
The Theory of Planned Behavior and Breast Self-Examination: Distinguishing Between Perceived Control...
15
The Theory of Planned Behavior and Breast Self-Examination: Distinguishing Between Perceived Control and Self-Efficacy PAUL NORMAN1 AND SARAH HOYLE University of Sheffield Sheffield, United Kingdom This paper reports an application of the theory of planned behavior (TPB) to the prediction of breast self-examination (BSE) intentions and behavior. The study also considered the distinction between perceived control and self-efficacy within the TPB and the additional predictive utility of past behavior. A sample of 95 women completed questionnaires based on the TPB and were followed up at I month. Support for the distinction between per- ceived control and self-efficacy was provided by principal components analysis. The TPB was found to he highly predictive of intention to perform BSE and subsequent BSE behav- ior. Regression analyses revealed self-efficacy and attitude to be predictive of intention to perform BSE. Intention, in turn, was the sole predictor of BSE at 1 -month follow-up. Past behavior was found to explain additional variance in intention, hut not BSE behavior at I-month follow-up. The results are discussed in relation to the conceptual status of the perceived behavioral control construct, and the practical implications of the results are highlighted. Breast cancer is one of the major causes of death among women (Heimann, Bradley, & Hellman, 1998). In the United Kingdom, 1 in 12 women will develop breast cancer during her lifetime (Steel, Cohen, & Porter, 1992). In the absence of primary prevention strategies, regular screening remains the best form of defense against the disease (American Cancer Society, 2002). Breast self-examination (BSE) is a low-cost and relatively simple activity that can be performed in con- junction with mammography or clinical breast examination. Regular (i.e., monthly) BSE has been associated with the detection of smaller tumors that are at a more favorable clinical stage (Hill, White, Jolley, & Mapperson, 1988). In turn, the early detection of breast cancer substantially increases survival rates (American Cancer Society, 2002). The performance of monthly BSE is therefore currently recommended for women aged 20 to 39 years, in addition to a clinical breast examination every 3 years, and for women aged 40 years and over, in con- junction with an annual mammogram and clinical breast examination (American 'Correspondence concerning this article should be addressed to Paul Norman, Department of Psychology, University of Sheffeld, Sheffield S 10 2TP, United Kingdom. E-mail: p.norman@ sheffield.ac. uk 694 Journal of Applied Social Psychology, 2004, 34, 4, pp. 694-708. Copyright 0 2004 by V. H. Winston & Son, Inc. All rights reserved
-
Upload
paul-norman -
Category
Documents
-
view
213 -
download
1
Transcript of The Theory of Planned Behavior and Breast Self-Examination: Distinguishing Between Perceived Control...

The Theory of Planned Behavior and Breast Self-Examination: Distinguishing Between Perceived
Control and Self-Efficacy
PAUL NORMAN1 AND SARAH HOYLE University of Sheffield
Sheffield, United Kingdom
This paper reports an application of the theory of planned behavior (TPB) to the prediction of breast self-examination (BSE) intentions and behavior. The study also considered the distinction between perceived control and self-efficacy within the TPB and the additional predictive utility of past behavior. A sample of 95 women completed questionnaires based on the TPB and were followed up at I month. Support for the distinction between per- ceived control and self-efficacy was provided by principal components analysis. The TPB was found to he highly predictive of intention to perform BSE and subsequent BSE behav- ior. Regression analyses revealed self-efficacy and attitude to be predictive of intention to perform BSE. Intention, in turn, was the sole predictor of BSE at 1 -month follow-up. Past behavior was found to explain additional variance in intention, hut not BSE behavior at I-month follow-up. The results are discussed in relation to the conceptual status of the perceived behavioral control construct, and the practical implications of the results are highlighted.
Breast cancer is one of the major causes of death among women (Heimann, Bradley, & Hellman, 1998). In the United Kingdom, 1 in 12 women will develop breast cancer during her lifetime (Steel, Cohen, & Porter, 1992). In the absence of primary prevention strategies, regular screening remains the best form of defense against the disease (American Cancer Society, 2002). Breast self-examination (BSE) is a low-cost and relatively simple activity that can be performed in con- junction with mammography or clinical breast examination. Regular (i.e., monthly) BSE has been associated with the detection of smaller tumors that are at a more favorable clinical stage (Hill, White, Jolley, & Mapperson, 1988). In turn, the early detection of breast cancer substantially increases survival rates (American Cancer Society, 2002). The performance of monthly BSE is therefore currently recommended for women aged 20 to 39 years, in addition to a clinical breast examination every 3 years, and for women aged 40 years and over, in con- junction with an annual mammogram and clinical breast examination (American
'Correspondence concerning this article should be addressed to Paul Norman, Department of Psychology, University of Sheffeld, Sheffield S 10 2TP, United Kingdom. E-mail: p.norman@ sheffield.ac. uk
694
Journal of Applied Social Psychology, 2004, 34, 4, pp. 694-708. Copyright 0 2004 by V. H. Winston & Son, Inc. All rights reserved
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 695
Cancer Society, 2002). However, despite the high risk of developing breast cancer and the efficacy of BSE to detect the disease at an early stage, many women do not perform BSE on a regular basis (Friedman, Nelson, Webb, Hoffman, & Baer, 1994; Murray & McMillan, 1993). Therefore, it is important to identify the psychosocial predictors of BSE. One model that may be usefully employed in this context is the theory of planned behavior (TPB; Ajzen, 1988, 1991).
