Therapeutic Silencing of KRAS Using Systemically...
11
Small Molecule Therapeutics Therapeutic Silencing of KRAS Using Systemically Delivered siRNAs Chad V. Pecot 1 , Sherry Y. Wu 2 , Seth Bellister 3 , Justyna Filant 2 , Rajesha Rupaimoole 2 , Takeshi Hisamatsu 2 , Rajat Bhattacharya 3 , Anshumaan Maharaj 4 , Salma Azam 5 , Cristian Rodriguez-Aguayo 6,7 , Archana S. Nagaraja 2 , Maria Pia Morelli 8 , Kshipra M. Gharpure 2 , Trent A. Waugh 9 , Vianey Gonzalez-Villasana 6 , Behrouz Zand 2 , Heather J. Dalton 2 , Scott Kopetz 8 , Gabriel Lopez-Berestein 6,7,10 , Lee M. Ellis 3 , and Anil K. Sood 2,6,10 Abstract Despite being among the most common oncogenes in human cancer, to date, there are no effective clinical options for inhibiting KRAS activity. We investigated whether systemically delivered KRAS siRNAs have therapeutic potential in KRAS-mutated cancer models. We identified KRAS siRNA sequences with notable potency in knocking down KRAS expression. Using lung and colon adenocar- cinoma cell lines, we assessed antiproliferative effects of KRAS silencing in vitro. For in vivo experiments, we used a nanoliposomal delivery platform, DOPC, for systemic delivery of siRNAs. Various lung and colon cancer models were used to determine efficacy of systemic KRAS siRNA based on tumor growth, development of metastasis, and downstream signaling. KRAS siRNA sequences induced >90% knock- down of KRAS expression, significantly reducing viability in mutant cell lines. In the lung cancer model, KRAS siRNA treatment demonstrated significant reductions in primary tumor growth and distant metastatic disease, while the addition of CDDP was not additive. Significant reductions in Ki-67 indices were seen in all treatment groups, whereas significant increases in caspase-3 activity were only seen in the CDDP treatment groups. In the colon cancer model, KRAS siRNA reduced tumor KRAS and pERK expression. KRAS siRNAs significantly reduced HCP1 subcutaneous tumor growth, as well as out- growth of liver metastases. Our studies demonstrate a proof-of-concept approach to therapeutic KRAS targeting using nanoparticle delivery of siRNA. This study highlights the potential translational impact of therapeutic RNA interference, which may have broad applications in oncology, especially for traditional "undruggable" targets. Mol Cancer Ther; 13(12); 2876–85. Ó2014 AACR. Introduction Since its discovery over 30 years ago (1, 2), the KRAS proto-oncogene has remained the single most elusive cancer target. Despite the vast heterogeneity of all malig- nancies, mutational activation of the RAS GTPases (HRAS, NRAS, and KRAS) is present in approximately one third of all cancers (3). Although these small mono- meric GTPases are part of a superfamily of more than 150 members, direct mutation of other members is rare (4). Typically, RAS activation is catalyzed by guanine nucle- otide exchange factors (GEF) to a GTP-bound state, and subsequently hydrolyzed by GTPase-activating proteins (GAP) to its inactive, GDP-bound state. However, KRAS missense mutations in codons 12, 13, or 61 sterically interfere with GAP hydrolysis, leading to constitutive activation and promotion of many cancer hallmarks, such as cellular proliferation, survival, cytoskeletal reorgani- zation, and motility (5). Although valiant attempts have been made to develop pharmaceutical inhibitors of mutant KRAS-driven cancers, KRAS itself is still widely regarded as "undruggable." 1 Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas. 2 Department of Gynecologic Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas. 3 Department of Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas. 4 The University of Texas, Austin, Texas. 5 Curriculum in Genetics and Molecular Biology, University of North Car- olina, Chapel Hill, North Carolina. 6 Department of Cancer Biology, The University of Texas MD Anderson Cancer Center, Houston, Texas. 7 Depart- ment of Experimental Therapeutics, The University of Texas MD Anderson Cancer Center, Houston, Texas. 8 Department of Gastrointestinal Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas. 9 Lineberger Comprehensive Cancer Center, University of North Carolina, Chapel Hill, North Carolina. 10 Center for RNA Interference and Non-Coding RNA, The University of Texas MD Anderson Cancer Center, Houston, Texas. Note: Supplementary data for this article are available at Molecular Cancer Therapeutics Online (http://mct.aacrjournals.org/). Current address for C.V. Pecot: University of North Carolina Lineberger Comprehensive Cancer Center, Department of Medicine, Chapel Hill, North Carolina. Corresponding Author: Anil K. Sood, The University of Texas MD Ander- son Cancer Center, Unit 1362, PO Box 301439, Houston, TX 77230-1439. Phone: 713-745-5266; Fax: 713-792-7586; E-mail: [email protected] doi: 10.1158/1535-7163.MCT-14-0074 Ó2014 American Association for Cancer Research. Molecular Cancer Therapeutics Mol Cancer Ther; 13(12) December 2014 2876 on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074
Transcript of Therapeutic Silencing of KRAS Using Systemically...

Small Molecule Therapeutics
Therapeutic Silencing of KRAS Using Systemically DeliveredsiRNAs
Chad V. Pecot1, Sherry Y. Wu2, Seth Bellister3, Justyna Filant2, Rajesha Rupaimoole2, Takeshi Hisamatsu2,Rajat Bhattacharya3, Anshumaan Maharaj4, Salma Azam5, Cristian Rodriguez-Aguayo6,7,Archana S. Nagaraja2, Maria PiaMorelli8, KshipraM. Gharpure2, Trent A.Waugh9, VianeyGonzalez-Villasana6,Behrouz Zand2, Heather J. Dalton2, Scott Kopetz8, Gabriel Lopez-Berestein6,7,10, Lee M. Ellis3, andAnil K. Sood2,6,10
AbstractDespite being among the most common oncogenes in human cancer, to date, there are no effective
clinical options for inhibiting KRAS activity. We investigated whether systemically delivered KRAS
siRNAs have therapeutic potential in KRAS-mutated cancer models. We identified KRAS siRNA
sequences with notable potency in knocking down KRAS expression. Using lung and colon adenocar-
cinoma cell lines, we assessed antiproliferative effects of KRAS silencing in vitro. For in vivo experiments,
we used a nanoliposomal delivery platform, DOPC, for systemic delivery of siRNAs. Various lung and
colon cancer models were used to determine efficacy of systemic KRAS siRNA based on tumor growth,
development of metastasis, and downstream signaling. KRAS siRNA sequences induced >90% knock-
down of KRAS expression, significantly reducing viability in mutant cell lines. In the lung cancer model,
KRAS siRNA treatment demonstrated significant reductions in primary tumor growth and distant
metastatic disease, while the addition of CDDP was not additive. Significant reductions in Ki-67 indices
were seen in all treatment groups, whereas significant increases in caspase-3 activity were only seen in
the CDDP treatment groups. In the colon cancer model, KRAS siRNA reduced tumor KRAS and pERK
expression. KRAS siRNAs significantly reduced HCP1 subcutaneous tumor growth, as well as out-
growth of liver metastases. Our studies demonstrate a proof-of-concept approach to therapeutic KRAS
targeting using nanoparticle delivery of siRNA. This study highlights the potential translational impact
of therapeutic RNA interference, which may have broad applications in oncology, especially for
traditional "undruggable" targets. Mol Cancer Ther; 13(12); 2876–85. �2014 AACR.
