The value of percutaneous cholangiography
5
GEORGE ET AL. : PERCUTANEOUS CHOLANGIOGRAPHY 779 in late obstruction. Secondly, since the fluid which is accumulating in the distended lumen of obstructed bowel has a cation composition identical to that of plasma, the concentration of serum electrolytes will not alter until late in obstruction. In addition, the extracellular compartment will be depleted rapidly and there will be an early reduction of the plasma volume, and shock will become manifest. Finally, the longer the obstruction persists the greater will the fluid losses become. A vicious circle will be set up in which the secretion of fluids will lead to further intestinal distension which, in turn, will aggravate secretion, and so on. The by-products of this vicious circle include excessive fluid losses and an increased risk of intestinal perforation. Treatment will be successful only if the distended gut is deflated by aspiration, the obstruction removed, and lost fluid replaced. Acknowledgements.-The experimental work described in this paper was conducted in the Wellcome Research Laboratories of the University of Glasgow and in the Departments of Surgery of the Western Infirmary, Glasgow, and of the Royal Infirmary, Cardiff. I wish to acknowledge my indebtedness to the heads of these departments, Professor W. L. Weipers, Professor Sir Charles Illingworth, and Professor A. P. M. Forrest, for their support, interest, and encouragement. I wish to thank several colleagues for their assis- tance in aspects of this work. Dr. G. F. Eglinton and Dr. G. Thomas, of the Departments of Chemistry in the University of Glasgow and University College, Cardiff, kindly allowed me to use their infra-red spectrophotometers for the determination of deuterium oxide. Dr. Michael Bluhm and Dr. James Valentine of the Regional Physics Department, Glasgow, and Mr. Glyn Owen of the South Wales Radiotherapy Service advised me on the radioactive aspects of the project. Part of this work was carried out with the aid of a grant from the Medical Research Council. REFERENCES AIRD, I. (1941), ‘Morbid !nfluences in Intestinal Obstruc- tion and Strangulation , Ann. Surg., 114, 385. ASHHURST, J. (1886), ?he International Encyclopaedia of Surgery, vol. 6. London: Macmillan. BERGLUND-LARSEN, U. (1956), ‘Determination of Small Amounts of D,O in Water, by Infra-red Spectroscopy’, Acta chem. scand., lo, 701. CANTOR, M. O., and REYNOLDS, R. P. (1957), Gastro- intestinal Obstruction. Baltimore: Williams and Wilkins. CLARKE, A. M., and SHIELDS, R. (1963), ‘The Role of the Intestine in Fluid and Electrolyte Conservation during Sodium Depletion’, Brit.3. Surg., 50,768. CODE, C. F., BASS, P., MCCLARY, G. B., lun., NEWNUM, R. L., and ORVIS, A. L. (1960), ‘Absorption of Wate;, Sodium and Potassium in Small Intestine of Dogs , Amer.3. Physiol., 199, 281. -- and MCINTIRE, F. C,. (1956), ‘Quantitative Deter- mination of Histamine , Meth. bzochem. Anal., 3, 49. DERBLOM, H., JOHANSSON, H., and NYLANDER, G. (1963), ‘Vascular Pattern of Intestinal Villi in the Obstructed Small Bowel of the Rat’, Surgery, 54, 780. DRUCKER, W. R., and WRIGHT, H. K. (1964), ‘Physiqlogy and Pathophysiology of Gastrointestinal Fluids , in Current Problems in Surgery. Chicago: Year Book Publishers. GAMBLE, J. L. (I~SI), Chemical Anatomy, Physiology and Pathology of Extracellular Fluid, 5th ed. Cambridge, Mass.: Harvard University Press. HARTWELL, J. A., and HOUGET, J. P. (1912), ‘Experimental Intestinal Obstruction in Dogs with Especial Reference to the Cause of Death and the Treatment by Large Amounts of Normal Saline Solution’, 3. Amer. med. Ass., 59, 82. PARKKULAINEN, K. V. (1962), ‘Simple Low Small Bowel Obstruction’, Acra chir. scand., suppl. 