THERAPEUTIC CANCER VACCINES Cancer Immunology and Immunotherapy Center St. Savas Cancer Hospital.
53
THERAPEUTIC CANCER VACCINES THERAPEUTIC CANCER VACCINES Cancer Immunology and Immunotherapy Center St. Savas Cancer Hospital
-
Upload
stewart-allison -
Category
Documents
-
view
221 -
download
2
Transcript of THERAPEUTIC CANCER VACCINES Cancer Immunology and Immunotherapy Center St. Savas Cancer Hospital.

THERAPEUTIC CANCER VACCINESTHERAPEUTIC CANCER VACCINES
Cancer Immunology and Immunotherapy CenterSt. Savas Cancer Hospital

To activate T cell responses against TAAsTo activate T cell responses against TAAsthat are of sufficient magnitude to eliminatethat are of sufficient magnitude to eliminate
tumor and prevent its recurrencetumor and prevent its recurrence
Why we vaccinate against cancer? Why we vaccinate against cancer?

Cancer immunoediting reoccurs during immunotherapiesCancer immunoediting reoccurs during immunotherapies
vacstart
vacend
Generate IR
Equilibrium
Anti-tumor response
Reduced tumor growth ratesReduced tumor growth rates
Increased OSIncreased OS
Escape(recurrences)
M e m o r yM e m o r y
Anti-tumor response
Elimination
tumortumorburdenburden conventional therapyconventional therapy

Cytotoxicgranules
Tumor cells can be recognized and destroyed by CD8Tumor cells can be recognized and destroyed by CD8++ T cells, T cells,thus a therapeutic vaccine needs to activate T cells recognizing tumor antigensthus a therapeutic vaccine needs to activate T cells recognizing tumor antigens
FasLFasL FasFas
perforin
CD8CD8++ tumortumor
1. Low numbers2. Low activation3. Short-lived immunity4. Wrong patient selection
Poor clinicaloutcome

How can we change this?How can we change this?
• Optimize vaccination methods
to yield highly activated tumor
specific CTLs in high numbers
and of long-lasting anti-tumor activity
• Combinatorial treatmentsImmune suppression
• Tregs, MDSCs, enzymes/cytokines etc.
Cytotoxicgranules
TumorTumor cellscells cancan bebe recognizedrecognized andand destroyeddestroyed byby CD8CD8++ T T cellscells,,thusthus a a therapeutictherapeutic vaccinevaccine needsneeds toto activateactivate T T cellscells recognizingrecognizing tumortumor antigensantigens
FasLFasL FasFas
perforin
CD8CD8++ tumortumor
1. Low numbers2. Low avidity3. Short-lived immunity
Poor clinicaloutcome
• Vaccinating patients with low tumor volume

Optimizing therapeutic cancer vaccinesOptimizing therapeutic cancer vaccines
tumorantigen
adjuvant vehicle
Multiple CTL peptidesfrom various tumor Ag restricted by various alleles.Helper peptides also needed
Viral vectorsDCs ?

Why helper peptides?Why helper peptides?
• CD8+ induction phase and CD8+ T cell memory
• Effector phase of CD8+ T cell at the tumor site

How to produce polyvalent vaccinesHow to produce polyvalent vaccines
1. Synthetic long peptides encompassing CTL + TH epitopes
2. Mixtures of synthetic peptides representing immunogenic CTL + TH epitopes
3. Recombinant proteins
Synthetic long peptides encompassing CTL + TH epitopes

HER-2 (776-790) is a promiscuous helper peptide that containsHER-2 (776-790) is a promiscuous helper peptide that contains multiple HLA-DR-specific binding motifs multiple HLA-DR-specific binding motifs
776 GVGSPYVSRLLGICL 790
DRB1*0101, DRB1*1501, DRB1*0404, DRB1*0401, DRB1*1101, DRB1*1302,DRB1*0701, DRB1*0802, DRB1*0901, DRB4*0101, DRB5*0101
Functional assaysDR1(High), DR3(Low), DR4(Intermediate-High), DR7(High), DR8(High), DR15(High), DR13(High), DR51(Low), DR52(Low), DR53(High)
Sotiriadou NN et al. 2001 Brit. J Cancer 85(10):1527 Salazar, LG et al. 2003 Clin Cancer Res 9:5559 http://www.syfpeithi.de
A2.1
A11, A3 A24
Syfpeithi
Syfpeithi