IntroductionSince its discovery over 30 years ago (1, 2), the KRAS
proto-oncogene has remained the single most elusivecancer target. Despite the vast heterogeneity of all malig-nancies, mutational activation of the RAS GTPases(HRAS, NRAS, and KRAS) is present in approximatelyone third of all cancers (3). Although these small mono-meric GTPases are part of a superfamily of more than 150members, direct mutation of other members is rare (4).Typically, RAS activation is catalyzed by guanine nucle-otide exchange factors (GEF) to a GTP-bound state, andsubsequently hydrolyzed by GTPase-activating proteins(GAP) to its inactive, GDP-bound state. However, KRASmissense mutations in codons 12, 13, or 61 stericallyinterfere with GAP hydrolysis, leading to constitutiveactivation and promotion ofmany cancer hallmarks, suchas cellular proliferation, survival, cytoskeletal reorgani-zation, and motility (5). Although valiant attempts havebeen made to develop pharmaceutical inhibitors ofmutant KRAS-driven cancers, KRAS itself is still widelyregarded as "undruggable."
1Division of Cancer Medicine, The University of Texas MD AndersonCancer Center, Houston, Texas. 2Department of Gynecologic Oncology,The University of Texas MD Anderson Cancer Center, Houston, Texas.3Department of Surgical Oncology, The University of Texas MD AndersonCancer Center, Houston, Texas. 4The University of Texas, Austin, Texas.5Curriculum in Genetics and Molecular Biology, University of North Car-olina, Chapel Hill, North Carolina. 6Department of Cancer Biology, TheUniversity of TexasMDAndersonCancerCenter, Houston, Texas. 7Depart-ment of Experimental Therapeutics, The University of Texas MD AndersonCancer Center, Houston, Texas. 8Department of Gastrointestinal MedicalOncology, The University of Texas MD Anderson Cancer Center, Houston,Texas. 9Lineberger Comprehensive Cancer Center, University of NorthCarolina, Chapel Hill, North Carolina. 10Center for RNA Interference andNon-Coding RNA, The University of Texas MD Anderson Cancer Center,Houston, Texas.
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Current address for C.V. Pecot: University of North Carolina LinebergerComprehensiveCancerCenter, Department ofMedicine,ChapelHill, NorthCarolina.
Corresponding Author: Anil K. Sood, The University of Texas MD Ander-son Cancer Center, Unit 1362, PO Box 301439, Houston, TX 77230-1439.Phone: 713-745-5266; Fax: 713-792-7586; E-mail:[email protected]
doi: 10.1158/1535-7163.MCT-14-0074
�2014 American Association for Cancer Research.
MolecularCancer
Therapeutics
Mol Cancer Ther; 13(12) December 20142876
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

Since the first report of RNAi in 1998 (6), there has beenan explosion in efforts to use such a strategy for thera-peutic gain (7). Therapeutic RNAi is especially attractivebecause it enables silencing of cancer molecular targetsthat otherwise may not be inhibited using conventionalapproaches. Although competitive ATP kinase inhibitors(e.g., imatinib) or mAbs (e.g., trastuzumab) have revolu-tionized treatment of some cancers (8, 9), the lack of suchsuccess in KRAS targeting prompted us to investigatewhether RNAi has therapeutic potential for drug devel-opment. Here, we report a proof-of-concept study in lungand colon cancer preclinicalmodels that demonstrates theefficacy of KRAS silencing using nanoparticle-mediatedsiRNA delivery. In addition, we demonstrate in severalmodels that KRAS silencing in vivo can potently inhibitdevelopment of metastatic disease, the cause of death inapproximately 90% of patients with cancer (10).
Materials and MethodsCell lines, maintenance, and transfection reagentsAll cell lines were maintained in 5% CO2/95% air at
37�C.Lung (A549 andH1299) andovarian (RMUG-S) cellswere obtained from the ATCC and maintained in RPMI1640 supplemented with 10% FBS and 0.1% gentamicinsulfate (GeminiBioproducts). The A549-Luciferase cellline was made following stable transduction with lenti-virus carrying the luciferase gene (the lentiviral vectorwas kindly provided by Craig Logsdon’s lab). The HCP1colon cell lines were obtained from a human-derivedxenograft model at the M.D. Anderson Cancer Centerunder an Institutional Review Board–approved protocolas recently described (11). Cell lines were routinely testedto confirm the absence of Mycoplasma, and all in vitroexperiments were conducted with 60% to 80% confluentcultures. All cells were reverse-transfected with RNAi-Max reagent (Invitrogen) using siRNAmolecules (Sigma)at a final concentration of 10 to 20 nmol/L. Media werechanged 4 hours following transfections to minimizetoxicity. The siRNA sequences used for KRAS siRNAexperiments are as follows:
Negative control: sense UUCUCCGAACGUGUCACGUAntisense ACGUGACACGUUCGGAGAASeq #1: sense GUGCAAUGAAGGGACCAGUA,Antisense UACUGGUCCCUCAUUGCACSeq #2: sense GUCUCUUGGAUAUUCUCGA,Antisense UCGAGAAUAUCCAAGAGACSeq #3: Sense CAGCUAAUUCAGAAUCAUU,Antisense AAUGAUUCUGAAUUAGCUG.
