The Stroke Oxygen Supplementation PILOT Study C. Roffe, K.Ali, A. Warusevitane, S. Sills, S....
24
The Stroke Oxygen Supplementation PILOT Study C. Roffe, K.Ali, A. Warusevitane, S. Sills, S. Pountain, P Jones, R Gray, P. Crome North Staffordshire Combined Healthcare Trust University Hospital of North Staffordshire Brighton and Sussex University Hospital University Hospital Birmingham Keele University The North Staffordshire Medical Institute
-
Upload
ethelbert-haynes -
Category
Documents
-
view
214 -
download
0
Transcript of The Stroke Oxygen Supplementation PILOT Study C. Roffe, K.Ali, A. Warusevitane, S. Sills, S....
The Stroke Oxygen Supplementation PILOT Study
C. Roffe, K.Ali, A. Warusevitane, S. Sills, S. Pountain, P Jones, R Gray, P. CromeNorth Staffordshire Combined Healthcare Trust
University Hospital of North StaffordshireBrighton and Sussex University Hospital
University Hospital BirminghamKeele University
The North Staffordshire Medical Institute

Background
Incidence of hypoxia 63% in the first 2 days
Sulter et al, J Neurol Sci 2000;179:65-9.

Oxygen saturation within the first 72 hours of acute stroke
Acute StrokeN=100
ControlsN=85
Age (years) 74 sd 8 72 sd 8
Awake SpO2 (mean) 94.5 sd 1.7 %*** 95.8 sd 1.7 %
Mean nocturnal SpO2 93.5sd 1.9 %** 94.3 sd 1.9 %
Lowest nocturnal SpO2 82.5 sd 6.4 %* 84.6 sd 7.8 %
Results are given as means, *p<0.05, **p<0.01, ***p<0.001
Roffe et al, Stroke 2003;34:2641-2645.

Adverse effects of hypoxia after stroke I
Early deterioration
Silva et al, Cerebrovasc Dis 2001;11(suppl 4):70
381 consecutive patients with acute strokeOxygen saturation <90 doubles risk of early deterioration.
Adverse effects of hypoxia after stroke II
Increased mortality
• N=153 assessed from arrival and during transfers till ward admission
• Hypoxia defined as SpO2<90 for >10% of assessment phase
• Oxygen saturation lowest during transfers
• Hypoxic pts are more likely to have a history of chest problems
• Hypoxia doubles mortality, but no longer significant if corrected for stroke severity
• No effect on long-term disability
Rowat et al. Cerebrovasc Dis 2006;21:166-172.

Unexpected nocturnal hypoxia in stroke patients
Time spent with an oxygen saturation <90% at night
52% more than 5 minutes
23% more than 30 minutes
15% more than 1 hour
Roffe et al, Stroke 2003;34:2641-2645

Experimental Evidence
• 100% oxygen increases oxygen delivery to the ischaemic brain in mice
• Infarct size at 2 days reduced by 45%
Shin, H. K. et al. Brain 2007 130:1631-1642
• 95% O2 reduced neurological deficit and infarct size in rats
Liu et al J Cereb Blood Flow Metab. 2006;26:1274-84.

Ronning and Guldvog, Stroke 1999;30:2033-37.
Routine oxygen supplementation
Oxygen
No oxygen
No oxygen
Oxygen
Oxygen
No oxygen
All strokes Mild strokes SSS>40 (top)Severe strokes SSS (bottom)

Selective high dose (45L/min) short burst oxygen supplementation
Methods—• acute stroke <12 h and perfusion-diffusion "mismatch" on MRI • RCT of high-flow oxygen via mask for 8 hours (n=9) vs room air (n=7)
Results— • Oxygen tended to improve stroke scale scores at 4 h and 1 week, and
significantly at 24 h, but there was no significant difference at 3 months.
• MRI lesion volumes were significantly reduced at 4 hours, but not subsequent time points.
• Cerebral blood volume and blood flow within ischemic regions improved
• More petechial hemorrhages (50% w oxygen vs 17% w room air)
Singhal et al . Stroke. 2005;36:797-802.

