The Unquiet Eye in General Practice. Session Aims Anatomy: Understand the anatomy and terminology...
20
The Unquiet Eye in General Practice
-
Upload
dwight-paul -
Category
Documents
-
view
216 -
download
0
Transcript of The Unquiet Eye in General Practice. Session Aims Anatomy: Understand the anatomy and terminology...
The Unquiet Eye in
General Practice
Session Aims
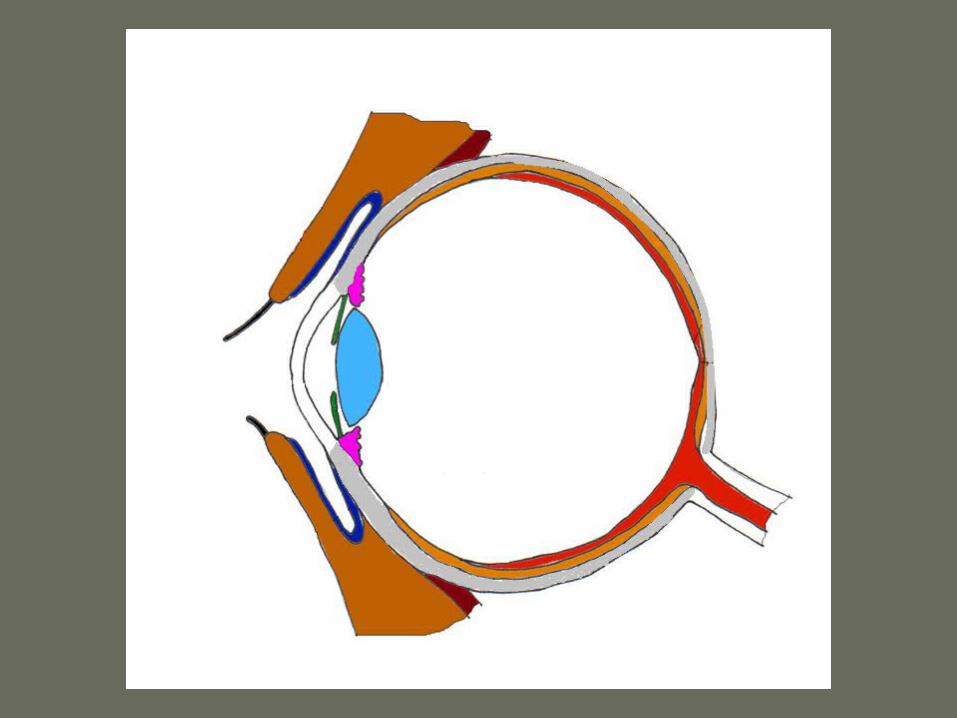
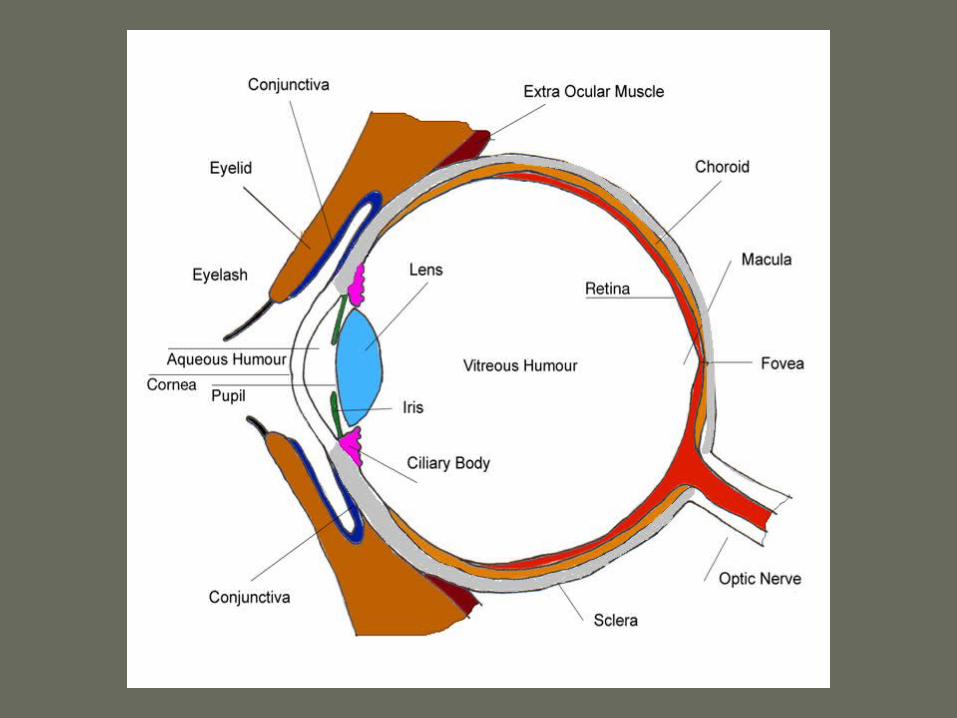
Anatomy: Understand the anatomy and terminology
History: What is a reasonable targeted eye history?
