The use of adaptive radiation therapy to reduce setup error: a prospective clinical study
6
PII S0360-3016(97)00567-1 ● Physics Contribution THE USE OF ADAPTIVE RADIATION THERAPY TO REDUCE SETUP ERROR: A PROSPECTIVE CLINICAL STUDY DI YAN, D.SC., ELLEN ZIAJA, M.D., DAVID JAFFRAY,PH.D., JOHN WONG,PH.D., DONALD BRABBINS, M.D., FRANK VICINI, M.D. AND ALVARO MARTINEZ, M.D., F.A.C.R. Department of Radiation Oncology, William Beaumont Hospital, Royal Oak, MI Purpose: Adaptive Radiation Therapy (ART) is a feedback treatment process that optimizes a patient’s treatment according to the patient specific information measured during the course of treatment. Utilizing an electronic portal imaging device (EPID) and a computer-controlled multileaf collimator (MLC), the ART process is currently being implemented in our clinic to improve the treatment accuracy by compensating for the treatment setup error. A prospective study was conducted to evaluate the feasibility and efficacy of the ART process for clinical use. Methods and Materials: The prospective study included 20 patients who underwent conventional radiotherapy on a linear accelerator equipped with an EPID and a MLC. No specific changes were made in the routine clinical procedures except daily portal images were obtained for each treatment field. Two-dimensional setup error for each treatment field was then measured offline using a software tool. The measured setup errors from initial treatment days were used to predict the systematic and random setup errors for each treatment field. An adjustment decision was made if the predicted systematic error was larger than or equal to 2 mm. Furthermore, the treatment field was extended if the predicted random setup error could not be effectively compensated by the predefined treatment setup margin. Instead of the conventional approach of patient repositioning, setup adjust- ment was implemented by reshaping the MLC field. The entire process from measuring setup error to reshaping the MLC field was performed offline through a computer network. After completion of a patient’s treatment, the systematic and random setup errors after adjustment were compared with those predicted prior to the adjustment. The accuracy of the adjustment, and the reliability and stability of the process were analyzed. Results: Treatment fields of 13 patients were modified to correct for systematic errors. The mean systematic error was 4 mm with a range of 2 to 7 mm before adjustment. It was reduced to 0.5 mm with a range of 0.2 to 1.4 mm after adjustment. There was no significant difference in random setup errors before and after adjustment. The ART process was found to be stable, as more than 95% of patient specific setup margins were predictable within 1 mm using the first four to nine fractions of treatment, confirming the feasibility of treatment plan reoptimi- zation with the ART process. Conclusions: The prospective study demonstrates that the ART process can be effectively implemented in routine clinical practice to improve treatment accuracy. This process is also ready to be further extended to reoptimize the treatment plan by incorporating the predicted patient specific setup variation. © 1998 Elsevier Science Inc. Adaptive radiation therapy, Treatment setup error, Treatment plan modification. INTRODUCTION Adaptive radiation therapy (ART) has been introduced to minimize the detrimental effects of treatment variation on the individual patient (8). It has been primarily designed to reoptimize the individual treatment plan and dose delivery according to the time course of treatment variation charac- terized during the course of radiation treatment. A retro- spective study (9) has demonstrated that the time course of treatment setup variation can be characterized early on during the treatment process, and compensated for by ad- justing the treatment field shape and prescription dose. In the retrospective study, treatment managed in the feedback process of ART was simulated by using the initial treat- ment-planning CT and daily portal images. It was assumed that during the course of treatment, the position and shape of the treatment field could be effectively reconformed using a MLC. However, these assumptions have not yet been con- firmed. The feasibility and reliability of the ART process in the routine clinical environment have not been established. In an initial effort to implement the ART process in our Presented at the 38th Annual ASTRO Meeting, Los Angeles, CA, October, 1996 Reprint request to: Di Yan, D.Sc., Department of Radiation Oncology, William Beaumont Hospital, 3601 W. Thirteen Mile Rd., Royal Oak, MI 48073-6769. Acknowledgements—The authors thank the following for their valuable assistance in this clinical study: John Robertson, M.D., Peter Chen, M.D., Carla Cook, M.D., Gary Gustafson, M.D., and Jannifer Stromberg, M.D. This work was supported in part by NCI Grants #CA71785 and #CA66074. Accepted for publication 3 July 1997. Int. J. Radiation Oncology Biol. Phys., Vol. 41, No. 3, pp. 715–720, 1998 Copyright © 1998 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/98 $19.00 1 .00 715
Transcript of The use of adaptive radiation therapy to reduce setup error: a prospective clinical study

PII S0360-3016(97)00567-1
● Physics Contribution
THE USE OF ADAPTIVE RADIATION THERAPY TO REDUCE SETUPERROR: A PROSPECTIVE CLINICAL STUDY
DI YAN, D.SC., ELLEN ZIAJA, M.D., DAVID JAFFRAY, PH.D., JOHN WONG, PH.D.,DONALD BRABBINS, M.D., FRANK VICINI, M.D. AND ALVARO MARTINEZ, M.D., F.A.C.R.
