
The Surgical Treatment of Transposition of the Great...
52
The Arterial Switch Operation for Transposition of the Great Arteries A Journey of 60 Years Jan M. Quaegebeur, M.D., Ph.D.
Transcript of The Surgical Treatment of Transposition of the Great...

The Arterial Switch Operation
for Transposition of the Great
Arteries
A Journey of 60 Years
Jan M. Quaegebeur, M.D., Ph.D.

Transposition of the Great Arteries
First description: M. BAILLIE
The morbid anatomy of some of the more important
parts of the human body – London (1797)
The term “Transposition of the aorta and pulmonary
artery”: J.R. FARRE
On malformations of the human heart – London (1814)

First attempts at TGA repair directed at the arterial
level
1954 MUSTARD (2 patients)
transfeer of LCA
description of 3 coronary pattern
1954 BJÖRK and BOUCKAERT (Karolinska)
experimental “switch-over” anastomosis
systemic LV pressure
1954 BAILEY operated on one patient with TGA + VSD who survived 30 hours
1955 KAY & CROSS
1961 IDRISS
1960 BAFFES: concept of coronary buttons (“triangulation”)


TRANSPOSITION of GREAT VESSELS – 34 cases

Fig. 4 Diagram of
coronary artery
variations in
transposition from
William Mustard’s 1954
report [19]
123




The Arterial Switch Operation for TGA
1976 A. JATENE: first successful ASO
TRUSLER, ROSS, YACOUB, BROM: series of ASO for complex TGA
HAZAN (Paris): series of primary ASO for simple TGA (100% mortality)
YACOUB: staged ASO (shunt ± PA banding) for TGA and intact ventricular septum
1983 CASTAÑEDA, QUAEGEBEUR: neonatal ASO for simple TGA
DAMUS, KAY, STANSEL (DKS) procedure: to avoid coronary transfer


Arterial Switch Operation

Arterial Switch Operation

Arterial Switch Operation

Arterial Switch Operation

Arterial Switch Operation

Arterial Switch Operation

Arterial Switch Option

Arterial Switch Operation


Quaegebeur 1986
70% 14%
3%
4.5%
7% 1.5%
Coronary Artery Branching Patterns

Jonas- Ped Cardiac Surgery Annual 2001
Single Coronary Artery Anatomy

Quaegebeur 1986
Intramural Coronary Arteries
Traverse aortic wall
High in sinus
Juxtacommissural

Intramural Coronary Arteries


German Heart Centre – Munich
Atrial/Arterial Switch Volume


Arterial Switch Operation (1978-1994)
Incremental risk factors for
death
1985 1988 1994
Lower birth weight
Large PDA
Morphology other than simple TGA
Intra-mural coronary artery
Longer myocardial ischemic time
Earlier date of operation

Arterial Switch for TGA 1990-2011
CHONY (N=555)
N Death %
Simple TGA 300 4 1.3
TGA, VSD 210 7 3.3
Taussig-Bing 45 3 6.6
Univentricular 14 2 14
IAA, VSD, TAPVR 1 1
Various 4 1
Total: 574 18 3.3

Arterial Switch for TGA
and Aortic Arch Obstruction (1990-2011)
Total N Death %
Simple TGA 300 7 0 0
TGA, VSD * 210 37 1 2.7
Taussig-Bing* 45 35 3 8.5
Total: 555 79 4 5
* 1 and 5 had IAA

Arterial Switch for TGA (1990-2011)
Mode of Death (N=18)
Acute Cardiac Failure 14 *
Premature- ECMO 1
Preop ECMO (Mecon. Asp.) 1
Acute Pulmonary Hemorrhage 1
Pulmonary Hypertension 1
* I
IUGR (l000g) in one
5 with Intramural Coron.

Arterial Switch for TGA (1990-2011)
Coronary Morphology and Death
Simple TGA VSD TB
1LCx- 2r 188 0 147 3 14 0
1L- 2CxR 55 0 15 1 4 0
Unusual 37 1 45 2 20 1**
Intramural 11 3* 4 2 2 2
* Bilateral Intramural in one
** Acute Pulmonary Hemorrhage

Risk Factors for Death after ASO for TGA±VSD
(n=513, 92 deaths) - CHSS
Patient p-value
LCA, LAD or Cx from Sinus 2: with intramural 0.07
no intramural 0.009
Multiple VSDs 0.001
Non-cardiac anomalies 0.14
PA Banding > 1 month 0.4
Older age 0.7
simple TGA 0.5
Support
Longer circulatory arrest time 0.03
Longer aortic cross-clamp time 0.03
Institutions
1 institution with better MR
10 High Risk institutions from Kirklin et al, Circulation Nov 1992

Risk factors for death after the ASO – Conclusions
Risk of death after ASO for TGA±VSD with
unusual coronary pattern is very low (<1%)
In several institutions, a single independent risk
factor for death after ASO cannot be identified
any longer
Unusual CAP is possibly associated with increased
risk, although most experienced centers have
neutralized this factor

