THE WE-CARE ROADMAP: A FRAMEWORK FOR ... - jami.org.ua · 120 THE WE-CARE ROADMAP: A FRAMEWORK FOR...
13
120 THE WE-CARE ROADMAP: A FRAMEWORK FOR IMPLEMENTATION OF PERSON-CENTRED CARE AND HEALTH PROMOTION IN MEDICAL ORGANIZATIONS Roman Lewandowski, PhD University of Social Sciences, Lodz, Poland Voivodeship Rehabilitation Hospital for Children in Ameryka, Poland Abstract As a result of a multinational and multi-industrial scientific project, a framework supporting implementation of Person-Centred Care (PCC) and Health Promotions (HP) has been developed. The framework has been called “WE-CARE Roadmap” and consists from five enablers: technology, quality measures, infrastructure, incentive systems and contracting strategies. (PCC) and (HP) are promising approaches to contain costs of healthcare while maintaining and even improving the quality of medical services. However, the implementation of PCC and HP in many organisations was unsustainable. They were implemented as projects or interventions but after the cause of implementation despaired (e.g. the research program was finished) the care slipped back into ‘usual care’. The WE-CARE Roadmap appears to have a great potential to become an important implementation tool ensuring PCC and/or HP sustainable functioning in medical organisations. Initial research has shown the WE- CARE Roadmap potential. However, the framework is not widely recognised and needs revision and explanation. The main barrier to more extensive usage of the framework may be the lack of comprehensive definitions and descriptions of the five enablers. What each enabler stands for, what it embraces, and what are the mechanisms through which the five enablers support the implementation of PCC and/or HP. Thus, the study revises and defines the enablers, as well as deepens the understanding, how each enabler separately and all of them together, as a system of enablers, facilitate the implementation of PCC and/or HP. The comprehensive definition of enablers and analysis of their functioning may help researchers to further investigate the promising framework and managers use it as a tool for PCC and/or HP implementation in their organisations. Keywords: healthcare management, person-centred care, health promotions, implementation sciences, healthcare quality, cost containment JEL Codes: M12, D22, I18 Received: August 17, 2020 Revised: September 15, 2020 Accepted: September 19, 2020 Lewandowski, R. (2020), “The WE-CARE Roadmap: A Framework for Implementation of Person-Centred Care and Health Promotion in Medical Organizations”, Journal of Applied Management and Investments, Vol. 9 No. 3, pp. 120-132. Introduction From decades developed countries have been suffering from the continuous growth of healthcare expenditure which has been faster than the GDP growth, what in the future may jeopardize the ability to provide high-quality healthcare to all citizens. This problem enforced representatives from 28 European countries of key players from the pharmaceutical industry, technology sector, academic researchers, and health professionals, together with patient representatives and politicians to establish the WE-
Transcript of THE WE-CARE ROADMAP: A FRAMEWORK FOR ... - jami.org.ua · 120 THE WE-CARE ROADMAP: A FRAMEWORK FOR...

120
THE WE-CARE ROADMAP: A FRAMEWORK FOR
IMPLEMENTATION OF PERSON-CENTRED CARE
AND HEALTH PROMOTION IN MEDICAL ORGANIZATIONS
Roman Lewandowski, PhD
University of Social Sciences, Lodz, Poland
Voivodeship Rehabilitation Hospital for Children in Ameryka, Poland
Abstract
As a result of a multinational and multi-industrial scientific project, a framework
supporting implementation of Person-Centred Care (PCC) and Health Promotions
(HP) has been developed. The framework has been called “WE-CARE Roadmap” and
consists from five enablers: technology, quality measures, infrastructure, incentive
systems and contracting strategies. (PCC) and (HP) are promising approaches to
contain costs of healthcare while maintaining and even improving the quality of
medical services. However, the implementation of PCC and HP in many organisations
was unsustainable. They were implemented as projects or interventions but after the
cause of implementation despaired (e.g. the research program was finished) the care
slipped back into ‘usual care’. The WE-CARE Roadmap appears to have a great
potential to become an important implementation tool ensuring PCC and/or HP
sustainable functioning in medical organisations. Initial research has shown the WE-
CARE Roadmap potential. However, the framework is not widely recognised and
needs revision and explanation. The main barrier to more extensive usage of the
framework may be the lack of comprehensive definitions and descriptions of the five
enablers. What each enabler stands for, what it embraces, and what are the
mechanisms through which the five enablers support the implementation of PCC
and/or HP. Thus, the study revises and defines the enablers, as well as deepens the
understanding, how each enabler separately and all of them together, as a system of
enablers, facilitate the implementation of PCC and/or HP. The comprehensive
definition of enablers and analysis of their functioning may help researchers to further
investigate the promising framework and managers use it as a tool for PCC and/or HP
implementation in their organisations.