HER-2(776-790) is immunogenic in vivo and has antitumor activityHER-2(776-790) is immunogenic in vivo and has antitumor activity(Voutsas I et al, IJC, 2007,121:2031; Gritzapis AD et al, (Voutsas I et al, IJC, 2007,121:2031; Gritzapis AD et al, Cancer Res. 2006Cancer Res. 2006, , 66:545266:5452; Gritzapis AD et al, Cancer Res, 2010, ; Gritzapis AD et al, Cancer Res, 2010, 70:268670:2686))
Ii-key/HER-2(776-790) hybrid (AE37) is more immunogenic than native HER-2(776-790)Ii-key/HER-2(776-790) hybrid (AE37) is more immunogenic than native HER-2(776-790)(Voutsas I et al, IJC, 2007,121:2031;(Voutsas I et al, IJC, 2007,121:2031; Gillogly ME et al, Gillogly ME et al, CIICII,, 2004 2004,,53:49053:490 )
A2.1/DR1/neuT+
TUBO.A2
HER-2(435-443)HER-2(435-443)+ HER-2(776-790)
HER-2(435-443)
0 25 50 75 1251000
50
100
150
200
250
Days
Tu
mo
r si
ze (
mm
2)
2
HER-2(435-443) + HER-2(776-790)
00
50
100
150
200
250
DaysT
um
or
size
(m
m)
25 50 75 125100 150 175 200
rechallengeTUBO.A2
APC
APC+HER-2(776-790)
APC+HER-2(776-790)+aDR
ELISPOT-IFNγ
020406080100120140160180200
no
IFN
γ sp
ots
(5x1
05 C
D4+
ce
lls)
cpm
Proliferation
0
4000
8000
12000
16000
20000
0
10
20
30
40
50
60
70
20:1 10:1 5:1
% s
peci
fic
51C
r re
leas
e
CD8+
CD8+ + HER-2 CD4+
CD8+ + Ii-key/HER-2 CD4+
E:T ratio
Activates CD4+ T cellsin DR4-transgenic animals
Days
Tu
mor
siz
e (m
m2 )
Cytotoxicity
CD8+
CD8+ + HER-2 CD4+
CD8+ + Ii-key/HER-2 CD4+

Vaccinating with Ii-key/HER-2(776-790)Vaccinating with Ii-key/HER-2(776-790)(AE37)(AE37)
HER-2/neuHER-2/neu++ prostate cancer patients. prostate cancer patients.A phase I studyA phase I study

Vaccination scheduleVaccination schedule(Perez SA et al. Clin Cancer Res 2010, 16(13):3495)(Perez SA et al. Clin Cancer Res 2010, 16(13):3495)
Vac(id): 0.5 ml HER-2(776-790) (500 μg)+GM-CSF (60 μg) x 2
Pre-DTH
Vac1+
BD
BD: blood drawingDR: dermal reaction
months0 1 2 3 4 5 6
Post-DTH
→2d (DR) →2d (DR) →2d (DR) →2d (DR) →2d (DR) →2d (DR)
Vac2+
BD
Vac3+
BD
Vac4+
BD
Vac5+
BD
Vac6+
BD
vac DTH
12Longterm

Durable immunity inducedDurable immunity inducedby the Ii-key/HER-2(776-790) vaccineby the Ii-key/HER-2(776-790) vaccine
pat
ien
ts w
ith
res
pon
se (
%)
IFN
γ sp
ecif
ic s
pot
s/10
6 PB
MC
HER-2(776-790)
100
80
60
40
20

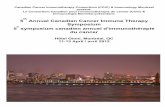
Immunological responses and toxicityImmunological responses and toxicity
Toxicity
T cell subset responses
23
0
5
10
15
20
25
No
of
res
po
ns
es
ICSCD4+γ+
orCD8+γ+
DTH γ+ ICS vs
DTH
Assay
23 23
19
Correlation between in vitro and in vivo immunologicalCorrelation between in vitro and in vivo immunologicalresponses in prostate cancer patients immunized responses in prostate cancer patients immunized
with Ii-key/HER-2(776-790)with Ii-key/HER-2(776-790)

