
Therapeutic Exercises DERMOT check list.ppt · 4. How should exercises be implemented as part of a...
70
Treatment2Go Exploring Hand Therapy Manual Therapeutic Exercises An Upper Extremity Regime Exploring Hand Therapy, Corporation d/b/a Treatment2Go www.handtherapy.com www.treatment2go.com 727-341-1674 Fax: 888-2704079 Treatment2Go is a trademark and d/b/a of Exploring Hand Therapy.
Transcript of Therapeutic Exercises DERMOT check list.ppt · 4. How should exercises be implemented as part of a...

Treatment2GoExploring Hand Therapy
ManualTherapeutic Exercises
An Upper Extremity Regime
Exploring Hand Therapy, Corporation d/b/a Treatment2Gowww.handtherapy.comwww.treatment2go.com
727-341-1674Fax: 888-2704079
Treatment2Go is a trademark and d/b/a of Exploring Hand Therapy.

POWER-WEB® INTERNATIONAL 835 Southeast Avenue, Suite 3
Tallmadge, OH 44278 Phone: (888) 823-0310 - (330) 630-5090
Fax: (330) 630-5091

Course Objectives:
• Participant will identify the different types of exercises used in rehab • Participant will be able to define the role of therapeutic exercises within the rehab plan of
care • Participant will be able to identify specific precautions for using therapeutic exercises • Participant will be able to demonstrate specific therapeutic exercises for selected joints of the
upper extremity • Participant will be able to identify methods to modify exercises to meet the specific demand
of patients

Therapeutic Exercises FAQ 1. Are therapeutic exercises occupation-based? Therapeutic exercises should be occupation-based. The reason is that each exercise should be selected to affect the patient’s functional level and it should be purposeful to the patient. Exercises should not be selected simply as a time-filler but instead for a functional purpose. Shoulder range of motion and strengthening exercises can be performed so a patient can put on a shirt, reach into their cabinet, and wash their hair. People must have range of motion and strength to perform those tasks so exercises are a step in the process. 2. What is the difference between Theraband, Theratubing, and dumbbells for
strengthening? All of the above items are used for strengthening exercises but each have different properties. Dumbbells come in a variety of resistance levels and require a good grip. During the exercise the dumbbell resists the motion. Theraband and Theratubing is a resistive elastic band or tube that provides both concentric and eccentric strengthening throughout the arc of motion. Both are easily used for home programs. 3. How do therapists know when to upgrade an exercise? There are different indicators for when to upgrade an exercise. These indicators rely on the therapist understanding the goal or purpose of the exercise. For example, if a swiss ball roll is used to increase wrist extension and the patient is able to demonstrate full passive or active-assisted extension, then the exercise would be discontinued and upgraded to active wrist extension. In addition, if the exercise is being performed to increase strength, such as the Digiflex for grip strengthening, the exercise should be upgraded when the patient no longer is challenged or experiences fatigue at the completion. 4. How should exercises be implemented as part of a patient’s plan of care? Exercises play a specific role in the patient’s plan of care. Consider the role of the exercises being planned. Are the exercises for range of motion, tendon gliding, edema management, strengthening, fine motor, etc. When implementing exercises, it is best to incorporate them into the treatment session over 1-3 sessions. By doing this, therapists can have the patient perform a small, select number of exercises and then assess the patient’s response to those exercises before implementing any additional exercises. This method allows the therapist to thoroughly evaluate the effectiveness of the exercise and identify any changes that need to be made. 5. Should a home exercises include exercises performed in therapy sessions?

Exercises selected for a home exercise program should be based on the specific needs of the patient. Due to this, patients may perform an exercise to increase shoulder active flexion at home and in the clinic. Often, exercises are chosen for the home program to reinforce exercises performed in the clinic. One important point to consider is that exercises performed in the clinic as a billable service are usually performed under the direction of a licensed therapist, so exercises at home may not be required the supervision of a therapist to be performed correctly. 6. Is it acceptable to have a patient perform more than 1 exercise to accomplish a
specific task? Yes. Often multiple exercises are selected to perform a specific task but each exercise may be performed in a different position, utilize different modes of resistance, or simulate a different functional task. For example, intrinsic strengthening can be performed with theraputty, hand helper, clothes pin, BP cuff, etc. 7. Is it better to adapt an exercise or to simply change the exercise to something
different? If a patient is having difficulty performing an exercise due to the position of the exercise then it is acceptable to change the position if it allows the patient the opportunity to perform it with less difficulty. If the mode of resistance is causing a patient difficulty, then the resistance level should be graded to meet the patient’s level of function but still be challenging. If the patient is unable to recruit the muscles necessary to perform the exercise, the exercise should simply be changed. If the exercise does not provide any challenge to the patient, the exercise should be changed or upgraded. 8. Are there any precautions to the use of therapeutic exercise? As with any treatment intervention, therapeutic exercises do have precautions. The most obvious precaution is that exercises must coincide with a patient’s postoperative status. Simply stated, this means that if the patient’s condition or surgical procedure has specific movement precautions or restrictions then the exercises performed should adhere to these guidelines. In terms of medical history, conditions such as high blood pressure, irregular heart rate, blood clots, asthma, COPD, CVA, etc. Make sure that a patient’s medical history will not present any adverse effects during therapy sessions. Also, consider the patient’s stage of healing or recovery. During the acute, inflammatory phase, exercises need to be selected carefully that will not increase the inflammatory process, cause increased pain or edema, or cause tissue damage. 9. Can an exercise be functional? Any exercise can be functional, even theraputty. As long as the exercise ultimately affects the patient’s functional outcome or simulates a functional task then it is functional. The most important aspect is that therapeutic exercises should be meaningful to the patient and their current functional demands.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 1
Therapeutic Exercises: An UE Regime
George LaCour, LOTR, CHT
Course Objectives
• Participant will identify the different types of exercises used in rehab
• Participant will be able to define the role of therapeutic exercises within the rehab plan of care
• Participant will be able to identify specific precautions for using therapeutic exercisesexercises
• Participant will be able to demonstrate specific therapeutic exercises for selected joints of the upper extremity
• Participant will be able to identify methods to modify exercises to meet the specific demand of patients
Why do we use therapeutic exercises?
Section I
An Introduction to Therapeutic Exercises
Chapter 1
Understanding the Role of Therapeutic Exercise
Role of Therapeutic Exercise
• To increase joint mobility
• To promote gliding of tendon / nerve and prevent adhesion formation
• To increase strength / stability
• To improve fine motor / dexterity
• To assist with maintaining connective tissue mobility and favorably affect scar tissue formation
• To decrease edema
• To restore normal active motion
• To decrease pain
• To improve joint / bone health
• To increase endurance

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 2
Most of All....
Therapeutic exercises are used to ultimately improve function.
Modes of Therapeutic Exercise
Passive
Active Resistive
Exercises
Passive Exercise
• Exercise is produced entirely by an outside force such as therapist, patient, machine, gravity.
• Passive exercise is used to maintain joint and soft tissue mobility as well as the mechanical elasticity of a muscle.
• Passive Exercise decreases edema assists with circulation enhances synovial• Passive Exercise decreases edema, assists with circulation, enhances synovial diffusion, and decrease pain.
• Indicated when pain, paralysis, spasticity, and weakness prevent a patient from actively maintaining full joint range of motion.
• Also used when joint mobilization and stretching techniques are required to improve joint and soft tissue mobility.
Active Exercise
• Used to maintain mobility, enhance synovial diffusion, and decrease pain.
• Because AROM can apply stress to joints, soft tissue, and tendons, active exercises are the preferred mode of exercise when the integrity of repaired structures is not a consideration.
A ti i l id f h i l l ti it d t tibilit f l• Active exercise also provides for mechanical elasticity and contractibility of muscles and helps to stimulate bone integrity to prevent demineralization.
• Active exercise is more effective than PROM in reducing edema because of the muscle-pump mechanism when there is active muscle contraction.
• Active-assisted exercises are a type of AROM exercise with assistance being provided by an outside force, either mechanically or manually
Resistive Exercise
• Resistance can be applied manually or from an external device.
• Isometric strengthening involves active contraction of the muscle for strengthening without any movement of the joint.
• Isotonic strengthening can be divided into concentric and eccentricIsotonic strengthening can be divided into concentric and eccentric.
• Concentric strengthening occurs while a muscle shortens.
• Eccentric strengthening occurs while a muscle lengthens.
Selecting the Appropriate Exercise
• Consider the current status and needs of the patient
• Are there any precautions related to the patient’s condition?
• Does the patient have any physical limitations which affect the performance of• Does the patient have any physical limitations which affect the performance of exercises?
• What is the objective of the exercise?
• What is the patient’s tolerance level?
• Any pain, fatigue, instability, etc?