290. REDFERN, W. T., CLOSE, A. S., and ELLISON, E. H. (1961), ‘ Experimental Bowel Obstruction ’, Arch. Surg., Chicago, 83, 27. SHIELDS, R. (1964), ‘Surgical Aspects of the Absorption of Water and Electrolytes by the Intestine’, Monographs in the Surgical Sciences, I, I 19. -- and CODE, C. F. (1961), ‘Effect of Increascd Portal Pressure on Sorption of Water and Sodium from the Ileum of Dogs’, Amer. J. Physiol., 200, 775. -- and ELMSLIE, R. G. (1962), ‘The Effect of Aldo- sterone on Absorption of Water and ,Electrolytes from the Ileum and Colon of the Dog , Brir. 3. Surg., 50, 96. VEAI.L, N., and VETTER, H. (1958), Radioisotope Techniques in Clinical Research and Diagnosis. London : Butter- worths. VISSCHER, M. B., FETCHER, E. S., CARR, C. W., GREGOR, H. P., BUSHEY, M. S., and BARKER, D. E. (1944a), ‘Isotope Tracer Studies on Movement of Water and Ions between Intestinal Lumen and Blood’, Amer. J. Physiol., 142, 550. -- VARCO, R. H., CARR, C. W., DEAN, R. B., and ERICKSON. D. (1944b). ‘ Sodium Ion Movement between ~ _.. I. Intestinaf Lumen and Blood’, Ibid., 141, 488. 2nd ed. Springfield, Ill.: Thomas. Year Book Publishers. WANGENSTEEN, 0. H. (1947), Intestinal Obstructions, WELCH, C. E. (1958), Intestinal Obstruction. Chicago : THE VALUE OF PERCUTANEOUS CHOLANGIOGRAPHY BY PHYLLIS GEORGE, W. B. YOUNG, J. G. WALKER, AND SHEILA SHERLOCK DEPARTMENTS OF SURGERY, RADIOLOGY. AND MEDICINE, ROYAL FREE HOSPITAL, LONDON PERCUTANEOUS cholangiography was first introduced Seldinger, 1962; Glenn, Evans, Mujahed, and by Huard and Do-Xuan-Hop in 1937, and has Thorbjarnarson, 1962; Wiechel, 1964). This pro- been used increasingly in various modified forms by cedure is of great help to the surgeon in elucidating workers in this country and abroad (Kidd, 1956; the difficult case of jaundice, and in demonstrating Kaplan, Traitz, Mitchell, and Block, 1961 ; Shaldon, the pathological anatomy when obstruction is known Barber, and Young, 1962; Arner, Hagberg, and to be present.
-
Upload
phyllis-george -
Category
Documents
-
view
212 -
download
0
Transcript of The value of percutaneous cholangiography

GEORGE E T AL. : PERCUTANEOUS CHOLANGIOGRAPHY 779
in late obstruction. Secondly, since the fluid which is accumulating in the distended lumen of obstructed bowel has a cation composition identical to that of plasma, the concentration of serum electrolytes will not alter until late in obstruction. In addition, the extracellular compartment will be depleted rapidly and there will be an early reduction of the plasma volume, and shock will become manifest. Finally, the longer the obstruction persists the greater will the fluid losses become. A vicious circle will be set up in which the secretion of fluids will lead to further intestinal distension which, in turn, will aggravate secretion, and so on. The by-products of this vicious circle include excessive fluid losses and an increased risk of intestinal perforation. Treatment will be successful only if the distended gut is deflated by aspiration, the obstruction removed, and lost fluid replaced.
Acknowledgements.-The experimental work described in this paper was conducted in the Wellcome Research Laboratories of the University of Glasgow and in the Departments of Surgery of the Western Infirmary, Glasgow, and of the Royal Infirmary, Cardiff. I wish to acknowledge my indebtedness to the heads of these departments, Professor W. L. Weipers, Professor Sir Charles Illingworth, and Professor A. P. M. Forrest, for their support, interest, and encouragement.
I wish to thank several colleagues for their assis- tance in aspects of this work. Dr. G. F. Eglinton and Dr. G. Thomas, of the Departments of Chemistry in the University of Glasgow and University College, Cardiff, kindly allowed me to use their infra-red spectrophotometers for the determination of deuterium oxide. Dr. Michael Bluhm and Dr. James Valentine of the Regional Physics Department, Glasgow, and Mr. Glyn Owen of the South Wales Radiotherapy Service advised me on the radioactive aspects of the project.
Part of this work was carried out with the aid of a grant from the Medical Research Council.