Keywords: healthcare management, person-centred care, health promotions,
implementation sciences, healthcare quality, cost containment
JEL Codes: M12, D22, I18
Received: August 17, 2020
Revised: September 15, 2020
Accepted: September 19, 2020
Lewandowski, R. (2020), “The WE-CARE Roadmap: A
Framework for Implementation of Person-Centred Care and
Health Promotion in Medical Organizations”, Journal of
Applied Management and Investments, Vol. 9 No. 3, pp.
120-132.
Introduction
From decades developed countries have been suffering from the continuous
growth of healthcare expenditure which has been faster than the GDP growth, what in
the future may jeopardize the ability to provide high-quality healthcare to all citizens.
This problem enforced representatives from 28 European countries of key players from
the pharmaceutical industry, technology sector, academic researchers, and health
professionals, together with patient representatives and politicians to establish the WE-

121
CARE project (Grant Agreement 602131) funded by the EU’s Seventh Framework
Programme for Research (FP7). During five workshops in 2014 and a conference in
April 2015, a framework called the WE-CARE Roadmap has been developed (Ekman
et al., 2016). The framework identifies the principal areas where interventions and
policies are required to address the major challenges for healthcare systems. The WE-
CARE Roadmap proposed two major themes Person-Centred Care (PCC) and Health
Promotion (HP) capable of increasing quality and contains costs in healthcare as well
as five critical enablers supporting the implementation of PCC and HP. These enablers
are: technology, quality measures, infrastructure, incentive systems and contracting
strategies (Ekman et al., 2016).
Person-Centred Care (PCC) and Health Promotions (HP) are promising
approaches to contain costs of healthcare while maintaining and even improving the
quality of medical services (Ekman et al., 2012; Fossey et al., 2006; Fors et al., 2016;
Fors et al., 2017). However, the implementation of PCC and HP in many organizations
was not sustainable. They were implemented as projects or interventions but after the
cause of implementation despaired (e.g. the research program was finished) the care
slipped back into ‘usual care’ (Alharbi et al., 2014; Moore et al., 2017). The WE-
CARE Roadmap appears to have a great potential to become an important
implementation tool ensuring PCC and/or HP sustainable functioning in medical
organizations. Some first research has shown the WE-CARE Roadmap potential
(Lloyd et al., 2020), however, the framework is not widely recognized and needs
revision and explanation. The main barrier to more extensive usage of the framework
may be the lack of comprehensive definitions and descriptions of the five enablers.
What each enabler stands for, what it embraces, and what are the mechanisms through
which the five enablers support the implementation of PCC and/or HP.
Thus the paper aims to revise and define the enablers, as well as deepens the
understanding, how each enabler separately and all of them together, as a system of
enablers, facilitate the implementation of PCC and/or HP. The comprehensive
definition of enablers and analysis of their functioning may help researchers to further
investigate the promising framework and managers use it as a tool for PCC and/or HP
implementation in their organizations.
Person-Centred Care and Health Promotion
Person-Centred Care (in Great Britain this concept is usually called Person-
Centred Coordinated Care (P3C)) is an approach getting its popularity in an increasing
number of countries. PCC usually entails three pillars (Britten et al., 2017, p. 408). The
first pillar consists of initiating a partnership by eliciting the patient narrative. The
narrative refers to the sick person’s description of their illness, symptoms and impact
the illness has on their lives. It embraces the person’s functioning in everyday life,
what capabilities they have, including patient’s social network, which could facilitate
treatment and everyday life. The ill person personal account about living with the
illness is in contrast to medical narratives that reflect the biomedical markers and
evidenced-based guidelines for treating the disease. The second pillar covers the
process of shared decision-making concerning treatment plan, based on sick person
capabilities, goals and weaknesses derived from patient narrative and medical
knowledge of the professional. The aim is to work together as a team. Patient, very
often their relatives and professionals, on equal terms – to achieve mutually agreed

122
treatment goals. The third pillar encompasses the process of permanent safeguarding
the partnership by documenting the sick person’s narrative and recommendations of a
professional as a jointly agreed treatment plan (Ekman et al., 2011; Lewandowski et
al., 2020).
Health Promotion (HP) is an approach in many cases working in synchronicity
with PCC and is understood here as a vehicle for supporting people to increase control
over their health by influencing individuals and communities mostly through
information while taking into consideration their life context and socioeconomic
conditions (Lloyd et al., 2020).
WE-CARE Roadmap and the Five Enables
The WE-CARE Roadmap was developed to support the implementation of PCC
and/or HP and make it a sustainable solution. However, so far there is very little
research about the framework. Especially there is a lack of comprehensive definitions
of the enablers.
Figure 1. Dimensions and critical enablers of the revised WE-CARE Roadmap
framework
Information system (quality measures)
In the first version of the framework used a narrow definition of the information
system, referring only to the quality measures. This appears an important omission. If
the framework is expected to contain costs it cannot avoid measuring them. Measuring
only quality may lead to increase in costs instead of their containment. The
measurement system should also be an important tool for monitoring the depth to
which the PCC and/or HP was implemented in a medical organization. Because
otherwise, the organization is unable to assess to what extent it works in concordance
with the PCC and/or HP approach. The information system has to measure for
example, how many patients are embraced with PCC and/or HP practices? For how
many patients professionals document patient's narrative? How accurately and how
deeply professionals follow the principles of the PCC approach? Thus, in the revised
framework the enabler ‘quality measures’ is exchanged by a more broad and relevant
category, an ‘information system’.