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 3
Defining the Types of Exercise
Passive Range of Motion
• Passive stretching can be done through the available ROM to maintain joint and soft tissue mobility or it can be done at end-range to lengthen shortened soft tissue structures.
• The corrective force should be applied in a gentle, slow, and sustained pp g , ,manner.
• When more than 1 structure is responsible for limitations in joint motion, separate exercises should be incorporated. (i.e. PIP flexion limited by joint tightness as well as intrinsic tightness)
Passive Range of Motion
• When stretching a joint, the hand or joint should be positioned to eliminate resistive force from surrounding muscle-tendon systems.
• The segment proximal to the joint being mobilized should be stabilized while the corrective force should be applied to the segment distal to the joint being mobilizedjoint being mobilized.
• As a general rule, the corrective force should be applied to the most distal portion of the segment distal to the joint being mobilized as this will provide a longer lever arm and increase the amount of force that can be transmitted to joint structures.
• When joint contractures are present, stretching should be proceeded by joint mobilization to be most effective.
• Limitations in joint motion may result from changes in the contractile and non-contractile components of muscle.
Passive Range of Motion
• While passive stretching procedures are capable of elongating both components, active inhibition techniques facilitate stretching of the contractile element of the muscle.
• Active inhibition techniques reflexively relax the muscle fibers to be elongated prior to the stretching maneuver.
• The contract-relax exercise is an example of active inhibition techniques.
• When stretching muscle-tendon systems that cross multiple joints, the muscle must be stretched over one joint at a time and then all joints simultaneously until
Passive Range of Motion
be stretched over one joint at a time, and then all joints simultaneously, until optimum length of soft tissues is achieved.
• To minimize compressive forces in the small joints, stretching should start with the small, distal joints, and proceed proximally.
Precautions for PROM
• Stretching exercise should be used with caution when osteoporosis is suspected.
• After prolonged immobilization, vigorous or overly aggressive stretching is discouraged because immobilization can result in the decrease of the tensile strength of connective tissue.
• Precaution should be used when stretching edematous tissue because it is more susceptible to injury than normal tissue. Use the unaffected side as a guide to determine normal range.
• The potential abuses of passive stretching are mobilization of unprotected joints, stretching of the wrong joint or structure, and the infliction of additional tissue trauma.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 4
Active Range of Motion
• When used to maintain joint mobility, active exercise should be performed through the full available ROM.
• Composite motions, such as fisting and thumb opposition to each digit, should be encouraged, as they reproduce normal functional activities.
• When active exercise is used to restore mobility in the presence of increasing tissue resistance, fast, ballistic movements are discouraged by instructing the patient to maintain the end range position so that a gentle stretch can be applied.
• When active exercise is used to restore motion in stiff joints, care must be taken to ensure that the corrective force is directed toward the stiff joint and not dissipated in the adjacent normal joints
• Immobilization produces muscle atrophy, with complete inactivity resulting in decreased strength at a rate of 5% per day.
• Resistance exercises not only increase muscle strength and endurance, but also improve the ability of the patient to actively mobilize stiff joints.
• Resistance exercise can be classified as either static (isometric) or dynamic (isotonic).
Resistance Exercise
( )
• Isometric exercise allows for strengthening without the stress to joints and soft tissue produced by dynamic exercise. Strength gains made with isometric exercise occur only at the joint angle at which the exercise is performed. As a result, the patient should exercise at several different joint angles throughout the range of motion.
• Isotonic exercise occurs when a muscle is subjected to a constant or variable resistance throughout the available range of motion.
• Resistance exercises that strengthen functional muscle groups should be selected.
Section II
Therapeutic Exercises by Joint
Chapter 2
The Shoulder
General Considerations
• The first priority for the shoulder is regaining passive range of motion.
• Passive range of motion is essential to prevent adhesive capsulitis as well as allow sufficient mobility for regaining active range of motion and strength.
• When focusing on active motion, it is best to begin with active-assisted motion as this will provide the patient with the opportunity to actively fire the muscle and monitor for any type of compensation.
• With active range of motion, it is best to begin in supine, progress to sitting, and finally to standing.
• For strengthening of the shoulder, exercises should target areas of weakness and strive to create a muscle balance to prevent compensation.
• NEVER neglect the muscles which control the scapula. The scapula is the cornerstone of shoulder motion and function.
Supplies Needed for this Chapter
• Small Ball or Pillow
• Cane or Piece of 3/4” PVC Pipe
• Dumbbell (1-2 #)
• Body Blade
• Swiss Ball
• Towel or Oven Mitt
• Pulleys
• Theratubing (Red or Green)
• Theraband (Red or Green)
• Plyoball (2-4#)
• Weighted Dowel (2#)
• Towel Roll or Foam Roll

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 5
Passive Range of Motion
• Passive range of motion should be performed in a supine position, if possible. This allows for easy handling by the therapist and stabilization of the scapula.
• Most patients are apprehensive and very guarded with passive motion.
• Passive motion begins with hand placement and overall handling by the therapist. The therapist should have one hand at the distal forearm and wrist while the other hand cups the distal humerus and elbow. The grip of the therapist should be firm but relaxed.
Passive Range of Motion
• Passive motion usually progresses as follows: ER; IR; Abduction; Flexion; Extension (depending on any applicable precautions)
• For ER/IR, the arm begins at 0 degrees abduction then progresses to 45 and finally 90 degrees of abduction.y g
• Passive motion allows for assessment of capsular tightness, teres tightness, subscapularis tightness, and any muscle guarding.
Pendulums
• Most basic form of shoulder exercise
• Often used in times of acute pain or immediately post-operatively
• Primary use of pendulums is to gently mobilize the glenohumeral joint and capsule.
• Pendulums are generally pain-free.
Pendulums
• Pendulums occur when motion of the shoulder is generated by the trunk and lower extremities.
• Pendulums can be modified and performed in a prone position to provide greater distraction and mobilization of the glenohumeral joint.
3 M ti ll Fl i /E t i Abd ti /Add ti• 3 Motions usually occur: Flexion/Extension; Abduction/Adduction; Rotation
• It is best on rotation to perform clockwise and counterclockwise
Pendulums
Flex/Ext Side-2-Side Rotation
Prone Pendulums
Flexion / Extension Rotation

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 6
Insert Video
Pendulums
Pulleys
• Pulleys can be a passive exercise, active-assisted, or a low-load stretch.
• Pulleys are a versatile exercise because they can be performed in the clinic or at home.
T b f d tl th l f ll h ld b t d th• To be performed correctly, the angle of pull should be correct and the patient should perform each “pull” slowly with a hold at end range.
Pulleys for Flexion
• Pulleys for flexion can be progressed in 3 stages:
1 Walk-out1. Walk out
2. Sitting
3. Standing
Pulleys Walk-out
• The patient grasps the handles of the pulleys with both hands.
• The patient relaxes both shoulders and arms and simply steps backward letting the tension on the pulley ropes pull th h ld i t fl ithe shoulder into flexion.
• Make sure the patient remains relaxed and also does not lean back as this can place too much traction on the shoulder joint.
Pulley Walk Out
A B
Pulleys in Standing
• The patient grasps the handles of the pulleys with both hands.
• The patient relaxes the affected shoulder and uses the unaffected arm to pull the rope which in turn raises the affected arm into flexion.
• If shoulder hiking is observed, the patient is actively trying to flex the shoulder. This should be avoided.
• Pulleys in standing can be used for flexion to 90 degrees.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 7
Standing Pulley for Flexion
A B
Pulleys in Sitting
• The patient is seated in a chair with the pulley positioned in line with the affected shoulder.
• The position of the chair will determine the level of stretch from the exercise.
• The patient grasps the handles of the pulleys with both hands.
• The patient relaxes the affected shoulder and uses the unaffected arm to pull the rope which in turn raises the affected arm into flexion.
• If shoulder hiking is observed, the patient is actively trying to flex the shoulder. This should be avoided.
• If the patient is guarded, have them use the affected arm to pull down the pulley.
Sitting Pulley for FlexionA B
Pulleys for Abduction
• The patient grasps the handles of the pulleys with both hands.
• The patient relaxes the affected shoulder and uses the unaffected arm to pull the rope which in turn raises the affected arm into abduction.p p
• At the first sign of tension with abduction, usually evidenced by hiking, the patient is instructed to actively depress the affected shoulder.
Standing Pulley for Abduction
A B
Insert Video
Pulleys

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 8
Cane exercises
• Also known as Wand or L-Bar
• Cane exercises can be a passive exercise, active-assisted, or an external stretch.
• Hand placement is key for performing the exercises correctly.
• Patient positioning will determine the mobilization of a specific structure.
Cane exercises: Supine Flexion
• Supine flexion should be performed with the palms facing up if possible.
• If this position is uncomfortable, the patient can be allowed initially to perform the exercise with the palms downexercise with the palms down.
• The patient begins at the knees and moves into flexion overhead.
• As the patient improves, weight can be added to provide a greater stretch or increased level of resistance for strengthening.
Supine Flexion with L-Bar
A B C
Cane exercises: Supine Scaption
• For supine scaption, the motion occurs in the plane of the scapula.
• The patient hold with the affected hand on the end of the cane with the thumb pointing in the direction of the motion.pointing in the direction of the motion.
• The unaffected hand begins at the level of the hip and moves the affected shoulder within the plane of the scapula.
• At end-range, the patient can push with the cane or the therapist can pull which will provide a level of distraction to the glenohumeral joint.
Supine Scaption with L-Bar
A B C
Cane exercises: ER
• For external rotation, this can be performed in standing or supine.
• Supine offers a better stretch but is often not tolerated during the painful stages of acute pain from an injury or surgery.
• In standing, make sure the patient moves the shoulder within the correct line of motion. Monitor the patient to make sure they are not performing shoulder abduction or elbow extension to substitute for shoulder external rotation.
• In supine, the shoulder can be moved through ER with the arm at 0/30/45/60/90 degrees of shoulder abduction.
• In supine monitor that the motion occurs in line with the axis of motion.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 9
Standing ER with L-Bar
A B C
Supine ER with L-Bar
A B C
Cane exercises: Abduction
• For abduction, the exercise can be performed in standing or in supine.
• Supine offers a better stretch without compensation as the scapula is fixed by the surface they patient is onsurface they patient is on.
• In standing, have the patient perform the exercise with their back against the wall to prevent compensation.
• Monitor for shoulder hiking or painful impingement. Both should be avoided.
• Initially, strive to have the patient reach 90 degrees of abduction and then progress.
Standing Abduction with L-Bar
A B C
Insert Video
Cane Exercises
Other Active-Assist Exercises
• Active-assisted exercises involve the use an external device to accomplish a motion.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 10
Swiss Ball Roll Exercises
• Swiss Ball Roll is an exercise used primarily when initiating active motion for shoulder flexion. It can also be used for horizontal abduction/adduction.
• Swiss Ball Roll can also be used for self-mobilization or stretching for shoulder flexion abduction and the thoracic spineflexion, abduction, and the thoracic spine.
• For standing swiss ball roll, the patient begins with the hand placed at the umbilical level on the front surface of the ball. The patient then pushes out to roll the ball.
• The size of the swiss ball helps to determine the level of flexion achieved and the amount of active motion required.
• The roll can also be performed in sitting to increase the incline for active motion.
Swiss Ball Roll
A B
Assisted Glides
• Assisted glides are used for retraining flexion, scapula mobilization, and for increasing strength for shoulder flexion and the scapula stabilizers.
• Assisted glides are progressed in 3 phases: Table; Incline; Wall
A th ti t i bl t t l t ti ti i t it th lid i d• As the patient is able to tolerate active motion against gravity, the glide is progressed.
• With the incline and wall glide, the objective is to maximize active flexion without compensation.
• At the first sign of shoulder hiking, the patient should return to the starting position.
• Tactile cues from the therapist on the top of the affected shoulder may help to avoid hiking. Also, taping of the scapula prior to the exercise can help.
Table Glides
A B
Incline Glide
Wall Glide