The TPB is one of the most widely applied models of health and social behavior (Ajzen, 2001; Armitage & Conner, 2001). According to the TPB, the proximal determinant of an individual’s behavior is his or her intention to per- form the behavior. This construct reflects the individual’s motivation to perform the behavior, and individuals with strong intentions are likely to exert more effort to engage in the behavior. Intention, in turn, is determined by three constructs. The first construct is the individual’s attitude toward or evaluation of performing the behavior. The second construct is the individual’s perception of the extent to which important others would approve of him or her performing the behavior (i,e., subjective norm). The third construct is the individual’s perception of con- trol over performing the behavior (i.e., perceived behavioral control). Thus, indi- viduals who have a positive evaluation of performing a behavior, who believe that important others would approve of them performing the behavior, and who perceive performance of the behavior to be under their control are likely to have strong behavioral intentions. The last of these three constructs, perceived behav- ioral control (PBC), was added to an earlier version of the model (i.e., theory of reasoned action, TRA; Ajzen & Fishbein, 1980) to extend the model to the pre- diction of nonvolitional behaviors.
As Ajzen (1988) argued, most behaviors are not under complete volitional control and are therefore subject to some degree of uncertainty. As a result, Ajzen proposed that PBC may have a direct effect on behavior that is unmediated by behavioral intention and presented two lines of argument to support this pro- posal. First, controlling for intention, high levels of PBC are likely to lead to suc- cessful behavioral performance because individuals with high levels of PBC are more likely to persist in the face of obstacles to the behavior. Second, PBC may be taken as a proxy measure for actual control. Thus, for those behaviors that are low in control, individuals’ ability to translate their intentions into behavior may be reduced.
The TPB has been applied extensively to the prediction of health and social behavior (for reviews, see Ajzen, 2001; Armitage & Conner, 2001; Conner & Armitage, 1998). Meta-analyses have indicated that the TPB explains between 40% and 50% of the variance in intention, and between 23% and 34% of the vari- ance in behavior (Sutton, 1998). Moreover, the addition of PBC to the model has received strong support. For example, Godin and Kok (1996) reported, in a meta- analysis of studies on the TPB and health behavior, on average, PBC explained
696 NORMAN AND HOYLE
an additional 13% of the variance in intention and an additional 13% of the vari- ance in behavior over and above the influence of TRA variables.
However, to date, there have been relatively few studies applying the TPB to the prediction of BSE intentions and behavior. Those studies that have been conducted provide support for the TPB, although they possess a number of short- comings. Van Ryn, Lytle, and Kirscht (1 996) employed a measure of self- efficacy in lieu of a measure of PBC and found that attitude, subjective norm, and self-efficacy were all significant independent predictors of BSE intentions. Inten- tion, in turn, was found to predict BSE at 6-month follow-up, although it should be noted that the behavioral measure in this study was “trying to perform BSE,” rather than actual BSE performance. McCaul, Sandgren, O’Neill, and Hinsz (1993) found that attitude and PBC were predictive of intention to perform BSE and that intention was the sole predictor of BSE at 3-month follow-up. However, in this study, the TPB variables were measured as part of an intervention study after women had received a health education session to promote BSE. Orbell, Hodgkins, and Sheeran (1 997) reported an application of the TPB to the predic- tion of BSE at 1-month follow-up, also as part of an intervention study, and again found that intention was the sole predictor of behavior. However, the results for the prediction of intention were not reported.
Despite the success of the TPB, a growing number of researchers have ques- tioned the conceptual clarity of the PBC construct (e.g., Armitage & Conner, 1999a, 1999b; Manstead & van Eekelen, 1998; Terry & O’Leary, 1995). In par- ticular, it is possible to make a distinction between perceptions of one’s ability to perform a behavior (i.e., self-efficacy) and perceptions of control over a behavior (i.e., perceived control). This distinction can be seen in Ajzen’s (1991) writings on the ways in which PBC may have a direct effect on behavior. First, PBC might be related to behavioral performance because individuals with high levels of per- ceived control are more likely to persist in the face of obstacles to the behavior. This conceptualization of PBC is similar to Bandura’s (1 977, 1986) notion of self-efficacy. Individuals with a strong sense of self-efficacy approach difficult goals, have a strong commitment to their goals, maintain a task focus, persist in the face of failure, and attribute failure to a lack of effort. Thus, a belief in one’s ability to perform a behavior is likely to facilitate behavioral performance. Sec- ond, PBC may act as a proxy measure for actual control, and behaviors that are subject to environmental constraints may be more difficult to perform. Thus, to the extent that perceptions of control over performance of a behavior are accu- rate, PBC will directly predict behavior. This conceptualization of PBC has more in common with Rotter’s (1966) locus of control construct, which focuses on individuals’ perceptions of control over the environment.
The empirical case for distinguishing between self-efficacy and perceived control has been examined in a number of studies that have conducted factor analyses of PBC items in relation to dietary behavior (Armitage & Conner,
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 697
1999a, 1999b; Povey, Conner, Sparks, James, & Shepherd, 2000), drug use (Armitage, Conner, Loach, & Willetts, 1999), exercise (Terry & O’Leary, 1995), condom use (White, Terry, & Hogg, 1994), and the achievement of high school grades (Manstead & van Eekelen, 1998). These studies have shown that items focusing on individuals’ confidence in their ability to perform a behavior (e.g., “I am confident that I can perform the behavior”) can be separated from items focusing on individuals’ perceptions of control over the behavior (e.g., “How much control do you have over whether or not you perform the behav- ior?”).
