The Treatment of the Axilla in the North of England Cancer Network. Henry Cain ST7 North Tyneside.
31
The Treatment of the Axilla in the North of England Cancer Network. Henry Cain ST7 North Tyneside.
-
Upload
florence-cooper -
Category
Documents
-
view
219 -
download
0
Transcript of The Treatment of the Axilla in the North of England Cancer Network. Henry Cain ST7 North Tyneside.

The Treatment of the Axilla in the North of England Cancer
Network.
Henry Cain ST7 North Tyneside.

• Current national and local guidelines.• Results of NECN axillary surgery audit.• Application of results in view of published
evidence (Z0011 and beyond)
National Guidelines regarding the staging of the Axilla.
UK- ABS Guidelines 2009 “All patients diagnosed with invasive breast cancer undergoing surgical treatment should have a pre-
operative axillary ultrasound scan, and if appropriate FNA or core biopsy should be carried out.”
“If a positive non-operative diagnosis of axillary nodal metastasis is made in a patient undergoing surgery for breast cancer, the patient should normally proceed to an axillary clearance”
“Sentinel node biopsy using the combined blue dye/radioisotope technique is a recommended axillary staging procedure for the majority of patients with early invasive breast cancer”
“When axillary node clearance is carried out, the level of anatomical dissection should be specified, and at least 10 nodes should be retrieved”
“Axillary recurrence should be minimised by effective staging and treatment where appropriate Minimum standard <5% axillary recurrence at 5 years Target <3% axillary recurrence at 5 years”

Local Guidelines regarding the staging of the Axilla.
NECN Breast Cancer Guidelines 2011
“SLNB is the standard of care for staging the axilla.”
“Pre-operative Axillary USS give additional pre-operative staging information”
“Patients with proven Histologically malignant lymph nodes are not suitable for SLNB”

Current National Guidelines for the treatment of the positive axilla.
UK- ABS Guidelines 2009‘if the SLN is positive (macro/micro-metastasis), further axillary
treatment (cALND or RT) as well as adjuvant systemic therapy is recommended
UK- NICE Guidelines 2009‘cALND is preferred - gives additional staging information’
USA- ASCO Guidelines 2005Panel recommends cALND for macro/micro-metastases regardless of
the method of detection.

Local Guidelines regarding the treatment of the positive axilla.
NECN Breast Cancer Guidelines 2011“Further treatment should be offered to patients with a
pre-operative diagnosis of metastatic cancer in the axillary nodes or who have micro or macro mets in the
SLNB.”
“ The preferred technique is ALND because it gives additional staging information. When further surgery is
deemed inappropriate the radiotherapy may be considered”
North of England Cancer Network Prospective Audit of Sentinel Lymph Node Biopsy and
Axillary Clearance for Breast Cancer• Audit compliance with local and national guidelines of pre-
operative axillary staging, sentinel lymph node identification, and axillary treatment following identification of a positive SLNB
• Audit adequacy of ALNC • Investigate the role of SLNB for large breast cancers• Investigate the value of ALNC following identification of axillary
lymph node micro-metastasis• Asses the value of intra-operative sentinel lymph node analysis

Results of the NCN Axillary surgery Audit.
• 480 patients included. • Data from Northumbria, North Tees and
Hartlepool, James Cook and Friarage, Cumbria, Sunderland and RVI.
• Age range 20-91 (mean 61)• 64% symptomatic, 36% screening.

Results.Tumour details where available.
Tumour Type Not recorded 19 (4%)
DCIS 38 (8%)
Invasive Ductal 350 (73%)
Invasive none ductal 73 (15%)
Tumour Size 0-19 mm 221 (47%)
20-50mm 205 (44%)
>50mm 43 (9%)
Tumour Grade 1 62 (14%)
2 216 (49%)
3 165 (37%)
LVI Yes 106 (24%)
No 349 (76%)

Pre-op Staging.
• 450 recorded.• 445 pre-op USS.• 5 no staging.• 7 additional MRI information.• 1 additional CT information.

Results of Pre-op Staging
Staging results.
N=445
USS normal 323
USS abnormal n=122
FNA 75
Core Bx 43
Both 4
Pathological Sample
Negative. 59
Positive. 63 (51%)
• 361 patients proceeded to SLNB following negative staging.
• 58 patients underwent ANC due to positive pre-op staging.

