Themedicalbiochemistrypage.org-Steroid and Thyroid Hormones
17
Steroid and Thyroid Hormones themedicalbiochemistrypage.org /steroid-hormones.php Introduction to the Steroid Hormones The steroid hormones are all derived from cholesterol. Moreover, with the exception of vitamin D, they all contain the same cyclopentanophenanthrene ring and atomic numbering system as cholesterol. The conversion of C 27 cholesterol to the 18-, 19-, and 21-carbon steroid hormones (designated by the nomenclature C with a subscript number indicating the number of carbon atoms, e.g. C 19 for androstanes) involves the rate-limiting, irreversible cleavage of a 6-carbon residue from cholesterol, producing pregnenolone (C 21 ) plus isocaproaldehyde. Common names of the steroid hormones are widely recognized, but systematic nomenclature is gaining acceptance and familiarity with both nomenclatures is increasingly important. Steroids with 21 carbon atoms are known systematically as pregnanes, whereas those containing 19 and 18 carbon atoms are known as androstanes and estranes, respectively. The important mammalian steroid hormones are shown below along with the structure of the precursor, pregneolone. Retinoic acid and vitamin D are not derived from pregnenolone, but from vitamin A and cholesterol respectively. Pregnenolone: produced directly from cholesterol, the precursor molecule for all C 18 , C 19 and C 21 steroids Progesterone: a progestagen, produced directly from pregnenolone and secreted from the corpus luteum, responsible for changes associated with luteal phase of the menstrual cycle, differentiation factor for mammary glands Aldosterone: the principal mineralocorticoid, produced from progesterone in the zona glomerulosa of adrenal cortex, raises blood pressure and fluid volume, increases Na + uptake Testosterone: an androgen, male sex hormone synthesized in the testes, responsible for secondary male sex characteristics, produced from progesterone Estradiol: an estrogen, principal female sex hormone, produced in the ovary, responsible for secondary female sex characteristics Cortisol: dominant glucocorticoid in humans, synthesized from progesterone in the zona fasciculata of the adrenal cortex, involved in stress adaptation, elevates blood pressure and Na + uptake, numerous effects on the immune system
-
Upload
elvis-florentino -
Category
Documents
-
view
18 -
download
1
description
Fitness for Penis: Top Ten Penis Enlargement Exercises
Transcript of Themedicalbiochemistrypage.org-Steroid and Thyroid Hormones
-
Steroid and Thyroid Hormonesthemedicalbiochemistrypage.org /steroid-hormones.php
Introduction to the Steroid HormonesThe steroid hormones are all derived from cholesterol. Moreover, with the exception of vitamin D, they allcontain the same cyclopentanophenanthrene ring and atomic numbering system as cholesterol. Theconversion of C27 cholesterol to the 18-, 19-, and 21-carbon steroid hormones (designated by thenomenclature C with a subscript number indicating the number of carbon atoms, e.g. C19 for androstanes)involves the rate-limiting, irreversible cleavage of a 6-carbon residue from cholesterol, producingpregnenolone (C21) plus isocaproaldehyde. Common names of the steroid hormones are widelyrecognized, but systematic nomenclature is gaining acceptance and familiarity with both nomenclatures isincreasingly important. Steroids with 21 carbon atoms are known systematically as pregnanes, whereasthose containing 19 and 18 carbon atoms are known as androstanes and estranes, respectively. Theimportant mammalian steroid hormones are shown below along with the structure of the precursor,pregneolone. Retinoic acid and vitamin D are not derived from pregnenolone, but from vitamin A andcholesterol respectively.
Pregnenolone: produced directly from cholesterol, the precursor molecule for all C18, C19and C21 steroids
Progesterone: a progestagen, produced directly from pregnenolone and secreted from thecorpus luteum, responsible for changes associated with luteal phase of the menstrual cycle,differentiation factor for mammary glands
Aldosterone: the principal mineralocorticoid, produced from progesterone in the zonaglomerulosa of adrenal cortex, raises blood pressure and fluid volume, increases Na+ uptake
Testosterone: an androgen, male sex hormone synthesized in the testes, responsible forsecondary male sex characteristics, produced from progesterone
Estradiol: an estrogen, principal female sex hormone, produced in the ovary, responsible forsecondary female sex characteristics
Cortisol: dominant glucocorticoid in humans, synthesized from progesterone in the zonafasciculata of the adrenal cortex, involved in stress adaptation, elevates blood pressure andNa+ uptake, numerous effects on the immune system
-
All the steroid hormones exert their action by passing through the plasma membrane and binding tointracellular receptors. The mechanism of action of the thyroid hormones is similar; they interact withintracellular receptors. Both the steroid and thyroid hormone-receptor complexes exert their action bybinding to specific nucleotide sequences in the DNA of responsive genes. These DNA sequences areidentified as hormone response elements, HREs. The interaction of steroid-receptor complexes with DNAleads to altered rates of transcription of the associated genes.
back to the top
Introduction to the Thyroid HormonesThe thyroid hormones (called thyronines) are all derived from the amino acid tyrosine within specificfollicle cells of the thyroid gland. The primary hormone secreted from the thyroid gland is thyroxine (T4:3,5,3'5'-tetraiodothyronine). Another hormone secreted from the thyroid, but at much lower levels, istriiodothyronine (T3).