Trafimow, Sheeran, Conner, and Finlay (2002) presented a range of experi- mental evidence to further support such a distinction. In a series of studies, they examined the distinction between perceived control (i.e., the extent to which an individual perceives the performance of a behavior to be under his or her voli- tional control) and perceived difficulty (i.e., the extent to which an individual perceives the performance of a behavior to be easy or difficult, which may equated with self-efficacy). Trafimow et al. demonstrated, for example, that it is possible to conduct manipulations that affect perceived control more than per- ceived difficulty, and vice versa. Furthermore, they found significant clustering of beliefs by type in a recall task suggesting that people form strong associations within but not between control and difficulty beliefs. Therefore, their findings provide strong support for the distinction between self-efficacy and perceived control.
Self-efficacy and perceived control also may have different relationships with intention and behavior. Terry and O’Leary (1995) argued that perceived control should have a direct effect on behavior, as external constraints may prevent individuals acting on their intentions. In addition, perceived control should be related to intention, as it is unlikely that individuals will intend to perform behaviors over which they believe they have little control. However, self-efficacy may only influence behavior via intention. According to Bandura (1 977), self- efficacy is a central determinant of motivation (i.e., intention). Individuals are unlikely to be motivated to perform a behavior when they lack confidence in their ability to perform the behavior. In addition, Bandura proposed that the influ- ence of self-efficacy on subsequent behavior should be mediated fully by motiva- tion. Thus, a direct relationship is not expected between self-efficacy and behavior.
Terry and O’Leary (1995) tested these predictions in a longitudinal study on exercise behavior. They found that self-efficacy was predictive of intention to exercise, whereas perceived control and intention were predictive of exercise behavior. Subsequent tests of these relationships have failed to fully replicate Terry and O’Leary’s findings. Self-efficacy, but not perceived control, is typi- cally found to be predictive of intention (Armitage & Conner, 1999a, 1999b; Armitage et a]., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000; White
698 NORMAN AND HOYLE
et al., 1994),2 whereas intention usually emerges as the sole significant indepen- dent predictor of behavior (Armitage & Conner, 1999a, 1999b; White et al., 1994, for condom use), although some studies have also reported direct effects for self-efficacy (Armitage et al., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000).
The TPB also has been criticized for failing to fully mediate the influence of past behavior. Past behavior is typically found to be the strongest predictor of future behavior, explaining variance over and above the influence of TPB vari- ables (Ajzen, 1991; Conner & Armitage, 1998; Ouellette & Wood, 1998). A meta-analysis conducted by Conner and Armitage indicated that past behavior explains, on average, an additional 13% of the variance in behavior, and an addi- tional 7.2% of the variance in intention over and above TPB variables. It has been suggested that past behavior should be included as an independent predictor variable in the TPB (e.g., Bentler & Speckart, 1979), although Ajzen (1987) argued that past behavior has no explanatory value in itself. Instead, Ajzen (1 988) argued that the influence of past behavior should be mediated by TPB variables. When past behavior is found to have a direct effect, this may be taken as evidence that the model is not sufficient and may benefit from the inclusion of additional variables (Ajzen, 1987).
The present study examines the predictive utility of the TPB in relation to BSE intentions and behavior. The study also considers the distinction between self-efficacy and perceived control and the sufficiency of the model as assessed by the influence of past behavior. It is predicted that the TPB will be predictive of BSE intentions and BSE performance at 1-month follow-up, but that the addition of past behavior will increase the amount of variance explained.
Method
Respondents and Procedure
A telesales company in the United Kingdom was approached to participate in the research. Questionnaires were distributed to 200 female employees at one of the company’s worksites. The women took away the questionnaires to complete in their own time and returned them to a deposit box at the worksite. Completed questionnaires were returned by 144 women (72.0% response rate). One month later, a second questionnaire was distributed to these women, and 95 completed
?A number of these studies have reported that perceived control has a significant negative beta weight in regression analyses (Armitage & Conner, 1999a, 1999b; Armitage et a]., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000). However, in such cases, it is likely that the significant beta weight was a result of a suppressor effect, as the bivariate correlation between perceived control and intention was positive (Tabachnick & Fidell, 1996).
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 699
questionnaires were returned (66.0% response rate). The mean age of the sample was 39.91 years, and respondents’ ages ranged from 18 to 63 years.
Measures
The Time 1 questionnaire included direct measures of the components of the TPB constructed in line with recommendations (Ajzen & Fishbein, 1980; Conner & Sparks, 1996). All of the TPB items were scored using 7-point response scales, ranging from -3 to +3, and coded so that high scores indicated high levels on the variable of interest.
Attitude. Respondents’ attitude toward performing BSE in the next month was assessed using four semantic differential scales. Each item began with the statement “For me to perform BSE in the next month would be . . .,” followed by the choices foolish-wise, bad-good, unimportant-important, and harmful- bene3cial (a = .76).
Subjective norm. Subjective norm was measured using three items. These items were, “Most people who are important to me think I should perform BSE in the next month” (agree-disagree), “Most people who are important to me would want me to perform BSE in the next month” (agree-disagree), and “Most people who are important to me would disapprove/approve of me performing BSE in the next month” (would approve-would disapprove; a = .75).
Perceived behavioral control. Six items were used to assess PBC over per- forming BSE in the next month. Three items were designed to measure self- efficacy, and three items were designed to measure perceived control.
