The Sleep Magazine- 2nd Issue
60
WWW.SLEEPGS.COM
-
Upload
the-sleep-magazine -
Category
Documents
-
view
229 -
download
8
description
The Sleep Magazine is the ONLY magazine 100% dedicated to Dental Sleep Medicine- The dental treatment of snoring and sleep apnea. The 2nd issue discusses sleep screening technology, online dental CE, Oral Appliance discussions, case presentations, and more.
Transcript of The Sleep Magazine- 2nd Issue
WWW.SLEEPGS.COM

DENTAL SLEEP MEDICINE
Ambulatory sleep study instrumentation (ASSI) has become a necessary
tool in the dental sleep physician’s armamentarium. Protocol though is often unclear regarding when to administer take home sleep tests for our OSA oral appliance therapy patients. Though space prevents a complete treatise on this subject, the following is a brief overview of ambulatory sleep study instrumentation protocol to help guide DSM physicians as to when and why. ASSI has gained recent near explosive interest in sleep medicine due to Medicare’s favorable view of such diagnostic instrumentation for obstructive sleep apnea (OSA) screening and diagnosis in the hands of sleep specialists. While many dental sleep physicians were first to introduce such instrumentation to their communities, often preceding their sleep medicine colleagues, (as in the case of the author, by nearly a decade) now everybody’s got ‘em. Several advantages exist when
comparing an ambulatory study to “big brother” polysomnography (PSG). Oftentimes, sleep labs are under built and patient waiting lists swell creating evaluation stagnation. Patient disability and geographic distance can also be effective barriers to lab studies. Age and emotional stressors can further prevent those most in need of expert diagnosis form entering the overnight lab environment. Finally, the expense of a technician-attended laboratory study can burden an individual financially prohibiting adequate and necessary testing. Other examples of PSG-phobia, PSG -avoidance, and PSG-inability abound shinning an encouraging spotlight on PSG’s newly recognized and cost effective alternative. ASSI testing does however harbor several disadvantages. For example, most ambulatory equipment lacks the ability to stage sleep providing more accurate AHI and RDI calculations. Under reported RDI/AHI values are a by-product of data dilution as EEGs are not generally enlisted to measure brain waves and stage sleep (For those interested, the Embletta X100 does offer 12+ lead capability including EEG). Another criticism of ASSI has been low end insensitivity: Is it an AHI of 12 or 21? Data loss due to unsupervised lead application and inadvertent loss can also confound data gathering and subsequent study interpretation. ASSI, though seemingly fraught with “nuisance factors”, is vital to DSM. Four examples of ASSI utility in DSM include: Patient screening - the screening ambulatory test performed on one’s existing patients recently identified by the dentist as a likely OSA sufferer. If the patient suffers from PDS (Patient Denial Syndrome), ASSI is an excellent screening tool to measure and demonstrate a patient’s sleep pathology. The author uses a “pass, and the test is free: fail, and you agree to see a sleep specialist” approach to effectively educate and motivate patients in denial. Pre-OAT post-PSG screening - ASSI scenario recommends a baseline test prior to beginning OAT when the new sleep patient presents with an outdated PSG. Often the dental sleep physician will inherit patients “MD-referred” for OAT based upon the results of 2-plus year old PSG. It is prudent to establish an office protocol whereby patients with PSGs older than 6-12 months routinely have an ambulatory sleep study performed prior to OAT so as to establish a baseline evaluation later followed
by additional ambulatory tests as treatment progresses. OAT titration update & maximum medical improvement re-evaluation - Often, patients will espouse that they feel better when, in fact, OSA persists. Placebo treatment effect can be tested by easily and affordably measuring the patient’s nocturnal condition with and without their appliance. When patient titration is completed, an MMI study should be performed and results communicated to the referring sleep specialist. This data, in the hands of the MD, will help him or her best direct re-evaluation diagnostics. The sleep specialist may determine that a follow-up PSG is unnecessary based upon your results and professional collaborative approach. Consider also how your referring sleep specialists value your level of OAT follow-up. Many sleep specialists have been burned by “drive-by” dentists wielding appliances that are unwilling or unable to follow-up with take home titration studies prior to turfing the unresolved mutual patient back to the referring MD; frustrating for the patient, the dentist and the sleep specialist. Several brands of ASSI are available for use by dentists to monitor their OAT patients. It is a good idea, prior to purchasing such instrumentation, to discuss which types of instruments your referring sleep specialists use. If the sleep centers you are going to work with use EMBLA equipment, for example, it might behoove you to also utilize EMBLA instrumentation (e.g., Embletta X100). Using data collection instrumentation or technology unfamiliar to your physician network does little to cultivate multidisciplinary confidence. Making a few phone calls to your future sleep specialist referrers regarding recommended instrumentation can be a great icebreaker when establishing your necessary MD-DDS relationships. OSA is no longer a simple case of oropharyngeal collapse. OSA, by definition, harbors co-morbid factors including several very serious and life threatening medical conditions. ASSI is a necessary and useful tool to help maximize OAT outcomes. Multiple PSGs used to follow patients’ progress is expensive and impractical. By incorporating ASSI into your dental sleep medicine practice, you will set a higher standard for your practice, your patients and your referring physicians.
Ambulatory Sleep Studies in DSM: When and Why?Let’s answer the call to action and start Saving Lives!
By Dr. J.Brian Allman, DDS, DABDSM, DAAPM, FAGD, FAACP, FICCMO, FAAFO, FASGD, Senior Instructor IAO
PSG
While PSG and ASSI have their differences; ASSI - a newly recognized cost effective alternative to OSA screening and diagnosis, is vital to DSM.
Under Built Labs Patient Waiting Lists Evaluation Stagnation Disability/Distance Barriers Age & Emotional Stressors Financial Burdens PSG Phobia, Avoidance, Inability
Inability to Stage Sleep Data Dilution Low End Insensitivity Data Loss - Due to unsupervised
lead application Confounded Data Gathering Study Interpretation
ASSI
WWW.SLEEPGS.COM
Internet Based Education
By Dr. Maurice Salama
p. 44-45
AcousticPharyngometry By Professor Fredberg
p. 37
Working WithTAP3
By Dr. Dan Tache
p. 33-35
Home Sleep TestsHelping Sleep
Labs By Randall Haupt, RPSGT
p. 14
OSA and Eye Vision
By Troy Bedinghaus
p. 56
table
ofco
nte
nts
1
DISCLAIMERDental Sleep Medicine Magazine, and all of the expert opinion herein, represents many years of dental sleep medicine practice. It is presented as a forum for the advancement of dental sleep medicine. The articles within this publication are the opinions/statements of the medical professionals featured. Sleep Group Solutions is a private medical equipment and education company producing and distributing medical equipment and services. SGS provides practitioners with appealing diagnostic and treatment alternatives and in no way offers medical advice in the sleep disorder industry.
SLEEP DISORDERSThe Fastest Growing
Dental Specialty
Change the way you practice dentistry for the health of your patients!
WWW.SLEEPGS.COM
The Field of Dental Sleep Medicine is Growing ...................................................................... 2
Helping Keep People A.W.A.K.E. .............................................................................................. 3
What is Your OSA Story? ........................................................................................................... 4
OSA the Camouflaged Killer .................................................................................................... 5
Is Your Team Snoozing? ........................................................................................................... 8
Rhinometry Not An Option! ...................................................................................................... 8
An Orthodontist’s Perspective on Sleep Disordered Breathing ............................................ 10
Protocol For Snoring Problems Male Age 18 .......................................................................... 11
Oxygen is Under-Rated .......................................................................................................... 12
Dr. Lucia Interview ........................................................................................................ 18-19
No Thanks Mister! I’ll Take Vanilla ............................................................................. 20-22
The Epworth Test .................................................................................................................. 20
United Sleep Diagnostics ..................................................................................................... 24
SGS Sleep Seminar Schedule ..................................................................................... 25-28
Obstructive Sleep Apnea and CPAP ..................................................................................... 29
Genetic Orthodontics .................................................................................................. 30-31
Developing a Sleep Physician Team .................................................................................... 32
The Emergence and Explosive Growth of OSA ..................................................................... 36
Sleeping Down Under ................................................................................................. 42-43
Introducing The Silent Sleep Trial Oral Appliance For Snoring And Sleep Apnea ............... 46
Pneumodontics .......................................................................................................... 48-51
Raising the Level of Suspicion ................................................................................... 53-55
Internet Based Education
p. 44-45
AcousticPharyngometry
p. 37
Working WithTAP3
p. 33-35
Home Sleep TestsHelping Sleep
Labs
p. 14
OSA and Eye Vision
p. 56

