The Treatment Utility of Assessment
12
The Treatment Utility of Assessment A Functional Approach to Evaluating Assessment Quality Steven C. Hayes Rosemery O. Nelson Robin B. Jarrett University of Nevada-Reno University of North Carolina at Greensboro University of Texas Health Science Center at Dallas ABSTRACT." In practical terms, the sine qua non of the modes, methods, devices, strategies, and theories of clin- ical assessment is their contribution to treatment outcome. The importance of this contribution has often been noted, but under many different labels and rationales. The re- sultant conceptual confusion has considerably restricted the visibility andfrequency of research in this critical area. In this article we propose a name for the impact of as- sessment on treatment outcome: the "treatment utility of assessment. "' Some of the questions that can be asked about the treatment utility of assessment are described, and methods appropriate for asking them are examined. Finally, the implications of this kind of utility for other approaches to evaluating assessment quality are analyzed. Clinical assessment is an important and fertile area of psychology, and yet there is general agreement that it has not been in a state of continuous and healthy growth (e.g., Bersoff, 1973; Korchin & Schuldberg, 1981; Rorer & Widiger, 1983). Compared to the early days of clinical psychology, there has been a decline in the emphasis on clinical assessment both in training and in practice (Gar- field & Kurtz, 1973, 1976; Levitt, 1973; Shemberg & Keeley, 1970). One reason may be that clinical assessment has not yet proven its value in fostering favorable treatment out- comes. As clinical psychologists have devoted more and more time to treatment activities, the practical value of assessment has come under closer scrutiny (McReynolds, 1985). Unfortunately, experienced clinicians have not al- ways found assessment data to be useful in treatment (Adams, 1972; Daily, 1953; Meehl, 1960; Moore, Bobbitt, & Wildman, 1968). Even the proponents of clinical as- sessment admit that "we do not believe that the current [high] status of testing is due to its demonstrated value" (Kaplan, Colarelli, Gross, Leventhal, & Siegel, 1970, p. 15). The lack of empirical evidence for the practical value of assessment has long been noted. In 1959, Meehl pointed out that, even if an assessment procedure is re- liable and valid, a clinician might "be seriously in error if he concluded therefrom that his tests were paying off in practice. On this question there is... no published empirical evidence" (p. 117). Twenty-two years later, Korchin and Schuldberg (1981) were still worried that "clinical assessment may not provide the kind of infor- mation needed by therapists. Objective evidence is slim" (p. 1154). More recently, McReynolds (1985) asked "Are tests helpful to the therapist? Amazingly, there has been little research on this crucial question" (p. 10). The pur- pose of the present article is to consider how to make better progress in understanding the role of assessment in successful treatment. Any lack of evidence on the clinical value of assess- ment is not caused by a lack of appreciation for its ulti- mate practical purposes. Korchin (1976) defined clinical assessment as "the process by which clinicians gain un- derstanding of the patient necessary for making informed decisions" (p. 124). Thus, the "basic justification for as- sessment is that it provides information of value to the planning, execution and evaluation of treatment" (Kor- chin & Schuldberg, 1981, p. 1154). Wiggins (1973) said, "Although measurement and prediction may be evaluated by formal psychometric criteria, such as reliability and validity, the outcomes of [assessment] decisions must be evaluated in terms of their utilities for individuals and institutions within our society" (p. 272, emphasis in orig- inal). Meehl (1959) phrased it as follows: "In what way and to what extent does this.., information help us in treating the patient?" (1959, p. 117). He called this ques- tion "ultimately the practically significant one by which the contributions of our [assessment] techniques must be judged" (p. 116). Definition of the Treatment Utility of Assessment The impact of clinical assessment on treatment outcome has been discussed under a wide variety of labels. Among other terms, it has been viewed as a matter of incremental validity (Mischel, 1968), concurrent validity (Meehl, 1959), construct validity (Edwards, 1970), predictive va- lidity (Lord & Novick, 1968), discriminative efficiency (Wiggins, 1973), and utility (Cronbach & Gleser, 1965). There is considerable confusion about the concepts rel- evant to the measurement of pragmatic clinical value. We propose to use the phrase the treatment utility of assessment to refer to the degree to which assessment is shown to contribute to beneficial treatment outcome, l 1 Earlier(Nelson & Hayes, 1979),we had used the term treatment validity. Although utility issues can indeed be consideredan aspect of validity,the present term seems more direct. November 1987 American Psychologist Copyright 1987 by the American Psychological Assooation, Inc. 0003-066X/87/$00.75 Vol. 42, No. I I, 963-974 963
Transcript of The Treatment Utility of Assessment

The Treatment Utility of Assessment A Functional Approach to Evaluating Assessment Quality
Steven C. Hayes Rosemery O. Nelson
Robin B. Jarrett
University of Nevada-Reno University of North Carolina at Greensboro University of Texas Health Science Center at Dallas
ABSTRACT." In practical terms, the sine qua non of the modes, methods, devices, strategies, and theories of clin- ical assessment is their contribution to treatment outcome. The importance of this contribution has often been noted, but under many different labels and rationales. The re- sultant conceptual confusion has considerably restricted the visibility and frequency of research in this critical area. In this article we propose a name for the impact of as- sessment on treatment outcome: the "treatment utility of assessment. "' Some of the questions that can be asked about the treatment utility of assessment are described, and methods appropriate for asking them are examined. Finally, the implications of this kind of utility for other approaches to evaluating assessment quality are analyzed.
Clinical assessment is an important and fertile area of psychology, and yet there is general agreement that it has not been in a state of continuous and healthy growth (e.g., Bersoff, 1973; Korchin & Schuldberg, 1981; Rorer & Widiger, 1983). Compared to the early days of clinical psychology, there has been a decline in the emphasis on clinical assessment both in training and in practice (Gar- field & Kurtz, 1973, 1976; Levitt, 1973; Shemberg & Keeley, 1970).
One reason may be that clinical assessment has not yet proven its value in fostering favorable treatment out- comes. As clinical psychologists have devoted more and more time to treatment activities, the practical value of assessment has come under closer scrutiny (McReynolds, 1985). Unfortunately, experienced clinicians have not al- ways found assessment data to be useful in treatment (Adams, 1972; Daily, 1953; Meehl, 1960; Moore, Bobbitt, & Wildman, 1968). Even the proponents of clinical as- sessment admit that "we do not believe that the current [high] status of testing is due to its demonstrated value" (Kaplan, Colarelli, Gross, Leventhal, & Siegel, 1970, p. 15).
The lack of empirical evidence for the practical value of assessment has long been noted. In 1959, Meehl pointed out that, even if an assessment procedure is re- liable and valid, a clinician might "be seriously in error if he concluded therefrom that his tests were paying o f f
in practice. On this question there i s . . . no published empirical evidence" (p. 117). Twenty-two years later, Korchin and Schuldberg (1981) were still worried that
"clinical assessment may not provide the kind of infor- mation needed by therapists. Objective evidence is slim" (p. 1154). More recently, McReynolds (1985) asked "Are tests helpful to the therapist? Amazingly, there has been little research on this crucial question" (p. 10). The pur- pose of the present article is to consider how to make better progress in understanding the role of assessment in successful treatment.
