
thelink - TEC Services Association Homepage · made me think about how inventions have changed the...
28
Aurumn 2013 the link The quarterly magazine of the Telecare Services Association – The industry body for Telecare and Telehealth TECHNOLOGY ENABLED SERVICES – TRANSFORMING EVERYDAY LIFE NOW IP AND CENELEC LISTEN • HEAR • UNDERSTAND • RESPOND THE ESSENTIAL JOURNEY TOWARDS INTEGRATION
Transcript of thelink - TEC Services Association Homepage · made me think about how inventions have changed the...

Aur
umn
2013
thelinkThe quarterly magazine of the Telecare Services Association – The industry body for Telecare and Telehealth
TECHNOLOGY ENABLED SERVICES – TRANSFORMING EVERYDAY LIFE
NOW IP AND CENELECLISTEN • HEAR • UNDERSTAND • RESPONDTHE ESSENTIAL JOURNEY TOWARDS INTEGRATION
This is my Freedom, what’s yours?Jim | Wellesbourne, Warwick
Tunstall Healthcare is the UK’s leading provider of telehealthcare solutions. Our technology and services play a key role in helping older people like Jim and those with long-term health and care needs to stay out of hospital or residential care and enjoy a better quality of life.
Tunstall LifeCare Freedom to live your life.
tunstall.com
We used to play down our local and I still dust down my old Gibson from time to time and let her rip – if only to annoy Barbara next door. When the time comes, I’ll leave her to my grandson, but I’ve got no plans on packing my guitar away just yet.
“”

thelink 3
thelink
Telecare Services Association, Membership Services Centre, Suite 8, Wilmslow House, Grove Way, Wilmslow, Cheshire, SK9 5AG.Telephone 01625 520320 Fax 01625 533021 Email [email protected]
inside:Welcome to the Autumn edition of the Link magazine. Where has the year gone? As October draws to a close, we look forward to the evenings drawing in and the autumnal leaves falling to the ground.
This seasonal idyll is a lovely picture for many of us, but the darker nights, and the onset of colder weather serves only to heighten the feelings of isolation felt by many people up and down the country. How wonderful it is, therefore, to read about the continued hard work, and the incredible innovations developed by TSA members to increase the safety and security, and improve the health, of individuals across the UK. In this edition, we feature CareConnectMe, a new TSA member on page 7, and member news on pages 8 to 9 from Peaks and Plains to Cornwall. Our Chair, Lorna Muir, poses the interesting question of ‘What’s in a name?’ on page 4, and changing times are discussed by Trevor Single, TSA’s Chief Executive, on page 5.
The forthcoming International Telecare and Telehealth Conference which will be held at the London Hilton Metropole Hotel on 14-16 November, will showcase many of the innovations, and service successes, that have resulted in real improvements in the care and health for so many people, through the workshops and interactive sessions, keynote speeches and exhibition stands. With the demand for telecare and telehealth growing, developments continuing across technologies and services, imminent publication of the Whole System Demonstrators findings, and initiatives such as DALLAS taking shape, the whole feel of the industry is continuing to evolve, and we expect much of the debate at conference to centre around this changing landscape, how it will affect the industry and how the industry will cope. This year, over 75 speakers will participate in conference to give delegates the opportunity to tailor conference to suit their own particular issues and interests. In this edition of the Link we give you a taste of our own countdown to conference on page 10, and present articles from our main event sponsors on pages 11 to 17, whose invaluable support enables us to make conference the largest gathering of telecare and telehealth industry experts in Europe.
My thanks go to all our contributors who continue to make the Link such a great read. As always, the Link is as good as its contributors, so please keep your articles coming in. The next edition will be the Winter edition, and the deadline for receipt of articles, and advertising bookings, is 5 December 2011. If you have a new innovation, a great case study, or an opinion that has to be shared then please email your words to me at [email protected]
I hope you enjoy this edition of the Link, and I look forward to seeing many of you at conference in November.
Loretta MacInnes, Editor
Designed by Blue Sky Commercial Art 0208 650 0220
Articles We welcome your contributions – from short good news stories, case studies and member news, to detailed opinion pieces and features. Email your news, views and concerns to [email protected] by the deadlines below.
AdvertisingIf you have a new product or service that you would like to promote to a highly targeted telecare and telehealth audience, full information relating to advertising rates, as well as to website advertising for job vacancies and tenders is available from TSA Members Services – email [email protected] or telephone 01625 520320.
Deadlines for next editions are:
Winter 2013/14Copy date for articles:7 December 2013Booking date for advertisements:7 December 2013Supply of advertising copy to printers: 7 January 2013Publication date:w/c 20 January 2014
Spring 2014Copy date for articles: 7 March 2014Booking date for advertisements:7 March 2014Supply of advertising copy to printers: 28 March 2014Publication date:w/c 14 April 2014
Link disclaimerThe opinions expressed in the individual articles in this publication do not necessarily represent the views of the Telecare Services Association or indeed the formal policy of the contributor’s organisation. Data and information contained in any article or advertisement cannot be, and has not been, checked or verified by TSA. The Association cannot accept responsibility for any actions or decisions taken by readers based on any of the content of this publication.
© Copyright Notice thelink and its contents are the copyright of the Association. The contents of thelink may be reproduced by TSA members provided articles are copied in full and their origination is acknowledged.
thelink – Media Information
Loretta MacInnes, Editor
4 Our inventions mirror our secret wishes
Lorna Muir, TSA Chair
5 3millionlives – under new ownership!
Trevor Single, Chief Executive, TSA
6 Opinion – The essential journey towards integration Dr. M. J. Rice, Kokomo
7 Listen Hear Understand Respond Alyson Bell, TSA
8 Conference
15 Developing the Workforce Joanne Hatfield, Hull University
17 Member News
22 Legal Speak Neil Matthews, Field Fisher Waterhouse
23 Standards
24 NOW IP and CENELEC Marian Preece, TSA
25 TSA new members, dates
26 TSA Code of Practice for Telecare and Telehealth
Autumn is here – how this year is flying by! TSA has been busy over the past few months. In addition to the usual activities relating to conference development, code of practice work and general member interaction, we have been carrying out a series of Engagement days, where we have invited members to tell us, warts and all, what they think of us. The article on page 7 is a summary of this activity so far, and details how you can still participate if you weren’t able to make the engagement days. Further chances for you to participate in this feedback, together with a report of findings, will take place at conference.
The past few months have been a bit of a rollercoaster for the sector. The news of O2 leaving the sector for the time being was disappointing, particular after their trail blazing work to develop the consumer market. However, there are policy focuses across the UK that offer huge opportunities for our market including the Digital Challenge, Dementia Challenge, Vulnerable Older People and Reducing Avoidable Deaths within the Department of Health; the Towards 2020 plan for Scotland and Transforming Your Care in Northern Ireland. The Welsh Assembly have a consultation on a proposed framework for delivering integrated health and social care which closes on 31 October 2013. So the future is bright. The issue is timing.
We focus on policy, strategy and delivery within the forthcoming International Telecare and Telehealth Conference, which takes place at the Hilton Birmingham Metropole on 11 – 13 November 2013. This event is supported by seven main event sponsors, who enable us to add value and content into the event each year. Further details about the conference, and articles from a number of our main event sponsors can be found on pages 8 – 14.
Workforce development is featured in an article from Hull University on page 15, and Member News can be found on pages 17 – 20 including a delightful poem from Gateshead Care Call. Field Fisher Waterhouse’s Legal Speak, on page 22, covers the care home sector and the first organisation to achieve accreditation to the TSA Integrated Code of Practice – Telehealth is reviewed on page 23.
Thanks to everyone who has submitted articles for this edition, and made it such an interesting read.
The deadline for articles and advertisement booking is 7 December 2013 for the Winter edition. Please book and submit early to enable us to place your article or advertisement within the plan.
I look forward to receiving your pieces, and to seeing you at conference.
Loretta MacInnesEditor
This is my Freedom, what’s yours?Jim | Wellesbourne, Warwick
Tunstall Healthcare is the UK’s leading provider of telehealthcare solutions. Our technology and services play a key role in helping older people like Jim and those with long-term health and care needs to stay out of hospital or residential care and enjoy a better quality of life.
Tunstall LifeCare Freedom to live your life.
tunstall.com
We used to play down our local and I still dust down my old Gibson from time to time and let her rip – if only to annoy Barbara next door. When the time comes, I’ll leave her to my grandson, but I’ve got no plans on packing my guitar away just yet.
“”

thelink 4
Summer was fantastic wouldn’t you agree? We had back to back days of glorious sunshine, a new Royal baby and what about the
excitement of Andy Murray winning Wimbledon – it was almost too much.
I could barely contain myself and more than once my heart was in my mouth just waiting for that final match point. Every detail of the match was captured on a computer system that tracked the course of the ball and displayed a record of its probable path as a moving image. The system, called Hawk-Eye, was developed in the United Kingdom by Dr Paul Hawkins and was originally used in 2001 for televised cricket. The system is used in many sports nowadays and replaces the sometimes fallible opinion of linesmen and referees often accused of being slightly shortsighted! So much technology is available today and it made me think about how inventions have changed the way we live.
The beginning of the 20th century marked spectacular developments in air travel with Count Zeppelin’s airship in 1900. In 1901 the first radio receiver successfully picked up a radio transmission and in 1902 the first lie detector machine was invented by James Mackenzie (it’s true!). The Wright brothers created the first gas powered airplane in 1903 and did you know that in the same year it was a woman, Mary Anderson, who invented the windscreen wiper? 1913 and Gideon Sundback
invented the modern zip and in 1919 we have the pop-up toaster as well as short wave radio created. During the 1920’s we were introduced to the first robot, traffic signals, frozen food, the loudspeaker and car radios. The 30’s brought us sellotape, radar, photocopiers, the ballpoint pen and jet engines. Inventions and discoveries are endless throughout the years and the 1960s have been described as having the most important changes in history – by the end of that decade we had landed a man on the moon.
In the last 10 years we’ve witnessed some technology developments that would previously have belonged in science fiction books and films but are now a reality. Translucent concrete, 3D televisions, the virtual keyboard to name a few. When people become convinced about new devices or technologies and see the benefits they bring they lose their mystery and simply become part of everyday life. Can you imagine our world without computers, microwaves, vacuum cleaners, televisions or mobile phones? (My husband suggested I cross out the vacuum cleaner....)
The history of inventions is fascinating and lots of prototypes have been refined and developed over years until they become the products we know today. For example, for the medical profession the first stethoscope was invented in France in 1816 and consisted of a wooden tube that was like a trumpet. The device had frequent redesigns and improvements before being ready for the market in 1852. Although refinements have carried on into the 21st century the 1852 model is seen as the standard for the commercial market. The sphygnometer, or blood pressure gauge to you and me, was invented in 1881 by
Samuel Ritter von Basch but modernised in 1901 by Harvey Cushing. It’s stated that Cushing made the instrument popular with his fellow medics who happily adopted it to use with patients. Indeed until the introduction of newer digital models we were quite familiar with nurses and doctors using a hand sized air pump and gauge to take readings. Ultrasound equipment that can be used for both diagnostics and treatments was introduced to the medical world during the 1940s and today we have the capability for 3D and 4D scanning.
In essence, where would we be without great minds, inventions and ingenious technology solutions but also where would we be without the modernisers and pioneers willing to take a chance and embrace the new improved product? Our annual conference theme this year is focussed on how technology enabled services can transform lives. There will be opportunities to hear and see how newly developed or refined assistive technologies make a huge difference, not only to the individual user or carer but to the service provider, the medic, the emergency service. We should be optimistic that even if it might take years to win people over to the possibilities of assistive technologies there are many of us trying and like Mr Cushing with his sphygnometer we will get there in the end. It was Lawrence Durrell who stated “our inventions mirror our secret wishes” and, ridiculed initially by his family, the man who invented the invisibility cloak stated “ if only they could see me now!” Have a happy Autumn.
Lorna MuirChair
Lorna Muir, Chair
OUR INVENTIONS MIRROR OUR SECRET WISHES