DENTAL SLEEP MEDICINE
The genesis of this magazine came from my experience
over the past few years in
Doctors always asked me what others are doing and I never had all the answers. Now, thanks to Dr. Allman, Dr. Rondeau, Dr. Tache, and all the other great doctors that offered advise and suggestions, we now have the Dental Sleep Magazine. In it
stories and cases from their own personal and up front perspective. I would like to thank my dear friend Dr. Maurice Salama for his wonderful article about the importance of education.
In the immediate future, we plan to open 20 SGS Sleep Study Clubs around the country and, thereafter,
add more all over the world. We are partnering with the leading doctors, most of whom are AADSM (American Academy Dental Sleep Medicine) members and Diplomats to accomplish this lofty goal. Each study club will arrange 2 to 4 seminars in its area and
consulting team to coach new members. This will help educate more dentists to treat the millions of patients suffering from Obstructive Sleep Apnea and Snoring. In the future, just log on to www.
you. Despite our rapid growth, there are
needs. Even if all the 170,000 dentists in the United States educate and treat
met. We recommend that you join us and
It would be our pleasure to feature all applicable articles in the Dental Sleep Magazine. If you would like to submit an article, please send it to us at [email protected]. Thanks for reading this magazine and for joining us in our efforts to reach all those patients in need of assistance with thier sleep disorders.
Sincerely,Rani Ben-DavidPresidentSleep Group Solutions
Tamir CohenCEO - Sleep Group [email protected]
The Field of Dental Sleep Medicine is GrowingHere at Sleep Group Solutions, we have accomplished a lot thanks to our wonderful clients, partners and affiliates.
by Rani Ben-David, President
2
“In my 6 years in the Dental Industry, I have developed and continue to develop a lot of relationships with doctors. I am often asked questions on companies and their products and what my input is on them. Before SGS came along, although I knew it was a good product, I had a hard time supporting the Eccovision System, because of lack of long-term support and empty promises. SGS has really turned this around and has a great knowledgeable supporting cast that goes above and beyond what’s expected of them. They have even helped mend relationships with older users that dealt with the previous company. I hold my relationships in high regard and would work with and refer doctors to SGS without hesitation.” - Shane, BioResearch
Rani Ben-DavidPresident
Eldar AdiGeneral [email protected]
Dr. Brian AllmanCo-Editor
Dr. Dan TacheCo-Editor
Contributed ArticlesDr. Brock RondeauDr. Chris HansenDr. Brian Billard
Dr. Dawne E. SlabachDr. Michael PecenkaDr. John T. HeraldDr. Steven J. ScheerDr. Gy Yatros
Dr. John FarringerDr. Donald E. FrantzDr. Melody A. Barron
Randall L. Haupt, RPSGTDr. Michael LuciaDr. John C. JeppesenDr. Robert L. HorchoverDr. Lisa MatristeDr. Maurice SalamaDr. Jamison R. Spencer
Donald BurkeCreative Director
Sleep Group Solutions16830 Northeast 19th AvenueNorth Miami Beach, FL 33162Toll-Free 1.866.353.3936Email: [email protected]

WWW.SLEEPGS.COM
For many people, doing what is good for you is not easy – like exercising several times a week, eating foods
that are healthy and following your treatment regime for your chronic disease. Adherence or compliance to therapy can be particularly onerous when it involves using a device like continuous positive airway pressure (CPAP) to treat obstructive sleep apnea. The mask, the hose, the air blowing in
So it is easy to understand why people might not use their therapy even if it is
The American Sleep Apnea Association
organization dedicated to educating the public about sleep apnea and enhancing the lives of those affected by the condition. The ASAA sponsors a network of support groups around the United States under the name A.W.A.K.E. that is an abbreviation for Alert, Well And Keeping Energetic. The A.W.A.K.E. support group model has three distinct objectives: mutual support, continuing education and empowerment. It is easy to think when faced with using a challenging therapy like CPAP that you are the only person in the world having to endure this hardship.
Helping Keep People A.W.A.K.E.Alert, Well and Keeping Energetic.
By Edward Grandi, Executive Diretor of American Sleep Apnea Association
The support group brings together people, some who have adapted well to treatment and others who are just getting started. There are questions the doctors can answer and then there are questions that when answered by someone living with the condition will make the newcomer feel much less alone. The treatment of sleep apnea continues to evolve. The support group is an
excellent way to stay up-to-date on new and alternative therapies. Expert speakers can provide information
on how to address certain treatment issues and to showcase improvements in the masks and devices. Continuing education about sleep apnea helps make the patient an informed consumer of healthcare, which is critical for maintaining good health. An apneic who feels supported in the treatment and is informed is an empowered patient – this is the ultimate objective of the support group. Not only is he or she adherent to their chosen therapy
can also “pay it forward” by helping to raise awareness about a serious potentially life threatening disease and to help others who may be facing the same challenges they faced before they found support. For more information about the A.W.A.K.E. Network of support groups
our web site: www.sleepapnea.org Dentist that want to join the A.W.A.K.E can contact Sleep Group Solutions at [email protected] or go to www.sleepgs.com.
An apneic who feels supported in the treatment and is informed is an empowered patient.
3WWW.SLEEPGS.COM