Examination: What is reasonable targeted eye examination?
Common causes of an unquiet eye:
– recognition and management
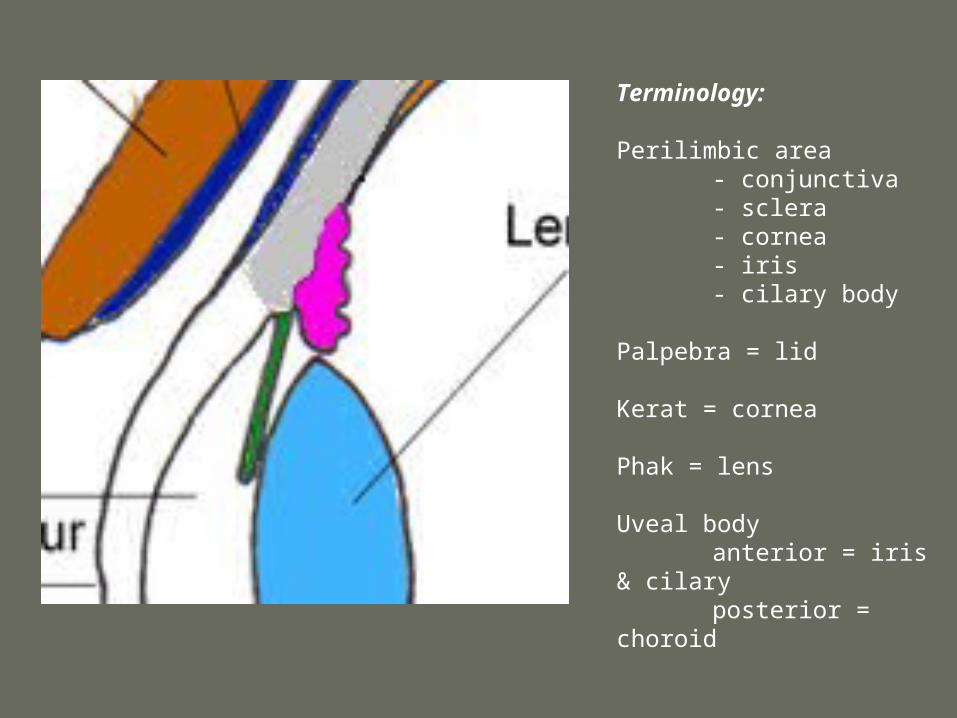
Terminology:
Perilimbic area- conjunctiva- sclera- cornea- iris- cilary body
Palpebra = lid
Kerat = cornea
Phak = lens
Uveal bodyanterior = iris & cilaryposterior = choroid

Ophthalmic History
Ophthalmic History
HOPC
Trauma (eye or head)
Pain – discomfort through to photophobia
Change in vision & visual disturbance
Contact Lenses
PMH – eye problems, CTDs, IBDs.