thelink 5
Trevor Single, Chief Executive
When 3millionlives was set up in January 2012 it was launched as a partnership approach between the Department of Health (DH) and industry, working together to address the barriers to the mainstreaming of telecare and telehealth. How could the headline results of the Whole System Demonstrator project be used as a base for driving through the ‘industrialisation’ of telecare and telehealth. The TSA was a lead partner in this approach and a really encouraging factor for the TSA was that most of the industry group itself was made up of individual TSA members.
The drive to bring real benefit to the lives of 3 million users within five years was always an ambitious goal – and it is right that such a clear objective has been set. Much work has been undertaken since January 2012 by DH and the industry group in starting to tackle the major barriers that stand in the way of main scale adoption, and starting to change the business model for implementation. What we didn’t envisage was the extent that the wholesale change and re-structuring of the NHS would have on this particular programme!
In April of this year, under the re-organisation of the NHS, responsibility for 3millionlives was transferred to NHS England from DH. With NHS England comes a new ownership and a fresh approach to achieving the goals of 3millionlives. Dr Martin McShane, who is the Domain Director for Long Term
Conditions at NHS England, has stated: “The 3millionlives programme has enormous potential in the delivery of technology for the improved care of people with long-term conditions, and since taking responsibility for delivery and implementation of this programme, NHS England has worked to further develop it. We have agreed with the 3millionlives Industry Group that it will no longer operate in its current form, and established an Integrated Care for 3millionlives Stakeholder Forum, at which industry representatives will be invited to have a significant presence. The group will bring them together with clinical leaders, providers, the third sector and local government, to focus on several key priority issues around delivery and implementation of integrated care for 3millionlives”.
This change, and the emphasis on integrated care, is a move that the TSA has been quick to welcome and meetings have already taken place with the lead official in NHS England on how the Association can be a key player, through its members, in tackling the priority issues. So the industry group has not been axed. Instead it has moved to be part of a wider ‘Integrated Care’ group. One of the difficulties faced by the industry group was the inability to secure engagement with the wider circle of interested parties – such as clinicians, commissioners, the third sector, and other groups. The new emphasis and focus by NHS England enables that dialogue to take place.
This has to be the right approach. What we now need to get agreement on is some clear targets and short term deliverables for 3millionlives. This will start to deliver confidence for our members that successful implementation and main scaling of telecare and telehealth can be achieved. A clear delivery plan from NHS England in terms of tackling the barriers means TSA with its members can work in partnership to achieve those goals. The approach of localising procurement within the CCGs has its merits, but it also makes driving central policy into that arena much more difficult.
I was speaking at a recent American Telemedicine Association conference in Canada on the UK approach to integrated care. And after presenting the headline findings from the WSD project I was told by the conference chair that it had to be a no brainer that telecare and telehealth should be implemented in the UK. A cancer drug with the success identified by the WSD project would be adopted immediately.
We have to clear the decks of the barriers that inhibit adoption! Under the new ownership of NHS England, with a wider partnering approach, and TSA members leading on delivery, 3millionlives is not axed. Just redesigned!
Trevor Single, Chief Executive
www.telecare.org.uk
3millionlives – Under new ownership!‘Key telehealth group axed’ read a recent press article in the Health Service Journal, claiming that the 3millionlives industry group has been closed down! Other articles have sought to cement the view that the industry group has failed and as a result been closed down. However, the real position is far from the speculative journalism that has been presented.

OPINION
thelink 6
The dogs might be trained to bark or fetch the insulin injection kit and the diabetic patient then must do something about the barking. He could either adjust his diet to moderate the sugar levels, or perhaps slip the dog a biscuit to cease the barking and make him complicit in the illicit feasting that triggered the sugar rush. The dog provides the self-management support and exacerbation alerting; but only the patient can perform the corrective tasks. These dogs perform a connected care model rather like Lassie in the movies, who every Saturday morning would connect those who can provide support, to those who fall down wells! Modern diabetic service dogs are better than Lassie as they detect changes in blood chemistry before someone falls down the well. In a connected care model for long term conditions, the question is: how should the service respond to the dog barking and whose cuff should the dog be tugging, to get support for his master.
The problem with the Diabetes ‘service’ dog model is cost. These wonderful creatures cost £20,000 each to train and a CCG Commissioner can buy a lot of Blood Glucose Meters for that price. The latest NHS report from Sir Bruce Keogh suggests that in the last 6 years the number of people diagnosed with diabetes has risen by a third and that by 2030 three in every four adults will suffer from either heart disease or diabetes. Therefore, long term condition management needs industrial scale solutions with low unit costs. We need economies of scale that allow repeatable NICE care procedures, carried out by lowest clinical grade staff. We need to design a service that de-personalises medical care into simple repeatable standard care. We have to treat those patients with high complex acute conditions, via an entirely different health care service than we treat low complexity, single or double morbid, chronic disease patients. Acute patient care needs highly personalised specialist care allowing physicans the full scope of medical freedom to act as they see fit. Chronic patient care needs evidence based guidelines that show which clinical tasks to perform at each moment to slow the progression of the disease. One is personalised medicine, performed by GPs; one is de-personalised disease management, overseen by GPs. GPs are good at diagnosing a disease, they are trained to prescribe evidence based treatment plans to ameliorate its progression. However when it comes to the longer term disease
follow up, the GPs as commissioners must help create the care delivery system that ensures their patients receive consistent high quality care, supervise the creation of the care plan to which the patient is assigned and ensure the plan is being adhered to by the nursing and call centre coordination staff. Treatment rules must be written so all members of a clinical team, not just those with a medical degree can follow them. In fact, it would be an inefficient Integrated Care system, if only the precious resources of people with medical degrees could help high volumes of patients follow a low complexity care pathway. Care coordination is a logical and necessary part of a disease management service in these high volume and low complexity care pathways. Integrated Care services should be delivered by a multi-disciplined care team of Allied Health Professionals lead by GPs and orchestrated and administered by an integrated care call centre.
This places a challenge to the TSA accredited monitoring centres. To be relevant in these new integrated health and social care support models, you must finish the up-skilling journey from social alarm centres, to assistive technology centres, to telehealth centres and finally to integrated care and support centres. The prize is worth the journey; the first wave of CCG tenders in this space, have a combined budget of approximately £1 Billion.
Trafford CCG requires a Patient Care Coordination Centre to track individual patient journeys and to provide close monitoring of vulnerable patients, by following them through their care journey. The Care Co-ordination centre will be the glue that holds together all the provision of local community, GP and scheduled care services. It is envisaged that all patient journeys will go through this service and the Centre will be an approximately 70 seat call centre staffed by non-clinical staff.
Cambridgeshire and Peterborough CCG are commissioning an integrated hospital and community service for older people which focuses on joining up unplanned acute and community care pathways. The lead provider will utilise the appropriate infrastructure to provide a single point of access, a single live directory and proactively scheduled patient appointments and transport. The CCG said: “Currently the focus is on measuring and paying for activity, such as hospital admissions. The CCG is proposing to dramatically change this
Like Guide Dogs for the Blind, we can now train Diabetes ‘service’ dogs to identify and assist diabetic patients during hypoglycemic and hyperglycemic attacks. These wonderful dogs smell body chemistry changes and can be trained to perform a series of tasks once alerted.
focus to improve quality and outcomes through supporting investment in community services, improving the way in which services are delivered and changing the funding approach. The new lead provider(s), will both provide services for older people, and be responsible for coordinating care for older people”
Ten bidders have been announced for the £800m Older People’s pathway: • AlbionCareAllianceCommunityInterest
Company• CambridgeshireandPeterboroughNHS
Foundation Trust with Cambridge University Hospitals NHS Foundation Trust• CapitawithCambridgeshireCommunity
Services NHS Trust, Circle Partnership and Oxford Health NHS Foundation Trust• CareUKwithLincolnshireCommunityHealth
Services NHS Trusts, Norfolk Community Health & Care NHS Trust, and United Health.• InterservewithCentralEssexCommunity
Services• NorthEssexPartnershipUniversityNHS
Foundation Trust• NorthamptonshireHealthcareNHS
Foundation Trust• Serco• UnitedHealthUK• VirginCareLtd
Oldham CCG have specified that their Integrated Care service be built around a ‘Patient Centred Medical Home’ which places the GPs at the centre of the integrated care approach. A non-clinical Call Centre is required to ensure care is coordinated and integrated between health care systems, for example across specialists, hospitals, home health agencies, and nursing homes.
Integrated Care is the future for Community Service and since 70% of budgets will be spent on LTCs, it is not surprising that CCGs are commissioning Integrated Care services to provide better standards of care whilst driving efficiencies into Community Services. Be ready, because TSA monitoring centres will provide a vital piece of the support network if Integrated Care is to work in localities.
Dr. M.J. Rice
Principal Consultant – Kokomo
www.kokomo.eu
THE ESSENTIAL JOURNEY TOWARDS INTEGRATION

thelink 7
TSA is striving to be an organisation that:
• leads,representsandpromotestechnology enabled care and support
• supportstheprovisionofhighqualitytechnology enabled care and support
• isfitforpurposetodelivertheTSAvisionand grow the industry
Ultimately, TSA wants to be a membership organisation that you feel proud to be a part of.
Through attending a number of forums across the country I have had the pleasure of gaining some insight into how we are serving you as members. As we move toward year two of our current three year business plan, I wanted to delve more deeply into your views of us as your representative body and find out where improvements should be made in order for us to become the organisation that you are proud to be a part of.
In order to gather your views, and to provide you with an environment where you could feel that you could be open, the Board gave approval to appoint an external consultant to facilitate a series of engagement days to begin this process. The information gathered would be used to develop the strategy and objectives for year two onwards of our business plan, and also to provide a benchmark to measure TSA against one of its performance targets of achieving a 90% customer satisfaction rate by 2016. As per the Collins definition – we wanted not only to listen, but to take heed – and then take action.
Members were invited to a series of open days across the country and we were delighted that members were able to take time out of their busy schedules to attend.
Feedback Lysa Morrison, the external facilitator for these events, is currently summarising your feedback from the four workshops that have been held to date, and has outlined below some of the comments received so far about the structure and content of the days:
“I was cynical at first but I really believe TSA might actually be listening this time”
“Enlightening that listening is the key focus”
“Look forward to the future”
“Very refreshing today”
“Today was a great idea and proves TSA are listening and deciding to take action”
“Buy in from suppliers by moving us and asking the right questions”
“Needs a result”
At first glance, the kind of feedback TSA has received so far has been very mixed. There are some excellent comments about what you like about TSA and what you want to see TSA do more of, such as: “Being a member of TSA helps me promote my business”; “be more strategic”; “we want more support around helping us achieve the Code of Practice and business models”.
There have also been some really useful constructive feedback around what you want TSA to do better or differently such as: “demonstrate better value for money”; “it feels like its them and us”; “the Code of Practice needs a review”.
The engagement continuesThis engagement process is ongoing. We would like as many members and non-members as possible to get involved and share their views and ideas. At one of the engagement workshops somebody said “we need help to work together as a group to make the cake bigger then we can all have a bigger slice!” The only way this can be achieved is if you are open and honest with TSA by telling us what works well, what you
want them to do more of, what doesn’t work so well and what you would like us to do differently.
If you weren’t able to attend one of the engagement days, you can still get involved by contacting Lysa Morrison at LMA directly via her email: [email protected] and she will send you a copy of the questions we have been asking at the engagement workshops. All feedback will kept completely confidential between the sender and LMA, and will be anonymised within the final report. We would be really grateful if you could contact Lysa and get your responses back to her by the 31 October 2013.
Next stepsOnce all the feedback has been received, I will present the findings back to members at an interactive session at conference. The session will begin to tie in your feedback with the business priorities and overall strategy.
The process does not end there. Lysa will be available at conference to gather further ideas and feedback from both members and non members. Engaging with you in an open and honest way will become an intrinsic part of our business to enable you to contribute your ideas and shape how TSA’s products and services are delivered.
Thank you to everyone who has contributed so far. Please do take the opportunity to contact Lysa and feed into the engagement process if you haven’t yet done so.
I look forward to meeting you at conference in November, or at a TSA event in the not too distant future. If you would like to contact me directly about any of the above, or any other industry issues please do so:
ENGAGEMENT
Listen Hear Understand Respond
Alyson Bell, Managing Director, TSA
The Collins dictionary definition of listening is: the act of taking heed; paying attention.
The TSA Vision‘People choosing technology enabled care
and support to enrich everyday life’