Animals, in vivo models, and tissue processingFemale athymic nude mice were purchased from the
NCI, FrederickCancer Research andDevelopment Center(Frederick, MD). These animals were cared for accordingto guidelines set forth by the American Association forAccreditation of Laboratory Animal Care and the U.S.Public Health Service policy on Human Care and Use of
Laboratory Animals. All mouse studies were approvedand supervised by the M.D. Anderson Cancer CenterInstitutional Animal Care and Use Committee. All ani-mals usedwere between 8 to 12weeks of age at the time ofinjection. For all animal experiments, cells were trypsi-nized, washed, and resuspended in Hanks’ balanced saltsolution (HBSS; Gibco) before injection. For the orthotopiclung cancer model, A549-Luc cells were injected by anintrapulmonary technique [7.5� 105 in 100 mL 1:1mixtureof HBSS and BDMatrigel (BD Biosciences)] as previouslydescribed (12). For the intrapulmonary injections, micewere anesthetizedwith ketamineþxylazine andplaced inthe right lateral decubitus position. Following skin clean-ing with an alcohol swab, an incision parallel to the ribcage between ribs 10 and 11 was made to visualize thelung through the thorax.A 1-mL tuberculin syringewith a30-g needle was used to inject the cell suspension directlyinto the lung parenchyma at the left lateral dorsal axillaryline. After injection, the incision was closed using surgeryclips, and the mice were turned on the left lateral decu-bitus until fully recovered.
For both colon cancer models, 2.5 � 105 HCP1 cells permouse in 100mLHBSSwere either injected subcutaneouslyor intrasplenic (experimental liver metastases model). Inthe liver metastases model, mice were anesthetized underisofluorane for splenic isolation and cell line injection (day1), as well as the following day after injection (day 2) toperform splenectomy (11). Treatment continueduntilmicein any group became moribund (approximately 3 weeks).
For the A549 xenograft time-kinetic experiment used toassess for KRAS knockdown following siRNA delivery,2.5� 106A549parental cellswere injected subcutaneouslyinto athymic nude mice. Mice were randomly assigned toreceive either negative control (NC) siRNA or the com-bination of KRAS siRNAs Seq #2 and #3 (150 mg siRNA/kg/mouse). After 4 weeks of cell line injection, siRNAspacked in 1,2-dioleoyl-sn-glycero-3-phosphatidylcholine(DOPC) nanoliposomes were delivered intraperitoneally,and one tumor per group was obtained at 24, 48, and 96hours following a single delivery.
For all therapeutic experiments, mice were randomlydivided and assigned to their respective treatment groups(n¼ 10mice/group). A dose of 150 mg siRNA/kg/mousewas packaged within DOPC nanoliposomes and deliv-ered intraperitoneally at twice weekly intervals as previ-ously described (13). For the A549 lung cancer model,treatment began 10 days after cell line injection andcontinued for approximately 4 weeks. A 160 mg dose ofpharmaceutical grade cisplatin (CDDP; 1mg/mL concen-tration) was administered to respective groups onceweekly intraperitoneally.Weekly imagingwasperformedusing the Xenogen IVIS 200 system within 10 minutesfollowing injection of D-Luciferin (150 mg/mL). Livingimage 2.5 software was used to determine the regions ofinterest (ROI), andaveragephoton radiance (p/s/cm2/sr)was measured for each mouse.
For the subcutaneous colon cancer model, tumors weremonitoreduntil theymeasuredapproximately 100mm3, as
In Vivo KRAS Silencing with siRNA
www.aacrjournals.org Mol Cancer Ther; 13(12) December 2014 2877
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

determined using the following formula: volume¼ (L�W� W)/2, where L equals the greatest dimension of thetumorandWequals theperpendicularmeasurementof thetumor. Twice-weekly treatment began once tumorsmeasured approximately 100 mm3 and continued untiltumors in any group were approximately 15 mm in anydimension. In the time-kinetic experiment, 2 weeksfollowing HCP1 cell line injection into a total of 4 mice,micewere randomly assigned to receive eitherNC siRNA-DOPC or KRAS siRNA (Seq #3)-DOPC. After a singleinjection, mice in each group were sacrificed, and tumorswere snap frozenat 48and96hours following the injection.
In all experiments, once mice in any group becamemoribund, they were all sacrificed, necropsied, andtumors were harvested. Tumor weights, number, andlocation of tumor nodules were recorded. In the A549orthotopic lung cancer model, tumor volume was deter-minedusing calipers as follows: volume¼ (L�W�W)/2,where L equals the greatest dimension of the tumor andWequals the perpendicular measurement of the tumor.Tumor tissue was either fixed in formalin for paraffinembedding, frozen in optimal cutting temperature (OCT)media to prepare frozen slides, or snap frozen for lysatepreparation.
Liposomal nanoparticle preparationsiRNA for in vivo intratumor deliverywas incorporated
intoDOPC.DOPCand siRNAweremixed in the presenceof excess tertiary butanol at a ratio of 1:10 (w/w) siRNA/DOPC (Supplementary Fig. S1). Tween 20 was added tothemixture in a ratio of 1:19 Tween 20:siRNA/DOPC. Themixture was vortexed, frozen in an acetone/dry ice bath,and lyophilized. Before in vivo administration, this prep-aration was hydrated with PBS at room temperature at aconcentration of 150 mg siRNA/kg per injection (eachmouse received 200 mL of DOPC:siRNA:PBS solution bythe intraperitoneal route).
ImmunoblottingLysates from cultured cells were prepared using mod-
ified RIPA buffer [50 mmol/L Tris–HCl (pH 7.4), 150mmol/L NaCl, 1% Triton, 0.5% deoxycholate] plus 25mg/mL leupeptin, 10 mg/mL aprotinin, 2 mmol/L EDTA,and 1 mmol/L sodium orthovana. To prepare lysates ofsnap-frozen tissue frommice, approximately 30mm3 cutsof tissue were disrupted with a tissue homogenizer andcentrifuged at 13,000 rpm for 30 minutes within modifiedRIPA buffer. The protein concentrationswere determinedusing a BCAProteinAssayReagent kit (Pierce Biotechnol-ogy). Lysates (100 mg/lane)were loaded and separated on8% sodiumdodecyl sulfate–polyacrylamide gels. Proteinswere transferred to a nitrocellulosemembrane by semidryelectrophoresis (Bio-RadLaboratories) overnight, blockedwith 5% milk for 1 hour, and then incubated at 4�C withprimary antibody [KRAS, 1:500, Abcam ab81075 (celllysates); KRAS, 1:500, Santa Cruz SC-30 (tumor lysates);pERK1/2, 1:1,000, Cell Signaling (4695); ERK1/2, 1:1,000,Cell Signaling (4376); pMEK1/2, 1:1,000, Cell Signaling
(2338); MEK1/2, 1:1,000, Cell Signaling (4694); Vinculin,1:1,000, Santa Cruz SC-25336] overnight. After washingwithTBST, themembraneswere incubatedwithhorserad-ish peroxidase (HRP)–conjugated horse anti-mouse IgG(1:2,000;GEHealthcare)for2hours.HRPwasvisualizedbyuse of an enhanced chemiluminescence detection kit(Pierce). To confirm equal sample loading, the blots wereprobed with an antibody specific for Vinculin. Densitom-etry was calculated using ImageJ software.