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 11
Supine Prayer Stretch
• Supine Prayer Stretch is used to increase shoulder flexion, especially when the patient is apprehensive and guarding during passive flexion by the therapist.
• The patient clasps both hands together, like a prayer, and the p p g , p y ,unaffected side assists to perform supine shoulder flexion.
• Flexion should be to the level of the chest or mouth initially and then progress overhead.
Supine Prayer Stretch
A B
Insert Video
Other Active-Assist Exercises
Rhythmic stabilization: Place & Hold
• Rhythmic stabilization is a form of exercise which is used to promote joint co-contraction which in turn increases joint proprioception and stability.
• A basic form of rhythmic stabilization for the shoulder is place/hold.
• For Place / Hold, the shoulder is placed in varying degrees of flexion with the elbow fully extended and the patient is asked to hold this position. Initially the shoulder is placed at 90 degrees and then at various points as stability improves.
Supine Place and Hold in 90 degrees Flexion
Rhythmic stabilization
• Rhythmic stabilization can also be performed in flexion and/or scaption with external stimulus applied by the therapist to challenge the joint.
• Rhythmic stabilization for ER/IR can be performed, initially with the patient in supine with the arm at 0 degrees abduction then progressed up to 90 degrees of abduction.
• As stability and strength increase, ER/IR can be challenged by having the patient hold this position in varying degrees of abduction while in sitting and standing with the therapist applying external stimulus.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 12
Rhythmic Stabilization for Flexion/Extension
Rhythmic Stabilization for ER/IR
Insert Video
Rhythmic Stabilization
Short-Arc Motion
• Short-arc motion is an extension of rhythmic stabilization by adding a component of active exercise by the patient.
• Instead of an outside stimulus being applied by the patient, the patient is instructed to perform short-arc motion in a smooth, controlled manner.
• As stability of the GH joint increases, the arc of motion is increased and resistance is added.
• This exercise is often used early in shoulder rehab as active exercise is initiated. Short-arm motion allows for the establishment of joint stability and co-contraction which helps to minimize compensatory shoulder hiking during active range of motion against gravity.
Short Arc Motion: Flexion/Extension
A B
Short Arc Motion: Adduction/Abduction
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 13
Insert Video
Short-arc Motion
Isometric Strengthening• Isometric strengthening involves active contraction of a muscle without
mobilizing the distal segment.
• Isometric strengthening should be slow and controlled with the patient holding the contraction for 3-5 seconds.
• Submax isometrics are a form of isometric exercise with the patient f 2 % f f fperforming 25% of normal contraction. This is most often performed
with the therapist providing manual resistance to monitor the force of contraction.
• Isometrics can be performed with feedback being provided by manual contact, a pillow, or a slightly deflated ball.
• Isometrics for shoulder ER/IR can also be performed with theratubing.
Isometric Shoulder Flexion
ISometric Shoulder Abduction
Isometric Shoulder ER
Isometric Shoulder IR

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 14
Insert Video
Isometrics
Isotonic Strengthening
• Isotonic strengthening involves active contraction of a muscle(s) with movement of the distal segment. This is otherwise known as an open chain exercise.
• Isotonic strengthening should be performed once active range of motion has been restored.
• Isotonic strengthening can be performed with dumbbells, weight cuffs, weighted dowels, or with resistive bands such as TheraBand or TheraTubing. CanDo also makes these products.
Isotonic Strengthening
• Isotonic strengthening should be performed in a smooth, slow, controlled motion with a hold.
• Hand placement during the motion can alter the difficulty of the exercise.
• Isotonic exercises should result in fatigue at their completion. It should not elicit pain.
• If a patient complains of pain or instability during the exercise, modifications may be necessary.
Isotonic Strengthening
Supine E i
ProneE i
TheratubingE i
StandingExercises
SidelyingE iExercises Exercises Exercises
(Dumbbell)Exercises
ConcentricEccentric
Plyometric
Exercises in Prone/Sidelying/Supine
• The advantage of performing exercises in these positions is the ability to control compensation.
• Strengthening is often performed in these positions initially then progressed to standing using the resistive bands.
• Once the patient is able to perform exercises in these positions with 2 lbs. resistance the patient is progressed to the resistive bands.
• ER/IR is often performed in supine initially as gravity is eliminated and the scapula is stabilized. As the patient improves, they are progressed to sidelying.
Supine Shoulder ER/IR
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 15
Exercises in Prone/Sidelying/Supine
• Sidelying ER should be performed with a towel roll to optimize the exercise.
• During sidelying ER, a towel can be used to prevent compensation and isolate motion. The patient should begin at the abdomen and then move in ER to neutral or 30 degreesThe patient should begin at the abdomen and then move in ER to neutral or 30 degrees of ER but not any farther.
• The patient can be instructed to hold the position which increases the level of difficulty.
• Sidelying IR is often difficult due to weight bearing on the affected shoulder.
Sidelying Shoulder ER
A B
Sidelying Shoulder IR
A B
Exercises in Prone/Sidelying/Supine
• Prone Horizontal Abduction can be performed with the forearm in varying positions (Forearm in neutral, pronation, supination) to change the level of difficulty.
• Prone horizontal abduction utilizes all posterior rotator cuff muscles as well as the scapula stabilizers.
• If the patient is compensating by using the scapula muscles, the exercise needs to be corrected.
• Often place/hold in the position of horizontal abduction can be used initially. The patient can lower the arm from the position through eccentric contraction.
Prone Horizontal Abduction
A B
Exercises in Prone/Sidelying/Supine
• Supine chest press is performed to assist with strengthening of the pectoralis muscles as well as the serratus anterior.
• Chest press can be performed with the can or a weighted dowel initially.p p g y
• A plyoball can be used (usually 4#) to perform the chest press and requires more dynamic stabilization. As the patient progresses, they can hold the plyoball to perform the chest press with a single arm which significantly increases the level of difficulty.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 16
Supine Chest Press
A B
Supine Chest Press with Plyoball
A B
Insert Video
Prone/Sidelying Exercises
Exercises in Standing
• Exercises in standing are the most challenging as there is no support to the scapula.
• The patient must be able to stabilize the scapula against the thoracic wall in order to complete the motion correctly or elsethoracic wall in order to complete the motion correctly or else compensation and impingement will occur.
• When performing exercises in standing both the affected and unaffected sides should perform the motion. This allows for balanced strengthening as well as proprioceptive training.
Open Can / Empty Can
• Open can is an exercise which promotes flexion in the scapula plane. It also allows for a focus on humeral head depression when initiating shoulder flexion.
• During open can, the thumb is point up, in the direction of the motion.
• Open can is targeted for flexion to 90 degrees but should be stopped at the level where any compensation is noted.
• Empty can is a more challenging exercise which isolates the supraspinatus. The thumb is pointing at the floor during this motion.
• Performing the exercises in front a mirror can be helpful to provide feedback to the patient. The patient can also perform the exercise with their eyes closed for proprioceptive training.
Open Can
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 17
Empty Can
A B
Exercises in Standing
• Put-em-up combines both scapula and shoulder motion.
• It is best performed with the back against the wall.
• The exercise begins with the arms relaxed. The patient moves into shoulder abduction at 90° and with the elbows flexed to 90° moves into ERabduction at 90 and with the elbows flexed to 90 moves into ER.
• During the motion the patient retracts and stabilizes their scapula.
Put-Em-Up
A B C
Exercises in Standing
• Standing horizontal abduction is performed with theraband to allow for concentric and eccentric strengthening of the scapula stabilizers and posterior rotator cuff.
• Initially, the exercise can be performed at the umbilical level and progressed to chest level.
• The patient may perform the exercise with their back against the wall for stabilization or sitting on a swiss ball for core strengthening.
Standing Horizontal Abduction
A B
Insert Video
Standing Exercises

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 18
Theratubing Exercises
• In general, exercises performed with theraband or theratubing allows for strengthening with both a concentric and eccentric contraction.
• Theratubing exercises should be performed slow and controlled for the most effective results.
• The starting and ending position of the arm during the exercise is g g p gimportant for proper strength training.
• For ER/IR with the arm by the side, a towel roll or foam roll is used to isolate the motion and promote scapula stabilization.
• PNF exercises are diagonals which are more advanced forms of strengthening. These exercises target muscle groups instead of an isolated muscle.
Shoulder Extension
A B
IR with Arm By Side
A B
ER with Arm By Side
A B
ER with Arm @ 90 degrees Abduction
A B
IR with Arm @ 90 degrees Abduction
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 19
PNF: John Travolta
A B
PNF: Close the Door
A B
Insert Video
Theratubing Exercises
UBE
• The UBE can be used for ROM if performed slowly without resistance
• The UBE can be adjusted in terms of height as well as resistance.e g as e as es s a ce
• The UBE is used for endurance training once the strengthening phase of rehab has been initiated.
Scapula Stabilization
• Scapula stabilization is imperative for proper shoulder function.
• Without scapula stabilization, there will be abnormal scapulohumeral rhythm which will result in limited motion, impingement, and eventually pain.
• Initially, scapula exercises focus on shoulder shrugs and rolls to isolate motion.
• The BOSU can be used to promote dissociation of the shoulder girdle mobilizing the scapula for depression.
• Scapula pinch is the initial exercise for scapula stabilization.
• As the patient improves, the scapula clock is added as this encompasses all muscles for scapula stabilization and assists with “setting” of the scapula
Scapula Stabilization with BOSU