Department of Radiation Oncology, William Beaumont Hospital, Royal Oak, MI
Purpose: Adaptive Radiation Therapy (ART) is a feedback treatment process that optimizes a patient’streatment according to the patient specific information measured during the course of treatment. Utilizing anelectronic portal imaging device (EPID) and a computer-controlled multileaf collimator (MLC), the ART processis currently being implemented in our clinic to improve the treatment accuracy by compensating for thetreatment setup error. A prospective study was conducted to evaluate the feasibility and efficacy of the ARTprocess for clinical use.Methods and Materials: The prospective study included 20 patients who underwent conventional radiotherapyon a linear accelerator equipped with an EPID and a MLC. No specific changes were made in the routine clinicalprocedures except daily portal images were obtained for each treatment field. Two-dimensional setup error foreach treatment field was then measured offline using a software tool. The measured setup errors from initialtreatment days were used to predict the systematic and random setup errors for each treatment field. Anadjustment decision was made if the predicted systematic error was larger than or equal to 2 mm. Furthermore,the treatment field was extended if the predicted random setup error could not be effectively compensated by thepredefined treatment setup margin. Instead of the conventional approach of patient repositioning, setup adjust-ment was implemented by reshaping the MLC field. The entire process from measuring setup error to reshapingthe MLC field was performed offline through a computer network. After completion of a patient’s treatment, thesystematic and random setup errors after adjustment were compared with those predicted prior to theadjustment. The accuracy of the adjustment, and the reliability and stability of the process were analyzed.Results: Treatment fields of 13 patients were modified to correct for systematic errors. The mean systematic errorwas 4 mm with a range of 2 to 7 mm before adjustment. It was reduced to 0.5 mm with a range of 0.2 to 1.4 mmafter adjustment. There was no significant difference in random setup errors before and after adjustment. TheART process was found to be stable, as more than 95% of patient specific setup margins were predictable within1 mm using the first four to nine fractions of treatment, confirming the feasibility of treatment plan reoptimi-zation with the ART process.Conclusions: The prospective study demonstrates that the ART process can be effectively implemented in routineclinical practice to improve treatment accuracy. This process is also ready to be further extended to reoptimizethe treatment plan by incorporating the predicted patient specific setup variation. © 1998 Elsevier Science Inc.
Adaptive radiation therapy, Treatment setup error, Treatment plan modification.
INTRODUCTION
Adaptive radiation therapy (ART) has been introduced tominimize the detrimental effects of treatment variation onthe individual patient (8). It has been primarily designed toreoptimize the individual treatment plan and dose deliveryaccording to the time course of treatment variation charac-terized during the course of radiation treatment. A retro-spective study (9) has demonstrated that the time course oftreatment setup variation can be characterized early onduring the treatment process, and compensated for by ad-
justing the treatment field shape and prescription dose. Inthe retrospective study, treatment managed in the feedbackprocess of ART was simulated by using the initial treat-ment-planning CT and daily portal images. It was assumedthat during the course of treatment, the position and shape ofthe treatment field could be effectively reconformed using aMLC. However, these assumptions have not yet been con-firmed. The feasibility and reliability of the ART process inthe routine clinical environment have not been established.
In an initial effort to implement the ART process in our
Presented at the 38th Annual ASTRO Meeting, Los Angeles,CA, October, 1996
Reprint request to: Di Yan, D.Sc., Department of RadiationOncology, William Beaumont Hospital, 3601 W. Thirteen MileRd., Royal Oak, MI 48073-6769.Acknowledgements—The authors thank the following for their
valuable assistance in this clinical study: John Robertson, M.D.,Peter Chen, M.D., Carla Cook, M.D., Gary Gustafson, M.D., andJannifer Stromberg, M.D. This work was supported in part by NCIGrants #CA71785 and #CA66074.