National and international Stroke Guidelines
UK National Clinical Guidelines for Stroke Arterial oxygen concentration should be maintained within normal limits 2004
Give Oxygen to maintain oxygen saturation at or above 95% 2008
European Stroke Initiative Recommendations for Stroke Management 2-4L/min when indicated in 2003
Oxygen if saturation<92% in 2007
American Stroke Association GuidelinesOxygen if saturation <95% in 2003 and 2005
Oxygen if saturation </=92% in 2007
National Clinical Guidelines for Stroke. RCP 2004, 2008, NICE 2008, EUSI 2004, ESO 2007; ASA, Stroke. 2003;34(4):1056-83, 2005;36:916-23, 2007;38:1655-1711.
Stroke Oxygen PILOT Study
Routine oxygen supplementation during the first three days after an acute stroke
Prospective randomized open study

Inclusion criteria Acute stroke
Less than 24 hours after hospital admission No definite indications for oxygen treatment
No definite contraindications for oxygen treatment No other serious medical condition limiting life expectancy
Consent or assent
Baseline assessment
No routine oxygen
Oxygen is not given routinely, but may be prescribed if definite clinical indications develop
Continuous humidified oxygen per nasal cannula for 72 h
3l/min if oxygen saturation at baseline is 94% 2/min if oxygen saturation at baseline in 94%
Randomise
Week 1 Neurological examination, complications
Night 2 Pulse oximetry
Month 6 Questionnaire functional outcome, quality of life

SOS Pilot Study Patient Accrual
0
50
100
150
200
250
300
350
Nov
-04
Jan-
05
Mar
-05
May
-05
Jul-0
5
Sep
-05
Nov
-05
Jan-
06
Mar
-06
May
-06
Jul-0
6
Sep
-06
Nov
-06
Jan-
07
Mar
-07
May
-07
Jul-0
7
Sep
-07
Nov
-07
Jan-
08
Mar
-08
Time Period (Monthly)
Pat
ien
t R
ecru
itm
ent
SOS PILOT Study – patient recruitment
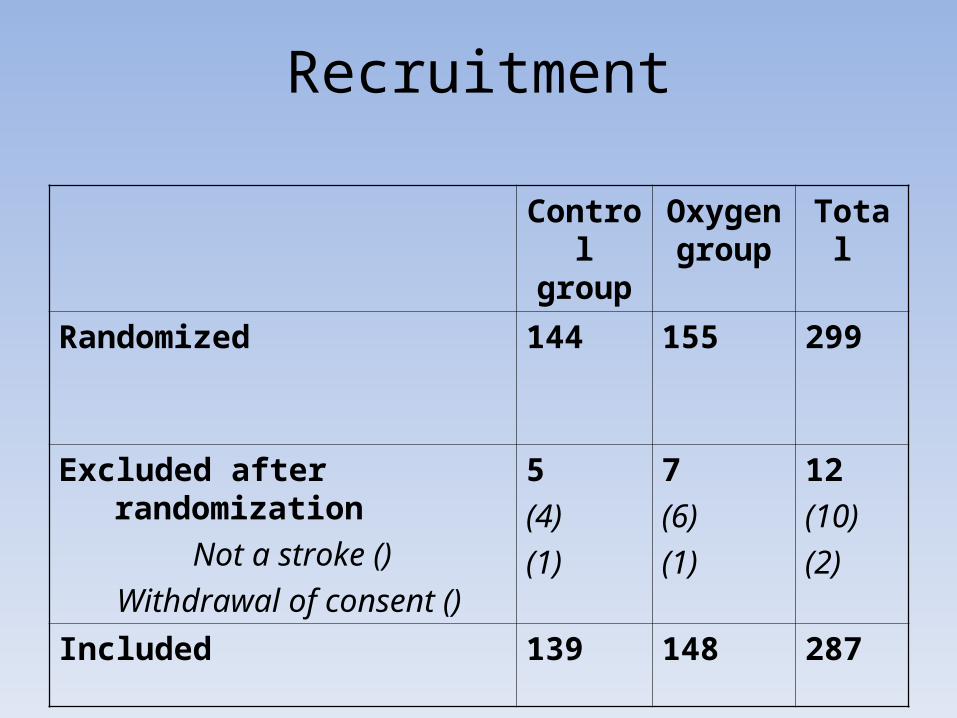
Recruitment
Control group
Oxygen group
Total
Randomized 144
155 299
Excluded after randomization Not a stroke () Withdrawal of consent ()
5(4)(1)
7(6)(1)
12(10)(2)
Included 139 148 287

