomical structure, biomechanics,
neuromuscular functioning, genetics, and hormones. While many studies have attempted to look
at these categories as separate entities, it is important to note the possible interplay between risk
factors.
Anatomical differences
Naturally, an area of initial interest regarding the gender disparity of the rate of ACL
injuries is the anatomical structure of the female ACL compared to the male ACL. The ACL
passes through the intercondylar femoral notch and moves within it during motion of the knee
joint. According to research by Shelbourne et al (1998) the rate of ACL injury is higher in people
with more narrow notches (defined as <15 mm), regardless of gender. However, they also found
that women, on average, have more narrow notches compared to men, which may account for the
greater incidence of ACL injuries. Further, the study showed that following ACL reconstruction
in which the new ACL size is standardized for both sexes, the higher rate of ACL tears in
patients with narrower notches is eliminated. As a result, Shelbourne et al concluded that the
width of the notch is not a causative factor of ACL tears, but a narrow notch does reflect a
smaller ACL housed within which may affect the susceptibility to injury. This study did not go
as far as to determine if a larger ACL (in terms of volume) represents a stronger ligament.

9
Although Shelbourne et al. and other authors have found that, on average, females have smaller
intercondylar notches even when accounting for smaller stature, various other studies prove this
finding to be controversial. Lombardo et al. (2005) did not find a significant correlation between
intercondylar notch width and ACL injuries, while LaPrade et al. (1994) found that athletes with
a narrower notch were at increased risk of ACL injury but found no difference in notch width
between genders. The controversies between studies seem to result from differences in study
designs and methodologies, such as imaging and measurement techniques. Regardless, the
equivocal results concerning the width of the intercondylar notch width with regards to female
ACL injuries highlight that fact that anatomy is not the sole determinate in ACL tears.
Hypotheses relating to different anatomical structure are not limited to the knee joint
specifically. Researchers have also investigated the role of the entire lower extremity in ACL
injury. The femur meets the tibia at an angle termed the quadriceps femoris angle or “Q angle.”
Clinically, it is defined as the angle in the frontal plane that is formed by the intersection of the
line that connects the center of the patella to the anterior superior iliac spine and the line that
connects the center of the patella to the tibial tubercle. In comparison to men, women not only
have an increased pelvic width, but they also have a shorter femoral length; these anatomical
differences result in females having an increased Q angle. According to studies by Zelisko et al.
(1982) and Haycock and Gillette (1976), a larger Q angle results in greater force placed on the
medial aspect of the knee, and essentially greater risk of ACL injury. Yet, studies by Gray et al.
(1985) and Endsley et al. (2003) showed no correlation between Q angle measurements and
injury rate. Thus, the results reveal that static anatomical measurements may not be the best
predictors of ACL injury in females.
10
According to Boden et al. (2000), the female athlete has increased joint laxity compared
to the male athlete. They reported that patients who suffered from ACL injuries demonstrated
excessive extension at the knee joint and increased ability to touch the palms of their hands to the
floor. Uhorchak et al. (2003) found that women with generalized joint laxity were at a 2.7 times
greater risk of ACL injury than females without joint laxity. Joint laxity has been shown to
increase knee hyperextension and knee valgus, which can put strain on the ACL. Boden et al.
also reported that ACL injured athletes displayed more lax hamstring muscles. While males
demonstrate decreased flexibility with age after puberty, females demonstrate increased
flexibility after puberty. Studies by Hewett et al. (2006) and Huston and Wojtys (1996) suggest
that a decrease in dynamic control of the knee in females could be partially caused by increased
hamstring flexibility during and after puberty. However, the co-contraction of the quadriceps and
the hamstring muscles needs to be considered to add more strength to this argument.