Quantitative real-time PCRFor mRNA quantification, total RNA was isolated
by using a Qiagen RNeasy kit. Using 500 ng of RNA,cDNA was synthesized by using a Verso cDNA kit(ThermoScientific) as per themanufacturer’s instructions.Analysis of mRNA levels was performed on a 7500 FastReal-Time PCR System (Applied Biosystems) with SYBRGreen–based real-time PCR. Specific primers for KRASF-TGACCTGCTGTGTCGAGAAT, R-TTGTGGACGAA-TATGATCCAA; 18S F-CGCCGCTAGAGGTGAAATTC,R-TTGGCAAATGCTTTCGCTC were used; 18S rRNAwas used as a housekeeping gene. PCR was done withreverse-transcribed RNA and 100 ng/mL of sense andantisense primers in a total volume of 20 mL. Each cycleconsisted of 15 seconds of denaturation at 95�C and 1minute of annealing and extension at 60�C (40 cycles).
Cell viability assayCell viability assays were performed by testing cell’s
ability to reduce the tetrazolium salt [3-(4,5-dimethylthia-zol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt] to a formazan. Briefly, cellswere seeded in a 96-well plate and were reverse trans-fected with either NC siRNA, KRAS siRNA (Seq #1, Seq#2, Seq #3 or the combination of Seq #2þ#3). At 24, 48, 72,96, and 120 hours following transfection, cells were incu-bated with 0.15% 3-(4,5-dimethylthiazol-2-yl)-2,5-diphe-nyltetrazolium bromide (MTT) for 2 hours at 37�C. In theA549 experiment, 10 to 20 nmol/L of siRNA was used asindicated, and in the H1299 and RMUG-S cell lines, 20nmol/L siRNAwas used. The supernatant was removed,cells were dissolved in 100-mLDMSO, and the absorbanceat 570 nm was recorded.
ImmunostainingStaining was performed in formalin-fixed, paraffin-
embedded tumor sections (8 mm thickness) or fromOCT-embedded frozen tissue sections. After deparaffini-zation, rehydration, and antigen retrieval or fixation, 3%H2O2was used to block the endogenous peroxidase activ-ity for 10 minutes. Protein blocking of nonspecific epi-topes was done using either 5% normal horse serum,1% normal goat serum, or 2.8% fish gelatin in PBS for20 minutes. Slides were incubated with primary antibodyfor Ki-67 (rabbit anti-mouse, 1:200, Abcam ab15580) orcleaved caspase-3 (BioCare Medical, 1:100) overnight at4�C. Terminal deoxynucleotidyl transferase-mediateddeoxyuridine triphosphate nick-end labeling (TUNEL)
Pecot et al.
Mol Cancer Ther; 13(12) December 2014 Molecular Cancer Therapeutics2878
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

stainingwasperformedusing thePromegaKit (Promega),and CD31 staining to assess microvessel density wasperformed as previously described (12, 14). For immuno-histochemistry, after washing with PBS, the appropriateamount of HRP-conjugated secondary antibody wasadded and visualized with 3,30-diaminobenzidine chro-mogen and counterstained with Gill’s hematoloxylin #3.Light field images were obtained using a Nikon Micro-phot-FXA microscope and Leica DFC320 digital camera.Proliferation and apoptotic indices were determinedusing 6 to 10 representative fields at �200 magnificationfor each tumor, whereas microvessel density was deter-mined at �100 magnification (5 tumors per group). Ki-67and cleaved caspase-3–positive cells per high-poweredfield were enumerated using Cell Profiler 2.0 software,whereas TUNEL-positive cells per high-powered fieldwere enumerated manually (15). Quantification was per-formed in a blinded fashion.
Statistical analysisFor animal experiments, 10 mice were assigned per
treatment group. This sample size provided 80% powerto detect a 50% reduction in tumor mass with 95%confidence. Mouse and tumor weights and the numberof tumor nodules for each group were compared usingthe Student t test (for comparisons of two groups) andthe ANOVA (for multiple group comparisons). Forvalues that were not normally distributed (as deter-mined by the Kolmogrov–Smirnov test), the Mann–Whitney rank sum test was used. A P value �0.05 wasdeemed statistically significant. All statistical tests weretwo-sided and were performed using GraphPad Prism6.0.
ResultsSelection of potent KRAS siRNA sequencesTo test the efficacy of KRAS silencing in vivo, we first
searched for siRNA sequences that potently inhibit KRASexpression regardless of the specificmissensemutation atcodons 12, 13, or 61. Low concentrations (20 nmol/L) oftwo siRNA sequences (Seq #2 and Seq #3) within thecoding sequence were found to inhibit KRAS mRNAexpression in mutant (A549 lung adenocarcinoma,KRASG12S) and wild-type (RMUG-S ovarian carcinoma)cell lines (Fig. 1A and B). Western blot analyses furtherconfirmed greater than 90% knockdown of KRAS proteinin mutant (A549) andwild-type (H1299, RMUG-S) cancercell lines (Fig. 1C). Compared with NC siRNA, a singletransfection of Seq #2 or Seq #3 siRNAs significantlyinhibited cell viability in the A549 cell line, but not in thewild-type cells (Fig. 1D), suggesting attenuated growth isnot due to off-target effects of the siRNA sequences and isconsistent with A549 having a KRAS oncogene "addic-tion" (16). Furthermore, the combination of Seq #2 and Seq#3 at low concentrations (10 nmol/L or 20 nmol/L) led tosubstantial reductions in cell viability (Fig. 1D). As com-pared with H1299, KRAS siRNA sequences #2 and #3 in
A549 led to marked reductions in pERK and pMEK,molecules involved in the downstream signaling of theMAPK pathway (Fig. 1E).