Accepted for publication 3 July 1997.
Int. J. Radiation Oncology Biol. Phys., Vol. 41, No. 3, pp. 715–720, 1998Copyright © 1998 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/98 $19.001 .00
715

clinic, a feedback process from on-line portal measurementsto off-line plan evaluation and modification is currentlybeing developed. Preliminary use of this process was lim-ited to improving the treatment positioning accuracy bycorrecting the systematic setup error alone. A prospectiveclinical trial was established to evaluate the clinical feasi-bility and reliability of the ART process. The evaluation wasperformed by testing (a) the improvement of treatment setupaccuracy, and (b) the stability and reliability of the ARTprocess when the treatment was intervened by reshaping theMLC field. The present study with these simple end pointsserves as a preparatory step before the launching of aprospective dose escalation study.
METHODS AND MATERIALS
The prospective study was performed on one of our linearaccelerators equipped with an EPID and a MLC. Patientstreated using the MLC were included in the study. The first20 patients enrolled in the study were used for followinganalysis, which included 10 prostate treatments, 4 treat-ments in the pelvic region, 3 lung treatments, 2 treatmentsof head and neck (h & n) cancers, and one treatment ofbladder cancer. All patients were treated using the conven-tional external beam therapy, which was planned usingeither two-dimensional (2D) or three-dimensional (3D)planning system. Custom-made alpha cradles were used toimmobilize those patients treated to the prostate, and ther-mal plastic masks were used for those treated to the headand neck region. All routine clinical procedures from treat-ment planning through portal film review were maintainedon these patients. No extra work load was placed on thetherapists except for the requirements of daily portal imag-ing, which has not yet become the standard procedure in ourclinic.
Each treatment field was shaped by the MLC using ourin-house MLC preparation system (3) and transferredthrough the computer network to the linear accelerator. Thedaily portal image of each treatment field was alignedoff-line to a reference image by a single individual using atreatment verification tool (6). The reference image wasobtained from the simulation film, which included a reticleat the planned treatment isocenter and an outline of thetreatment field. Throughout the entire study, daily setuperrors for each treatment field were delineated separatelyusing two translational errors (mm) and one rotational error(degree). These errors were defined in the isocenter plane ofthe reference image with the reticle as the 2D coordinatesystem.
After each daily fraction, the time course of a patient’ssetup error was analyzed using the treatment evaluationsoftware (7). The systematic and random setup errors ofeach treatment field, defined as the mean and the standarddeviation of the daily setup errors in the entire treatmentcourse, were predicted (7, 9). In addition, the number ofdaily portal measurements needed for a confident predictionwas proposed (9). It has been demonstrated in a previous
study (9) that both the systematic and random setup errorscould be predicted to be within61 and60.5 mm, respec-tively, at a $95% confidence level using#9 initial dailyportal measurements. Furthermore, the number of initialdays of portal measurement needed to obtain the predictionwith a 95% confidence level is also dependent on themagnitude of the random setup error. It has been repre-sented by an empirical formula,n 5 Min{9, 4 1 2(s 2 1)},where n is the number of daily portal measurements re-quired, ands is the predicted random error. This formulaimplies that for anys $ 1 mm, 4–9 days of portal imagingwill be needed for a confident prediction. On the other hand,if drift on a treatment position was detected by the evalua-tion software, setup errors of this position would not becharacterized using the systematic and random setup errors.Instead, a ‘‘dynamically weighted average’’ on the dailysetup errors measured from previous treatments was used topredict the time trend, and the residual standard deviationbetween prediction and daily measurement was used toquantify the corresponding random feature of the treatmentposition (7). The confidence of the prediction for a driftprocess has not been evaluated. The above empirical for-mula with replacement of the predicted random setup errorto the residual standard deviation has been used in theevaluation software to verify a potential drift of treatmentposition.