Accurate measurement of quality of care and costs in a proper span of care and
scope of time is one of the most important condition to achieve improvement in health
care (Porter, 2010). However, proper measurement is extremely difficult since many
patients suffer from multiple medical conditions and are treated by many providers at

123
the same time. Quality in healthcare could be measured in three fundamental areas:
structure, processes and outcomes (Donabedian, 1966; Lewandowski and Kowalski,
2008).
Structure embraces all of the factors that create the context in which care is
delivered. This comprises the physical facility such as buildings, IT, medical
equipment; human resources (levels of professional and social skills). The structure is
often the simplest area of quality to observe and measure and it may be the primary
cause of problems identified in processes (Donabedian, 2003).
Processes could be classified as technical procedures including diagnosis and
treatment, but also preventive care, patient education and interpersonal processes
regarding how care is delivered and involvement of patients’ families and members of
their social networks. According to Donabedian (2003), the measurement of processes
is almost equivalent to the measurement of quality of care since processes encompass
all aspects of healthcare delivery. Thus processes are core components which should be
adjusted for sustainable implementation of PCC and/or HP.
Outcome covers all the effects of healthcare on patients or populations, including
improvements of different aspects of patients’ health, experience and especially health-
related quality of life. Outcomes could be seen as the most important indicators of
quality since neither good healthcare structure nor the best processes guarantee an
improvement in patients quality of life. Porter claims that ‘Measuring, reporting, and
comparing outcomes is perhaps the most important step toward unlocking rapid
outcome improvement and making good choices about reducing costs. Outcomes are
the true measures of quality in health care.’ (2010b, p. 1). However, measurement of
outcomes of healthcare intervention is very difficult since identifying relations between
structure, processes and outcomes require large research sample, considering many
personal and socio-environmental factors, and long-term follow-ups - as outcomes may
take considerable time to become observable (Donabedian, 2003; Kowalski et al.,
2015). In order the quality and costs could be used for comparison and learning, they
should be measured for each condition, with the presence of the other conditions used
for risk adjustment (Porter, 2010).
The measurement of the two other areas (structure and processes) without
measuring outcomes tends to distort efforts taken by the professionals and providers.
Measurement of structure could lead to excessive staffing and investment spending.
Measurement of processes may be equal to control of people behaviour that may lead
to micro-management and incremental improvements limiting ground-breaking
innovations. Since innovations cannot be achieved while following rigid behaviour
rules. Only measuring all of these three areas with a substantial focus on measuring
actual outcomes, may allow comparison between today’s care and innovative care.
Improvement in healthcare quality without slowing down the cost increase is
unsustainable. Although management accounting is well developed on a providers’
level there is still a lack of systems capable to track costs of patients’ treatment during
the whole cycle of care including other providers. This means that current cost
measurement is fragmented, reflecting patients’ costs in a particular medical setting, do
not allow to monitor costs of the individual patient through the entire chain of
providers patients are going through and for all their medical conditions
(Lewandowski, 2014). This fragmentation excludes the possibility of comparing costs
against outcomes and thus evaluate what value healthcare is delivering. The only

124
comparison of outcomes with costs gives the opportunity to contain spending by
reallocation of patients to more efficient types of services, eradicate of non-value-
adding procedures and better utilize resources (Porter and Teisberg, 2006). Well
established measurement and sophisticated analysis (e.g.: Kriksciuniene et al., 2019a;
Kriksciuniene et al., 2019b) allow learning and improvement of healthcare by the
delivery of adequate information and knowledge to decision makers.
Technology
One of the most important themes of the technology area is an information
technology (IT), which has been the driver for many latest innovations in most
industries. IT does not only allow the information flow regarding Electronic Health
Record (EHR) but also supports the collection of information, application of incentive
systems and contracting strategies.
IT enables the building of information systems containing time series of different
quality measures including periodically repeated Patient Reported Measures (PRMs)
which could be analysed for assessment factors influencing the process behaviour
(Kriksciuniene et al., 2019b) and the cause-effect relationship as well as strengthen the
interdependences among measures (Kriksciuniene et al., 2019a). Wearable electronic
devices could deliver health and activity-related data which together with artificial
intelligence and machine learning could serve in the implementation of PCC and HP
(Giżewski et al., 2008; Ognjanović et al., 2020; Mountford et al., 2016). All these may
lead to innovative ways of increasing quality and containing costs. IT role is to cope
with the communication gap, ensure interactive data flow, which can build new
knowledge and wisdom. Consequently, communication processes become more
efficient in terms of cost reduction and better quality.