REFERENCES AIRD, I. (1941), ‘Morbid !nfluences in Intestinal Obstruc-
tion and Strangulation , Ann. Surg., 114, 385. ASHHURST, J. (1886), ?he International Encyclopaedia of
Surgery, vol. 6. London: Macmillan. BERGLUND-LARSEN, U. (1956), ‘Determination of Small
Amounts of D,O in Water, by Infra-red Spectroscopy’, Acta chem. scand., lo, 701.
CANTOR, M. O., and REYNOLDS, R. P. (1957), Gastro- intestinal Obstruction. Baltimore: Williams and Wilkins.
CLARKE, A. M., and SHIELDS, R. (1963), ‘The Role of the Intestine in Fluid and Electrolyte Conservation during Sodium Depletion’, Brit .3. Surg., 50,768.
CODE, C. F., BASS, P., MCCLARY, G. B., lun., NEWNUM, R. L., and ORVIS, A. L. (1960), ‘Absorption of Wate;, Sodium and Potassium in Small Intestine of Dogs , Amer.3. Physiol., 199, 281. -- and MCINTIRE, F. C,. (1956), ‘Quantitative Deter-
mination of Histamine , Meth. bzochem. Anal., 3 , 49.
DERBLOM, H., JOHANSSON, H., and NYLANDER, G. (1963), ‘Vascular Pattern of Intestinal Villi in the Obstructed Small Bowel of the Rat’, Surgery, 54, 780.
DRUCKER, W. R., and WRIGHT, H. K. (1964), ‘Physiqlogy and Pathophysiology of Gastrointestinal Fluids , in Current Problems in Surgery. Chicago: Year Book Publishers.
GAMBLE, J. L. ( I ~ S I ) , Chemical Anatomy, Physiology and Pathology of Extracellular Fluid, 5th ed. Cambridge, Mass.: Harvard University Press.
HARTWELL, J. A., and HOUGET, J. P. (1912), ‘Experimental Intestinal Obstruction in Dogs with Especial Reference to the Cause of Death and the Treatment by Large Amounts of Normal Saline Solution’, 3. Amer. med. Ass., 59, 82.
PARKKULAINEN, K. V. (1962), ‘Simple Low Small Bowel Obstruction’, Acra chir. scand., suppl. 290.
REDFERN, W. T., CLOSE, A. S . , and ELLISON, E. H. (1961), ‘ Experimental Bowel Obstruction ’, Arch. Surg., Chicago, 83, 27.
SHIELDS, R. (1964), ‘Surgical Aspects of the Absorption of Water and Electrolytes by the Intestine’, Monographs in the Surgical Sciences, I, I 19. -- and CODE, C. F. (1961), ‘Effect of Increascd Portal Pressure on Sorption of Water and Sodium from the Ileum of Dogs’, Amer. J . Physiol., 200, 775. -- and ELMSLIE, R. G. (1962), ‘The Effect of Aldo- sterone on Absorption of Water and ,Electrolytes from the Ileum and Colon of the Dog , Brir. 3. Surg., 50, 96.
VEAI.L, N., and VETTER, H. (1958), Radioisotope Techniques in Clinical Research and Diagnosis. London : Butter- worths.
VISSCHER, M. B., FETCHER, E. S. , CARR, C. W., GREGOR, H. P., BUSHEY, M. S . , and BARKER, D. E. (1944a), ‘Isotope Tracer Studies on Movement of Water and Ions between Intestinal Lumen and Blood’, Amer. J . Physiol., 142, 550.
-- VARCO, R. H., CARR, C. W., DEAN, R. B., and ERICKSON. D. (1944b). ‘ Sodium Ion Movement between
~ _ . . I. Intestinaf Lumen and Blood’, Ibid., 141, 488.
2nd ed. Springfield, Ill.: Thomas.
Year Book Publishers.
WANGENSTEEN, 0. H. (1947), Intestinal Obstructions,
WELCH, C. E. (1958), Intestinal Obstruction. Chicago :
THE VALUE OF PERCUTANEOUS CHOLANGIOGRAPHY BY PHYLLIS GEORGE, W. B. YOUNG, J. G. WALKER, AND SHEILA SHERLOCK
DEPARTMENTS OF SURGERY, RADIOLOGY. AND MEDICINE, ROYAL FREE HOSPITAL, LONDON
PERCUTANEOUS cholangiography was first introduced Seldinger, 1962; Glenn, Evans, Mujahed, and by Huard and Do-Xuan-Hop in 1937, and has Thorbjarnarson, 1962; Wiechel, 1964). This pro- been used increasingly in various modified forms by cedure is of great help to the surgeon in elucidating workers in this country and abroad (Kidd, 1956; the difficult case of jaundice, and in demonstrating Kaplan, Traitz, Mitchell, and Block, 1961 ; Shaldon, the pathological anatomy when obstruction is known Barber, and Young, 1962; Arner, Hagberg, and to be present.