Once achieving a confident prediction, a clinical decisionwas made to determine if the actual treatment field neededto be modified to compensate for the setup error. In thisstudy, the clinical decision for a nondrift setup processincluded (a) adjusting the position of the MLC leaves tocorrect for the systematic translational error if the predictedsystematic error$2 mm, and/or adjusting the collimatorrotation to correct for the systematic rotational error if theprediction$2 degrees, and (b) increasing the setup margin(i.e., treatment field margin to compensate for setup erroralone) if the planned setup margin was inadequate to com-pensate for the predicted random setup error. In this study,the number of modifications were limited to one per treat-ment field for the nondrift process. The 2-mm threshold forcorrecting the systematic translational error was determinedin consideration of the accuracy of the prediction, whichwas within 1 mm, and the accuracy of portal imagingmeasurement, which was assumed to have an average un-certainty within 1 mm. The 2-degree threshold for thesystematic rotational error was defined due to similar con-siderations. The decision of the setup margin extension wasonly applied to the treatment when the setup margin wasdefined in the pretreatment planning. In this case, the pre-defined treatment margin for the setup variation could beused to compare with the predicted random error, and todecide if the planned setup variation could be used tocompare with the predicted random error, and to decide ifthe planned setup margin needed to be extended. It isimportant to recall that in this prospective study, no treat-ment field was reduced even if a predicted random setuperror was smaller than the one anticipated in the initial
716 I. J. Radiation Oncology● Biology ● Physics Volume 41, Number 3, 1998

treatment planning process. Treatment field or margin re-duction was not implemented in current process because themain purpose of the study was to test the feasibility of theART, and dose modification was not included in the currenttreatment protocol. Once more, the setup error was cor-rected and compensated for by reshaping the MLC througha computer network, instead of repositioning the patient bythe therapists. The MLC reshaping was implemented againon the MLC preparation system, and the new MLC file forthe remaining treatments was transferred to overwrite theold MLC file after the physician’s approval. Furthermore,the above thresholds for modification decision were alsovalid for a drift process. However, in the case of a driftprocess, there was no limit on the number of modifications.
The systematic and random setup errors of the treatmentafter adjustment were compared with those prior to theadjustment. The residual systematic error after adjustmentwas used to evaluate the accuracy and reliability of the ARTprocess. Furthermore, the difference between the randomsetup errors before and after adjustment was used as ameasure of the stability of the ART process.
Finally, patient specific setup margins were calculated todemonstrate the potential advantages of the ART process inpursuing treatment dose escalation. Treatment setup mar-gins for each patient were determined when a confidentprediction was achieved. The setup margins were calculatedby adding the predicted systematic error to twice the pre-dicted random setup error for each coordinate direction ofthe treatment field if no adjustment was applied, or, if anadjustment was applied, by adding 1 mm (tolerance of theprediction for the systematic error) to twice the predictedrandom setup error. When parallel opposed fields wereused, the systematic and random setup errors were calcu-lated by taking the average from both fields to minimize thepotential measurement error and to minimize the confound-ing influence of 3D out of plane rotations. Until treatmentwas completed, predicted setup margins of the individual
patient were compared to those actual setup margins thatwere calculated from all of the portal measurements afterthe prediction and/or adjustment.
RESULTS
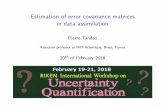
Twenty-seven of total 71 treatment fields (38%), whichwere included in 13 of the 20 patients, were modified tocorrect for systematic errors. Among these 27 fields, 20fields were adjusted on only one of the coordinate direc-tions, 6 were adjusted on both the coordinate directions, and1 was adjusted on both the coordinate directions and rota-tion. Therefore, a total of 34 translational adjustments wereperformed on the 13 patients. Figure 1 shows the number ofinitial days of portal imaging that were required to obtain aconfident prediction of the systematic and random setuperrors for each adjustment. It is compared to the number ofdays actually used before adjustment of the MLC prescrip-tion. The latter was larger due to two reasons: (a) a largernumber of portal measurements were used when both di-rections in a treatment field were adjusted; and (b) a timedelay occurred while awaiting the physician’s approval ofthe new MLC prescription. On average, 6 days of portalimaging were required for a confident prediction.
Figure 2 shows the systematic translational errors beforeand after the MLC adjustments. The mean systematic trans-lational error was 4 mm, with a range of 2 mm to 7 mmbefore adjustment. It was reduced to 0.5 mm, with a rangeof 0.2 mm to 1.4 mm after adjustment. Figure 3 shows thecorresponding results for the random setup errors. The dif-ference in the random setup errors before and after the MLCadjustments was small. It had value less than 0.5 mm for94% of the adjustments, confirming the confidence of theprediction process and the stability of the adjustment pro-cess. In addition, positional drifts were verified on threetreatment fields, which included two prostate treatments andone pelvic treatment. In two of these fields, the direction of
Fig. 1. The number of initial days of portal imaging that were required for a confident prediction of the systematic andrandom setup errors, and the number of treatment days that were actually used before the MLC modification for the 34translational adjustments.