Contracting Strategies
Contracting strategies (CS) are methods of financing of medical services at the
macro and meso levels. CS are usually sets of conditions related to structural,
processual and outcome quality measures and other factors (e.g. patient-related risk
factors) constructed by payers to influence the behaviour of healthcare providers
towards groups of patients by the flow of financial resources. In Europe there are
various types of contracts, among others: capitation, case-mix, fee for service, pay-for-
performance, fixed budget, and each of them stimulates different behaviour of
providers. For example, fee for service incentivizes to a greater number of services
(some unnecessary), but capitation and a fixed budget to the opposite direction (under
treatment) (Getzen, 1997).
To counteract these adverse phenomena more complex case-mix systems were
introduced which makes the amount of the payment dependent on patients’ condition
or diagnosis, demographics, such as gender or age, delivered treatment, and length of
hospitalization. However, some providers used case-mix conditions to screen patients
and apply pressure on doctors to admit only the profitable ones (Covaleski et al., 1993;
Lewandowski, 2014). Hence, contracting strategies should reward providers activities
related to PCC and/or HP such as listening to patients’ narrative and identification of
patients personal goals, co-creation of treatment and care plans, improvement in patient
self-efficacy and HP behaviours. All these activities are performed on the interpersonal
level between patients including their social networks and professionals. Thus,

125
professionals’ motivation to follow PCC and/or HP approach is a paramount issue.
Thinking about the construction for an environment facilitating PCC and/or HP
implementation on a large scale, such as national or European scale, it has to be
remembered that contracting strategies could significantly affect how managers of
medical providers shape organizational infrastructure, measurement and incentive
systems as well as employed technologies. Although professionals would advocate
PCC and/or HP approach, managers cannot support them against incentives enforced
by contracting strategies implemented by the payers and even cannot buffer
professionals from the incentives produced by contracting strategies since
professionals are the core operational staff delivering medical services and producing
organizational results (Lewandowski, 2013; Lewandowski and Sułkowski, 2018).
Incentive Systems
Incentive system should create motivation for both professionals and patients to
work according to PCC and/or HP principles. Motivation is a fundamental component
of any human activity and as such is a central constituent of medical services delivery
(Goncharuk, 2018; Goncharuk et al., 2020; Franco et al., 2002), personal health and
well-being (Fisher et al., 2003). The problem of incentive systems and motivation
relates to healthcare employees and patients to greater extend that in ‘usual care’, since
PCC and HP by definition require more intense personal involvement in the
relationship during treatment process by both parties.
Although motivation is a complex issue (Ryan and Deci, 2000) it could be
condensate to two main forces: extrinsic or intrinsic (Cerasoli et al., 2014; Flamholtz,
1996). When people behave in a certain way because they are interested in something,
and the behaviour arises from within the individual because an activity itself is
satisfying, in other words, the behaviour is driven by internal rewards - incentives are
intrinsic. When people follow a particular behaviour due to the rewards they expect to
receive from others (praise, pay) - incentives are extrinsic.
Extrinsic rewards require an assessment tool which could compere actual
behaviour with the standard, and reword the behaviour which follows the standard.
Assessment processes could be either subjective, based on supervisor ratings or
objective build on quantitative measures of performance. Objective assessment calls
for accurate and verifiable measures viable to reflect real performance in pivotal areas.
If measures do not meet these requirements might be manipulated, or people could in
good faith achieve good levels of measures but cause the harm to the expected
performance (cf. Malina and Selto, 2001). In the treatment processes employing PCC
and/or HP, these measures have to clearly address PCC and/or HP fundamentals, such
as elicitation of the patient narrative and the depth/strength of the partnership. These
features are very complex to assess using quantitative measures. However even if
quantitative measures would be designed, studies suggest that extrinsic motivators,
especially financial one are positively related to the number of tasks completed but not
with their quality (Ferreira and Otley, 2009). This suggests that incentive systems
should be built on qualitative assessment rather than on a quantitative one. But the
proper qualitative evaluation by superior of employee performance regarding
elicitation of the patient narrative and the depth/strength of the partnership is also not
straight forward.
Taking into account the complexity of the incentive systems based on extrinsic

126
motivators in PCC and HP approach and potential risk of their failure the intrinsic
motivation would be the preferable solution. But intrinsic motivation is hardly
dependent on external activity undertaken by organizational managers. The problem
with external incentives is extremely significant since no matter whether the extrinsic
rewards are objective (e.g. based on quantitative measures) or subjective (based on
supervisor assessment) tend to undermine intrinsic motivation for rewarded behaviour
(Deci et al., 1999; Levy et al., 2017). This could be one of the reasons, why sustainable
implementation of PCC and/or HP are not frequent (Alharbi et al., 2014; Moore et al.,
2017)
In this disadvantageous situation, some hope could be given by a human-
focused-design (Sanchez-Gordón et al., 2016). Human-focused-design defines people
intrinsic motivators and gives tools that allow effectively refer to these motivators to
increase professionals’ and patients’ positive experience with performed work, which
may increase their involvement in the treatment process (level of engagement in the
narrative, partnership and documentation). Designing patients and professionals
experience in the context of identifying and referring to their intrinsic motivators could
significantly increase the quality of care without increasing costs (Sanchez-Gordón et
al., 2016). It has been proven that human-focused-design solutions improve the degree
of compliance with medical recommendations and healthy living principles by patients
(Guthrie et al., 2015).
