THE YEW TREE PROJECT - Lewisham Council - Council...
31
THE YEW TREE PROJECT SUPPORT FOR CARERS OF THOSE AT THE END OF LIFE ANNUAL REPORT 2010-11 “I think it’s absolutely brilliant. It helped me personally to a huge extent. It’s a service run by human beings for human beings” YTP Carer
Transcript of THE YEW TREE PROJECT - Lewisham Council - Council...
THE YEW TREE PROJECT
SUPPORT FOR CARERS OF THOSE AT THE END OF LIFE
ANNUAL REPORT 2010-11
“I think it’s absolutely brilliant. It helped me personally to a huge
extent. It’s a service run by human beings for human beings”
YTP Carer
YEW TREE PROJECT ANNUAL REPORT
YEAR 1: JUNE 2010 – JUNE 2011
CONTENTS
PAGE
1 Executive summary 2
2 Service breakdown and commentary 4
3 Achievements and learning 9
4 Challenges 11
5 Case studies 14
6 Carer feedback 17
7 Bereavement support needs 21
8 Assessment of service model 23
9 Recommendations for future service provision 26
10 APPENDIX 1: Carer comments from feedback forms 28
11 APPENDIX 2: Informal carer comments 31
1. EXECUTIVE SUMMARY
After an initial planning phase, the Yew Tree Project (YTP) was launched in June 2010 under
direction of the South East London Marie Curie Delivering Choice Programme, with funding
from Pfizer and a brief to provide support to carers of those at the end of life (EOL). Referrals
were accepted of any carer over the age of 16 where either carer of cared for person was
registered with a GP in the borough of Lewisham. Additional funding was secured from NHS
Lewisham with a particular focus on providing advance care planning and Power of Attorney to
carers, in particular of those with dementia.
As a pilot project, funding was for a period of 12 months, but following a promising start both
MCDCP and NHS Lewisham offered extension funding to the end of the current financial year
(March 2012).
The project is based at Carers Lewisham (CL), part of the Princess Royal Trust for Carers
network of carers’ centres and well-established as the primary support for family and informal
carers in the borough. YTP offers specialised support drawing on and extending services
provided by CL and in its breadth and focus not duplicated by any other local agency.
Service impact was monitored from the outset, with feedback from carers supported indicating
positive improvements in every area evaluated, ranging from a 4% increase in carers’ attention
to their own health to a 28% increase in confidence in sources of help and information (see
table 5.3.4 below). Practical and emotional support was offered as anticipated and additional
needs identified, in particular around and following the period of bereavement. Feedback from
carers was overwhelmingly positive. Shortfalls in local service provision for EOL carers were
also identified and proposals made to address these.
The situation of those who devote often very substantial resources in the form of time and
finances to caring for partners, relatives and friends is only slowly being recognised but has
major implications for resource planning. With a recent report finding that investment of less
than £5m in Princess Royal Trust Carers’ Centres holistic carers support yielded an estimated
social return of at least £73m a year,1 there are strong financial incentives for supporting
projects of this kind. While all carers are liable to suffer poor health, increased stress, social
1 Carers’ Centres: What impact do they have? Baker Tilly / PRTC, 2011

isolation and financial disadvantage, the emotional impact is inevitably higher when the person
being cared for is a loved one passing through a terminal illness. The Yew Tree Project shows
that cost-effective support can be successfully targeted to this group with demonstrable effect
on their overall wellbeing.
2. SERVICE BREAKDOWN AND COMMENTARY
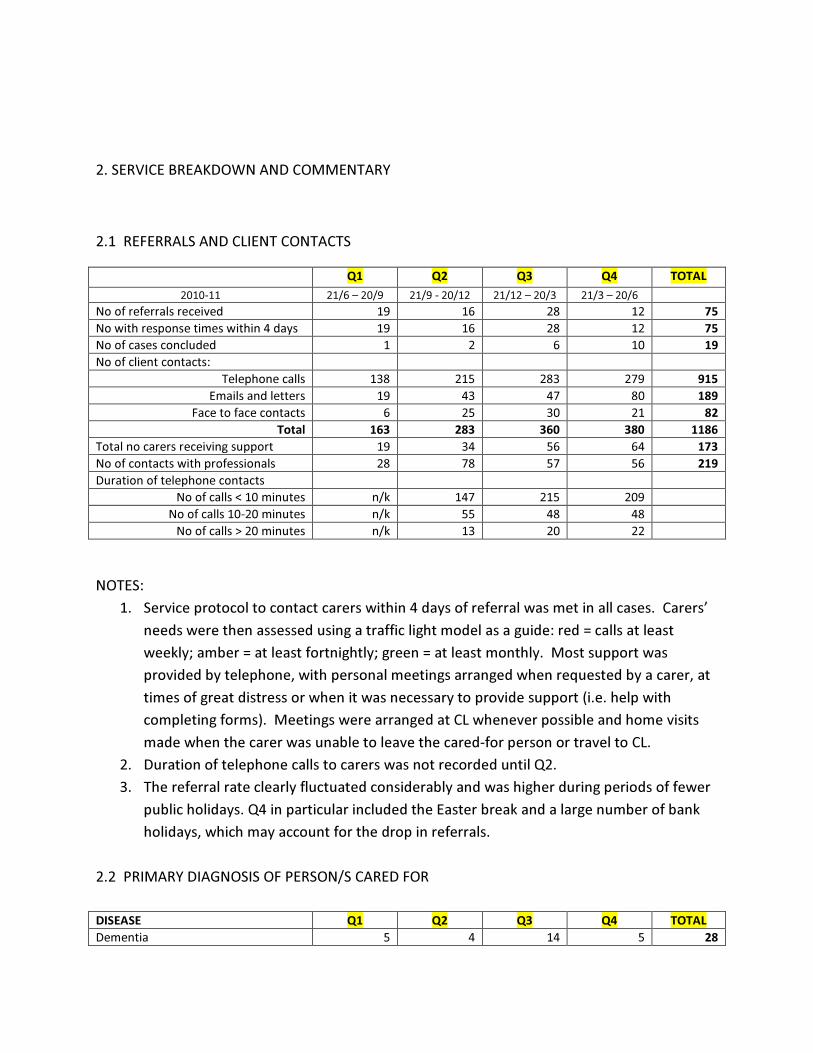
2.1 REFERRALS AND CLIENT CONTACTS
Q1 Q2 Q3 Q4 TOTAL
2010-11 21/6 – 20/9 21/9 - 20/12 21/12 – 20/3 21/3 – 20/6
No of referrals received 19 16 28 12 75
No with response times within 4 days 19 16 28 12 75
No of cases concluded 1 2 6 10 19
No of client contacts:
Telephone calls 138 215 283 279 915
Emails and letters 19 43 47 80 189
Face to face contacts 6 25 30 21 82
Total 163 283 360 380 1186
Total no carers receiving support 19 34 56 64 173
No of contacts with professionals 28 78 57 56 219
Duration of telephone contacts
No of calls < 10 minutes n/k 147 215 209
No of calls 10-20 minutes n/k 55 48 48
No of calls > 20 minutes n/k 13 20 22
NOTES:
1. Service protocol to contact carers within 4 days of referral was met in all cases. Carers’
needs were then assessed using a traffic light model as a guide: red = calls at least
weekly; amber = at least fortnightly; green = at least monthly. Most support was
provided by telephone, with personal meetings arranged when requested by a carer, at
times of great distress or when it was necessary to provide support (i.e. help with
completing forms). Meetings were arranged at CL whenever possible and home visits
made when the carer was unable to leave the cared-for person or travel to CL.