Ophthalmic Examination
Full Ophthalmic Examination
Acuity: RE & LE C & UC Snellen
External eye: Inspection
Fluorescein
Internal eye: Pupil & iris
Fundoscopy
Other bits: Fields Colour vision Eye movements]
Some causes of an unquiet eye
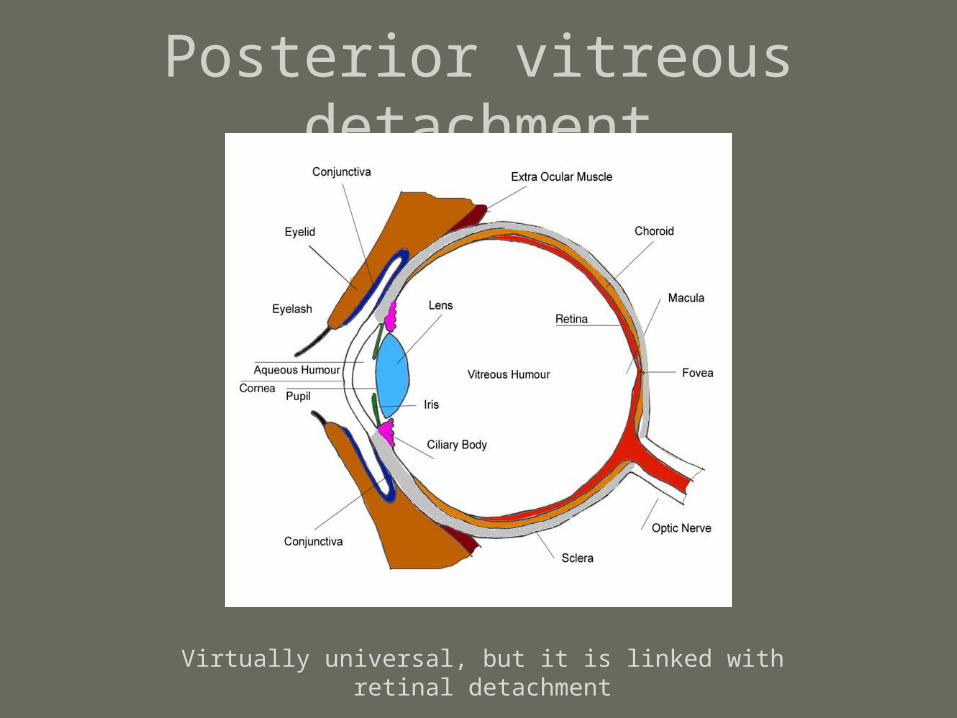
Posterior vitreous detachment
Virtually universal, but it is linked with retinal detachment
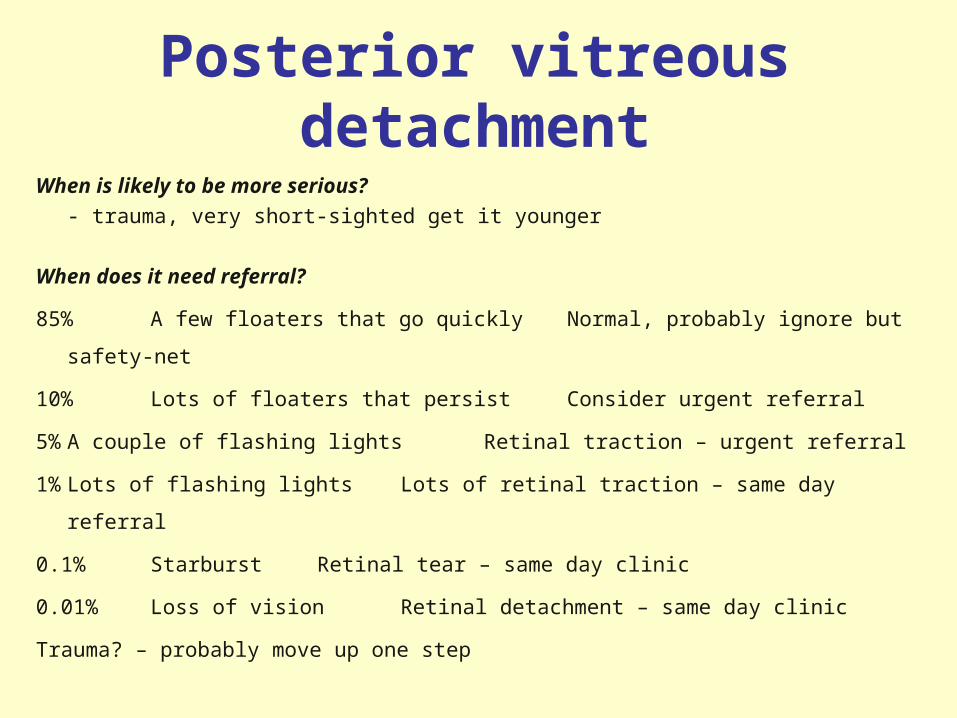
Posterior vitreous detachment
When is likely to be more serious?