thelink 8
The 2013 International Telecare and Telehealth Conference has a theme that some will see as aspirational – but the transformation of everyday life is a fact for those individuals who are currently receiving these services. There are many more people who should be benefiting and the number of people who are potentially missing out will grow as the population ages and we encounter the increasing pressures across health and social care.
So how do we make the step change from these services going from bolt-on, to becoming an integral part of health and social care delivery, and where people choose the services either by request to their clinician or care provider, or directly from a service supplier?
This year’s conference programme is focussed on this key question. The answer is multi-faceted. Policy, strategy, delivery – we have to influence all of these in order to ensure technology enabled services play their important part in this transformation agenda.
Plenary speakers include key health and social care policy makers from across the UK: Norman Lamb MP, Minister of State for Care and Support will deliver a key note address on Tuesday 12 November. He will be joined by Edwin Poots MLA, Minister for Health, Social Services and Public Safety, Northern Ireland and Michael Matheson MSP, Minister for Public Health, Scottish Government. The strategies that are being developed to deliver this transformation will be outlined and open for questioning from expert speakers including George Crooks, Medical Director for NHS 24 and Director of the Scottish Centre for Telehealth & Telecare and Sandie Keene, President, Association of Directors of Adult Social Services.
Commissioners of these services must have a clear understanding of what’s on offer and how technology enabled services fit within service redesign. On Monday 11 November, we have a commissioner focussed session where we will hear from health and social care professionals who are making significant changes to their service delivery. We invite all TSA members who are coming to full conference to bring their commissioner on this day to ensure they can benefit from this session. All attendees must be registered, so if you intent to take advantage of this offer, please email your commissioners details to [email protected] once you have completed your own full conference booking form.
In addition to the expert speakers within plenary, conference has a series of workshops across Monday and Tuesday, where delegates can learn from experts across four key streams:
• Personcentredcare
• DevelopingandCommissioningQualityServices
• ServiceIntegration
• ServiceRedesign
Breakout sessions include a mix of interactive workshops and seminar presentations. The full selection is available online (http://www.telecare.org.uk/conference/breakout-sessions) and attendees can pre-select their choice for each session. I recommend that you do pre-select as soon as possible as workshop rooms have maximum capacities, and popular sessions fill up quickly.
The Exhibition Zone remains the place for business, featuring the leading organisations who develop, supply and deliver these vital technologies and services. All refreshment breaks and lunches (on Monday and Tuesday) take place in the Exhibition Zone, and attendees will have plenty of opportunity to view the latest technology and services on offer. We also feature a central speaking area within the exhibition zone, where additional workshops will run.
As always, conference features a full entertainment programme. On Monday, the evening will begin in the Exhibition Zone, where a number of exhibitors will welcome delegates for a fun start to the evening. Attendees can have a drink, interact with the exhibitors and participate in the launch of the ALIP project. Dinner on Monday will feature the Code of Practice Awards and dancing with a disco until late. Tuesday will feature an International Reception hosted by UKTI, pre-dinner drinks (pay bar) in the Library Suite and the Gala Dinner (black tie optional) featuring the announcement of the winners of this year’s Crystal Awards, followed by a live band. Each year we feature a raffle at the Gala Dinner, and this year the benefiting organisations will be the Automated Defibrillator charity in support of the work by Fabrice Muamba, our guest speaker on Tuesday 12 November and Help the Heroes in recognition of our event running across Remembrance Day.
Business development is a key part of conference, and new for this year is a
partnership with UKTI. UKTI will be running a ‘Meet the Buyers’ session throughout conference, where a number of overseas organisations who are interested in doing business in the UK will have the chance to meet UK organisations during conference. Attendees will be given the opportunity to book appointments before the start of conference, and further details will be emailed to all attendees as soon as they become available.
Conference is a major event for TSA. Each year we have the support of main event sponsors, who enable us to begin development early in the year and add extra value for conference attendees. Without their support we would be unable to put on such a full event, and we thank each of our main event sponsors, outlined below, for their commitment:
Bosch Healthcare
Chubb Community Care
Green Access
Medvivo
Solutions4Health
Tunstall
Verklizan
A number of our sponsors have written articles for this edition, and they are featured over the next few pages.
On Wednesday 13 November we will be running a feedback session, presented by Alyson Bell, on the independent TSA engagement that has been carried out over the past months (see the article on page 7 of this edition for more information). Conference attendees (members and non members) are invited to participate and we look forward to presenting the findings and gaining further insights from you all.
The full conference will be CPD certified. Not only is it the main networking event for the sector, but it is also valuable certified professional development. Bookings are still being taken, so if you haven’t secured your place yet, you can find all the details on the TSA website: www.telecare.org.uk/conference. Alternatively, contact the TSA office ([email protected]) and we will email a booking form to you. I look forward to meeting you at Conference in November.
Loretta MacInnes
www.telecare.org.uk
Technology Enabled Services – Transforming Everyday Lives
11- 13 November 2013, Hilton Birmingham Metropole

thelink 9
CONFERENCE
Our ageing population is leading us to rethink the structure of our society in so many ways. It is no coincidence that all three main political parties are advocating their own take on an integrated health and social care system, whether that’s through a single budget, department or governance structure. The end goal is the same – to get health and social care working together.
There is good reason for this. As we get older we increasingly rely on both services. Therefore, as more and more people rely on both these services, the systemic disconnect between the two will be ever more unsustainable.
The problem is that while we debate this, time is moving on. For the arguments around implementing technology into health and social care are not purely intellectual. There’s a cold economic reality that makes this conversation necessary.
We need to start finding ways to reduce the number of health and social care professionals working with an increasing number of patients. The concept of service integration is at the centre of that objective.
Integral to this integration is taking pre-emptive action to prevent users moving unnecessarily between the two services. A key component of this is to ensure that people are able to remain in their homes, comfortably, for as long as possible.
This goal lies at the heart of our commitment to provide more ambient and user friendly solutions which combine monitoring services, fixed telecare systems and mobile solutions that deliver a “virtual safety net” for users and families.
The baby boomer generation, of which I’m one, is increasingly taking on the role of carer for their parents, who are now entering old age. Inevitably one of the key concerns for those caring for their parents, whether in their own home or at a care home, is the dangers associated with a bad fall. It is a stark statistic that falls are a major cause of injury and death among the over 70s and account for more than 50% of hospital admissions for accidental injury.
Our ambient solution’s primary function is to detect those falls as soon as possible to ensure a rapid and appropriate response. A quickly dealt with tumble can mean the difference between easy treatment in the home and possibly a distressing trip to A&E. When this costs as much as £2000 per admission it is not only an emotional argument but an economic one too.
The smart sensors built into our system also avoid unnecessary ‘false alarms’ that can lead to the call out of staff (costing money) or more importantly worried family members. These solutions therefore offer carers peace of mind - knowing that there are professionals on the end of the line who have the latest information on the whereabouts of your loved one is a huge weight off anyone’s shoulders.
Gerry Allmark, Director, Sales and Account Management, Bosch Healthcare UK and Non-Executive Director, Telecare Services Association
It is difficult to read a health publication, comment piece, or political speech on health and social care these days without having your attention drawn to the pending demographic challenges we face.

thelink 10
CONFERENCE
The effectiveness of telehealth, in terms of improved outcomes for patients, efficiency savings and cost effectiveness is a continual hotbed of debate. Clinicians, commissioners and providers alike have a myriad of opinions and experiences. With this in mind, and in an effort to bridge the knowledge gap left by studies such as the Whole Systems Demonstrator, The Medvivo Group, a leading telehealth provider, has been working with Professor Nick Bosanquet at Imperial College London to assess the effectiveness of telehealth interventions.
The Portsdown Group Practice operates across 4 surgeries and covers Portsmouth and the surrounding areas. Of the 30,000 patients, 14.5% of the practice population is aged over 65.
Dr Julian Neal, Senior Partner at the Portsdown Practice explains, “Long-term conditions are becoming an increasing problem in general practice, and these patients will inevitably need extra attention after the initial diagnosis and during more challenging periods of their diseases. This means that a significant proportion of our patients will benefit from telehealth at one time or another.”
Portsdown Group Practice is an innovative practice who wanted to improve and increase the services they offered patients through efficiency savings and empowering patients to self-manage their long-term conditions.
Using Medvivo’s wealth of experience the services that have often been the hardest for traditional services to offer have been identified:
• Compositionofclinicalprotocolsreflectingthe input and approval of senior specialists
• Supportinpatientrecruitment
• Scheduling&performinginstallations
• Trainingthepatientinhowtousetheequipment
• Nurse-ledClinicalcasemanagement
Dr Julian Neal, Senior Partner at The Portsmouth Group Practice.
Using the organisations HomePod, patients record their vital signs and answer pertinent questions about their health which allows nurses to gain a greater insight into their disease and enables them to optimize their treatment enabling much needed support during difficult times, empowering them to take greater control and gain understanding about their condition.
Dr Julian Neal explains, “Telehealth is about doing things differently. At the moment the NHS is facing a deluge of work, most of which is actually to do with ageing population with long term conditions. You simply cannot allow the triaging of every individual patient who has a telehealth system in their home to be done by people who are currently working in the community, all that does is it adds to their current workload rather than improves it. So central case management is the way that you get the financial and the efficiency gain.
“For example we see diabetic patients 3 times a year on average, so we are getting 3 snapshots a year of how they really are. With telehealth we can measure their blood pressure, their pulse, their blood glucose levels, how they are feeling on a daily basis without involving any of the current partners or practice staff by monitoring this remotely by a specialist nurse that we trust, who can, by him or herself look after between 200 and 300 patients quite easily every day. And that is a revolutionary new way of delivering healthcare to people living with long term conditions”.
www.medvivo.com
A case study investigating the effectiveness and cost effectiveness of a fully managed telehealth service in the management of COPD patients and Heart Failure patients in a GP Practice setting.
This session will provide an update on a unique observational study conducted by Medvivo, Prof Nick Bosanquet, Imperial College London and the Portsdown GP Practice Group, Portsmouth. Donal Markey, the Clinical Director of Telehealth at Medvivo will speak at the TSA’s annual conference and will be presenting the latest results of this on-going 2-year study in his workshop on the 11th November, 2pm.
THE PORTSDOWN CASE STUDYAN OVERVIEW OF THE FORTHCOMING CONFERENCE WORKSHOP
• De-installationandcleaningofequipmentto pass on to the next patient
• Supportofdataanalysis–bothquantitative and qualitative
This reflects the most effective and efficient model of telehealth delivery. Additionally, robust project management should be in place to support the initiation and expansion of telehealth services, supporting the NHS teams to deliver high quality services they want for their patients.
A key component of an effective telehealth intervention is having dedicated Specialist Nurses managing telehealth patients. This not only ensures the scalability of the service but also the guarantee that effective, meaningful interventions are taking place, keeping patients healthy and in the comfort of their own home.
The aim of ‘The Complete Telehealth Solution’ (the service being delivered to The Portsdown Group Practice) is to reduce hospital admissions for patients with conditions such as COPD and CHF thus reducing the acute care costs for these patient cohorts.
“Working in partnership with Medvivo has given us the opportunity to support our patients whilst enabling our clinicians to focus on the most complex cases. The Complete Telehealth Solution is the only viable option to ensure high standards of care are met and maintained during this time of efficiencies, and actually represents improved care pathways for Long Term Conditions through self-management
“It is clear that telehealth is good for patients; clinical outcomes are improved, lives are saved and admissions are prevented. Patient engagement with their long term condition also increases. My own experience of telehealth suggests that significant cost savings can only be generated if a central nurse-led case management service is at the heart of any telehealth service” explains

thelink 11
CONFERENCE
As a developer of integrated care systems for management of long term conditions (LTCs), Solutions4Health is highly positive about the change because, in its new form, 3millionlives will bring together clinical leaders, providers, the third sector and local government. Together, we will focus on key priority issues around delivery and implementation of integrated care through a partnership matrix approach of clinical advocacy, service improvement and technology strategy. It puts the programme right at the heart of those areas where it can have a maximum impact, and Solutions4Health is right behind the move.
NHS England is fully operational, so we expect the new brand owners to be proactive, tying up loose ends and making sure that issues on LTCs are in the right hands. We intend to play an active role, because we already understand technology within an integrated care setting, as our track record in community health programmes shows.
More
To be a telehealth company in isolation would be too limiting for our organisation. We have hands-on healthcare experience, alongside the technical innovation and knowhow, giving us a deeper understanding and involvement in healthcare delivery,
which is what the NHS needs in order to move forward with the application of technology. Our focus is on providing self-management systems that support clinicians as well as patients, playing an important role in managing and monitoring LTCs, keeping in contact, handling data and involving the clinician at key points in the event of an exacerbation.
For years, we have been supporting the NHS – and now, local authorities - to deliver their targets and outcomes. We understand how to let people in hard to reach parts of the community access our services, be they health checks, smoking cessation or chronic condition self-management programmes.
Our integrated care pilot for heart failure, in development at London’s Whipps Cross Hospital, has a selected patient cohort, self-monitoring and entering data for remote monitoring by specialist nurses. Under the guidance of consultant cardiologist Dr Sandy Gupta (also a member of our medical board), the pilot is aimed at increasing patient freedom, testing the network infrastructure and our case manager software, and exploring the range of devices that can be used at either end of the communication chain.
For this and other pilots, we are working inpartnershipwithQualcomm,using
Backing the Move towards INTEGRATED CARE
their open network “ecosystem” – which will enable many more mass market opportunities for Solutions4Health, as well as other enterprising companies.
Successful telehealth service delivery requires a good understanding of the care pathway, an ability to develop strong relationships with the project stake holders, and being able to work through a complex hierarchy of hospital GPs, practice GPs, pharmacies and community organisations – something that NHS England knows well.
When it comes to the technology, our information management systems allow input and comprehensive data monitoring support at all stages, and in a number of ways. Moving to a web-enabled user interface has meant flexible access which, with so many different kinds of users, has become essential. Our internet-based iTelehealth® systems, accommodate online video communications, and incorporate Microsoft’s HealthVault secure personal health record database. As overall service providers and administrators, we also need to track service performance, monitor costs, generate invoices and produce reports.
www.solutions4health.co.uk
By John Guyatt, TeleHealth & Information Systems Director, Solutions4Health Ltd
The 3millionlives programme has renewed its potential to deliver technology for
the improved care of people with long-term conditions. Now in the ownership of
NHS England, it’s especially positive that it will be associated with a much broader
range of technology solutions, integrated care services and organisations.