2. Duration of telephone calls to carers was not recorded until Q2.
3. The referral rate clearly fluctuated considerably and was higher during periods of fewer
public holidays. Q4 in particular included the Easter break and a large number of bank
holidays, which may account for the drop in referrals.
2.2 PRIMARY DIAGNOSIS OF PERSON/S CARED FOR
DISEASE Q1 Q2 Q3 Q4 TOTAL
Dementia 5 4 14 5 28
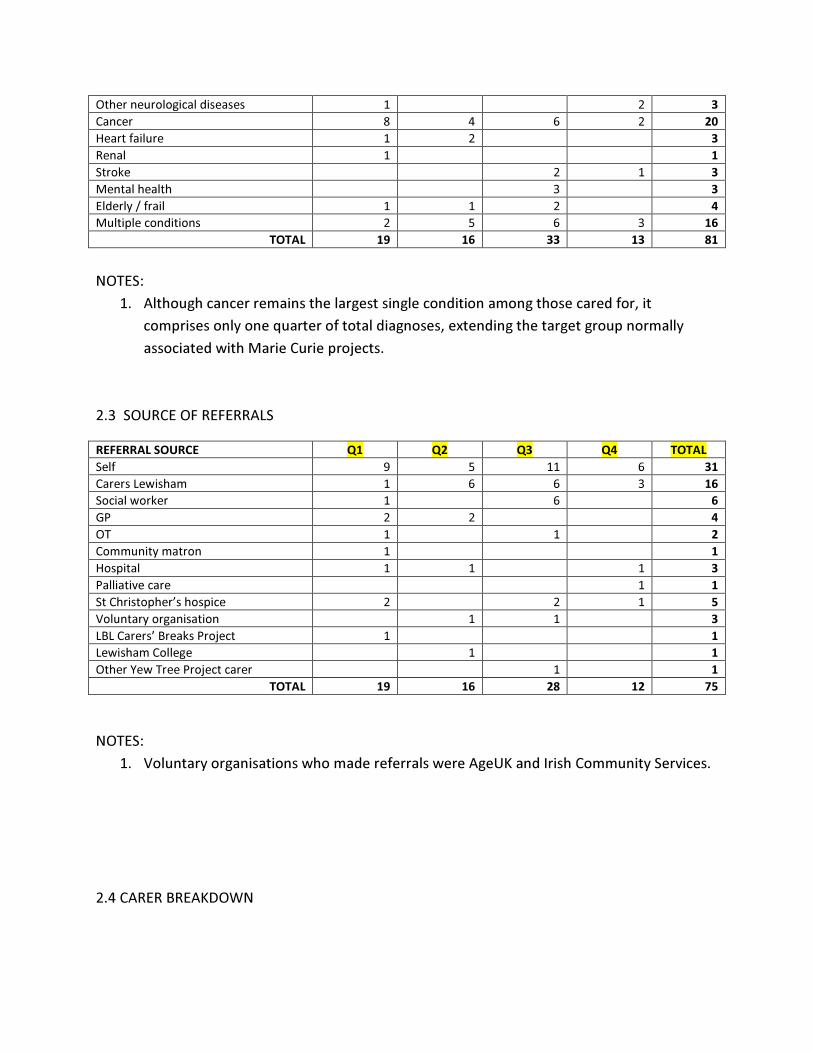
Other neurological diseases 1 2 3
Cancer 8 4 6 2 20
Heart failure 1 2 3
Renal 1 1
Stroke 2 1 3
Mental health 3 3
Elderly / frail 1 1 2 4
Multiple conditions 2 5 6 3 16
TOTAL 19 16 33 13 81
NOTES:
1. Although cancer remains the largest single condition among those cared for, it
comprises only one quarter of total diagnoses, extending the target group normally
associated with Marie Curie projects.
2.3 SOURCE OF REFERRALS
REFERRAL SOURCE Q1 Q2 Q3 Q4 TOTAL
Self 9 5 11 6 31
Carers Lewisham 1 6 6 3 16
Social worker 1 6 6
GP 2 2 4
OT 1 1 2
Community matron 1 1
Hospital 1 1 1 3
Palliative care 1 1
St Christopher’s hospice 2 2 1 5
Voluntary organisation 1 1 3
LBL Carers’ Breaks Project 1 1
Lewisham College 1 1
Other Yew Tree Project carer 1 1
TOTAL 19 16 28 12 75
NOTES:
1. Voluntary organisations who made referrals were AgeUK and Irish Community Services.
2.4 CARER BREAKDOWN
Of the 75 carers supported in the first year of the project, 57 (76%) were female and 18 (24%)
male. Carers self-identified ethnically as follows:
White
British
White
Other
Black
British
Black
Caribbean
Black
African
Asian
British
Asian Other
Female 37 4 2 6 3 1 1 3
Male 13 0 1 1 1 1 0 1
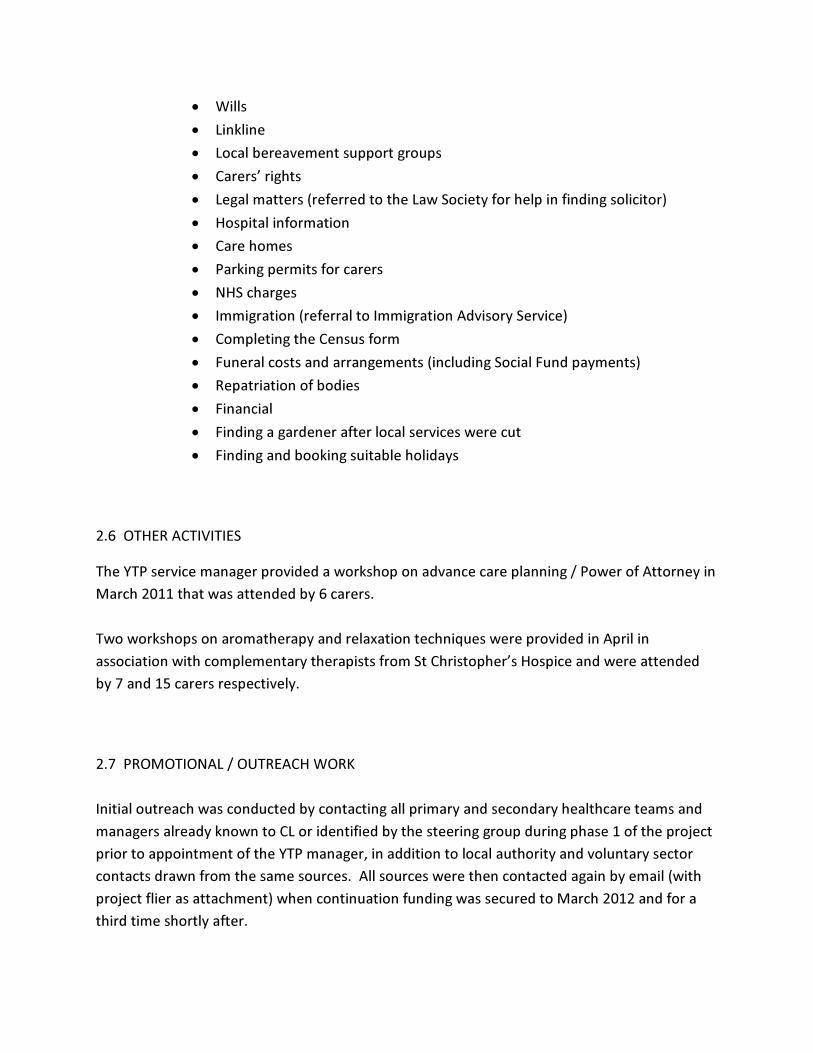
2.5 SUPPORT PROVIDED TO CARERS
SUPPORT Q1 Q2 Q3 Q4 TOTAL
Emotional support 19 34 55 60 168
Assistance/support with benefit claims 4 6 6 7 23
Form filling 2 2 1 3 8
Assistance with ACP/Power of Attorney 14 4 15 6 39
Registration with CL respite service 9 4 10 5 28
Request for counselling 5 4 7 6 22
Referral to other CL services 11 4 21 36
Provision of EOL information 8 5 9 3 25
Needs assessment/ Soc Services referral 5 8 11 11 35
Bereavement support 3 11 13 10 37
Liaising with hospital/ hospice 1 1 2
Advocacy 1 5 3 3 12
Signposting 3 2 2 3 10
Referral to palliative care/ MC night nurses 2 1 3
General information 8 5 16 17 46
TOTAL 92 93 154 156 495
NOTES:
1. Emotional support has emerged as the core of the service. For a note on issues
encountered here, see 3.1 MONITORING.