Biomechanical differences
Biomechanical risk factors of female ACL injuries have been areas of in-depth research
because they are modifiable, as opposed to anatomical risk factors. The knee, hip, and ankle have
been focused on during research in order to determine the contribution of each joint to ACL
injury. According to research done by Hutchinson and Ireland (1995), planting and cutting
(29%), straight knee landing (28%), and one step-stop landing with the knee hyperextended
(26%) are the most commonly observed movements involved in female noncontact ACL
injuries. The posture and lower extremity alignment of females during these movements may put
the athlete at increased risk of ACL injury. In general, women change direction in a more erect
position than men, which can result in decreased flexion in the knee and hip, increased valgus in
11
the knee, and greater activation of the quadriceps muscles- all of which can add strain to the
ACL.
A study by Hewett et al. (2006) showed that knee abduction was more than 8° greater in
patients who had suffered ACL injuries as compared to the control group. It is likely that the
increased valgus moment contributed to the mechanism of ACL injury in those patients. Ford et
al. (2005) used motion analysis to demonstrate that during cutting movements, females display
greater knee abduction angles compared to male athletes. Looking at both of these studies
together, it can be inferred that the knee valgus position of female athletes during change of
direction increases the likelihood of ACL injury. However, in terms of knee flexion, research has
been inconclusive. A study by Malinzak et al. (2001) found that females had less knee flexion
compared to males during a side step movement, while Mclean et al (2005) did not report a
gender difference during the same movement. Withrow et al. (2006) reported less knee flexion in
females during landing from a 60 cm height but not from a 20 cm height. Fagenbaum and
Darling (2003), in contrast, found that females actually demonstrated greater knee flexion angles
compared to males during a drop jump landing. Without further research, the evidence indicates
that female knee flexion angles are similar to those of males during athletic maneuvers.
The hip biomechanics of a female during landing may contribute to ACL injury risk.
Lephart et al. (1997) reported that women land with greater hip internal rotation than men, and
Zazulak et al. (2007) found that while the gluteus maximus can minimize excessive hip rotation,
it is activated less in females than in males. Ford et al. (2005) found differences in hip
stabilization in the dominant versus nondominant sides of the female athlete. Women land with
greater external hip adduction and decreased hip flexion angles on the dominant side. Greater
external hip adduction may cause instability during dynamic movement, and in combination with
12
asymmetry, can lead to valgus positioning of the knee while landing. As already mentioned,
valgus loading on the knee puts strain on the ACL.
Increased ankle eversion, represented by the medial side of the foot remaining planted on
the ground while the lateral side elevates off the ground, may contribute to the gender disparity
in ACL tears. Ford et al. (2005) found that during change of direction, female athletes had a
greater ankle eversion than male athletes. Consequences of excessive ankle eversion are valgus
knee stress, anterior tibial translation, and increased loading on the ACL (Nyland et al, 1997).
However, foot pronation and internal tibial rotation also couple with ankle eversion.
A relationship between core stability and ACL injury risk has been the speculated. The
core is “the strength and function of the abdominal, back extensor, and pelvic floor muscles that
contribute to stability of the lumbopelvic-hip region complex” (Biering-Sorensen, 1984). The
core is considered a person’s center of gravity and is where all movements originate. A stable
core allows for efficient movements of the lower extremity and helps to reduce forces on the
joints. Although the effects of core stability on ACL injury risk remain controversial, results
from an analysis of 104 varsity college athletes indicate a positive correlation between measures
of core stability and risk for lower extremity injury (Ireland, 2002). A study done on competitive
alpine skiers by Raschner et al. (2006) concluded that not only are female skiers more at risk for
ACL tears, but also that absolute core strength is a predicative variable in female alpine skiers.
More research is necessary to consider core strength a significant risk factor for female ACL
injuries, but this research topic is worth pursuing.
Neuromuscular differences
Neuromuscular control is defined as “the unconscious efferent response to an afferent
signal about dynamic joint stability” (Silvers & Mandelbaum, 2007). Control of the knee
13
involves the interaction between feedforward and feedback systems. The feedforward system
anticipates forces on the knee and activates muscles in order to protect the knee joint. The
feedback system is reflexive in nature, and results from the force on the joint. On the onset of
puberty, males and females begin to display differences in neuromuscular development. Hewett
et al. (2007) found that the neuromuscular development of females lags behind the increase in
size and weight during puberty, whereas the neuromuscular development and physical
development of males generally coincide. Until neuromuscular control improves, a lack of
coordination in the adolescent female may contribute to the increased risk of ACL injury.