- trauma, very short-sighted get it younger
When does it need referral?
85% A few floaters that go quickly Normal, probably ignore but safety-net
10% Lots of floaters that persist Consider urgent referral
5%A couple of flashing lights Retinal traction – urgent referral
1%Lots of flashing lights Lots of retinal traction – same day referral
0.1% Starburst Retinal tear – same day clinic
0.01% Loss of vision Retinal detachment – same day clinic
Trauma? – probably move up one step

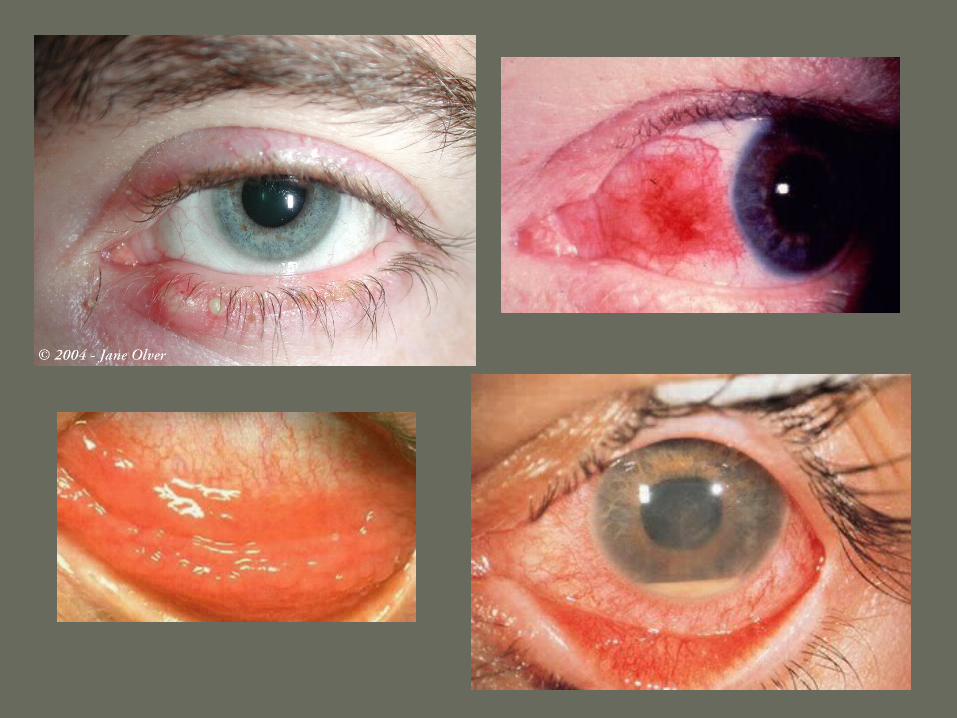
Blepharitis:
Lid cleaning
