The Urinary System
52
The Urinary System Chapter 26
-
Upload
yvette-hyde -
Category
Documents
-
view
21 -
download
0
description
The Urinary System. Chapter 26. Functions figure 26.1. ___________- Excrete waste in urine Regulate blood volume & composition (ions, pH) Help regulate blood pressure Synthesize glucose Release erythropoietin Participate in vitamin D synthesis - PowerPoint PPT Presentation
Transcript of The Urinary System

The Urinary System
Chapter 26

Functions figure 26.1
___________- Excrete waste in urine Regulate blood volume & composition (ions, pH) Help regulate blood pressure Synthesize glucose Release erythropoietin Participate in vitamin D synthesis
___________ – transport urine from kidneys to urinary bladder
Urinary bladder– stores urine, capacity≈ 700-800mL ____________ – discharges urine from the body




Kidney
Regulates ___________________ composition Na+, K+, Ca2+ , Cl-, and HPO4 2-
Regulate _______________ Excrete H+ Conserve HCO3 –
Reg. __________________ – conserve or elim water blood volume bp, blood vol bp
Regulating ___________ Secrete: renin bp, or adjust blood volume
Maintaining blood osmolarity- reg water & solute loss Hormones: calcitrol (active Vit D), ________________________ Regulate blood glucose- use glutamine in gluconeogenesis Excreting waste and foreign substances

Kidney anatomy figure 26.3
Retroperitoneal 3 layers surrounding
Renal capsule – deepest Adipose capsule Renal fascia – superficial, anchors to ab wall
_______________- fissure where following emerge: Renal aretery Renal vein Ureter
Internally, 2 distinct regions: Renal _________ – superficial Renal _________ – deep, arranged in renal pyramids




Nephron figure 26.5 a & b
Functional unit of the kidney, 2 parts: _________________ – where blood plasma is filtered
Glomerulus – capillary network Glomerular (Bowman’s) capsule – epithelial cup
_________________ – into which the filtrate is passed Proximal convoluted tubule (PCT) Loop of Henle (LOH) Distal convoluted tubule (DCT)
Types: __________ nephron- short LOH, blood from peritubular cap __________________ nephron- close to medulla, long LOH
Long loops enable excretion of very dilute or very [ ]



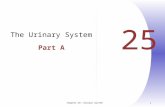
Renal corpuscle fig 26.6
__________________- capillary network Glomerular (Bowman’s) capsule- double
walled epithelial cup that surrounds the capillaries Blood plasma is filtered & collected in capsule Filtered fluid then passes thru renal tubule _____________- visceral, modified simple
squamous cells, wrap around glomerular capillaries & form inner wall of capsule
Outer wall (parietal) is simple squamous




Renal physiology, 3 processes
_______________________ Water & most solutes: capillary renal capsule
_______________________ Filtered fluid move thru tubule Cells reabsorb 99% of water & useful solutes
Returns to blood via Peritubular capillaries Vasa recta
________________________ Removes substances from blood
Urine contains these excreted substances: wastes, drugs, excess ions


Glomerular filtration fig 26.8
Filtration fraction- amt of plasma in ______________ that becomes glomerular filtrate = 16-20% of plasma
Daily volume of glomerular filtrate: 150L female,180L male >99% returned to blood, 1-2 L urine/day
Substances pass _________________: Glomerular endothelial cells = fenestrated
Between capillaries mesangial cells – regulate GF Basal lamina Podocytes w/ pedicel create filtration slits
____________ & ______________________ Most plasma proteins, blood cells & platelets DO NOT

The filtration membrane, fig 26.8

Net filtration pressure, figure 26.9
Glomerular filtration dependent on these 3: Glomerular blood hydrostatic pressure
Blood pressure in glomerular capillaries Promotes filtration
Capsular hydrostatic pressure Hydrostatic P exert by fluid in capsular space Opposes filtration
Blood colloid osmotic pressure Presence of proteins in blood plasma Opposes filtration


Glomerular filtration rate (GFR)
Filtrate formed in renal corpuscles of both kidneys each minute 125 mL/min male, 105 mL/min female Homeostasis req it to be ≈ constant
If too ↑, substance not reabsorbed, lost in urine If too , not enough waste excreted
Directly related to P determining NFP Regulation:
Adjusting _______________ to glomerulus Alter glomerular capillary __________- filtration

Regulation of GFR, table 26.2
1. _____________________ Myogenic mechanism- smooth muscle
contraction – wall of afferent arteriole ↑ bp, stretch wall, smooth mus contracts,
narrow lumen renal blood flow GFR Tubuloglomerular feedback- macula densa
provide feedback to glomerulus If GFR ↑ due to ↑ bp, filtered fluid flows faster,
less time for reabsorption nitric oxide not released & ________________ constricted

Regulation of GFR (2)
2. _____ regulation- kidney bv supplied by SympNS Release NE vasoconstrict (exercise, hemhorrrage)
Blood flow , GFR urine output, conserve blood volume ↑ blood flow to other body tissues
At rest, bv dilated & autoregulation occurring 3. ___________ regulation-
Angiotensin II- GFR by vasoconstriction Atrial natriuretic peptide (ANP) secreted when ↑ blood
vol relax mesangial cells ↑ SA ↑ GFR