Any lack of evidence on the clinical value of assess- ment is not caused by a lack of appreciation for its ulti- mate practical purposes. Korchin (1976) defined clinical assessment as "the process by which clinicians gain un- derstanding of the patient necessary for making informed decisions" (p. 124). Thus, the "basic justification for as- sessment is that it provides information of value to the planning, execution and evaluation of treatment" (Kor- chin & Schuldberg, 1981, p. 1154). Wiggins (1973) said, "Although measurement and prediction may be evaluated by formal psychometric criteria, such as reliability and validity, the outcomes of [assessment] decisions must be evaluated in terms of their utilities for individuals and institutions within our society" (p. 272, emphasis in orig- inal). Meehl (1959) phrased it as follows: "In what way and to what extent does t h i s . . , information help us in treating the patient?" (1959, p. 117). He called this ques- tion "ultimately the practically significant one by which the contributions of our [assessment] techniques must be judged" (p. 116).
Definition of the Treatment Utility of Assessment The impact of clinical assessment on treatment outcome has been discussed under a wide variety of labels. Among other terms, it has been viewed as a matter of incremental validity (Mischel, 1968), concurrent validity (Meehl, 1959), construct validity (Edwards, 1970), predictive va- lidity (Lord & Novick, 1968), discriminative efficiency (Wiggins, 1973), and utility (Cronbach & Gleser, 1965). There is considerable confusion about the concepts rel- evant to the measurement of pragmatic clinical value.
We propose to use the phrase the treatment utility of assessment to refer to the degree to which assessment is shown to contribute to beneficial treatment outcome, l
1 Earlier (Nelson & Hayes, 1979), we had used the term treatment validity. Although utility issues can indeed be considered an aspect of validity, the present term seems more direct.
November 1987 �9 American Psychologist Copyright 1987 by the American Psychological Assooation, Inc. 0003-066X/87/$00.75 Vol. 42, No. I I, 963-974
963

An assessment device, distinction, or strategy has this kind of utility if it can be shown that treatment outcome is positively influenced by this device, distinction, or strategy. The treatment utility of assessment deserves to be termed a type of utility because it relates closely to the functional thrust of that psychometric term. The need to qualify the word utility with the adjective treatment is justified by two facts. First, utility has been almost ex- clusively evaluated in terms of personnel decisions (e.g., Wiggins, 1973). The issues and methods involved in demonstrating the impact of assessment on treatment outcomes differ significantly from the methods appro- priate to the analysis of personnel decisions. Second, in personnel matters the concept of utility has come to refer primarily to the cost-benefit ratio of assessment strategies. This is why it was originally distinguished from predictive validity (Mischel, 1968). The treatment utility of assess- ment is not primarily a matter of cost-benefit analysis but of the demonstration of a particular type of benefit.
Barriers to Research on the Treatment Utility of Assessment Theorists have long believed that research on the treat- ment utility of assessment should be feasible. "It is well within the capacity of available research methods and clinical facilities to determine what, if any, is the prag- matic advantage of a personality assessment" (Meehl, 1959, p. 125). Why then has there continued to be so little research?
There are several possible reasons. First, because of conceptual confusion about the psychometric concepts relevant to the treatment utility of assessment, little has been written about the kinds of methods appropriate to treatment utility questions. In the present article, we present a taxonomy of treatment utility methods in the hope of alleviating this problem.
Second, "Clinical p s y c h o l o g i s t s . . , often make a sharp cleavage between their roles as diagnostician and therapist" (Blatt, 1975, p. 336). Assessment is often not integrated into the therapy process. When the two are disconnected, the value of assessment seemingly turns on the question, Is this diagnosis correct? not Is this assess- ment useful in treatment? Some clinicians even fear that the assessment process is negatively intrusive on the ther- apeutic alliance. By focusing on the contribution of as- sessment to treatment outcome, treatment utility provides an approach for the testing of such concerns and may itself help integrate assessment and treatment roles.
Another part of the problem may lie in the belief that complete psychometric purity is necessary before the treatment utility of assessment can be shown or even examined. Wiggins (1973), who has emphasized the
The authors would like to thank Paul McReynolds for his helpful com- ments on an earlier draft of this article.
Correspondence concerning this article should be addressed to Steven C. Hayes, Department of Psychology, University of Nevada-Reno, Reno, NV 89557-0062.
practical importance of assessment more than most psy- chometric theorists, noted the possibility that "concern with the technical problems of measurement . . . has resulted in a relative neglect of the broader context in which such problems arise, namely, the optimal assign- ment of men to jobs or treatments" (p. 272). As we will show, there seems to be little reason to delay treatment utility research until psychometrically perfect devices are developed.
Finally, research on the treatment utility of assess- ment did not have a proper intellectual context until the last few years. Two trends in particular have now come together to make such research both possible and im- portant: the increased specificity of treatment and of as- sessment, and the emphasis on more theoretically oriented therapy research.
Treatment and Assessment Specificity
In earlier eras of clinical psychology, most psychothera- pists practiced according to general schools of therapy. When clinicians apply the same general approach to most clients, assessment data can have few treatment impli- cations (e.g., Wallen, 1956). With the arrival of more spe- cific interventions, however, the need for guidance by as- sessment data becomes more obvious. Paul's (1969) well- known admonition that one should seek to identify which treatment works best for whom now carries a sense of contemporary urgency.
Compared to the early days of clinical psychology, today there are literally hundreds of competing types of psychosocial inter- ven t ions . . , what qualities of this person, or aspects of his or her life situation and environment, recommend that he or she be seen in what type of therapy, with what kind of therapist, using what kind of technique? This is the question facing us today. (Korchin & Schuldberg, 1981, p. 1155)
Similarly, the early eras of clinical assessment tended to emphasize more global measures of personality. The treatment implications of such measures are often cor- respondingly vague, especially because general personality characteristics may be apparent to the clinician without an elaborate assessment process. This may be one reason that traditional assessment rarely alters the diagnostic judgments of clinicians, much less their treatment plans (Adams, 1972). Many contemporary assessment devices, however, are now quite specific, measuring specific be- havior patterns, specific cognitions, and so on. With spe- cific assessment devices, more specific treatment impli- cations can be explored.
Theory-Oriented Treatment Research
Psychotherapy researchers now agree that simply showing that therapy works is relatively uninteresting. As the recent special issues of the American Psychologist and the Jour- nal of Consulting and Clinical Psychology (Kazdin, 1986; VandenBos, 1986) show, psychotherapy researchers are adopting a more conceptually oriented process approach. The renewed emphasis on the role of theory in therapy research (e.g., Forsyth & Strong, 1986) enhances the im-
964 November 1987 �9 American Psychologist

portance of the treatment utility of assessment. As we will discuss later, the theoretical importance of treatment research tends to emerge at the interface between assess- ment and treatment. In addition, there seems to be agree- ment that "future psychotherapy outcome research should, at a minimum . . . . [explore] the relative advan- tages and disadvantages of alternative treatment strategies with different specific psychological and behavioral dif- ficulties" (VandenBos, 1986, p. 111), moving away from "undifferentiated treatment [as] the status quo" (Miller & Hester, in press; see also McLean, 1981; Shaw, 1981). Thus, the field may now be intellectually ready to tackle the treatment utility of assessment.
Several Beginning Examples The questions that can be asked about the treatment util- ity of assessment span the range of those relevant to as- sessment in general. Several short examples may serve as an introduction to the flexibility of the approach.