Infrastructure
Infrastructure could be understood very broadly as all physical and nonphysical
environments within which health services are delivered. However, in WE-CARE
Roadmap some important areas are distinguished separately, such as IT, information
systems (quality measures – in the previous version of the Roadmap), incentives and
contracting strategies. Thus, here infrastructure is defined as the all other aspects of the
physical and nonphysical environment such as buildings and medical equipment, a
different type of organizations (e.g.: hospitals, outpatient clinics, charities), internal
structure of these organizations (Lewandowski, 2010) quality and management systems
(Lewandowski, 2009) and relationships between these organizations, professions and
professional associations, medical guidelines and protocols, education and training
infrastructure, policy regulators, accreditation institutions (Kautsch and Lewandowski,
2009), just to mention a few. But the main challenge is how to transform sufficient part
of this infrastructure in such a way that it supports the implementation and sustainable
development of PCC and/or HP.
How the Enables of the WE-CARE Roadmap Works
The five enablers build into the WE-CARE Roadmap are strongly interwoven.
Any changes in one enabler must be synchronized with the others, so as not to cause
conflicting behaviours. Albeit enablers perform different functions in the process of
supporting the implementation and functioning of PCC and/or HP, to some extent they
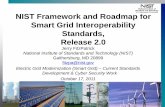
overlap each other. Figure 2 shows the mutual relations between enablers. The PCC
and/or HP implementation process should start from adapting the general PCC and/or
HP principles to the local conditions of a given organization (box 1). The result of this
adaptation should be policies, instructions, procedures and guidance of behaviour
tailored to individual providers, the scope of treated medical conditions and the forms

127
of provided care.
Processes:
- Delivery of care
- Development of sup orting PCC and HP
- Implementation o
according to PCC and HP standards and procedures
sup orting PCC and HP
/or
p /or
/orf
p
Infrastructure
Technology
Design of:- -
Contracting strategiesIncentives
PCC and HP
standardsand procedures
/or
Information about /orPCC and HPstandards and procedures
Information system:
o measuresQuality (costs) measuresHealth utcomes
- -
Results:High qualityLow ostc
Financial and non-financial rewards , when providers follow PCC and/or HP requirements
Adjustment of /or
principles tothe specific organisation
PCC and HP
Evaluative feedback
Corrective feedback
1
2
3
5
Figure 2. Interrelationships between enablers in the WE-CARE Roadmap
framework
These policies, instructions, procedures, and guidelines should incorporate into
the processes of care and treatment, including creating the appropriate infrastructure
and implementing supporting technologies (box 2). The specification and adaptation of
PCC and/or HP to a specific organization also allows the design of adequate
‘contracting strategies’ and ‘incentive systems’ at various levels of the organizational
structure (box 3). Incentives have to create guidelines in such a way that, every
employee must know exactly what to do to support the PCC and/or HP in their
organization.
Technology fulfils many functions in PCC and/or HP. In addition to purely
medical functions related to MHR, the support of the treatment and diagnosis process
itself, technology is an important element backing the implementation, functioning,
and improvement of PCC and/or HP. The critical function of technology (IT) is to
collect data on the quality and costs of treatment, on the activities performed by
professionals and on patients' condition and experience. IT systems must not only
support, but taking into account the level of information of the contemporary medical
organizations, IT must be the main vehicle of the information system. The information
system has to embrace all structures capable of collecting, processing, storing and
analysing data on the functioning of PCC and/or HP (also those collected manually).
Only such a comprehensive information system may allow an adequate assessment of
PCC and/or HP functioning in a given organization and consequently improve
outcomes of treatment and care processes (box 4). It is worthy to mention, that
information system in the shape described above is similar to many concept

128
functioning in organizational studies, such as Management Information Systems,
Performance Measurement and Management Systems, including Balanced Scorecard
(Lewandowski, 2008).
The information systems produce numbers which can serve to monitor the extent
to which PCC and/or HP goals and standards have been achieved. This means that they
can be used in two different modes: diagnostic and interactive (Lewandowski et al.,
2018, pp. 144–150; Simons, 1994). In diagnostic mode to assess whether the
modification of other enablers brings expected outcomes. And also to measure the
performance of care teams, individual providers and chains of providers as well as the
entire organization in order to take ‘corrective actions’. The corrective actions are
based on the ‘corrective feedback’ (box 5) which is the results of the comparison
between established targets and their achievement.
In diagnostic mode measures (corrective feedback) allow the providers of care
(box 2) take the self-corrective actions within their processes of care when measures
are not achieving earlier planned levels. Similarly, organizational leaders responsible
for the implementation of PCC and/or HP may undertake corrective actions when the
functioning of PCC and/or HP is not on the track. In other words, when the quality and
costs of medical services deviate in the wrong direction. Organizational leaders may
‘keep the implementation of PCC and/or HP on track’ by many actions, for example,
they can adjust ‘contracting strategies’, ‘incentive system’ and ‘infrastructure’ or
technological support.