thelink 12
CONFERENCE
NHS Calderdale Clinical Commissioning Group (CCG) and Calderdale Metropolitan Borough Council (CMBC) are working in partnership with leading telehealthcare provider Tunstall Healthcare, to provide advanced telehealth and telecare solutions that will help to support people with long-term conditions.
NHS Calderdale CCG has worked alongside service providers to develop a new model of care to increase the level of support in care homes and improve outcomes. The new model includes the development of a multi-disciplinary team, who will be available to support and advise staff in care homes on the prevention and proactive management of the needs of older people, including fall prevention and medication management.
A crucial part of the model focuses on the development of telehealth and telecare in 25 care homes, and will include the UK’s largest deployment into care homes. By supporting the analysis and treatment of people with care needs, this will improve their quality of life, and offer additional support for carers and family members.
This part of the programme is rolling out in two phases. Phase one is focusing on providing telecare solutions to 25 nursing and residential homes across the region.
Carl Stevenson, Manager at Summerfield House Nursing Home in Halifax said: “The introduction of the telecare solution at Summerfield House will provide extra reassurance for our residents that staff will be alerted immediately, should they require assistance. The range of sensors gives telecare users the peace of mind that their needs are being monitored at all times.”
Phase two will enable a further 500 residents in care homes to benefit from telehealth solutions by early 2014. Recent studies have shown that emergency hospital admissions grew by 4% in Calderdale, between 2008 and 2011. The region’s new approach will help to avoid unnecessary hospitalisation through early intervention, management of risks and improved medicine compliance as well as supporting people with round the clock assistance.
Dr Steven Cleasby, Clinical Lead for Care Homes and Safeguarding, at NHS Calderdale CCG, said: “As part of our Commissioning Plan for 2012/13, we set out a clear objective to transform health within Calderdale by looking to improve patient care and safety, whilst also addressing some of the challenges faced by clinicians in primary care. Telehealth and telecare provides us with the opportunity to encourage self-management and better care and support. In turn this can help reduce costs on the NHS caused in part by unnecessary hospital and GP visits.
“Working with GPs, we have identified the opportunity to help people with long-term conditions, and to help better manage the risks of everyday living for local care home residents, reducing the pressure on services and enhancing quality of life.”
Calderdale Council’s Cabinet Member for Adults, Health and Social Care, Cllr Bob Metcalfe, said:
“Calderdale Council is very pleased and committed to be working in this partnership to provide more personal safeguarding and reassurance for both care residents and their families, with the introduction of telecare and telehealth in local care homes.”
Supporting patients with Chronic Obstructive Pulmonary Disease (COPD)
Telehealth will initially be offered to 24 COPD patients in their own home at any one time, with the initiative expected to develop and to benefit many more patients in the region. Each patient will receive Tunstall’s mymedic solution, which will enable clinicians to remotely monitor vital signs including blood pressure, pulse rate, and blood oxygen levels on a daily basis. The objectives are to support early discharge and prevent hospital admissions, improve self-management, prevent future complications for those with COPD who haven’t yet started to access extensive healthcare, and support the COPD specialist nurses’ workload.
Joanna Birch, Clinical Director for Intermediate Care and Community (CHFT) said: “The ability to self-manage a long term condition can be
life changing. Providing telehealth to patients with COPD gives them a better understanding of their condition and allows them to make choices that will improve independence and quality of life. With guidance from our team of specialist nurses, the initiative will go some way to reducing unplanned emergency admissions and supporting early discharge of patients with COPD.”
A patient currently using the service, said: “Telehealth is helping me to better understand and manage my condition. The equipment is really easy to use and it gives me more confidence knowing that the nursing team can keep a close eye on my readings, and help me if I need it.”
NHS Calderdale serves a population of 213,000 people, with 18% of people in Calderdale recorded as having a long-term condition. Those people with long-term conditions who are frequently admitted to hospital also account for 36.5% of overall bed day usage.
This new initiative is in the early stages of delivery, providing a service into people’s homes under the supervision and with the dedicated assistance of Calderdale and Huddersfield NHS Foundation Trust COPD specialist nurses. This new approach will help to avoid hospitalisation through early intervention, management of risks and improved medicine compliance.
NHS Calderdale CCG is also working alongside service providers to develop a new model of careaspartofits“QuestforQualityinCareHomes” initiative, which will increase the level of support in care homes and improve outcomes for up to 1000 residents.
www.tunstall.com
NHS Calderdale Clinical Commissioning Group Launches “Quest for Quality in Care Homes” and new Telehealth Initiative

thelink 13
CONFERENCE
In 2013, thirty years later, Verklizan has grown beyond all expectations. Our UMO monitoring platform is now in use by 267 organisations across 14 countries, providing telecare and telehealth services to over 842,000 people. This year we celebrate other important anniversaries across the group: UMO was born 20 years ago, our business in Germany is now 10 years old, the Spanish subsidiary is 6 and the UK business is 5 years old.
To help in our celebrations, we have invited some of our TSA Code of Practice accredited customers to join us on our stand at the TSA International Telecare and Telehealth Conference in November. Come and visit us on stands 18 and 19 to see how they use UMO to deliver their unique services – and learn how UMO will transform the way you offer your own services.
Paul Shead, Managing Director, Verklizan Ltd
www.verklizan.co.uk
In 1983, Kajagoogoo were high in the charts with Too Shy, with Limahl sporting a non-too-shy peacock mullet. Clark Kent was battling his “gone bad” self in Superman III, and Ewoks were fighting off storm troopers in Return of the Jedi. I was wearing white socks with my school uniform and wearing my tie back to front “skinny style”. The same year in Holland, three young engineers formed a company called Verklizan.
Astraline is a TSA accredited ARC based in Poynton, Cheshire and is part of “Johnnie” Johnson Housing. Established in 2000, and benefitting from being part of a housing association with over 40 years of experience, Astraline has around 80 corporate clients from a variety of industries. We offer monitoring and call handling services including telecare, lone worker monitoring, anti-social behaviour logging and out of hours call handling.
As the first organisation in the UK to implement UMO, Astraline is proud of its history of working with Verklizan over the past 5 years to maximise our use of the UMO system. UMO’s open protocol approach enables Astraline to monitor any industry standard devices, and future-proofs our investment by ensuring that we will be able to monitor new devices including those operating the BS8521 protocol. UMO also allows us to monitor both social alarm and lone worker traffic from one system.
Using UMO enables Astraline to offer bespoke services to meet the needs of
clients. One particularly valuable feature is the ability for us to offer our clients a hosted solution. This allows a client to take their own calls during working hours using Astraline’s UMO system, and then hand over to Astraline for the out of hours shifts, safe in the knowledge that this is a seamless transition without the need for any data transfer – it’s all in our system already! For many clients this can be a ‘win/win’ scenario, enabling them to benefit from Astraline’s investment in the UMO technology, and Astraline’s proven 24/7 operation, but also allowing the client to retain their own direct service to their residents during ‘core’ hours. The client can also directly access our UMO database to maintain their residents’ data themselves, again removing the need for exchanging sensitive information.
This year we celebrate 26 years of providing quality services to enable people to live independently in their own homes. Wherever possible we provide end to end services, with needs and risk assessment, installation, monitoring, response and domiciliary care through to crisis care response. We tailor the service to the person from the menu of services and equipment, as well as the most cost effective way for them to pay. We link in with other organisations and charities such as Homeground to find funding for those who cannot afford it themselves. We are accredited to the TSA Code of Practice and also to CHAS to ensure quality health and safety standards across theboard.OurCQCregistrationallowsus to bring direct personal care into the portfolio, and our responders are moving and handling trained which means that we can assist with lifting and avoiding unnecessary ambulance callouts.
We work in partnership with Local Authorities and other providers to bring a bespoke solution to the challenges that the economic climate and funding cuts bring.
In 2011 we entered a unique partnership with Suffolk County Council as a 50/50 Community Interest Company ; Suffolk Careline; who now provide county-wide monitoring, response, installations, a wide range of assistive technology and Crisis Response. Our aim is to promote the services Telecare and Assistive Technology and raise awareness of what is available which will allow people to remain in their own homes safely and cost effectively. We use UMO to seamlessly deploy our services to multiple offices across England.

CONFERENCE
thelink 14
Well you can now with the implementation of an intelligent hub and bespoke infra-structure you can design and offer a solution that allows to bring all of your communities and services together seamlessly, this in turn means that you can offer a better level of care and support to your clients and allows you to have both a better understanding of your systems and their current status.
i-Care from Green Access is an intelligent home hub that can bring together all services to offer you a single device solution, so no longer do you need a dispersed alarm, door entry, telephone or separate Telehealth device. In addition to combining all services into a single device the i-Care adapts with the user’s needs, so as health conditions change the device can adjust in line to ensure that you have the flexibility to receive the very best personalised care from today’s technology.
All of these benefits can only be achieved by offering a unique approach to technology, as the I-care embraces a truly open platform. This in turn allows you to integrate and utilise other manufacturer devices with our system. So if you have existing pendants, sensors, pull cords these can all be retained therefore reducing further change for the users or disruption to décor. So whether these devices are hard wired or wireless the I-care hub can accept them and communicate with them.
The i-Care added security levels ensuring piece of mind and flexibility in terms of the frequency on which the device is monitored. i-Care is monitored via a digital heartbeat frequently so as the care provider you will know the status of every device remotely as regularly as every 4 minutes, this can of course be adjusted to suit your care provision plans but we feel it is imperative that you know the current status at all times.
The concerns that we hear and face on a daily basis with the implementation of an i-Care system is that to provide a broadband connection is expensive, well this is not the case as the system only requires a VOIP telephone line which any standard telephone line can be converted to for as little as a £1 per month (dependant on provider). Other telephone line issues include outlying properties with no internet, well we can look at telephone conversions or we can even offer a plug in device allowing GSM/GPRS solution for these instances. We can even build these fail safes into the system in the event of an internet connection drop out.
Monitoring station connectivity is achievable with the i-Care system as it is capable of working with a variety of ARC’s. In summary as long as the ARC’s can receive an incoming IP signal then we can communicate, even if they can’t our in house design team can design solutions to allow full communication. But i-Care doesn’t just offer signal and identification alerts it can offer two way video link to allow you to asses the full extent of the residents needs. This in turn offers the resident greater re-assurance that the alert is being actioned and they know that they are receiving the most personal level of attention possible.
Green Access part of AME international manufacturing group, who have a vast experience in working with companies such as BT, GE Medical, Samsung and other Blue Chip Companies, we can fully offer a solution that can bring healthcare and communications together.
But most of all we feel that you should be able to access worldwide forefront technology, that is designed for you as an individual and develops with your needs. So if you need a medication reminder, you need connection to family members, you require Telehealth facilities, 2 way video conferencing or incoming mail alerts for communication from your care provider you can have these facilities readily and easily accessible, because this to us is what personalised care can offer through the power of technology.
By achieving this you have a true “futureproof” solution that offers you products and services that you require and allows you to stay connected with loved ones and carers, offering a peace of mind and re-assurance.
www.greenaccess.plc.uk
Are you striving to offer your residents, clients and customers a solution that can connect your services and communities together to offer the best provision of care?
In today’s world of technology where we can watch TV whilst on the move why can’t you do this?
11 – 13 November 2013Birmingham Hilton Metropole
DON’T MISS OUT – SECURE YOUR PLACE TODAYwww.telecare.org.uk/conference
email: [email protected]
thelink 15
WORKFORCE DEVELOPMENT
Telehealth and Telecare: Developing the Workforce
However, new technologies can provide approaches to care that improve clinical outcomes, enhance quality of life and deliver cost savings. The use of telehealth and telecare interventions is becoming increasingly commonplace and mainstream, but examples of formal education focused on these modalities of care are few and far between. This lack of workforce development opportunities is a drag on the wider adoption and acceptance of telehealth and telecare: if staff are not aware of the applications, benefits and challenges of new technologies, then their willingness to embrace new services will be reduced.
At the University of Hull, the Faculty of Health and Social care recognised the lack of provision in this area and has worked to develop a range of modules and programmes. In September 2010 an introductory ‘Telehealth and Telecare’ module was launched. The success of this module has now led to the development of named programmes of study. These are offered to those with different academic backgrounds and aspirations: degree level programmes are open to all with experience of previous learning, whilst our Masters programmes require applicants to have a previous degree.
Telehealth and telecare use technology to overcome geographical and logistical challenges in care; our modules and programmes mirror this approach by using technology to remotely provide educational content. All the modules can be completed via e-learning or within a student’s own workplace. Our virtual learning environment allows presentations, supporting materials and suggested reading to be accessed online. The online work can be accessed at any time
that week to fit in with the individual’s work and personal commitments. Assessments vary throughout the programme (including essays, poster presentations and work-based projects) and vary according to the level of study. The modules can also be accessed as standalone modules if an individual doesn’t wish to complete a full programme of study.
The University Advanced Diploma in Telehealth or University Advanced Diploma in Telecare is at level 6 (degree level). The programmes include 3 modules over one academic year.
The Masters level programmes (level 7) follow a similar structure, though the expectations of students are higher. The aim of this programme is to provide students with an in-depth understanding of the principles and practice of telehealth or telecare. They will enable them to critically evaluate the evidence base for interventions, systematically analyse the ethical, legal and economic issues associated with these services, and allow them to justify adoption of this evidence-base in their own place of work.
At level 7 studies there will be an expectation of systematic thinking, initiative and use of change management strategies to promote widespread deployment of telehealth or telecare to enhance care provision.
The level 6 and level 7 modules have a number of shared modules, albeit delivered at different levels, covering slightly different content and with different assessment strategies.
Telehealth and Telecare (elearning) – This module provides an introduction to the benefits, challenges and operation of telehealth and telecare services. There is discussion of clinical, technological, financial
and political drivers for the development of telehealth and telecare. Students are asked to analyse the evidence base for telehealth and telecare services, drawing conclusions about the benefits to users and carers.
Telehealth or Telecare: Application in practice/Telecare: Application in practice (e-learning) – These modules allow students to discuss the concepts of telehealth or telecare in more detail. They address the services available for individuals and service providers, evaluating the different approaches to delivering/implementing telehealth or telecare. This helps students to understand and discuss some of the challenges associated with large-scale implementation and deployment of technology enhanced care nationally and internationally. At level 7 studies there is an expectation of systematic thinking, initiative and use of change management strategies to promote widespread deployment of telehealth or telecare to enhance care provision. The level 7 modules also address complex decision-making concepts and identification of strategies to overcome resistance to change.
Work based learning – This module asks students to apply knowledge of telehealth or telecare services to their own environment. The assessment includes the identification of problems that exist in practice and development of appropriate and innovative work based solutions to problems using critical evaluation of the literature.
The techniques used deliver the modules and programmes allow students to complete them without ever needing to attend the University of Hull in person, Students are provided with access to the University wide range online resources and individual support by an academic supervisor.
For employees of public-sector health and social care providers within Yorkshire and the Humber, the modules and programmes are fully-funded by the Local Education and Training Board. Costs for individuals elsewhere in the UK will vary depending on the modules and levels of study selected.
Joanne Hatfield Lecturer/Programme Leader in Technology Enhanced Care University of Hull
www.hull.ac.uk
Telehealth and Telecare (e-learning) (20 credits)One semester (12 weeks)
Work based learning (20 credits)2 semesters (24 weeks)
Telehealth: Application in practice (e-learning)
20 creditsOne semester (12 weeks)
Award University Advanced Diploma
in Telehealth
Telecare: Application in practice (e-learning)
20 creditsOne semester (12 weeks)
Award University Advanced Diploma
in Telecare
Telehealth and Telecare (e-learning) (20 credits)One semester (12 weeks)
Work based learning (20 credits)2 semesters (24 weeks)
Telehealth: Application in practice (e-learning)
20 creditsOne semester (12 weeks)
Award Post-Graduate Certificate
in Telehealth
Telecare: Application in practice (e-learning)
20 creditsOne semester (12 weeks)
Award Post-Graduate Certificate
in Telehealth
As the population continues to age, so will the prevalence of long-term conditions and reliance on health and social care providers.