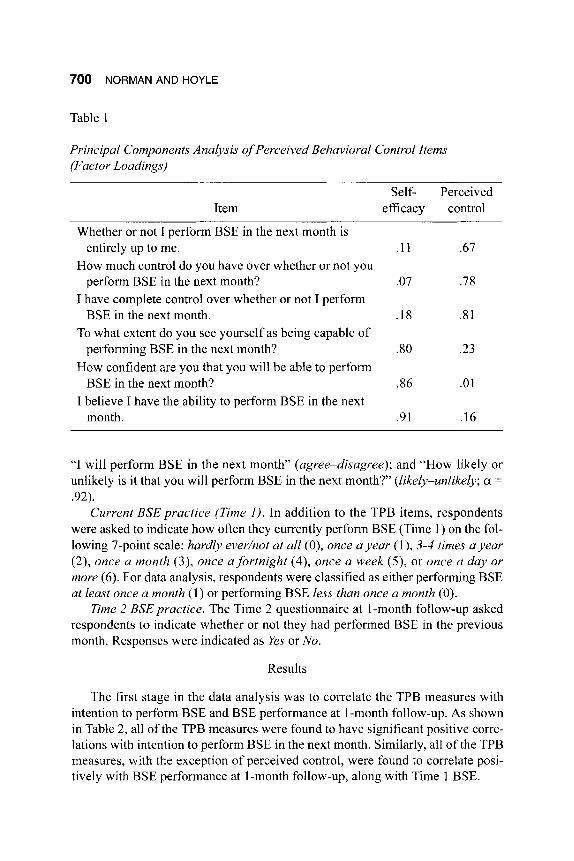
Principal components analysis extracted two factors with eigenvalues greater than 1 .OO, explaining 45.6% and 22.6% of the variance in item scores. In order to aid the interpretation of the factor solution, a varimax rotation was performed. Items with a factor loading greater than 0.55 were included for the interpretation of a factor (Table 1). On the basis of this analysis, two scales were constructed to cover PBC.
The first scale included the three items that focused on self-efficacy: “To what extent do you see yourself as being capable of performing BSE in the next month?” (capable-incapable); “How confident are you that you will be able to perform BSE in the next month?” (sure-unsure); and “I believe I have the ability to perform BSE in the next month” (agree-disagree; a = 34). The second scale included the three items that focused on perceived control: “Whether or not I per- form BSE in the next month is entirely up to me” (agree-disagree); “How much control do you have over whether or not you perform BSE in the next month?” (complete control-very little control); and “I have complete control over whether or not I perform BSE in the next month” (agree-disagree; a = .60).
Behavioral intention. Behavioral intention was assessed using three items. These items were, “I intend to perform BSE in the next month” (agree-disagree);
700 NORMAN AND HOYLE
Table 1
Principal Components Analysis of Perceived Behavioral Control Items (Factor Loadings)
Self- Perceived Item efficacy control
Whether or not I perform BSE in the next month is
How much control do you have over whether or not you
I have complete control over whether or not I perform
To what extent do you see yourself as being capable of
How confident are you that you will be able to perform
I believe I have the ability to perform BSE in the next
entirely up to me. . I1 .67
perform BSE in the next month? .07 .78
BSE in the next month. .I8 .8 1
performing BSE in the next month? .so .23
BSE in the next month? 3 6 .o1
month. .91 .16
“I will perform BSE in the next month” (agree-disagree); and “How likely or unlikely is it that you will perform BSE in the next month?’ (likely-unlikely; a =
.92). Current BSE practice (Time I ) . In addition to the TPB items, respondents
were asked to indicate how often they currently perform BSE (Time 1) on the fol- lowing 7-point scale: hardly everhot at all (O), once a year (l), 3-4 times a year (2), once a month (3), once a fortnight (4), once a week (9, or once a day or more (6) . For data analysis, respondents were classified as either performing BSE at least once a month (1) or performing BSE less than once a month (0).
Time 2 BSE practice. The Time 2 questionnaire at 1 -month follow-up asked respondents to indicate whether or not they had performed BSE in the previous month. Responses were indicated as Yes or No.
Results
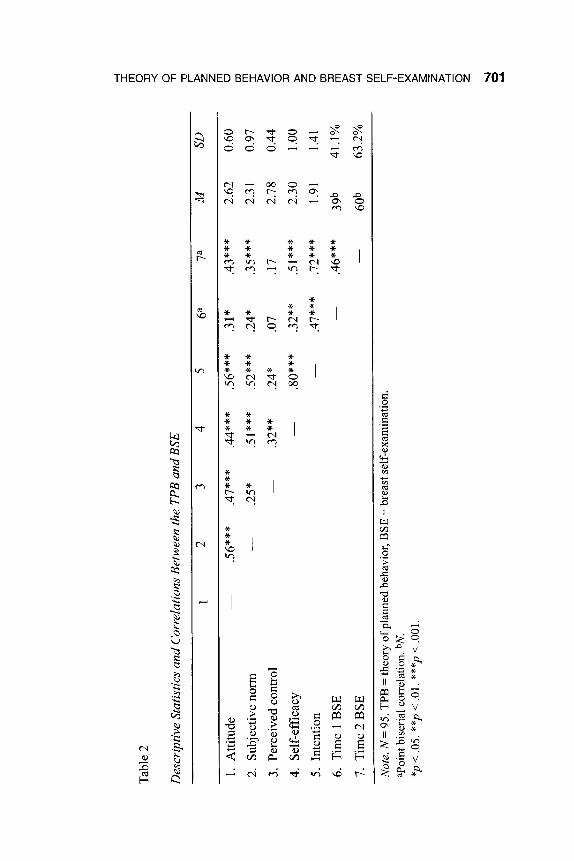
The first stage in the data analysis was to correlate the TPB measures with intention to perform BSE and BSE performance at I-month follow-up. As shown in Table 2, all of the TPB measures were found to have significant positive corre- lations with intention to perform BSE in the next month. Similarly, all of the TPB measures, with the exception of perceived control, were found to correlate posi- tively with BSE performance at 1-month follow-up, along with Time 1 BSE.