2. Most counselling referrals were received internally by CL, with bereaved carers who
had not already commenced counselling at CL being referred to Lewisham
Bereavement Counselling Service.
3. Other CL services carers were referred to include specialist support groups for
challenging behaviour, dementia carers or to develop coping strategies; coffee
mornings and social events; help in getting back to work and the Fix Yourself A Break
scheme to provide holidays for carer and cared for person. As all carers were sent
regular newsletters listing all CL events, it is likely that some attended other events
outside the Yew Tree Project.
4. For comments on bereavement support, see Part 6.
5. General information was requested and provided in areas including:
• Wills
• Linkline
• Local bereavement support groups
• Carers’ rights
• Legal matters (referred to the Law Society for help in finding solicitor)
• Hospital information
• Care homes
• Parking permits for carers
• NHS charges
• Immigration (referral to Immigration Advisory Service)
• Completing the Census form
• Funeral costs and arrangements (including Social Fund payments)
• Repatriation of bodies
• Financial
• Finding a gardener after local services were cut
• Finding and booking suitable holidays
2.6 OTHER ACTIVITIES
The YTP service manager provided a workshop on advance care planning / Power of Attorney in
March 2011 that was attended by 6 carers.
Two workshops on aromatherapy and relaxation techniques were provided in April in
association with complementary therapists from St Christopher’s Hospice and were attended
by 7 and 15 carers respectively.
2.7 PROMOTIONAL / OUTREACH WORK
Initial outreach was conducted by contacting all primary and secondary healthcare teams and
managers already known to CL or identified by the steering group during phase 1 of the project
prior to appointment of the YTP manager, in addition to local authority and voluntary sector
contacts drawn from the same sources. All sources were then contacted again by email (with
project flier as attachment) when continuation funding was secured to March 2012 and for a
third time shortly after.
In the first year of the project, written notices were provided for Lewisham LINk eBulletin (3
issues), Inside Palliative Care (journal of the National Council for Palliative Care), Grapevine
(Voluntary Action Lewisham newsletter), Lewisham Social Workers Bulletin and the Marie Curie
Delivering Choice Programme newsletter.
The service manager also gave presentations to GPs at the EOL Local Enhanced Service launch,
the Pensioners Forum, clinical staff at South Lewisham Group Practice, Lewisham District Nurse
forum and Lewisham GP Forum (themed meeting on carers), plus met with palliative care
teams at St Christopher’s, Lewisham and Guy’s Hospitals, South London and Maudsley Trust
Mental Health of Older Adults team, the Alzheimer’s Society, Seniors, a local GP surgery
practice manager (by request) and NHS Lewisham Carers Support and Development Officers
and EOL Service Improvement Facilitator.
He also attended meetings of the EOL Stakeholders Group, Carers Partnership Board and LBL
Carers Working Group and did outreach work at LBL Pensioners’ Day, as well as attending
training in benefits and support of older people at Carers UK and EOL care and dementia at St
Christopher’s.
3. ACHIEVEMENTS AND LEARNING
Table 6.3.4 below summarises the effects of the project on carers’ ability to continue in a caring
role, as stated by the carers themselves. There was an improvement in every one of the 5
categories measured. Carers’ attention to their own health rose by 4.0%; confidence in being
able to carry on caring rose by 12.5%; overall ability to cope with caring increased by 18.6%; the
feeling of being supported as a carer rose by 26.4%; and carers’ confidence in knowing where to
go for help and information rose by 28.0%. There is clear evidence from this and from carers’
feedback (see also Appendix 1 and 2) that the project was successful in enabling informal carers
to continue in their caring role, with improved wellbeing for carers matched by financial savings
to healthcare and support agencies.
Other achievements/ learnings include:
• All carers referred to YTP were contacted within 4 working days, providing fast as well as
flexible support.
• As a cross-agency project, YTP effectively increased links between disparate healthcare
and other agencies, providing a focus on the needs of EOL carers and drawing referrals
from a broad range of sources. It is hoped that the relationships that developed

through the project will outlast it and have a continuing effect on providing a more
holistic service delivery locally.
• While support can be delivered effectively through a telephone-based project, some
home visits were necessary alongside appointments arranged at CL. Face-to-face
meetings increase carers’ confidence in the support provider and tended to produce
more positive feedback overall.
• Repeated outreach and promotional work is needed to maintain referrals from external
agencies, possibly as a result of staff turnover but also because where carer awareness
is not well-established the attention given to carers will be less and the referral rate will
drop at busy times, holiday periods or other times of staff shortage. This is a challenge
faced by all carer support organisations but has particular relevance in the present case
in such areas as building closer ties between EOL carer support and the Gold Service
Framework (GSF).
See also 9 Recommendations for future service provision.
4. CHALLENGES
4.1 MONITORING
As with any project of this nature, monitoring will become imprecise where service filters down
into minor acts of support and encouragement which are harder to log than a clearly defined
act such as contacting a social worker to request a care plan review. The main issue is around
the nature of emotional support, which has emerged as the principal service offered.
All carers – and in particular carers of those at EOL or with dementia who may already be
experiencing anticipatory grieving – are likely to appreciate a friendly call showing interest in
their situation and possibly offering practical assistance. However, the provision of practical
support in itself very often has emotional impact. Informing a carer of someone with dementia
that their immediate financial difficulties can be addressed by arranging a lasting power of
attorney, or providing a sitting service so that a carer can have a free afternoon to attend to
personal affairs, for example, are strictly speaking practical interventions but will have great
emotional impact on the carer, providing reassurance and helping reduce stress. Most carers
indicated most of the time they were pleased, relieved or thankful to receive telephone calls
and those feeling particularly stressed appeared less so at the end of calls, which is why
providing emotional support appears as the single largest form of support in table 2.4.
4.2 OUTREACH AND REFERRALS
See 2.6 for outreach and promotional work undertaken and 2.3 for referral sources.
Referrals from Social Services fluctuated greatly and were highest after additional promotional
work by Natasha Dunbar at LB Lewisham (i.e. reminder emails sent “in house” along with
display of posters), although the peak was not sustained. Experience at CL and another carers
centre suggests that referrals from all organisations to non-statutory bodies tend to be
considered low priority and drop at times of staff shortage, holiday periods etc.
Referrals from GPs and primary care sources overall were disappointingly low. All surgeries
were notified / reminded of the project several times during the year and all had previously
been sent promotional material by CL requesting attention to carers’ needs. It would appear
that many patients identified on the GSF register will have carers who were not identified for
referral by GPs. More work remains to be done in this area.
Some referrals from healthcare sources were made at a late stage in the patients’ lives (several
deaths occurred within a week of referral), minimising the support that could be offered. There
is some evidence that doctors are reluctant or unable to make accurate EOL prognoses2, yet
earlier referral would clearly help optimise service provision. It must also be recognised,
however, that not all patients are willing to ask for or hear such a prognosis and some who do
will then not share information in order to protect their carers, leading to an information lag
that will affect what support can then be offered to carers.