Target Behaviors and Classification
Research on the treatment utility of assessment can ad- dress which target behaviors should be the focus of treat- ment in specific patient subtypes. In one empirical ex- ample, patients with social skills problems were divided into two groups: those with apparent skills deficits and those with apparent suppression of skills because of social anxiety (Trower, Yardley, Bryant, & Shaw, 1978). This had been a popular distinction in the social skills literature (e.g., Hersen & Bellack, 1977), but the relationship be- tween identifying skills deficits or social anxiety and find- ing differential treatment outcomes had not been shown. Trower et al. (1978) showed that socially deficient patients showed greater improvement with social skills training than with systematic desensitization, whereas socially anxious patients showed equal improvement under either treatment. Thus, the assessment distinction between skills deficits and social anxiety can be said to have a degree of treatment utility, but only for the skills deficit group.
There are a number of other examples of treatment utility research examining specific patient subtypes, al- though they are surprisingly rare given their obvious im- portance. For example, studies have shown the treatment utility of assessment distinctions between types of insom- nia (Borkovec, Grayson, O'Brien, & Weerts, 1979), anx- iety (Altmaier, Ross, Leary, & Thornbrough, 1982; Elder, Edelstein, & Fremouw, 1981; Ost, Jerremalm & Johans- son, 1981; Shahan & Merbaum, 1981), dysmenorrhea (Chesney & Tasto, 1975), and depression (Paykel, Prusoff, Klerman, Haskell, & DiMascio, 1973).
Note that in studies of this type, treatment utility is based on a nexus of assessment devices, theoretical dis- tinctions, and treatment approaches. An assessment dis- tinction can originally have no treatment utility, but may acquire it when theories and treatments that make effec- tive use of the distinction are later developed. Thus, the treatment utility of assessment reflects not only on the assessment device, but also on its theoretical and practical context. Mischel (1968) noted this point clearly:
It is hard to separate the validity of a test from the validity of the personality construct it supposedly measures. The utility of statements a b o u t . . , constructs of psychodynamic theory, for example, depends on the value of the predictions and treatment decisions to which they lead in the individual case. The utility of the results reflects both on the theoretical constructs and on the test procedures from which these results are generated. (p. 104)
Devices and Instruments
Another question that could be addressed from a treat- ment utility approach is whether given assessment devices are useful. Apparently, no studies have yet been conducted that are designed to measure directly the treatment utility of given devices, but in principle the strategy seems straightforward. For example, suppose one wished to as- sess the treatment utility of using self-monitoring diaries to guide treatment planning, above and beyond that pro- vided by questionnaires. All subjects could complete both questionnaires and self-monitoring diaries, but self-mon- itoring data for only half the subjects would be made available to therapists designing their treatment programs. If these subjects improved more than those whose treat- ment plans were based on questionnaires alone, then the treatment utility of using self-monitoring data would be established for this particular disorder. In a similar fash- ion, the treatment utility of interviews, role-plays, pro- jective tests, and other devices could be evaluated.
Strategies
The treatment utility of general assessment strategies can also be assessed. For example, the treatment utility of a functional analysis of the individual client's problems can be determined by comparing the progress of clients with individually designed treatment programs to those re- ceiving a standard treatment package for a given disorder. A host of similar questions can be asked in the same way. Does objective assessment aid in effective treatment to a greater extent than projective assessment? Does the use of single-subject evaluation designs improve treatment more than not using such designs? Is the use of psycho- metrically pure instruments generally more valuable in treatment planning than the use of other instruments? Many of the most central questions in clinical assessment are of this type, and yet often the field has generated vir- tually no data directly relevant to them. Research on the treatment utility of assessment provides a method for an- swering such questions.
A M e t h o d o l o g i c a l T y p o l o g y
Research on the treatment utility of assessment requires considerable attention to the question being asked. It seems useful to describe a typology summarizing the kinds of treatment utility studies that can be done and to discuss ways in which methodological difficulties can be avoided. Some of the various areas of assessment that can be evaluated using treatment utility studies are sum- marized in Table I. Each row describes a specific kind of study and the question it asks. The last three columns briefly describe the methods appropriate to each question,
November 1987 �9 American Psychologist 965

_r
el 0
0. el
z
_ ~ . ~ :~.~ : '~ ~
~ - I _ 8 3 o (/) .--
- ~ ; ~
(/) <
"~ ~ ~~ ~ O
~.-8
gSel~ E=
e- O
e',
8 0
._~ 8 I--
~ 1 7 6 1 7 6 ~E~ 8 :3 (~ el r o ~ | ~ s ~ ~ -o ~6
;.~ ~ .~.~ ~ I.-- F-
~- E el
~=: (/) 'e-
l"-
E
D-
8
o
"6
F-
~.o_
I
E
E
8 ~ ~ 8
JE O
O
8
"R
~. O
I--
~ e l e l
~ E
e-"
m o �9
~ O * - , s N ._~
O E ~
I--
~ 8 Tel
r el
8
O 'O
I--
E
*.-, :3 .--~ O "O ~
E "0 0 E ".~ el _m m
.~- ._~
e-. ~1.
.Q
m 0
~ ~ E E
el
E
8 E
e-
~
o~
E O E O t--
el = | E ~
_~ ~ - ~ :3 ::3 .-- Q. ~t. {" ~ E
~ o
966 November 1987 �9 American Psychologist

i+ p, +,
i
o"
0
+ o .
I -
o
8
0
o -
~-6~ ~o~ E ~o
8~,~'~'8 , ~ . = o o -6| . . , o . | ~9#
. ~ ~ -6~ ...... ,ooo . . . . S "~
~ ..9-6
Z
-6 8 ~ I ~
- ~ . _ ~ _ + o ~ E m +~,~ ~176 i ~ ~ ~ o~ ~ . e - ~ t ~ . ~
= e E �9 - - t~ O ~
0 9 .g
t-- t ~
~ |
+
s
�9 0 c ~ c
~ . ' 0
~J
+
E
~ 8 = 0+
~ > ~
~o
. -- </} 9 ~ "6_o
N
%
c
9
-~- 8 c
, ~ ~ ~.~.-
c O~
0 ~ ::3 ~ .., 9
~ . ~ .~8 ~=o :~.~.
I -
i-+ ~ + - o . ++ ~+++
~|
-6~ 0
9 o
0 ~ ~~
0 ~ L..
I"-
o
e- 0 ~ E
"~ 0
-6~
. ~ e.. o e~
8 c
. _ O ~ ~Eg
o
November 1987 �9 Amer i can Psychologist 967

organized by types of desigri: group comparison and time- series (with the main question either being asked within or between subjects). In this section, we will briefly elab- orate on some of the questions that can be asked about the treatment utility of assessment and the methods that can be used.
Post Hoc Identification of Dimensions
One approach to the treatment utility of assessment is to administer treatment to many persons and then to identify aspects of the assessment that help predict who will re- spond to therapy. This is a well-known strategy with a long tradition in clinical science (Beutler, 1979; Miller & Hester, in press). For example, a review of research in depression by Bielski and Friedel (1976) found that higher social class, insidious onset, anorexia, weight loss, middle and late insomnia, and psychomotor disturbance predicted a favorable response to tricyclic medication. In contrast, neurotic, hypochondriacal, and hysterical traits; multiple prior episodes; and delusions predicted a poor response.