The primary site of T 3 generation is in peripheral tissues via the deiodination of thyroxine. T3 is the mostbiologically active form of thyroid hormone and exerts its effects by binding to the thyroid hormone receptor(TR). TR is a member of the steroid hormone/thyroid hormone superfamily of nuclear receptors. There aretwo known TR genes, one encoding TR and the other encoding TR. Synthesis of the thyroid hormonesis controlled by the actions of the anterior pituitary hormone, thyroid stimulating hormone (TSH). Theactions of the thyroid hormones maintain optimal lipid and carbohydrate metabolic homeostasis. Althoughthe thyroid gland is not essential for life, hypothyroidism in fetal life and in early childhood results inreduced growth (dwarfism) as well as severe mental retardation. Hypothyroidism in adulthood isassociated with reduced resistance to cold as well as mental and physical impairment. At the other end ofthe spectrum, hyperthyroidism in adults is associated with excessive heat generation, metabolic wasting,cardiac dysfunction (tachycardia), tremors and anxiety.
back to the top
Steroid Hormone Biosynthesis ReactionsThe particular steroid hormone class synthesized by a given cell type depends upon its complement ofpeptide hormone receptors, its response to peptide hormone stimulation and its genetically expressedcomplement of enzymes. The following indicates which peptide hormone is responsible for stimulating thesynthesis of which steroid hormone:
Luteinizing Hormone (LH): progesterone and testosterone
Adrenocorticotropic hormone (ACTH): cortisol
Follicle Stimulating Hormone (FSH): estradiol
Angiotensin II/III: aldosterone
The first reaction in converting cholesterol to C 18, C19 and C21 steroids involves the cleavage of a 6-carbon group from cholesterol and is the principal committing, regulated, and rate-limiting step in steroidbiosynthesis. The enzyme system that catalyzes the cleavage reaction is known as P450-linked side chaincleaving enzyme (P450ssc) or 20,22-desmolase, or cholesterol desmolase, and is found in themitochondria of steroid-producing cells, but not in significant quantities in other cells.
-
Mitochondrial desmolase is a complex enzyme system consisting of cytochrome P450, and adrenadoxin (aP450 reductant). The activity of each of these components is increased by two principal cAMP- and PKA-dependent processes. First, cAMP stimulates PKA, leading to the phosphorylation of a cholesteryl-esteresterase and generating increased concentrations of cholesterol, the substrate for desmolase. Second,long-term regulation is effected at the level the gene for desmolase. This gene contains a cAMP regulatoryelement (CRE) that binds cAMP and increases the level of desmolase RNA transcription, thereby leadingto increased levels of the enzyme. Finally, cholesterol is a negative feedback regulator of HMG CoAreductase (HMGR) activity (see regulation of cholesterol synthesis). Thus, when cytosolic cholesterol isdepleted, de novo cholesterol synthesis is stimulated by freeing HMGR of its feedback constraints.Subsequent to desmolase activity, pregnenolone moves to the cytosol, where further processing dependson the cell (tissue) under consideration.
The various hydroxylases involved in the synthesis of the steroid hormones have a nomenclature thatindicates the site of hydroxylation (e.g. 17-hydroxylase introduces a hydroxyl group to carbon 17). Thesehydroxylase enzymes are members of the cytochrome P450 class of enzymes and as such also have anomenclature indicative of the site of hydroxylation in addition to being identified as P450 class enzymes(e.g. the 17-hydroxylase is also identified as P450c17). The officially preferred nomenclature for thecytochrome P450 class of enzymes is to use the prefix CYP. Thus, 17-hydroxylase should be identifiedas CYP17A1. There are currently 57 identified CYP genes in the human genome.
Primary Enzyme Activities of Steroid Hormone Biosynthesis
steroidogenic acuteregulatory protein
StAR mediates mitochondrialimport of cholesterol
all steroidogenic tissues exceptplacenta and brain
desmolase, P450ssc CYP11A1 cholesterol-20,23-desmolase
steroidogenic tissues
3-hydroxysteroiddehydrogenase type 1
HSD3B2 3-hydroxysteroiddehydrogenase
steroidogenic tissues
P450c11 CYP11B1 11-hydroxylase only in zona fasciculata and zonareticularis of adrenal cortex
P450c17 CYP17A1 two activities: 17-hydroxylase and 17,20-lyase
steroidogenic tissues
P450c21 CYP21A2 21-hydroxylase not expressed in the zonareticularis
aldosterone synthase CYP11B2 18-hydroxylase exclusive to zona glomerulosa ofadrenal cortex
estrogen synthetase CYP19A1 aromatase gonads, brain, adrenals, adiposetissue, bone
17-hydroxysteroiddehydrogenase type 3
HSD17B3 17-ketoreductase steroidogenic tissues
sulfotransferase SULT2A1 sulfotransferase liver, adrenals5-reductase type 2 SRD5A2 5-reductase steroidogenic tissues
-
back to the top
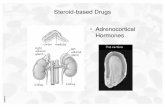
Steroids of the Adrenal CortexThe adrenal cortex is responsible for production of three major classes of steroid hormones:glucocorticoids, which regulate carbohydrate metabolism; mineralocorticoids, which regulate the bodylevels of sodium and potassium; and androgens, whose actions are similar to that of steroids produced bythe male gonads. Cholesterol, acquired from the diet or from LDL, or produced de novo in adrenal corticalcells, serves as the precursor for all of the adrenal steroid hormones. Cholesterol uptake from the bloodoccurs through the binding of LDL to the LDL receptor. Chronic stimulation of the adrenal cortex by ACTHleads to increased LDL receptor gene expression resulting in increased receptor density.
The adrenal cortex is composed of three main tissue regions: zona glomerulosa, zona fasciculata, andzona reticularis. Although the pathway to pregnenolone synthesis is the same in all zones of the cortex, thezones are histologically and enzymatically distinct, with the exact steroid hormone product dependent onthe enzymes present in the cells of each zone. Many of the enzymes of adrenal steroid hormone synthesisare of the class called cytochrome P450 enzymes. These enzymes all have a common nomenclature anda standardized nomenclature. The standardized nomenclature for the P450 class of enzymes is to use theabbreviation CYP. For example the P450ssc enzyme (also called 20,22-desmolase or cholesteroldesmolase) is identified as CYP11A1. In order for cholesterol to be converted to pregnenolone in theadrenal cortex it must be transported into the mitochondria where CYP11A1 resides. This transportprocess is mediated by steroidogenic acute regulatory protein (StAR). This transport process is the rate-limiting step in steroidogenesis.