Sentinel Node Biopsy Technique.
• 400 recorded 277 (69%) dual technique.• 33 blue dye only.• 90 radio-isotope only. • 2 documented as failed > ANS/Clearence.• 1- 15 sentinel nodes taken (mode 1) • None sentinel (or sample) nodes taken in
addition to sentinel node in 42 cases.
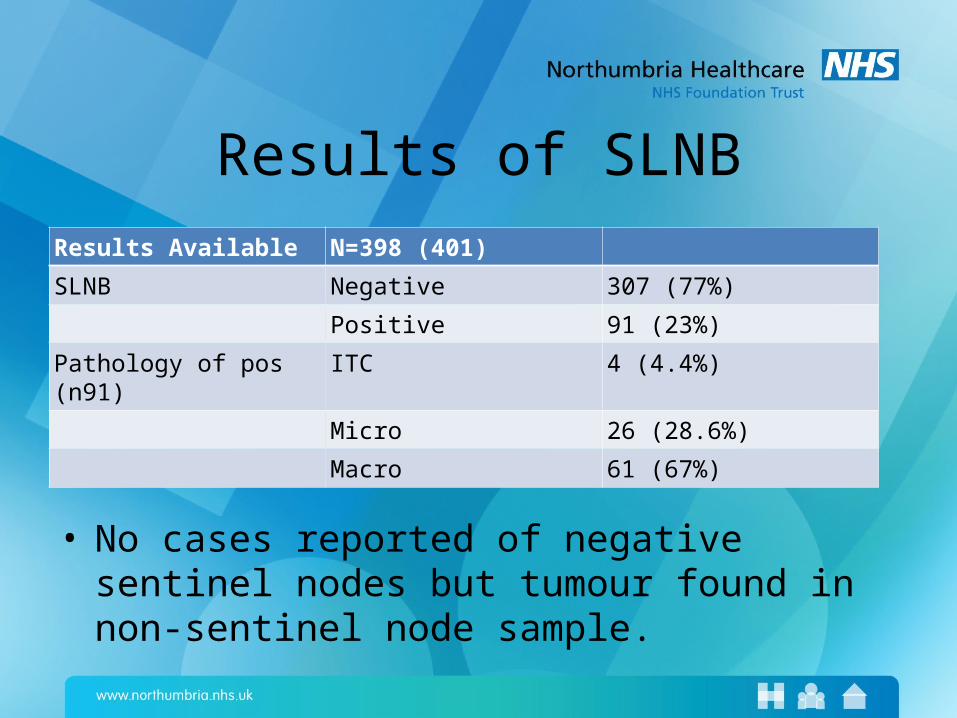
Results of SLNBResults Available N=398 (401)
SLNB Negative 307 (77%)
Positive 91 (23%)
Pathology of pos (n91) ITC 4 (4.4%)
Micro 26 (28.6%)
Macro 61 (67%)
• No cases reported of negative sentinel nodes but tumour found in non-sentinel node sample.

Treatment of positive SLNB
SLNB result No treatment ANC DXT ANC&DXT
Positive (91) 13 (14%) 57 (63%) 20 (22%) 1 (1%)
ITC (4) 3 1
Micro met (26) 5 (19%) 16 (61%) 4 (15) 1 (4%)
Macro met (61) 4 (7%) 40 (66%) 17 (28%) 0

Axillary Lymph Node Clearance.
ANC results N=125
Indication Pos pre-op 58 (46%)
Pos SLNB 50 (40%)
Pos intra op ass 4 (3%)
Other 13 ( 11%)
Nodes Removed Mode 13
< 10 nodes 26 (20%)

Results of ANC for positive SLNBSLNB result ANC negative ANC Positive
Positive (n50) 39 (78%) 11 (22%)
ITC (n1) 0 1 (100%!!) (3/5)
Micro (n15) 12 (80%) 3 (20%)
Macro (n34) 27 (79%) 7 (21%)
• 8/11 had 3 or less further nodes.• 2 had 4 further positive nodes.• 1 had 5 further positive nodes.• Micro mets 2= 1 node , 1 = 2 nodes.• No significant predictive value for tumour type, size, grade or
LVI.