717Prospective study for the ART● D. YAN et al.

the drift alternated during the course of treatment; no clin-ical action was taken to correct for the drift. For the thirdtreatment field, the drift was adjusted twice during thecourse of treatment.
Treatment fields of one prostate patient and one h & npatient were increased in the ART process. For the prostatepatient, the lateral setup margin in the anterior–posteriorfields was increased to compensate for a large random setuperror (4 mm in the patient’s lateral direction), which waspredicted after the first 9 days of treatment. The patient whowas being treated to the nasal cavity had a random setuperror of 1 mm predicted after the first 4 days of treatment atthe superior–inferior edge of the bilateral opposed fields.The reproducibility of this treatment position encouragedthe treating physician to trim the inferior edge of the eyeblock for more adequate coverage of the superior border ofthe maxillary sinus.
In the present study, no treatment setup margin wasreduced and no prescription dose was changed during thecourse of treatment. However, the patient specific setupmargins for all 20 patients, which were predicted in earlydays of treatment and achievable in the ART process, wereplotted in Fig. 4. Figure 5 shows the difference betweenthese predicted margins and the actually calculated margins.It has the mean of 0.3 mm and the standard deviation of 0.4mm. This implies that at least 95% of patient specific setupmargins can be predicted within 1 mm in the first four tonine fractions of treatment.
DISCUSSION AND CONCLUSIONS
Adaptive radiation therapy explores a new application ofdynamic control process to radiation treatment (8). In theprocess, the frequency of modification that should be per-
Fig. 2. The predicted systematic setup errors (translational errors) prior to the MLC adjustment compared with the actualsystematic setup error after MLC adjustment for the 34 translational adjustments.
Fig. 3. The predicted random setup errors (translational errors) prior to the MLC adjustment compared with the actualrandom setup error after MLC adjustment for the 34 translational adjustments.
718 I. J. Radiation Oncology● Biology ● Physics Volume 41, Number 3, 1998

formed to optimize the treatment is not only dependent uponthe possible theraputic gain, but also on current technology.As the process was implemented into our clinic, we insuredthat no additional treatment time was required for eachpatient. To accomplish this goal, the daily portal image wasanalyzed off line, and the beam delivery was modified usingthe MLC through a computer network. Therefore, the rou-tine clinical treatment time and therapist’s responsibilitywere not changed. The major increase of workload wasoff-line registration of portal images, which had to be man-ually performed for each patient during the initial days oftreatments. Once the setup error was characterized and thebeam modified, the daily portal imaging was continuouslyperformed in case of a large catastrophic error or possibletime-trend drift. However, in this study, only 1 of 20 pa-tients benefited from the continuous daily imaging. There-fore, portal imaging with a lower frequency after confidentprediction as proposed by the other researchers (1) can alsobe performed.
Conventionally, a patient will be repositioned based uponthe setup error determined from a single portal measure-ment, or most efficiently, based upon a ‘‘few’’ portal mea-surements (1, 2, 4, 7). The ART process, on the other hand,is focused on incorporating the setup variation characterizedduring the initial days of treatments to reoptimize the treat-
ment plan and dose delivery for the remaining treatments.Therefore, a confident prediction for both the systematic andrandom setup errors is required to achieve the goal of thetreatment plan reoptimization. In theory, the daily patientsetup process of radiation treatment is a stochastic process,which is predictable if the process is ergodic. To examinethis, the systematic and random setup errors before and afterimplementing the adjustments were compared in this pro-spective study. The results demonstrate that the process ofdaily treatment setup was not disturbed by the ART proce-dures. The setup process was predictable, justifying a treat-ment plan reoptimization in the early stages of the treatmentcourse.
Implementation of the ART process requires a new clin-ical infrastructure, in which the clinical treatment proce-dures such as treatment planning, treatment verification,treatment evaluation, and treatment adjustment are not per-formed as independent tasks. Instead, a closed-loop treat-ment process will be used to apply the patient specificinformation measured during the treatment course to reeval-uate and to reoptimize the treatment plan. An optimal wayto implement this feedback process integrates new technol-ogies such as a 3D treatment planning system, an on-lineimaging device, and MLC through an information and con-trol network. With the ART process, the physician couldpotentially act as a central controller to manipulate a pa-tient’s treatment using a computer network.