Research of this sort often correlates patient outcome with such measures as the Minnesota Multiphasic Per- sonality Inventory (MMPI; e.g., Shealy, Lowe, & Ritzler, 1980; Strassberg, Reimherr, Ward, Russell, & Cole, 1981), locus of control devices (e.g., Poole, Dunn, Sanson-Fisher, & German, 1981; Woodward & Jones, 1980), self-efficacy measures (e.g., DiClemente, 1981; Williams, Dooseman, & Kleifield, 1984), or demographic characteristics (e.g., Dumas & Wahler, 1983; Ellsworth et al., 1979). These measures are probably popular because they are com- monly collected at the beginning of treatment and thus provide ready data bases for post hoc examination.
At an applied level, these reported relations at times are not useful. They may identify variables that are dif- ficult or impossible to change, such as global personality characteristics or the chronicity of the disorder itself (e.g., Bollard, 1982; Brown & Lewinsohn, 1984; Miller & Joyce, 1979). Factors may be identified that predict poor treatment response, without corresponding knowledge about how to produce a beneficial response in these same individuals. Furthermore, research of this sort has often failed to find consistent or strong correlations between assessment measures and outcomes. It is common to see such studies reporting correlations that account for 5% to 10% of the variance in outcome (e.g., Luborsky, Mintz, & Christoph, 1979). Despite the many studies of this type, there is little evidence that they are leading to increasingly effective treatments, though they may help in resource allocation within institutions. There are several possible sources of the limited value of post hoc analyses to treat- ment outcome.
Theproblem of the individual. In a typical post hoc approach to treatment utility, large numbers of subjects have been assessed pretreatment and posttreatment on the target behavior. The degree of improvement is then correlated with other assessment measures, and certain subject characteristics are identified that predict treatment outcome.
Unfortunately, in this type of study, treatment re-
sponsivity at the level of the individual is not determined. Improvement could be due to extraneous variables (real but uncontrolled sources of changes), to measurement inconsistencies (variation in the measurement process it- self), or to treatment effectiveness. It is generally assumed that extraneous variables and measurement inconsisten- cies are evenly distributed and are reflected in interin- dividual variability. Intergroup variation that is large rel- ative to intragroup variation is thus thought to be treat- ment related. At the level of the individual, however, knowledge about treatment-produced successes and fail- ures (widely agreed to be important, see Gendlin, 1986) cannot be identifed. Thus, any correlations found be- tween the improvement of individuals and their pretreat- ment characteristics mix all three sources of variability in the correlation (treatment, extraneous variables, and measurement inconsistency). It should be no surprise that such correlations tend to be low and inconsistently ob- tained.
One solution to this problem is to identify treatment responsiveness at the level of the individual, that is, to use individual time-series designs (Hayes, 1987). This ap- proach will probably require just as many subjects as the previous approach, but because individual assessment results will now be correlated with individually identified treatment effects, stronger external validity for post hoc correlations seems likely. Even so, the other problems with post hoc studies seem likely to continue.
Selection of measures. "Going fishing" with many premeasures and a mountain of data from a given treat- ment program is unlikely to yield highly useful relation- ships. Post hoc analyses of theoretically derived premea- sures are more likely to be useful because it is unlikely that chance correlations will emerge in systematic accord with theoretical expectations. When such measures are available, however, there may be enough conceptual clar- ity about the issues to warrant more powerful a priori research strategies.
Inconsistencies between the studied group and ap- plication. The post hoc approach is sensitive to any in- consistencies between the original study and formal cross- validation studies or the clinical environment itself. Thus, treatment utility cannot be assumed with post hoc studies until additional research or application has been done. In contrast, if a treatment utility relation is predicted a priori and successfully shown, then some degree of ro- bustness (external validity) in our conceptualization has already been documented (Hayes, 1987). It is to such a priori treatment utility strategies that we now turn.
A Priori Group Comparison Approaches: Single Dimension Studies
In a priori treatment utility studies, the assessment ques- tion is known before the data are collected, and the meth- ods are designed accordingly. There are several distinct types. We will first describe studies that can be conducted on single dimensions with group comparison approaches. Single dimension studies assess whether a specific assess- ment difference relates to treatment outcome. Most e x -
968 November 1987 �9 American Psychologist

perimental research that has been done on the treatment utility of assessment fits into this category, although few of these examples used the obtained data deliberately to evaluate assessment. There are three subtypes: manipu- lated assessment, manipulated use, and obtained differ- ences.
Manipulated assessment. In this type of study, as- sessment data are at issue. A single group of subjects is randomly divided into two or more subgroups, and either the collection or availability of assessment data is varied systematically. The therapist then designs and implements treatment in accord with the data available. For example, data from a particular device may be made available for only one subgroup. Differential outcomes between groups confirm the treatment utility of assessment characteristics manipulated. Manipulated assessment studies could ad- dress such questions as the treatment utility of the MMPI, multimodal assessment, projective tests, and so on.
Manipulated use. These studies are somewhat sim- ilar in design to manipulated assessment studies, but they differ fundamentally because the same assessment infor- mation is available for all subjects. The researcher ma- nipulates the way in which the assessment information is used. A study we conducted (Jarrett, Nelson, & Hayes, 1981) is one of a handful of examples and contains an instructive flaw. We attempted to compare an idiograph- ically based treatment of depression with a nomothetic approach. In the idiographic group, subjects received treatment modules that matched their specific weak- nesses. For example, a subject with frequent irrational thoughts received a cognitive module, subjects with poor social skills received a social skills module, and so on. In the nomothetic group, subjects received modules yoked to the iodiographic subjects.
The results showed no differential effect for treat- ment matching. In this study an interesting, and for our purposes, illuminating methodological problem was missed, however. Unfortunately, many in the yoked treatment group also (by chance) received needed treat- ment, as indicated by their pretreatment assessment. A manipulated use study can avoid this problem by adopting rules for the use of assessment data in one group and adopting contrary rules for their use in the other. For example, in one group treatment can be matched to as- sessment, and in the other treatment can be deliberately cross-matched with assessment. Two subsequent studies under these conditions have confirmed the value of id- iographic treatment matching for depression and for social inadequacy (McKnight, Nelson, Hayes, & Jarrett, 1984; Nelson, Hayes, Jarrett, & McKnight, 1983).
Obtained differences. In this third type of a priori study, subjects are divided into groups nonrandomly, based on assessment differences. Subjects then receive one type of treatment. If outcome differs between the groups, the treatment utility of subject differences is shown. This is a more common approach than the preceding two. It is the simplest experimental version of post hoc studies that seek to identify treatment responders and nonre- sponders. For example, Keller (1983) found that a group
of depressed community volunteers with low pretreat- ment scores on the Dysfunctional Attitude Scale (DAS; Weissman, 1980) showed a greater response to cognitive therapy than did their counterparts with high scores. Keller argued that these data contradict the notion that cognitive therapy is more "relevant" (better matched) to subjects with high scores on the DAS.
Note that these three types of studies all examine the interface between assessment and treatment by pro- ducing or observing differences in only one aspect of the assessment-treatment equation. In manipulated assess- ment studies, assessment or available assessment infor- mation varies, but ways in which available assessment information are used are the same. In manipulated use studies, assessment information is the same, but the link between assessment and treatment varies. In obtained difference studies, assessment outcomes are observed to vary, but both assessment methods and treatment are the same for all.