780 BRIT. J. SURG., 1965, Vol. 52, No. 10, OCTOBER
INDICATIONS investigation, are to have a laparotomy. Absence of This method of investigation is indicated in patients clinical jaundice, as in intermittent cholangitis where
with obscure jaundice of more than I month's dura- the serum bilirubin may be less than 2 mg. per cent, tion, where it is impossible to distinguish between does not preclude use of the method. hepatocellular disease and intrahepatic or extra- The approach is either from the anterior aspect, hepatic obstruction of the main bile-ducts. I t is also just to the right of the xiphisternum, or laterally of value where jaundice, or attacks of cholangitis, through an intercostal space. The anterior approach have occurred after any operation on the gall-bladder, is used in the majority of cases as we feel it preferable
to be able to examine the site of liver puncture if operation follows. Where there is dense scar tissue from previous operations, the lateral approach may be advantageous.
The method of intubation used is that described by Shaldon and others (1962). A flexible polyethylene tube (internal diameter 1.5 mm.) is drawn over a 20-gauge steel needle approximately 15 cm. long (Fig. I). This is introduced directly into the liver, and the needle is then withdrawn, leaving the tube in place. A tap adaptor and a syringe containing normal saline are then attached and suction is applied to the polyethylene tubing as it is slowly
cent hypaque (usually 20-40 ml.) is injected, under I ~ c . I.-iYeedle and polyethylene tubing used for percutaneous
Fholangiography (Shaldon and others, 1962). (Reproduced from withdrawn. Once bile is aspirated, sufficient 45 per Gusiroenierolo~,y '. )
A B FIG. z.-Cnse I . A, Choledochus cyst. The right hepatic duct system only has filled and is moderately dilated. N o contrast medium has entered the duodenum. 6, The left hepatic duct system has now been filled by separate cannulation and is also moderately dilated.
bile-ducts, or upper abdominal organs, where there is the possibility of recurrent or residual stones, or damage to part of the biliary tree. Finally, the biliary tree can be visualized in patients with known obstruc- tive jaundice, where the exact site, nature, and extent of the lesion are in doubt.
TECHNIQUE Before undertaking the investigation it is important
that the prothrombin time and platelet count be estimated and the former corrected, where necessary, by the administration of vitamin K. Also I ml. of the relevant contrast medium should be given intra- venously to test for any adverse reaction. The investigation is carried out under screen control in the X-ray department. General anaesthesia is used for children, unduly nervous patients, and often also in those patients who, irrespective of the result of the
screen control, to obtain optimum filling of the duct system. The use of a flexible tube allows the patient to move, cough, or breathe, or be repositioned without risk of damage to the liver.
After intubation of a duct, a specimen of bile is obtained for culture as a coliform infection is fre- quently present. T o diminish the risk of septicaemia from this source, the patients are given broad- spectrum antibiotic cover. If a dilated duct is entered, the tube is left in situ after completion of the radio- graphic examination to provide drainage and diminish the risk of biliary leakage.
Experience has shown that if a duct has not been entered after five attempts the biliary system is unlikely to be dilated. However, if the patient is known to have a main-duct obstruction, such as a stricture, then it is justifiable to attempt further punctures in order to provide the surgeon with vital

GEORGE E T AL. : PERCUTANEOUS CHOLANGIOGRAPHY
creas or arnpulia of Vater
Carcinoma of bile- ducts
Biliary stricture Biliary calculi Liver metastases
information. In cases where the initial cannulation has demonstrated only part of the main-duct system, it is worth-while performing a second puncture directed towards the unfilled part of the biliary tree.
Case 1.-In this patient cholangiograms (Fig. 2 ) were obtained by intubation of the right and left hepatic duets separately. The films revealed a choledochus cyst, completely obstructed at the site of a previous anastomosis to the duodenum. At operation calculi completely filling the upper part of the cyst and extending into right and left hepatic ducts were found to have been responsible for the incomplete filling at the first puncture.