Therapeutic efficacy of KRAS siRNAs in a lungcancer model
Using our well-characterized DOPC nanoliposomes(Supplementary Fig. S1; ref. 13), we have recently dem-onstrated highly effective systemic delivery of oligonu-cleotides in orthotopic lung cancer models (12). Throughexploitation of the enhanced-permeability and retention(EPR) effect (7), we also demonstrated the ability tosystemically deliver siRNAs to metastatic lesions (12).Thus, for all in vivo experiments, we assessed therapeuticefficacy of KRAS targeting with DOPC-mediated siRNAdelivery.
Wefirst assessedwhether systemically deliveredKRASsiRNAs can knock down KRAS expression in vivo. Fourweeks following subcutaneous injection of 2.5� 106 A549cells, compared with NC siRNA, following a single injec-tion of KRAS siRNAs Seq #2 and #3, A549 tumors hadsustained knockdown of KRAS protein expression for upto 96hours (Fig. 2A).Wehavepreviously observed similarpatterns of knockdown with other targets, with reboundtypically occurring around 5 to 6 days after delivery(13, 17). Next, to evaluate longitudinal effects of KRASsiRNA treatment, we used luciferase-labeledA549 (A549-Luc) cells to enable IVIS imaging. Furthermore, becausecisplatin (CDDP) is the backboneof lung cancer treatment,we assessed whether chemotherapy and KRAS targetingwould have enhanced antitumor effects. In addition toprimary tumors, this model demonstrated the ability toform mediastinal lymph node and chest wall metastases(Fig. 2B).
One week following orthotopic injection of 7.5 � 105
A549-Luc cells, mice were randomly assigned to thefollowing treatment groups (n ¼ 10 mice/group): (i) NCsiRNA-DOPC, (ii) KRAS siRNA-DOPC, (iii) NC siRNA-DOPCþCDDP, and (iv) KRAS siRNA-DOPCþCDDP. Forthe KRAS siRNA treatment groups, Seq #2 and Seq #3were combined. For theCDDP treatment groups, 160mgofCDDP was given intraperitoneally once weekly. Oneweek after cell line injection, twice-weekly treatmentcommenced and weekly imaging was performed (Fig.2C). Following fourweeks of systemic therapy, comparedwith control siRNA treatment, mice in the KRAS siRNAtreatment group had an 81% reduction in luminescence (P< 0.01), whereas the addition of CDDP did not lead tosignificant reductions in the NC siRNAþCDDP or KRASsiRNAþCDDP groups (Fig. 2D and E). Longitudinalassessments of luciferase activity demonstrated signifi-cant growth inhibition from KRAS siRNA treatment (Fig.2F), and rapid disease progression during the last week oftreatment was significantly attenuated as compared withNC siRNA (Fig. 2G). Following four weeks of treatment,all mice were sacrificed, and an extensive necropsy ofgross tumor burden was quantified. As compared withcontrol siRNA, significant reductions in primary tumor
In Vivo KRAS Silencing with siRNA
www.aacrjournals.org Mol Cancer Ther; 13(12) December 2014 2879
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

size (KRAS siRNA: 50%, P ¼ 0.003; NC siRNAþCDDP:6%, P ¼ 0.24; KRAS siRNAþCDDP: 73%, P ¼ 0.008) andaggregate mass of distant metastases (KRAS siRNA: 77%,P ¼ 0.0002; NC siRNAþCDDP: 11%, P ¼ 0.85; KRASsiRNAþCDDP: 74%, P ¼ 0.009) were only observed inthe KRAS siRNA treatment groups (Fig. 2H and I andSupplementary Fig. S2). The number of distantmetastaseswas only significantly decreased in the KRAS siR-NAþCDDP group (Fig. 2J). Intriguingly, only the KRASsiRNA treatment groups had significantly less frequent
mediastinal metastases, whereas NC siRNAþCDDP didnot (Fig. 2K). Taken together, systemically deliveredKRAS siRNAs demonstrated significant therapeuticactivity on the primary tumor as well as control of met-astatic spread, while the addition of cytotoxic chemother-apy was not additive.
To further assess the biologic effects of systemic KRASsiRNA treatment, we stained the tumor samples for pro-liferation, apoptosis, and angiogenesis markers. Com-pared with control siRNA, significant increases in
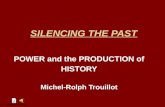
Figure 1. Selection of KRAS siRNAsequences and inhibition ofproliferation in a mutant cell line.A, relative knockdown of KRASmRNA following transfection ofKRAS-mutant (A549; G12S) andwild-type (RMUG-S) cell lines using20 nmol/L siRNA. B, mature mRNAKRAS map demonstrating thebinding sites of the selected KRASsiRNA Seq #1, #2, and #3 (red) inrelation to the region of G12 and13 codon mutations. (Note: blackdesignates the coding sequence,CDS). C, Western blots for KRAS(top) and b-actin (bottom) 48 hoursfollowing transfection of NC siRNAor KRAS siRNAs Seq #2 and #3.D, MTT viability assays followingtransfection of KRAS mutant andwild-type cell lines. A549 wastransfected with either NC siRNA,KRAS siRNAs Seq #1, #2, #3 orboth Seq #2 and #3 (all at 10 nmol/L) or both Seq #2 and #3 (at20 nmol/L), as indicated.H1299 and RMUG-S cell linesweretransfected with 20 nmol/L ofsiRNA. E, Western blot analyses ofA549 and H1299 cell lines 48 hoursfollowing transfection with 20nmol/L of the respective siRNA.���, P < 0.0001.
Pecot et al.
Mol Cancer Ther; 13(12) December 2014 Molecular Cancer Therapeutics2880
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

caspase-3 activity and TUNEL staining were observed inall treatment groups, with the greatest effects seen in theKRAS siRNAþCDDP group (Fig. 3A and B). Comparedwith control siRNA, significant reductions inKi-67 indiceswere seen in all treatment groups (KRAS siRNA: 34%;NCsiRNAþCDDP: 52%; KRAS siRNAþCDDP: 36%; all P <0.0001; Fig. 3C). Also, compared with control siRNA, alltreatment groups had significant reductions in microves-sel density (KRAS siRNA: 61%; NC siRNAþCDDP: 55%;KRAS siRNAþCDDP: 76%; all P < 0.001; Fig. 3D). Com-paredwithNC siRNAþCDDP, KRAS siRNAþCDDPhad
a 45% reduction in microvessel density (P < 0.05, Fig. 3D).These data indicate that in vivo silencing of KRAS intumors leads to induction of apoptosis and inhibition ofproliferation and angiogenesis. Although the combina-tion of KRAS siRNA with cisplatin had additive biologiceffects on the tumors (Fig. 3A–D), there were no appreci-able effects on overall disease burden at the time ofnecropsy. Although these findings suggest combiningKRAS silencing and cisplatin may not have additivetherapeutic effects, the dose chosen may have beensubtherapeutic.