Through the measurement process per se, information system draw the attention
to subjects (areas) of measurement. This tends to influence the behaviour of the staff
and even patients when quantitative goals are set in the treatment plan. It is long
recognized that the measurement process itself invokes self-correction actions
(Flamholtz, 1996) and thus the measurement become themselves an incentive.
In the interactive mode, the information system facilitates the process of learning
how the whole idea of PCC and/or HP and five enablers functioning in a particular
setting. Here measures are used to ask questions, explore problems and challenge
assumptions. Whether the actions undertook to design each of the five enablers were
appropriate in a given environment? Maybe different measures should be used? Maybe
the strategy of PCC and/or HP implementation should be changed? By using the
‘information system’ interactively the PCC and/or HP actual general assumptions
could be confronted and modified.
Conclusions
The aim of the research was the clarification of definitions of the enablers the
theoretical analysis of mechanisms through which the WE-CARE Roadmap facilitate
the implementation of PCC and/or HP in medical organizations. This research was
important since some studies take for granted the effectiveness of the WE-CARE
Roadmap as an implementation tool (Lloyd et al., 2020). While there is neither
empirical nor theoretical research proving the effectiveness of the framework. The
important conclusion of the study is the necessity to more broadly define the
measurement. Not only restrain it to medical quality, but also include other areas such
as costs, and the functioning of the PCC and HP processes itself.
The study showed that enablers influence implementation of PCC and/or HP by
many mechanisms. Firstly the WE-CARE Roadmap indicates areas on which

129
organizational leaders should concentrate to eradicate or at least diminish barriers and
strengthen facilitators to create a friendly environment for the implementation.
Secondly, the five enablers working together may amplify its facilitating force. For
example, ‘technology’ and ‘information systems’ working together might create a
much stronger impact than each of them separately. Additionally, ‘technology’ and
‘information systems’ significantly enhanced the impact of ‘incentive systems’ through
the measurement process and the possibility to generate accurate reports and share
them among professionals and patients.
Hence from the analysis appears that WE-CARE Roadmap may be a valuable
tool supporting the implementation of PCC and/or HP in medical organizations and
consequently improve quality and contain costs of healthcare systems. It has to be
noticed, however, that this theoretical analysis can only be treated as an encouragement
for further research based on empirical studies of implementations of PCC and/or HP
in medical organizations where WE-CARE Roadmap was used as an implementation
tool.
Acknowledgements
This research was partly funded by COST Action CA15222 “European network
for cost containment and improved quality of care” (costcares.eu), 2016-2020 and the
National Science Centre, Poland (Grant Number: 2015/17/B/HS4/02747).
References
Alharbi, T.S., Carlström, E., Ekman, I. and Olsson, L.E. (2014), “Implementation of
person-centred care: management perspective”, Journal of Hospital
Administration, Vol. 3 No. 3, pp. 107-120.
Britten, N., Moore, L., Lydahl, D., Naldemirci, O., Elam, M. and Wolf, A. (2017),
“Elaboration of the Gothenburg model of person‐centred care”, Health
Expectations, Vol. 20 No. 3, pp. 407-418.
Cerasoli, C.P., Nicklin, J.M. and Ford, M.T. (2014), “Intrinsic motivation and extrinsic
incentives jointly predict performance: A 40-year meta-analysis”, Psychological
Bulletin, Vol. 140 No. 4, pp. 980-1008.
Covaleski, M.A., Dirsmith, M.W. and Michelman, J.E. (1993), “An institutional theory
perspective on the DRG framework, case-mix accounting systems and health-
care organizations”, Accounting, Organizations and Society, Vol. 18 No. 1, pp.
65-80.
Deci, E.L., Koestner, R. and Ryan, R.M. (1999), “A meta-analytic review of
experiments examining the effects of extrinsic rewards on intrinsic motivation”.
Psychological Bulletin, Vol. 125 No. 6, pp. 627-668.
Donabedian, A. (1966), “Evaluating the quality of medical care”, The Milbank
Memorial Fund Quarterly, Vol. 44 No. 3, pp. 166-206.
Donabedian, A. (2002), An Introduction to Quality Assurance in Health Care, Oxford
University Press, Oxford.
Ekman, I., Busse, R., van Ginneken, E., Van Hoof, C., van Ittersum, L., Klink, A.,
Kremer, J.A., Miraldo, M., Olauson, A. and De Raedt, W. (2016), “Health-care
improvements in a financially constrained environment”, The Lancet, Vol. 387
No. 10019, pp. 646-647.
Ekman, I., Swedberg, K., Taft, C., Lindseth, A., Norberg, A., Brink, E., Carlsson, J.,

130
Dahlin-Ivanoff, S., Johansson, I.-L., Kjellgren, K., Lidén, E., Öhlén, J., Olsson,
L.-E., Rosén, H., Rydmark, M. and Sunnerhagen, K.S. (2011), “Person-centered
care—ready for prime time”, European Journal of Cardiovascular Nursing, Vol.