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 20
Scapula Pinch
Scapula Clock
Shrug Pinch Depress
Rows
• The row is progressed in 3 phases: standing 1-arm, prone, and standing with theratubing.
• For the standing 1-arm row, the patient moves from a relaxed position to a position of shoulder retraction. I instruct the patient to “start the lawn mower”.
• In prone, the patient moves the arm from the starting position to a position of retraction with the upper arm at the level of the trunk. The therapist should be able to palpate the scapula as it is retracted and adducted. Make sure to keep the shoulder adducted during the exercise.
• In standing, the row is most effective if performed bilaterally with theratubing. The patient will perform a low row with the arms by the side. As the hands approach the trunk, the patient will supinate the forearm triggering additional scapula pinch.
Standing 1-Arm Row
A B
Prone Row
A B
Bilateral Low Row
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 21
Scapula Stabilization withShoulder Extension
• Prone shoulder extension is initiated to strengthen the posterior shoulder, latissimus, and lower trapezius. The patient can perform the exercise with the forearm in neutral, prone, or supination to change the level of difficulty.
• The patient should extend the arm, with the elbow locked in extension and the wrist locked in neutral, to a point level with the hip.
• As the patient improves with prone shoulder extension, they can then be progressed to Shut-the-door in standing and or Latissimus pulldowns.
Prone Shoulder Extension
A B
Shut The Door
A B
Lat Pulldown
A B
Serratus Punch
• Serratus punches are performed in supine initially to support the scapula. The patient performs a chest press-type motion and then lifts the scapula from the table to engage the serratus anterior.
• A dumbbell can be used as resistance.
• A plyoball can also be used and is more challenging to the patient to stabilize throughout the exercise.
• Serratus punch can also be performed in standing with theratubing.
Supine Serratus Punch
A B
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 22
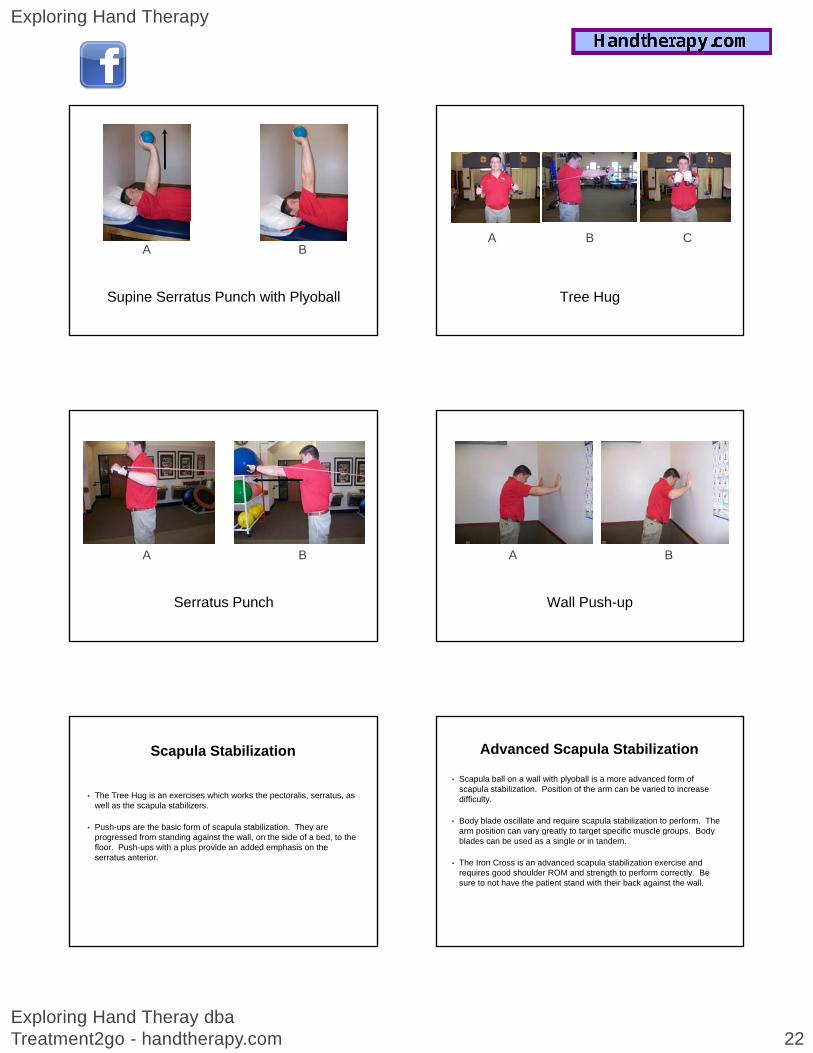
Supine Serratus Punch with Plyoball
A B
Serratus Punch
A B
Scapula Stabilization
• The Tree Hug is an exercises which works the pectoralis, serratus, as well as the scapula stabilizers.
• Push-ups are the basic form of scapula stabilization. They are p p yprogressed from standing against the wall, on the side of a bed, to the floor. Push-ups with a plus provide an added emphasis on the serratus anterior.
Tree Hug
A B C
Wall Push-up
A B
Advanced Scapula Stabilization
• Scapula ball on a wall with plyoball is a more advanced form of scapula stabilization. Position of the arm can be varied to increase difficulty.
• Body blade oscillate and require scapula stabilization to perform. The arm position can vary greatly to target specific muscle groups Bodyarm position can vary greatly to target specific muscle groups. Body blades can be used as a single or in tandem.
• The Iron Cross is an advanced scapula stabilization exercise and requires good shoulder ROM and strength to perform correctly. Be sure to not have the patient stand with their back against the wall.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 23
Scapula Stabilization with Ball on Wall
Body Blade: Single
A B
Body Blade: Bilateral
A B
Prone Scapula “T” and “W”
A B
Iron Cross
A B C
Insert Video
Scapula Stabilization

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 24
Stretching
• Stretching is a necessary part of the rehab of the shoulder. Position of the shoulder and the application of stress will determine the structure being targeted for stretch.
All t t h h ld b f d ith th t t b i h ld i iti f t t h• All stretches should be performed with the structure being held in position of stretch for 5-10 seconds per repetition.
• Capsular stretches can be performed manually or with the assistance of an outside device (cane, swiss ball, etc)
Capsular Stretching
• Capsular stretches can be performed manually or with the assistance of an outside device (cane, swiss ball, etc)
Posterior Capsular Stretch
A B
Anterior Capsular Stretch
A B
Anterior Capsular Stretch
Internal Rotation Stretch
• IR can be stretched in standing with a towel, in sidelying, or in supine.
• With a towel, the patient will pull the affected arm straight across the buttocks initially to perform the stretch. Once the patient is able to reach across and touch the opposite buttock the towel stretch is progressed over the shouldertouch the opposite buttock, the towel stretch is progressed over the shoulder.
• In sidelying, the patient will be on their unaffected side. The patient will then simply let the affected arm drape anterior across the chest and the weight of their arm will perform the stretch. A 1-2# weight can also be used to elicit a stronger stretch.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 25
IR Stretch with Towel
A B
Corner Stretch
• The pectoralis can be stretched manually in supine or with the corner stretch .
• For the corner stretch, the patient will place one foot forward into the corner. The h d l d th ll I iti ll th ti t h ld k th h d dhands are placed on the wall. Initially, the patient should keep the hands around the lower chest level and eventually progress to shoulder level.
• The patient will stabilize their hands on the wall and then stretch the pectoralis by leaning forward onto their anteriorly placed foot until a stretch is felt in the anterior chest area.
Corner Pectoralis Major Stretch
A B
Stretching
• Flexion can be stretched with a corner wall glide, swiss ball on wall, or self mobilization.
• For the corner wall glide, the patient performs a wall glide moving the shoulder into flexion with the corner serving as a guide and a block. At the end-range, the patient can lean into the wall to achieve full stretch.
• The swiss ball roll on the wall allows the patient to actively move against gravity into flexion. At their maximum point of flexion, the ball will assist with an end-range stretch.
• Self-mobilization resembles a table glide, except the patient leans forward allowing the table surface to further mobilize the shoulder into flexion.
Corner Wall Flexion Stretch
Swiss Ball Roll on Wall
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 26
Self Mobilization: Flexion
A B
Additional Shoulder Stretches
• Self-mobilization for ER at 90 degrees abduction
• ER door stretch
• Low-load ER stretch
Self Mobilization: ER with ABduction
A B
ER Door Stretch
A B
Low-Load ER Stretch
Insert Video
Shoulder Stretches
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 27
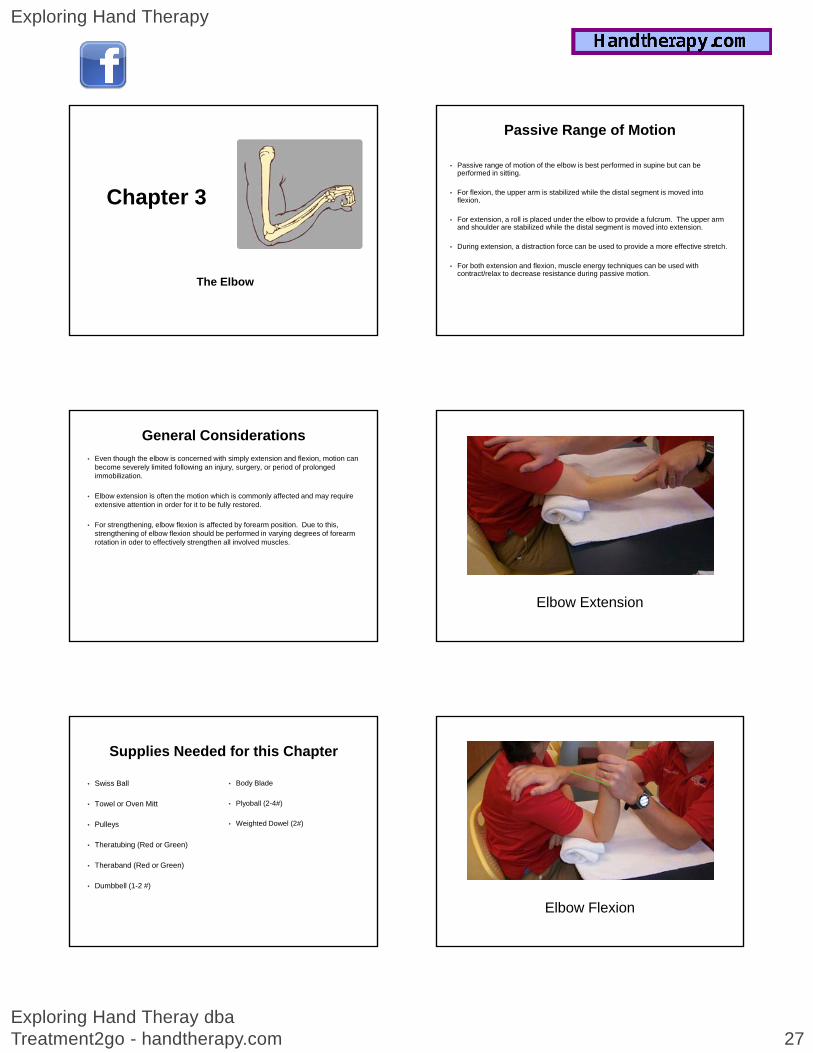
Chapter 3
The Elbow
General Considerations
• Even though the elbow is concerned with simply extension and flexion, motion can become severely limited following an injury, surgery, or period of prolonged immobilization.
• Elbow extension is often the motion which is commonly affected and may require extensive attention in order for it to be fully restored.
• For strengthening elbow flexion is affected by forearm position Due to thisFor strengthening, elbow flexion is affected by forearm position. Due to this, strengthening of elbow flexion should be performed in varying degrees of forearm rotation in oder to effectively strengthen all involved muscles.
Supplies Needed for this Chapter
• Swiss Ball
• Towel or Oven Mitt
• Pulleys
• Body Blade
• Plyoball (2-4#)
• Weighted Dowel (2#)
• Theratubing (Red or Green)
• Theraband (Red or Green)
• Dumbbell (1-2 #)
Passive Range of Motion
• Passive range of motion of the elbow is best performed in supine but can be performed in sitting.
• For flexion, the upper arm is stabilized while the distal segment is moved into flexion.
• For extension a roll is placed under the elbow to provide a fulcrum The upper armFor extension, a roll is placed under the elbow to provide a fulcrum. The upper arm and shoulder are stabilized while the distal segment is moved into extension.
• During extension, a distraction force can be used to provide a more effective stretch.
• For both extension and flexion, muscle energy techniques can be used with contract/relax to decrease resistance during passive motion.
Elbow Extension
Elbow Flexion