-
Synthesis of the various adrenal steroid hormones from cholesterol. Only the terminal hormone structuresare included. 3-DH and 4,5-isomerase are the two activities of 3-hydroxysteroid dehydrogenase type 1(gene symbol HSD3B2), P450c11 is 11-hydroxylase (CYP11B1), P450c17 is CYP17A1. CYP17A1 is asingle microsomal enzyme that has two steroid biosynthetic activities: 17-hydroxylase which convertspregnenolone to 17-hydroxypregnenolone (17-OH pregnenolone) and 17,20-lyase which converts 17-OHpregnenolone to DHEA. P450c21 is 21-hydroxylase (CYP21A2, also identified as CYP21 or CYP21B).Aldosterone synthase is also known as 18-hydroxylase (CYP11B2). The gene symbol forsulfotransferase is SULT2A1. Place your mouse over structure names to see chemical structures. Clickhere for a larger format picture.
Conversion of prenenolone to progesterone requires the two enzyme activities of HSD3B2: the 3-hydroxysteroid dehydrogenase and 4,5-isomerase activities. Zona glomerulosa cells lack the P450c17that converts pregnenolone and progesterone to their C17 hydroxylated analogs. Thus, the pathways to theglucocorticoids (deoxycortisol and cortisol) and the androgens [dehydroepiandosterone (DHEA) andandrostenedione] are blocked in these cells. Zona glomerulosa cells are unique in the adrenal cortex incontaining the enzyme responsible for converting corticosterone to aldosterone, the principal and mostpotent mineralocorticoid. This enzyme is P450c18 (or 18-hydroxylase, CYP11B2), also called aldosteronesynthase. The result is that the zona glomerulosa is mainly responsible for the conversion of cholesterol tothe weak mineralocorticoid, corticosterone and the principal mineralocorticoid, aldosterone.
-
Cells of the zona fasciculata and zona reticularis lack aldosterone synthase (P450c18) that convertscorticosterone to aldosterone, and thus these tissues produce only the weak mineralocorticoidcorticosterone. However, both these zones do contain the P450c17 missing in zona glomerulosa and thusproduce the major glucocorticoid, cortisol. Zona fasciculata and zona reticularis cells also containP450c17, whose 17,20-lyase activity is responsible for producing the androgens, dehydroepiandosterone(DHEA) and androstenedione. Thus, fasciculata and reticularis cells can make corticosteroids and theadrenal androgens, but not aldosterone.
As noted earlier, P450ssc is a mitochondrial activity. Its product, pregnenolone, moves to the cytosol,where it is converted either to androgens or to 11-deoxycortisol and 11-deoxycorticosterone by enzymes ofthe endoplasmic reticulum. The latter 2 compounds then re-enter the mitochondrion, where the enzymesare located for tissue-specific conversion to glucocorticoids or mineralocorticoids, respectively.
back to the top
Regulation of Adrenal Steroid SynthesisAdrenocorticotropic hormone (ACTH), of the hypothalamus, regulates the hormone production of the zonafasciculata and zona reticularis. ACTH receptors in the plasma membrane of the cells of these tissuesactivate adenylate cyclase with production of the second messenger, cAMP. The effect of ACTH on theproduction of cortisol is particularly important, with the result that a classic feedback loop is prominent inregulating the circulating levels of corticotropin releasing hormone (CRH), ACTH, and cortisol.
Mineralocorticoid secretion from the zona glomerulosa is stimulated by an entirely different mechanism.Angiotensins II and III, derived from the action of the kidney protease renin on liver-derivedangiotensinogen, stimulate zona glomerulosa cells by binding a plasma membrane receptor coupled tophospholipase C. Thus, angiotensin II and III binding to their receptor leads to the activation of PKC andelevated intracellular Ca2+ levels. These events lead to increased P450ssc activity and increasedproduction of aldosterone. In the kidney, aldosterone regulates sodium retention by stimulating geneexpression of mRNA for the Na+/K+ATPase responsible for the reaccumulation of sodium from the urine.
The interplay between renin from the kidney and plasma angiotensinogen is important in regulatingplasma aldosterone levels, sodium and potassium levels, and ultimately blood pressure. Among the drugsmost widely employed used to lower blood pressure are the angiotensin converting enzyme (ACE)inhibitors. These compounds are potent competitive inhibitors of the enzyme that converts angiotensin I tothe physiologically active angiotensins II and III. This feedback loop is closed by potassium, which is apotent stimulator of aldosterone secretion. Changes in plasma potassium of as little as 0.1mM can causewide fluctuations (50%) in plasma levels of aldosterone. Potassium increases aldosterone secretion bydepolarizing the plasma membrane of zona glomerulosa cells and opening a voltage-gated calciumchannel, with a resultant increase in cytoplasmic calcium and the stimulation of calcium-dependentprocesses.
Although fasciculata and reticularis cells each have the capability of synthesizing androgens andglucocorticoids, the main pathway normally followed is that leading to glucocorticoid production. However,when genetic defects occur in the 3 enzyme complexes leading to glucocorticoid production, largeamounts of the most important androgen, dehydroepiandrosterone (DHEA), are produced. These lead tohirsutism and other masculinizing changes in secondary sex characteristics.
back to the top
-
Functions of the Adrenal Steroid HormonesGlucocorticoids: The glucocorticoids are a class of hormones so called because they are primarilyresponsible for modulating the metabolism of carbohydrates. The overall actions of the glucocorticoids is toincrease the production of glucose while simultaneously inhibiting all other metabolic pathways not directlyinvolved in glucose production. However, it is important to note that most glucocorticoids bind to themineralocorticoid receptor and as such exhibit mineralocorticoid-like activities. Cortisol is the mostimportant naturally occurring glucocorticoid. As indicated in the Figure above, cortisol is synthesized in thezona fasciculata of the adrenal cortex. When released to the circulation, cortisol is almost entirely bound toprotein. A small portion is bound to albumin with more than 70% being bound by a specific glycosylated -globulin called transcortin or corticosteroid-binding globulin (CBG). Between 5% and 10% of circulatingcortisol is free and biologically active. Glucocorticoid function is exerted following cellular uptake andinteraction with intracellular glucocorticoid receptors (GR) as discussed below. Cortisol inhibits uptake andutilization of glucose resulting in elevations in blood glucose levels. Glucocorticoids act as insulinantagonists and also suppress the release of insulin both effect leading to reduced glucose uptake andenhanced hepatic gluconeogenesis. The effect of cortisol on blood glucose levels is further enhancedthrough the increased breakdown of skeletal muscle protein and adipose tissue triglycerides whichprovides energy and substrates for gluconeogenesis. Glucocorticoids also increase the synthesis ofgluconeogenic enzymes. The increased rate of protein metabolism leads to increased urinary nitrogenexcretion and the induction of urea cycle enzymes.