Risk factors for death after the ASO – Conclusions
Aortic arch obstruction, multiple VSD’s and possibly
low birth weight continue to impact outcomes
negatively
A combination of variables (although N is small) can
complicate the ASO in any form of TGA
Institutional differences in Volume and Experience
can be associated with differences in outcomes,
irrespective of patient variables
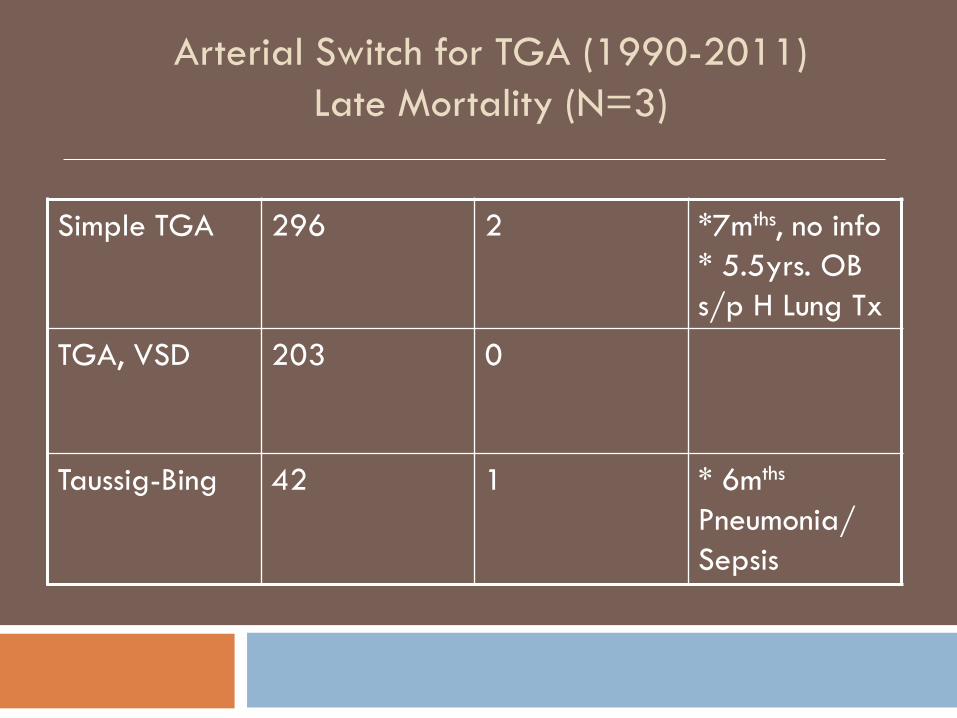
Arterial Switch for TGA (1990-2011)
Late Mortality (N=3)
Simple TGA 296 2 *7mths, no info
* 5.5yrs. OB
s/p H Lung Tx
TGA, VSD 203 0
Taussig-Bing 42 1 * 6mths
Pneumonia/
Sepsis

Survival after the ASO (Leiden 1977-2007)
Independent risk factors for early death
• Cross-clamp time (coronary problems at ASO)
• No Lecompte (earlier date of ASO)
Independent risk factor for late death
• Coronary problems at ASO
• Pacemaker implantation

Arterial Switch : Late Reoperations and Cardiac Interventions
Simple TGA (300) TGA, VSD (210) TB (45)
Supravalv PS 9 8 2 3 3 6
Coarc 1 - - 1 2 4
Supravalv PS
& Coarc
2
Subvalve,
Valve PS
1 2 4
HLTx 1
PPM 1
Ao V Replace. 1
6/17 PA Interventions Needed Reoperation

Reoperations after the ASO
(Leiden 1977-2007)
Independent risk factors • Older age at ASO
• Ao Arch Anomalies
• Coronary problems at ASO
• Duration of P.O. Ventilation

Supravalvar Pulmonary Stenosis
Incidence <10% (CHSS)
Etiology
Small neo-pulmonary root
Inadequate PA mobilization
Pursestring effect
Inappropriate Lecompte
? Patch material
Reintervention rate -0.5% /yr

Cause of Reoperation in 756 survivors
after ASO (Angeli, Eur. JCTS 2008)
Early ( ≤ 1yr) Late (mean 6.5 yrs)
Coronary obstruction 4 18
Ao Coarctation 4 -
RVOTO 2 11
LVOTO - 3
Tracheal
Compression
- 1
Pulmon.Hypertension - 2
Pacemaker 1 -
Total = 46

Coronary Artery Obstruction After the Arterial Switch Operation
for Transposition of the Great Arteries in Newborns
Bonhoeffer et al, JACC 1997
165 patients had coronary angioplasty
2 wks – 15 yrs after arterial switch
Coronary Obstruction
N n° %
Evidence of myocardial ischemia 25 13 52%
Prospective (Nl ECG, ECHO) 105 6 5.7%
“Single ostium” technique 35 11 31%

Aortic Root and LV 20 years after the ASO
(Vandekerckhove et al. Eur. JCTS 2009)
• LVESD and LVEDD were normal
• Septal and posterior wall thickness normal
• Mild decrease in SF in 10%
• No coronary obstruction

Aortic Root and LV 20 years after the ASO
(Vandekerckhove et al. Eur. JCTS 2009)
• AR: None-Trivial 28 72%
Mild 5 13%
Mod 6 15%
• AVR in 1 patient 10 yrs post ASO
-had discrete Sub AS
• Larger diameter of SV, STJ when mild or moderate AR
• Reinterventions in 7 pts
* Supravalv PS 3
* Left PA stenosis 1
* Subvalv AS, AVR 1
* Balloon Ao Coarc 2






• Ao Root dilation (2 ≥ 3) develops over time after
ASO
• Not progressive in late follow- up
• Considerable overlaps between Z-values of Ao
Root and degree of AR
• Risk factors for ARD: -Previous PA Band
-Technical factors
• 2.4% had neo-aortic valve surgery
from Schwartz et al. Circ 2004




