Tabl
e 2
--I I
rn
< B
Des
crip
tive
Stat
istic
s an
d C
orre
latio
ns B
etw
een
the
TPB
and
BSE
1 2
3 4
5 6a
7a
M
SD
1. A
ttitu
de
-
.56*
**
.47*
**
.44*
**
.56*
**
.31*
.4
3***
2.
62
0.60
2. S
ubje
ctiv
e nor
m
-
.25*
.5
1***
.5
2***
.2
4*
.35*
**
2.31
0.
97
3. P
erce
ived
cont
rol
.32*
* .2
4*
.07
.17
2.78
0.
44
4. S
elf-
effic
acy
-
.80*
**
.32*
* .5
1***
2.
30
1.00
5. I
nten
tion
-
.47*
**
.72*
**
1.91
1.
41
6. T
ime
1 B
SE
-
.46*
**
39b
41.1
%
7. T
ime2
BSE
-
60b
63.2
%
-
Not
e. N
= 9
5. T
PB =
theo
ry o
f pla
nned
beh
avio
r, B
SE =
brea
st s
elf-
exam
inat
ion.
aP
oint
bis
eria
l cor
rela
tion.
bN
. *p
< .0
5. *
*p <
.01.
***
p < .0
01.
R -0 z
Z
rn 0
m I
6 rn 2 B D z 0 m ID rn
D
v)
--I
702 NORMAN AND HOYLE
Table 3
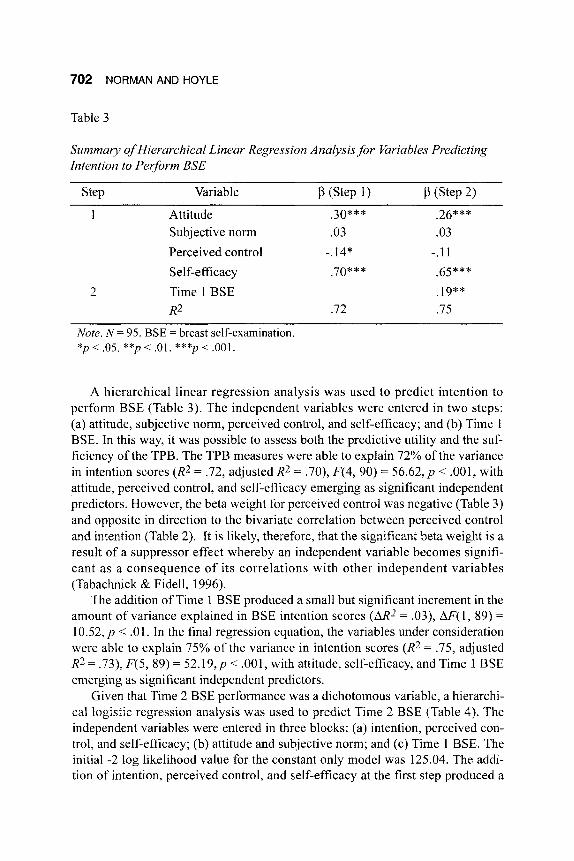
Summary of Hierarchical Linear Regression Analysis,for Variables Predicting Intention to Perform BSE
Step Variable P (Step 1) P (Step 2) I Attitude .30*** .26***
Subjective norm .03 .03 Perceived control -.14* -.11 Self-efficacy .70*** .65***
R2 .72 .75 2 Time 1 BSE .19**
Note. N = 95. BSE = breast self-examination. *p < .05. **p < .01. ***p < .001.
A hierarchical linear regression analysis was used to predict intention to perform BSE (Table 3). The independent variables were entered in two steps: (a) attitude, subjective norm, perceived control, and self-efficacy; and (b) Time 1 BSE. In this way, it was possible to assess both the predictive utility and the suf- ficiency of the TPB. The TPB measures were able to explain 72% of the variance in intention scores (R2 = .72, adjusted R2 = .70), F(4, 90) = 56.62, p < .001, with attitude, perceived control, and self-efficacy emerging as significant independent predictors. However, the beta weight for perceived control was negative (Table 3) and opposite in direction to the bivariate correlation between perceived control and intention (Table 2). It is likely, therefore, that the significant beta weight is a result of a suppressor effect whereby an independent variable becomes signifi- cant as a consequence of its correlations with other independent variables (Tabachnick & Fidell, 1996).
The addition of Time 1 BSE produced a small but significant increment in the amount of variance explained in BSE intention scores (a2 = .03), AF( 1, 89) =
1 0 . 5 2 , ~ < .01. In the final regression equation, the variables under consideration were able to explain 75% of the variance in intention scores (R2 = .75, adjusted R2 = .73), F(5,89) = 5 2 . 1 9 , ~ < .OOl , with attitude, self-efficacy, and Time 1 BSE emerging as significant independent predictors.