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 28
Active-Assist Exercises
• Active-assist exercises for the elbow are similar to those used for the shoulder.
• Swiss ball roll is used to promote extension and flexion.
• Pulleys can be used for extension stretch with active flexion from the extended position.
• Table glides can be used for both extension and flexion with stress to the medial and lateral elbow controlled.
• The UBE is used for ROM of the elbow with resistance set to zero. The chair position will determine if the exercise targets extension or flexion.
Swiss Ball Roll
A B
Table Glides
A B
UE Ergometer for ROM
Isotonic StrengtheningIsotonic Strengthening
Elbow Extension with Theratubing
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 29
Elbow Extension with Slotted Pulleys
A B
Elbow Flexion with Slotted Pulleys
A B
Elbow Flexion with Dumbbell
A B
Self-Stretching & Low Load Stretching
• Self-stretching is difficult for the elbow.
• Passive stretching performed by the patient is often not effective as they are unable to sustain a stretch that effectively improves range of motion.
• The elbow flexion stretch is effective for increasing elbow flexion. The patient iti i il t th t f ll h h th ti t ll thassumes a position similar to that for a wall push-up, however the patient pulls the
arms down the wall forcing the elbow into flexion.
• Another method for increasing elbow flexion is to place the patient in supine. The patient holds a weight or a plyoball. The patient relaxes allowing for the weight (plyoball) to push the elbow into a flexed position.
• For elbow extension, a towel roll is placed under the elbow and a weight is applied to the distal segment. The patient hold this position for an allotted time to achieve results.
Elbow Flexion Stretch
A B
Elbow Flexion Stretch with Plyoball
A B

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 30
Elbow Extension Stretch
A B
Demonstration
Elbow Low-Load Stretching
Chapter 4Chapter 4
The Forearm
General Considerations
• Just as the elbow is affected by immobilization, so is the forearm.
• Restoring forearm rotation can be deceiving because often patients will compensate when performing their exercises so it will appear that the motion has been restored when, in fact, it has not.
• When performing any exercise for pronation or supination, it is best to have the elbow at 90 degrees with the arm by the side as this will help to prevent compensation.
Supplies Needed for this Chapter
• Desensitization Buckets (or Bowls filled with Dried Beans, Rice, or Corn)
• Theratubing (Red or Green)
• Wrist Roll
• Mr. Wrister
• PuttyCiser
• Theraband (Red or Green)
• Dumbbell (1-2 #)
• Hammer or Crescent Wrench
• Theraband Flexbar (Red or Green)
y
• Velcro Board
Passive Range of Motion
• The most difficult aspect of performing passive range of motion to the forearm is hand placement.
• The most common mistake therapists make is that they hold onto the patient’s hand when performing passive supination or pronation.
• The correct hand placement for passive motion of the forearm isThe correct hand placement for passive motion of the forearm is proximal to the wrist on the distal radius and ulna.
• Active inhibition is a technique commonly used when performing passive range of motion. It is a contract-relax technique which helps the patient to decrease guarding and/or spasms which are limiting passive motion.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 31
Forearm Supination
Forearm Pronation
Active Range of Motion
• AROM of the forearm can be performed with numerous activities.
• Tubs of media such as beans, corn, or rice can be used. Patients can use their hand to scoop the media or they can use a utensil such as a cooking spoon, ice scoop, or ice cream scoop and this will allow for simulation of the supination motion.
• Patients can use the Minnesota Rate of Manipulation or the Bolt Board for the Bennett pHand Dexterity test to perform supination and pronation. These can even be timed to establish baselines.
• A deck of cards or dominos can also be used to perform the activity in the clinic or at home.
• The Wrist-R-Ciser allows for both pronation and supination.
• The Wrist Roll can be used without weight for active supination/pronation.
Supination Pick-up
Supination Scoop
Supination / Pronation with Scoop

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 32
Wrist AROM with Wrist-R-Ciser
Pronation / Supination with Wrist Roll
1 2
Demonstration
Forearm AROM Exercises
Isotonic Strengthening• Isotonic strengthening for the forearm should mirror the arm position used
for AROM with the arm by the side and the elbow flexed, if possible.
• In the clinic and at home a hammer or other hand tool is readily available for use for forearm strengthening. Items such as a cooking spoon, a rolling pin, a crescent wrench, or a hammer can be used to strengthen pronation or supination.
• The Theraband Flexbar can also be used strengthening. While holding the Flexbar with the palms down, the motion strengthens the supinators. While holding the Flexbar with the palms up, the motion strengthens pronation.
• The Bennett Hand Tool test can be used as well as a weight well to strengthen forearm pronation/supination.
• The Wrist Roll or Mr. Wrister can also be used to strengthen the forearm
• The Power Web can also be used.
Supination with Hammer
1 2 3
Pronation with Hammer
1 32

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 33
Supination with Theraband Flexbar
1 2
Pronation with Theraband Flexbar
1 2
Pronation / Supination with Wrist Roll
1 2
Supination with weight
1 2
Pronation with weight
1 2
Pronation with Theratubing
1 2

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 34
Supination with Theratubing
1 2
Supination / Pronation with Power Web
Demonstration
Forearm Strengthening
Isotonic Strengthening (PuttyCiser)
• The PuttyCiser is a versatile tool that can be used to strengthen the forearm.
• Different tools are available as well as different resistance levels with theraputty.p y
Supination / Pronation with
Puttyciser
Forearm Supination with Puttyciser

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 35
Demonstration
Forearm Strengthening with PuttyCiser
Isotonic Strengthening (Velcro Board)
• The Velcro board is another tool which can be used for strengthening.
• Patients can perform pronation/supination with the long handle dowel or with the Key pinch.p
ForearmSupination / Pronation
Using Velcro Board Key Attachment
Forearm Supination / Pronation
Using Velcro Board Dowel Roll Attachment
Demonstration
Forearm Strengthening with Velcro Board
Chapter 5Chapter 5
The Wrist

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 36
General Considerations
• The wrist is concerned with extension, flexion, radial deviation, and ulnar deviation.
• Following any type of immobilization, the wrist can be affected in terms of soft tissue tightness as well as extrinsic muscle-tendon tightness.
• Exercises must target all structures involved to be effective for the wrist.
• For grip strength, the patient must have adequate wrist extension so this motion must be a focus on any treatment program.
• Strengthening of the wrist should be performed with caution initially to prevent any tendinitis or if any wrist instability is suspected.
Supplies Needed for this Chapter
• Swiss Ball
• Wobble Board
• Wrist X-R-Ciser
• Dumbbell (1-2 #)
• Blood Pressure Cuff
• Theraband FlexBar (Red or Green)
• Wrist Roll or Mr. Wrister
• Theratubing (Red or Green)
• Theraband (Red or Green)
• PuttyCiser
• Velcro Board
• Plyoball (2-4#)
• Dowel with Slotted Weights
• Small Foam or Nerf Ball (Tennis Ball Can be substituted)
Passive Range of Motion
• Passive range of the motion for the wrist can be painful following prolonged immobilization or with persistent edema due to the lack of mobility within the carpal rows. Due to this, patients often benefit from joint distraction or joint mobilization prior to passive motion.
• Passive motion of the wrist can be performed with the forearm pronation or with the forearm in a neutral positionforearm in a neutral position.
• Some therapists prefer to manually stabilize the proximal phalanx. Others prefer to use the edge of a treatment table or an elevation wedge. The main factor to monitor is that wrist motion is not impeded by any structure.
Wrist Extension
1 2
Wrist Flexion
A B
Active-Assist Exercises
• The Swiss Ball is an effective method for increasing wrist ROM. It is primarily used for increasing wrist extension.
• A Wobble Board is a treatment tool used mostly by Physical Therapists to treat the ankle. It can also be used to increase wrist flexion.
• When using the Wobble Board it is imperative for the forearm to maintain contact with the table during the exercise.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 37
Wrist Extension with Swiss Ball Roll
1 2
Wrist Flexion with Swiss Ball Roll
1 2
Wrist Extension with Wobble Board
1 2
Wrist Flexion with Wobble Board
1 2
Demonstration
• Wrist AAROM with Swiss Ball
Active Range of Motion
• Active range of motion should focus on extension, flexion, radial deviation, and ulnar deviation.
• The most common response of patients when performing AROM of the wrist is to lift the forearm off of the table or wedge to compensate. Be sure to stabilize the forearm when performing exercises.
AROM f th i t b ff t d b ft ti ti ht ll ti ht i th• AROM of the wrist can be affected by soft tissue tightness as well as tightness in the extrinsic extensors/flexors of the wrist.
• Due to this, patients may have greater range of motion when the extrinsics are not placed on stretch during the motion. For example, wrist flexion may have a greater measurement when the patient performs this motion with a relaxed fist versus a closed fist.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 38
Active Range of Motion
• When performing wrist extension, patients with weak wrist extensors will compensate by using the finger extensors.
• Isolate the wrist extensors by having the patient hold a towel roll, a dowel, or a small foam ball when performing the motion.
• For radial/ulnar deviation, these exercises can be performed with the forearm in a neutral or pronated position. Find the position of greatest stretch when performing this motion.
• For AROM, the wrist roll, Mr. Wrister, and weight wells are useful tools in the clinic.
Wrist Flexion/Extension with Wrist Roll (no weight)
Wrist AROM with Wrist-R-Ciser
Demonstration
Wrist AROM
Isometric Strengthening
• Isometric strengthening of the wrist is often used for arthritis and also for TFCC injuries in addition to other conditions.
• Manual resistance can be applied for extension, flexion, radial deviation, and ulnar deviation but often therapists would like to quantify the force.
• Muscle myometers are available commercially for use but are expensive. Another alternative is a BP cuff. The BP cuff provides feedback to the therapist as well as the patient in regards to the amount of force being generated when performing the exercise.
Isometric Wrist Extension with BP Cuff