Biological and immunological parameters Biological and immunological parameters pre vac, post vac, and at long termpre vac, post vac, and at long term

Other trials using AE37Other trials using AE37
1. Phase I, NN, disease-free breast cancer patients(completed standard therapies) (Holmes JP et al. JCO 2008, 26:3426)
2. Phase II, randomized, single-blinded, NP, NN (at high risk for recurrence),disease free breast cancer patients (Peoples GE)
3. Phase II, randomized, single-blinded, non-metastatic, castrate resistantprostate cancer patients in combination with anti-androgen treatment(preparing)

How to produce polyvalent vaccinesHow to produce polyvalent vaccines
1. Synthetic long peptides encompassing CTL + TH epitopes
2. Mixtures of synthetic peptides representing immunogenic CTL + TH epitopes
3. Recombinant proteins

HPV-E6 1 325019
65418055
957110985
12091140109
158127
Vaccine composition
HPV-E7 1 355622
7743
9864
Adjuvant: Montanide ISA-51
Vaccination against HPV-16 oncoproteinsVaccination against HPV-16 oncoproteinsfor vulvar intraepithelial neoplasia for vulvar intraepithelial neoplasia
(Dutch Cancer Society, Leiden University) (Kenter GG et al, N Engl J Med 2008 361:1838)

Vaccine schedule
vaccinations q3w x 3-4 Each vaccine consisted of: 3.9 mg of peptide (total 0.3mg x 13) in 2.8 ml PBS
Kenter GG et al, N Engl J Med 2008;361:1838
Clinical Results at 24 mo after vaccination
Complete responses: 9/30Partial responses: 6/30

Correlation between immunologic and clinical responsesCorrelation between immunologic and clinical responses(Kenter GG et al, N Engl J Med 2009 361;19)(Kenter GG et al, N Engl J Med 2009 361;19)

Multi-peptide vaccination with IMA 901 in advanced RCCMulti-peptide vaccination with IMA 901 in advanced RCC(Immatics Biotech, GmbH) (Walter S et al. Nat. Med. 2012;18:1254)(Immatics Biotech, GmbH) (Walter S et al. Nat. Med. 2012;18:1254)
A therapeutic cancer vaccine consisting of 10 synthetic tumor-associated CTL peptides,identified by:
• isolating HLA-peptide complexes from primary RCC specimens
• determining their sequences by MS
• selection based on over-expression of their encoding genes
• immunogenicity tests
Plus a TH (Pan DR class II) peptide

Study designStudy design
Patients withAdvanced RCC
(n=68)
Randomization1
1
cyclo+IMA901+GM-CSF (i.d)
placebo+IMA901+GM-CSF (i.d)
17 vaccinations over 9 months

Immune response and clinical outcomeImmune response and clinical outcome((Walter S et al. Nat. Med. 2012;18:1254Walter S et al. Nat. Med. 2012;18:1254))
Cyclo+IMA-treated patientstotal patients
Cyclo+IMA
IMA

Phase III study – IMPRINT Phase III study – IMPRINT (Rini B et al. ASCO 2011)(Rini B et al. ASCO 2011)
IIMA 901 MA 901 MMulti-ulti-PPeptide vaccine eptide vaccine RRandomized andomized INTINTernational ernational
Advanced/Metastatic RCC
STRATIFICATION• Risk (low vs intermediate)• Region (European vs US)• Nephrectomy (yes vs no)
Randomization
Cyclo + IMA901 + sunitinib Sunitinib
Cyclo: 300 ng/m2
IMA901: 10 vaccinations over 4 monthsSunitinib: 5 cycles
3 2
Sunitinib 1st cycle
PRIMARY ENDPOINT• OS
SECONDARY ENDPOINTS• PFS-Safety• Immunomonitoring
Recruiting
330 patientsEnd of enrolment: 2nd half 2012

How to produce polyvalent vaccinesHow to produce polyvalent vaccines
1. Synthetic long peptides encompassing CTL + TH epitopes
2. Mixtures of synthetic peptides representing immunogenic CTL + TH epitopes
3. Recombinant proteins
soluble PulsedDCs
Recombinantviruses