Given that Time 2 BSE performance was a dichotomous variable, a hierarchi- cal logistic regression analysis was used to predict Time 2 BSE (Table 4). The independent variables were entered in three blocks: (a) intention, perceived con- trol, and self-efficacy; (b) attitude and subjective norm; and (c) Time 1 BSE. The initial -2 log likelihood value for the constant only model was 125.04. The addi- tion of intention, perceived control, and self-efficacy at the first step produced a
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 703
Table 4
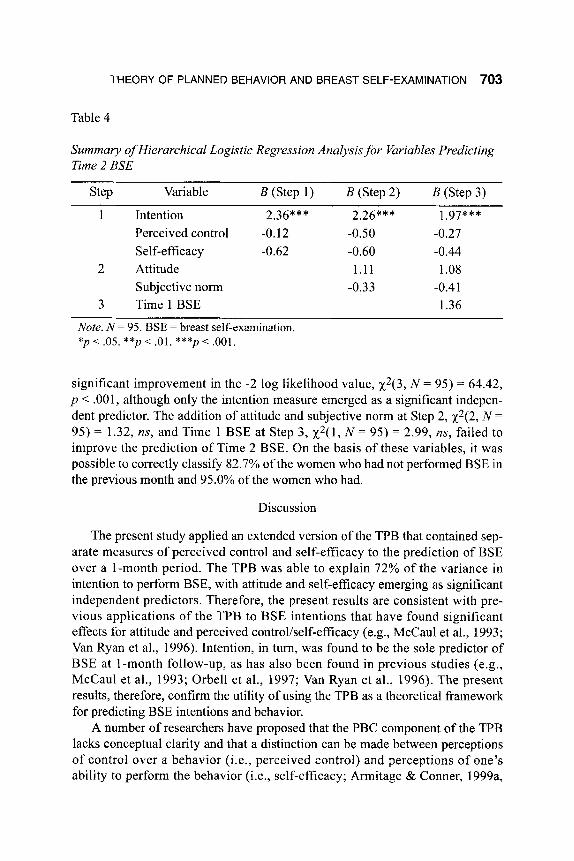
Summary of Hierarchical Logistic Regression Analysis for Variables Predicting Time 2 BSE
Step Variable B (Step 1) B (Step 2) B (Step 3)
1 Intention 2.36*** 2.26*** 1.97*** Perceived control -0.12 -0.50 -0.27 Self-efficacy -0.62 -0.60 -0.44
2 Attitude 1.11 1.08
3 TimelBSE 1.36 Subjective norm -0.33 -0.4 1
Note. N = 95. BSE = breast self-examination. *p < .05. **p < .01. ***p < ,001.
significant improvement in the -2 log likelihood value, x2(3, N = 95) = 64.42, p < .OO 1, although only the intention measure emerged as a significant indepen- dent predictor. The addition of attitude and subjective norm at Step 2, x2(2, N =
95) = 1.32, ns, and Time 1 BSE at Step 3, x2( 1, N = 95) = 2.99, ns, failed to improve the prediction of Time 2 BSE. On the basis of these variables, it was possible to correctly classify 82.7% of the women who had not performed BSE in the previous month and 95.0% of the women who had.
Discussion
The present study applied an extended version of the TPB that contained sep- arate measures of perceived control and self-efficacy to the prediction of BSE over a 1-month period. The TPB was able to explain 72% of the variance in intention to perform BSE, with attitude and self-efficacy emerging as significant independent predictors. Therefore, the present results are consistent with pre- vious applications of the TPB to BSE intentions that have found significant effects for attitude and perceived control/self-efficacy (e.g., McCaul et al., 1993; Van Ryan et al., 1996). Intention, in turn, was found to be the sole predictor of BSE at 1-month follow-up, as has also been found in previous studies (e.g., McCaul et al., 1993; Orbell et al., 1997; Van Ryan et al., 1996). The present results, therefore, confirm the utility of using the TPB as a theoretical framework for predicting BSE intentions and behavior.
A number of researchers have proposed that the PBC component of the TPB lacks conceptual clarity and that a distinction can be made between perceptions of control over a behavior (i.e., perceived control) and perceptions of one’s ability to perform the behavior (i.e., self-efficacy; Armitage & Conner, 1999a,
704 NORMAN AND HOYLE
1999b; Manstead & van Eekelen, 1998; Terry & O’Leary, 1995). In the present study, a principal components analysis revealed that items focusing on percep- tions of control (e.g., “How much control do you have over whether or not you perform BSE in the next month?”) and self-efficacy (e.g., “How confident are you that you will be able to perform BSE in the next month?”) loaded onto sepa- rate factors. Similar results have been reported in previous factor analyses of PBC items (e.g., Armitage & Conner, 1999a, 1999b; Armitage et al., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000; Terry & O’Leary, 1995; White et al., 1994), suggesting that the empirical case for distinguishing between perceived control and self-eficacy is now well established.
Terry and O’Leary (1995) further suggested that measures of perceived con- trol and self-efficacy should have different relationships with intention and behavior, with both self-efficacy and perceived control being predictive of inten- tion, but only perceived control having a direct effect on behavior. In the present study, self-efficacy, but not perceived control, was positively associated with intention. However, neither self-efficacy nor perceived control was predictive of behavior. Instead, intention was the sole predictor of BSE at 1-month follow-up. Therefore, the present results are broadly in line with previous studies that have shown self-efficacy to be a consistent predictor of intention, whereas per- ceived control is rarely predictive of intention (Armitage & Conner, 1999a, 1999b; Armitage et al., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000; Terry & O’Leary, 1995; White et al., 1994). Moreover, intention typically is found to be the sole predictor of behavior (Armitage & Conner, 1999a, 1999b; Armitage et al., 1999; Povey et al., 2000; White et al., 1994, for condom use), although some studies also have reported direct effects for self-efficacy (Armitage et al., 1999; Manstead & van Eekelen, 1998; Povey et al., 2000). Armitage and Conner (2001) estimated that the average correlation between self- efficacy and intention ( r = .44) is stronger than that between perceived control and intention ( r = .23). Similarly, the average correlation between self-efficacy and behavior ( r = .35) is also stronger than that between perceived control and behavior ( r = .IS).