In addition to the metabolic effects of the glucocorticoids, these hormones are immunosuppressive andanti-inflammatory. Hence, the use of related drugs such as prednisone, in the acute treatment ofinflammatory disorders. The anti-inflammatory activity of the glucocorticoids is exerted, in part, throughinhibition of phospholipase A2 (PLA2) activity with a consequent reduction in the release of arachidonicacid from membrane phospholipids. Arachidonic acid serves as the precursor for the synthesis of variouseicosanoids. Glucocorticoids also inhibit vitamin D-mediated intestinal calcium uptake, retard the rate ofwound healing, and interfere with the rate of linear growth.
Mineralocorticoids: The major circulating mineralocorticoid is aldosterone. Deoxycorticosterone (DOC)exhibits some mineralocorticoid action but only about 3% of that of aldosterone. As the name of this classof hormones implies, the mineralocorticoids control the excretion of electrolytes. This occurs primarilythrough actions on the kidneys but also in the colon and sweat glands. The principle effect of aldosteroneis to enhance sodium reabsorption in the cortical collecting duct of the kidneys. However, the action ofaldosterone is exerted on sweat glands, stomach, and salivary glands to the same effect, i.e. sodiumreabsorption. This action is accompanied by the retention of chloride and water resulting in the expansionof extracellular volume. Aldosterone also enhances the excretion of potassium and hydrogen ions from themedullary collecting duct of the kidneys.
Androgens: The androgens, androstenedione and DHEA, circulate bound primarily to sex hormone-binding globulin (SHBG). Although some of the circulating androgen is metabolized in the liver, the majorityof interconversion occurs in the gonads (as described below), skin, and adipose tissue. DHEA is rapidlyconverted to the sulfated form, DHEA-S, in the liver and adrenal cortex. The primary biologically activemetabolites of the androgens are testosterone and dihydrotestosterone which function by bindingintracellular receptors, thereby effecting changes in gene expression and thereby, resulting in themanifestation of the secondary sex characteristics.
back to the top
Clinical Significance of Defective Adrenal Steroidogenesis
-
Defective synthesis of the steroid hormones produced by the adrenal cortex can have profound effects onhuman development and homeostasis. In 1855 Thomas Addison identified the significance of the"suprarenal capsules" when he reported on the case of a patient who presented with chronic adrenalinsufficiency resulting from progressive lesions of the adrenal glands caused by tuberculosis. Adrenalinsufficiency is, therefore, referred to as Addison disease. In the absence of steroid hormone replacementtherapy, Addison disease can rapidly cause death in a little as 12 weeks.
In addition to diseases that result from the total absence of adrenocortical function, there are syndromesthat result from hypersecretion of adrenocortical hormones (hypercortisolemia). In 1932 Harvey Cushingreported on several cases of adrenocortical hyperplasia that were the result of basophilic adenomas of theanterior pituitary. Hypercortisolemias that manifest due to adrenocortical hyperplasia are referred to asCushing syndrome, whereas, hypercortisolemias due to excessive anterior pituitary secretion of ACTH arereferred to as Cushing disease.
Despite the characterizations of adrenal insufficiency and adrenal hyperplasia, there remained uncertaintyabout the relationship between adrenocortical hyperfunction and virilism (premature development of malesecondary sex characteristics). In 1942 this confusion was resolved by Fuller Albright when he delineatedthe differences between children with Cushing syndrome and those with adrenogenital syndromes whichare more commonly referred to as congenital adrenal hyperplasias (CAH). The CAH are a group ofinherited disorders that result from loss-of-function mutations in one of several genes involved in adrenalsteroid hormone synthesis. In the virilizing forms of CAH the mutations result in impairment of cortisolproduction and the consequent accumulation of steroid intermediates proximal to the defective enzyme. Allforms of CAH are inherited in an autosomal recessive manner. There are two common and at least threerare forms of CAH that result in virilization. The common forms are caused by defects in either CYP21A2(21-hydroxylase, also identified as just CYP21 or CYP21B) or CYP11B1 (11-hydroxylase). The majority ofCAH cases (9095%) are the result of defects in CYP21A2 with a frequency of between 1 in 5,000 and 1in 15,000. Three rare forms of virilizing CAH result from either defects in 3-hydroxysteroiddehydrogenase (HSD3B2), placental aromatase or P450-oxidoreductase (POR). An additional CAH iscaused by mutations that affect either the 17-hydroxylase, 17,20-lyase or both activities encoded in theCYP17A1 gene. In individuals harboring CYP17A1 mutations that result in severe loss of enzyme activitythere is absent sex steroid hormone production accompanied by hypertension resulting frommineralocorticoid excess.
back to the top
Gonadal Steroid HormonesAlthough many steroids are produced by the testes and the ovaries, the two most important aretestosterone and estradiol. These compounds are under tight biosynthetic control, with short and longnegative feedback loops that regulate the secretion of follicle stimulating hormone (FSH) and luteinizinghormone (LH) by the pituitary and gonadotropin releasing hormone (GnRH) by the hypothalamus. Lowlevels of circulating sex hormone reduce feedback inhibition on GnRH synthesis (the long loop), leading toelevated FSH and LH. The latter peptide hormones bind to gonadal tissue and stimulate P450ssc activity,resulting in sex hormone production via cAMP and PKA mediated pathways. The roles of cAMP and PKAin gonadal tissue are the same as that described for glucocorticoid production in the adrenals, but in thiscase adenylate cyclase activation is coupled to the binding of LH to plasma membrane receptors.