DENTAL SLEEP MEDICINE4
Throughout my years of educating dentists and physicians how to identify, diagnose and treat OSA in their
people seem to have a story about how OSA has affected their life in some way. Some stories refer to relationships and how sleep apnea and snoring have driven a husband and wife to sleep in separate bedrooms. Some stories are health related, one friend of mine had a heart attack at
age 40 and it was only after this event did he realize that apnea was the underlying cause.
Many others have not been as lucky. NFL Hall of Fame
widely attributed to untreated OSA. Millions of others, perhaps even one of your friends or family members have suffered similar fates caused by OSA without a diagnosis. Did you know that 70% of stroke victims have sleep apnea? (Bassetti et al. Sleep. 1999)
of attention, what is statistically more dangerous than drunk driving? The answer is tired driving and OSA is a huge contributing factor. Sleep apnea deprives people of the clean rejuvenating sleep they need and replaces it
pressure and heart rate increases. As a result, people suffering from OSA are seven to twelve times more likely to be involved in an auto accident because of their
excessive sleepiness. Did you know that sleeping for only 4 hours results in equivalent reaction times to those of someone with a blood alcohol content of .08%? This leads me to one, of my many, OSA stories. On January 6th, 2008 a bus load of skiers was traveling back from a Utah ski resort to my hometown of Phoenix, AZ. My father-in-law along with a few of his friends were on this trip. As the bus passed near the four
corners area with hundreds of miles of mountain and desert in every direction its speed began to increase. This
continued prompting one passenger to yell at the driver to slow down. A while later the speed began to increase again, this
time nobody yelled at the driver. On board video showed passengers
bracing for impact as the bus approached
expression remained unchanged – he was sleeping! The bus virtually disintegrated as it rolled down an embankment throwing almost every passenger out. My father-in-
but treatable injuries. 9 people died that night including 2 of his friends. Over 15 months later, in April 2009, the NTSB reported that the driver suffered from sleep apnea and faulted his fatigue as the cause of the accident. There is no other disease or disorder as deadly as OSA that is undiagnosed to this level. If you are not already screening and treating patients I ask that you take a course and get started. Preventing heart attacks and strokes is truly rewarding. Taking a tired driver off the road could change the lives of countless others.
one and not even know it.
What Is Your O.S.A. Story?Many people seem to have a story about how OSA has affected their life in some way.
by John Nadeau, Vice President, Sleep Group Solutions

WWW.SLEEPGS.COM 5
Thank you all for your overwhelming and enthusiastic response to our inaugural issue of
Dental Sleep Medicine Magazine released earlier this year. Comments have been unanimously positive prompting SGS founders, Rani Ben-David and Tamir Cohen, to publish a second installment with an even broader dental scope including topics related not only to dental sleep medicine, but to advanced dental restorative techniques as well. Volume 2 uniquely embodies the
as a clinical resource offering numerous articles from seasoned “wet-
experts. Dental sleep medicine is now experiencing explosive demand from savvy dental consumers seeking CPAP alternatives as well as dentists eager to become involved in providing oral appliances for snoring and OSA. As one devoted to “spreading
role, I have found our sleep seminar attendees increasing in number, level of sophistication and genuine enthusiasm. More dentists are anxious to add dental sleep medicine to their practices
communities and bottom line. Standing on the sidelines ignoring our responsibility to include OSA screening of our patients is a tragic oversight in modern dental diagnosis and, in my opinion, we clearly
have a moral obligation to screen for sleep disordered breathing conditions. It is time to also include examination protocol in dental school education. Shame on us for not embracing our responsibility to upgrade our clinical acumen with more vigor!. Obstructive sleep apnea is an “insidious and treacherous health
hazard” (Dr. Keropian) fueling a dramatic rise in morbidity and mortality statistics under the cloak of heart disease, cerebrovascular insult, obesity and hormonal dysfunction conditions. OSA is truly an under-diagnosed and
can be easily screened, referred, diagnosed and treated via a multidisciplinary collaborative medical model which does, in fact, include dental therapeutics. It is this clinical disconnect that dentistry must rectify by playing a vital, if not primary, role. Not tomorrow morning, but, this morning. I am excited to be involved with Dental Sleep Medicine Magazine. I am also excited to incite my profession to become involved in the medical-dental sleep medicine model. Please, use these clinical articles as a reference and guide to advance your dental sleep medicine
contributors. And lastly, continue to attend
Killer!Dental Sleep Magazine - clinical articles to advance your dental sleep medicine education journey
by J. Brian Allman, DDS, Co-Editor DSM Magazine
lectures and seminars to further your
many,many more dental seep medicine physicians out there!
Enjoy Volume 2!
J. Brian Allman, DDS, DABDSM, DAPM, FAGD, FAACP, FICCMO, FIAO, FASGD, FAAFOCo-editor DSM Magazine
Awards
Orthopedics
Memberships
DENTAL SLEEP MEDICINE
Cone Beam 3D Imaging Systems
NewTom VGi Flex–The Mobile Scanning Center
Sleep Apnea, Airway Studies,TMJ Analysis
Perfect for Group Practices
Large FOV, Smallest Focal Spot
Setting the Standard in Patient Care.
914.592.6100 800.592.6666
www.afpimaging.com
Contact Daniel Fields for More Information1-800-592-6666 EXT 101
“NewTom VG has become an important tool in the diagnosis, treatment and patient education of sleep
apnea for my dental practice”
– Michael L. Gelb DDS, MS
The Global Imaging Leader
Experience | Trust | Innovation6
Is Your Team Snoozing?co
nti
nued
educ
atio
n
Who can ignore the onslaught of information about Sleep Apnea
Long time suffers of Sleep Apnea are now being inundated with information about an alternative to the dreaded CPAP machine. This media blitz has patients hitting the internet hungry for information and wondering if they too can exchange the traditional ball and chain for a more conventional method of treating apnea. This certainly is the new wave in dentistry and an incredible opportunity for dentists to increase their bottom line, but how?
incorporating Sleep Apnea alternatives into your practice repertoire is Education - Just as potential
information, so are dentists. You
numerous seminars at various levels. It is important to educate your entire team about Sleep Apnea Dentistry. Think about
team approach to be successful! Everyone on the team has to know how to “walk the walk” and “talk the talk”. Your team
should be familiar with basic dental sleep
appliances used to treat sleep apnea, and be comfortable discussing basic sleep apnea questions.
Basic Systems - Once you have
to establish basic systems for everyone to
chart for your team to follow for sleep patients which includes detailed steps of the appointment process beginning with the initial phone call. Your system should detail each step of the appointment process including scripting for your team to follow in regards to insurance and treatment questions. It is imperative
to differentiate your practice from the
own Sleep Apnea treatment modalities.
but the key is to write the process down so
that everyone is clear as to what needs to be done and who is responsible for each step. Role-playing - is also an integral part
to ironing out any obstacles, glitches, or communication
Marketing - You
begin marketing Sleep Apnea treatment. By adding a few questions to your medical history pertaining to Sleep Apnea or adding the Epworth Sleep Test to your new patient paperwork, screenings will automatically become part of your routine. Your educated team can take this important screening information and discuss alternatives with your patient before you even enter the treatment
room to conduct an exam. Chances are with one simple question, “Do you or someone you know snore?” you will be well on your way to incorporating Sleep Apnea alternatives into your practice.
Dawn Patrick is the owner of In Office Coaching, a coaching company focusing on building exceptional teams, one system at a time. By focusing on teams one-on-one to develop customized systems, daily stress is reduced and the profitability of the practice is increased. Dawn is also Practice Administrator for Fairlington Dental located in Arlington, Virginia.
For more information on In Office Coaching, visit www.InOfficeCoaching.com or contact Dawn Patrick directly at [email protected]
Are you losing potential Sleep Apnea Patients?
by Dawn Patrick