In sum, there is considerable evidence to support the distinction between perceived control and self-efficacy. In addition, self-efficacy appears to be a stronger predictor of both intention and behavior. Some researchers have proposed that it may be advantageous to simply replace the PBC component of the TPB with self-efficacy (e.g., DeVries, Backbier, Kok, & Dijkstra, 1995; DeVries, Dijkstra, & Kuhlman, 1988), and Ajzen’s (1991) contention that PBC and self-efficacy are synonymous would appear to support such a proposal. More recently, though, Ajzen (2002) proposed a hierarchical model of the PBC con- struct in which perceived control and self-efficacy are two separate components that together comprise the higher order concept of PBC. Such a model accounts for the results of previous studies that have shown that it is possible to distinguish
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 705
between perceived control and self-efficacy, while ensuring the unitary nature of the PBC construct within the TPB. However, it is unclear how the postulation of such a higher order construct, over and above perceived control and self-efficacy, adds to development of the TPB and the prediction of intention and behavior.
The present study also considered the influence of past behavior in the TPB as a means for assessing the sufficiency of the model (Ajzen, 1987). When past behavior was added to the regression equation after the TPB measures, it was found to lead to a small but significant improvement in the prediction of intention, but a nonsignificant improvement in the prediction of behavior. These results are slightly different from those found in previous applications of the TPB that have shown that past behavior explains additional variance in both intention and behavior (Conner & Armitage, 1998). However, it should be noted that in the present study, the intention-BSE correlation (Y = .72) was stronger than that reported in many tests of the intention-behavior relationship (Sheppard, Hartwick, & Warshaw, 1988).
In conclusion, the present results have a number of practical implications for the development of theory-based interventions to increase the performance of BSE (Hardeman et al., 2002). Intention was the sole predictor of BSE perfor- mance at 1-month follow-up, and intention, in turn, was predicted by attitude and self-efficacy. Therefore, to increase women’s intentions to perform BSE and their subsequent behavior, interventions should seek to encourage positive attitudes and strengthen feelings of self-efficacy. While the present study did not assess the beliefs underlying attitude and self-efficacy, it is likely that interventions will need to highlight the positive benefits of performing BSE in relation to the bene- fits of the early detection of breast cancer.
In addition, Bandura (1986) outlined four main sources of self-efficacy, and these may be targeted directly to enhance feelings of self-efficacy in relation to BSE. First, self-efficacy may be enhanced through personal mastery experience. For example, it might be possible to split the performance of BSE into various subgoals so that each is mastered in turn. Second, vicarious experience is an important source of self-efficacy. As a result, it might be beneficial to incorporate practical demonstrations of BSE into interventions (Boyle, Michalek, Bersani, Nernoto, & Mettlin, 198 1 ; Craun & Deffenbacher, 1986). Third, standard persuasive techniques can be used to strengthened self-efficacy. For example, such techniques could be incorporated into health education leaflets and pres- entations (Windsor, Kronenfeld, Org, & Kilgo, 1980). Finally, one’s emotional state is an important source of self-efficacy, and high levels of anxiety might be taken to indicate low levels of self-efficacy. Given that the threat of breast cancer could produce feelings of anxiety among women (Lerman & Schwartz, 1993; Valdimarsdottir et al., 1999, interventions should be careful not to overempha- size the threat of breast cancer. In addition, relaxation techniques might need to be taught to those women who are particularly worried about breast cancer.
706 NORMAN AND HOYLE
References
Ajzen, I. (1 987). Attitudes, traits, and actions: Dispositional prediction of behavior in personality and social psychology. In L. Berkowitz (Ed.), Advances in experimental social psychology (Vol. 20, pp. 1-64). New York, NY: Academic Press.
Ajzen, I. (1 988). Attitudes, personality, and behavior. Milton Keynes, UK: Open University Press.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179-2 1 1.
Ajzen, I. (2001). Nature and operation of attitudes. Annual Review of Psychology,
Ajzen, I. (2002). Perceived control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychologv, 32,665-683.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall.
American Cancer Society. (2002). Breast cancer facts andfigures, 2001-2002. New York, N Y Author.
Armitage, C. J., & Conner, M. (1999a). Distinguishing perceptions of control from self-efficacy: Predicting consumption of a low-fat diet using the theory of planned behavior. Journal of Applied Social Psychology, 29,72-90.
Armitage, C. J., & Conner, M. (1999b). The theory of planned behaviour: Assessment of predictive validity and “perceived control.” British Journal of Social Psychology, 38,35-54.
Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behav- iour: A meta-analytic review. British Journal of Social Psychology, 40,
Armitage, C. J., Conner, M., Loach, J . , & Willetts, D. (1999). Different percep- tions of control: Applying an extended theory of planned behavior to legal and illegal drug use. Basic andApplied Social Psychology, 21, 301-316.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 19 1-2 15.
Bandura, A. (1 986). Social foundations of thought and action: A cognitive social theory. Englewood Cliffs, NJ: Prentice-Hall.
Bentler, P. M., & Speckart, G. (1979). Models of attitude-behavior relations. Psy- chological Review, 86,452-464.
Boyle, M., Michalek, A., Bersani, G., Nernoto, T., & Mettlin, C. (1981). Effec- tiveness of a community program to promote early breast cancer detection. Journal of Surgical Oncology, 18, 183-188.
Conner, M., & Armitage, C. (1998). Extending the theory of planned behavior: A review and avenues for further research. Journal of Applied Social Psychol-
52,27-58.
471-499.
ogy, 28, 1429-1464.
THEORY OF PLANNED BEHAVIOR AND BREAST SELF-EXAMINATION 707
Conner, M., & Sparks, P. (1996). The theory of planned behaviour and health behaviours. In M. Conner & P. Norman (Eds.), Predicting health behaviour (pp. 12 1 - 162). Buckingham, UK: Open University Press.