The stability of the knee depends on the strength and recruitment of the surrounding
musculature. The quadriceps and hamstrings muscles work together in an antagonist-agonist
relationship to protect the knee joint from excessive anterior tibial translation and knee
abduction. The quadriceps muscle serves as the antagonist to the ACL such that it increases the
anterior shear force on the tibia, while the hamstring muscle serves as the agonist by preventing
excessive anterior translation of the tibia. Failure of the ACL can result from weakened strength
or slowed activation of the hamstrings in comparison to the quadriceps. A study done by
Malinzak et al. (2015) used electromyography analysis to measure hamstring and quadriceps
activity in males and females when landing from a jump and performing cutting maneuvers. The
resulting data showed that females had greater quadriceps activity and less hamstring activity
compared to males. Also, females contracted their hamstring fibers 50 milliseconds slower than
males and with less intensity. A quadriceps dominant mechanism during landing or cutting puts
the female at increased risk for ACL injury because of the increased displacement of the tibia
and greater stress on the ACL. Myer et al. (2005) reported a low ratio of medial quadriceps to
lateral quadriceps recruitment and an increase in lateral hamstring firing in female athletes
14
compared to males. The combined imbalance of musculature in the portions of the quadriceps
and hamstrings increases the risk of ACL injury because it results in knee valgus positioning and
greater anterior shear force on the knee (Rozzi et al, 1999).
The musculature of the hip also contributes to the dynamics of the knee. Zazulak et al.
(2015) reported that women have lesser gluteal muscle firing compared to men, and this decrease
in musculature activation in the hip produces more force in the lower extremity which causes
valgus collapse in the knee. Additionally, Griffin et al. (2000) reported that decreased activation
of the hip muscles reduces the maximum activation of the quadriceps and hamstrings, and
therefore, reduces the capacity of the load that can be placed on the lower extremity without
causing injury.
Genetic differences
Varying gene expression has been an area of speculation concerning the difference in the
rates of male and female ACL tears. With the advancement in genetic analysis, the correlation
between genetics and ACL injury has been increasingly researched. A recent study done by
Johnson et al. (2015) used biopsies of ruptured ACL tissue from seven males and seven females
between the ages of 12 and 22. Microarray analysis identified thirty-two genes with significant
differential expression between the male and female specimens, and three of these genes code for
specific proteins related to ACL’s structure. Two genes, ACAD and FMOD, are known to
regulate the extracellular matrix of the ligament, and these genes were upregulated in the female
tissue samples compared to the male tissue samples. The gene WISP2 functions in collagen
turnover and production and was downregulated in the female biopsies. Johnson et al. concluded
that the significant difference in the female gene expression of ACAD, FMOD, and WISP2 may
lead to weaker ACL’s in females compared to males. While this study is a noble starting point
15
for research into the correlation between female genes and ACL injury, it is limited in that it uses
samples of already ruptured ACL tissue.
Hormonal differences
Hormonal differences between males and females that emerge during puberty have been
thought to contribute to the gender disparity in ACL injury rates. Specifically, the hormonal
changes during the 28 day female menstrual cycle have been an area of active research
concerning ACL injury. The menstrual cycle can be divided into three phases: the follicular
phase (days 1-9), the ovulatory phase (days 10-14), and the luteal phase (days 15-28). During the
early follicular phase, low concentrations of the sex hormones, progesterone and estrogen, are
present; however, a spike in estrogen occurs during the late follicular phase and continues into
the ovulatory phase. The luteal phase is marked by a rise in progesterone, in addition to a rise in
the hormone relaxin in the second half of the stage. With the discovery of hormone receptor sites
on the ACL, the variations in the concentrations of progesterone, estrogen, and relaxin have been
studied to determine the effect on the structure of the ACL.