WWW.SLEEPGS.COM
Cone Beam 3D Imaging Systems
NewTom VGi Flex–The Mobile Scanning Center
Sleep Apnea, Airway Studies,TMJ Analysis
Perfect for Group Practices
Large FOV, Smallest Focal Spot
Setting the Standard in Patient Care.
914.592.6100 800.592.6666
www.afpimaging.com
Contact Daniel Fields for More Information1-800-592-6666 EXT 101
“NewTom VG has become an important tool in the diagnosis, treatment and patient education of sleep
apnea for my dental practice”
– Michael L. Gelb DDS, MS
The Global Imaging Leader
Experience | Trust | Innovation7WWW.SLEEPGS.COM 7
DENTAL SLEEP MEDICINE8
Electrodiagnostic instrumentation has catapulted heath care diagnoses
is no different. In fact, rhinometry in particular, offers essential utility when screening prospective oral appliance therapy patients. Understanding the modern approach to treating obstructive sleep apnea mandates abandoning the old model of treating patients in a near vacuum and pursuing, cultivating and embracing a multi-disciplinary collaborative medical approach to treating this insidious and deadly pandemic condition. This medical-dental model involves now a quartet of modalities used both synergistically and adjunctively. A four pronged approach to treating OSA patients leverages the talents and expertise of aware dentists, ENTs, allergists and sleep specialists providing the best outcomes. The four pronged approach can be likened to four
intersecting one another. The four
following disciplines and therapies: positive airway pressure (PAP), surgery, oral appliance therapy and nasal patency therapies. While the
“players”, the fourth, nasal patency, is a relative newcomer.
Nasal patency, as revealed in current literature, plays a vital role in OSA therapy. Research shows that nasal airway resistance (NAR) can positively or
and OA therapies. Higher NAR negatively
evaluate nasal patency as part of our OA screening protocol. Not all patients referred for OAT will
have had endoscopic examination to rule out the possibility of nasal blockage. It behooves the astute dental sleep medicine physician to use rhinometry to easily, quickly, economically and non-invasively evaluate nasal patency which can
OAT prognoses for OSA sufferers. Abnormal test results should alert the
dentist to follow-up with ENT referral for expert paranasal sinus evaluation. Close attention to this narrowest member of the OSA therapy quartet will increase OA outcomes and put the ability to examine the initial few centimeters of our airway into the skilled hands of our dental sleep colleagues. The following case illustrates the utility of rhinometry in dental sleep medicine practice and should also raise concern for rhinometry non-users. In fact, the author welcomes all collegial discussion regarding the use of rhinometry ([email protected]).
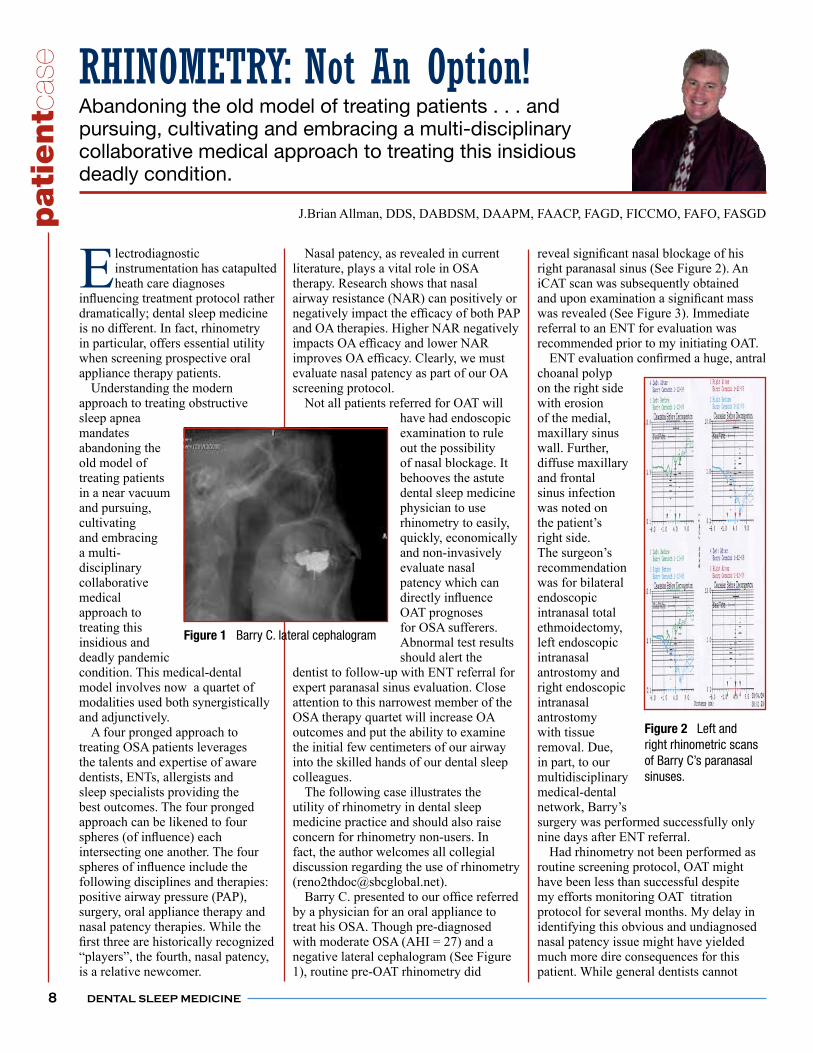
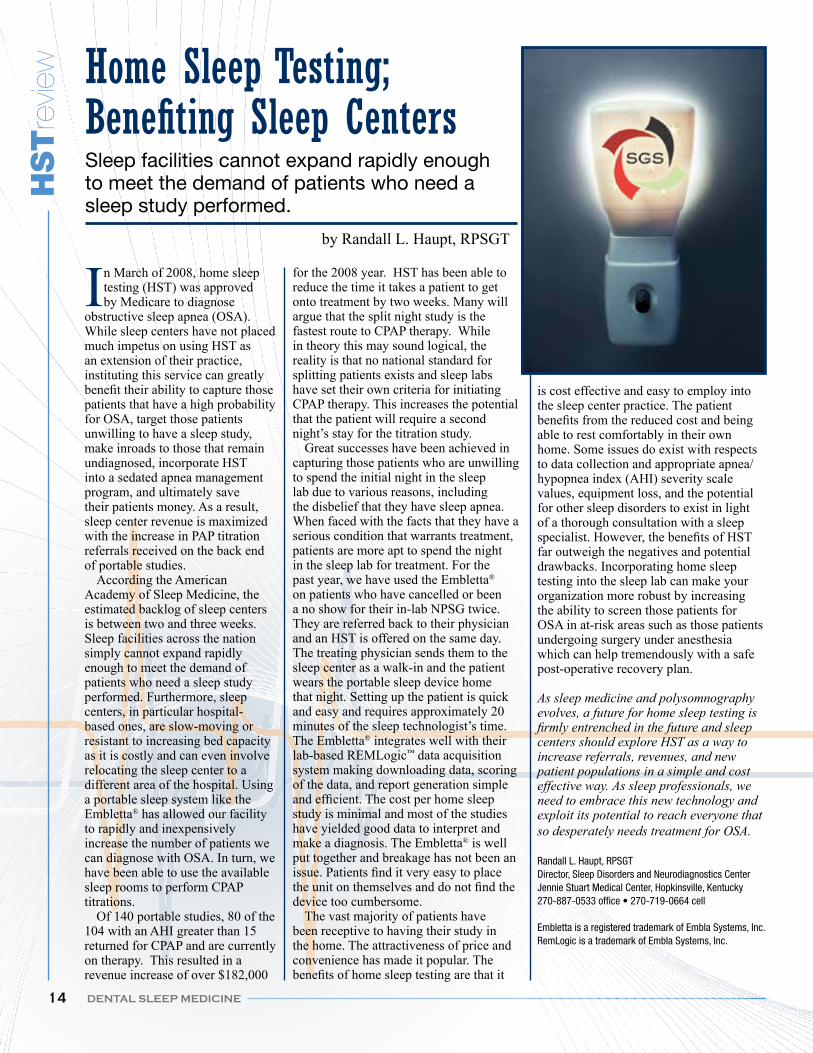
by a physician for an oral appliance to treat his OSA. Though pre-diagnosed with moderate OSA (AHI = 27) and a negative lateral cephalogram (See Figure 1), routine pre-OAT rhinometry did
right paranasal sinus (See Figure 2). An iCAT scan was subsequently obtained
was revealed (See Figure 3). Immediate referral to an ENT for evaluation was recommended prior to my initiating OAT.
choanal polyp on the right side with erosion of the medial, maxillary sinus wall. Further, diffuse maxillary and frontal sinus infection was noted on
right side.
recommendation was for bilateral endoscopic intranasal total ethmoidectomy, left endoscopic intranasal antrostomy and right endoscopic intranasal antrostomy with tissue removal. Due, in part, to our multidisciplinary medical-dental
surgery was performed successfully only nine days after ENT referral. Had rhinometry not been performed as routine screening protocol, OAT might have been less than successful despite my efforts monitoring OAT titration protocol for several months. My delay in identifying this obvious and undiagnosed nasal patency issue might have yielded much more dire consequences for this patient. While general dentists cannot
RHINOMETRY: Not An Option!
J.Brian Allman, DDS, DABDSM, DAAPM, FAACP, FAGD, FICCMO, FAFO, FASGD
Abandoning the old model of treating patients . . . and pursuing, cultivating and embracing a multi-disciplinary collaborative medical approach to treating this insidious deadly condition.
pat
ientc
ase
Figure 1 Barry C. lateral cephalogram
Figure 2 Left and right rhinometric scans of Barry C’s paranasal sinuses.