Cross Keys Homes – Your cost-effective outsource solution for:
www.crosskeyshomes.co.uk/lifeline
• Telecaremonitoringservice
• Disasterrecovery
• Alarmresponse
• Out-of-hourscallhandling
• Anti-socialbehaviourreporting
• Domesticviolencereporting
• Loneworkermonitoring
• Telehealthmonitoring
• TelephoneStarsurvey
Support your customers 24-hours a day, 365 days a year!
To find out more or to see how we can help your business deliver excellent customer service call us: 01733 385101.
1879 - CKH - corporate lifeline ad A4_final (new TSA logo).indd 1 10/07/2013 11:42

thelink 17
A remarkable dog has been presented with a special retirement award by the lifeline telecare provider, Welbeing, in recognition of his long and faithful service to his epilepsy suffering owner, Kerrie Graham of Shawbirch, Telford.
Jara, a 15 year old Labrador/Collie cross, was trained nine years ago by the charity, Dog Aid, to help Kerrie whenever she has a seizure. As soon as one occurs he pulls an alarm cord in her flat that alerts the Welbeing Lifeline control centre who then send for assistance. As well as sounding the alarm Jara is trained to fetch Kerrie’s medication and to bring a special ball on a rope which he can use to help pull Kerrie upright as she comes out of a fit.
“He’s a remarkable dog and he even senses when I’m going to have a seizure before any detectable signs appear. He just comes and sits in front of me and stares at me and I know it’s about to happen,” explains Kerrie.
Forty year old Kerrie has suffered from epilepsy since her teens but was recently diagnosed with POTS Syndrome, a rare condition that was only discovered in the past few years. POTS Syndrome means Kerrie’s body can’t control her blood pressure resulting in dizziness, chronic fatigue and seizures, sometimes brought on by the simplest of movement.
“I’m extremely limited in what I can do physically but having Jara has helped me get out of the house. Two years ago my health deteriorated leaving me with more severe mobility problems but even in his old age Jara gives me confidence to go for short walks.
“I also have my Welbeing Lifeline alarm which I wear on me all the time around the house and garden. The service is so good. They don’t just provide an emergency response, they also encourage me to call them whenever I feel concerned about anything. It’s so reassuring
having someone at the end of the line no matter what the problem or the time is.”
Jara has also helped Kerrie indulge in her passion for art. “Having him gave me the confidence to go to a special art class in Telford. I love drawing and painting. I can’t describe how much it means to me to be able to do it. It’s such a release from my restricted life.”
Commenting on the award, John England, regional manager for Welbeing, said; “When we heard Jara was being retired we thought we should do something to recognise him for being such a great friend to Kerrie and a vital link with the service we offer.”
Sadly, at 15 years old, Jara is no longer able to provide Kerrie with the physical support she needs. However, she is too attached to him to replace him so he will end his days in retirement by her side.
www.welbeing.org.uk
Did you know that:a) 94% of UK adults have a mobile phone and
15% of them don’t have a landline at home.b) almost all telecare services rely solemnly on
one access (fixed or mobile) c) almost all telecare services only provide
emergency and location d) most people think telecare devices are
stigmatizing e) 87% of grown up children would like to be
involved in caring for their parents.
So why doesn’t Telecare:a) provide telecare with a Senior Mobile Phone?b) use backup and roaming SIMs?c) help with medication, health control,
daily tasks,...?d) use attractive and discrete devices?e) use a cooperative approach?
True-Kare is a new service that introduces a paradigm shift in the Telecare and Telehealth industry, because address simultaneously all of these issues and at same time ensure the quality and standards of telecare.
True-Kare service enables one person or an organisation to provide remote care to an elderly person, based on the communication between two central interfaces: a web self care portal (WSC) and a phone specifically developed for telecare.
With this service, True-Kare provides a possibility for telecare organisations to enlarge their customer base, to offer new services to their existing customer base and to upgrade the quality of the service that they are providing today to the elder population.
A care giver can manage the entire service in the WSC and the elderly will simply use the True-Kare senior mobile phone. The service was already made for easy integration with platforms, as it is with Novalarm UMO.
As most people resist using a specific device (like a GPS tracker), and only 13% of elderly people use a smartphone, True-Kare developed a care gateway inside a senior phone.
In order to guarantee the maximum uptime True-Kare phone uses has 2 SIM cards, one card, provided by True-Kare (in roaming with all networks available in the UK). True-Kare SIM supports all communications associated with the service, except voice calls and SMS that are made with customers’ normal SIM card.
The service allows for the following forms of remote support:•dailyactivities•medication•healthindicatorscontrol (Blood Pressure, Glucose, temperature andweight)•GPSlocationandsafetyarea(geofencing)•emergency•simplifyphoneusage
In addition, several other devices can be linked to the phone in order to provide more complete care. Currently, True-Kare has FOUR devices:
•SOSWatch•SOSKeychain•BloodPressureMeter•BTInterfaceforaGlucoseMeter(Lifescan UltraEasy)
Instead of adopting carephones and SOS pendants, that are stigmatizing, True-Kare uses the best of telecare technology inside of normal and attractive devices, like a mobile phone designed for senior people, an SOS Watch or an SOS Keychain.
Also, in order to allow for a user-friendly (and automatic) control of health indicators, True-Kare developed own brand Blood Pressure Meter and a Bluetooth interface to connect with J&J Lifescan glucose meter.
True-Kare believes that this service can change the shape of the UK telecare industry, as is already being evidential in France, Portugal, Netherlands, and Austria.
The World Summit Award, can give a push in the promotion of this revolutionary service to monitoring centres and distributors in the UK with a goal of creating strong partnerships and leveraging the unexplored potential of telehealth & telecare market.
www.true-kare.com
Cross Keys Homes – Your cost-effective outsource solution for:
www.crosskeyshomes.co.uk/lifeline
• Telecaremonitoringservice
• Disasterrecovery
• Alarmresponse
• Out-of-hourscallhandling
• Anti-socialbehaviourreporting
• Domesticviolencereporting
• Loneworkermonitoring
• Telehealthmonitoring
• TelephoneStarsurvey
Support your customers 24-hours a day, 365 days a year!
To find out more or to see how we can help your business deliver excellent customer service call us: 01733 385101.
1879 - CKH - corporate lifeline ad A4_final (new TSA logo).indd 1 10/07/2013 11:42
MEMBER NEWS
‘ALARM’ DOG JARA GIVEN WELBEING RETIREMENT AWARD
New benchmark for telecare services worldwideTrue-Kare wins UN world summit award in e-Health & Environment, raising the benchmark for telecare services worldwide.

thelink 18
Hospital DischargeSARH is also now able to offer free telecare services to hospital patients to allow them to return home much quicker.
The You First Telecare team has partnered with Stafford District General Hospital to launch a Hospital Discharge package, which will provide six weeks of free telecare and assistive technology support.
The service will help patients to recover safely in the comfort of their home and regain their independence after their stay in hospital, resulting in quicker discharges.
Assistive technology will help them settle back into their homes with the confidence that they have 24 hour support.
At the end of the six-week trial period the customer can decide whether they want to keep the service or not, if they decide not to then the telecare team will refer them to other support agencies as required.
Around two thirds of their telecare customers are referred from GPs, social workers and other professional agencies.
After consulting with health professionals at Stafford Hospital it was clear there was potential for telecare services to greatly benefit patients, wishing to recover at home but who were not sure what support they could access.
Karen Foster, Business Development Manager, said: “This new offer means that customers who might be hesitant about using the telecare service can experience it free of charge before making a decision. It allows the hospital to feel safe discharging the customer, knowing that they will have 24 hour support within their own home.”
Stacey Wain, Occupational Therapist with South Staffordshire and Shropshire Healthcare NHS Foundation Trust, said: “Through direct communication with the SARH You First Telecare Team, referrals for the provision of assistive technology within a patients’ home are straight forward and without fuss.
“I can always rely on the team’s expertise in assistive technology if I have any queries or challenging cases. The service provided directly benefits patients in our care in the hospital, enabling a safe and timely discharge process which, without this technology, may not be possible.”
www.sarh.co.uk
The scheme will provide training and support to care staff in residential homes and independent living schemes in Staffordshire – making sure staff know how to use equipment most effectively and are fully trained on new technologies as they are rolled out.
It is being piloted with two Staffordshire independent living schemes for customers with severe learning and physical disabilities.
The scheme will see their You First Telecare team’s expert staff, carry out monthly visits to ensure care professionals are confident and skilled in using the range of specialist assistive technology they provide, and undertaking maintenance checks for the equipment.
They will also assess whether the existing equipment is working for the customer and what other equipment could be introduced to support them.
The aim is to empower customers to live with greater independence and dignity by reducing the need for support from carers where assistive technology can be used effectively.
Karen Foster, Business Development Manager, said: “This new partnership scheme will improve customers’ quality of life, helping them to stay safe within their homes for longer but without necessarily needing carers around the clock.
“Provision of care is widely used as a first response to meet customers’ increased support needs, when assistive technology could provide a more efficient response, for example, in overnight monitoring. This is where assistive technology could offer customers greater control, dignity and independence in their care.
“Technology moves at such a fast pace that it can be hard for care staff to keep up and some of the equipment is very complex and specialised. Our team will make sure they are confident using all equipment to their maximum effectiveness.”
Reducing the need for round-the-clock carers will also have a positive impact on the cost to the customer and social services.
It currently costs Staffordshire County Council approximately £125,000 a year per customer to provide 24 hour care.
Reducing care provision from 24 hours to 10 hours a day and replacing with assistive technology could save up to £72,000 a year.
The new scheme offers many other benefits including reductions in ambulance call outs and hospital admissions, more timely hospital discharges, linked case management and care plan development and reduced call outs as a result of the regular training and maintenance visits.
Karen added: “As well as improving quality of life for customers the scheme has the potential to greatly reduce care costs for the local authority and customers directly, while Staffordshire County Council benefits from a localised service with an expert team.”
MEMBER NEWS
Training and Maintenance Service
Stafford and Rural Homes’ (SARH) You First Telecare team has partnered with Staffordshire County Council in a new scheme to maximise the effective use of assistive technology and increase independence for customers.
Stafford and Rural Homes’ (SARH) develop key partnerships to improve services across health and social care.