Chloramphenicol ointment if acute
Link with seborrhoeic dermatitis
Link with styes & chalazion
Chalazia:
– warm compress, refer after 4-6m
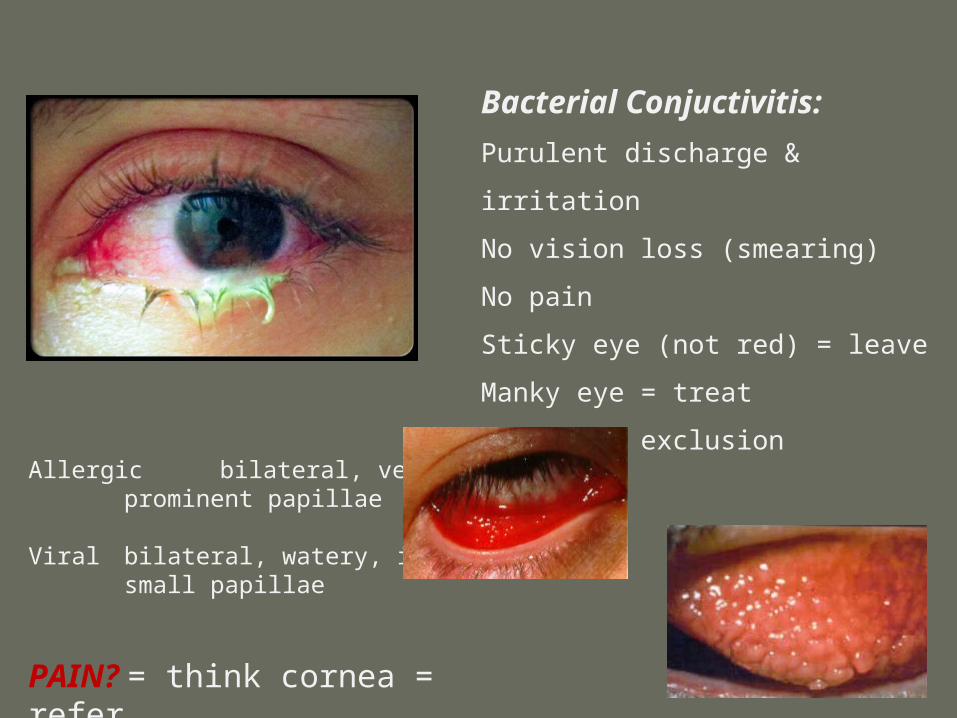
Bacterial Conjuctivitis:
Purulent discharge & irritation
No vision loss (smearing)
No pain
Sticky eye (not red) = leave
Manky eye = treat
No school exclusion
Allergic bilateral, very itchyprominent papillae
Viral bilateral, watery, irritatedsmall papillae
PAIN? = think cornea = refer
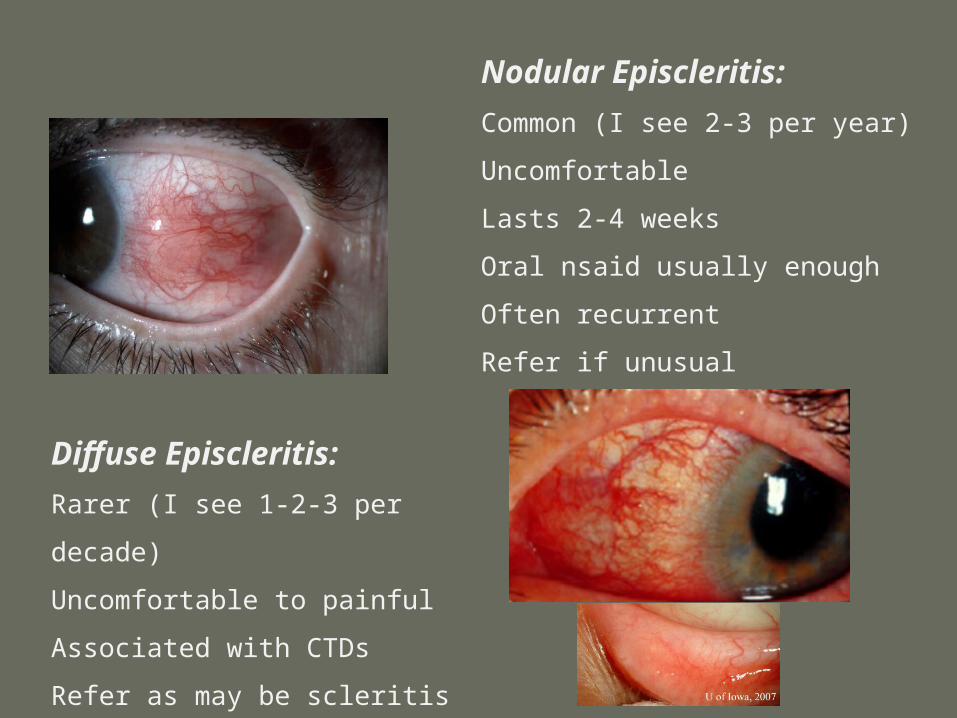
Nodular Episcleritis:
Common (I see 2-3 per year)