WWW.SLEEPGS.COM
utilize endoscopic procedures, thank goodness for rhinometry!
Editorial note: In my opinion, electrodiagnostic equipment such as pharyngometry and rhinometry are not an option.
is basic to modern dental sleep medicine. Read about the utility of pharyngometry in our next DSM Magazine. Brian.
9
Figure 3:Barry’s right paranasal sinus. A substantial blockage of the paranasal sinuses is eas-ily missed by the dental sleep physician without rhinometry.
Sleep Group Solutions supports the American Sleep Apnea Association
and is working in collaboration with there AWAKE program.
SGS Clients if you would like to be a speaker in the
A.W.A.K.E program in your area please contact us at [email protected]
and will put you in contact with your local AWAKE Group.

DENTAL SLEEP MEDICINE10
My wife kicks me in the middle of the night. She “claims” it is to
suspect otherwise. How many times have we heard similar stories from our patients? This was me approximately twenty years ago. After doing some research I knew I would not wear the CPAP. The Elastic Mandibular Advancement (EMA®) appliance was created as a treatment alternative. The primary treatment mechanism of opening the bite and gently moving the mandible forward is achieved with the use of elastic straps that offer varying degrees of mandibular advancement. To increase effectiveness, button hooks and elastic straps are placed in the cheek area encouraging maximum anterior tongue
dictate vertical opening. To be patient friendly, it had to be as small and as noninvasive as possible. The elastic straps allow unsurpassed lateral movement and overall TMJ comfort. The hard base of the EMA® Custom increases the tooth anchorage, stabilizing the teeth. There are several things I have observed during my years of clinical experience that I feel are important to keep in mind when treating sleep disordered breathing: ORAL CAVITY SIZE - Orthodontists have focused on the size of the oral cavity, concerned that the size of the maxilla and mandible is large enough to allow straight teeth upright over basal bone. Why does oral cavity size matter? Tongues have not gotten smaller. With a smaller oral cavity, because of evolution, diet or dentistry, the crowded tongue is forced posterior blocking the oral pharynx. TOOTH MOVEMENT - Is a change
a relocation of the condoyle in the fossa? With continual night time mandibular advancement, both are to be considered. To discourage tooth movement, orthodontists must increase “tooth anchorage”. It is easy to tip teeth with appliances constructed with soft liners and clasps. The EMA® appliance, like retainers, is made out of hard material
tipping. It is important to communicate to the patient information about relocation of the condoyle. Instruct the patient to chew sugar free gum after removal of their sleep appliance each morning to help recapture the condoyle. SITE OF CLOSURE ADVANCEMENT VS. VERTICAL
(Henke, Kuna and Frantz), 75% of the subjects tested closed at or above the velophaynx. All subjects closing below the velopharynx treated with the EMA® appliance had AHI reductions to less than six events per hour. This was achieved through mandibular advancements and between 8 and 14 mm of vertical opening (anterior). Our best responder, (AHI reduced from 101 to 10 events per hour) was open 14mm. It is believed that the vertical or caudal displacement brings the soft palate forward and depresses the tongue via the anterior and posterior tonsillar pillars. I have recently been increasing the vertical on patients with great success. AVOIDING TMJ PAIN - When
sleep disordered breathing is properly treated, TMJ and other maladies seem to remediate. If you have a TMJ pain patient with sleep disordered breathing, the last thing you want to do is to lock their mandible forward in one position. The EMA® appliance allows you to gradually move the mandible forward with straps of varying lengths and degrees of
to the musculature of the patient. The elastic straps allow unlimited lateral excursion. Adjusting the bite pads (with a dental bur) is also important. If one side is minutely higher than the other, the high side
will create TMJ pain. PATIENT SELECTION - Examination of the oral cavity will give you a world of information:
Wear facets on the molars and bicuspids Scalloped lateral boarder of the
genioglossus Orthodontics and/or bicuspid extractions Soft palate, short or long webbed shaped
with inferior border very close to the posterior wall of oral pharynx
Uvula – short and pink or long and red (from vibrating all night)
Range of mandibular advancement Retrognathic Neck size (18 or larger indicates breathing
problem) and BMI (29 or greater is 9 -12 times more likely to have OSA)
An Orthodontist’s Perspective of Sleep Disordered Breathing
By Donald E. Frantz, DDS
Fifty years clinical experience and the evolution of the EMA® Appliance
DENTAL SLEEP MEDICINE