thelink 19
Background
In the last two years there has been a significant technology shift in Sweden – it was decided by the Swedish Government, through dialogue with the local authorities, that all analogue social alarms would be replaced with digital Carephones.
How did this come about?
The Government in collaboration with the National Board of Health and Welfare, issued guidance on social alarms and, the Swedish Post and Telecom Authority (PTS), the equivalent to Ofcom in the UK, made a survey and analysis of the Swedish social alarm market.
The Swedish Institute of Assistive Technology (SIAT) were commissioned by the Swedish Government to produce a report “Social alarms - new technologies for new infrastructures.” The purpose of this detailed report was “to carry out development and research to inform and support local authorities in improving security in their social alarm services, as a result of the technology shift to digital networks in telecommunications”.
The SIAT’s strong recommendation to local authorities was not to mix analogue and digital technologies and unfortunately, DTMF and STMF communication protocols were encountering problems operating on Sweden’s digital (NGN) networks. This applied to both hard wired devices and GSM devices connected via the mobile network.
With this advice, there was to be an enforced change from analogue to digital systems. The Swedish local authorities faced major challenges as there were over 200,000 analogue social alarms in individual homes needing to be replaced.
The Swedish local authorities commenced a nationally coordinated purchasing agreement of social alarms, communication and response centre services. Individual authorities received a better price and were provided
with a future proof technology with an open communication protocol so that they were not “locked” to a particular supplier, which was often the case with the traditional analogue systems. To date more than 20,000 analogue units have been replaced with many more scheduled for replacement in the near future.
The SIAT also developed an open protocol (SCAIP) for digital communication with the industry. The new common protocol is based on an open SIP based foundation and mirrors many of the characteristics of the NOWIP initiative in the UK.
The Benefits
Alarm calls between the user and the monitoring centre are instant, just like sending an email.
With a digital alarm, user safety and security is ensured because the social alarms send frequent control signals, ‘heartbeats’ every minute to the receiver. Traditional analogue social alarms simply can’t do this. A digital solution is always online and any breakdown of the communication link is instantly reported.
Upgrades of software can be enabled automatically and remotely without needing to visit the service user.
Conclusion
In the UK the same commercial drivers for more efficient and lower cost communication by the telecommunication companies will certainly result in similar issues regarding compatibility between analogue social alarms and digital networks.
As well as learning from Sweden’s experiences we should consider the implementation of a nationally coordinated programme to ensure that service users are not at risk and that future proof, secure technology is deployed.
CareTech is a Swedish based company that researches, develops and manufactures high-quality social alarms and Telecare, now available in the UK. The organisation was chosen by the Swedish Association of Local Authorities and the Swedish Institute of Assistive Technology (SIAT) to research, develop and manufacture the world’s first IP/digital Carephone and in 2009 released a revolutionary product called “CareIP®”. This was the world’s first Carephone designed to be used on a digital broadband service rather than an analogue phone line. Also available is a GSM option which can be fitted with a SIM card to provide an immediate, easily installed solution for people who no longer have a fixed phone line.
CareTech are now working with various UK service providers that have an IP/digital ready control centre and trials of our IP/digital Carephones are being carried out with great success.
www.caretech.se
The move to digital Carephones THE TECHNOLOGY SHIFT IN SWEDEN
Some of the Swedish local authorities using digital carephones
MEMBER NEWS
Sweden was the first European country to undergo a technology shift in the field of social alarms and Telecare services. This trend is now being followed with great interest by other European countries including the UK.

thelink 20
MEMBER NEWS
A walk through the freedom of technology.
To begin with Ruth moved into the organisation’s very sheltered housing development at Castlebrae Glebe, Edinburgh for a short time. Staff assessed her needs and capabilities whilst Ruth explored whether the options and choices offered by them were to her liking.
Staff wished to heighten Ruth’s self esteem and self worth. It was hoped that increasing contact with others would improve Ruth’s quality of life.
Ruth was introduced to a higher level of independent living when she moved in on a permanent basis. The housing support staff team at Castlebrae Glebe were available 24/7 and one to one support provided for Ruth 11 hours per week. Local authority homecare staff also called in regularly.
At all times Ruth could call Bield Response 24 (BR24) via pull cords or by pendant if she needed help or just wanted someone to talk to.
Ruth happily took part in different activities on offer and enjoyed life at Castlebrae Glebe, interaction with others was greatly increased improving her overall quality of life.
Ruth’s mental health worsened during 2008. Staff were concerned about Ruth’s late night excursions often involving police search and rescue. The monitoring organisation installed door exit monitors so that the local staff team could keep Ruth safe and at home with less or no police help.
In 2012 it was recognised that more than door exit monitors were needed. Following a multi-disciplinary care planning meeting, a GPS tracking device worn as a watch was given to Ruth. The device allowed Ruth to walk freely within a preset and safe area, only alerting the monitoring centre when Ruth walked out with the safe zone. This technology gave Ruth another year of independent living.
Ruth’s mental health worsened again in 2012 and this time proved harder to stabilise and she was taken to hospital to manage the decrease in her health. It was with a heavy heart the team decided a residential care place would be the long term plan to manage and ensure Ruth’s safety.
The organisaiton is proud to have helped to significantly improve the quality of Ruth’s life for nearly 7 years. This was possible through person centred assessment and care planning. A dedicated local staff team and the use of technology and inspirational ideas enhanced Ruth’s wellbeing and created much needed calm in an anxious life.
Bield launched its new strapline last year; “Free to Be”. Ruth’s story shows how the diverse use of technology and support puts people at the heart of what we do.
www.bield.co.uk
Bield first met Ruth in 2006 when she was 60 years old. At this time Ruth had been living in institutional care for around 10 years. Ruth lives with mental health problems and first came
into contact with psychiatric services when she was 37.
GATESHEAD Care Call
In time of stress, we can, often, hear people say,
‘Remember, we are but a simple phone call away.’
In reality however, there are few who mean it too.
The best of these outfits by far, are Gateshead’s Care Call Crew.
No matter what the time may be, whether it be day or night,
They’re always at the working end of the big red flashing light.
You can make a call, push a button, or, even pull a string.
No matter what, you know that very soon the phone will ring.
So, quite quickly, a soothing voice will bring to you its cheer,
As it calls to let you know that someone’s help is very near.
And when they come, you know, they will be there to being relief.
Once again to restore to you, a strong sense of belief/
Yet, even while displaying such a purposeful intent,
There will still be several customers who show some discontent.
Refusing to answer doors, because they want to stay in bed,
Or only listening to what they want to hear, instead of what was said.
While seeming happy to waste time and refusing to admit,
That they really need the company, even for a little bit.
They may criticise, berate and even say it does not matter,
But, you know that they’ll feel better, for a quick ten minute natter.
So, keep on doing what you do, may it last a lifetime long.
And, by the way, I have to say, we love the birthday song.
Mr Dennis Bell, Care Call Service User since October 2008
www.gateshead.gov.uk
thelink 21
NHS Ayrshire and Arran analysis shows that over 5 years the telehealth service could save 40% a sum of over £100,000.
I used to be really bad at taking my medication and quite often would end up very ill or even having to go into hospital, since I’ve had the equipment
I get a phone call from one of the girls and they tell me to start taking my antibiotics, I haven’t been in hospital since this started.
NHS Ayrshire and Arran have been improving the patient pathway for Chronic Obstructive Pulmonary Disease (COPD) with the use of telehealth self-management.
Evaluations have shown a 26% reduction in GP appointments, 70% reduction in emergency admissions to hospital and an 86% reduction in Ayrshire Doctors On Call (ADOC) contacts. Not only does this represent a reduced cost pressure to the local health service, but it also represents significant benefits to the patient.
Telehealth has also shown to stabilise patients’ health as their health professionals are able to easily monitor their condition daily. Another benefit has been the facilitation of a much closer working relationship between NHS Ayrshire and Arran and Local Authority staff in the joint management of COPD.
This has streamlined the pathway as awareness has been increased and duplications of assessments are likely to reduce.
One of the most significant benefits of this service is the
empowerment of patients to self-manage their condition, by helping them recognise their symptoms and giving them confidence to go about their daily lives. Medication adherence has also improved as they can see the correlation with their health.
Because we check the alerts daily, we have managed to contact a number of patients showing early signs of exacerbation of COPD and advised them to start their medicines in reserve. ”“
Clinician
Patient
“”

However, the issues and risks highlighted by these headlines don’t reflect the reality across the entire health and social care sector. Indeed there are areas where the outlook is much brighter. Clearly a polarised, two-tier and two-speed system now exists within the care home market for older people.
Within the publicly funded sector, care home operators have seen income being squeezed from two sides. Margins have been declining as local authorities baseline rates have been frozen or, at best, increased at below inflation rates, while food and energy costs have soared. At the same time, occupancy levels have fallen as local authorities shift the focus towards lower cost domiciliary care. The resulting falls in real income have created huge pressures for an already highly geared sector which is also having to adjust to greater regulatory scrutiny amid the public’s concerns over the quality of residents’ care. Independent operators in this sector have thus increasingly turned to “quasi” private pay residents (i.e. those paying “top-up” fees over and above what local authorities are prepared to pay) to subsidise the care of publicly funded residents. With many of the larger operators in this sector having already concluded their financial restructurings, it is therefore the smaller operators who are at most risk of the financial failure highlighted by Company Watch.
Accordingly, the last few years have seen the funding profile for the care of older people shifting towards private pay, a trend that is likely to continue for the foreseeable future. In 2012/13 the percentage of residents paying the full costs of long term care fees rose to 43.4% from 41% in the previous year. Accordingly, for operators in the private pay sector the outlook appears favourable,
despite the fact that they face some of the same operational challenges as their publicly funded counterparts. Private pay fee rates are rising steadily, generating strong revenue growth for those operators whose business model focuses on wealthier residents. Of course, the situation is not consistent across the country, with the proportion of private pay residents increasing most noticeably in the affluent south.
Demand for care home beds is expected to rise significantly in line with an ageing population, which alongside the widespread recognition that much of the existing care home stock is of poor quality creates a need for significant investment to fund the roll out of new care homes. Although bank funding (particularly development finance for new stock) remains difficult to access, capital is being introduced from other sources, such as the private equity sector, which remains an enthusiastic acquirer and funder of healthcare assets. In particular, there is a strong appetite for high quality, branded care home assets developed by the likes of Signature, Sunrise and Hallmark which have the look and feel of up-market hotels.
One interesting recent trend is the emergence of overseas investors, notably from the Far East and US, as active participants in the wider UK healthcare property sector. Malaysian Employees Provident, alongside various co-investors, acquired 12 Spire Healthcare Hospitals earlier this year through a sale and leaseback transaction. But it is US investors who have shown the greatest interest in the UK care home sector.
US real estate investment trusts (REITs) have been particularly active bidders for care home assets in recent times. For example, last year saw Health Care REIT, Inc acquire 5 Sunrise
thelink 22
Senior Living communities from Sunrise and Pramerica for £154 million which they then followed with the acquisition of a further 17 Sunrise communities from Morgan Stanley Real Estate Fund. Also last year, HCP, Inc made a significant investment in Four Seasons Health Care’s capital restructuring. The 3 top US healthcare REITs, who between them are valued at more than 10 times the aggregate size of the UK healthcare REIT market, own nearly 3,500 properties in the US and are now seeking to diversify away from their home territory and invest in overseas healthcare assets. With the UK population of over 65s expected to grow by over 60% by 2035 and the private pay UK care home market far less mature than in the US, the UK has understandably become a focus for US REITs’ interest.
Compared to the more restricted UK REIT regime, US REIT legislation allows US REITs to target a wider pool of healthcare real asset assets, which can include operational assets employing care home staff within their portfolio, as long as those staff are under the supervision of an independent care manager. This has resulted in the increased use of operational management contracts within the acquired real estate portfolios where the REIT appoints a specialist, branded operator to run the care home under a long term, institutional form of management agreement. This same model has been used successfully for many years in the hotel industry and its adoption looks likely to grow in the UK care home sector in the years ahead.
The entry of new investors into the sector, particularly from overseas, is already shaping innovation and helping fund improvements in the quality of accommodation and care, albeit currently at the premium end of the market where discerning consumers and their families assert their influence. There is naturally a sense of hope that this “raising of the bar” will have long-lasting impact beyond the private pay, affluent parts of the country and filter down into the rest of the care home sector.
Neil Matthews, PartnerField Fisher Waterhouse LLP
www.ffw.com
Care Home Sector
LEGAL SPEAK
No-one would deny that the care home sector has experienced a torrid few years. 2011 will probably be judged the low-point for the industry given the negative publicity surrounding the demise of Southern Cross, at that time the country’s largest independent operator, and shocking reports of residents being abused by staff at other homes. Two years on and hardly a day goes by without another alarming headline about the latest controversy in the care home sector. Recent examples include the revelation that over 1 million people have been forced to sell their family home in the past 5 years to pay for their care, and a separate research paper from Company Watch which revealed that one third of UK care homes are at “above average” risk of financial failure.