A decision upon the need for operation is made on completion of the procedure. If the investigation was undertaken to exclude a main-duct lesion in a case of obscure jaundice, an unsuccessful cholangiogram is usually followed by a period of further observation. The possibility of hepatocellular disease precludes operation because of the risk of an exacerbation of the disease or even liver failure which may ensue in these cases (Harville and Summerskill, 1963). There is no indication for operation in cases where a non- obstructed biliary tree has been demonstrated, but these patients require careful observation for signs of haemorrhage or peritonitis. No evidence of these complications was found in the 3 cases in our series who were managed in this way.
When a dilated biliary radicle is entered above an obstructive lesion operation within 4 hours to obviate the risk of biliary leakage is mandatory. In known cases of obstruction the procedure is undertaken to provide the surgeon with information beforehand, and therefore operation follows irrespective of the result. In negative cases an operative cholangiogram is indicated.
COMPLICATIONS At operation a little haemorrhage was often seen
at the site of liver puncture. In 2 cases there was a larger collection of blood, about 500 ml. being present in the peritoneal cavity in each case, but active bleeding had stopped. Occasional instances of haemorrhage have been reported in other series (Nurick, Patey, and Whiteside, 1953; Arner and others, 1962; Glenn and others, 1962; Wiechel, 1964). Biliary peritonitis was not encountered in our patients, although this complication also has been recorded (Kaplan and others, 1961; Arner and others, 1962; Glenn and others, 1962). In our series other organs, including the gall-bladder, stomach, and large bowel, were each, on occasion, inadvertently punctured. In no case was there any untoward effect and the surgeon was unable to identify the site of puncture at operation. There were no deaths occurring as a result of the procedure.
In earlier series occasional deaths from this investigation were reported and it is felt that the use of a flexible tube, the correction of any abnormal clotting mechanism, and the obligatory operation, covered by a broad-spectrum antibiotic, in all cases where a dilated duct system is cannulated, have contributed to the absence of mortality in the present series.
RESULTS AND DISCUSSION Percutaneous cholangiography was attempted in
137 patients with success in 97 instances (Table I ) . 5 1
28 0
23 5 33 9
8 3 2 1
78 I
In 94 of these an obstructive lesion was demonstrated and the biliary tree showed dilatation. An undilated normal biliary tree was demonstrated in 3 patients, where the bile-ducts in 2 and the gall-bladder in a third had been fortuitously punctured. The diagnoses in these patients finally proved to be primary biliary cirrhosis in 2 patients and prolonged cholestatic drug jaundice in the third. Laparotomy was performed in the 94 patients where an obstructive lesion was demonstrated, but not in the 3 with an undilated tree.
A major bile-duct could not be cannulated in 17 patients with varying types of hepatocellular disease (primary biliary cirrhosis, atypical hepatitis, or drug
Table I.-ANALYSIS OF RESULTS OF PERCUTANEOUS CHOLANGIOGRAPHY
I I
Carcinoma of Dan- I I 28
28 A2
Hepatocellular jaun- dice
Cholangitis with no biliary dilatation or obstruction
Riliary atresia
Total
jaundice) and the diagnosis was subsequently con- firmed by the clinical course and biopsy in every instance. Cannulation was also unsuccessful in 4 patients with cholangitis in the absence of obstruction and in a child with atresia. The diagnosis was confirmed in all 4 at laparotomy.
In contrast, no cholangiogram was obtained in 18 patients although biliary pathology was later shown to be present. Surprisingly, there was no biliary dilatation in 3 cases of biliary stricture and 2 of biliary calculi. Sclerosing cholangitis with biliary irregu- larity and narrowing was found on operative chol- angiography in 4 other cases (included in the group ‘biliary stricture’, Table I). In 4 patients there was extensive growth in the liver (3 bile-duct carcinoma, I liver metastases) which had prevented location of an enlarged bile-duct. In 3 patients studied early in the series only 2 or 3 attempts were made and success might have been obtained had more been undertaken. An extremely hard liver due to congenital fibrosis prevented the satisfactory introduction of the catheter in a young patient with biliary stricture, and in another ‘ failed’ case operation revealed the biliary tree to be packed with stones.
Transhepatic percutaneous cholangiography may be of great value in cases of obscure jaundice by demonstrating an obstructive lesion. For example, carcinoma of the hepatic ducts is sometimes missed at laparotomy if the lesion is within the liver substance and no operative cholangiogram is performed.