Intra-operative Assessment.Intra op ass
(n=91)SLNB
negativeSLNB
postiveMicro Macro
Negative 75 (87%) 12 (13%) 3 9
Positive 0 4 (100%) 1 3
•Of the 12 false negatives 9 went on to have ANC following positive SLNB•Of the 4 positive intra op assessment all went on to have ANC.•Of these 2 were negative •1 had 1 micro met in 20 nodes •1 had 5/13 macro mets. •Sensitivity 25%, Specificity 100%, PPV 100%, NPV 86%

Results of pre op staging.
• 22% cases false negative pre op staging overall but 15% for macro mets alone. • Sensitivity 39%, Specificity 98% PPV=90% NPV 78%• 52/112 cases of positive axilla were identified by pre-op staging (46%)
Pre op ass
(n=419)
SLNB or ANC
negative
SLNB or ANC
positive
ITC Micro Macro
Negative (n361)
281 80 (22%)
3 22 55 (15%)
Positive (n=58)
6(10%) 52
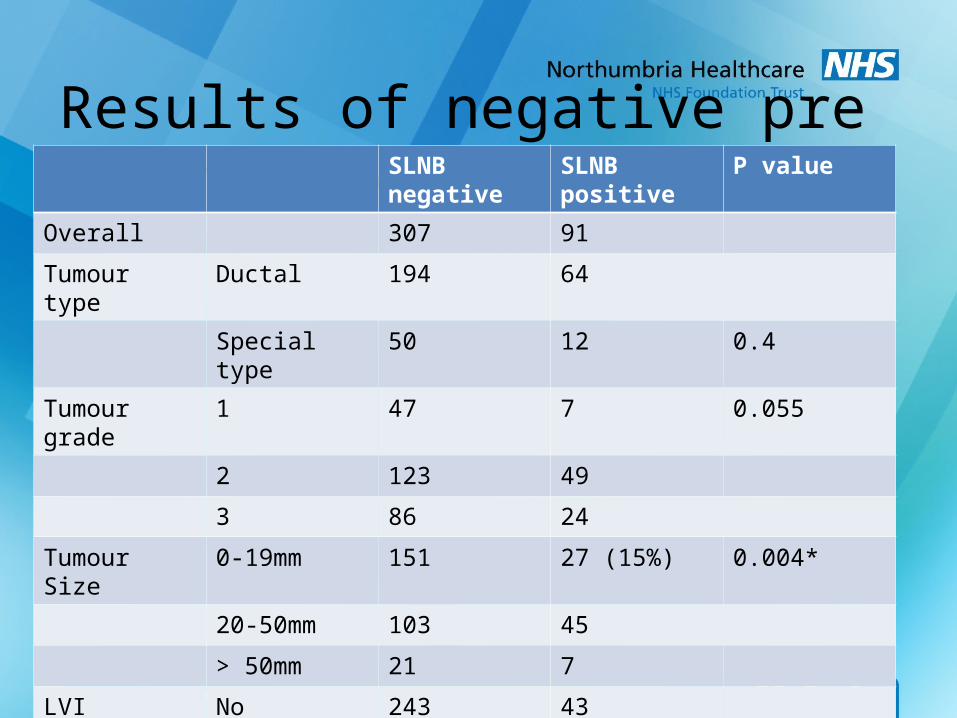
Results of negative pre op staging. SLNB negative SLNB positive P value
Overall 307 91
Tumour type Ductal 194 64
Special type 50 12 0.4
Tumour grade 1 47 7 0.055
2 123 49
3 86 24
Tumour Size 0-19mm 151 27 (15%) 0.004*
20-50mm 103 45
> 50mm 21 7
LVI No 243 43
Yes 24 33 (58%) <0.0001*
Pre op FNA/Bx No 238 72
Yes 43 8 0.3

SLNB in T3 tumours
• 28/43 underwent SLNB• 8/28 (29%) positive 6 went on to ANC• 12/43 positive pre op staging went on to ANC.• 20 ANC 14 (70%) positive

Summary
• Excellent rate of pre-op staging with adequate effectiveness.
• SLNB applied in majority of cases.• 23% of SLNB positive.• 20% of ANC for micro mets had further disease.• 21% of ANC for macro mets had further disease.

North of England Cancer Network Prospective Audit of Sentinel Lymph Node Biopsy and
Axillary Clearance for Breast Cancer• Audit compliance with local and national guidelines of pre-
operative axillary staging, sentinel lymph node identification, and axillary treatment following identification of a positive SLNB
• Audit adequacy of ALNC • Investigate the role of SLNB for large breast cancers• Investigate the value of ALNC following identification of axillary
lymph node micro-metastasis• Asses the value of intra-operative sentinel lymph node analysis

Axillary conservation
• We accept local recurrence rates of 5-10%over 10 years following breast conservation and RT
• So why do we agonise over axillary recurrence rates of 1-2% over 5 years after SLNB
• Especially as the evidence that axillary recurrence rates translate to survival differences is hard to come by?
• Yet the morbidity of ALND is all too clear

Case for ANC.
cALND is therapeutic– SLNB is a staging test only so require cALND to
eradicate any residual axillary disease – Improves local disease control– Improves survival
cALND gives additional useful prognostic information– Total nodal disease burden– This information helps refine adjuvant treatment

Case against ANC• Majority do not have further nodal disease
– Minimal additional prognostic information– Now have better biological prognostic markers
• Residual axillary disease does not translate into local recurrence– Evidence that ALND has survival gain in any BC patient is
limited
• cALND represents overtreatment with substantial morbidity

Is there a group of patients that following a positive SLNB be spared and ANC?
• Relevant Studies.• Z0011.• Application to these Audit results.