4.3 PROJECT DELIVERY
Some carers with intensive caring responsibilities find it hard to come to CL for appointments,
yet time constraints minimised the number of home visits that could be offered. Support levels
per carer increased as time and workload allowed, but personal contacts with carers often
revealed support needs that carers were less likely to offer over the telephone, leading to
2 “A study led by the Harvard researcher Nicholas Christakis asked the doctors of almost five
hundred terminally ill patients to estimate how long they thought their patient would survive,
and then followed the patients. Sixty-three per cent of doctors overestimated survival time.
Just seventeen per cent underestimated it. The average estimate was five hundred and thirty
per cent too high. And, the better the doctors knew their patients, the more likely they were to
err.” – Atul Gawande, “Letting go: What should medicine do when it can’t save your life?”, New
York Times, 2 August 2010.

greater or more nuanced support being provided. The implication is that the greater the face-
to-face contact with carers, the more carers feel able to confide and the broader the range of
needs that can be addressed.
4.4 LOCAL SERVICE SHORTFALLS
Several shortfalls in overall service provision to EOL carers in Lewisham were identified through
the project:
4.4.1 Counselling. Many carers of loved ones at the end of life are naturally highly
distressed around the time of death and would benefit from the opportunity for
short-term counselling. The value of this is recognised by hospitals and hospices
commonly offering bereavement support to the families of patients, while the need
is arguably greater where the bereaved have also been in an emotionally and
practically demanding caring situation that may have been the major feature of their
lives for some considerable time. Many carers supported by YTP were provided
counselling by CL, but others were unable to consider their personal needs until too
late and then missed out on counselling because for funding reasons CL is unable to
provide this service to former (bereaved) carers. Such carers were signposted to
Lewisham Bereavement Counselling Service but often reported a long wait before
counselling began, meaning the only counselling-type support they received at the
time of greatest needs was from the YTP service manager. It would be greatly
beneficial to carers if an interim service were made available; see Recommendations
in part 8.
4.4.2 Childcare. One carer of her husband with cancer, both around 40 years old, had
three young children only one of whom had started at nursery. They experienced
great difficulties whenever the husband attended his fairly frequent hospital
appointments, when his wife needed to accompany him but the children were not
advised to go with her. Neither the Children and Family nor Young Adults teams of
Lewisham Social Services, nor an agency carrying out contract work for LBL who it
was suggested could help (as it turned out, incorrectly), nor SureStart were able to
provide emergency childcare to cover hospital appointments, and no other
voluntary or other agency was identified. It remains unclear if this is an endemic
problem or whether solutions have been reached by other local authorities.
5. CASE STUDIES

These vignettes are included to give a clearer idea of the kind of support provided by the Yew
Tree Project. Some details (including names) have been changed to protect anonymity, but all
are taken from actual cases.
5.1 FINANCIAL WORRIES – ALICIA
Alicia is a Latin American woman in her 70s who speaks English as her second language but can
have difficulty understanding some things – especially official documents. She had been
registered as a carer with CL for some time when her husband, already ill with cancer, took a
downturn and was admitted to hospital. At this point Alicia was referred to YTP, with the first
need being to help notify the Disability and Carers Service of the hospitalisation to protect
against benefit overpayments. Alicia was aware that her husband was nearing the end of life,
asked for information about this and was able to discuss her own and his needs. When her
husband died without being discharged, Alicia suffered great anxiety and panic attacks, for
which she received emotional support and a counselling referral. She had a lot of difficulty in
sorting out the couple’s financial affairs, reclaiming benefits in her own name, sorting out her
late husband’s pension, dealing with rent arrears and applying for a tenancy transfer to her own
name. The YTP manager assisted her with home visits to complete forms and deal with
paperwork, helped with a Social Fund application to cover funeral costs while the benefits were
being reassessed and eventually referred her to a specialist financial adviser to advise on
longer-term planning. After also arranging for a translation and personal help with the Census
form, Alicia was able to get through the difficult period following her husband’s death, feeling
more relaxed and able to take charge of the household finances which her husband had always
seen to.
5.2 CHANGES IN THE FAMILY – TOM, MARGARET AND PENNY
Tom was registered at CL as a carer for his wife Margaret, who suffers from rheumatoid
arthritis. But when Tom was unexpectedly diagnosed with a terminal illness and given only a
short time to live, the family had to make major adjustments very quickly. Margaret, with
limited mobility herself and feeling shocked, was able to visit Tom in hospital when their adult
daughter Penny came to drive her, but Penny lived a long distance away outside London and
was under pressure herself as a working single mum. Penny registered as a carer too, and first
of all Social Services were notified of the change in the family’s circumstances and Margaret’s
increased needs now Tom wasn’t able to support her. Penny needed to assess the financial
implications of reducing her work hours in order to spend more time in London with her
parents, which was done by assessing her benefit entitlements. She also requested counselling
near her home and the family obtained a Linkline alarm for Margaret. Practical concerns like
finding a gardener were dealt with, and both women were given emotional support during
Tom’s final illness. After Tom died, Penny dropped round to discuss practical arrangements
(registering the death, arranging the funeral) and was also given information to support her
teenage daughter in her own grieving for her grandfather. As the family readjusted to deal with
Tom’s loss, YTP ensured that Margaret’s care plan was reviewed and upgraded so Penny could
return to work and caring for her children.
5.3 COMPLEX NEEDS – KIRSTY
Kirsty was referred to YTP by a District Nurse who was concerned about the high level of needs
of Kirsty and her family. Kirsty, in her 20s, was caring for an elderly grandmother with a
degenerative disease; Kirsty’s mother was caring for a son with multiple disabilities as well as
looking after Kirsty’s young daughter, and Kirsty was also supporting an elderly and frail aunt
who lived nearby. Like most of the family, Kirsty suffered from both a physical condition and
learning disabilities which when added to bad experiences at the hands of “the authorities”
made them wary of outside agencies and intent on looking after themselves as much as they
could.
At the time of referral, however, Kirsty needed help. She found it hard to understand and deal
with official letters, and so was facing a large bill for care visits which the family were unable to
pay. The YTP manager liaised with LBL’s head of financial assessment who clarified that charges
had been made because proof of Kirsty’s grandmother’s financial situation had not been
provided, and then met with Kirsty to go through her papers and find what was needed. This
also began a long process of earning Kirsty’s trust so further support could be offered, which
included contacting Social Services for a needs reassessment, beginning to arrange a school
place for Kirsty’s daughter, discussing advance care planning needs and the option of applying
for power of attorney, identifying and then working closely with the palliative care team
involved in the grandmother’s care, registering with CL’s occasional respite sitting service,
negotiating with a debt collection agency, finding ways for Kirsty to open a bank account
without a passport or driving licence (advice obtained from the director of the British Banking
Association), making a special application for a tenancy transfer and helping with ongoing
benefit concerns. It became clear that Kirsty and her family were sensitive to what they felt to
be shortfalls in service provision but sometimes also reluctant to accept outside support: a
place was found for Kirsty on a Think Families course which would mentor and guide her into
gaining skills and employment, but she couldn’t take this up in the end because of uncertainties
in the family and her grandmother’s reluctance at the time to accept home visits from
careworkers. Attempts to encourage Kirsty to attend a drop-in group near her home provided
by CL were unsuccessful, but as her grandmother’s health visibly deteriorated Kirsty was able to

begin to overcome the family’s reluctance to face the inevitable and for the first time began
considering how to ensure her grandmother was buried in the family plot with her late husband
and what she should do about funeral arrangements. Her anxieties could still make her
suspicious of outsiders, but in YTP she was often ready to trust and at times actively turn to an
outside agency for help.