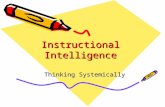
Figure 2. Therapeutic efficacy ofKRAS siRNA delivery in a lungcancer model. A, A549 tumorexpression of KRAS at 24, 48, and96 hours following a single deliveryof either NC siRNA or KRAS siRNA(Seq#2þ #3); n¼ 3mice/treatmentgroup. B, representativemetastatic mediastinal lymph node(dotted circle) and chest wall (whitearrows) metastatic lesions of theorthotopic A549 lung cancermodel. C, schematic of orthotopicA549-Luc cell line injectionfollowed by imaging and treatmentintervals. D, representativeluminescent images of tumor-bearing mice after the fourth weekof treatment. E, averageluminescence by treatment groupfollowing four weeks of treatment.F, longitudinal luminescent signalsfor each treatment group. G, deltaof photon radiance during the lastweek of treatment for eachtreatment group.H, greatest cross-sectional dimension of the primarytumor (in mm); I, total aggregatemass of metastatic burden (ingrams); and J, total number ofmetastatic lesions for eachtreatment group. For allexperiments, eachmouse received150 mg siRNA/kg/mouse dissolvedin 200 mL of PBS by theintraperitoneal route. For thetherapeutic experiment, twice-weekly siRNA injections weregiven. Cisplatin (CDDP) was givenonce weekly by intraperitonealinjection at a dose of 160 mg/mouse. n ¼ 10 mice per group;all measurements demonstratemean � SEM; P values calculatedusing the Student t test. K,frequency of mediastinalmetastases by treatment group. Pvalue was determined using the c2
test. �, P < 0.05; ��, P < 0.01; and���, P < 0.001.
In Vivo KRAS Silencing with siRNA
www.aacrjournals.org Mol Cancer Ther; 13(12) December 2014 2881
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

Biologic effects of KRAS siRNA in colon cancermodels
Next, using a recently characterized patient-derivedcolon cancer cell line with a KRASG12D mutation (11),HCP1, we assessed whether downstream mediators ofKRAS signaling are abrogated following KRAS siRNA .
treatment. Three weeks after early passage HCP1 subcu-taneous tumors were created, mice were randomlyassigned to receive a single injection of either NCsiRNA-DOPC or KRAS siRNA-DOPC. Similar to before(Fig. 2C), at both 48- and 96-hour timepoints, clear reduc-tions inKRASandpERKsignaling (Fig. 4A)wereobserved.
Nu
mb
er K
i67
cells
/hp
fN
um
ber
mic
rove
ssel
s/h
pf
NC siRNA KRAS siRNA NC siR+CDDP KRAS siR+CDDP
Nu
mb
er C
C3
cells
/hp
fN
um
ber
TU
NE
L+
cells
/hp
f
A
D
C
B
NC siRNA
KRAS siRNA
KRAS siRNA +
CDDP
NC siRNA +
CDDP
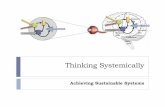
Figure 3. Biologic indices following KRAS siRNA and/or cisplatin treatment in a lung cancer model. Paraffin-embedded A549 tumors at the end of treatmentwere stained for cleaved caspase-3 (A) or TUNEL (B) to assess for apoptosis. C, staining for Ki-67was used to assess for proliferation indices. All imagesweretaken at�200magnification. D, CD-31 stainingwas performed to assess formicrovessel density. All imageswere taken at�100magnification. For all biologicindices, 5 to 10 representative images per tumor were obtained; n ¼ 5 tumors per group. All measurements demonstrate mean � SEM; P values werecalculated using the Student t test. �, P < 0.05; ��, P < 0.01; and ���, P < 0.001.
Pecot et al.
Mol Cancer Ther; 13(12) December 2014 Molecular Cancer Therapeutics2882
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

Next, we assessed whether systemic KRAS siRNAcould inhibit tumor growth in a colon cancer model.Following subcutaneous injection of 2.5� 105 HCP1 cells,tumors weremonitored until reaching approximately 100mm3. Mice were randomly assigned to the followingtreatment groups (n ¼ 10 mice/group): (i) NC siRNA-DOPC or (ii) KRAS siRNA-DOPC. Twice-weekly treat-ments were given and tumor volumetric assessmentswere made with calipers every three days. As soon asone week after treatment, significant reduction in tumorgrowth was noted in the KRAS siRNA-DOPC group, andfollowing two weeks of treatment, tumors were 68.6%smaller (P ¼ 0.033) than the NC siRNA group (Fig. 4B).Because the predominant site of distant metastasis in
patients with colon cancer is the liver, we assessedwheth-er KRAS siRNA would be effective in an experimentalmetastasis model. Splenectomy was performed one dayfollowing intrasplenic injection of 2.5 � 105 HCP1 cells,andmicewere randomly assigned to the following groups(n ¼ 10 mice/group): (i) NC siRNA-DOPC or (ii) KRASsiRNA-DOPC. As before, for the KRAS siRNA treatmentgroups, Seq #2 and Seq #3 were combined. Systemictreatment began 5 days following cell line injection andcontinued until mice in either group became moribund(22 days). Following nearly 3 weeks of treatment, KRASsiRNA led to a 73% reduction in aggregate metastaticdisease (P¼ 0.014; Fig. 4C) and a trend toward a reductionin the number of gross metastatic liver lesions (P ¼0.09; Fig. 4D and E). Notably, no mice in any of thetherapeutic experiments exhibited any overt signs of
toxicity from KRAS siRNA treatment, such as decreasedfeeding habits, activity, or total body weight. Takentogether, systemically delivered KRAS siRNAs signifi-cantly inhibited primary tumor growth and outgrowthof distant metastases in lung and colon cancer modelsdriven by mutant KRAS.