The contribution of estrogen concentrations on ACL injury is a controversial area of
research. A study done by Wojtys et al. (2002) found that there is an increased incidence of
noncontact ACL injuries during the ovulatory phase of the menstrual cycle and a decreased
incidence during the follicular phase. In contrast, Slauterbeck et al. (1999) saw the greatest
number of ACL injuries just before menstruation, during the luteal phase. Myklebust et al.
(1998) reported an increase in ACL injury during the follicular phase during menstruation. The
variance in the findings may be contributed to menstrual phase definitions and sex steroid
measurements. Additionally, the studies rest on the assumptions that all females have a normal
16
28 day cycle with consistent phase lengths. Study designs that take into account the unique
characteristics of each female’s menstrual cycle should be aimed for in future research.
Fluctuating hormone concentrations during the menstrual cycle may decrease ligament
strength, and therefore, contribute to female ACL injuries. Booth and Tipton (1969) found that
estradiol, a type of estrogen, significantly decreases ligament strength, and Samuel et al. (2007)
found that relaxin decreases soft tissue tension. In an in vitro study, Yu et al. (1999) found an
inverse relationship between the concentration of estrogen and ACL fibroblasts throughout the
menstrual cycle and proposed that females may be more prone to ACL injury because of the
direct effect of estrogen on collagen synthesis in the ligament. Slauterbeck et al. used a rabbit
model to study the effect of estrogen on failure load of the ACL. They found that with an
increased concentration of estrogen, the tensile properties and the failure load of the ACL
decreased. In contrast, Strickland et al. (2003) observed no differences in maximum force,
stiffness, failure load, or failure site in sheep with estrogen implants, and Seneviratne et al.
(2004) concluded that there were no clinically significant changes in the material properties of
sheep ACL in vivo due to estrogen fluctuation during the menstrual cycle. Joint laxity resulting
from hormonal changes has also been speculated as a cause of increased ACL injury rate. Wojtys
et al found an increase in knee joint laxity during the ovulatory phase of the menstrual cycle,
while Heitz et al. (1999) reported that ACL laxity increased across the cycle. However,
Karageanes et al. (2000) found no difference in laxity throughout the cycle. Currently, research
conducted on physically active women with normal and comparable menstrual cycles is lacking
and should be a direction for future study.
Although it seems as if hormones have an effect on ACL collagen production and knee
laxity to a certain extent, the neuromuscular and biomechanical repercussions of the biological

17
changes need to be considered. Estrogen directly and indirectly affects the female neuromuscular
system. Sarwar et al. (1996) found that during the ovulatory phase of the cycle, quadriceps
strength increases and muscle relaxation slows, which may put a female at increased risk for
ACL injury. Estrogen also affects the central nervous system. Lebrun et al. (1995) found
differences in isokinetic strength, anaerobic and aerobic capacity, and endurance in females
throughout different phases of the menstrual cycle. Motor skills were found to decrease during
premenstrual phases in a study performed by Posthuma et al. (1987). Taking all research into
account, hormones are likely to be a contributor to the neuromuscular control of the knee joint,
but must be considered in light of the other risk factors.
PREVENTION
The purpose of researching the causes of noncontact ACL injuries in females is to be able
to implement prevention programs to reduce their incidences. Considering the many physical,
emotional, and financial consequences that are involved with ACL injuries, great efforts have
been taken to develop effective injury prevention strategies, especially for females. While
anatomical, genetic, and hormonal risk factors are important to research for the sake of
understanding how and why ACL injuries occur, these factors are not as easily modifiable as
biomechanical and neuromuscular risk factors. For this reason, the prevention of ACL injuries in
females has been primarily focused on biomechanical and neuromuscular training.
The abundance of available research relating to ACL injuries has resulted in a variety
prevention programs with different elements. However, each one seems to place emphasis on
landing and cutting with knee and hip flexion, avoiding knee valgus position, increasing the
strength of the hamstring, gluteus medius, and hip abductor muscles, and decelerating under
control (Silvers & Mandelbaum, 2007). Time of implementation (such as preseason or during
18
season), frequency, and duration differ amongst the programs. Additionally, the targeted age
group, skill level, and sport contribute to the variety of prevention techniques.