WWW.SLEEPGS.COM 11
You can predict the success of an oral appliance by asking the patient to snore while in a supine position. In the middle of this “snore” have them advance their mandible. If they cannot snore with the mandible forward, you can predict success. If advancement alone does not completely stop snoring, have them open and move forward at the same time. If this maneuver stops snoring, this will show the amount of vertical opening needed for that particular patient. PATIENT TREATMENT - The speed with which mandibular advancement
straps on the EMA® Custom appliance depends entirely on the patient. Pain (or lack thereof) can dictate the forward titration of the mandible. If mandibular advancement is not achieving treatment goals, add vertical displacement to the mandible. This can be easily accomplished by adding orthodontic acrylic to the bite pads after roughening with a bur. RELATIONSHIPS WITH SLEEP DOCS - Patients deserve the very best treatment available which I believe is achieved via a team approach including a sleep specialist and a dentist. My expertise and interest lies in the oral cavity and not in the intricacies of scoring polysomnograms. The EMA® appliance was initially created to treat one patient. Over the years it has grown in popularity and we have turned over worldwide distribution to Myerson, the tooth company. Should you be interested in additional information, their website is myersontooth.com/sleepbetter. As always, feel free to contact me through our website at openairway.com. My wife still kicks me at night, but we have ruled out breathing cessation as the motivating factor . . . EMA® Custom appliance. EMA® Custom appliance straps. Showing one length of strap in each of
(durometers). Available in
When an 18 year old male
new patient, what is your protocol? Are you concerned about his weight, the size of his neck, or the size of his airway? When we went to dental school, we learned to take a complete medical history including previous diseases, operations, etc. We also learned how to do a periodontal examination to check for periodontal disease, as well as an examination of the hard tissues for the presence of dental
and considered the best alternatives to replace them. Most dental schools worldwide do not educate dentists on how to identify patients who snore and have obstructive sleep apnea. This seems
eduction when you realize the comorbid factors of untreated obstructive sleep apnea, i.e. cardiovascular disease including high blood pressure, heart attacks, hypercapnia, cardiac arrhythmias, and strokes. Other health complications include type 2 diabetes
The medical profession, in my opinion, is also not adequately educating medical doctors to play a greater role in the diagnosis and treatment of these patients. Dr. Wayne Halstrom, one of the pioneers of obstructive sleep apnea (OSA), had to have a serious motor vehicle accident due to excessive daytime sleepiness, before he was sent for a sleep study, where he was subsequently diagnosed with obstructive sleep apnea. There are three recommended treatments for patients who snore and
Protocol For Snoring Problems Male Age 18
By Brock Rondeau, D.D.S., I.B.O., D.A.B.C.P.
An invaluable addition to appliances and treatment for sleep disordered patients.
treatment recommended by the medical profession is the CPAP device. I do recommend this form of treatment for patients who are diagnosed with the polysomnogram and have severe OSA. The problem is that while the CPAP is successful in the majority of obese patients with severe OSA, the compliance rate with mild to moderate OSA patients is extremely poor. The American Academy of Sleep Medicine in the January 2006 issue of Sleep made the statement that for mild to moderate OSA, the oral appliance is
patient compliance is much higher with the oral appliance which is extremely comfortable. The key to success is to eliminate any airway obstructions in the nasal, oral or throat areas prior to the fabrication of the oral appliance. I believe that the compliance rate in
appliance. The third treatment option is the surgical approach. Most patients would prefer the oral appliance rather than the CPAP or surgery. However, some patients with enlarged tonsils or adenoids, deviated septums, enlarged turbinates, polyps, tumors in the nasal area, enlarged uvula, or low soft tissue palatal drape do require surgery for resolution of these problems. With regard to the age 18, overweight, male patient who comes to
protocol be for this patient? Would you give him an Epworth Sleepiness Scale? Would you measure his neck? Would you be suspicious of snoring or obstructive sleep apnea? An early diagnosis of our younger patient could
Continued on Page 47

DENTAL SLEEP MEDICINE12
Oxygen Is Really Under-Rated!
by Dr. Melody A. Barron
It is a simple Truth
This is a common phrase I use
on a daily basis. It gets my point across. The importance of it is emphasized when you consider how long you can go without food and water as compared to how long we can go without oxygen. We think about it on an airplane (you know the mask demonstration and all) or in the hospital. Look at the havoc that it wreaks
It is a major health problem! The prevalence of the disorder may be underestimated due to fact that the disease is often undiagnosed, but
the multitude of health problems that often co-exist. It is so often overlooked in a patient by physicians and dentists alike. The patient very often is taking one or several medications for one or many of the “symptoms,” but the presence of sleep disordered breathing was totally overlooked. This is one of those
times when “guilty until proven innocent” by polysomnogram (PSG) is a good rule of thumb. Dentists are in the best position to recognize it if we remember what to look for. We treat patients and their families for years usually on a regular basis. We should keep our eyes and ears open. Are there noticeable changes in the patient and their health. We are doctors after all. It is not all about teeth. You will be the hero for that patient if “YOU” recognize the possibility of this health problem which has serious health implications. To begin add these simple questions to your health history:
Other things to look for (I call them my RED FLAGS):
regularly? (Prescription or OTC)
Are they tired “all the time”?
anytime? (This could be driving.)
When the patient has their mouth open can you see the oropharynx? Does their tongue seem to be everywhere? Does the tongue retract into the oropharynx when they open? Can you see their uvula?If there is evidence of bruxism, you should always suspect the presence of sleep disordered breathing. Remember “guilty until proven innocent,” they may destroy the beautiful dental work you just placed. Ask that patient have they ever had a sleep study. You will be surprised how may have had a sleep study, been prescribed a CPAP and do not use it anymore. The patient will be pleasantly surprised that you recognized that possibility. The patient can be female, male or a child.
have sleep apnea to simply treat them for
licensure to make this diagnosis. Assuming that the patient just snores, is making a
diagnosis! An accurate diagnosis is made by
physician. If the sleep study is negative for the presence of sleep apnea, OK now you know! After this diagnosis is determined, then the process of determining the best method of treatment can be treatment planned. This can be Oral Appliance (OA) therapy, CPAP only or combination of both. Training and experience in treating with oral appliance therapy along with a good interdisciplinary care relationship with a
for the patient.
oral appliance therapy, learn to recognize it
The AADSM can help to guide you toward a dentist in your area. You will be shocked that when you start looking at your patients
a time when that recognition may save that
quality of life. Who knows, you could even be looking in the mirror! Dr. Barron is a graduate of the University of Tennessee College of Dentistry, class of 1992. She graduated with honors, and received the American Association of
growth and development of the craniofacial complex for that graduating class. Previous to attending UT College of Dentistry, Dr.
degree in Medical Technology and had a ten-year career in a hospital medical laboratory. She has treated patients with general orthodontics since 1994. Dr. Barron has limited her practice to the treatment of Temporomandibular Joint Disorders and Sleep Disorders by Oral Appliance Therapy since 2006. She is owner and director of the TMJ and Sleep Therapy Centre of Memphis.
Dr. Barron holds memberships in the following:Academy of Dental Sleep Medicine(AADSM)American Academy of Sleep Medicine(AASM)International Association of Orthodontics/American Academy of Functional Orthodontics(IAO,AAFO)American Academy of Craniofacial Pain(AACP)American Academy of Pain Management(AAPM)
Common Co-Morbidities of SLEEP DISORDERED BREATHING:
The list goes on and on!
DENTAL SLEEP MEDICINE