A Priori Group Comparison Approaches: Multiple Dimension Studies
More complex questions can be asked about the treatment utility of assessment by crossing the simpler types of questions just described (see Table 1). We term these "multiple dimension" studies. For example, groups de- veloped as in a manipulated assessment study can then be matched with treatment in two or more distinct ways. Such a manipulated-assessment/manipulated-use study asks if different available assessment information has varying effects on two or more methods of using assess- ment information. A practical example might be a study that asks if an individual functional analysis is more suc- cessful when direct measures of overt behavior are avail- able compared to when they are not. Similarly, in an obtained differences/manipulated use study, the use of available assessment information can be manipulated within two patient groups. A practical example might compare the effects of treating the most severe problem first in both depressed and agoraphobic populations. Other possible types of multiple dimension studies are shown in Table I.
Frequent examples exist for only one type of a priori multiple dimension study. One way obtained differences studies are elaborated is to cross distinct patient groups with two or more distinct treatment approaches. The resultant obtained differences/two-or-more-treatments study asks if two or more types of treatment interact with two or more types of patients. This approach is partic- ularly elegant when each patient group theoretically im- plies and is crossed with a distinct treatment approach. The resultant factorial design tests not only the treatment utility of the patient group distinctions but also the con- ceptual and theoretical distinctions that gave rise to them and their implied therapies.
Simons, Lustman, Wetzel, and Murphy (1985) have provided an illustration. These investigators divided the sample of depressed patients according to their pretreat- ment scores on Rosenbaum's (1980) Self-Control Scale.
November 1987 �9 American Psychologist 969

Subjects were treated (based on random assignment within patient types) with either cognitive therapy or a regimen of nortriptyline. Subjects with high scores on the Self-Control Scale showed a better response to cognitive therapy than those with low scores. In contrast, subjects with low scores on the Self-Control Scale showed a better response to nortriptyline than those with high scores. This is a particularly sophisticated example because the study was based on a theoretically significant distinction be- tween these two types of patients and a similar distinction between the two treatments used. Thus, the results vali- date not only the usefulness of the Self-Control Scale, but also, in part, the theoretical distinction on which the study was based. Other examples of this type of study have been provided by Abramowitz, Abramowitz, Roback, and Jackson (1974); Meichenbaum, Gilmore, and Fedoravi- cius (1971); Prusoff, Weissman, Klerman, and Rounsa- ville (1980); and Safran, Alden, and Davidson (1980).
A Priori Time-Series Approaches: Main Question Between Subject
In the various group comparison approaches to treatment utility, the relation between outcome and assessment is addressed at the level of the group. Unfortunately, as ar- gued earlier, most group comparison studies do not allow identification of those individuals who actually improved because of treatment per se. Indeed, the statistical mea- surement of outcome is a controversial matter in its own right (e.g., Cronbach, Gleser, Nanda, & Rajaratnam, 1972), and the concept of treatment utility does not ab- solve the researcher of the need to defend the statistical methods used to measure outcome.
The need to identify individual treatment responders c a n be solved by using time-series designs with all indi- vidual subjects (Barlow, Hayes, & Nelson, 1984). These individual analyses can be collapsed into conditions or groups. Researchers can then conduct the same types of studies outlined above, but in a more precise manner.
For example, in a manipulated assessment study, some subjects would receive treatment based on different assessment information than others, but all treatments would be analyzed within subject (e.g., through an A-B- A-B or other time-series design). By collecting many such subjects the researcher can (a) still analyze in a pre-post fashion, if desired; (b) identify at the level of the individual the successes and failures caused by treatment in each group; and (c) begin to correlate observed differences with treatment success and failure, given each assessment ap- proach. The main questions, however, remain between- subject questions because the manipulations are done be- tween subjects.
A Priori Time-Series Approaches: Main Question Within Subject
Questions about the treatment utility of assessment can also be asked using within-subject designs, except for those single dimension studies involving obtained differences. Such research usually requires the use of a design that enables two or more treatments to be compared within
subject. Many such designs exist (Barlow et al., 1984; Hayes, 1981), but perhaps the most powerful is the Al- ternating Treatment Design (ATD; Barlow & Hayes, 1979). The ATD consists of the random or semirandom alternation of two or more conditions where alternations are possible about once per meaningful unit of measure- ment. If measures are most meaningful when grouped by the week, for example, conditions should be capable of alternating about once each week (determined randomly or semirandomly). This allows differential treatment ef- fectiveness to be determined within an individual.
As an example, a manipulated assessment study could be done examining the impact of popular projective tests. Two sets of assessment data would be developed for each of several clients. One set could be based on a com- prehensive assessment battery without projectives whereas the second set would include projectives. Expert clinicians skilled in these types of assessment would devise a treat- ment program for each client, based on each of the two sets of data. If the two suggested programs were distinct, they both could now be delivered within subject in an ATD fashion. In this way one could determine the dif- ferential impact of these types of assessment data on treatment outcome. A wide variety of assessment devices, approaches, or packages could be assessed in this manner.
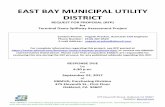
As another example, consider obtained differences- two or more treatments studies. In this type, subjects may be divided into types of subjects based on assessment data. Unlike a purely post hoc approach, however, relatively pure types can be sought and obtained, which allows for a less confounded examination of the relation between obtained differences and outcome. Two or more treat- ments are then applied within subject, and differential effects are assessed. An example is the study by McKnight et al. (1984). Subjects were obtained who were depressed and either had (a) poor social skills but few irrational cognitions, (b) irrational beliefs but adequate social skills, or (c) problems in both areas. After a short baseline, all subjects received both social skills training and cognitive therapy in an ATD fashion. The degree of self-reported depression is shown in Figure 1. As can be seen, the sub- jects with only social skills problems improved most fol- lowing social skills training, whereas the reverse was true for subjects with problems only in the cognitive area. Subjects with problems in both areas improved as rapidly in either condition. Thus, the suspected relation between these obtained differences and two types of therapies was confirmed.
Pseudo Treatment Utility: Manipulated Target Studies
There is a final and important type of study that does not truly evaluate the treatment utility of assessment, but appears to do so. It seems important to distinguish the treatment utility of assessment from therapeutically useful strategies in general. Often a given syndrome or disorder will contain several possible target behaviors. For example, in depression one could target overt social behavior, cog- nitive behaviors, and so on. If treatments that target cog- nitions are consistently superior to those that target social
970 November 1987 �9 American Psychologist

Figure 1 Differentia/Effectiveness of Cognitive Therapy and Social Skills Training for Three Types of Depressed Clients
Ad~pted from "Importance of Treating Individually-Assessed Response Classes in the Amelioration of Depression" by D. L. McKnight, R. O. Nelson, S. C. Hayes, & R. B. Jarrett, 1984, Behavior Therapy, 15, pp. 324,326, 329. Copyright 1984 by tt~e Association for Advanceme~ of Behavior Therapy. Used by permission.
behavior, one might be tempted to say that selecting cog- nition as a target behavior in depression has "treatment utility." Note, however, that this is not an evaluation of assessment because assessment is not used to determine the specific targets or the treatment received. In such studies, researchers may monitor the targets themselves, but they do nothing with this information other than to evaluate the impact of treatment. Manipulated target studies, although valuable, are not studies about the treatment utility of assessment.