The biosynthetic pathway to sex hormones in male and female gonadal tissue includes the production ofthe androgens, androstenedione and dehydroepiandrosterone. Testes and ovaries contain an additionalenzyme, a 17-hydroxysteroid dehydrogenase, that enables androgens to be converted to testosterone.
-
In males, LH binds to Leydig cells, stimulating production of the principal Leydig cell hormone,testosterone. Testosterone is secreted to the plasma and also carried to Sertoli cells by androgen bindingprotein (ABP). In Sertoli cells the 4 double bond of testosterone is reduced, producingdihydrotestosterone. Testosterone and dihydrotestosterone are carried in the plasma, and delivered totarget tissue, by a specific gonadal-steroid binding globulin (GBG). In a number of target tissues,testosterone can be converted to dihydrotestosterone (DHT). DHT is the most potent of the male steroidhormones, with an activity that is 10 times that of testosterone. Because of its relatively lower potency,testosterone is sometimes considered to be a prohormone.
Synthesis of the male sex hormones in Leydig cells of the testis. P450SSC, 3-DH, and P450c17 are thesame enzymes as those needed for adrenal steroid hormone synthesis. 17,20-lyase is the same activity ofCYP17A1 described above for adrenal hormone synthesis. Aromatase (also called estrogen synthetase) isCYP19A1. 17-ketoreductase is also called 17-hydroxysteroid dehydrogenase type 3 (gene symbolHSD17B3). The full name for 5-reductase is 5-reductase type 2 (gene symbol SRD5A2). Place yourmouse over structure names to see chemical structures.
Testosterone is also produced by Sertoli cells but in these cells it is regulated by FSH, again actingthrough a cAMP- and PKA-regulatory pathway. In addition, FSH stimulates Sertoli cells to secrete
-
androgen-binding protein (ABP), which transports testosterone and DHT from Leydig cells to sites ofspermatogenesis. There, testosterone acts to stimulate protein synthesis and sperm development.
In females, LH binds to thecal cells of the ovary, where it stimulates the synthesis of androstenedione andtestosterone by the usual cAMP- and PKA-regulated pathway. An additional enzyme complex known asaromatase is responsible for the final conversion of the latter 2 molecules into the estrogens. Aromatase isa complex endoplasmic reticulum enzyme found in the ovary and in numerous other tissues in both malesand females. Its action involves hydroxylations and dehydrations that culminate in aromatization of the Aring of the androgens.
Synthesis of the major female sex hormones in the ovary. Synthesis of testosterone and androstenedionefrom cholesterol occurs by the same pathways as indicated for synthesis of the male sex hormones.Aromatase (also called estrogen synthetase) is CYP19A1.
Aromatase activity is also found in granulosa cells, but in these cells the activity is stimulated by FSH.Normally, thecal cell androgens produced in response to LH diffuse to granulosa cells, where granulosacell aromatase converts these androgens to estrogens. As granulosa cells mature they develop competentlarge numbers of LH receptors in the plasma membrane and become increasingly responsive to LH,increasing the quantity of estrogen produced from these cells. Granulosa cell estrogens are largely, if notall, secreted into follicular fluid. Thecal cell estrogens are secreted largely into the circulation, where theyare delivered to target tissue by the same globulin (GBG) used to transport testosterone.
back to the top
Thyroid HormonesThe thyroid hormones, referred to as the thyronines, are synthesized from the amino acid tyrosine withinspecialized cells of the thyroid gland. The two major thyroid hormones are triiodothyronine (T3) andthyroxine (T4). Within the periphery the major actions of thyroid hormone are exerted via T3. Synthesis of
-
the thyroid hormones is controlled via the action of the anterior pituitary hormone, thyroid stimulatinghormone, TSH. In addition to pituitary control, synthesis of the thyroid hormones requires iodine uptakeinto the thyroid gland and incorporation into tyrosine. The primary functions for the thyroid hormones arefetal and post-natal development, development of the CNS, modulation of cardiac function throughregulation of myocardial contraction and relaxation, renal water clearance, gastrointestinal motility, thermalregulation, energy expenditure, and regulation of lipid metabolism. The thyroid gland also synthesizes thepeptide hormone, calcitonin, from parafollicular C cells. However, calcitonin has no physiological role inhumans but the protein is an important marker for thyroid medullary carcinomas.
Primary Activities of Thyroid Hormone (T3)
Adipose tissue catabolic activation of lipolysis and triglyceride breakdown; increases -adrenergic receptor density
Bone developmental promotes bone growth and differentiationCentralnervoussystem
developmental promotes development of nervous tissue
Gastrointestinalsystem
metabolic increases carbohydrate absorption
Heart both inotropicandchronotropic
increases density of -adrenergic receptors; enhances cardiacresponses to catecholamines; enhances ATPase activity of -myosinheavy chain
Liver metabolic increases gluconeogenesis and glycogen breakdown; increasescholesterol metabolism; enhances production of LDL receptors
Muscle catabolic enhances protein breakdown; increases speed of contraction andrelaxation; increases -adrenergic receptor density
Iodine Homeostasis
Iodine is a critical micronutrient due to its role in the generation of functional thyroid hormones. Dietaryintake of iodine is recommended to be 150g/day for adults and 50-200g/day for children. In the US, andother developed countries, the use of iodized sodium chloride (salt) ensures an adequate daily intake formost individuals.
The basolateral membrane of thyroid gland cells (thyrocytes) transports iodide into the cell from thecirculation. The transporter is called the Na+/I symporter (NIS) which is encoded by the SLC5A5 gene.The NIS transporter move two moles of Na+ and one mole of I into the thyrocyte. The transporter is ableto produce intra-thyrocyte iodide concentrations that are 20-40 fold higher than that in the circulation. Theexpression of the thyrocyte SLC5A5 gene is controlled via the actions of TSH. In addition to regulatedexpression, TSH controls the migration of NIS into and out of the basolateral membranes of the thyrocyte.Mutations in the SLC5A5 gene result in thyroid dyshormonogenesis type 1 (TDH1).