MAGE-A3 plus AS15 immunostimulant (TLR-L) in patients with NSCLC MAGE-A3 plus AS15 immunostimulant (TLR-L) in patients with NSCLC (Pujol J-L et al. JCO 2012;30(15):7013(Pujol J-L et al. JCO 2012;30(15):7013
(suppl. May20); ASCO Annual Meeting Proceedings)(suppl. May20); ASCO Annual Meeting Proceedings)
NSCLC• stage IB (T2N0) and stage II (T1-2N1), T3N0)• MAGE-A3 by qPCR• Complete resection• Recovered (DS 0-1)
Stratified• Stage IB vs II• Squamous vs non-squamous• LN sampling vs dissection
R1
2
MAGE-A3Administration 300 μg im.• Induction q3wx5• Maintenance q3wx8• Total 27 months
PlaceboSame schedule
Double-blindn=122

HR=0.73one-sided logrank test p=0.093
Impact of predictive gene signature on disease-free survivalImpact of predictive gene signature on disease-free survival
DFS: Interval from the date of surgical resection to the date of recurrence OR death,irrespective of cause of deathHR: Hazard ratio calculated by Cox analysis
Total population
HR=0.57one-sided logrank test p=0.099
HR=0.78one-sided logrank test p=0.387
Gene signature negative Gene signature positive

Active immunization toward the MAGE-A3 antigen in patientsActive immunization toward the MAGE-A3 antigen in patientswith metastatic melanoma with metastatic melanoma (Kruit W et al. ASCO 2011, JCO 2011;29(15):8535 (May 20 Suppl.))(Kruit W et al. ASCO 2011, JCO 2011;29(15):8535 (May 20 Suppl.))
Open-labeled/non-controlled
MAGE-A3+, unresectable stage III-IV M1acutaneous Melanoma
Rn=36 n=36
MAGE-A3administration 300 mg imq3wx5→q3mx24 max
+ +
TLR-4L TLR-4L+
TLR-9L
=AS02B=AS15
CR n=0 n=3PR n=1 n=1IR 21% 69%Med OS 19 months 33 months

3 6 9 12 15 18 21 24 27 30
Time (months)
DF
S
HR=0.31
Efficacy of MAGE-A3 in metastatic melanoma is associated Efficacy of MAGE-A3 in metastatic melanoma is associated to immune microenvironmentto immune microenvironment
GS(+) (n=21):10.3 monthsGS(-) (n=14):2.3 months

Phase III study – MAGRIT (Vansteenkiste J. et al. ASCO 2007) Phase III study – MAGRIT (Vansteenkiste J. et al. ASCO 2007) MMAGE-A3 as AGE-A3 as AAdjuvant Non-Small Cell Lundjuvant Non-Small Cell LunGG Cance CanceRR
IImmunommunoTTherapyherapy
Resectable NSCLC
Surgery
Pathological stage IB, II, IIIA
No chemo Up to 4 cycles ofplatinum-based chemo
Randomization Randomization
MAGE-A3 + AS15 placebo MAGE-A3 + AS15 placebo
2,270 patients double-blind, randomized trial
Primary endpoint: Disease free survivalSecondary endpoint: Validation of gene signature predictive of response to therapy

Phase III, double blind randomized trial– DERMA Phase III, double blind randomized trial– DERMA (Kirkwood JM et al. J Clin. Oncol. ASCO Proceedings 2011, 29:Abstr. TPS 232)(Kirkwood JM et al. J Clin. Oncol. ASCO Proceedings 2011, 29:Abstr. TPS 232)
Resectable regionallyadvanced melanoma
Stratification• Stages (IIIB, IIIC)•TNM nodal category (N1-N3)• Primary category (Tx-0, T1-2, or T3 or T4)• Prior treatment (IFN, anti-CTLA4)
Randomization
Placebo
2 1
PRIMARY ENDPOINT• DFS
MAGE-A3+AS15
SECONDARY ENDPOINT• OS, safety, health-related quality of life, validation of gene signature associated with MAGE-A3+AS15 benefit
Schedule: q3w x 5 + q12w x 8
Recruiting
1300 patients
Surgery