According to an analysis of prevention programs by Renstrom et al. (2008), a successful
program incorporates “neuromuscular training/control, muscle strengthening, plyometrics, as
well as education and feedback regarding body mechanics and proper landing patterns in a
dynamic atmosphere.” The most successful programs were initiated 6 weeks prior to regular
season practice and competitions. The training should take 15-20 minutes and should be
performed at least 3 times per week. In order to reinforce proper landing and cutting techniques,
the program should be continued throughout the season, and may be incorporated as part of a
warm-up routine. The athlete should receive feedback from a teammate or coach who know and
understand the safe position that the athlete should maneuver in. Using a mirror or video
recording is also helpful so that the athlete can analyze their own form.
Plyometrics drills mimic the maneuvers of real sport situations in a controlled setting.
Cutting, jumping, and lateral movements are incorporated into high intensity agility drills that
challenge the athlete to maintain proper form throughout the duration. Emphasis should be
placed on beginning and ending a cut or jump with flexed knees and hips. Additionally, the
knees should not angle inward, and more weight should be distributed to the front of the foot
upon landing. Plyometric drills can train the athlete to perform explosive movements with proper
muscle recruitment and mechanics. As the program advances, drills should increase in difficulty
and disturbances should be incorporated in order to simulate the unpredictable nature of athletics
(Myer et al., 2008).
In order to consistently and naturally maintain proper form, strength training is a
necessary component of a prevention program. Because research has shown that hamstring
19
recruitment is lacking in many females, hamstring strengthening should be a point of emphasis.
Strengthening of hip abductors and gluteus medius muscles may also reduce the likelihood of
landing in a knee valgus position. Coordination of movement can also be improved through core
strengthening exercises. Lastly, any asymmetry in strength should be resolved in order to
maintain balance (Myer et al., 2008).
Just as the form for shooting a basketball is a technique taught by a coach, athletic
maneuvers such as jumping and cutting should be similarly taught. The development of poor
habits at a young age like landing in an erect stance may exaggerate a female’s predisposition to
ACL injury when competition and intensity increase with age. Therefore, a prevention program
involving mainly plyometrics should be started before puberty in females in order to avoid poor
development of neuromuscular and biomechanical patterns. Ideally, the program should be able
to be easily taught and supervised by a coach. In order to increase the likelihood of participation
and adherence, it also should be enjoyable for youth girls. However, as a female enters into
puberty, the prevention program should intensify to account for strength deficits and/or
asymmetry.
CONCLUSION
The female athlete has a 4-6 times greater risk of suffering a noncontact ACL injury
while participating in the same sport as a male counterpart. Much research has produced
inconclusive evidence as to the reason for the gender disparity regarding injury. It is likely that
the disparity is multifactorial in nature, resulting from differences in anatomy, biomechanics,
neuromuscular control, genetics, and hormones amongst males and females. Because
biomechanical and neuromuscular patterns can be modified to a certain extent, ACL injury
prevention programs have targeted these risk factors. Ideally, prevention programs in females

20
should be initiated as soon as athletic participation begins in order to prevent maladaptive
athletic maneuvers that may put the athlete at risk. Hopefully, with the increased awareness of
the female disposition to ACL injuries, young female athletes will be encouraged to participate
in prevention programs, and the gender gap in injury rates will narrow.
Works Cited
21
Barber-Westin, Sue D., and Frank R. Noyes. ACL Injuries In The Female Athlete: Causes, Impacts, And Conditioning Programs. Dordrecht: Springer, 2012. Discovery eBooks. Web. 16 Oct. 2014.
Biering-Sorensen, F. “Physical Measurements as Risk Indicators for Low-Back Trouble over a One-Year Period.” Spine 9.2 (1984): 106-119.
Berns, G. S., M. L. Hull, and H. A. Patterson. "Strain in the Anteromedial Bundle of the Anterior Cruciate Ligament Under Combination Loading." Journal of Orthopaedic Research 10.2 (1992): 167-76. SCOPUS. Web. 25 Feb. 2015.