Craun, A. M., & Deffenbacher, J. L. (1987). The effects of information, behav- ioral rehearsal, and prompting on breast self-exams. Journal of Behavioral Medicine, 10, 351-365.
De Vries, H., Backbier, E., Kok, G., & Dijkstra, M. (1995). The impact of social influences in the context of attitude, self-efficacy, intention, and previous behavior as predictors of smoking onset. Journal of Applied Social Psychol-
De Vries, H., Dijkstra, M., & Kuhlman, P. (1 988). Self-efficacy: The third factor besides attitude and subjective norm as a predictor of behavioral intentions. Health Education Research, 3,273-282.
Friedman, L. C., Nelson, D. V., Webb, J. A., Hoffman, L. P., & Baer, P. E. (1994). Dispositional optimism, self-efficacy, and health beliefs as predictors of breast self-examination. American Journal of Preventive Medicine, 10,
Godin, G., & Kok, G. (1996). The theory of planned behavior: A review of its applications to health-related behaviors. American Journal of Health Promo- tion, 11, 87-98.
Hardeman, W., Johnston, M., Johnston, D. J., Bonetti, D., Wareham, N. J., & Kinmonth, A. L. (2002). Application of the theory of planned behavior in behavior change interventions: A systematic review. Psychology and Health,
Heimann, R., Bradley, J., & Hellman, S. (1998). The benefits of mammography are not limited to women ages older than fifty years. Cancer, 82,
Hill, D., White, V., Jolley, D., & Mapperson, K. (1 988). Self-examination of the breast: Is it beneficial? Meta-analysis of studies investigating breast self- examination and extent of disease in patients with breast cancer. British Medical Journal, 297,271-275.
Lerman, C., & Schwartz, M. (1993). Adherence and psychological adjustment among women at high risk for breast cancer. Breast Cancer Research and Treatment, 8, 145-155.
Manstead, A. S. R., & van Eekelen, S. A. M. (1998). Distinguishing between per- ceived behavioral control and self-efficacy in the domain of academic achievement intentions and behavior. Journal of Applied Social Psychology,
McCaul, K. D., Sandgren, A. K., O’Neill, H. K., & Hinsz, V. B. (1993). The value of the theory of planned behavior, perceived control, and self-efficacy expectations for predicting health-protective behaviors. Basic and Applied Social Psychology, 14,23 1-252.
0~,25,237-257.
1 30- 135.
17, 123-158.
2221-2226,
28, 1375-1392.

708 NORMAN AND HOYLE
Murray, M., & McMillan, C. (1993). Health beliefs, locus of control, emotional control, and women’s cancer screening behaviour. British Journal of Clinical
Orbell, S., Hodgkins, S., & Sheeran, P. (1997). Implementation intentions and the theory of planned behavior. Personality and Social Psychology Bulletin, 23, 945-954.
Ouellette, J., & Wood, W. (1998). Habit and intention in everyday life: The mul- tiple processes by which past behavior predicts future behavior. Psychologi- cal Bulletin, 124, 54-74.
Povey, R., Conner, M., Sparks, P., James, R., & Shepherd, R. (2000). Applica- tions of the theory of planned behaviour to two dietary behaviours: Roles of perceived control and self-efficacy. British Journal of Health Psychology, 5,
Rotter, J . B. (1 966). Generalized expectancies for internal and external control of reinforcement. Psychological Monographs: General and Applied, 80, 1 - 18.
Sheppard, B. H., Hartwick, J., & Warshaw, P. R. (1 988). The theory of reasoned action: A meta-analysis of past research with recommendations for modifica- tions and future research. Journal of Consumer Research, 15, 325-343.
Steel, C. M., Cohen, B., & Porter, D. (1992). Familial breast cancer. Seminal Cancer Biolqp, 3, 141-150.
Sutton, S. (1998). Predicting and explaining intentions and behavior: How well are we doing? Journal of Applied Social P.yychology, 28, 13 17- 1338.
Tabachnick, B. G., & Fidell, L. S. (1996). Using multivariate statistics. New York, NY: Harper Collins.
Terry, D. J., & O’Leary, J. E. (1995). The theory of planned behaviour: The effects of perceived behavioural control and self-efficacy. British Journal of Social Psychology, 34, 199-220.
Trafimow, D., Sheeran, P., Conner, M., & Finlay, K. A. (2002). Evidence that per- ceived behavioural control is a multidimensional construct: Perceived control and perceived difficulty. British Journal ofSocial Psychology, 41, 101-1 21.
Valdimarsdottir, H. B., Bovbjerg, D. H., Kash, K. M., Holland, J. C., Osborne, M. P., & Miller, D. G. (1995). Psychological distress in women with a familial risk of breast cancer. Psycho-Onco/ogy, 4, 133- 141.
Van Ryn, M., Lytle, L. A., & Kirscht, J. P. (1996). A test of the theory of planned behavior for two health-related practices. Journal of Applied Social Psychol-
White, K. M., Terry, D. J., & Hogg, M. A. (1994). Safer sex behavior: The role of attitudes, norms, and control factors. Journal of Applied Social Psychology,
Windsor, R. A., Kronenfeld, J . J., Ory, M. G., & Kilgo, J. S. (1 980). Method and design issues in evaluation of community health education programs: A case study in breast and cervical cancer. Health Education Quarterb, 7, 203-218.
PSycholOa, 32, 87- 100.
121-139.
OD, 26, 871-883.
24,2 164-2 192.


