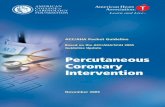
Case z-An So-year-old patient (Fig. 3), with a history of two previous negative laparotomies, had received a course of steroids and was still jaundiced.
78 2 BRIT. J. SURG., 1965, Vol. 52, No. 10, OCTOBER
Percutaneous cholangiography revealed a carcinoma at the junction of the right and left hepatic ducts which proved at operation to be too extensive for removal. By following the track outlined in the radiograph, it was possible to dilate the narrowed area, and pass a polythene tube through the growth to relieve the jaundice. The patient is well z years later.
T h e necessity of an operation may be avoided if the cholangiogram shows a normal biliary tree, or if it i s unsuccessful due to the absence of dilatation.
Case 3.-A man had undergone a negative laparotomy 4 months previously and was still jaundiced. As a result of the normal cholangiogram (FG. 4) he was treated conservatively as a case of drug jaundice.
Vital information can be obtained in cases of biliary stricture where exact knowledge of the anatomy allows
FIG. 3.-Case 2. Carcinoma of the hepatic ducts. There is gross dilatation of the right duct system. The left main duct has not tilled because of the extensive lesion at the junction of right and left hepatic ducts. The common hepatic and bile-ducts, the cystic duct, and the gall-bladder are undated .
PIG. S.--Care 4. Stricture of the lower end of the common bile-duct. T h e gall-bladder and main pancreatic duct are also visualized.
the surgeon to proceed directly to the area of the stricture. In patients where the stricture lies within the liver it is valuable to know the depth and direction of available dilated duct.
Case q.--In this patient with a stricture at the lower end of the common bile-duct (Fig. 5 ) , it was relatively easy to follow the upper border of the duodenum, locate the lesion, and perform a dilatation and sphincterotomy.
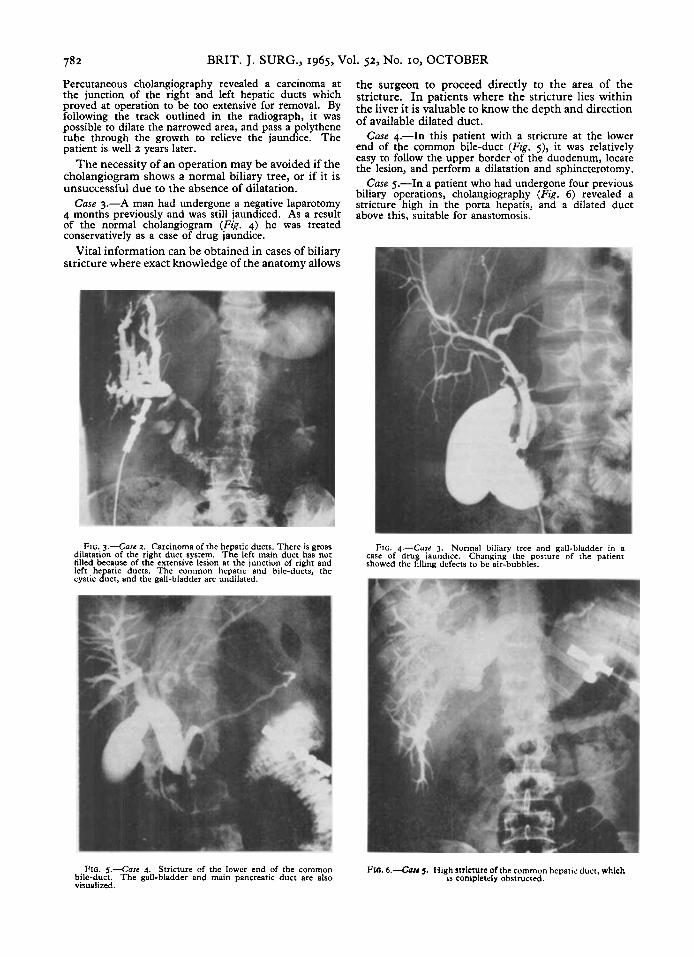
Case 5.-In a patient who had undergone four previous biliary operations, cholangiography (Fig. 6) revealed a stricture high in the porta hepatis, and a dilated duct above this, suitable for anastomosis.
FIG. 4.-Case 3. Normal biliary tree and gall-bladder in a case of drua .jaundice. Changing the posture of the patient showed the llina defects to be air-bubbles.