WWW.SLEEPGS.COM 13
Approved PACE Program ProviderFAGD/MAGD Credit
Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement
1/2008 to 2/28/2012
Brock Rondeau, D.D.S., I.B.O., D.A.B.C.P.Diplomate International Board for OrthodonticsDiplomate American Board of Craniofacial PainOver 18,000 Dentists have attended his courses and study clubs
Oral Appliances to Treat
Snoring and Sleep Apnea
The Dentist’s Role in Snoring and Sleep Apnea
2009 - 2010 Course Locations
Course Fee
Toronto, ON August 28 & 29, 2009San Francisco, CA December 12 & 13, 2009Toronto, ON January 9 & 10, 2010Chicago, IL April 24 & 25, 2010
Doctors $995 / Staff $395Course fee includes extensive 288 page course manual and article CD.Earn 14 CE Hours.
Why You Should Take This Course
The American Academy of Dental Sleep Medicine in the January 2006 issue of “Sleep” recommends the use of oral appliances as the first treatment option for patients with mild to moderate sleep apnea. This presents a tremendous opportunity for dentists to become involved in the ever increasing new field of sleep disorders.
Course Content
Sleep Apnea Symptoms and Causes Sleep Examinations and Forms Hospital Sleep Studies (Polysomnogram) Home Sleep Studies Pharyngometer to Evaluate Pharyngeal Airway Rhinometer to Evaluate Nasal Airway Different Sleep Cycles Summary of Sleep Disorders CPAP - Continuous Positive Air Pressure Surgical Solutions for Sleep Apnea Comparison of Different Oral Appliances References and Articles Marketing Your Sleep Practice
90 million people in North America suffer from
sleep disorders including insomnia, snoring
and sleep apnea. Dentists need to become
involved in helping these patients.
DENTAL SLEEP MEDICINE14
HST
revie
w
In March of 2008, home sleep testing (HST) was approved by Medicare to diagnose
obstructive sleep apnea (OSA). While sleep centers have not placed much impetus on using HST as an extension of their practice, instituting this service can greatly
patients that have a high probability for OSA, target those patients unwilling to have a sleep study, make inroads to those that remain undiagnosed, incorporate HST into a sedated apnea management program, and ultimately save their patients money. As a result, sleep center revenue is maximized with the increase in PAP titration referrals received on the back end of portable studies. According the American Academy of Sleep Medicine, the estimated backlog of sleep centers is between two and three weeks. Sleep facilities across the nation simply cannot expand rapidly enough to meet the demand of patients who need a sleep study performed. Furthermore, sleep centers, in particular hospital-based ones, are slow-moving or resistant to increasing bed capacity as it is costly and can even involve relocating the sleep center to a different area of the hospital. Using a portable sleep system like the Embletta® has allowed our facility to rapidly and inexpensively increase the number of patients we can diagnose with OSA. In turn, we have been able to use the available sleep rooms to perform CPAP titrations. Of 140 portable studies, 80 of the 104 with an AHI greater than 15 returned for CPAP and are currently on therapy. This resulted in a revenue increase of over $182,000
for the 2008 year. HST has been able to reduce the time it takes a patient to get onto treatment by two weeks. Many will argue that the split night study is the fastest route to CPAP therapy. While in theory this may sound logical, the reality is that no national standard for splitting patients exists and sleep labs have set their own criteria for initiating CPAP therapy. This increases the potential that the patient will require a second
Great successes have been achieved in capturing those patients who are unwilling to spend the initial night in the sleep lab due to various reasons, including the disbelief that they have sleep apnea. When faced with the facts that they have a serious condition that warrants treatment, patients are more apt to spend the night in the sleep lab for treatment. For the past year, we have used the Embletta® on patients who have cancelled or been a no show for their in-lab NPSG twice. They are referred back to their physician and an HST is offered on the same day. The treating physician sends them to the sleep center as a walk-in and the patient wears the portable sleep device home that night. Setting up the patient is quick and easy and requires approximately 20
The Embletta® integrates well with their lab-based REMLogic™ data acquisition system making downloading data, scoring of the data, and report generation simple
study is minimal and most of the studies have yielded good data to interpret and make a diagnosis. The Embletta® is well put together and breakage has not been an
device too cumbersome. The vast majority of patients have been receptive to having their study in the home. The attractiveness of price and convenience has made it popular. The
is cost effective and easy to employ into the sleep center practice. The patient
able to rest comfortably in their own home. Some issues do exist with respects to data collection and appropriate apnea/hypopnea index (AHI) severity scale values, equipment loss, and the potential for other sleep disorders to exist in light of a thorough consultation with a sleep
far outweigh the negatives and potential drawbacks. Incorporating home sleep testing into the sleep lab can make your organization more robust by increasing the ability to screen those patients for OSA in at-risk areas such as those patients undergoing surgery under anesthesia which can help tremendously with a safe post-operative recovery plan.
As sleep medicine and polysomnography evolves, a future for home sleep testing is
centers should explore HST as a way to increase referrals, revenues, and new patient populations in a simple and cost effective way. As sleep professionals, we need to embrace this new technology and exploit its potential to reach everyone that so desperately needs treatment for OSA.
Randall L. Haupt, RPSGT
Jennie Stuart Medical Center, Hopkinsville, Kentucky
Embletta is a registered trademark of Embla Systems, Inc. RemLogic is a trademark of Embla Systems, Inc.
Home Sleep Testing;
by Randall L. Haupt, RPSGT
Sleep facilities cannot expand rapidly enough to meet the demand of patients who need a sleep study performed.
WWW.SLEEPGS.COM 15
DENTAL SLEEP MEDICINEDENTAL SLEEP MEDICINE16

WWW.SLEEPGS.COM
For More Information Call:
1-866-363-3936
17
Rondeau Seminars Jointly O!ered With Sleep Group Solutions

DENTAL SLEEP MEDICINE18
I sat down with Dr. Lucia to ask him a few questions that I thought
Dental Sleep Medicine community as a whole and here are his answers.
DSM: What was your
sleep medicine?
My fellowship training was at Wake Forest, which had a dental school across the
with the dental students and the program, I had a high level of interest at a multidisciplinary level. At an annual national sleep meeting, I enrolled in the dental lectures and spent the day learning about oral appliance therapy and dental sleep medicine. After hearing the lectures, I decided that dentistry was an important facet of sleep medicine
DSM: How did you become involved with Dr. Allman, a dentist in Reno, NV?
I started practice in Sparks in 2000, looking for individuals that
for referral sources and
trusted colleagues. In 2005, Dr. Allman contacted me as he was developing his sleep practice and I decided that he was a very well educated dentist that I would feel comfortable referring my patients to. Eventually we developed the “Sierra Sleep Group,” which is a study group of medical professionals of many
connections and advancements in our
DSM: Tell me a little more about this study group;; how would another doctor or dentist go about starting something similar?
dentist, sleep specialist and an ENT physician and built from there. It is important to wait for the right people to
the group. Hand pick people that you can develop a professional relationship with and that you can feel comfortable sending your patients to. From the network that is built between the members, you can effectively refer and co-treat in a much more collegial way. Dentists are not outliers, they should be an integrated part of the healthcare team. What grows from the study group
The main goal was to create interaction
paths very often. We meet once a month,
for communication that cannot happen during the day with patients.
DSM: What would you say is the
best way for a dentist to initiate a relationship with a sleep specialist, such as yourself?
Having a practice representative can be very helpful, you can have them drop off cards and or letters to declare intentions
the dentist and the MD. Your staff can represent you very well, and may
may not want to work with because of any number of factors such as staff,
can do a sort of “screening” and set up
would want to work with.
and sell the fact that you are a resource. Use an evidence based vs retail
to make a quick buck, you will not get referrals. Try not to “oversell” or use non
the physician. Use data that can back up what you do, “no wallet biopsies.” What
making ability. Remember, everything
No “free exams,” cheap interactions are not wanted referral sources. It is very important to market yourself as a professional you have been through
Remember, we need you as a resource
apprehensive about meeting your sleep specialist, even if the relationship does not develop right away, be patient. If you presented yourself well and made a
MD
Inte
rvie
w Dr. Michael LuciaTriple board certified physician with both academic and private practice roots and strong ties to medical education. He is the Medical Director and lead physician at Sierra Pulmonary and Sleep Institute, a pulmonary function lab, comprehensive pulmonary rehabilitation facility, four bed AASM-accredited sleep lab, complete cardiopulmonary stress testing lab and allergy clinic.