2. rec. PAP/GM-CSF 2. rec. PAP/GM-CSF pulsedpulsed on mature DCs on mature DCs Sipuleucel-T (ProvengeSipuleucel-T (Provenge®®) (Dendreon) ) (Dendreon)
Leukapheresis Monocytes + PAP/GM-CSF DC40 hr
infuse
CTL attack tumor
cells
In vivoT cell
activation
CD4+
CD8+
Randomized Phase 3 IMPACT TrialRandomized Phase 3 IMPACT Trial ( (Kantoff P et al, N Engl J Med 2010 363:411)Kantoff P et al, N Engl J Med 2010 363:411)
Asymptomatic or Minimally Symptomatic Metastatic
Castrate Resistant
Prostate Cancer (N=512)
Placebo Q 2 weeks x 3
Sipuleucel-T Q 2 weeks x 3
2:1
SURVIVAL
Primary endpoint: Overall SurvivalSecondary endpoint: Time to Objective Disease Progression

IMPACT Overall SurvivalIMPACT Overall Survival
0 6 12 18 24 30 36 42 48 54 60 660
25
50
75
100
Per
cen
t S
urv
ival
Survival (months)
P = 0.032 (Cox model)HR = 0.775 [95% CI: 0.614, 0.979]
Median Survival Benefit = 4.1 Mos.
Sipuleucel-T (n = 341)Median Survival: 25.8 Mos.
Placebo (n = 171)Median Survival: 21.7 Mos.
23.1%
31.7%

Open label, randomized phase II study:Open label, randomized phase II study:sequencing of sipuleucel-T and ADT on immune responsessequencing of sipuleucel-T and ADT on immune responses
in patients with prostatic cancer in patients with prostatic cancer (Antonarakis S et al. ASCO 2011, 29:Abstr.TPS(Antonarakis S et al. ASCO 2011, 29:Abstr.TPS 189) 189)
Prostate Ca patients with rising PSApost-primary therapy, non-metastatic
STRATIFICATION• PSADT (≤ 3 mo vs >3 mo)• Type of primary therapy (RP or XRT vs RP+XRT)
Randomization
Sipuleucel q2w x 32wks ADT
ADT 3mo Sipuleucel
n=30 n=30
PRIMARY ENDPOINT• immune responses to PA2024 and PAP during Sipuleucel-T and after at wks 2, 6, 12 and months 6, 9, 12, 15, 18• PSA/Testosterone: every 3 months until month 18
SECONDARY ENDPOINT• Safety• Time of PSA recurrence• Change in PSADT
Accrual Dec. 2011

Randomized, open label phase III study: sipuleucel-T plus ADT vs ADTRandomized, open label phase III study: sipuleucel-T plus ADT vs ADT in patients with prostate cancer in patients with prostate cancer (Fizazi K et al. J Clin. Oncol. ASCO 2011, 29:Abstr.TPS 188)(Fizazi K et al. J Clin. Oncol. ASCO 2011, 29:Abstr.TPS 188)
Metastatic, androgen-dependent(hormone sensitive) prostate cancer
Randomization
Sipuleucel-T + ADTn=842
ADT only n=842
1 1
PRIMARY ENDPOINT• overall survival
SECONDARY ENDPOINTS• Safety• Time to castration resistance• Chemotherapy free survival
Accrual Dec. 2011
ADT until castration-level testosterone

The PSA-TRICOM vaccine: PSA LFA-3 ICAM-1 B7-1
COCOstimulatory MMolecules
TRITRIad
Pox viruses1. Replicate within the cytoplasm of infected cells. Do not insert their genetic sequences in the host genome2. Infect DCs and tumor cells3. Large genome (can accommodate large transgenes)4. Engineered recombinants are stable
3. Recombinant proteins 3. Recombinant proteins encodedencoded by poxviruses by poxviruses

PROSTVAC: PSA-TRICOM (Therion Biologics Corporation)PROSTVAC: PSA-TRICOM (Therion Biologics Corporation)

PROSTVAC: PSA-TRICOM (Therion Biologics Corporation)PROSTVAC: PSA-TRICOM (Therion Biologics Corporation)

Poxviral-based PSA targeted immunotherapy in metastatic castration resistant prostate cancerPhase II randomized, controlled, double blind study(NCI study) ((NCI study) (Kantoff P et al, J Clin Oncol 2010, 28:1094)Kantoff P et al, J Clin Oncol 2010, 28:1094)
Vaccinia-PSA-Tricom
Fowlpox-PSA-Tricom
0 1/2 2 3 4 51
GM-CSF
months
prime
boosts
Placebo: empty vector
Heterologous prime-boost regimen
On PSA-TRICOM 25.1 8.5On placebo 16.6
median OS (mo) median OS benefit (mo)
p=0.006