5.4 RAHUL – MAKING PLANS
Rahul’s wife has a mental health condition which is normally stable on medication but which
sometimes means she stops being Rahul’s co-carer for her mother, who lives with them and has
dementia, and needs Rahul’s support herself. To further complicate matters, their adult
daughter, already in sheltered housing for mental illness of her own, has now been diagnosed
with a kidney condition that requires regular hospital appointments.
Rahul’s needs included talking through the needs of the family as a whole, working out how
they were going to support themselves and what contingency plans they needed to cover
various possible situations. Rahul himself contacted Social Services to request a care plan
review after being given the number and advised of his right to a carer’s assessment. After
attending a workshop given on the subject by the YTP manager, he also decided to apply for a
Lasting Power of Attorney for his mother-in-law, and also explored his own rights in respect to
Carers Allowance so he could continue doing occasional work without losing his benefits. He
was doubtful about using CL’s sitting service because his mother-in-law preferred being cared
for by the family, but a way was found around this and he gained some badly needed free time
for himself. He and his wife had difficulties visiting their daughter while she recuperated
because the daughter lived in a parking restricted area, but a solution was found in applying for
a carer parking permit and the family was able to remain self-sufficient.
6. CARER FEEDBACK
6.1 MONITORING PROCESS
As part of an ongoing monitoring process, feedback was collected in the following forms from
carers who received support from YTP:
1. Carers Feedback Questionnaire 1 [CFQ1] was sent within a month or so of initial contact
asking carers to assess how well they had managed in 5 areas before receiving support.
The 5 areas related to the carer’s ability to cope with caring, ability to take care of their
own health, feeling of being supported as a carer, ability to carry on caring and
knowledge of where to seek help and information. These categories are those used by
CL, so statistics are compatible with overall carer support. The CFQ1 form also included
an open invitation for any additional comment the carer wished to make.
2. To enable an impact evaluation of the project, supported carers were asked to complete
a similar form [CFQ2] asking their responses to the same 5 questions after receiving
support, with the open comments option as before plus an additional question asking
carers to rate the support on a scale from excellent to poor. The initial intention was to
send this to carers after support had ended and allowing a period of 3-4 months before
contacting bereaved former carers, but because the level of post-bereavement support
delayed the closure of many cases there were time constraints in obtaining sufficient
data within the 12 month period covered by this report. To address this, carers whose
cases were closed or who had been receiving YTP support for a lengthy period (at least
3-4 months) were contacted by a volunteer at CL and asked to complete the form over
the telephone.
3. A third form [CFQ3] bearing identical questions to CFQ2 but accompanied by a
differently worded cover letter was sent to a small number of carers whose cared for
person had died shortly after being referred to YTP, making it inappropriate to attempt
the “before” and “after” impact measurement of CFQ1 and 2.
Carers were made to understand that responses could be anonymous, although 1 in 5 of those
returning a CFQ1 chose to sign or put their name to the form. Additional comments from forms
are included in Appendix 1.
In addition to the forms listed above, carer comments were noted informally during telephone
and (occasionally) personal contacts, at points where the carer appeared to be offering a
comment on the service overall. These anonymised comments are included in Appendix 2.
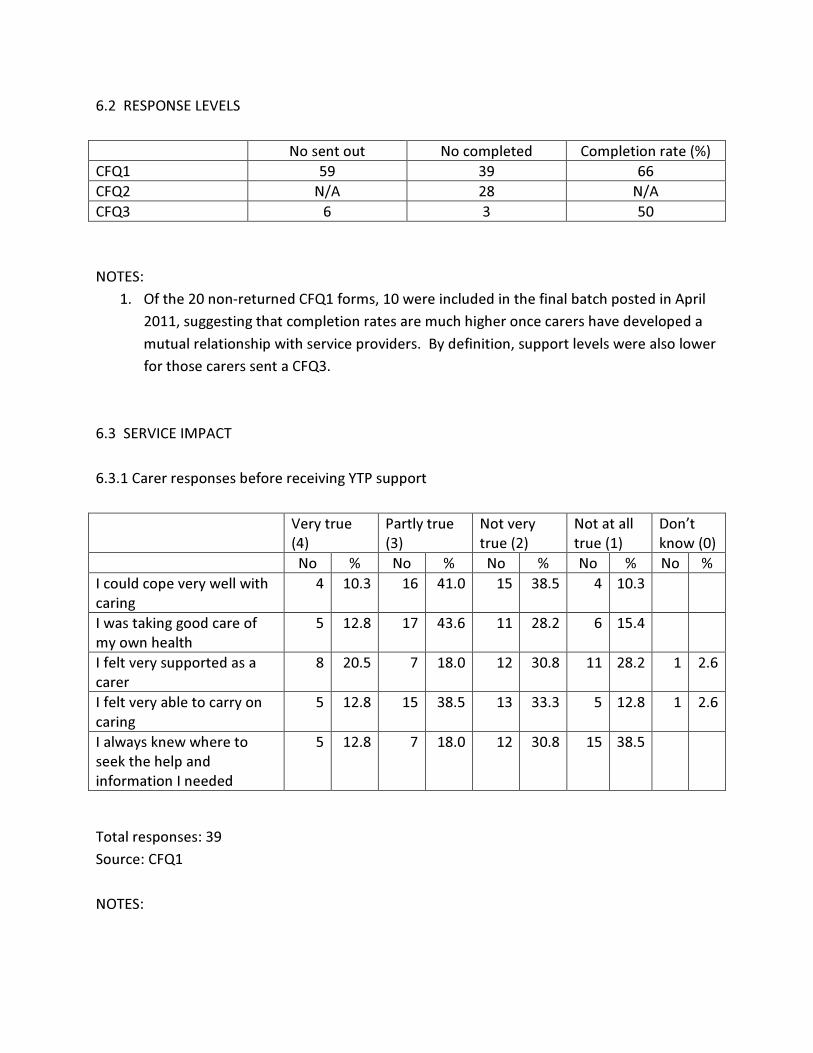
6.2 RESPONSE LEVELS
No sent out No completed Completion rate (%)
CFQ1 59 39 66
CFQ2 N/A 28 N/A
CFQ3 6 3 50
NOTES:
1. Of the 20 non-returned CFQ1 forms, 10 were included in the final batch posted in April
2011, suggesting that completion rates are much higher once carers have developed a
mutual relationship with service providers. By definition, support levels were also lower
for those carers sent a CFQ3.
6.3 SERVICE IMPACT
6.3.1 Carer responses before receiving YTP support
Very true
(4)
Partly true
(3)
Not very
true (2)
Not at all
true (1)
Don’t
know (0)
No % No % No % No % No %
I could cope very well with
caring
4 10.3 16 41.0 15 38.5 4 10.3
I was taking good care of
my own health
5 12.8 17 43.6 11 28.2 6 15.4
I felt very supported as a
carer
8 20.5 7 18.0 12 30.8 11 28.2 1 2.6
I felt very able to carry on
caring
5 12.8 15 38.5 13 33.3 5 12.8 1 2.6
I always knew where to
seek the help and
information I needed
5 12.8 7 18.0 12 30.8 15 38.5
Total responses: 39
Source: CFQ1
NOTES:

1. Some carers feeling very able to cope before TYP contact noted they were already being
supported by agencies such as St Christopher’s Hospice. Internal CL referrals were also
already receiving support.
6.3.2 Carer responses after receiving YTP support
The support I have had
from Carers Lewisham
[has]...