In order to continue the uptake of iodide, thyrocytes must transport the Na + back into the circulation whichis catalyzed by a Na+/K+-ATPase. The incorporation of iodine into tyrosine occurs in the lumen of thyroidfollicles (the colloid) and it is transported across the thyrocyte apical membrane via the action of a Cl/I
-
exchanger identified as pendrin (SLC26A4). Mutations in the SLC26A4 gene are the cause of Pendrinsyndrome (PDS), also known as thyroid dyshormonogenesis type 2B (TDH2B). PDS is associated withcongenital deafness and thyroid dysfunction resulting in goiter.
Although the thyroid gland is the primary tissue requiring iodine for its hormonal functions, salivary glands,gastric mucosa, choroid plexus, mammary glands, and the ciliary body of the eye express the SLC5A5gene.
Thyroid Hormone Synthesis
Chronic stimulation of the thyroid gland, via TSH binding to its receptor on thyrocytes, causes an increasein the synthesis of a major thyroid hormone precursor, thyroglobulin. Thyroglobulin is a large homodimericglycoprotein with a molecular weight of 660,000. Although thyroglobulin contains 140 tyrosine residues,only four in each subunit serve as substrates for iodination. Following thyroglobulin synthesis andglycosylation the homodimeric protein is incorporated into exocytic vesicles. Thyroglobulin is thenexoctosed through the apical membrane into the closed lumen of thyroid follicles (the colloid), where itaccumulates as the major protein of the thyroid gland and where maturation takes place. Within the colloidiodide (I) is oxidized to I+ by thyroid peroxidase (TPO; also called thyroperoxidase) found only in thyroidtissue. The oxidation reaction catalyzed by TPO requires hydrogen peroxide (H2O2) which is produced byan NADPH oxidase complex often referred to as thyroid oxidase. TPO and the NADPH oxidase complexare all associated in a large complex at the apical membrane of thyrocytes. The NADPH oxidase iscomposed multiple subunits encoded by different genes. These genes include dual oxidase 1 (DUOX1)and dual oxidase 2 (DUOX2). Another gene required for the function of the NADPH oxidase complex isDUOXA2 (dual oxidase maturation factor 2) which is involved in the maturation and membrane localizationof DUOX2. The activity of the NADPH oxidase is also regulated via the actions of TSH. The addition of I+to tyrosine residues of thyroglobulin is catalyzed by TPO at the thyrocyte apical membrane-colloidinterface. The products of this reaction are thyroglobulin complexes containing monoiodotyrosyl (MIT) anddiiodotyrosyl (DIT) residues. Two molecules of DIT condense to form T4 while a molecule of MIT and oneof DIT condense to form T3. Mutations in the TPO gene are associated with thyroid dyshormonogenesistype 2A (THD2A)
-
Structures of the primary thyroid hormonesMature, iodinated thyroglobulin contains approximately three molecules of T4 and one molecule of T3.Following the iodination reactions, thyroglobulin is taken up into vesicles at the colloid-apical membraneinterface via a process referred to as pinocytosis. These vesicles then fuse with lysosomes. Lysosomalproteases degrade thyroglobulin releasing T3 and T4, as well as inactive iodotyrosines and amino acids.T3 and T4 are then secreted into the circulation. These compounds are very hydrophobic and require acarrier protein for delivery to target tissues. In the plasma, T3 and T4 are primarily (70%) bound to a carrierglycoprotein known as thyroxin-binding globulin (TBG) and are disseminated throughout the body in thisform. In addition to TBG, T3 and T4 can be carried in the blood bound to transthyretin (formerly thyroxine-binding prealbumin) or albumin.
The feedback loop that regulates T3 and T4 production is a single short negative loop, with the T3 and T4being responsible for down-regulating anterior pituitary TSH secretion. Conversely, continuously secretedhypothalamic thyrotropin-releasing hormone (TRH) is responsible for up-regulating pituitary TSHproduction. Pituitary thyrotrope secretion of TSH is the net result of the negative effects of T3 and T4 andthe positive effect of TRH.
T3 is the more biologically active thyroid hormone and T4 is converted to T3 within peripheral tissues viathe actions of a 5'-deiodinase (thyroxine deiodinase type 1; DIO1). This deiodinase is also present in thethyroid gland and plays a critical role in overall regulation of iodide homeostasis in this tissue. Deiodinationof MIT and DIT also takes place within the thyroid gland. These reactions are catalyzed by an NADPH-dependent flavoprotein (iodotyrosine deiodinase; IYD) which recognizes MIT and DIT but not T3 nor T4.The iodine released from MIT and DIT is reused for hormone biogenesis.
Thyroid Hormone Receptors
Thyroid hormones act by binding to cytosolic receptors of the steroid-thyroid hormone receptor superfamily(nuclear receptors) identified as thyroid hormone receptors (TR). There are two TR receptors designatedTR and TR encoded by the THRA and THRB genes, respectively. The THRA gene is located onchromosome 17q21.1. The THRB is located on chromosome 3p24.2. The mRNAs from both genes aresubject to alternative splicing. This results in the TR1, TR2, and TR3 isoforms from the THRA gene andTR1 and TR2 from the THRB. Each of these thyroid hormone receptors possesses the characteristicdomains of all members of the nuclear receptor family: ligand-binding domain (LBD), DNA-binding domain(DBD), and activation function domain (AFD).