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 39
Demonstration
Wrist Isometrics with BP Cuff
Isotonic Strengthening -Dumbbells & Theratubing
• Isotonic wrist strengthening can focus on extension, flexion, and radial/ulnar deviation.
• With dumbbells there are options. Patients can use metal dumbbells,With dumbbells there are options. Patients can use metal dumbbells, coated dumbbells, and even soft weights. All offer different grip sizes which makes it easy to accommodate different needs of the patient.
• Patients with arthritis or following a distal radius fracture often respond better to the soft weights because it does not require a tight grip.
• For all motions, it is important to hold the position for maximum strengthening.
Wrist Extension with weights
1 2
Wrist Flexion with Weights
1 2
Wrist Radial Deviation with Weight
1 2
Wrist Extension with Theratubing
1 2

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 40
Wrist Flexion with Theratubing
1 2
Demonstration
Wrist Isotonic StrengtheningDumbbells / Theratubing
Isotonic Strengthening -TheraBand Flexbar & Wrist Roll
• Exercises with the Flexbar can be performed with the elbows bent or fully extended depending on the difficulty of the exercise.
• The unaffected hand stabilizes the Flexbar while the patient grasps the Flexbar and completes the exercise. For extension, the patient should reach and grasp the Flexbar in a slightly flexed posture and then twistreach and grasp the Flexbar in a slightly flexed posture and then twist into extension. The patient should see the lines on the Flexbar move for feedback.
• There are different colors of Flexbars which coincide with the different resistance levels.
• The Wrist Roll and Mr. Wrister are performed in the same manner as the Flexbar, however a weight is added for resistance.
Wrist Extension with Theraband Flexbar
1 2
Wrist Flexion with theraband Flexbar
1 2
Wrist Flexion/Extension with Wrist Roll

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 41
Demonstration
Wrist Isotonic StrengtheningFlexbar / Wrist Roll
Isotonic Strengthening -PuttyCiser
• The PuttyCiser offers a variety of options.
• There are numerous tools available for exercise and the different colors of theraputty provide variations in resistance.
• Exercises with the PuttyCiser can be isometric or isotonic and this can be dictated by changes in the putty resistance.
• The only limitation with the PuttyCiser are with people suffering from arthritis. The grip required can sometimes aggravate their arthritis so it is important to monitor the patient for pain/swelling.
Wrist Extension with Puttyciser
Wrist Flexion with Puttyciser
Wrist ulnar Deviation with Puttyciser
Wrist Radial/Ulnar Deviationwith PuttyCiser

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 42
Wrist Ulnar Deviation with PuttyCiser
Demonstration
Wrist Isotonic StrengtheningPuttyCiser
Isotonic Strengthening -Velcro Board
• The Velcro Board offers another option for resistance training.
• There are 2 lines of velcro hook on the board, a narrow and a wide. The wider strip provides an increased level of resistance.
• For wrist flexion and extension, the roller with dowel handle is used. For patients who have a limited grip, a piece of pipe insulation can be added to increase the handle size. Coban can also be added to the handle to improve the texture of the handle to increase grip capability.
• The exercise can be graded differently. For instance, 1 pass forward and back is considered 1 repetition. The patient can perform 5-10 repetitions.
Wrist Flexion with Velcro Board
Wrist Extension with Velcro Board
Demonstration
Wrist Isotonic StrengtheningVelcro Board

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 43
Isotonic Strengthening - Plyoball
• The plyoball can be used for wrist strengthening but it does require the patient have acceptable grip strength in order to manage the plyoball.
• Most commonly, the 2 or 4 lbs. plyoball are used.
• For wrist extension, the patient can perform a plyoball hold with the forearm t d Th f 3 10 titi h ldi th l b ll f 15 60 dpronated. They can perform 3-10 repetitions holding the plyoball for 15-60 seconds.
• For flexion, the patient will supinate the forearm and perform a plyoball toss. Usually 10-20 repetitions will fatigue the patient.
• The exercise can also be graded lower using items such as a Nerf ball, tennis ball, or baseball.
• Patient can also use a basketball to dribble for wrist flexion. For wrist extension, patients can hold a football.
Wrist Extension with plyoball Hold
Wrist Flexion with Plyoball toss
Demonstration
Wrist Isotonic StrengtheningPlyoball
Isotonic Strengthening -Eccentric Extension / Flexion
• Some patients will require eccentric strengthening of the wrist. For diagnoses such as epicondylitis or TFCC injuries, these exercises are often better tolerated by the patient without increasing pain.
• For eccentric strengthening, the muscle being targeted is placed in a shortening position and the patient slowly lengthens the muscle to strengthenposition and the patient slowly lengthens the muscle to strengthen.
• For use with the Flexbar, the patient will stabilize the Flexbar with the affected hand and then twist the Flexbar with the unaffected hand. At that point, the patient’s affected hand will eccentrically allow the Flexbar to return to its resting position.
• For flexion, the unaffected hand will twist the Flexbar into extension, once the position is achieved, the affected hand will slowly allow the Flexbar to return to its resting state. This provides for eccentric wrist flexion. For extension it is the opposite.
Eccentric Wrist Extension with Flexbar
1 32

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 44
Eccentric Wrist Flexion with Flexbar
1 32
Eccentric Wrist Extension with Dumbbell
1 2
Eccentric wrist Flexion with Dumbbell
1 2
Demonstration
Wrist Eccentric Strengthening
Low-Load Stretchfor the Wrist
Wrist Extension Stretch
• For wrist extension, the patient is placed with the wrist over the edge of a table, bed, or wedge and the forearm is stabilized.
• A weight is applied to provide the stretch into an extended position while theinto an extended position while the patient “attempts” to relax.
• In the picture, a cuff weight is attached to a piece of Theraband to provide increased resistance and it is also easier to place on the patient for this stretch.
• Usually this stretch begins at 1 minute and is progressed.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 45
Wrist Flexion Stretch
• For wrist flexion, the patient is placed with the wrist over the edge of a table, bed, or wedge and the forearm is stabilized.
• A weight is applied to provide the stretch into an flexed position while the patient “attempts”an flexed position while the patient attempts to relax.
• In the picture, a cuff weight is attached to a piece of Theraband to provide increased resistance and it is also easier to place on the patient for this stretch. Patients can also simply hold a dumbbell.
• Usually this stretch begins at 1 minute and is progressed.
Chapter 6
The Hand
General Considerations
• For the hand, numerous structures can be involved with an injury or surgery. Before proceeding with any type of exercise, it is imperative to know all structures involved.
• Exercises for the hand can target the intrinsics, extrinsics, nerves, and also soft tissue structures.
Passi e motion of the hand sho lder incl de indi id al joints (MCP/PIP/DIP)• Passive motion of the hand shoulder include individual joints (MCP/PIP/DIP), composite motion, and the intrinsics.
• Strengthening of the hand can be performed but therapists must monitor the CMC of the thumb as well as the IP joints of the fingers for any type of inflammatory repsonse as this could be a sign of joint instability or arthritis.
Supplies Needed for this Chapter
• Dowel or Highlighter
• Finger Crutch and Finger Platter
• Theratubing (Red or Green)
• Calibrated Spring Loaded Grip
• Velcro Board
• Plyoball (2-4#)
• Rubber band
• Hand Helper
• Cando Via Hand Exerciser
• Digiflex (3-5#)
• Dowel with Slotted Weights
• Theraband Flexbar (Red or Green)
• PuttyCiser
• Theraputty (Soft or Medium)
Supplies Needed for this Chapter
• Digi-Extend
• ArchXerciser
• Chinese Spheres or Square Blocks
• Clothes Pin or Chip Clip
Passive Range of Motion
• When stretching a joint, the hand or joint should be positioned to eliminate resistive force from surrounding muscle-tendon systems.
• The segment proximal to the joint being mobilized should be stabilized while the corrective force should be applied to the segment distal to the joint being mobilizedthe joint being mobilized.
• As a general rule, the corrective force should be applied to the most distal portion of the segment distal to the joint being mobilized as this will provide a longer lever arm and increase the amount of force that can be transmitted to joint structures.
• Passive motion should be be slow with the structure being placed on stretch and held in the position for 5-10 seconds with each repetition.

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 46
Intrinsic Passive Stretching
1 2
Extrinsic Extensor Stretch
Extrinsic Flexor Stretch
Option A Option B
Extrinsic Flexor Stretch with foam roll
Extrinsic Flexor Stretch using Swiss ball
Active Range of MotionActive Range of Motion

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 47
Flexor Tendon MobilizationFlexor Tendon Mobilization
• Place-hold is the form of active exercise that applies the least amount of force on the tendon while producing the same tendon excursion as would occur with active motion.
• The fingers are passively placed in a position of flexion and the patient is asked to “hold” this position.
Place-Hold Exercise
• The wrist should be in neutral.
• Demo
Place and Hold
When using a prop, the patient is instructed to gently maintain contact but to not strain or squeeze in an attempt to hold the object. A styrofoam cup is excellent.
Blocking Exercises
• Blocking exercises can be used to isolate motion of a joint or tendon.
• Blocking exercises can be performed for the flexor or extensor tendons.
Blocking exercises do impart a certain amount of stress so they should• Blocking exercises do impart a certain amount of stress so they should only be used when repaired structures can withstand increased stress.
• Blocking can be performed with manual blocking or the use of an object such as the edge of a table, a pencil/pen, a dowel, or a Finger Crutch or Finger Platter.
• The Finger Platter is excellent for use with blocking exercises in the clinic or for home programs.
PIP Blocking
Block just proximal the PIP and have the patient actively flex.
PIP Blocking with Finger Crutch
and Finger Platter

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 48
DIP Blocking
Block just proximal the DIP Patient flexes DIP
DIP Blocking with Finger Crutch
and Finger Platter
Demonstration
Blocking Exercises
• Flexor tendon glides are a useful for of active motion exercises.
• They are commonly used following tendon repairs, fractures, trigger finger release, and carpal tunnel release surgeries due to their ability to effectively mobilize the flexor tendons and prevent adhesion formation.
Flexor Tendon Glides
• With the hook position, maximum gliding is achieved between the FDS/FDP tendons.
• With the full fist position, the FDP achieves maximum gliding with respect to sheath and bone as well as a substantial amount of gliding over the FDS tendon.
• With the straight fist position, there is maximum glide of the FDS with respect to the flexor sheath and bone.
• Maximum FPL gliding is obtained by flexing the IP and MP joints of the thumb fully
• Once the patient is able to perform the exercises with the wrist in neutral, instruct them to perform the same exercises with the wrist in extension to produce
Flexor Tendon Glides
p pmaximum total excursion.
Straight Fist Position