Boden, BP, Dean GS, Feagin JA Jr, Garrett WE Jr. “Mechanisms of Anterior Cruciate Ligament Injury.” Orthopedics. 26.6 (2000):573‐578.
Booth, F. W., and C. M. Tipton. “Effects of Training and 17-B Estradiol upon Heart Rates, Organ Weights, and Ligamentous Strength of Female Rats.” Internationale Zeitschrift Für Angewandte Physiologie, Einschliesslich Arbeitsphysiologie 27.3 (1969): 187–197. Print.
Endsley ML, Ford KR, Myer GD, Slauterbeck JR, Hewett TE. “The Effects of Gender on Dynamic Knee Stability and Q-angle in Young Athletes. Ohio Physical Therapy Association Fall Conference; Columbus, OH. 2003. Conference Presentation.
Fagenbaum, Ray, and Warren G. Darling. “Jump Landing Strategies in Male and Female College Athletes and the Implications of Such Strategies for Anterior Cruciate Ligament Injury.” The American Journal of Sports Medicine 31.2 (2003): 233–240. Print.
Fleming, B. C., et al. "The Effect of Weightbearing and External Loading on Anterior Cruciate Ligament Strain." Journal of Biomechanics 34.2 (2001): 163-70. SCOPUS. Web. 25 Feb. 2015.
Ford, Kevin R., et al. "Gender Differences in the Kinematics of Unanticipated Cutting in Young Athletes." Med Sci Sports Exerc 37.1 (2005): 124-129.
Gray, J., et al. "A Survey of Injuries to the Anterior Cruciate Ligament of the Knee in Female Basketball Players." International Journal of Sports Medicine 6.6 (1985): 314-6. SCOPUS. Web. 26 Feb. 2015.
Griffin, Letha Y. et al. “Noncontact Anterior Cruciate Ligament Injuries: Risk Factors and Prevention Strategies.” Journal of the American Academy of Orthopaedic Surgeons 8.3 (2000): 141–150. Print.
Haycock, CE, and Gillette, JV (1976). “Susceptibility of Women Athletes to Injury: Myth or Reality,” JAMA. 236: 163-165.

22
Heitz, N. A. et al. “Hormonal Changes throughout the Menstrual Cycle and Increased Anterior Cruciate Ligament Laxity in Females.” Journal of Athletic Training 34.2 (1999): 144–149. Print.
Hewett, Timothy E., Sandra J. Shultz, and Letha Y. Griffin. Understanding and Preventing Noncontact ACL Injuries. Champaign, IL: Human Kinetics, 2007. Print
Hewett, Timothy E., Gregory D. Myer, and Kevin R. Ford. “Anterior Cruciate Ligament Injuries in Female Athletes Part 1, Mechanisms and Risk Factors.” The American Journal of Sports Medicine 34.2 (2006): 299–311. ajs.sagepub.com. Web. 26 Feb. 2015.
Huston, L.J., Wojtys, E.M., “Neuromuscular Performance Characteristics in Elite Female Athletes.” American Journal of Sports Medicine. 24 (1996): 427–436.
Hutchinson MR, Ireland ML. “Knee Injuries in Female Athletes.” Sports Medicine. 19.4 (1995): 288–302.
Ireland, Mary Loyd. “The Female ACL: Why is it More Prone to Injury?” Orthopedic Clinics of North America. 33.4 (2002): 637-651.
Jackson, Douglas W., ed. The Anterior Cruciate Ligament: Current and Future Concepts. New York: Raven, 1993. Print.
Johnson, Jeffrey S. et al. “Gene Expression Differences Between Ruptured Anterior Cruciate Ligaments in Young Male and Female Subjects.” The Journal of Bone & Joint Surgery 97.1 (2015): 71–79. jbjs.org. Web. 25 Mar. 2015.
Karageanes, S. J., K. Blackburn, and Z. A. Vangelos. “The Association of the Menstrual Cycle with the Laxity of the Anterior Cruciate Ligament in Adolescent Female Athletes.” Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine 10.3 (2000): 162–168. Print.