Tubular reabsorption PCT
______ & _______ reabsorbed in large quantities ≈65% of filtered water reabsorbed Na+/glucose (phosphate, sulfate, aa) symporters Na+/H+ antiporter
_________ (HCO3-) reabsorbed- fac diffusion
_________ of water Concentrates remaining solutes in PCT Passive reabsorption of other solutes:
Cl-, K+, Ca2+, Mg2+, urea
Urea and ammonia ____________ by PCT

PCT

PCT

PCT, 2nd half

Tubular reabsorption (2) Loop of Henle
Descending limb: ___________ is reabsorbed (15% of filtered water)
Ascending limb: Na+, K+, 2Cl- symporters
most K+ leaks back into tubule thru channels Ca2+, HCO3-, ____________- ascending LOH virtually impermeable to
water not automatically coupled to reabsorption of other solutes like
in PCT Filtrate osmolarity as ascend (ions, not water reabsorb)

Ascending LOH

Tubular reabsorption (3) DCT:
Na+ Cl- symporter reabsorption PTH causes reabsorption of Ca2+ Water 10-15%, (at this point 80% already ab)
* by time fluid reaches end of DCT 90-95% of filtered solutes & water have been returned to bloodstream
Collecting duct: ______ reabsorb thru leak channel Na+/K+pumpblood ______ reabsorbed by intercalated cells, secreted in
variable amounts thru leak channels of principal cells

DCT & collecting duct

Tubular secretion
Secretion of H+ helps control ___________ Secretion of others for ____________ from body
PCT H+ and NH4
+ ions, urea
DCT H+ ions, (K+ by principal cells at end of DCT)
Collecting duct K+/ H+ /NH4
+ ions (depending on salt, pH balance)

Hormonal effects table 26.4
Angiotensin II-(released when blood volume, bp) GFR Stim antiporter reabsorb Na+, Cl-, H2O in PCT Stim release aldosterone
Aldosterone: ( plasma K+) K+ secretion, Na+, Cl-, H20 reabsorbed
ADH- ( osm of ECF or blood volume) water reabsorption in DCT
ANP- (stim by atria stretch, blood volume) secretion of Na+ (natriuresis)
Suppress reabsorption at PCT urine output (diuresis) ANP suppresses ADH & aldosterone secretion

Figure 26.17

Dilute & concentrated, fig 26.18
Body __________ depends largely on kidney Large volume, dilute urine when fluid intake
Asc LOH & DCT rel impermeable to water End of DCT & collecting duct impermeable to
water when ADH ________ Small volume, concentrated: fluid intake
ADH enabled by osmotic gradient Differences in solute & water permeability along
LOH & collecting duct Countercurrent flow in Des & Asc LOH

Dilute urineformation

Countercurrent mechanism
Hairpin shape of LOH- countercurrent flow Descending limb: one direction
Very permeable to water I.F. osmolarity > than inside tube water→ out As fluid moves down- gradient, osmolarity ↑
Impermeable to solutes except urea Ascending limb: opposite direction
Impermeable to water Symporters reabsorb Na+, Cl-
Fluid osmolarity as ascending

Countercurrent mechanism (2)
____________: loops working similar to LOH Descending- renal medulla I.F. more [ ]
More Na+, Cl-, urea diffuse into blood Blood osmolarity
Ascending- I.F. increasingly less [ ] Ions diffuse out of Asc vasa recta Reabsorbed water diffuses from I.F. vasa
recta Osmolarity of blood leaving vasa recta only
slightly higher than what entered O2 & nutrients dropped off w/out gradient



Constituents of urine (lab, p60)
ORGANIC Urea Creatinine Uric acid
INORGANIC Chloride Sodium Potassium Sulfates Phosphates Ammonia Calcium Magnesium

Diuretics
______________ – elevated urine flow rate Substances slow renal reabsorption of water
Often prescribed for _________________ Lower blood volume lower bp Most interfere w/mechanism for Na+ reabsorption
Naturally occurring: Caffeine- inhibits Na+ reabsorption Alcohol- inhibits ADH secretion

Dialysis- “to separate”
_________ of large solutes from smaller ones by diffusion thru selectively permeable mem
Kidneys so impaired that unable to function __________dialysis- filter patient’s blood by
removing wastes, excess electrolytes & fluids and return blood to patient
Hemodialyzer, dialysis membrane Dialysate- solution formed to maintain diffusion
gradients & add needed substances Peritoneal dialysis- catheter & dialysate

Flow from nephron to urethra
(Nephron: Bowman’s capsulePCTLOHDCT) Collecting duct Papillary duct Minor calyx Major calyx Renal pelvis Ureter Urinary bladder Urethra

Micturition
Urination or voiding Discharge of urine from urinary bladder Voluntary (SNS) & involuntary (ANS) muscle
contractions When 200-400mL stretch receptors trigger
________________- S2-S3 spinal reflex Contraction of detrusor Relaxation- internal urethral sphincter muscle
Filling causes sensation before reflex occurs _______________- lack of voluntary control

Clinical connections
Diabetes insipidus- nephrogenic- kidneys do not respond to __________ ADH receptors may be damaged Or kidneys may be damaged
UTIs- infection of urinary system or presence of large # of microbes in the urine Urethritis- inflammed urethra Cystitis- inflammed urinary bladder Pyelonephritis- inflammed kidneys, if chronic-
scar tissue forms

Medical terminology
Polyuria- excessive urine formation- maybe due to D.M. and ___________________- Inflammation of kidney involving glomeruli
often from allergic rxns to toxin produced by streptococcus
Anuria- absence of urine formation Oliguria- abnormally slight or infrequent
urination