0
5
10
15
20
25
30
35
40
All patients Patients withHalabi <18 mo
Patients withHalabi >18 mo
OS
(m
onth
s) Median survival predictedby Halabi
Actual medianOS
Halabi nomogram: LDH, PSA, alkaline phosphatase, hemoglobin, Gleacon sum , ECOG performance status, visceral disease
17.4
26.6
12.3
14.620.9
37.3
p=0.035
(Gulley JL et al, CII 2010, 59:663)(Gulley JL et al, CII 2010, 59:663)
Immunologic and prognostic factors associated with overallImmunologic and prognostic factors associated with overall survival employing survival employing a poxviral-based PSA vaccine in metastatica poxviral-based PSA vaccine in metastatic castrate-resistant prostate cancercastrate-resistant prostate cancer

Randomized phase II study: flutamide with or without Randomized phase II study: flutamide with or without PSA-TRICOM in patients with prostate cancer PSA-TRICOM in patients with prostate cancer
(NCI) (Bilusic M et al. ASCO 2011)(NCI) (Bilusic M et al. ASCO 2011)
non-metastatic, castrate resistant prostatecancer patients with rising PSA
STRATIFICATION• PSADT
Randomization
Flutamide+
PSA-TRICOM
Flutamide
PRIMARY ENDPOINT• TTP (biochemical recurrence, metastatic disease)
n=32 n=32

PSA-TRICOM combined with Docetaxel and Prednisone in treating patients with PSA-TRICOM combined with Docetaxel and Prednisone in treating patients with metastatic castrate resistant prostate cancer (Phase II/ NCI)metastatic castrate resistant prostate cancer (Phase II/ NCI)
Schedule: Course-1 Course-2
Days: 1 15 29 43 59
VacciniaPSA-TRICOM
FowlpoxPSA-TRICOM
Docetaxel q21dPrednisone q1dx2
x 12 cycles
85 - 106
(1) - (21)
Arm I: PSA-TRICOM + chemo
Objectives:Primary: OSSecondary: - Time to radiographic progression - PSA response rates - Immune responses
Arm II: chemo
Recruiting
Randomization