Kiapour, A. M., and M. M. Murray. “Basic Science of Anterior Cruciate Ligament Injury and Repair.” Bone & Joint Research 3.2 (2014): 20–31.PMC. Web. 26 Feb. 2015.
LaPrade RF, Burnett QM. “Femoral Intercondylar Notch Stenosis and Correlation to Anterior Cruciate Ligament Injuries.” Am J Sports Med. 22.2 (1994):198–302.
Lebrun, C. M. et al. “Effects of Menstrual Cycle Phase on Athletic Performance.” Medicine and Science in Sports and Exercise 27.3 (1995): 437–444. Print.
Lephart, Scott M. et al. “The Role of Proprioception in the Management and Rehabilitation of Athletic Injuries.” The American Journal of Sports Medicine 25.1 (1997): 130–137. ajs.sagepub.com. Web. 26 Feb. 2015.
23
Lombardo, Stephen, Paul M. Sethi, and Chad Starkey. “Intercondylar Notch Stenosis Is Not a Risk Factor for Anterior Cruciate Ligament Tears in Professional Male Basketball Players An 11-Year Prospective Study.” The American Journal of Sports Medicine 33.1 (2005): 29–34. ajs.sagepub.com. Web. 26 Feb. 2015.
Malinzak, Robert A. et al. “A Comparison of Knee Joint Motion Patterns between Men and Women in Selected Athletic Tasks.” Clinical Biomechanics 16.5 (2001): 438–445. ScienceDirect. Web. 26 Feb. 2015.
Markolf, K. L., et al. "Direct Measurement of Resultant Forces in the Anterior Cruciate Ligament. an in Vitro Study Performed with a New Experimental Technique." Journal of Bone and Joint Surgery - Series A 72.4 (1990): 557-67. SCOPUS. Web. 25 Feb. 2015.
McLean, Scott G., Xuemei Huang, and Antonie J. van den Bogert. “Association between Lower Extremity Posture at Contact and Peak Knee Valgus Moment during Sidestepping: Implications for ACL Injury.”Clinical Biomechanics 20.8 (2005): 863–870. ScienceDirect. Web. 26 Feb. 2015.
Myer, Gregory D. et al. “Trunk and Hip Control Neuromuscular Training for the Prevention of Knee Joint Injury.” Clinics in sports medicine 27.3 (2008): 425–ix. PubMed Central. Web. 27 Feb. 2015.
Myer, Gregory D., Kevin R. Ford, and Timothy E. Hewett. “The Effects of Gender on Quadriceps Muscle Activation Strategies during a Maneuver That Mimics a High ACL Injury Risk Position.” Journal of Electromyography and Kinesiology 15.2 (2005): 181–189. ScienceDirect. Web. 26 Feb. 2015.
Myklebust, G. et al. “A Prospective Cohort Study of Anterior Cruciate Ligament Injuries in Elite Norwegian Team Handball.” Scandinavian Journal of Medicine & Science in Sports 8.3 (1998): 149–153. Print.
Nyland JA, Shapiro R, Caborn DN, Nitz AJ, Malone TR. “The Effect of Quadriceps Femoris, Hamstring, and Placebo Eccentric Fatigue on Knee and Ankle Dynamics during Crossover Cutting.” J Orthop Sports Physical Therapy. 25.3 (1997): 171–184.
Peterson, J.R., and B.J. Krabak. "Anterior Cruciate Ligament Injury. Mechanisms Of Injury And Strategies For Injury Prevention."Physical Medicine And Rehabilitation Clinics Of North America (2014): Scopus®. Web. 16 Oct. 2014.
Petersen, W, and T Zantop. "Anatomy of the Anterior Cruciate Ligament with Regard to its Two Bundles." Clinical Orthopaedics & Related Research 454.(2006): 35-47. CINAHL Complete. Web. 16 Oct. 2014.
24
Posthuma, B. W. et al. “Detecting Changes in Functional Ability in Women with Premenstrual Syndrome.” American Journal of Obstetrics and Gynecology 156.2 (1987): 275–278. Print.