DiscussionMultiple approaches have been attempted to target
mutant RAS signaling; however, to date, no pharmaco-logic inhibitors are currently in clinical use. Although theability to develop ATP-competitive inhibitors with nano-molar affinities has led to clinical efficacy (8), the lowpicomolar binding affinity of small GTPases for GTP andmilimolar cellular concentrations of GTP make thisapproach far less feasible (4). Furthermore, the conforma-tional changes following substitution of glycine (onlyamino acid without a side chain) for other residues in the"finger loop" sterically interferes with GAP activity, mak-ing development of GAP-mimics unlikely (18). Althoughtargeting the prenylation process of KRAS with farnesyltransferase inhibitors showed initial preclinical promise(19), enthusiasm was dampened by lack of efficacy inclinical trials (20). Most recent efforts have turned towardsynthetic-lethality approaches as well as targeting ofdownstream signaling mediators of KRAS pathways(21, 22). Although such approaches have shown preclin-ical efficacy (23), compensatory mechanisms, toxicityfrommultiple inhibitors, andultimately efficacy in clinicaltrials are important hurdles that remain.
Figure 4. Time-kinetics andtherapeutic efficacy of KRASsiRNA in a colon cancer model.A, Western blot demonstratingeffects of a single KRAS siRNAtreatment on KRAS protein anddownstream pERK signaling 48and 96 hours following delivery insubcutaneous HCP1 tumors,n ¼ 2 mice/treatment group. B,effects of KRAS siRNA on tumorgrowth in a colon cancer model(HCP1) based on tumor volume.C, following injection of HCP1 cellsinto the spleen, mice wererandomized and assigned to eitherNC siRNA or KRAS siRNA (Seq #2and #3) treatment. Followingapproximately 3 weeks oftreatment, aggregate burden ofmetastatic disease and totalnumber of liver metastases (D)were assessed. E, representativetumors from NC siRNA and KRASsiRNA treatment groupsdemonstrating liver metastases attime of necropsy. n ¼ 10 mice/group; all measurementsdemonstrate mean � SEM;P values were calculated using theStudent t test (�, P < 0.05).
In Vivo KRAS Silencing with siRNA
www.aacrjournals.org Mol Cancer Ther; 13(12) December 2014 2883
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

Using mutant KRAS models of lung and colon cancer,we demonstrate the therapeutic potential of systemicallydelivered RNAi as a novel treatment modality. Althoughtherapeutic effects were seen through decreased down-stream signaling and inhibition of proliferation, we alsoobserved significant decreases in the frequency and bur-den of distant metastases. KRAS siRNA delivery as atherapeutic approach has many characteristics that makeit desirable for further drug development. First, so far thefirst-in-human clinical trials using nanoparticle-mediatedsiRNA delivery have been safe, well tolerated, and insome cases have led to complete pathologic responses inmetastatic disease (24, 25). Second, although in this proof-of-concept study, siRNAsequences that targeted all formsof mutant KRAS (and wild-type) were used, siRNAsequences that preferentially target only the mutant allelecould be developed, thus theoretically avoiding toxicityfrom targeting the wild-type protein in normal tissues.Lastly, although other current approaches rely uponblocking the effects of mutant KRAS, whose downstreammediators consist of a highly complex circuitry, use ofRNAi aims at eliminating the functional capstone, KRASitself. Although therapeutic RNAi has important chal-lenges of its own, such as developing targeted platformsthat are biocompatible and potently inhibit target expres-sion, the field is rapidly moving forward and turning thisapproach into a reality (7).
Disclosure of Potential Conflicts of InterestL.M. Ellis is a consultant/advisory board member for Genentech/
Roche, ImClone/Lilly and Amgen. No potential conflicts of interest weredisclosed by the other authors.
Authors' ContributionsConception and design: C.V. Pecot, S.Y. Wu, H.J. Dalton, G. Lopez-Berestein, L.M. Ellis, A.K. SoodDevelopment of methodology: C.V. Pecot, S.Y. Wu, C. Rodriguez-Aguayo, V. Gonzalez-Villasana, A.K. SoodAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): C.V. Pecot, S.Y. Wu, J. Filant, R. Rupaimoole,
T. Hisamatsu, R. Bhattacharya, A. Maharaj, S. Azam, C. Rodriguez-Aguayo, T.A.Waugh, B. Zand, H.J. Dalton, S. Kopetz, G. Lopez-Berestein,A.K. SoodAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis):C.V. Pecot, S.Y.Wu, J. Filant, A.S. Nagaraja,K.M. Gharpure, V. Gonzalez-Villasana, S. Kopetz, G. Lopez-Berestein,A.K. SoodWriting, review, and/or revision of the manuscript: C.V. Pecot, S.Y. Wu,R. Bhattacharya, A.S. Nagaraja, M.P. Morelli, K.M. Gharpure, H.J. Dalton,S. Kopetz, G. Lopez-Berestein, L.M. Ellis, A.K. SoodAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): C.V. Pecot, S. Bellister, T.A.Waugh,A.K. SoodStudy supervision: C.V. Pecot, M.P. Morelli, G. Lopez-Berestein,L.M. Ellis, A.K. Sood
AcknowledgmentsThe authors thank Donna Reynolds for expertise in
immunohistochemistry.
Grant SupportPortions of this work were supported by the NIH (CA016672,
CA109298, P50 CA083639, P50 CA098258, CA128797, U54 CA151668,CA177909, and U24CA143835), the Cancer Prevention Research Instituteof Texas (RP110595), the Ovarian Cancer Research Fund, Inc. (ProgramProject Development Grant), the Department of Defense (OC073399,W81XWH-10-1-0158), the RGK Foundation, the Gilder Foundation, theBlanton-Davis Ovarian Cancer Research Program, and the Betty AnneAscheMurray Distinguished Professorship (to A.K. Sood). C.V. Pecot wassupported by a grant from theNCI (T32 training grant CA009666), the 2011Conquer Cancer Foundation ASCO Young Investigator Award, the Ben F.Love Fellowship in Innovative Cancer Therapies, the Jeffrey Lee CousinsFellowship in Lung Cancer Research, and the DoCM Advanced ScholarProgram. S.Y. Wu was supported by Ovarian Cancer Research Funds,Foundation for Women’s Cancer, and Cancer Prevention Research Insti-tute of Texas training grants (RP101502 and RP101489). S. Kopetz was inpart supported byNIHgrant CA172670. S. Azamwas supported in part bya grant from the National Institute of General medical Sciences underaward 5T32 GM007092. L.M. Ellis was in part supported by NIH grantR01CA157880, DOD CA100879, and the William C. Liedtke, Jr., Chair inCancer Research.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received January 27, 2014; revised September 2, 2014; acceptedSeptember 19, 2014; published OnlineFirst October 3, 2014.