AstheDirectorofQualityandPerformance,Iwas responsible for the preparation of the audit.
The accreditation comes just eight months after Medvivo became accredited to the TSA Code for its Telecare service, at platinum level. As a newly formed organisation, (Wiltshire Medical Services acquired Telehealth Solutions earlier this year), we are very pleased that efforts to integrate our services have been so successful.
Audit preparation
As an organisation, we were very keen to become accredited to the Code, which is the first of its kind. We can now evidence that we are delivering person-centred assistive technology services of the highest standard.
Having only recently undertaken the Telecare audit, we were able to build upon this to demonstrate a truly integrated model of delivery.
There were a couple of areas which were initially a little difficult to interpret, but as always our Inspector, Christopher Waller and the TSA’s Marian Preece were on hand to provide support and advice.
The Day of the Audit
The audit was very similar to our previous experience, which took place over 2 days. The pre-audit was useful in helping us to clarify those areas that were a little ambiguous and to ensure we were fully prepared for part 2. Slightly, unbelievably, this was also thedaythattheCareQualityCommissionpaid an unannounced inspection; still it provided additional evidence for the Clinical Governance section!
The final audit took place at our premises in Watford, from which our telehealth clinical case management hub operates. This provided us with the opportunity to showcase our fully managed service and the benefits that deployment of telehealth can offer.
The TrustCall team are also still congratulating themselves after receiving their first TSA accreditation. The service was inspected in 2011 and after passing with flying colours, everyone involved in the success wanted to dedicate their time to gaining further accreditation in monitoring. Without wanting to dampen the spirits of the team, Fran Gudger, TrustCall Manager, also realised they would all need to be fully competent in providing the monitoring service, and further training and practice would be necessary to meet the high standards required by the TSA.
With this in mind, it was a conscious decision to keep the focus of the annual re-inspection in 2012 on four TSA modules; Referrals, Service Tailoring, Installation and Response. Despite the initial excitement to want to grow and gain more accreditations, the team were mindful that the monitoring accreditation was key to expand the business and help win future contracts as TrustCall wanted its reputation of
delivering the highest standards of telecare services, to be on everyone’s lips. TrustCall had recently started to provide CCTV monitoring as well as handling emergency out of hours repairs calls for Trafford Housing Trust, so this meant the team had already gone through a huge change, involving learning a number of new skills.
After a lot of hard work collating evidence, staff training, attention to detail regarding KPIs, and checking and re-checking their procedures, Fran and her team decided they were ready for a full inspection this year on all modules, including monitoring.
All of their exertion’s paid off when, after a two day inspection, TrustCall were informed that they had achieved the standards required for accreditation in all areas. They are now looking forward to another visit from the inspector and hope to attain European Standard status.
Managing Director of Independent Living, Rodger Cairns, commented how proud he was of his team for their continued
commitment to independent living and pride in the monitoring service they run,
“As the population becomes increasingly elderly, telecare is set to become ever more important, helping people to live independently for longer. Local authorities, housing associations and health organisations are increasingly turning to telecare to support ageing populations, other adults with support needs, and their carers. We’re thrilled to have been awarded this accreditation by the Telecare Services Association, which will help us in our ambition to grow our service”
TrustCall operate a 24-hour a day, 365 days per year service, with support tailored closely to an individual’s needs.
On 4th July 2011, TRAFFORD HOUSING TRUST opened its first in-house alarm monitoring centre, TrustCall. TrustCall has grown in strength and recognition since its birth 2 years ago, and was started after the local authority stopped operating its own alarm call handling service. The launch of TrustCall, which is supported by Trafford Housing Trust, saw a more interactive and bespoke service being offered than previously and a more holistic person-centred telecare service emerging. This proved a huge success for customers as well as satisfaction for the staff that handle alarm calls, as efficiency and customer service levels increased, which is very important when you have over 4,000 service users.
The TSA Integrated Code of Practice – Telehealth was awarded to Medvivo in August, the first organisation to achieve this standard. This demonstrates the drive and dedication of everyone at Medvivo to deliver high-quality, safe and effective solutions.
STANDARDS
thelink 23
What next?
As an organisation, we believe that the audit is simply the beginning of the journey. Full and continued compliance with the Code is important to us as a way of helping embed and sustain best working practices across the organisation. Every team member has had a role to play in this, and I’d like to say again well done to everyone for the hard work and dedication that won us this Integrated Code.
We are dedicated to providing integrated care to customers, enabling them to stay in the comfort of their own home and live as independently as possible. We strive to provide the highest quality of care through our integrated assistive technology solutions and look forward to many more years of successful collaboration with our partners in delivering these services.
Michelle Reader, Director of Quality and Performance
www.medvivo.com
www.traffordhousingtrust.co.uk

NOWIP PROGRESS
thelink 24
TSA helps to secure the inclusion of the IP Protocol in the CENELEC work programme
TSA is delighted to announce that the IP protocol work programme has been included in the Cenelec Standards Working Group – WG4 which is chaired by Chris Dodd from Tunstall.
Paul Shead, TSA Director, Supply Sector, stated ‘I think this is excellent news, and is exactly what we requested in our recent letter to the standards bodies. It means that the NOW IP protocol can be tabled along with any other relevant documents and protocols to enable the publication of a single European standard for the use of IP with telecare alarms and services. We now need to discuss with the NOW IP group about formally releasing this document for use in the development of this Standard’.
The journey so far:TSA sets the industry standards for the delivery of telecare and telehealth services through its Integrated Code of Practice which is externally inspected by a UKAS accredited inspection body. TSA has for many years also been involved in the delivery of standards for social alarms signalling protocols, resulting in the development of BS8521. The aim of this work was to provide a replacement to the BS 7369:1991 social alarm DTMF signalling protocol implementation employed by manufacturers within the social alarm market place to enable a solution toward meeting the requirements of the then market place. BS8521 – Specification for dual-tone multi-frequency (DTMF) signalling protocol for social alarms systems - was intended to ensure that Telecare users can benefit from improved equipment interoperability, irrespective as to the source of their equipment.
MARIAN PREECE, OPERATIONS MANAGER
The focus of the proposal is too narrow, as it intends to use the Social Care Alarm Internet Protocol (SCAIP) protocol as the foundation of the work. We have concerns that SCAIP does not reflect the needs of the European community and has only a regional focus. For example, SCAIP only facilitates IP communication involving dispersed alarms, not grouped systems. We understand that this is because Sweden only uses dispersed alarms, whereas the UK and other European countries use both dispersed alarms and grouped systems (also known as warden call systems). In the UK, nearly half of telecare users utilise grouped systems.
We propose that an alternative protocol called NOW IP is considered in the work plan, and we are in discussions with the NOW IP group to confirm that it will be made available for use. This has been established through the cooperation of the major telecare equipment manufacturers across the UK and Europe, and covers the requirements for both dispersed and grouped systems. There may also be other relevant IP standards to be investigated and considered.
I should be grateful If you would confirm that our comments have been posted to the appropriate people, including TC79/CLC/WG4.
Arrangements are in hand to call a meeting of the NOW IP Group to be held at the TSA Conference in November to discuss this issue and to discuss with the Group about formally releasing the NOWIP documentation for use by the Cenelec Technical Committee TC79/CLC/WG4 and to nominate experts to sit on the working group.
A calling notice for the NOW IP meeting has been issued for the next meeting of the NOW IP Group.
Marian Preece
Operations Manager
Following the finalization of BS8521 in 2009, TSA commenced work on the development of the NOW IP (Internet Protocol) for social alarms signalling. A great deal of work has been completed within this project and testing regimes for the NOW IP have also been carried out via the British Standards Institute (BSI) and a final push to complete the NOW IP (Internet Protocol) for use within the UK is now being planned.
TSA became aware in July 2013 of the possible creation of a new Technical Committee to develop a series of standardization deliverables setting out the technical and service requirements for each link in the service chain of social care alarms.
The proposition proposed a series of European standards that would cover the development of the links in the service chain of the social care alarms (both services and products). The standards would facilitate the procurement and delivery of services and products in the new technical environment in Europe.
TSA provided a robust response to the BSI, in the following vein:
TSA does not support the proposal as outlined in the Letter from CEN BT with the proposal from SIS for a new committee to cover Social chain for social care alarms as it currently stands:
We agree that there is a need for a published international standard for IP communications with telecare. We do not agree that a new committee or working group is required. There is already an established CENELEC Technical Committee TC79/CLC/WG4 which is responsible for drafting and maintaining the EN50134 Social alarm systems standards. This group is convened by Chris Dodd. The parts already published include product standards for social alarm systems, including Part 1: System Requirements; Part 2: Trigger devices. Part 3: Local Unit and Controller and Part 7: Application Guidelines for the delivery of the service, including the service chain as referred to in the proposal. We believe that Working Group 4 is the right home for this work item, and that the EN50134 document structure can accommodate a new part for IP communications.