Pro. 6.-Cau 3. High stricture of the common hepails duct, which Is Completely obstructed.

GEORGE ET AL. : PERCUTANEOUS CHOLANGIOGRAPHY 783
The visualization of the biliary tree by percutaneous described. T h e indications for the procedure and cholangiography may augment the clinical diagnosis results obtained in 137 patients studied by this in cases of obstructive jaundice and allow the planning technique are discussed. No serious complications of the operation in advance. were encountered and the examination frequently
Case 6.-In a 73-year-old woman, diagnosed as having provided information obtainable by no other means carcinoma of the pancreas on barium-meal examination, of investigation. A number of patients with hepato- the investigation showed a grossly dilated biliary tree cellular jaundice were spared an unnecessary opera- with multiple stones in the common bile- and hepatic tion. When surgery was indicated, the site of
FIG. 7 . 4 a s e 6 . Multi le stones in the common hepatic and bile-ducts. An irregular &ling defect (indicated by the arrow) was found at operation tu be caused by a carcinoma of the gall-bladder.
ducts. There was also a filling defect of the common hepatic duct, found later to be caused by a carcinoma of che gall-bladder (Fig. 7).
Carcinoma of the pancreas can usually be diagnosed without recourse to a percutaneous cholangiogram, but the investigation may be of value.
Case 7.-A man with obstructive jaundice gave a history of a negative laparotomy, and was still icteric. He was loath to undergo another operation, but when it was explained to him that it would be possible to tell by means of a radiograph if his condition would benefit from further surgery he readily agreed. The radiograph showed a typical picture of carcinoma of the pancreas (Fig. 8). The diagnosis was confirmed at operation and his jaundice relieved.
I t will be seen therefore that although the procedure will provide valuable information in the majority of patients with an obstructed biliary tree, its use in the differential diagnosis of jaundice must be in conjunc- tion with the combined clinical picture and bio- chemical results. Thus, i n the present series, 18 jaundiced patients with obstructive lesions had negative cholangiograms for the reasons outlined above. Percutaneous cholangiograms alone should not be relied upon in making a decision whether to operate in a jaundiced patient.
SUMMARY Cholangiography by means of a polyethylene
catheter introduced percutaneously into the liver is
FIG. 8 . 4 a s e 7. Carcinoma of head of pancreas involving the common bile-duct. and causing complete biliary obstruction.
exploration and probable details of the operation to be carried out could be decided beforehand, thus reducing the operating time to the advantage of both patient and surgeon.
REFERENCES ARNER, O., HAGBERG, S., and SELDINGER, S. I. (1962),
‘ Percutaneous Transhepatic Cholangiography. Puncture of Dilated and Non-dilated Bile Ducts under Roentgen Television Control’, Surgery, 52, 561.
GLENN, F., EVANS, J. A., MUJAHED, Z., and THORRJARN- ARSON, B. (1962), ‘Percutaneous Transhepatic Cholan- giography’, Ann. Surg., 156, 451.
HARVILLE, D. D., and SUMMERSRILL, W. H. J. (1963)~ ‘Surgery in Acute Hepatitis. Causes and Effects’, 3. Amer. med. ASS. , 184, 257.
HUARD, P., and DO-XUAN-HOP (1937), ‘La Ponction Transhepatique des Canaux Biliaires ’, Bull. SOC. mid- chir. Indoch., 15, 1090.
KAPLAN, A. A., TRAITZ, J. J., MITCHELL, S. D., and BLOCK, A. L. (1961), ‘Percutaneous Transhepatic Cholangiography ’, Ann. inzern. Med., 54, 856.
KIDD, H. A. (1956), ‘Percutaneous Transhepatic Cholan- giography ’, Arch. Surg., Chicago, 72, 262.
NURICK, A. W., PATEY, D. H., and WHITESIDE, C. G. (1953), ‘ Percutaneous Transhepatic Cholangiography in Diagnosis of Obstructive Jaundice’, Brit. 3. Surg., 41, ..- LI ‘
SHALDON, S., BARBER, K. M., and YOUNG, W. B. (1962)~ ‘ Percutaneous Transhepatic Cholangiography ’, Gastro- enterology, 42, 371.
WIECHEL, K.-L. (1964), ‘ Percutaneous Transhepatic Cholangiography ’, Arta chir. scand., suppl. 330.