All of the TR bind to a specific response element in target genes termed the thyroid hormone responseelement (TRE). The TRE is composed of repeated DNA sequences with different configurations. Evidenceindicates that TRs can bind to TREs as monomers or homodimers. However, the major form of the TRbound to a TRE is a heterodimer with retinoid X receptor (RXR). The RXR binding site is upstream of thetwo directly repeated half-sites of the TRE. The TRE half-sites each contain the sequence T(A/G)AGGTCAas direct repeats separated by a 4 bp spacer. This is referred to as the DR4 element. The RXR responseelement is GGGGTCA. An important property of TRs is their ability to bind TREs constitutively in theabsence of thyroid hormone. In this unliganded state, TR generally represses basal transcription. Bindingof thyroid hormone to TR triggers a conformational change in the receptor, resulting in activatedtranscription of target genes.
Transcriptional activation by TR is mediated not only by ligand binding but by the activity of severalcoactivator proteins. Steroid receptor coactivator-1 (SRC-1) was the first nuclear receptor coactivatorcharacterized and it has been shown to enhance the activity of ligand-bound TR. The significance of therole of SRC-1 in thyroid hormone function is evident from the fact that loss of this coactivator results in T3
-
resistance. Several other members of the SRC family of coactivators have been shown to enhance thefunctions of TR. Coactivators of the SRC family associate with p300/CBP [CBP: CREB (cAMP responseelement-binding protein)-binding protein]. Given that p300/CBP interacts with and mediates the activationof other transcriptional regulation factors it is clear that this protein is a regulator of multiple signaltransduction pathways in addition to its role in steroid/thyroid hormone receptor functions.
Thyroid Hormone Biogenesis Disorders
Numerous inherited disorders in the biogenesis of the thyroid hormones have been described. All of thesedisorders are associated with congenital hypothyroidism. Currently seven distinct gene defects are knownthat result in this type of disorder. Three of these disorders were indicated in the discussion above, TDH1,TDH2A, and TDH2B.
TDH1 Na+/I symporter (NIS):SLC5A5 chromosome 19p13.2p12
TDH2A thyroid peroxidase, TPO chromosome 2p25
recurrent goiter, complete iodide release
TDH2B pendrin: SLC26A4 chromosome 7q31
sensorineural hearing loss, goiter, partial iodide release, enlargedvestibular aqueduct
TDH3 thyroglobulin, TG chromosome 8q24
large goiters with soft and elastic consistency
TDH4 tyrosine deiodinase, IYD chromosome 6q25.1
goiter, continuous iodine and tyrosine loss in the urine, delayedpsychomotor development, stunted growth
TDH5 dual oxidase maturationfactor 2: DUOXA2 chromosome 15q15.3
goiter
TDH6 dual oxidase 2 (DUOX2):thyroid oxidase 2 chromosome 15q15.3
partial or defective iodide organification
back to the top
Hypo- and HyperparathyroidismNumerous congenital and acquired forms of hypothyroidism and hyperthyroidism are the result ofalterations in the expression, processing, and function of the TSHR. The most common TSHR disorderresulting in hyperthyroidism (thyrotoxicosis) is Graves disease. Graves disease is caused by thyroid-stimulating autoantibodies (TSAb, also called thyroid-stimulating immunoglobulins, TSIs) which bind to andactivate the human TSH receptor, leading to the thyrotoxicosis characteristic of this disease. TSAbs bind tothe TSH receptor and mimic the TSH stimulation of the thyroid gland by increasing intracellular cAMP. Thehyperactivated thyroid then secretes excessive T3 and T4. Graves disease is classified as a form ofthyrotoxicosis, the name for the clinical syndrome resulting from tissues exposed to high levels of thyroidhormones. One theory proposed for the development of the TSAb is that there is a defect in suppressor Tcells that allows helper T cells to stimulate B cells to produce thyroid autoantibodies. The clinical featuresof Graves disease are thyrotoxicosis, goiter (enlarged thyroid gland), an ophthalmopathy in the form of
-
exophthalmos (eyes bulge out), and dermopathy in the form of pretibial myxedema (localized lesions of theskin, primarily in the lower legs, resulting from the deposition of hyaluronic acid).
At the other end of the spectrum are disorders that lead to hypothyroidism. Deficiency in iodine is the mostcommon cause of hypothyroidism worldwide. Indeed the practice of producing iodized table salt was tostem the occurrence of hypothyroidism. When hypothyroidism is evident in conjunction with sufficientiodine intake it is either autoimmune disease (Hashimoto thyroiditis) or the consequences of treatments forhyperthyroidism that are the cause. In the embryo, thyroid hormone is necessary for normal developmentand hypothyroidism in the embryo is responsible for cretinism, which is characterized by multiplecongenital defects and mental retardation. Because the neurological consequences of congenitalhypothyroidism are severe, neonatal screening for thyroid hormone levels at birth is routine. Most infantsborn with congenital hypothyroidism appear normal at birth. However, if left untreated the symptoms willinclude a thick protruding tongue, poor feeding, prolonged jaundice (which exacerbates the neurologicalimpairment), hypotonia (recognized as "floppy baby syndrome"), episodes of choking, and delayed bonematuration resulting in short stature.
back to the top
Steroid and Thyroid Hormone ReceptorsThe receptors to which steroid and thyroid hormones bind are ligand-activated proteins that regulatetranscription of selected genes. Unlike peptide hormone receptors, that span the plasma membrane andbind ligand outside the cell, steroid/thyroid hormone receptors are found in the cytosol or the nucleus in theabsence of ligand. All of these receptors belong to the steroid and thyroid hormone receptor super-family ofreceptors. This large family of receptors includes the androgen receptor (AR), the progesterone receptor(PR), the estrogen receptor (ER), the thyroid hormone receptor (TR), the vitamin D receptor (VDR), theretinoic acid receptors (RARs), the mineralocorticoid receptor (MR), and the glucocorticoid receptor (GR).This large class of receptors is known as the nuclear receptors.