Very much
(4)
A little (3) Not very
much (2)
Not at all
(1)
Don’t
know (0)
No % No % No % No % No %
... helped me cope better
with caring
26 83.9 4 12.9 1 3.2
... helped me take better
care of my health
20 64.5 7 22.6 2 6.5 2 6.5
... helped me feel more
supported as a carer
27 87.1 3 9.7 1 3.2
... helped me to carry on
caring
26 83.9 1 3.2 2 6.5 2 6.5
... given me a better idea of
where to seek the help and
information I need[ed]
27 87.1 2 6.5 1 3.2 1 3.2
Total responses: 31
Source: CFQ2 + CFQ3. [Square brackets indicate slight wording differences on forms which
allowed for whether or not caring had ended.]
NOTES:
1. One respondent raised new support needs before completing responses by telephone
and was referred to CL staff before completion. Unfinished answers are entered as
“Don’t know.”
2. One carer contacted the YTP manager after receiving a CFQ3 to ask whether to
complete a response that would be very negative. On being encouraged to do so, she
returned a form with all questions answered “Not at all,” an overall rating of “Poor”
and a comment which read in full: “I seemed unable to access any help in spite of
completing forms and ringing and giving information when my husband was taken into
hospital in late September 2010 – then Carers began to put various things into place
for when he came out of hospital. Sadly he passed away in hospital. It would be very
helpful if there could be easier access. As we had to change Dr’s surgery and had new
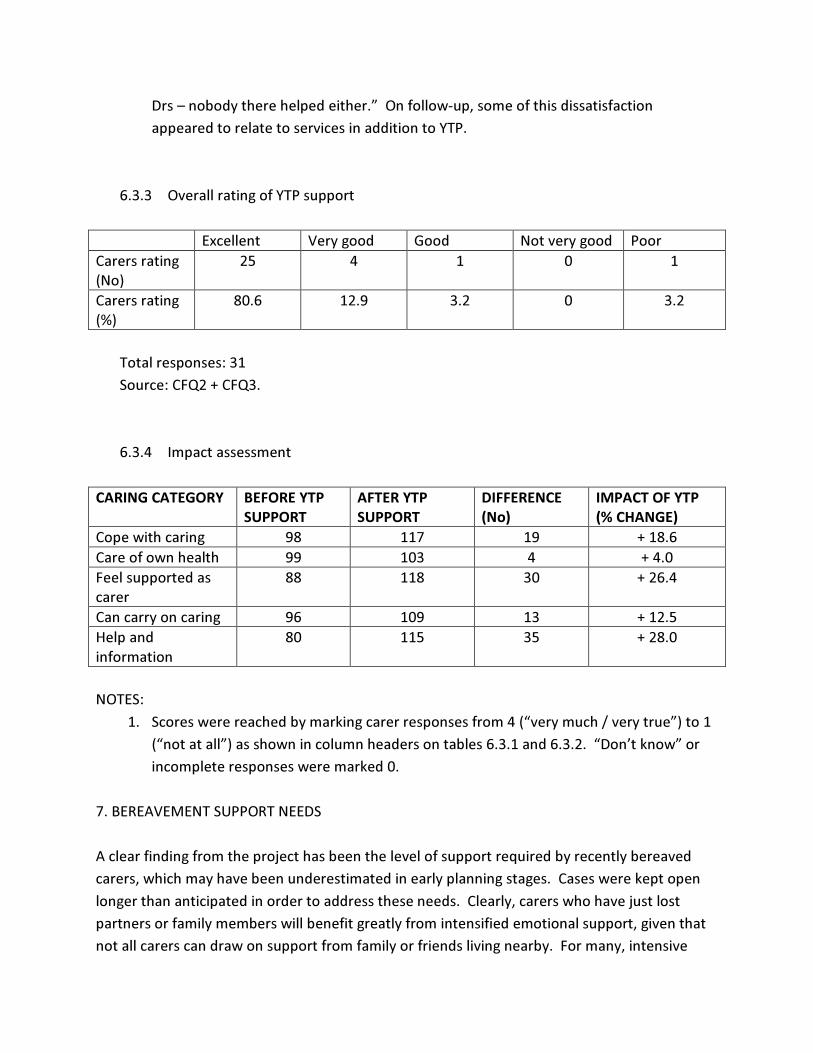
Drs – nobody there helped either.” On follow-up, some of this dissatisfaction
appeared to relate to services in addition to YTP.
6.3.3 Overall rating of YTP support
Excellent Very good Good Not very good Poor
Carers rating
(No)
25 4 1 0 1
Carers rating
(%)
80.6 12.9 3.2 0 3.2
Total responses: 31
Source: CFQ2 + CFQ3.
6.3.4 Impact assessment
CARING CATEGORY BEFORE YTP
SUPPORT
AFTER YTP
SUPPORT
DIFFERENCE
(No)
IMPACT OF YTP
(% CHANGE)
Cope with caring 98 117 19 + 18.6
Care of own health 99 103 4 + 4.0
Feel supported as
carer
88 118 30 + 26.4
Can carry on caring 96 109 13 + 12.5
Help and
information
80 115 35 + 28.0
NOTES:
1. Scores were reached by marking carer responses from 4 (“very much / very true”) to 1
(“not at all”) as shown in column headers on tables 6.3.1 and 6.3.2. “Don’t know” or
incomplete responses were marked 0.
7. BEREAVEMENT SUPPORT NEEDS
A clear finding from the project has been the level of support required by recently bereaved
carers, which may have been underestimated in early planning stages. Cases were kept open
longer than anticipated in order to address these needs. Clearly, carers who have just lost
partners or family members will benefit greatly from intensified emotional support, given that
not all carers can draw on support from family or friends living nearby. For many, intensive
daily care of a dying relative has been their primary concern for a period of weeks, months or
even longer, and a sometimes helpless sense of needing to readjust the whole of their life’s
focus can make the normal process of grieving even more difficult. In addition, however, carers
potentially face a raft of practical issues to attend to on the death of the patient, especially
when the death was not in a hospice or hospital whose staff will normally assist. In addition to
practicalities addressed in the MCCC Bereavement booklet, which focuses largely on registering
the death and arranging the funeral, these can include:
• Reassessment of care needs. Many elderly carers themselves have needs and may have
been in a mutually co-caring situation for example with a spouse. Some will need
assistance in gaining a reassessment or Care Plan review from Social Services.
• Housing needs. Some carers move in with the person they are looking after only to find
their tenancy insecure after the patient’s death. Carers require advice around local
social housing policy (in Lewisham, tenancies are only automatically transferred once
within the family and occupants given a formal grace period of 28 days before being
required to vacate) as well as possible advocacy and assistance in making special
representations to the local authority.
• Financial advice. On the demise of (in particular) a spouse, the surviving partner may
need to notify benefit providers (for the DWP, the AA/DLA Helpline on 08457 123456 is
helpful), pension or mortgage providers as well as reassess their own financial security.
Some carers will need referral to specialised debt management advisers, especially in
the not uncommon cases where the carer has given up paid employment in order to
care for someone and has suffered financially as a result.
• As TV licences are free to people over 75, most couples will apply in the name of the
first partner to reach this age. In many marriages this will be the male who is also
statistically more likely to be the first to die. It can be distressing for surviving partners
under 75 to find they are inadvertently breaking the law and helpful to advise them of
requirements at a suitable time after the bereavement.
• The Bereavement Register (www.the-bereavement-register.org.uk or 01732 467940)
can stop unwanted mail being sent to the deceased, which can be painful for survivors.
• Some carers will need to amend their will (or decide to make one) after a bereavement
and need help finding a solicitor, i.e. through the Law Society.
• For counselling needs, see Part 4.4 LOCAL SERVICE SHORTFALLS.