RCT into Treatment of positive SLNB • ACOSOG Z0011
– Local recurrence, OS and DFS is equivalent for low burden (micro and macro), H&E detected SLN disease, with or without cALND after median FU 6yrs
• Guiliano et al Annals of Surgery 2010 252(3) 426-433• Guiliano et al JAMA 2011 305 (6) 569-606
• IBCSG Trial 23-01 SABCS 2011– Local recurrence, OS and DFS is equivalent for
VERY low burden (micro and ITC), IHC or F/S detected disease with or without ALND after median FU 5 years

Z0011Randomised trial to establish role of cALND in SLN
positive patients 1999-2004
SLN +ve (H&E) randomised to cALND or not. – All T1/T2 ( <5cm): BCT +RT– Adjuvant therapy not controlled (at discretion)– Compared OS,DFS, loco-regional control
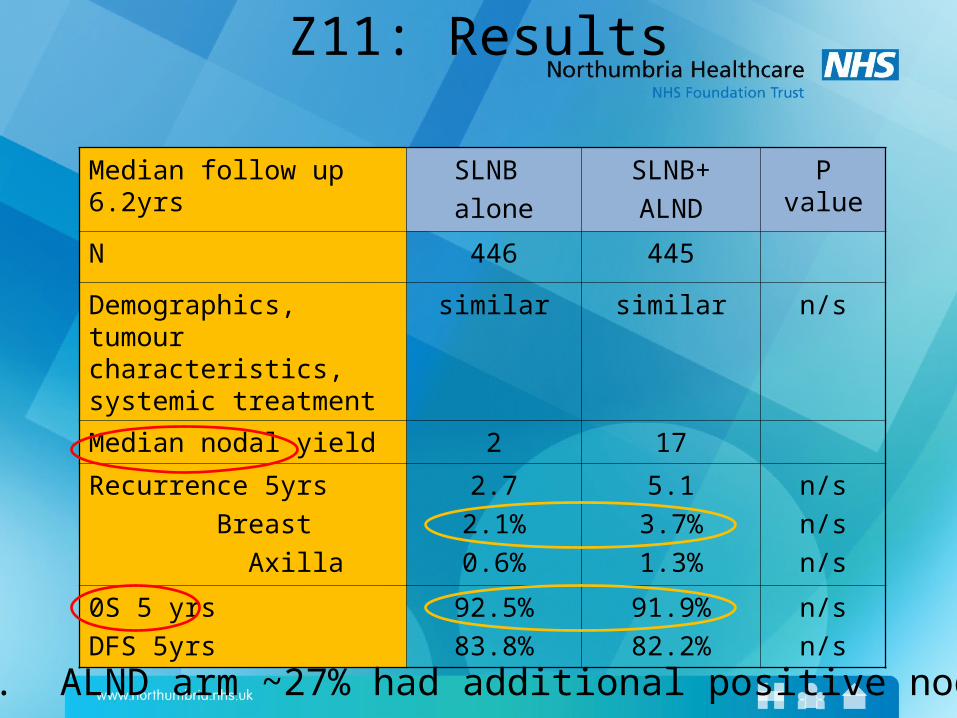
Z11: Results
Median follow up 6.2yrs SLNB
alone
SLNB+
ALND
P value
N 446 445
Demographics, tumour characteristics, systemic treatment
similar similar n/s
Median nodal yield 2 17
Recurrence 5yrs
Breast
Axilla
2.7
2.1%
0.6%
5.1
3.7%
1.3%
n/s
n/s
n/s
0S 5 yrs
DFS 5yrs
92.5%
83.8%
91.9%
82.2%
n/s
n/s
*NB. ALND arm ~27% had additional positive nodes

Application Z0011 to our results.
• Difficult due to limitations in audit regarding surgery type and adjuvant DXT but...
• Similar pos ANC following pos SLNB.• Flaws with Z0011 but best we have at the
moment.• Future trials awaited AMAROS & POSNOC??• Can pts afford for us to wait?

Thank you.