10 No. 4, pp. 248-251.
Ekman, I., Wolf, A., Olsson, L. E., Taft, C., Dudas, K., Schaufelberger, M. and
Swedberg, K. (2012), “Effects of person-centred care in patients with chronic
heart failure: the PCC-HF study”, European Heart Journal, Vol. 33 No. 9, pp.
1112-1119.
Ferreira, A. and Otley, D. (2009), “The design and use of performance management
systems: An extended framework for analysis”, Management Accounting
Research, Vol. 20 No. 4, pp. 263-282.
Fisher, W.A., Fisher, J.D. and Harman, J. (2003), “The information-motivation-
behavioral skills model: A general social psychological approach to
understanding and promoting health behavior”, Social Psychological
Foundations of Health and Illness, Vol. 22, pp. 82-106.
Flamholtz, E. (1996), “Effective organizational control: a framework, applications, and
implications”, European Management Journal, Vol. 14, pp. 596-611.
Fors, A., Swedberg, K., Ulin, K., Wolf, A. and Ekman, I. (2017), “Effects of person-
centred care after an event of acute coronary syndrome: two-year follow-up of a
randomised controlled trial”, International Journal of Cardiology, Vol. 249, pp.
42-47.
Fors, A., Taft, C., Ulin, K. and Ekman, I. (2016), “Person-centred care improves self-
efficacy to control symptoms after acute coronary syndrome: a randomized
controlled trial”, European Journal of Cardiovascular Nursing, Vol. 15 No. 2,
pp. 186-194.
Fossey, J., Ballard, C., Juszczak, E., James, I., Alder, N., Jacoby, R. and Howard, R.
(2006), “Effect of enhanced psychosocial care on antipsychotic use in nursing
home residents with severe dementia: cluster randomised trial”, BMJ, Vol. 332
No. 7544, pp. 756-761.
Franco, L. M., Bennett, S. and Kanfer, R. (2002), “Health sector reform and public
sector health worker motivation: a conceptual framework”, Social Science &
Medicine, Vol. 54 No. 8, pp. 1255-1266.
Getzen, T.E. (1997), Health economics: fundamentals and flow of funds, John Wiley &
Sons, Hoboken.
Goncharuk, A.G. (2018), “Exploring a motivation of medical staff”, The International
Journal of Health Planning and Management, Vol. 33 No. 4, pp. 1013-1023.
Goncharuk, A.G., Lewandowski, R. and Cirella, G.T. (2020), “Motivators for medical
staff with a high gap in healthcare efficiency: Comparative research from Poland
and Ukraine”, The International Journal of Health Planning and Management,
In Press.
Guthrie, N., Bradlyn, A., Thompson, S.K., Yen, S., Haritatos, J., Dillon, F. and Cole,
S.W. (2015), “Development of an accelerometer-linked online intervention
system to promote physical activity in adolescents”, PloS One, Vol. 10 No. 5,
e0128639.
Kautsch, M. and Lewandowski, R. (2009), “Health Care Services Quality Certification
in Poland (System certyfikacji jakosci uslug w systemie ochrony zdrowia)”,
Polityka Społeczna, Vol. 3 No. 36, pp. 11-16.

131
Kowalski, I.M., Dwornik, M., Lewandowski, R., Pierożyński, B., Raistenskis, J.,
Krzych, Ł.J. and Kiebzak, W. (2015), “Early detection of idiopathic scoliosis–
analysis of three screening models”, Archives of Medical Science, Vol. 11 No. 5,
pp. 1058-1064.
Kriksciuniene, D., Sakalauskas, V. and Lewandowski, R. (2019a), “Evaluating the
interdependent effect for Likert scale items”, in Abramowicz, W., Corchuelo, R.
(Eds.), Business Information Systems Workshops, Springer International
Publishing, Cham, pp. 26-38.
Kriksciuniene, D., Sakalauskas, V. and Lewandowski, R.A. (2019b), “Process Mining
of Periodic Rating Scale Survey Data Using Analytic Hierarchy Process”, in:
Business Information Systems Workshops: BIS 2018 International Workshops,
Springer, Cham, pp. 86-95.
Levy, A., DeLeon, I.G., Martinez, C.K., Fernandez, N., Gage, N.A., Sigurdsson, S.O.
and Frank‐Crawford, M.A. (2017), “A quantitative review of overjustification
effects in persons with intellectual and developmental disabilities”, Journal of
Applied Behavior Analysis, Vol. 50 No. 2, pp. 206-221.
Lewandowski, R.A. (2010), “Rozwój zarządzania procesowego w polskich szpitalach”,
w: Wawak T.(red. nauk.). Komunikacja i jakość w zarządzaniu, Wydawnictwo
Uniwersytetu Jagiellońskiego, Kraków, pp. 159-169.
Lewandowski, R. (2013), “Perspective of control in the light of professional and
managerial role within health care organisations”, Przedsiębiorczość i
Zarządzanie, Vol. 14, pp. 215-227.