References1. Shih C, Padhy LC, Murray M, Weinberg RA. Transforming genes of
carcinomas and neuroblastomas introduced into mouse fibroblasts.Nature 1981;290:261–4.
2. Shih C, Weinberg RA. Isolation of a transforming sequence from ahuman bladder carcinoma cell line. Cell 1982;29:161–9.
3. Downward J. Targeting RAS signalling pathways in cancer therapy.Nat Rev Cancer 2003;3:11–22.
4. Vigil D, Cherfils J, Rossman KL, Der CJ. Ras superfamily GEFs andGAPs: validated and tractable targets for cancer therapy? Nat RevCancer 2010;10:842–57.
5. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation.Cell 2011;144:646–74.
6. Fire A, Xu S, Montgomery MK, Kostas SA, Driver SE, Mello CC. Potentand specific genetic interference by double-stranded RNA in Caenor-habditis elegans. Nature 1998;391:806–11.
7. Pecot CV, Calin GA, Coleman RL, Lopez-Berestein G, Sood AK. RNAinterference in the clinic: challenges and future directions. Nat RevCancer 2011;11:59–67.
8. Druker BJ, Guilhot F, O'Brien SG, Gathmann I, Kantarjian H,Gattermann N, et al. Five-year follow-up of patients receivingimatinib for chronic myeloid leukemia. N Engl J Med 2006;355:2408–17.
9. Smith I, ProcterM,GelberRD,GuillaumeS,FeyereislovaA,DowsettM,et al. 2-year follow-up of trastuzumab after adjuvant chemotherapy inHER2-positive breast cancer: a randomised controlled trial. Lancet2007;369:29–36.
10. Gupta GP,Massagu�e J. Cancermetastasis: building a framework. Cell2006;127:679–95.
11. Lu J, Ye X, Fan F, Xia L, Bhattacharya R, Bellister S, et al.Endothelialcells promote the colorectal cancer stem cell phenotype through asoluble form of Jagged-1. Cancer Cell 2013;23:171–85.
12. Pecot CV, Rupaimoole R, YangD, Akbani R, IvanC, LuC, et al. Tumourangiogenesis regulation by the miR-200 family. Nat Commun2013;4:2427.
13. Landen CN Jr, Chavez-Reyes A, Bucana C, Schmandt R, Deavers MT,Lopez-Berestein G, et al. Therapeutic EphA2 gene targeting in vivousing neutral liposomal small interfering RNA delivery. Cancer Res2005;65:6910–8.
14. ShahzadMM, LuC, Lee JW, Stone RL,Mitra R,Mangala LS, et al. Dualtargeting of EphA2 and FAK in ovarian carcinoma. Cancer Biol Ther2009;8:1027–34.
15. Lamprecht MR, Sabatini DM, Carpenter AE. CellProfiler: free, versatilesoftware for automated biological image analysis. Biotechniques2007;42:71–5.
Pecot et al.
Mol Cancer Ther; 13(12) December 2014 Molecular Cancer Therapeutics2884
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

16. Singh A, Settleman J. Oncogenic K-ras "addiction" and syntheticlethality. Cell Cycle 2009;8:2676–7.
17. Halder J, Kamat AA, Landen CN Jr, Han LY, Lutgendorf SK, Lin YG,et al. Focal adhesion kinase targeting using in vivo short interferingRNA delivery in neutral liposomes for ovarian carcinoma therapy.Clinical Cancer Res 2006;12:4916–24.
18. MalumbresM, BarbacidM. RASoncogenes: the first 30 years. Nat RevCancer 2003;3:459–65.
19. Kohl NE, Omer CA, Conner MW, Anthony NJ, Davide JP, deSolms SJ,et al. Inhibition of farnesyltransferase induces regression of mammaryand salivary carcinomas in ras transgenic mice. Nat Med 1995;1:792–7.
20. SharmaS,KemenyN,KelsenDP, IlsonD,O'Reilly E, ZaknoenS, et al. Aphase II trial of farnesyl protein transferase inhibitor SCH 66336, givenby twice-daily oral administration, in patients with metastatic colorec-tal cancer refractory to 5-fluorouracil and irinotecan. Ann Oncol2002;13:1067–71.
21. Barbie DA, Tamayo P, Boehm JS, Kim SY, Moody SE, Dunn IF, et al.Systematic RNA interference reveals that oncogenic KRAS-drivencancers require TBK1. Nature 2009;462:108–12.
22. Young A, Lyons J, Miller AL, Phan VT, Alarcon IR, McCormick F. Rassignaling and therapies. Adv Cancer Res 2009;102:1–17.
23. Engelman JA, Chen L, Tan X, Crosby K, Guimaraes AR, Upadhyay R,et al. Effective use of PI3K and MEK inhibitors to treat mutant KrasG12D and PIK3CA H1047R murine lung cancers. Nat Med2008;14:1351–6.
24. Davis ME, Zuckerman JE, Choi CH, Seligson D, Tolcher A, AlabiCA, et al. Evidence of RNAi in humans from systemically admin-istered siRNA via targeted nanoparticles. Nature 2010;464:1067–70.
25. Tabernero J, Shapiro GI, LoRusso PM, Cervantes A, Schwartz GK,Weiss GJ, et al. First-in-humans trial of an RNA interference thera-peutic targeting VEGF and KSP in cancer patients with liver involve-ment. Cancer Discov 2013;3:406–17.
www.aacrjournals.org Mol Cancer Ther; 13(12) December 2014 2885
In Vivo KRAS Silencing with siRNA
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074

2014;13:2876-2885. Published OnlineFirst October 3, 2014.Mol Cancer Ther Chad V. Pecot, Sherry Y. Wu, Seth Bellister, et al. siRNAsTherapeutic Silencing of KRAS Using Systemically Delivered
Updated version
10.1158/1535-7163.MCT-14-0074doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2014/10/04/1535-7163.MCT-14-0074.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/13/12/2876.full#ref-list-1
This article cites 25 articles, 3 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/13/12/2876.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/13/12/2876To request permission to re-use all or part of this article, use this link
on June 24, 2018. © 2014 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 3, 2014; DOI: 10.1158/1535-7163.MCT-14-0074