When these receptors bind ligand they undergo a conformational change that renders them activated torecognize and bind to specific nucleotide sequences. These specific nucleotide sequences in the DNA arereferred to as hormone-response elements (HREs). When ligand-receptor complexes interact with DNAthey alter the transcriptional level (responses can be either activating or repressing) of the associatedgene. Thus, the steroid-thyroid family of receptors all have three distinct domains: a ligand-binding domain(LBD), a DNA-binding domain (DBD) and a transcriptional regulatory domain, referred to as the activationfunction domain (AFD). Although there is the commonly observed effect of altered transcriptional activity inresponse to hormone-receptor interaction, there are family member-specific effects with ligand-receptorinteraction. Binding of thyroid hormone to its receptor results in release of the receptor from DNA. Severalreceptors are induced to interact with other transcriptional mediators in response to ligand binding. Bindingof glucocorticoid leads to translocation of the ligand-receptor complex from the cytosol to the nucleus.
The receptors for the retinoids (vitamin A and its derivatives ) are identified as RARs (for retinoic acid, RAreceptors) and exist in at least three subtypes, RAR, RAR and RAR. In addition, there is another familyof nuclear receptors termed the retinoid X receptors (RXRs) that represents a second class of retinoid-responsive transcription factors. The RXRs have been shown to enhance the DNA-binding activity ofRARs and the thyroid hormone receptors (TRs). The RXRs represent a class of receptors that bind theretinoid 9-cis-retinoic acid. There are three isotypes of the RXRs: RXR, RXR, and RXR and eachisotype is composed of several isoforms. The RXRs serve as obligatory heterodimeric partners fornumerous members of the nuclear receptor family including PPARs, LXRs, and FXRs (see below and theSignal Transduction page). In the absence of a heterodimeric binding partner the RXRs are bound to
-
hormone response elements (HREs) in DNA and are complexed with co-repressor proteins that include ahistone deacetylase (HDAC) and silencing mediator of retinoid and thyroid hormone receptor (SMRT) ornuclear receptor corepressor 1 (NCoR).
Model for NR interactions with corepressors: An example of the transcription corepressor complexesassociated with both the RXR and RAR heterodimeric transcription factor complex at an HRE, and severalbasal transcription factors associated with RNA pol II at a target gene transcriptional start site. Thepresence of histone deacetylases (e.g. HDAC3) leads to removal of any chromatin activating histoneacetylation sites causing formation of transcriptionally repressed chromatin structure.
RXR is widely expressed with highest levels liver, kidney, spleen, placenta, and skin. The critical role forRXR in development is demonstrated by the fact that null mice are embryonic lethals. RXR is importantfor spermatogenesis and RXR has a restricted expression in the brain and muscle. The major differencebetween the RARs and RXRs is that the former exhibit highest affinity for all-trans-retinoic acid (all-trans-RA) and the latter for 9-cis-RA.
Additional super-family members are the peroxisome proliferator-activated receptors (PPARs). The PPARfamily is composed of three family members: PPAR, PPAR/, and PPAR. Each of these receptorsforms a heterodimer with the RXRs. The first family member identified was PPAR and it was found byvirtue of it binding to the fibrate class of anti-hyperlipidemic drugs or peroxisome proliferators.Subsequently it was shown that PPAR is the endogenous receptor for polyunsaturated fatty acids.PPAR is highly expressed in the liver, skeletal muscle, heart, and kidney. Its function in the liver is toinduce hepatic peroxisomal fatty acid oxidation during periods of fasting. Expression of PPAR is alsoseen in macrophage foam cells and vascular endothelium. Its role in these cells is thought to be theactivation of anti-inflammatory and anti-atherogenic effects. PPAR is a master regulator of adipogenesisand is most abundantly expressed in adipose tissue. Low levels of expression are also observed in liver
-
and skeletal muscle. PPAR was identified as the target of the thiazolidinedione (TZD) class of insulin-sensitizing drugs. The mechanism of action of the TZDs is a function of the activation of PPAR activityand the consequent activation of adipocytes leading to increased fat storage and secretion of insulin-sensitizing adipocytokines such as adiponectin. PPAR is expressed in most tissues and is involved in thepromotion of mitochondrial fatty acid oxidation, energy consumption, and thermogenesis. PPAR servesas the receptor for polyunsaturated fatty acids and VLDLs. Current pharmacologic targeting of PPAR isaimed at increasing HDL levels in humans since experiments in animals have shown that increasedPPAR levels result in increased HDL and reduced levels of serum triglycerides.
Genome wide association screening (GWAS) has demonstrated a role for polymorphisms in the PPARgene in the etiology of type 2 diabetes. As indicated above, pharmacologically, TZDs are useful in thetreatment of the hypoglycemia associated with type 2 diabetes. The TZDs bind to and alter the function ofPPAR resulting in reductions in circulating triglycerides which secondarily leads to reduced serumglucose levels and subsequently increased insulin sensitivity. It is still not completely clear how impairedPPAR signaling can affect the sensitivity of the body to insulin or indeed if the observed mutations are adirect or indirect cause of the symptoms of insulin resistance.
In addition to the nuclear receptors discussed here additional family members (discussed in more detail inthe Signal Transduction page) are the liver X receptors (LXRs), farnesoid X receptors (FXRs), thepregnane X receptor (PXR), the estrogen related receptors (ERR and ERR), the retinoid-related orphanreceptor (ROR), and the constitutive androstane receptor (CAR).
back to the top
Return to The Medical Biochemistry Page
Michael W King, PhD | 19962014 themedicalbiochemistrypage.org, LLC | info @themedicalbiochemistrypage.org
Last modified: April 6, 2015
Steroid and Thyroid HormonesIntroduction to the Steroid HormonesIntroduction to the Thyroid HormonesSteroid Hormone Biosynthesis ReactionsPrimary Enzyme Activities of Steroid Hormone Biosynthesis
Steroids of the Adrenal CortexRegulation of Adrenal Steroid SynthesisFunctions of the Adrenal Steroid HormonesClinical Significance of Defective Adrenal SteroidogenesisGonadal Steroid HormonesThyroid HormonesPrimary Activities of Thyroid Hormone (T3)Structures of the primary thyroid hormones
Hypo- and HyperparathyroidismSteroid and Thyroid Hormone ReceptorsLast modified: April 6, 2015