The Theoretical Impact of Treatment Utility Research Treatment utility research sets the stage for important theoretical development, in part because it points out dif- ferences that are functionally important and thus require theoretical explanation. For example, there are undoubt- edly many functionally distinct subtypes of patients cur- rently mixed together in popular diagnostic systems. Yet even when researchers think they have reliably identified a distinct subtype, they do not know if the distinction is trivial until its treatment utility is established. Indeed, differential response to treatment is itself a good way to identify important patient subtypes in the first place.
Until the sources of treatment utility are identified, however, practices can have treatment utility and still not have much theoretical significance. Suppose, for example, that repeated assessment throughout the course of treat- ment can be shown to have some degree of treatment utility. Researchers would then have to identify the vari- ables that control or maximize the contribution that re- peated assessment makes to treatment effectiveness. They might examine whether it increases the probability that the clinician will engage in other behaviors (e.g., praising improvements), which in turn produce the therapeutic advantages. Researchers might see if the repeated assess- ment increases a client's contact with relative improve- ments, serving as an incentive for effective action. Thus, over time, treatment utility research should fuel concep- tual as well as technological progress as the processes re- sponsible for treatment benefits are identified.
The advantage of treatment utility research in this regard is twofold. First, it naturally guides researchers in the field toward theorizing based on nontrivial differences (i.e., those that actually make an impact on treatment outcome). Second, researchers examining a particular link between assessment and treatment usually will have some theoretical analysis that leads them to believe that there might be such a link. If it is found, the viability of the theoretical construction increases incrementally. If not, that is also revealing. The few available treatment utility studies already suggest that previous conceptualizations are often only partially confirmed (e.g., Trower et al., 1978), or fail to be confirmed at all (e.g., Keller, 1983). Thus, in addition to enhancing treatment outcome, treatment utility research can improve our understanding of behavior and contribute to clinical science.
Psychometric Criteria and Treatment Utility As noted earlier, the slow pace of research on the treat- ment utility of assessment may be due in part to the belief that such questions cannot be asked until all psychometric hurdles are cleared. Psychometrics is based fundamentally on the concepts of reliability and validity. Reliability refers to the consistency of scores obtained by the same persons when examined with a given assessment device under systematically changing circumstances (e.g., different times, different items, different examiners, different in- ternal divisions of the test). Validity refers to what an
November 1987 * American Psychologist 971

assessment device measures' and how well it does so (An- astasi, 1982). To put it another way, reliability deals with relations among scores on the same device, whereas va- lidity deals with relations among scores on different de- vices (Campbell & Fiske, 1959). Generalizability theory (Cronbach et al., 1972) more systematically categorizes the various types of reliability and validity as universes of generalization (e.g., across scores, item, time, setting, or method).
Reliability and validity are thus based on the con- sistency of measurement. Classical psychometrics views consistency as the hallmark of a good assessment device. In psychometric theory, an observed score is a composite of the true value plus measurement error. Often, the true score is taken to be a hypothetical entity, which is typically assumed to be enduring and stable because it supposedly reflects an enduring, stable, internal entity or trait. Clas- sical test theory (Lord & Novick, 1968) avoids the platonic connotations of true scores, but still translates quality assessment into an issue of the degree of underlying con- sistency. In short, psychometrics evaluates assessment structurally, not functionally.
Many types of consistency seem orthogonal to the issue of the treatment utility of assessment. For example, a measure could readily have treatment utility without internal consistency. 2 Suppose we measure the number of environmental stressors present in a client's life. There is no reason in general to suppose that clients who just lost a spouse will also have just been fired. Thus, high internal consistency should not necessarily be expected. This does not mean that clients with high degrees of en- vironmental stress will not respond differently to treat- ment than clients with low levels of environmental stress. Many kinds of psychometric criteria are not sufficient, and at times may not even be necessary, for treatment utility.
To take this point to its logical extreme, it is useful to recognize that there may even be times when an as- sessment process could have treatment utility without the assessment report having any reliability or validity what- soever. All psychometric evaluations are of assessment results (e.g., reports, diagnoses, scores, profiles) and not of the actual process of conducting an assessment (e.g., giving the test, watching the patient respond to it). There- fore, if this assessment process can have treatment utility, then some tests or procedures may be psychometrically invalid and still have treatment utility on that basis. This controversial claim can perhaps be seen in the belief, common among many clinicians, that projective tech- niques may be useful even if their reliability and validity are not readily established (Blatt, 1975; Zubin, Eron, & Schumen, 1965). Suppose that clinicians varied widely in the way they interpreted a particular projective test. Such a test could not have reliability or validity. If only the actual test report was at issue, the test also could not have treatment utility because the same test performance
2 The authors thank Marilyn Demerest for suggesting this example.
would lead to different scores, diagnoses, or profiles and thus to different treatment recommendations. Even so, the process of giving this "unreliable" test could have treatment utility. For example, in giving the test and in watching the client respond, the clinician may unwittingly learn more about the client's personality. The clinician might then behave more effectively in treatment even though he or she may be unable to verbalize the relation between the test, the client's personality, and the clinical decisions. In some ways, this possibility seems to match what many clinicians say about the use of projective de- vices in experienced clinical hands. Whether the claim could be supported is an empirical matter, but it is one that traditional psychometric evaluation cannot deter- mine. It is a treatment utility question that could be ad- dressed using a manipulated assessment study.
What this shows is that the relation between psy- chometric criteria and treatment utility is often open to question. Thus, there seems to be little reason to insist in principle that treatment utility must be the last step in the evaluation of a given assessment device, distinction, or approach. Treatment utility is shown by a well-designed study, regardless of the state of previous psychometric evaluations.
This is not to say that reliability and validity should be ignored in treatment utility research. Suppose a cli- nician devised a test, proceeded directly to an assessment of its treatment utility, and failed to find any. The failure could be due to poor reliability of various kinds, the lack of appropriate treatment, a lack of treatment integrity, or a host of other possible problems other than the prac- tical uselessness of the dimension the clinician was trying to measure. Thus, psychometric evaluations limit the possible sources of a failure to find treatment utility. It also seems reasonable to expect measures with good re- liability and validity to be more likely to have treatment utility, though this is largely an empirical question. Fur- thermore, it is impossible to build a science of assessment totally on treatment utility alone. Knowing the effect on treatment outcome itself requires assessment, and that means that treatment utility must ultimately be based on measures that are themselves not validated in this manner.
Once an aspect of assessment (e.g., a device, ap- proach, or distinction) has been shown to have treatment utility, it is also then possible to use traditional psycho- metric evaluations to expand the value of the finding. For example, suppose that a given measure has been shown conclusively to distinguish two subgroups of patients who respond differently to various treatments. If a second measure separates patients into virtually the same subgroups, then it must also have treatment utility. A problem comes in, however, when the relation between the two measures is only moderate. Then the treatment utility of the new measure cannot be assumed because it is not certain that the area of shared variability is itself responsible for the treatment utility shown with the first measure.
Treatment utility is not the only functionally based means by which to evaluate assessment. It is possible for
972 November 1987 �9 American Psychologist

assessment to p roduce descr ip t ions tha t cur ren t ly have no t r ea tmen t utility, bu t con t r ibu te to the unders tand ing of a given disorder. The degree to which assessment con- t r ibutes to the knowledge base may be thought o f as an issue of the "conceptua l ut i l i ty" o f assessment. Trea tment utility and conceptual uti l i ty are undoubted ly related, but they are dis t inguishable . For example , a device may con- t r ibute to t r ea tmen t ou t come (it has t r e a tmen t uti l i ty), but for theoret ical ly unc lear reasons (it does no t yet have conceptual utility). Similarly, a device may be theoretically useful and as yet be useless in te rms of t rea tment outcome. For present purposes , the po in t is s imply that there are i m p o r t a n t goals for assessment o ther than t r ea tmen t out- come. Trea tmen t ut i l i ty should not , therefore, be thought o f as the only functional grounds for evaluat ing assessment quality.