Uncomfortable
Lasts 2-4 weeks
Oral nsaid usually enough
Often recurrent
Refer if unusual
Diffuse Episcleritis:
Rarer (I see 1-2-3 per decade)
Uncomfortable to painful
Associated with CTDs
Refer as may be scleritis
(looks the same)

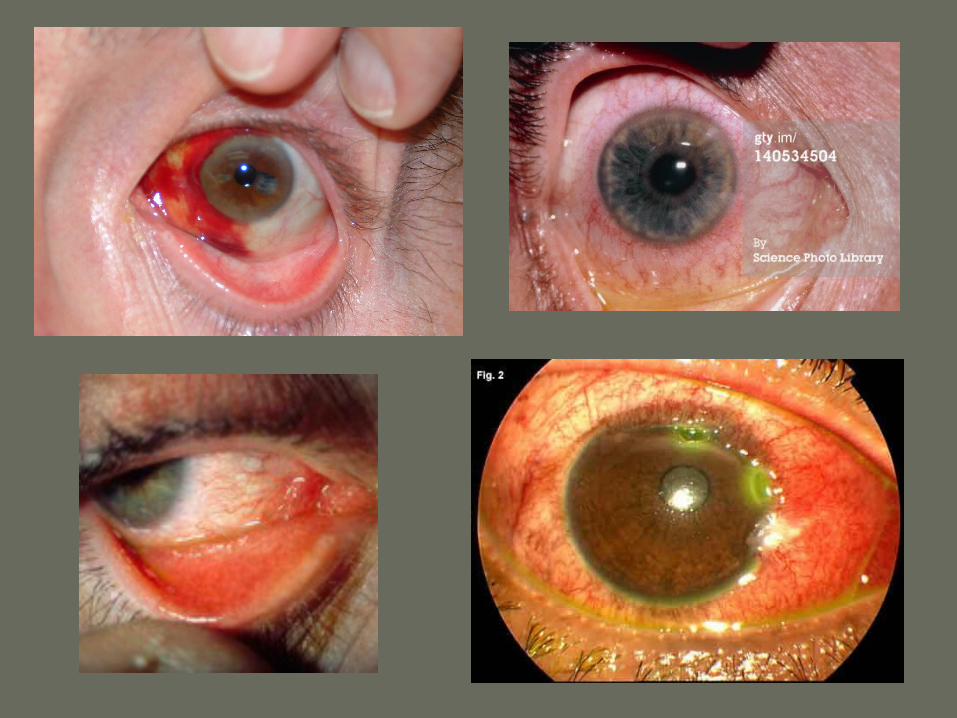
Subconjunctival Haemorrhage:
Common (I see 2-3 per year)
Trauma or spontaneous
[think BP & anti-coag]
Uncomfortable
Lasts 2-4 weeks
Can look very alarming with a
swollen and bulging conjunctiva
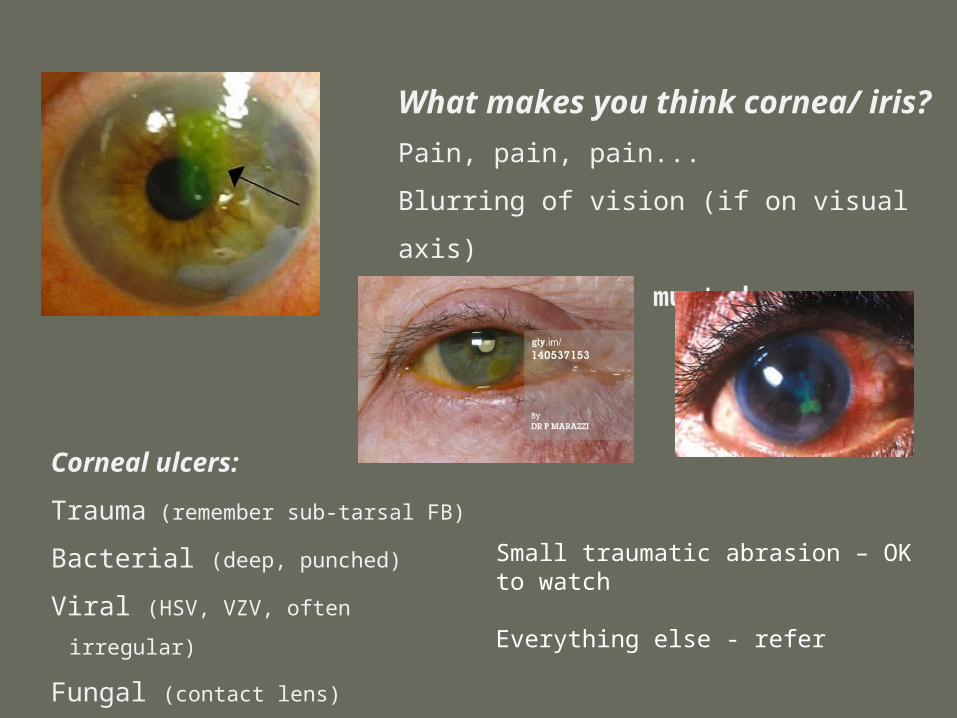
What makes you think cornea/ iris?