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 49
Full Fist Position
Hook Fist Position
Demonstration
Flexor Tendon Glides
• The muscle bellies of the FDS tendons are independent, allowing independent PIP flexion of each digit.
• Isolated FDS exercises are done by flexing one finger at a time at the PIP joint, with the uninvolved hand keeping the other fingers in extension.
Isolated FDS Glide
• This exercise produces gliding of the superficialis tendons not only with respect to other superficialis tendons, but also with respect to the profundus tendon which is rendered inactive when the other 3 profundus tendons are held in extension.
• Demo
FDS Glides
Extensor Tendon Mobilization• Restoration of normal tendon glide in the extensor tendons presents a unique
challenge.
• At the finger level, the EDC, interossei, and lumbrical tendons form a complex extensor mechanism.
• Adhesions can form at any point along the system, limiting active and passive finger flexion as well as active finger extension.
• The specific exercise selected to facilitate extensor tendon glide depends on the location of the adhesions.
• Lack of full active extension at the MP joint indicates an adhesion of the EDC, which is the sole extensor of the MP.
• An extensor lag present at the PIP and DIP joints indicates adhesion of the extensor expansion, composed of the EDC, interossei, and lumbricals.
• Demo

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 50
EDC Glide
EDC Glide with Dowel
The patient grasps an object to isolate the MCP
Patient actively extends the MCP
Reverse Blocking
Block just proximal the PIP Patient extends the PIP/DIP
Reverse Blocking with Finger Platter
StrengtheningStrengthening
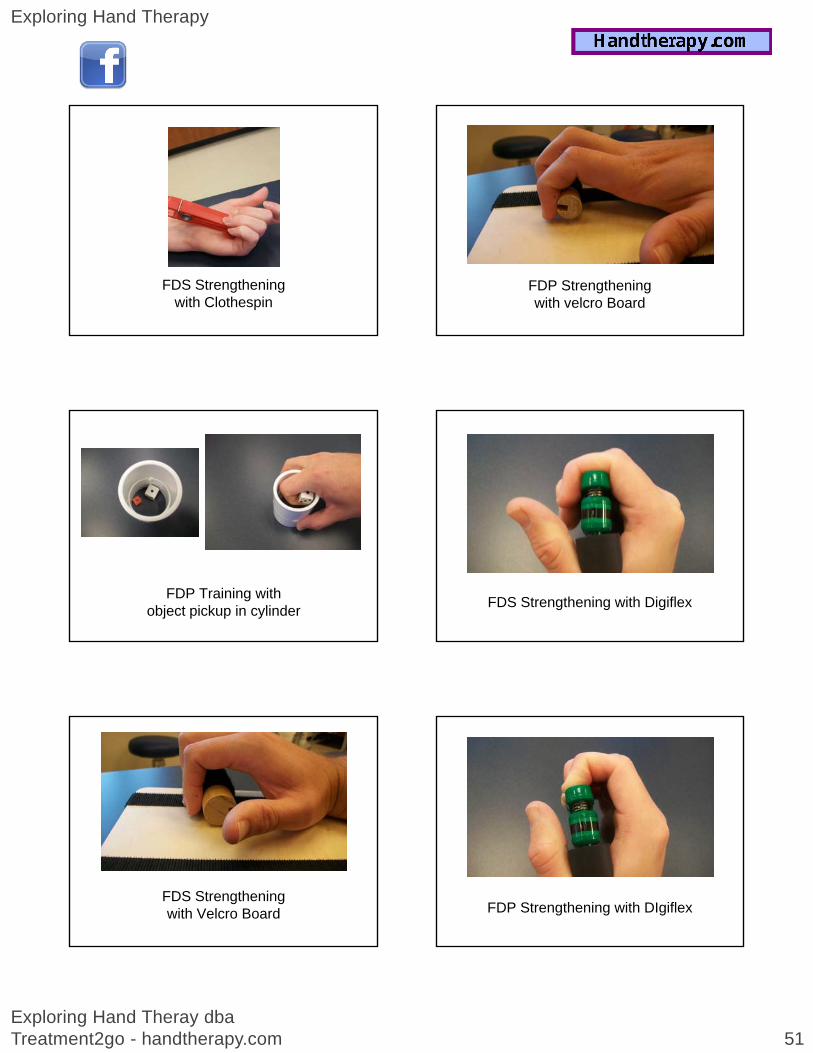
Strengthening - Flexor Tendons
• When strengthening the flexor tendons, the focus of a specific tendon depends on motion at a specific joint level.
• For the FDS, the exercise focuses on the PIP joint while the FDP focuses on the DIP joint.
• Strengthening of the flexor tendons can be accomplished by manual resistance• Strengthening of the flexor tendons can be accomplished by manual resistance from the therapist but it can also be accomplished from tools such as Theraputty, Digiflex, CanDo Via Exerciser, Hand Helper, ArchXerciser, Velcro Board, Clothespins, Power Web, and the PuttyCiser.
• Demo
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 51
FDS Strengthening with Clothespin
FDP Training with object pickup in cylinder
FDS Strengthening with Velcro Board
FDP Strengthening with velcro Board
FDS Strengthening with Digiflex
FDP Strengthening with DIgiflex

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 52
FDP Strengthening with Cando Via Exerciser
FDP Strengthening with Hand Helper
1 2
FDP Strengthening using Archxerciser
FDS Strengthening with Archxerciser
FDS Strengthening with Theraputty
FDP Strengthening with Theraputty
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 53
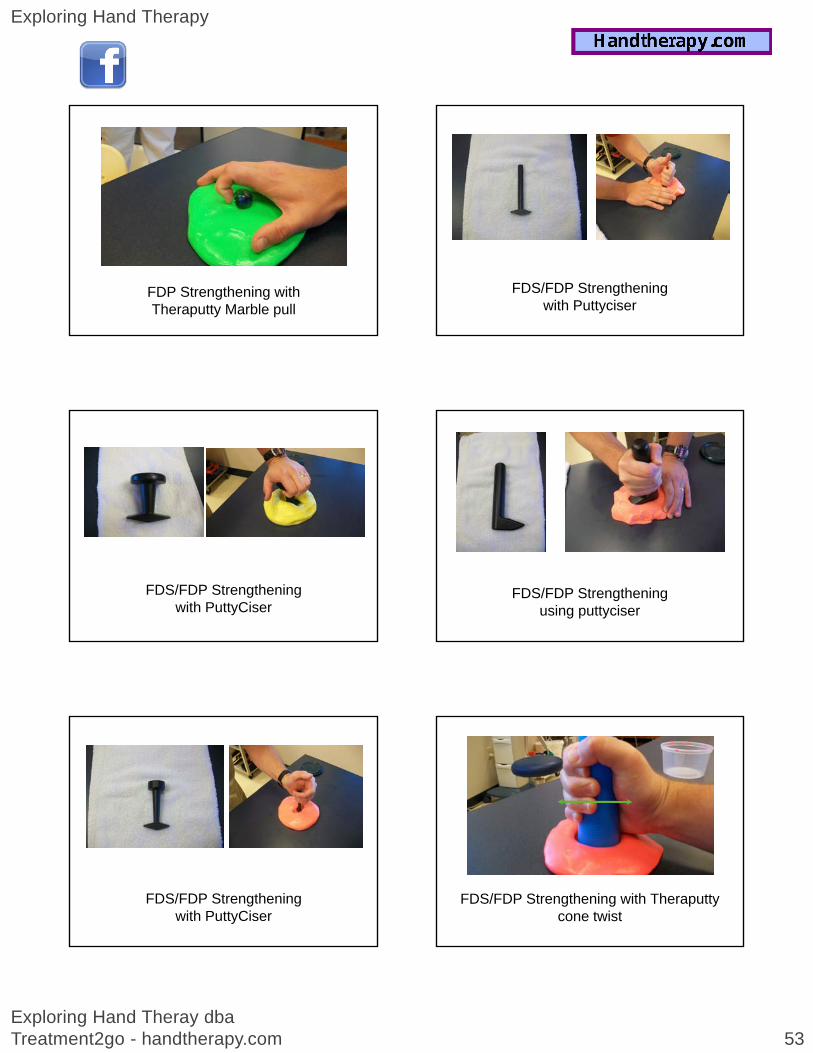
FDP Strengthening with Theraputty Marble pull
FDS/FDP Strengthening with PuttyCiser
FDS/FDP Strengthening with PuttyCiser
FDS/FDP Strengthening with Puttyciser
FDS/FDP Strengthening using puttyciser
FDS/FDP Strengthening with Theraputty cone twist

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 54
FDS/FDP Strengthening with Power Web
FDS/FDP Strengthening with dowel & slotted weights
Strengthening - Extensor Tendons
• When strengthening the extensor mechanism, the focus depends on motion at a specific joint level.
• For the EDC, the exercise focuses on extension of the MCP joint with the IPs flexed.
• For the intrinsic muscles of the extensor mechanism, the exercises focus on extension of the PIP and DIP joints and are most effective with the MCP in flexion.
• Strengthening of the extensor can be accomplished by manual resistance from the therapist but it can also be accomplished from tools such as Theraputty, Velcro Board, Finger Weights, and the Digi-Extend.
• The Digi-Extend is excellent for use in the clinic and for home program use.
• Demo
With the velcro board, the patient actively extends the MCP while maintaining the PIP/DIP in flexion.
The PIP/DIP may be taped with coban to isolate the motion of the MCP.
EDC Strengthening with velcro board
EDC Strengthening using theraband
1 2
EDC Glide using Finger Weights