Modification of the treatment field shape using MLCmakes the ART process possible to correct for the system-atic error, and to compensate for the random setup error byonly reshaping the MLC once. Most importantly, reshapingthe treatment fields allows one to compensate for any targetshape change due to a distortion of the patient position orinternal organ motion. Moreover, adjusting the MLC fieldallows accurate adjustment as small as 0.2 mm, minimizesthe possibility of ‘‘unsettling’’ the patient, and reduces thework load of the therapists. However, although reshapingthe treatment field alone can be used to compensate for thetarget shape change on the beam’s-eye-view plane due to3D out of plane rotation, it may not be acceptable when a
Fig. 4. The patient specific setup margins that were predicted in the first four to nine fractions of the treatment.
Fig. 5. The difference between the predicted setup margin and theactually calculated setup margin on each coordinate direction oftreatment field.
719Prospective study for the ART● D. YAN et al.

specific setup of conformal therapy has to be precisely keptto avoid a critical adjacent organ. In this case, adjustmentsin the ART may also need to include the gantry or treatmentcouch rotation.
As mentioned above, reduction of the PTV or setupmargin and escalation of the prescription dose were notimplemented in this preliminary study. Patients in this pro-spective study have been treated using the conventionaltreatment plan and prescription dose. However, the results(Fig. 4) demonstrate that a large number of patients could betreated using a smaller setup margin and therefore be qual-ified for more aggressive conformal treatment. Meanwhile,a few patients had to be treated conservatively in this study,
and their treatment margin had to be increased to compen-sate for the large setup variation. Treatment margin modi-fication can be implemented in the ART process consideringeither the clinical target volume (CTV) (5) or a criticalorgan. In the case that the CTV cannot be confidentlydetermined or the toxicity of a critical adjacent organ is ofgreater concern, the margin associated with normal organcan be used as the guideline to adjust the treatment field.
In conclusion, the ART process is efficient in the routineclinic to improve treatment accuracy. This process is also readyto be further extended to reoptimize the treatment plan byincorporating the predicted patient specific variation.
REFERENCES
1. Bel, A.; Van Herk, M.; Bartelink, H.; Lebesque, J. V. Averification procedure to improve patient setup accuracy usingportal images. Radiol. Oncol. 29:253–260; 1993.
2. Denham, J. W.; Dally, M. J.; Hunter, K.; Wheat, J.; Leslie, G.;Fahey, P. P.; Hamilton, C. S. Objective decision-making fol-lowing a portal film: The results of a pilot study. Int. J. Radiat.Oncol. Biol. Phys. 26:869–876; 1993.
3. Du, M. N.; Yu, C. X.; Wong, J. W.; Symons, M.; Yan, D.;Matter, R. C.; Martinez, A. A multi-leaf collimator prescriptionsystem for conventional radiotherapy. Int. J. Radiat. Oncol.Biol. Phys. 30:707–714; 1994.
4. Dutreix, A.; van der Schueren, E.; Leunens, L. Quality controlat the patient level: Action or retrospective introspection. Ra-diol. Oncol. 25:146–147; 1992.
5. ICRU Report 50, International Commission of Radiation Units
and Measurements, Prescribing, Recording and Reporting Pho-ton Beam Therapy, 1993.
6. Wong, J.; Yan, D.; Michalski, J.; Graham, M.; Halverson, K.;Harm, W.; Purdy, J. The cumulative verification image analysistool for off-line evaluation of portal images. Int. J. Radiat.Oncol. Biol. Phys. 33:1301–1310; 1995.
7. Yan, D.; Wong, J.; Gustafson, G.; Martinez, A. A new modelfor ‘‘accept or reject’’ strategies in off-line and on-line mega-voltage treatment evaluation. Int. J. Radiat. Oncol. Biol. Phys.31:943–952; 1995.
8. Yan, D.; Vicini, F.; Wong, J.; Martinez, A. Adaptive radiationtherapy. Phys. Med. Biol. 42:123–132; 1997.
9. Yan, D.; Wong, J.; Vicini, F.; Michalski, J.; Pan, C.; Frazier, A.;Horwitz, E.; Martinez, A. Adaptive modification of treatmentplanning to minimize the deleterious effects of treatment setuperrors. Int. J. Radiat. Oncol. Biol. Phys. 38:197–206; 1997.
720 I. J. Radiation Oncology● Biology ● Physics Volume 41, Number 3, 1998