thelink 25
Carephone Ltd Supply 1 t/a The Carephone16 Sheaf Street Daventry NN11 4ABStephen Westley, [email protected] 0800 849 9254Peter Simmonds RPI (Ind)4 Windsor RoadRadyr, Cardiff CF15 [email protected] 784629 SitexOrbis Limited FullLisa HamptonBeaufort House, Cricketfield RoadUxbridge,[email protected] 559 152
Close Circuit Security Services Limited AssociateMartin HulseStuart House, Valepits Road Garretts Green, BirminghamB33 0TD [email protected] 604 4499
Serco Group Plc FullJane Krzyzanowski9 Fodderty WayDingwall Business Park, DingwallRoss Shire IV15 [email protected] 366 933
Newcastle City Council AssociateColin WilliamsCivic Centre, Barras BridgeNewcastle Upon Tyne NE1 [email protected] 211 5286
Abbott Healthcare Products Limited Supply 1Mansbridge RoadWest EndSouthamptonHampshireSO18 [email protected] 467 083
Kirklees Council FullFlint Street, FartownHuddersfield HD1 [email protected] 414 788
John Burgess RPI (Ind)253 Tring Road, Aylesbury Buckinghamshire HP20 1PH [email protected] 155 076
Air Liquide (Homecare) Ltd FullAlpha House, Wassage WayDroitwich, WorcestershireWR9 0NX [email protected] 07970 234 328
KC Supply 237 Carr Lane, HullYorkshire HU1 [email protected] 817 424
Connected Health Full3B Boucher Business StudiosGlenmanchen Place, BelfastAntrimBT126QHTerence.brannigan@connected-health.co.uk02890 329 777
CAir (UK) Ltd Supply 1190 Hanson Lane, HalifaxWest Yorkshire HX1 [email protected]
Healthmatic Supply 1t/a H2EvidenceRedman Road, CalneWiltshire SN11 [email protected]
TesTime Limited Supply 1Suite 20 The Courtyard30 Worthing Road, HorshamWest Sussex RH12 [email protected]
Macmillan Cancer Support RPI (Cust Rep)89 Albert [email protected]
trueCall Ltd Supply 12 Old Palace Lane, RichmondSurrey TW9 [email protected]
New Members
Membership as at 30.09.2013Full Associate RPI Supply TOTAL
211 56 35 68 370
TSA NEWS
@TeleServAssoc
Join the conversation
www.telecare.org.uk
www.linkedin.com/company/2518630
MELANIE YOUNG
JENNA LYNCH
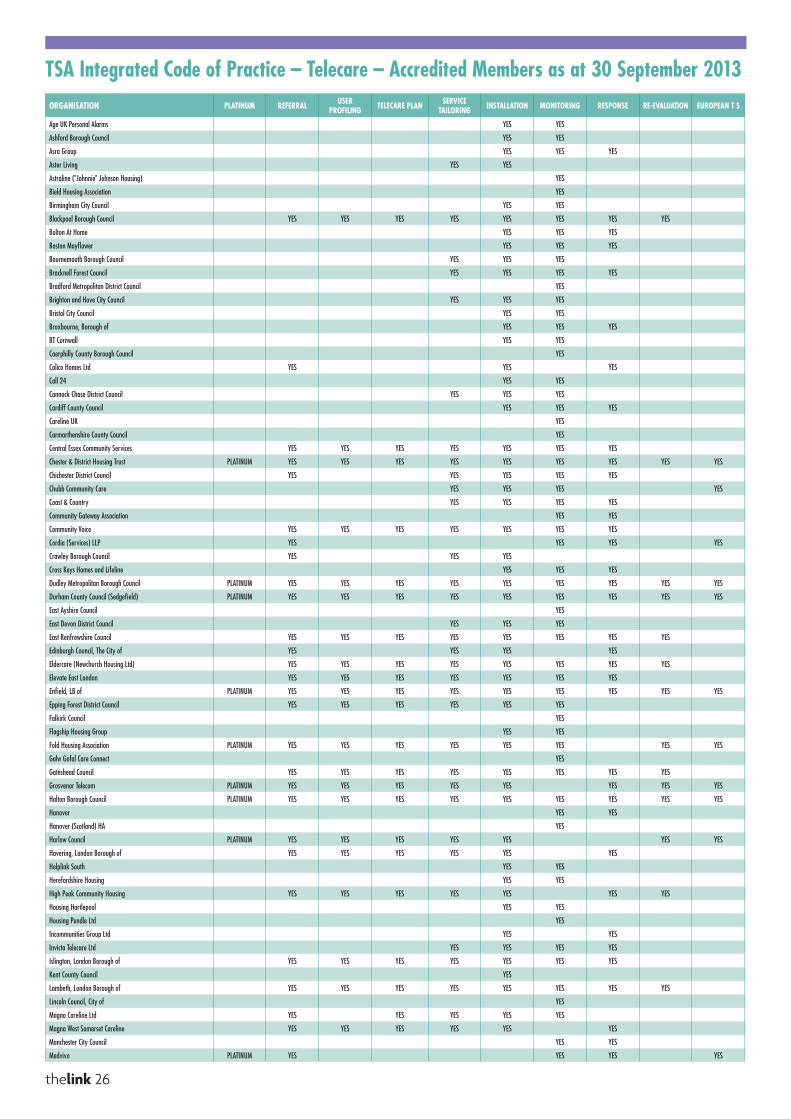
thelink 26
ORGANISATION PLATINUM REFERRAL USER PROFILING TELECARE PLAN SERVICE
TAILORING INSTALLATION MONITORING RESPONSE RE-EVALUATION EUROPEAN T S
Age UK Personal Alarms YES YES
Ashford Borough Council YES YES
Asra Group YES YES YES
Aster Living YES YES
Astraline ("Johnnie" Johnson Housing) YES
Bield Housing Association YES
Birmingham City Council YES YES
Blackpool Borough Council YES YES YES YES YES YES YES YES
Bolton At Home YES YES YES
Boston Mayflower YES YES YES
Bournemouth Borough Council YES YES YES
Bracknell Forest Council YES YES YES YES
Bradford Metropolitan District Council YES
Brighton and Hove City Council YES YES YES
Bristol City Council YES YES
Broxbourne, Borough of YES YES YES
BT Cornwall YES YES
Caerphilly County Borough Council YES
Calico Homes Ltd YES YES YES
Call 24 YES YES
Cannock Chase District Council YES YES YES
Cardiff County Council YES YES YES
Careline UK YES
Carmarthenshire County Council YES
Central Essex Community Services YES YES YES YES YES YES YES
Chester & District Housing Trust PLATINUM YES YES YES YES YES YES YES YES YES
Chichester District Council YES YES YES YES YES
Chubb Community Care YES YES YES YES
Coast & Country YES YES YES YES
Community Gateway Association YES YES
Community Voice YES YES YES YES YES YES YES
Cordia (Services) LLP YES YES YES YES
Crawley Borough Council YES YES YES
Cross Keys Homes and Lifeline YES YES YES
Dudley Metropolitan Borough Council PLATINUM YES YES YES YES YES YES YES YES YES
Durham County Council (Sedgefield) PLATINUM YES YES YES YES YES YES YES YES YES
East Ayshire Council YES
East Devon District Council YES YES YES
East Renfrewshire Council YES YES YES YES YES YES YES YES
Edinburgh Council, The City of YES YES YES YES
Eldercare (Newchurch Housing Ltd) YES YES YES YES YES YES YES YES
Elevate East London YES YES YES YES YES YES YES
Enfield, LB of PLATINUM YES YES YES YES YES YES YES YES YES
Epping Forest District Council YES YES YES YES YES YES
Falkirk Council YES
Flagship Housing Group YES YES
Fold Housing Association PLATINUM YES YES YES YES YES YES YES YES
Galw Gofal Care Connect YES
Gateshead Council YES YES YES YES YES YES YES YES
Grosvenor Telecom PLATINUM YES YES YES YES YES YES YES YES
Halton Borough Council PLATINUM YES YES YES YES YES YES YES YES YES
Hanover YES YES
Hanover (Scotland) HA YES
Harlow Council PLATINUM YES YES YES YES YES YES YES
Havering, London Borough of YES YES YES YES YES YES
Helplink South YES YES
Herefordshire Housing YES YES
High Peak Community Housing YES YES YES YES YES YES YES
Housing Hartlepool YES YES
Housing Pendle Ltd YES
Incommunities Group Ltd YES YES
Invicta Telecare Ltd YES YES YES YES
Islington, London Borough of YES YES YES YES YES YES YES
Kent County Council YES
Lambeth, London Borough of YES YES YES YES YES YES YES YES
Lincoln Council, City of YES
Magna Careline Ltd YES YES YES YES YES
Magna West Somerset Careline YES YES YES YES YES YES
Manchester City Council YES YES
Medvivo PLATINUM YES YES YES YES
TSA Integrated Code of Practice – Telecare – Accredited Members as at 30 September 2013
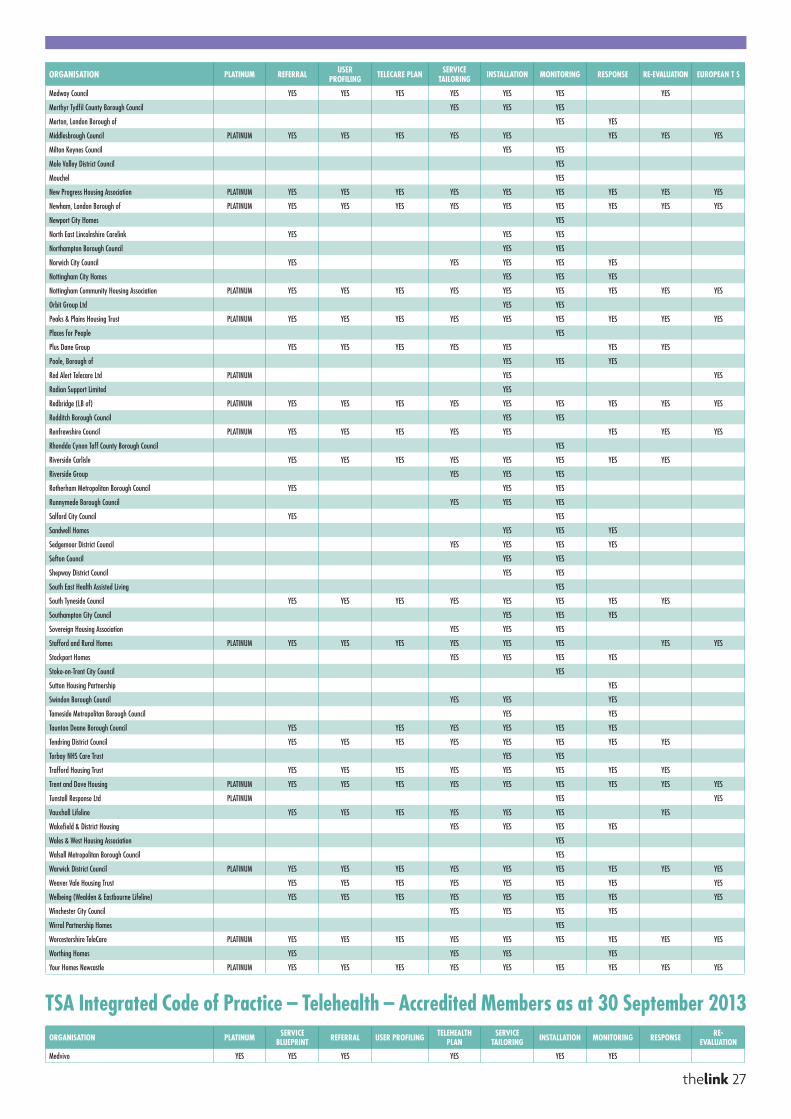
ORGANISATION PLATINUM REFERRAL USER PROFILING TELECARE PLAN SERVICE
TAILORING INSTALLATION MONITORING RESPONSE RE-EVALUATION EUROPEAN T S
Medway Council YES YES YES YES YES YES YES
Merthyr Tydfil County Borough Council YES YES YES
Merton, London Borough of YES YES
Middlesbrough Council PLATINUM YES YES YES YES YES YES YES YES
Milton Keynes Council YES YES
Mole Valley District Council YES
Mouchel YES
New Progress Housing Association PLATINUM YES YES YES YES YES YES YES YES YES
Newham, London Borough of PLATINUM YES YES YES YES YES YES YES YES YES
Newport City Homes YES
North East Lincolnshire Carelink YES YES YES
Northampton Borough Council YES YES
Norwich City Council YES YES YES YES YES
Nottingham City Homes YES YES YES
Nottingham Community Housing Association PLATINUM YES YES YES YES YES YES YES YES YES
Orbit Group Ltd YES YES
Peaks & Plains Housing Trust PLATINUM YES YES YES YES YES YES YES YES YES
Places for People YES
Plus Dane Group YES YES YES YES YES YES YES
Poole, Borough of YES YES YES
Red Alert Telecare Ltd PLATINUM YES YES
Radian Support Limited YES
Redbridge (LB of) PLATINUM YES YES YES YES YES YES YES YES YES
Redditch Borough Council YES YES
Renfrewshire Council PLATINUM YES YES YES YES YES YES YES YES
Rhondda Cynon Taff County Borough Council YES
Riverside Carlisle YES YES YES YES YES YES YES YES
Riverside Group YES YES YES
Rotherham Metropolitan Borough Council YES YES YES
Runnymede Borough Council YES YES YES
Salford City Council YES YES
Sandwell Homes YES YES YES
Sedgemoor District Council YES YES YES YES
Sefton Council YES YES
Shepway District Council YES YES
South East Health Assisted Living YES
South Tyneside Council YES YES YES YES YES YES YES YES
Southampton City Council YES YES YES
Sovereign Housing Association YES YES YES
Stafford and Rural Homes PLATINUM YES YES YES YES YES YES YES YES
Stockport Homes YES YES YES YES
Stoke-on-Trent City Council YES
Sutton Housing Partnership YES
Swindon Borough Council YES YES YES
Tameside Metropolitan Borough Council YES YES
Taunton Deane Borough Council YES YES YES YES YES YES
Tendring District Council YES YES YES YES YES YES YES YES
Torbay NHS Care Trust YES YES
Trafford Housing Trust YES YES YES YES YES YES YES YES
Trent and Dove Housing PLATINUM YES YES YES YES YES YES YES YES YES
Tunstall Response Ltd PLATINUM YES YES
Vauxhall Lifeline YES YES YES YES YES YES YES
Wakefield & District Housing YES YES YES YES
Wales & West Housing Association YES
Walsall Metropolitan Borough Council YES
Warwick District Council PLATINUM YES YES YES YES YES YES YES YES YES
Weaver Vale Housing Trust YES YES YES YES YES YES YES YES
Welbeing (Wealden & Eastbourne Lifeline) YES YES YES YES YES YES YES YES
Winchester City Council YES YES YES YES
Wirral Partnership Homes YES
Worcestershire TeleCare PLATINUM YES YES YES YES YES YES YES YES YES
Worthing Homes YES YES YES YES
Your Homes Newcastle PLATINUM YES YES YES YES YES YES YES YES YES
ORGANISATION PLATINUM SERVICE BLUEPRINT REFERRAL USER PROFILING TELEHEALTH
PLANSERVICE
TAILORING INSTALLATION MONITORING RESPONSE RE-EVALUATION
Medvivo YES YES YES YES YES YES
thelink 27
TSA Integrated Code of Practice – Telehealth – Accredited Members as at 30 September 2013
Described below are just some of the new telecare/telehealth features and services we shall be demonstrating:
Jontek limitedC A R I N G T H R O U G H I N N O V A T I O N
If you would like any further information, please visit our website:
www.jontek.com or Call: 0161 430 3366
Handle Calls Anytime Anywhere (HCAA)Provides more flexibility on how you manage your centre’s calls, for example to take into account a sudden surge in demand or perhaps staff sickness?
Allows staff to access the system from anywhere across your organisation or even for staff to handle calls safely and securely from home giving you the flexibility to virtually extend your monitoring centre.
Benefits include:
1. Flexible working for call centre staff and management.
2. Cost savings and working efficiencies.
3. Fully compatible with landlines, mobiles and desk phones
with extensions.
4. Promotes joined up working and sharing of data, for key
stakeholders based at various locations.
Asset ManagerProvides a flexible stock ordering system with full reporting capability to manage the ordering, receipt and distribution of stock.
Provides advance reporting for:
1. Minimum stock levels, with alerts when the threshold is reached.
2. Maintenance of stock, service dates, battery replacement etc.
3. A breakdown of equipment spend by, supplier, product etc.
DR ManagerMakes the task of transferring to/from your Disaster Recovery site much easier by allowing authorised users to automatically divert/transfer the phone lines between sites using the DR Manager utility.
Health and Social Care Integration Transformation NewsJontek are pleased to announce Answer-link 2013 has been further integrated with the Florence Telehealth System, providing the opportunity for much greater integration between Health and Social Care, in line with the aims and objectives of the Governments Health and Social Care Transformation Fund (ITF) which provides an opportunity to transform care so that people are provided with better integrated care and support.
FlorenceTM is part of the NHS ‘Simple Telehealth’ solutionSimple Telehealth is designed to enable many thousands of patients to take responsibility for the monitoring and management of their own condition or treatment.
Top 10 Change requests as voted by our customers The Top 10 most popular change requests as voted by all our customers on the Jontek member User Forum.
Revised TSA Code of Practice KPI Reports for 2013Update to the TSA Code of Practice Suite of Reports taking into account changes for 2012/13 including the 3 Million Lives report.
In line with our promise to all Jontek customers, this major software upgrade willbe provided free of charge, as part of our annual support and maintenance contract, protecting your investment for the future.
Answer-link 2013 Telecare and Telehealth Conference 2013Jontek are pleased to announce we shall be exhibiting at the forthcoming TSA conference in November where we shall be featuring some of the new features of our Annual Software upgrade for 2013.


