Summary Trea tmen t ut i l i ty provides the potent ia l for a science o f cl inical assessment tha t is bui l t on evidence o f successful con t r ibu t ions to t rea tment . As such, it is an i m p o r t a n t me thod o f examin ing the qual i ty o f a s s e s s m e n t - - o n e in which the word quali ty is direct ly re la ted to a central funct ion o f cl inical assessment. To date , the role o f t reat- men t ut i l i ty has been bur i ed by conceptua l confusion, poor ly a r t icu la ted methods , and inapprop r i a t e l inkage to s t ructura l psychomet r ic cri ter ia . The present ar t ic le was designed to help in these areas. Trea tment utility research has also been h indered by nonspecif ic types of therapy, nonspecific types o f assessment, unnecessary divisions between the role o f assessor and therapist , and an over- emphas i s on technique over conceptua l advancement . The t rends in the field all seem posit ive in these areas. Thus, the t ime now seems ripe for a vigorous expans ion of research on the contr ibut ion of assessment to t rea tment outcome. Because t r ea tmen t uti l i ty provides the pract ical basis for a concern with cl inical assessment, it seems im- por t an t to proceed rap id ly to its demons t ra t ion .
REFERENCES
Abramowitz, C. V, Abramowitz, S. 1., Roback, H. B., & Jackson, C. (1974). Differential effectivene~ of directive and nondirective group therapies as a function of client internal-external control. Journal of Consulting and Clinical Psychology, 42, 849-853.
Adams, J. (1972). The contribution of the psychological evaluation to psychiatric diagnosis. Journal of Personality Assessment, 36, 561- 566.
Altmaier, E. M., Ross, S. L., Leary, N. R., & Thornbrough, M. (1982). Matching stress inoculation's treatment components to clients' anxiety mode. Journal of Counseling Psychology, 29, 331-334.
Anastasi, A. (t982). Psychological testing (5th ed.). New York: Macmillan. Barlow, D. H., & Hayes, S. C.(1979). Alternating treatment design: One
strategy for comparing the effects of two treatments in a single subject. Journal of Applied Behavior Analysis, 12, 199-210.
Barlow, D. H., Hayes, S. C., & Nelson, R. O. (1984). The scientist- practitioner: Research and accountability in clinical and educational settings. New York: Pergamon.
Beutler, k E. (1979). Toward specific psychological therapies for specific conditions. Journal of Consulting and Clinical Psychology, 47, 882- 897.
Bersoff, D. N. (1973). Silk purses into sow's ears: The decline of psy-
chological testing and a suggestion for its redemption. American Psy- chologist, 28. 892-899.
Bielski, R., & Friedel, R. O. (1976). Prediction of tricyclic response. Archives of General Psychiatry, 33, 1479-1489.
Blatt, S. J. (1975). The validity of projective techniques and their research and clinical contribution. Journal of Personality Assessment, 39. 327- 343.
Bollard, J. (1982). A 2-year follow-up of bedwetters treated by dry-bed training and standard conditioning. Behaviour Research and Therapy, 20, 571-580.
Borkovec, T. D., Grayson, J. B., O'Brien, G. T., & Weerts, T. C. (1979). Relaxation training of pseudoinsomnia and idiopathic insomnia: An electroencephalographic evaluation. Journal of Applied Behavior Analysis, 12, 37-54.
Brown, R. A., & Lewinsohn, P. M. (1984). A psychoeducational approach to the treatment of depression: Comparison of group, individual, and minimal contact procedures. Journal of Consulting and Clinical Psy- chology, 52, 774-783.
Campbell, D. T., & Fiske, D. W. (1959). Convergent and discriminant validation by the multitrait-multimethod matrix. Psychological Bul- letin, 56, 81-105.
Chesney, M. A., & Tasto, D. L. (1975). The effectiveness of behavior modification with spasmodic and congestive dysmenorrhea. Behaviour Research and Therapy, 13, 245-253.
Cronbach, L. J., & Gleser, G. C. (1965). Psychological tests andpersonnet decisions (2nd ed.). Urbana: University of Illinois Press.
Cronbach, L. J., Gleser, G. C., Nanda, H., & Rajaratnam, N. (1972). The dependability of behavioral measures. New York: Wiley.
Daily, C. A. (1953). The practical utility of the clinical report. Journal of Consulting Psychology, 17, 297-302,
DiClemente, C. C. (1981). Self-efficacy and smoking cessation mainte- nance: A preliminary report. Cognitive Therapy and Research, 5, 175-187.
Dumas, J. E., & Wahler, R. G. (1983). Predictors of treatment outcome in parent training: Mother insularity and socioeconomic disadvantage. Behavioral Assessment, 5, 301-313.
Edwards, A. L. (1970). The measurement of personality traits by scales and inventories. New York: Holt, Rinehart & Winston.
Eider, J. P., Edelstein, B. A., & Fremouw, W. J. ( 1981). Client by treatment interactions in response acquisition and cognitive restructuring ap- proaches. Cognitive Therapy atut Research. 5, 203-210.
Ellsworth, R. B., Collins, J. E, Casey, N. A., Schoonover, R. A., Hickey, R. H., Hyer, L., Twemlow, S. W., & Nesselroade, J. R. (1979). Some characteristics of effective psychiatric treatment programs. Journal of Consulting and Clinical Psychology, 47. 799-817.
Forsyth, D. R. & Strong, S. R. (1986). The scientific study of counseling and psychotherapy: A unificationist view. American Psychologist, 41, 113-119.
Garfield, S. L., & Kurtz, R. (1973). Attitudes toward training in diag- nostic testing: A survey of directors on internship training. Journal of Consuhing and Clinical Psychology, 40, 350-355.
Garfield, S. L., & Kurtz, R. (1976). Clinical psychologists in the 1970s. American Psychologist, 31, 1-9.
Gendlin, E. T. (1986). What comes after traditional psychotherapy re- search? American Psychologist, 41, 131-136.
Hayes, S. C. (1981). Single-case experimental designs and empirical clinical practice. Journal of Consulting and Clinical Psychology. 49, 193-21 I.
Hayes, S. C. (1987). Strategies of research applicable to on-line clinical intervention. In A. M. McLane (Ed.), Classification of nursing di- agnoses (pp. 79-96). St. Louis: Mosby.
Hersen, M., & Bellack, A. S. (1977). Research and practice in social skills training. New York: Plenum.
Jarrett, R. B., Nelson, R. O., & Hayes, S. C. (1981, November). An initial investigation of treatment vatidity: A methodology for evaluating behavioral assessment. Paper presented at the meeting of the Asso- ciation for Advancement of Behavior Therapy, Toronto, Canada.
Kaplan, M. L., Colarelli, N. J., Gross, R. B., Leventhal, D., & Siegel, S. M. (1970). The structural approach in psychological testing. New York: Pergamon.