8. ASSESSMENT OF SERVICE MODEL

YTP was established as a telephone-based support service based at an established carers’
centre. Some implications of this are assessed here.
8.1 TELEPHONE SUPPORT
The theoretical advantage of offering support by telephone is that more carers can be
contacted and supported during the same time period. Some carers nevertheless required or
requested personal meetings, either by appointment at CL or by home visits in those frequent
cases where carers felt unable to leave the caring situation. Personal meetings usually provided
a much more detailed interaction, with a wider range of issues being raised and apparently a
higher degree of trust in the project on the part of carers. Inevitably, workload always
increased to fill the available time, so comparisons of this kind were possible.
Not all carers, who are by definition likely to be in a demanding and stressful situation, respond
positively to what may feel like “cold calling” from an outside agency. There was occasionally
some confusion between YTP/ CL and statutory services, with both negative and positive
results, but on the whole the reputation and status of CL in the local community was a major
benefit (see 8.2 below). Several carers, including in particular some of the elderly, appeared to
be reluctant to reveal much to a stranger over the telephone: the spectre of the “bad social
worker” who puts family members “into care” may still haunt some carers.
On the whole a telephone service would appear to be effective, providing there is sufficient
flexibility built in to allow for face-to-face meetings in addition, which was usually possible in
the present case.
8.2 LOCATION OF PROJECT
Probably the crucial factor in YTP’s achievements was the fact that it was based in an already
well-established carers centre. Essentially, this meant:
• Potential referring agencies were likely already to be aware of the centre and could
refer all carers without having to refer to specific project criteria;
• Referrals could then be sorted and allocated to YTP in-house at CL;
• Carers already registered, sometimes with low levels of support, could be identified and
directed to YTP after a change in the condition of their cared-for person (a major source
of referrals); and
• YTP carers could benefit from a raft of additional services not available elsewhere in the
borough, ranging from support groups and occasional respite to social and relaxation
events, as well as draw on the counselling service and collected expertise of CL staff.
Not having access to these services would have made support of EOL carers immensely more
difficult, and much carer feedback indicated the benefits carers had gained by being able to
draw on a broad range of services from the same source.
8.3 SERVICE DIFFERENTIATION
Some elements of the service provided by YTP are available from other local agencies, but no
other project offers the same range and focus. The specific advantages offered by a project
such as YTP are:
• One-stop service. As noted above, the fact that YTP was embedded in an already
established carers’ centre gave access to a wide range of support services, including
support groups, relaxation and social events unique to the area.
• Carer focus. Unlike most primary and secondary healthcare, the primary focus was on
carers rather than patients. Carers with intensive caring responsibilities, including many
carers of those at EOL, are much more likely than average to suffer ill health in turn, so
supporting them acts to reduce future demand on health services.
• Early intervention. Carers of those with dementia were able to be identified before the
condition had progressed too far and while advance care planning / power of attorney
were still possible.
• Pro-active support. YTP is pro-active, contacting carers at intervals according to
assessed level of need rather than waiting for carers to request support. This helps
reduce the isolation commonly reported by carers, works to prevent breakdowns in the
caring situation and helps avert the increased demand on public services that would
follow.
• Counselling. Even with the difficulty noted in 4.4.1, carers who had entered counselling
prior to their bereavement were able to continue receiving counselling support
afterwards without the lengthy wait encountered with local bereavement counselling
services.

9. RECOMMENDATIONS FOR FUTURE SERVICE PROVISION
9.1 Post holder
I would suggest that as well as having ideally had experience of being a carer and if possible a
carer of someone at the end of life, any future post holder should have counselling
qualifications. EOL carers are likely to be highly distressed at times, and the range of
communication is also limited in the case of telephone conversations between people who
have never met. I’m aware of having drawn on my own counselling skills in talking to carers,
both in establishing a climate of trust where a carer can express their fears and worries to a
“stranger” and in terms of “holding” strong and difficult emotions which carers themselves may
find it hard to face up to. There are also issues of dealing with potentially unnerving or
frightening thoughts and emotions that the death of a loved one can evoke, a necessary
understanding of the mourning process and an awareness of the risk of retraumatising a carer if
a response is misjudged at a sensitive time.
9.2 Location of service
As stated above (see 8.2), a service such as YTP will benefit immensely from being linked as
closely as possible with pre-existing carer support services. Without this, it could still be
possible to provide a basic “befriending”-type service, but the potential positive effects for
carers will be greatly diminished.
9.3 Referrals
Weaknesses identified in the present referral system could be addressed by:
9.3.1 Providing GP surgeries with small cards in stands for doctors, practice nurses and
front-desk staff to hand to carers as they are identified. This would not replace the
need for practices to register carers but would act as a prompt and a reminder (i.e. GPs
have cards in sight on their desk). This has been successful elsewhere and is
inexpensive. GPs are clearly working toward multiple targets and will benefit from aids
to increasing their awareness of carers’ needs.
9.3.2 Wherever possible, all agencies obtaining carer consent to a referral would hand
the carer a project flyer provided to them in advance as part of the project’s promotion,
which would in turn reduce possible confusion on the carer’s part when the contact call
is made and help improve confidence and trust from the outset.
9.4 Counselling
See 3.4.1 for service shortfall identified in Lewisham, a problem arising from a relative
inflexibility in counselling provision and delays in assessing and allocating counselling clients
which make it hard to access counselling at the “right time” prior to and after their

bereavement. It would be a significant improvement to identify funds to provide for a
counsellor with appropriate (bereavement) training who can be on call at short notice to
provide short-term support to carers at the time of greatest need.
MIKE DISS
YTP Service Manager
August 2011

APPENDIX 1: CARER COMMENTS FROM FEEDBACK FORMS
Carers completing feedback questionnaires were given the option to make any additional
comments they wished. In all, 76.1% of respondents chose to do so (69.2% for the first
questionnaire rising to 85.7% for the second and third). Nearly all comments were positive (see
6.3.2 for the main exception), with the predominant feeling being one of gratitude for the
support received:
Thank you so much for all your help you have given and advice. Even when I thought
there was nothing you could do, you still did, you cared for me! Without your help I
wouldn’t and nor would my Dad be so happy.
I think the service is very good. Mike always contacts me and tells me what’s going on.
It’s very helpful.
I am very grateful to know that there is someone there to help if I need them.
I feel like someone is listening. I don’t feel desperate and depressed. I am very grateful
that the support I have received has given me the strength to ‘be there’ for my mum.
I have had outstanding continuing support and received consistent counselling for
bereavement. Words can really not express my sincere gratitude to Lewisham Carers.
Thank you so much.
Carers often noted personal improvements they had felt in themselves as a result of being
supported, including increased confidence and feeling less isolated:
Since joining Carers I feel more secure.
Carers Lewisham has made a huge difference as I feel I now have somewhere to go for
help and support. It is wonderful to know I am not the only person who struggles with
caring.
I decided to care for my mother rather than have her end up in a residential nursing
home. Once I took up the role of carer, I felt totally isolated and unsupported by all the
local authorities. It was suggested I register with Lewisham Carers which I did. They are
now the first port of call if I have any problems or concerns. Lewisham Carers in my
opinion are my support and guidance.
I’m quite happy with the service – it’s a lifeline to us. At least now I can open up and talk
to people, and that’s very important to me.
Many carers saw the support they received from the Yew Tree Project in the context of broader
support from Carers Lewisham, either because YTP had linked them to other services or
because they were already being supported by CL before being identified as appropriate for
referral as EOL carers. Carers often referred to the value of the drop-in groups and social
gatherings which helped them overcome feelings of isolation and build up support networks.
Since going to Carers Lewisham, I feel so much support has been given to me and I am
now beginning to feel more confident. I look forward to my coffee mornings on
Tuesdays and feel so good to be part of society again. Thank you so much.