Baseline ResultsControl N=139
Oxygen N=148
Age (mean) 72 sd 12 73 sd 12
Sex (n ( % male)) 71 (51%) 65 (44%)
GCS (mean) 15 sd 1 15 sd 1
COPD 12 (9%) 14 (9%)
LVF 18 (13%) 16 (11%)
IHD 37 (27%) 35 (24%)
AF 19 (14%) 34 (23%)
TIA 3 (2%) 4 (3%)
TAC 24 (17%) 24 (16%)
PAC 45 (32%) 47 (32%)
POC 6 (4%) 6 (4%)
LAC 58 (42%) 58 (39%)

Baseline Results Cont…
Control (no O2) N=139
Treatment (O2) N=148
Time admission to recruitment (hh:mm, mean)
12:07 sd 7:15 12:49 sd 7:13
Respiratory Rate at presentation (mean) 18 sd 3 18 sd 3
Oxygen at presentation (mean) 97 sd 2% 97 sd 2%
Oxygen at randomisation (mean) 96 sd 2% 96 sd 2%

Effect of oxygen supplementation on oxygen saturation
(mean, sd) Control N=126
OxygenN=139
Mean nocturnal SpO2 94% (2) 96% (2)***
4% Oxygen desaturation index 3 (14) 2 (6)*
Lowest SpO2 88% (5) 89%(6)**
Time with SpO2>98 (minutes)a 71 (444) 147 (166)***
Time with SpO2<95 (minutes)a 224 (158) 121 (141)***
Time with SpO2<90 (minutes)a 16 (42) 8 (23)
SpO2: oxygen saturation a Time corrected to a standard 8 hour night *p<0.05, **p<0.01, ***p<0.01
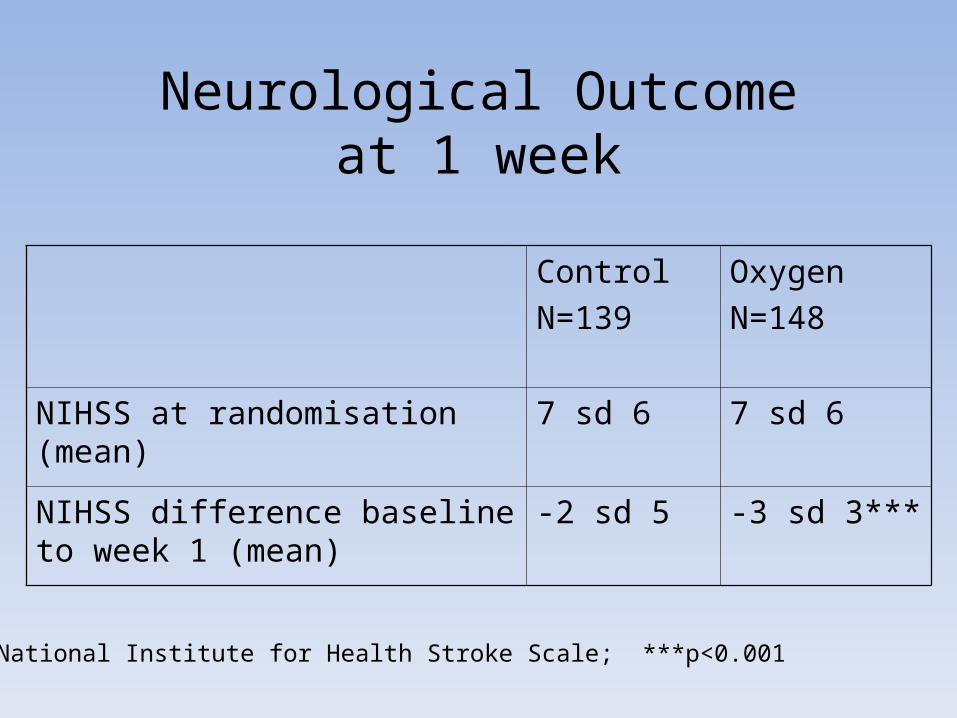
Neurological Outcomeat 1 week
Control N=139
Oxygen N=148
NIHSS at randomisation (mean) 7 sd 6 7 sd 6
NIHSS difference baseline to week 1 (mean)
-2 sd 5 -3 sd 3***
NIHSS: National Institute for Health Stroke Scale; ***p<0.001

Other results at 1 week
Control N=139
Oxygen N=148
Highest temperature (mean, sd) 37 (1) 37 (1)Highest heart rate (mean, sd) 92 (19) 92 (16)Highest systolic (mean, sd) 166 (28) 167 (29)Highest diastolic (mean, sd) 92 (15) 93 (19)Antibiotics given (N) 22 (16%) 27 (18%)O2 given outside of protocol (N) 16 (12%) 12 (8%)
Sedatives given (N) 9 (6%) 9 (6%)