Pain, pain, pain...
Blurring of vision (if on visual axis)
Must do acuity, must do fluorescein
Corneal ulcers:
Trauma (remember sub-tarsal FB)
Bacterial (deep, punched)
Viral (HSV, VZV, often irregular)
Fungal (contact lens)
Small traumatic abrasion – OK to watch
Everything else - refer
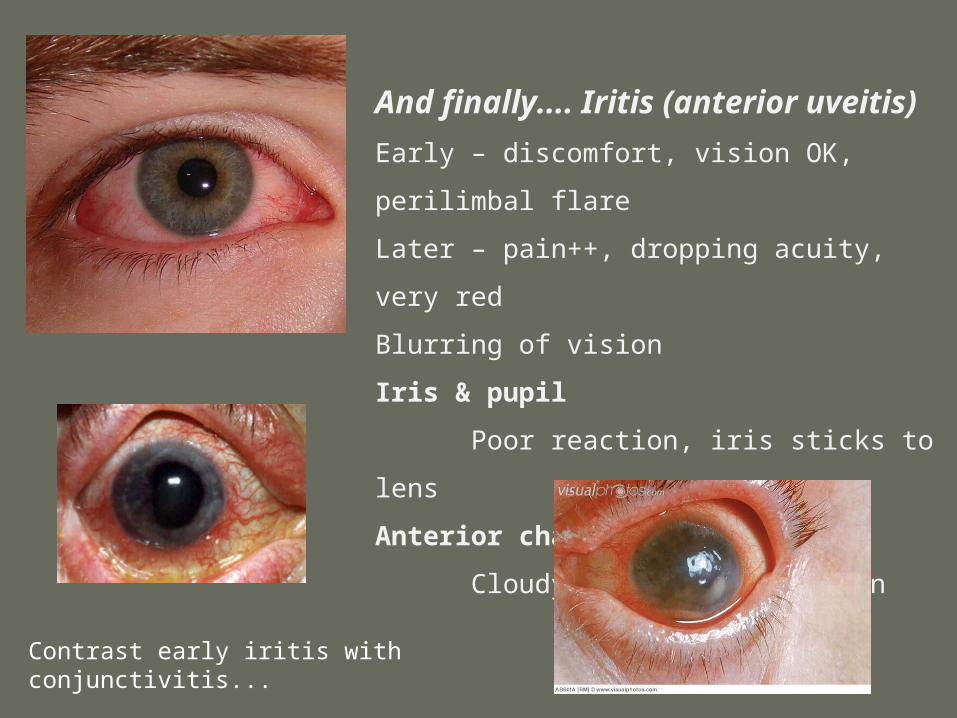
And finally.... Iritis (anterior uveitis)
Early – discomfort, vision OK, perilimbal flare
Later – pain++, dropping acuity, very red
Blurring of vision
Iris & pupil
Poor reaction, iris sticks to lens
Anterior chamber
Cloudy (exudate), hypopyon
Contrast early iritis with conjunctivitis...
Key Messages
Anatomy Understand the anatomy and terminology
History What is a reasonable targeted eye history?
(Trauma, pain, vision change, contact lens)
Examination What is reasonable targeted eye examination?
(Acuity & Fluorescein)
Mild versions can be very similar:
episcleritis, viral conjunctivitis, iritis
If in doubt, review in 24-48hrs.