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 55
Extensor Intrinsic Strengtheningwith velcro board
Extensor Intrinsic Strengtheningusing finger Weights
EDC Strengthening with Digi-Extend
1 2
Extensor Strengthening with Digi-Extend
Strengthening - Grip
• Strengthening of grip can be accomplished from tools such as Theraputty, Velcro Board, Eggserciser, Foam Ball, Hand Helper, Digiflex, CanDo Via, Stovall Calibrated Hand Grip, Plyoball, and Dowel with Slotted Weights.
• When choosing an exercise for increasing grip strength, the therapist must consider the amount of finger flexion available, grip comfort, presence of arthritis or joint instability and the amount of grip desiredor joint instability, and the amount of grip desired.
• For patients with arthritis, grip strengthening should be done with the least amount of stress to the joints of the hand.
• Demo
Grip using Memory Foam Ball
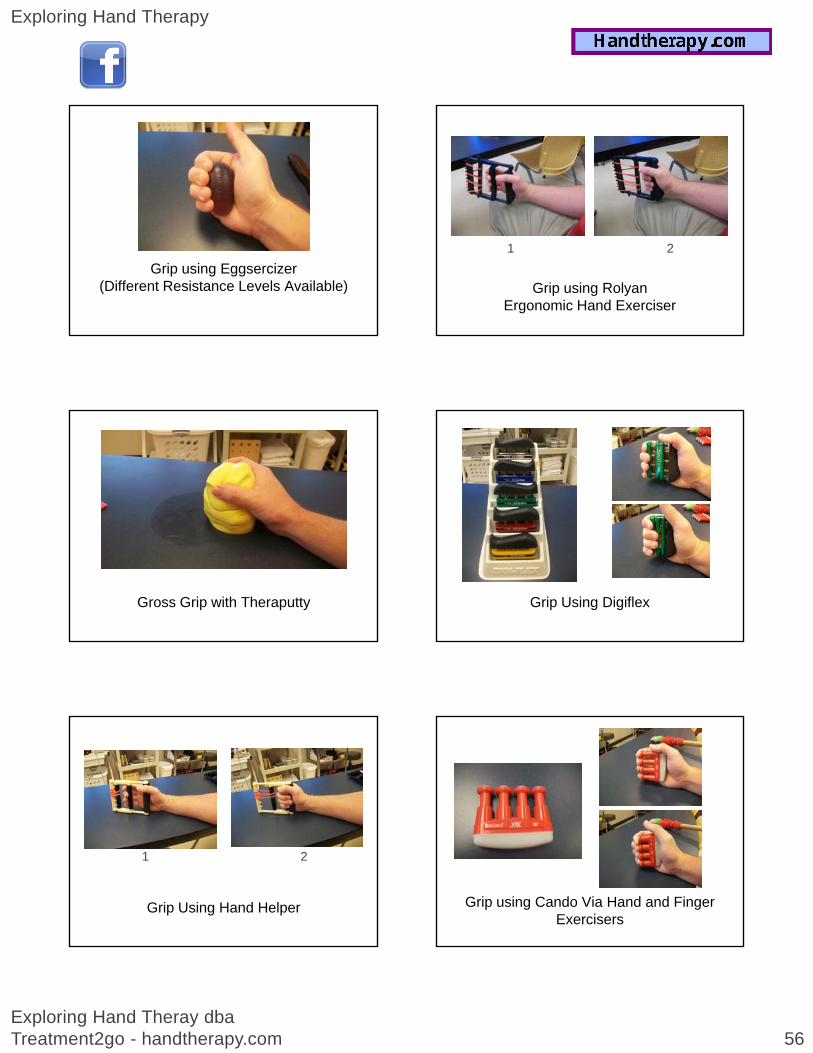
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 56
Grip using Eggsercizer(Different Resistance Levels Available)
Gross Grip with Theraputty
Grip Using Hand Helper
1 2
Grip using Rolyan Ergonomic Hand Exerciser
1 2
Grip Using Digiflex
Grip using Cando Via Hand and Finger Exercisers

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 57
Grip using Stovall Calibrated Hand Grip
1 2
Sustained Grip with Plyoball hold
Sustained Gripwith dowel & slotted weights
Chapter 7 -- Strengthening - Intrinsics
• Strengthening of the intrinsics can be accomplished from tools such as Theraputty, Eggserciser, Hand Helper, Stovall Calibrated Hand Grip, PuttyCiser, Clothespins, Power Web, and Rubberbands.
• Demo
Intrinsic Strengthening with Hand Helper
1 2
Intrinsic Strengthening withCalibrated Hand Grip
1 2

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 58
Intrinsic Strengthening with Puttyciser
Intrinsic Strengthening with Puttyciser
Intrinsic Strengthening with Puttyciser
Intrinsic Strengthening with Puttyciser
Intrinsic Strengthening with Theraputty Drag
Intrinsic Strengthening with Theraputty

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 59
Intrinsic Strengthening with Rubberband
Intrinsic Strengthening with Rubberband
Intrinsic Strengthening with Rubberband
Intrinsic Strengthening with Clothespin
Intrinsic Strengthening with Clothespin
Intrinsic Strengthening with Theraputty

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 60
Intrinsic Strengthening with Power Web
Strengthening - Thumb
• Strengthening of the intrinsics can be accomplished from tools such as Theraputty, Hand Helper, Stovall Calibrated Hand Grip, PuttyCiser, Clothespins, Digi-Extend, Ice Cream Scoop, Power Web, and Rubberbands.
• Demo
Lateral Pinch with Clothespin
Radial Abduction with Rubberband
Thumb Strengthening withCalibrated Hand Grip
1 2
Thumb Adduction withCalibrated Hand Grip
1 2

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 61
Thumb Abduction and Extension with Digi-Extend
1 2
Thumb Strengthening with Flexbar
Thumb Strengthening with Puttyciser
Thumb Flexion / Adductionwith Puttyciser
THUMB STRENGTHENING WITH PUTTYCISER
THUMB STRENGTHENING WITH PUTTYCISER

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 62
THUMB ADDUCTION WITH PUTTYCISER
LATERAL PINCH WITH ICE CREAM SCOOP
PINCH WITH OBJECT PICKUP USING TWEEZERS
Lateral PINCH WITH THERAPUTTY
TRIPOD PINCH WITH THERAPUTTY
TIP PINCH WITH THERAPUTTY

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 63
Chapter 9FINE MOTORFINE MOTOR
OBJECT MANIPULATION
SQUARE BLOCK MANIPULATION
SPHERICAL MANIPULATION
SINGLE OBJECT PICK UP
OBJECT PICK UP
GROSS GRASP AND Manipulation of Media

Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 64
Chapter 10Chapter 10
Tips from the Field
Answers to Common Questions
Does it help to apply heat or ice before exercises?
• Heat can be applied but with caution. Heat applied for longer than 10 minutes can decrease muscle endurance causing early fatigue with exercise.
• Due to this, if the goal of exercise is to increase strength, heat may not be indicated in order to achieve maximum results. If the goal of exercise is for stretching or passive motion, heat may be beneficial.
• If the goal of exercise is to increase ROM and heat is applied, the exercise needs to be performed during or immediately following the heat in order to be effective.
• Ice applied for 5 minutes has been shown to increase muscle strength during exercises, however, ice applied for >5 minutes has been shown to limit the effectiveness of exercises for strengthening.
• Heat should also be used with caution when pain is present or there is an acute inflammatory response as this could aggravate patient’s symptoms or place them at a greater risk for tissue injury.
How do you choose which exercise to perform?
• Following the initial assessment, a problem list is formed based on the objective findings and patient complaints.
• Based on the patient’s diagnosis, related precautions, medical history, objective findings, and unique functional status, exercises are selected.findings, and unique functional status, exercises are selected.
• Each exercise should be selected to target a specific limitation. If an exercise has no purpose or no longer contributes to the patient’s progression then it should no longer be performed.
Does the order of exercises matter?
• When formulating the exercise program consider the role of each exercise selected.
• If the exercise is for ROM or stretching, the exercises should proceed in the progression of the targeted structures. For example, in the hand intrinsic stretching could be performed before passive or active motion at the individual IP
f ffjoints of the hand in order to contribute to more effective composite motion.
• In the shoulder, stretching exercises should be performed before AA/AROM exercises. These exercises would be performed before strengthening exercises.
Should passive range of motion be performed before or after other exercises?
• If active range of motion or strengthening exercises are to be performed as part of the exercise program, then passive range of motion should be performed first to be the most beneficial.
• If the patient has muscle spasms, guarding, or pain, then they would most likely benefit from passive range of motion at the end of the therapy session as other exercises or modalities could decrease symptoms and make passive motion more tolerable and effective.
• If edema is present, measures to address edema should be performed first followed by active motion (if allowed) followed by passive range of motion.
• In some circumstances passive range of motion can be performed at the start and end of the therapy session.
Exploring Hand Therapy
Exploring Hand Theray dba Treatment2go - handtherapy.com 65
How do you determine the amount of sets and repetitions for an exercise?
• Much depends on the tolerance of the patient. Whether the exercise is for range or for strengthening, the patients tolerance should be assessed. Another factor to consider is the purpose of the exercise: range of motion, passive stretching, low-load stretching, or strengthening.
• For range of motion and passive stretching consider the stage of healing, status of affected tissues and the focus of the exercise For delicate structures therapistsaffected tissues, and the focus of the exercise. For delicate structures, therapists may for 2 sets of 5 repetitions or simply 1 set of 10 repetitions. If more aggressive stretching is needed, the sets and reps may be increased to 2-3 sets of 10-15 repetitions.
• For strengthening, the intent of the exercise is to fatigue the target muscle(s). Because of this, an exercise may cause fatigue with 1 set of 10 repetitions or it may not occur until 3 sets of 15 repetitions.
• For low-load stretching, the exercise should be performed for a minimum of 30 second intervals to be effective. The maximum for a low-load stretch depends heavily on the amount of force.
Does the speed of exercise performance matter?
• For all exercises to be effective, they need to be slow and controlled.
• Passive range of motion or stretching exercises should take the target tissue to the point of stretch and be held in this position for 10 secondspoint of stretch and be held in this position for 10 seconds.
• Active range of motion and strengthening exercises should be performed slowly and held for 3-7 seconds to achieve maximum muscle contraction and build strength and endurance.
• Endurance training requires a consistent speed in order to be effective.
• Plyometric training is the only exception to this and it requires quick motions.
Should exercises be painful?
• No exercise should ever be painful.
• The old saying of “No pain, no gain” is no longer considered valid.
• Exercises may elicit soreness, muscle spasms, cramping, or a tightness whichExercises may elicit soreness, muscle spasms, cramping, or a tightness which can be uncomfortable but they should never be considered PAINFUL.
• Be sure to explain the difference between soreness and pain to the patient.
When should exercise(s) be stopped, placed on hold, or discontinued?
• Exercises that are causing increased pain or edema should be stopped.
• Exercises that cannot be performed due to joint instability should be stopped.
• Exercises that are not effective for their intended purpose should be stopped or discontinued.
• If a patient has a change in status reporting increased pain, swelling, or instability with exercises or following treatment then exercises should be stopped and revised.
• If a patient’s pain level increases, exercises should be placed on hold until the patient’s pain is able to be managed.
FINAL ThoughtsFINAL Thoughts...
References
• The Athlete’s Shoulder - James Andrews and Kevin Wilk. Churchill Livingstone, 1994.
• Sports-Specific Rehabilitation - Robert Donatelli. Churchill Linvingstone, 2007
• Concepts in Hand Rehabilitation - Barbara Stanley and Susan Tribuzi. F.A. DavisConcepts in Hand Rehabilitation Barbara Stanley and Susan Tribuzi. F.A. Davis Company, 1992
• Fundamentals in Hand Therapy: Clinical Reasoning and Treatment Guidelines for Common Diagnoses of the Upper Extremity - Cynthia Cooper. Mosby, 2007
• www.wikipedia.org


















