The Value of a Chest X-Ray in Diagnosing Pneumonia in SIRS Patients Lacking Respiratory Symptoms in...
1
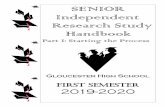
The Value of a Chest X-Ray in Diagnosing Pneumonia in SIRS Patients Lacking Respiratory Symptoms in York Hospital’s Emergency Department Michelle Lynch Department of Biological Sciences, York College of Pennsylvania Results Methods Objectives Conclusion To determine the prevalence of pneumonia and the predictive properties of a chest x-ray in the evaluation of SIRS for patients with and without respiratory symptoms Hypothesis: Patients with SIRS criteria and no respiratory symptoms have a lower prevalence of pneumonia and do not require a chest x-ray on initial work up A history and physical was more effective in diagnosing pneumonia than a chest x-ray (sensitivity 100% and 65% respectively) None of the patients with SIRS lacking respiratory symptoms were diagnosed with pneumonia and Chest X-rays were not necessary in their diagnosis Combined with supportive findings from additional studies, chest x- rays can be used more judiciously to limit radiation exposure and reduce medical costs Systemic Inflammatory Response Syndrome (SIRS ) • Bodily response caused by a wide variety of issues • Related to sepsis, which is SIRS specifically caused by infection • Requires two or more of the following symptoms: * Tachycardia [>90 bpm] * Hypo/Hyperthermia [<96.0 °F or >100.4 °F ] * High Respiratory Rate [>20 breaths/minute] * Low/High WBC [<4,000/μL or >12,000/μL] Pneumonia • Infection in one or more lobes of the lungs • Symptoms include: cough, fever, shortness of breath • 5.6 million cases per year in U.S., 1/5 requiring hospitalization • Leading cause of death by infectious disease Chest X-Ray • Required in the diagnosis of pneumonia • Infection infiltrates are seen as white opaque patches • Benefits: clear indicator of infiltrates • Drawbacks: costly ($50-$400), radiation exposure Acknowledgements Thank you to Dr. Kochert, Dr. Ryles, Dr. Lalani, and Mrs. Stahlman from York Hospital and Dr. Kaltreider and Dr. Boehmler from York College Radiologyinfo.org • Retroactive chart review of York Hospital Emergency Department patients receiving a chest x-ray in Dec. 2010 • Those with at least two SIRS criteria were included • Pediatric and DNR/comfort care only patients and those with known pneumonia or a chronic abnormal chest x-ray were excluded • Charts were reviewed to determine: * Presence or absence of respiratory symptoms at ED presentation Respiratory Symptom (RS) : Dyspnea, Tachypnea, Cough, Chest Pain, Hypoxia, and Focal Lung Findings * Radiology interpretation of ED chest x- ray * Discharge Diagnosis (Gold standard for pneumonia diagnosis ) • Fisher’s exact test and descriptive statistics were used 1053 charts reviewed 23 (14.9%) with Pneumonia 0 (0%) with Pneumonia 39 with no RS 154 with one or more RS 193 charts included 860 Excluded Introducti on History and Physical Chest X-Ray Sensitivity 100% (95% CI: 82- 100%) 65% (95% CI: 43- 83%) Specificity 23% (95% CI: 17- 30%) 86% (95% CI: 80- 91%) + Likelihood Ratio 1.3 (95% CI: 1.2- 1.4) 4.6 (95% CI: 2.9- 7.4) - Likelihood Ratio 0 (95% CI: 0-0.8) 0.4 (95% CI: 0.2- 0.7) http://emedicine.medscape.com/article/168402-overview http://www.wellspan.org/body.cfm?id=91 Table 1. Effectiveness of methods in the diagnosis of pneu References Bone, R., et al. 1992. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 101:1644-55. Lutfiyya, M., et al. 2006. Diagnosis and treatment of community- acquired pneumonia. Am. Family Physician 73:442-450. Verma, V., et al. 2011. The utility of routine admission chest X-ray films on patient care. European Journal of Internal Medicine 22:286– 288.