PSA-TRICOM (Bavarian Nordic) Randomized PSA-TRICOM (Bavarian Nordic) Randomized double-blind Phase III Studydouble-blind Phase III Study
Primary endpoint: Overall SurvivalSecondary endpoint: Progression Free Survival
Asymptomatic or Minimally
Symptomatic Metastatic Castrate Resistant
Prostate Cancer (N=1600)
Asymptomatic or Minimally
Symptomatic Metastatic Castrate Resistant
Prostate Cancer (N=1600)
Empty vector +placebo
Empty vector +placebo
PROSTVAC-VFTricom + GM
PROSTVAC-VFTricom + GM P
R O
G R E S
S I O N
P R O
G R E S
S I O N
SURVIVAL
SURVIVAL
Treated at physician discretion
Treated at physician discretion
PROSTVAC-VFTricom + placebo
PROSTVAC-VFTricom + placebo
Not recruiting yet
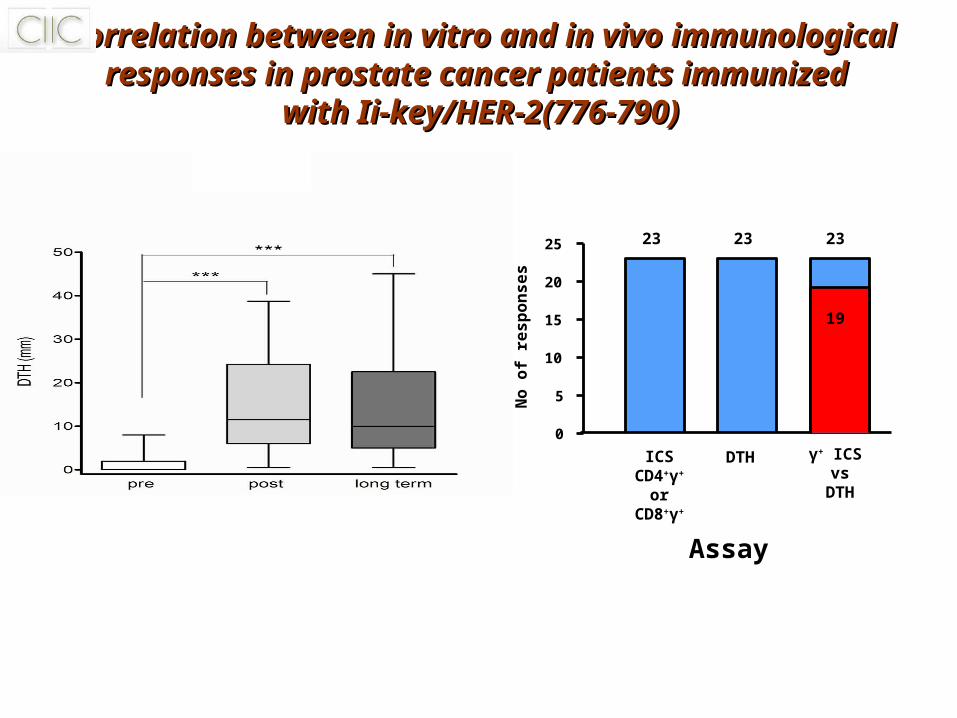
Optimizing the vaccine formulation for developingOptimizing the vaccine formulation for developingeffective therapeutic vaccineseffective therapeutic vaccines
tumorantigen
adjuvant vehicle
Polyvalentantigens
PoxvirusDCsTLR-L ?
PGE2PGE2
AdenosineAdenosine
ROSROS
TGF-TGF-ββ IL-10IL-10IDOIDO ArginaseArginase
iNOSiNOS
COX2COX2ectonucleotidasesectonucleotidasesPD-L1PD-L1
MICA/BMICA/B
TMVTMV
gangliosidesgangliosides
tumorantigen
adjuvant vehicle
Polyvalentantigens
PoxvirusDCsTLR-L ?
tumorantigen
adjuvant vehicle
Polyvalentantigens
PoxvirusDCsTLR-L ?
tumorantigen
adjuvant vehicle
Polyvalentantigens
PoxvirusDCsTLR-L ?
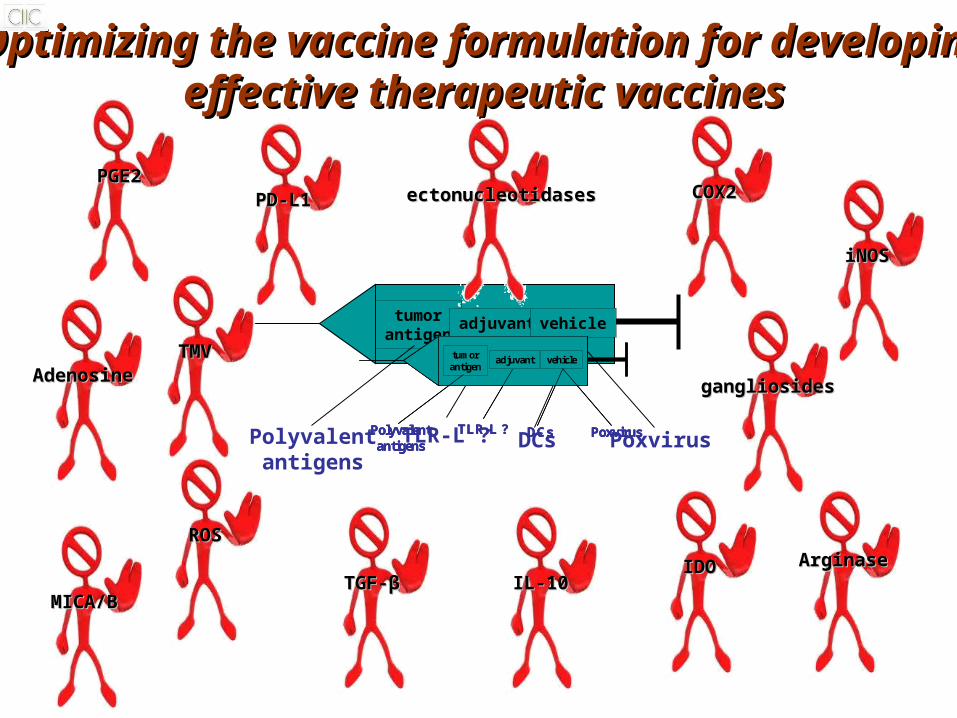
Combinatorial treatmentsCombinatorial treatments
Vaccine + something
chemotherapy
- PSA-TRICOM + Docetaxel/Prednisone- MAGRIT (MAGE-A3 + Platinum)- IMPRINT (IMA901 + cyclo)
- Temozolomide (TMZ) + telomerase helper peptide (phase I/II / stage IV melanoma) (Norwegian Cancer Society)(Kyte JA et al. Clin. Cancer Res. 2011, 17:4568)
-TG-4010/MVA-MUC1-IL2 (Transgene/Novartis) + chemo in NSCLC (stage IV) (Phase III)- CDX-110/EGFRvIII-KLH (Celldex Therapeutics)+ TMZ in glioblastoma (phase III)
- Autologous Id-KLH+GM-CSF (BiovaxID /Biovest International)+chemotherapy in Follicular lymphoma (Phase III) (Schuster SJ et al. JCO 2011, 29:2748)
- Stimuvax BLP25 (MUC1+TLR-4L in liposome) (Oncothyreon/Merck) + cyclo in NSCLC after chemoradiotherapy (Phase III)