Carers Lewisham enabled me to know my rights as a carer, supported me in dealing with
service providers for the people I care for, gave me confidence in dealing with issues, and
helped me in taking care of myself. I especially appreciate the carers drop-in sessions
and the social events which provide respite from caring.
A fine organisation. I felt so isolated before I found them. I feel they really do recognise
the role I play as a carer, and all the good and bad aspects of that. Also through carers I
have built a network of support friends who are always there for each other.
Without the help and support of Carers and the other users I think I would have gone
mad or died of exhaustion. Thank you.
Some respondents said they valued the reliability of YTP:
Very consistent in telephoning and aftercare.
Mike was very supportive with lots of things and he kept in contact with me.
In my caring role I come across problems at times but I know there is always a friendly
and caring person I can get in touch with at Carers for advice. I can pick up the phone
and call or just drop in at the office. There is always a caring person to discuss your
problems with, which makes life more at ease.
I think that having someone you can talk to at any time helps a lot even if you don’t use
all the facilities available. Knowing that there is someone you can turn to helps a lot.
As noted, carers who felt motivated to make additional comments were almost unanimously
positive. One carer did note a peerceived shortfall in services offered:
Would like more for carers who work full-time (at times they can get to them – e.g.
evenings / weekends).
For any future evaluation of similar projects, it could be felt helpful to probe more deeply into
perceived shortcomings of the type of support made available. The nature of the feedback
received is doubtless affected by the respondents’ usually fraught emotional state at this period
in their lives, the strong sense of gratitude for a helping hand offered at an extremely
challenging time and the need to remain sensitive and delay the request for a retrospective
assessment until a suitable time after a bereavement. Even allowing for this, the great majority
of voluntary comments made by carers were unhesitatingly positive.
A huge thank you for all the help I have received from Mike.
I think everything is great – a great service.
APPENDIX 2: INFORMAL CARER COMMENTS
These comments were logged during support calls to carers; in 3 cases with several comments
noted from the same call. The comments were unsolicited and carers were not aware their
comments were being recorded.
1. “It’s nice to know someone’s there – if I need advice I only need to pick up the phone”
(7/9/10)
2. 18/10/11:
a. “I feel daily very humble & so grateful that people come & take an interest. I have
you to count on whenever I need.”
b. “It’s very comforting to know I only have to reach out & I will get help. Believe
me, it gives me a feeling of security.”
c. “I seriously & honestly think all of you are doing a very wonderful job. It’s so
kind of you. I know I can talk to you honestly like I can’t to anyone else.”
d. “You’ve all been so wonderful & I mean it when I say I don’t feel alone now
because I can pick up the phone & say “hey Mike, what do I do?” & you’ll have
an answer. After so long without having anyone to turn to, it’s such a relief to
know you’re there.”
e. “Quite honestly, you are my counsellor, because you’re the only one I can talk to
like this. You’ve got me to bare my soul to you & I’ve never done that to anyone
else.”
3. “Although I don’t use many of the services you offer, I’m really grateful that you
remember and take the time to keep calling me – that means a lot.” (7/12/10)
4. “It’s the Carers right now who are my lifeline” (10/12/10)
5. “Thank you for calling. You don’t know how important it is for me to have someone on
the other end of the phone I can rely on. It means a lot” (10/12/10)
6. “You’ve made me feel better already. It makes me feel better to know someone doesn’t
think I’m talking a load of rubbish and takes the time to listen to me” (13/12/10)
7. “I’m very grateful for your calming voice on the phone” (20/12/10)
8. “Thank you very much for your care & concern. It really does matter that there’s
someone who realises things can get difficult sometimes” (20/12/10)
9. “It’s nice to know somebody cares about me” (5/1/11)
10. “”It’s nice to know if I need to know something there’s somewhere I can call – if I have a
problem I can pick up the phone and you’ll help. Thank you very much – you’re doing a
grand job Mike!” (11/1/11)
11. 28/1/11:
a. “It’s so kind of you to ring up every now & again to see how I am – that is nice.”
b. “I wish you luck in all you do. You’re a tremendous asset to the Carers … You’re
a tremendous man for answering questions.”
12. “Throughout all this you’ve stayed in constant contact – you’re the only one who has. It’s
a shame the other services don’t do that, then people wouldn’t be in such a bad way. It’s
such a vital thing” (31/1/11)
13. “You’ve been an absolute saint – and I mean that!” (2/2/11)
14. “I like when you ring – it’s nice” (8/2/11)
15. “Everyone knows about CL – what a lifeline it is for all of us. Look at X, how much he’s
changed. He’s thinking about doing voluntary work now, it’s turned him right round –
he’s got a goal to aim at now” (8/2/11)
16. “There are up days and down days, but at least we have CL. I really can’t praise you
enough for all the things you’ve done for us. It gives us a life” (21/2/11)
17. “I wanted to ring to say thanks. I just met you briefly but you were lovely. You gave me
information about Macmillan nurses and mum had them for a few days before she died.
She’d only been out of hospital a week but she said she wanted to be at home and that
was where she died. It was so peaceful – I don’t have any regrets at all. I was with her
when she drew her last breath. Thanks very much for caring” (22/2/11)
18. “Half the time they [Social Services] don’t do what they say they will. It’s only you that
keeps pushing” (1/3/11)
19. “Thank you for ringing & talking to me. I always feel better after we’ve spoken on the
phone” (30/3/11)
20. “Things are starting to happen now, and it’s all thanks to you” (1/4/11)
21. “It’s nice to know there’s some support there, because I must admit sometimes I get very
tired” (1/4/11)
22. “Thank you very much for your words of comfort & support over the last few weeks. It’s
helped me get through all this” (12/4/11)
23. “It’s nice to know you’re there and you can speak to someone if you get too stressed out”
(13/4/11)
24. “You have the special touch & you do come through for all of us. I don’t think there’s
been anyone else in your position [at CL]. I’ve certainly never spoken in this depth with
anyone else. This relationship is very important to me, & I think to others too – not that
we spend all our time talking about you, of course!” (10/5/11)
25. “Just sitting down talking to you has been a lovely moment. I feel rested and cheered up
now. God bless you” (10/5/11)
26. “I really appreciate that you’ve taken time to call [after my bereavement] just in case I
was feeling wobbly or anything” (16/5/11)
27. “I would love to have the money to take you out for a meal – you, the hospice and the
hospital have been so good to me all this time. I don’t know how I’d have managed
without you” (18/5/11)
28. 3/5/11:
a. Three months ago I didn’t have anyone on my side – now I’ve got you. It’s great
to know I can pick up the phone or drop in to one of your groups and find out how
other people cope with this.
b. I know I have you on my side and I can turn to you and ask you when I need
something. I’m really lucky to have you on board.
c. When I wanted a power of attorney and asked at CL I was totally shocked. It was
so nice to come to you and not go to a solicitor who would only look at pound
signs and not bother about [my husband’s] and my needs emotionally. I don’t
think I would have got it delivered and explained the way you did. When I came
to CL I just thought maybe you could recommend a more caring solicitor.
d. Thanks very much for getting back in touch – I feel very relaxed now and ready to
deal with whatever comes up.
29. “Thank you for all your help and support. You’ve been a true friend” (7/6/11)
30. “Thanks for ringing – it’s been a relief to have someone to talk to” (8/6/11)
31. “You’ve been a real friend & I’ve been able to talk to you freely. I’m not asking, but you
seem to have walked down this road yourself and have sympathy and understanding. I
feel I can say almost anything to you and you’ll understand. If you can give love and
understanding that’s what people really need, isn’t it?” (16/6/11)