-
Upload
linda-wright -
Category
Documents
-
view
216 -
download
3
Transcript of The Value of a Chest X-Ray in Diagnosing Pneumonia in SIRS Patients Lacking Respiratory Symptoms in...

The Value of a Chest X-Ray in Diagnosing Pneumonia in SIRS Patients Lacking Respiratory Symptoms in York Hospital’s Emergency Department
Michelle Lynch Department of Biological Sciences, York College of Pennsylvania
ResultsMethods
Objectives
Conclusion
To determine the prevalence of pneumonia and the predictive properties of a chest x-ray in the evaluation of SIRS for patients with and without respiratory symptoms
Hypothesis: Patients with SIRS criteria and no respiratory symptoms have a lower prevalence of pneumonia and do not require a chest x-ray on initial work up
A history and physical was more effective in diagnosing pneumonia than a chest x-ray (sensitivity 100% and 65% respectively)
None of the patients with SIRS lacking respiratory symptoms were diagnosed with pneumonia and Chest X-rays were not necessary in their diagnosis
Combined with supportive findings from additional studies, chest x-rays can be used more judiciously to limit radiation exposure and reduce medical costs
Systemic Inflammatory Response Syndrome (SIRS)•Bodily response caused by a wide variety of issues•Related to sepsis, which is SIRS specifically caused by infection•Requires two or more of the following symptoms:
* Tachycardia [>90 bpm]* Hypo/Hyperthermia [<96.0 °F or >100.4 °F ]* High Respiratory Rate [>20 breaths/minute]* Low/High WBC [<4,000/μL or >12,000/μL]
Pneumonia •Infection in one or more lobes of the lungs•Symptoms include: cough, fever, shortness of breath•5.6 million cases per year in U.S., 1/5 requiring hospitalization•Leading cause of death by infectious disease
Chest X-Ray•Required in the diagnosis of pneumonia•Infection infiltrates are seen as white opaque patches•Benefits: clear indicator of infiltrates•Drawbacks: costly ($50-$400), radiation exposure
AcknowledgementsThank you to Dr. Kochert, Dr. Ryles, Dr. Lalani, and Mrs. Stahlman from York Hospital
and Dr. Kaltreider and Dr. Boehmler from York College
Radiologyinfo.org
• Retroactive chart review of York Hospital Emergency Department patients receiving a chest x-ray in Dec. 2010
• Those with at least two SIRS criteria were included
• Pediatric and DNR/comfort care only patients and those with known pneumonia or a chronic abnormal chest x-ray were excluded
• Charts were reviewed to determine:* Presence or absence of respiratory symptoms at ED
presentation Respiratory Symptom (RS): Dyspnea, Tachypnea, Cough, Chest Pain, Hypoxia, and Focal Lung Findings
* Radiology interpretation of ED chest x-ray* Discharge Diagnosis (Gold standard for pneumonia
diagnosis )
• Fisher’s exact test and descriptive statistics were used
1053 charts reviewed
23 (14.9%) with Pneumonia
0 (0%) with Pneumonia
39 with no RS154 with one or more RS
193 charts included
860 Excluded
Introduction
History and Physical Chest X-RaySensitivity 100%
(95% CI: 82-100%)65% (95% CI: 43-83%)
Specificity 23% (95% CI: 17-30%)
86% (95% CI: 80-91%)
+ Likelihood Ratio 1.3 (95% CI: 1.2-1.4)
4.6 (95% CI: 2.9-7.4)
- Likelihood Ratio 0(95% CI: 0-0.8)
0.4 (95% CI: 0.2-0.7)
http://emedicine.medscape.com/article/168402-overview
http://www.wellspan.org/body.cfm?id=91
Table 1. Effectiveness of methods in the diagnosis of pneumonia
ReferencesBone, R., et al. 1992. American College of Chest Physicians/Society of Critical Care Medicine Consensus
Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 101:1644-55.
Lutfiyya, M., et al. 2006. Diagnosis and treatment of community-acquired pneumonia. Am. Family Physician 73:442-450.
Verma, V., et al. 2011. The utility of routine admission chest X-ray films on patient care. European Journal of Internal Medicine 22:286–288.