Combinatorial treatmentsCombinatorial treatments
Vaccine + something Biological therapy
tyrosine kinase inhibitors
• Sunitinib + IMA901 in RCC (IMPRINT/Phase III) (Immatics)
• DCs+AuTu mRNA+CD40L (AGS-003) + sunitinib in RCC (Phase III) (Argos Therapeutics)

Combinatorial treatmentsCombinatorial treatmentsVaccine + something
hormonaltherapy
clinicallylocalizeddisease
biochemicalrecurrence
castration-resistantdisease (non-metastatic)
metastatic disease(hormone sensitive)
Androgen ablation
• Primary therapy (radiotherapy and/or surgery)• androgen ablation
• monitoring• androgen ablation
Secondaryandrogen ablation
increasingPSA level
sipuleucel T
sipuleucel T
PSA-TRICOM

Cancer vaccines must induce cellular immune responses beforeCancer vaccines must induce cellular immune responses beforethey can affect tumor burden or patient survivalthey can affect tumor burden or patient survival
Immunotherapy
Proper activation of the immune system
Robust immunologic antitumor response
Clinical efficacy
Patients to be vaccinated should be sufficiently healthy for a sufficiently long time to benefit
Vaccinate at earlier disease stage or in the adjuvant setting/metastatic indolent disease

• Phase II PSA-TRICOM study
• Ongoing Phase III PSA-TRICOM study
• Phase II MAGE-A3 study in NSCLC
• Phase III MAGE-A3 MAGRIT
• Phase III MAGE-A3 DERMA
• Phase III BiovaxID study with follicular lymphoma patients
• Phase III Oncophage study (autologous HSP gp96 preparations) patients with stage I and stage II RCC → trend for increased RFS
• Phase III OncoVAX study (autologous irradiated tumor cells+BCG) patients with stage II but not stage III colorectal cancer → significant increase of RFS
• Phase II E75 study (HER-2 (369-377)) breast cancer patients with less aggressive tumors (HER-1+, 2+, low grade) had significant increased RFS
Vaccinate at earlier disease stage or in the adjuvantVaccinate at earlier disease stage or in the adjuvant setting/metastatic indolent diseasesetting/metastatic indolent disease

ConclusionsConclusions
• Improvements in vaccine formulations
• Combinatorial treatments
• Vaccinating patients with low tumor burden (i.e. early disease, adjuvant setting) will improve clinical efficacy
• Prognostic and predictive biomarkers are needed
• Intermediate biomarkers by early disease

AcknowledgementsAcknowledgements
CIICDr. SA PerezDr. M PapamichailDr. IF VoutsasDr. AD GritzapisDr. P TzonisE. PappouE. Anastasopoulou
Urology ClinicDr. A ThanosDr. S Bisias
Antigen Express Inc.Dr. R HumphreysDr. E von Hofe
University of TurinProf. G ForniProf. F Cavallo
MD Anderson Medical Center TX, USA Dr. EA Mittendorf Dr. GE Peoples
University of TuebingenDr. C Gouttefangeas

Thank you – Questions?Thank you – Questions?