Raschner, Christian et al. “The Relationship between ACL Injuries and Physical Fitness in Young Competitive Ski Racers: A 10-Year Longitudinal Study.” British Journal of Sports Medicine 46.15 (2012): 1065–1071. NCBI PubMed. Web.
Renstrom, P. et al. “Non-Contact ACL Injuries in Female Athletes: An International Olympic Committee Current Concepts Statement.” British Journal of Sports Medicine 42.6 (2008): 394–412. NCBI PubMed. Web.
Rozzi, Susan L. et al. “Knee Joint Laxity and Neuromuscular Characteristics of Male and Female Soccer and Basketball Players.” The American Journal of Sports Medicine 27.3 (1999): 312–319. Print.
Samuel, Chrishan S., Edna D. Lekgabe, and Ishanee Mookerjee. “The Effects of Relaxin on Extracellular Matrix Remodeling in Health and Fibrotic Disease.” Advances in Experimental Medicine and Biology 612 (2007): 88–103. NCBI PubMed. Web.
Sarwar, R, B B Niclos, and O M Rutherford. “Changes in Muscle Strength, Relaxation Rate and Fatiguability during the Human Menstrual Cycle.” The Journal of Physiology 493.Pt 1 (1996): 267–272. Print.
Seneviratne, Aruna et al. “The Effect of Estrogen on Ovine Anterior Cruciate Ligament Fibroblasts: Cell Proliferation and Collagen Synthesis.” The American Journal of Sports Medicine 32.7 (2004): 1613–1618. Print.
Shelbourne, K. Donald, Thorp J. Davis, and Thomas E. Klootwyk. “The Relationship Between Intercondylar Notch Width of the Femur and the Incidence of Anterior Cruciate Ligament Tears A Prospective Study.” The American Journal of Sports Medicine 26.3 (1998): 402–408. Print.
Silvers, Holly Jacinda, and Bert R Mandelbaum. “Prevention of Anterior Cruciate Ligament Injury in the Female Athlete.” British Journal of Sports Medicine 41.Suppl 1 (2007): i52–i59. PMC. Web. 26 Feb. 2015.
Slauterbeck, James et al. “Estrogen Level Alters the Failure Load of the Rabbit Anterior Cruciate Ligament.” Journal of Orthopaedic Research 17.3 (1999): 405–408. Web.
Strickland, Sabrina M. et al. “Lack of Hormonal Influences on Mechanical Properties of Sheep Knee Ligaments.” The American Journal of Sports Medicine 31.2 (2003): 210–215. Print.

25
Uhorchak, John M. et al. “Risk Factors Associated with Noncontact Injury of the Anterior Cruciate Ligament: A Prospective Four-Year Evaluation of 859 West Point Cadets.” The American Journal of Sports Medicine 31.6 (2003): 831–842. Print.
Withrow, Thomas J. et al. “The Effect of an Impulsive Knee Valgus Moment on in Vitro Relative ACL Strain during a Simulated Jump Landing.” Clinical Biomechanics 21.9 (2006): 977–983. ScienceDirect. Web. 26 Feb. 2015.
Wojtys, Edward M. et al. “The Effect of the Menstrual Cycle on Anterior Cruciate Ligament Injuries in Women as Determined by Hormone Levels.” The American Journal of Sports Medicine 30.2 (2002): 182–188. Print.
Yu, W. D. et al. “Effect of Estrogen on Cellular Metabolism of the Human Anterior Cruciate Ligament.” Clinical Orthopaedics and Related Research 366 (1999): 229–238. Print.
Zazulak, Bohdanna T. et al. “The Effects of Core Proprioception on Knee Injury A Prospective Biomechanical-Epidemiological Study.” The American Journal of Sports Medicine 35.3 (2007): 368–373.ajs.sagepub.com. Web. 26 Feb. 2015.
Zelisko, John A., H. Bates Noble, and Marianne Porter. “A Comparison of Men’s and Women’s Professional Basketball Injuries.” The American Journal of Sports Medicine 10.5 (1982): 297–299.ajs.sagepub.com. Web. 26 Feb. 2015.