Lewandowski, R. (2009), “Zastosowanie Zrównoważonej Karty Wyników i Modelu
Doskonałości EFQM w publicznych organizacjach ochrony zdrowia”, Przegląd
Organizacji, No. 4, pp. 32–36.
Lewandowski, R. (2008), “Wykorzystanie Zrównoważonej Karty Wyników w
organizacjach ochrony zdrowia–studium przypadku”, Współczesne Zarządzanie,
No. 4, pp. 84-95.
Lewandowski, R. and Kowalski, I. (2008), “W poszukiwaniu obiektywnych metod
pomiaru jakości usług medycznych”, in Lewandowski, R. (Ed.), Współczesne
Wyzwania Strukturalne i Menedżerskie w Ochronie Zdrowia, Katedra
Organizacji i Zarządzania, Wydział Nauk Ekonomicznych Uniwersytetu
Warmińsko Mazurskiego, Olsztyn, pp. 253-266.
Lewandowski, R., Kożuch, A. and Sasak, J. (2018), Kontrola zarządcza w placówkach
ochrony zdrowia, Wolters Kluwer Polska, Warszawa.
Lewandowski, R., Lewandowski, J. and Czaprowski, D. (2020), “Opieka zorientowana
na osobę jako narzędzie poprawy jakości i powstrzymania wzrostu kosztów
opieki zdrowotnej”, Med Og Nauk Zdr, Vol. 26 No. 2, pp. 129-133.
Lewandowski, R.A. (2014), “Cost Control of Medical Care in Public Hospitals–a
Comparative Analysis”, International Journal of Contemporary Management,
Vol. 13 No. 1, pp. 125-136.
Lewandowski, R.A. and Sułkowska, J. (2017), “Levels of hybridity in healthcare
sector”, in Teczke, J., Buła, P. (Eds.), Management in the Time of Networks,
Cross-Cultural Activities and Flexible Organizations, Cracow University of
Economics, Cracow, pp. 147-162.
Lewandowski, R.A. and Sułkowski, Ł. (2018), „New Public Management and
Hybridity in Healthcare: The Solution or the Problem?”, in Savignon, A.B.,

132
Gnan, L., Hinna, A., Monteduro, F. (Eds.), Hybridity in the Governance and
Delivery of Public Services, Studies in Public and Non-Profit Governance,
Emerald Publishing Limited, Bingley, pp. 141-166.
Lloyd, H. M., Ekman, I., Rogers, H. L., Raposo, V., Melo, P., Marinkovic, V.D.,
Buttigieg, S.C., Srulovici, E., Lewandowski, R.A., Britten, N. (2020),
“Supporting Innovative Person-Centred Care in Financially Constrained
Environments: The WE CARE Exploratory Health Laboratory Evaluation
Strategy”, International Journal of Environmental Research and Public Health,
Vol. 17 No. 9, pp. 3050.
Malina, M.A. and Selto, F.H. (2001), “Communicating and controlling strategy: An
empirical study of the effectiveness of the balanced scorecard”, Journal of
Management Accounting Research, Vol. 13 No. 1, pp. 47-90.
Moore, L., Britten, N., Lydahl, D., Naldemirci, Ö., Elam, M. and Wolf, A. (2017),
“Barriers and facilitators to the implementation of person‐centred care in
different healthcare contexts”, Scandinavian Journal of Caring Sciences, Vol. 31
No. 4, pp. 662-673.
Mountford, N., Kessie, T., Quinlan, M., Maher, R., Smolders, R., Van Royen, P.,
Todorovic, I., Belani, H., Horak, H., Ljubi, I. and Lewandowski, R. (2016),
Connected Health in Europe: Where are we today?, University College, Dublin.
Ognjanović, I., Lewandowski, R., Šendelj, R., Krikščiūnienė, D. and Eraković, J.
(2020), “Model Driven Approach for Development of Person-Centred Care in
Stroke Rehabilitation”, Studies in Health Technology and Informatics, Vol. 272,
pp. 338-341.
Porter, M.E. (2010), “What Is Value in Health Care?”, New England Journal of
Medicine, Vol. 363 No. 26, pp. 2477-2481.
Porter, M.E. and Teisberg, E.O. (2006), Redefining health care: creating value-based
competition on results, Harvard Business Press, Brighton.
Ryan, R.M. and Deci, E.L. (2000), “Self-determination theory and the facilitation of
intrinsic motivation, social development, and well-being”, American
Psychologist, Vol. 55 No. 1, pp. 68-78.
Sanchez-Gordón, M.L., Colomo-Palacios, R. and Herranz, E. (2016), “Gamification
and human factors in quality management systems: mapping from octalysis
framework to ISO 10018”, in Kreiner, C., O’Connor, R.V., Poth, A., Messnarz,
R. (Eds.), European Conference on Software Process Improvement, Springer,
Cham, pp. 234-241.
Simons, R. (1994), Levers of control: How managers use innovative control systems to
drive strategic renewal, Harvard Business Press, Brighton.