Kazdin, A. E. (t986). Editor's introduction to the special issue. Journal of Consulting and Clinical Psychology, 54. I.
November 1987 �9 A m e r i c a n Psychologist 973

Keller, K. E. (1983). Dysfunctional attitudes and cognitive therapy for depression. Cognitive Therapy and Research, 7, 437-444.
Korchin, S. J. (1976). Modem clinicalpsychology. New York: Basic Books. Korchin, S. J., & Schuldberg, D. ( 1981 ). The future of clinical assessment.
American Psychologist, 36, 1147-1158. Levitt, E. E. (1973). Internship versus campus: 1964 and 1971. Profes-
sional Psychology, 4, 129-132. Lord, E M., & Novick, M. R. (1968). Statistical theories of mental test
scores. Reading, MA: Addison-Wesley. Luborsky, L., Mintz, J., & Christoph, P. (1979). Are psychotherapeutic
changes predictable? Comparison of a Chicago counseling center pro- ject with a Penn psychotherapy project. Journal of Consulting and Clinical Psychology,, 47, 469-473.
McKnight, D. L., Nelson, R. O., Hayes, S. C., & Jarrett, R. B. (1984). Importance of treating individually-assessed response classes in the amelioration of depression. Behavior Therapy, 15, 315-335.
McLean, P. D. ( 1981 ). Matching treatment to patient characteristics in an outpatient setting. In L. P. Rehm (Ed.), Behavior therapy for depression (pp. 197-207). New York: Academic.
McReynolds, P. (1985). Psychological assessment and clinical practice: Problems and prospects. In J. N. Butcher & C. D. Spielberger (Eds.), Advances in personality assessment (Vol. 4, pp. 1-30). HiUsdale, N J: Erlbaum.
Meehl, P. E. (1959). Some ruminations on the validation of clinical procedures. Canadian Journal of Psychology, 13, 102-128.
Meehl, P. E. (1960). The cognitive activity of the clinician. American Psychologist, 15, 19-27.
Meichenbaum, D., Gilmore, J., & Fedoravicius, A. (1971). Group insight versus group desensitization in treating speech anxiety. Journal of Consulting and Clinical Psychology, 36, 410-421.
Miller, W. R., & Hester, R. K. (in press). Matching problem drinkers with optimal treatments. In W. R. Miller & N. Heather (Eds.), Treating addictive behaviors: Processes of change. New York: Plenum.
Miller, W. R., & Joyce, M. A. (1979). Prediction of abstinence, controlled drinking, and heavy drinking outcomes following behavioral self-con- trol training. Journal of Consulting and Clinical Psychology, 47, 773- 775.
Mischel, W. (1968). Personality and assessment. New York: Wiley. Moore, G. H., Bobbitt, W. E., & Wildman, R. W. (1968). Psychiatric
impressions of psychological reports. Journal of Clinical Psychology, 24, 373-376.
Nelson, R. O., & Hayes, S. C. (1979). Some current dimensions of be- havioral assessment. Behavioral Assessment, 1, 1-16.
Nelson, R. O., Hayes, S. C., Jarrett, R. B., & McKnight, D. L. (1983). The treatment utility of dimensions of social skills. Unpublished manuscript. (Available from R. O. Nelson, Department of Psychology, University of North Carolina at Greensboro, Greensboro, NC 27412)
Ost, L. G., Jerremalm, A., & Johansson, J. (1981). Individual response patterns and the effects of different behavioral methods in the treatment of social phobia. Behaviour Research and Therapy, 19, 1-16.
Paul, G. L. (1969). Behavior modification research: Design and tactics. In C. M. Franks (Ed.), Behavior Therapy. Appraisal and status (pp. 29-62). New York: McGraw-Hill.
Paykel, E. S., Prusoff, B. A., Klerman, G. L., Haskell, D., & DiMascio,
A. (1973). Clinical response to amitriptyline among depressed women. Journal of Nervous and Mental Disease, 156, 149-165.
Poole, A. D., Dunn, J., Sanson-Fisher, R. W., & German, G. A. (1981). The rapid smoking technique: Subject characteristics and treatment outcome. Behaviour Research and Therapy, 20, 1-7.
Prusoff, B. A., Weissman, M. M., Klerman, G. L., & Rounsaville, B. J. (1980). Research Diagnostic Criteria subtypes of depression: Their role as predictors of differential response to psychotherapy and drug treatment. Archives of General Psychiatry, 37, 796-801.
Rorer, L. G., & Widiger, T. A. (1983). Personality structure and assess- ment. Annual Review of Psychology, 34, 431-463.
Rosenbaum, M. (1980). A schedule for assessing self-control behaviors: Preliminary findings. Behavior Therapy, 11, 109-121.
Safran, J. D., Alden, L. E., & Davidson, P. O. (1980). Client anxiety as a moderator variable in assertion training. Cognitive Therapy and Research, 4, 189-200.
Shaw, B. E (1981). Matching treatment to patient characteristics in an inpatient setting. In L. P. Rehm (Ed.), Behavior therapy for depression (pp. 209-229). New York: Academic.
Shahan, A., & Merbaum, M. (1981). The interaction between subject characteristics and self-control procedures in the treatment of inter- personal anxiety. Cognitive Therapy and Research, 5, 221-224.
Shealy, R. C., Lowe, J. D., & Ritzler, B. A. (1980). Sleep onset insomnia: Personality characteristics and treatment outcome. Journal of Con- suiting and Clinical Psychology, 48, 659-661.
Shemberg, K., & Keeley, S. (1970). Psychodiagnostic training in the psychiatric setting: Past and present. Journal of Consulting and Clinical Psychology, 34, 205-211.
Simons, A. D., Lustman, P. J., Wetzel, R. D., & Murphy, G. E. (1985). Predicting response to cognitive therapy of depression: The role of learned resourcefulness. Cognitive Therapy and Research, 9, 79-90.
Strassberg, D. S., Reimherr, E, Ward, M., Russell, S., & Cole, A. ( 1981 ). The MMPI and chronic pain. Journal of Consulting and Clinical Psychology, 49, 220-226.
Trower, P., Yardley, K., Bryant, B. M., & Shaw, P. (1978). The treatment of social failure: A comparison of anxiety-reduction and skills-ac- quisition procedures on two social problems. Behavior Modification, 2, 41-50.
VandenBos, G. R. (1986). Psychotherapy research: A special issue. American Psychologist, 41, 111-112.
Wallen, R. W. (1956). Clinical psychology: The study of persons. New York: McGraw-Hill.
Weissman, A. N. (1980, April). Assessing depressogenic attitudes: A validation study, Paper presented at the meeting of the Eastern Psy- chological Association, Hartford, CT.
Wiggins, J. S. (1973). Personality and prediction: Principles of personality assessment. Reading, MA: Addison-Wesley.
Williams, S. L., Dooseman, G., & Kleifield, E. (1984). Comparative effectiveness of guided mastery and exposure treatments for intractable phobias. Journal of Consulting and Clinical Psychology, 52, 505-518.
Woodward, R., & Jones, R. B. (1980). Cognitive restructuring treatment: A controlled trial with anxious patients. Behaviour Research and Therapy, 18, 401--407.
Zubin, J., Eron, K. D., & Schumen, E (1965). An experimentalapproach to projective techniques. New York: Wiley.
974 N o v e m b e r 1987 �9 A m e r i c a n Psychologis t