Completeness of follow –up at 6 months
Control n=139
Oxygen n=148
Total n=287
Outcome known Questionnaire returned Death before 6 mo follow-up
134 (96%)113 (81%)21 (15%)
144 (97%)118 (80%)26 (17%)
278 (97%)
Outcome not known 5 (4%) 4 (3%) 9 (3%)

How was the questionnaire completed?
Control Group
OxygenGroup
Total
By the participant alone 36 (38%) 41 (50%) 77 (44%)
By the participant with help from others 21 (22%) 18 (22%) 39 (22%)
By someone else 37 (39%) 23 (28%) 60 (34%)
No of participants answering this question 94 82 176
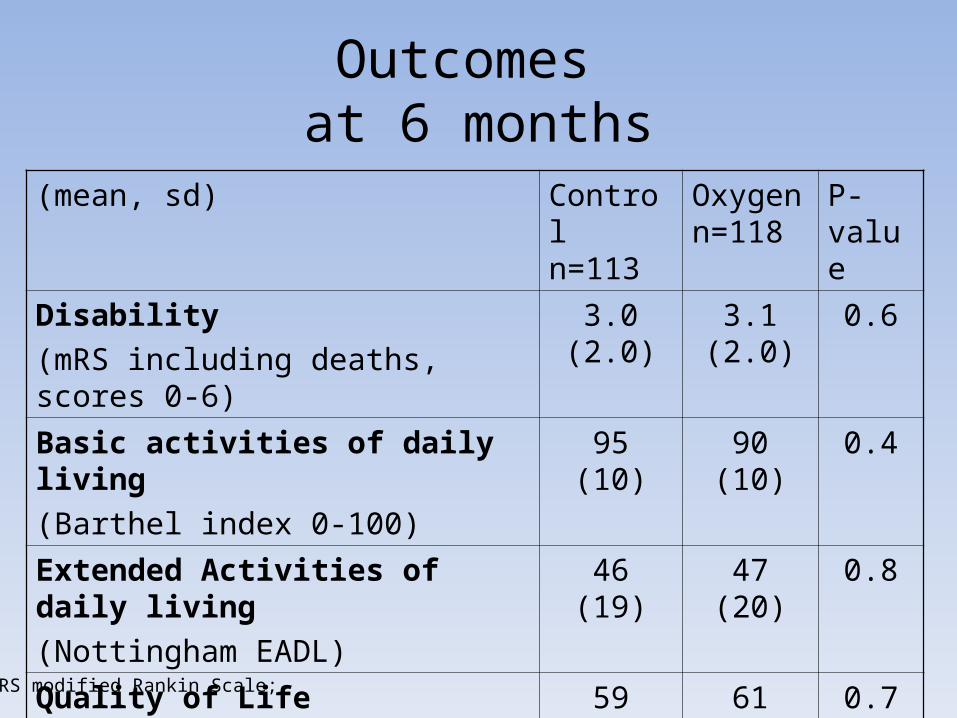
Outcomes at 6 months
(mean, sd) Control n=113
Oxygen n=118
P-value
Disability (mRS including deaths, scores 0-6)
3.0 (2.0) 3.1 (2.0) 0.6
Basic activities of daily living (Barthel index 0-100)
95 (10) 90 (10) 0.4
Extended Activities of daily living (Nottingham EADL)
46 (19) 47 (20) 0.8
Quality of Life (EuroQuol)
59 (25) 61 (25) 0.7
mRS modified Rankin Scale;

Conclusion 1This pilot study demonstrates
1. That routine oxygen supplementation effectively increased oxygen saturation when given in a non- intensive clinical environment
2. That oxygen supplementation was well tolerated without observable adverse effects
3. That the outcomes are feasible and deliver over 95% returns at 1 week (clinical) and 6 months (questionnaire)
Conclusion 2This pilot study was not powered to look at neurological or
functional outcomes or to do subgroup analyses
Results so far are that routine oxygen supplementation
• Led to a small but statistically significant improvement in neurological outcome at 1 week
• Had no significant effect on mortality and functional outcome at 6 months
A larger study is required to determine whether routine oxygen supplementation is effective in reducing neurological deficit and improving functional outcome