WWW.SLEEPGS.COM 19
solid impression, when they need you, (and they will) your name will be on the top of their list.
DSM: How do you feel the collaboration between dentists and MD Sleep Specialists will affect the OSA population as a whole?
Healing for all is affected by sleep. Dental disorders are worse with sleep disorders, poor immune function is also associated with sleep disorders. Who else is better to capture more patients with simple screening than the dentist? More patient awareness = more treatment and fewer problems as a whole. Dentists can provide great input as a trusted advocate for that patient. Dentists that are treating OSA without an MD on their team may be missing huge pieces of the puzzle that we are more equipped to deal with. As a sleep center we have the ability to treat any co-morbid factors that the patient may
OSA is accompanied by co-morbid factors.
DSM: You made a distinction between Sleep Centers and Sleep Labs. can you tell me about the differences? What should a dentist look for?
A Sleep Center is comprehensive, there
running the center. They must have a clinic to treat all types of sleep disorders. They also treat both adult and pediatric patients. A Sleep Lab does testing on adults OR children, not both. They do not have a full clinic, they only treat airway disorders. This means no treatment of things like Narcolepsy, allergies, cardiac function etc. There
physician reading the studies at both, however, at the sleep center, that physician can actually treat anything that is found. I would recommend a Sleep Center, personally. The other accreditation
standard that you want to make sure that you look at is either JCAHO (Joint Commission on Accreditation of Healthcare Organizations) accreditation or AASM (American Academy of Sleep Medicine) accreditation. JCAHO does not have clinical standards. They check for HIPPA compliance, licensing compliance, health and safety requirements compliance, etc. They are a hospital accreditation commission that
for sleep medicine. For AASM accreditation, the center has to meet about 31 pages of criteria, from clinical
studies, how technicians are trained, etc. to computer monitor size and a gamete of other criteria. It is a much more
a continuous basis. All of the guideline criteria are on the AASM website, should anyone want to see them. We are an AASM accredited Sleep Center, so we meet all of those standards.
DSM: Finally, do you have any advice for dentists who are establishing their relationships with sleep specialists and starting their sleep practice?
My advice would be to jump into this, wholeheartedly. Do your research,
team and go for it! Standards are changing and medicare is helping the process. The accreditation process is changing and evolving, look for younger doctors who are fellowship trained, they will have dental sleep medicine education. Home studies are a wave of the future and they are coming to be a huge part of this market, for both dentists and sleep specialists, home studies are a very valuable tool. Also, when working with sleep
specialists, follow up questions are important to ask, if they do follow up with their CPAP patients, they will need you because of non-compliance. Every
they need another option, and they will eventually try Oral Appliance Therapy once, impress them from the beginning. Look at CPAP compliance with your sleep specialist, use numbers that show how much the patients are wearing their CPAP. The Medicare requirement is 4 hours per night, 4 or more nights per week between day 30 and 90. You can ask for their compliance statistics and go from there (They should have at least an estimate). DME companies have to prove that the patient is wearing the CPAP also the sleep specialist must see the patient to document the subjective improvement within that 30-90 days. Labs that are not trained in these requirements will suffer because they
compliance. Dentists should know these guidelines and practice the same things with visit protocol and follow up. The changes on the horizon will
you should be there when it is time!
Thank you so much to Dr. Lucia for his expertise and his candid answers. We hope that this article will give you a little insight as to what the sleep specialist in your area is thinking, and how you can start developing your multidisciplinary team.
Dr. Michael Lucia’s new, custom designed, state-of-the-art facility Sierra Pulmonary Sleep Institute has nearly 7,000 square feet of clinical space.

DENTAL SLEEP MEDICINE20
Dental Sleep Medicine
By Dr. Dan Taché, DDS
If any of your patients look like these and tell you that they are aware of clenching, grinding, headaches in
the morning, sensitive teeth, excessive daytime sleepiness, GERD, sleep poorly and snore, then you owe it you your patients (and family members yet) to get hold of some of the concepts in this brief article and if you are a DENTAL SPECIALIST (yes, YOU) or just a walking down the street general dentist, just minding your own business, ditto-you have to know this stuff! So, for all of you out there who are doing ok without the hassle of having to learn something new that smacks of medicine, perhaps a little more information might help. Like many of you, I too am a general dentist, and I did not go looking for this, in fact, I am not a writer, never had a Journalism course, so why am I even pounding the keys and doing this? I am editorializing and I just looked that word up. Well, I had my epiphany and got religion and now I have this burden to inform my fellow colleagues that in fact, ALL of us are staring this stuff in the face nearly every day and ALL DAY LONG and if you are treating the effects of sleep and breathing problems and unaware of
or HOW it is that people wear their front teeth down the way that some of them do. Knocking off all manner of enamel and then our veneers and crowns? You must have asked yourself that question an
you what a lot of us think about that at the
No, Thanks Mister, I’ll Take Vanilla!
REWARD (love, respect and gratitude of your patient) for identifying the often-missed cause of these common dental
-sive intake of soda pop, or stress and please, oh please, for the love of everything that is holy, not loss of anterior guid-ance or malocclusion!
end of this article but for now, just a little more background information. This whole Dental Sleep Medicine
send this stuff out when it shows up in
not so easy. Whether you realize it or not,
with it! Well wait, perhaps I am being a bit arrogant, so allow me impart some information, perhaps you might see them as insights, as I did and if and when you GET IT, you may get a little excited too.
to make is that having an understanding of Dental Sleep Medicine is not merely for the few who are willing to treat people with sleep apnea who cannot tolerate Continuous Positive Air Pressure (CPAP) machines. No, it is far more basic than that. Most patients, who come to us, do so because they oftentimes have complaints about the effects of sleep disordered breathing (SDB) and for many of those complaints, a patient may quite often seek help from a dentist totally unaware that these problems are a result of UNDIAGNOSED SDB! The reason that the patient is suffering from signs and
only is he or she unaware that the problem exists but so too is the physician and dentist.
PREVALENCE
Sleep disorders are a very common
problem for many of our patients, both the (very) young and old. Epidemiological and cohort studies conducted in Wisconsin, Pennsylvania, and Spain show estimated prevalence of obstructive sleep apnea upwards of 28% in adults1 and as high as 18% in a pediatric populations2 and that does not account for the prevalence of just upper airway resistance (aka: benign snoring) that in some studies show a prevalence of 38%3. So, why all of the interest and hoop-la about this? Sure, I feel sorry for the kids and adults who have this problem but honestly, why should I care about it? I have so much information to keep abreast of like new cements, resin systems, the
software, that new laser I need (want) and the list goes on. the fact is that some or many common dental problems are clinical manifestations of sleep and breathing problems and if you are treating the effects but ignoring the cause, you are neglecting to recognize that SDB can be life-threatening. A number of recent articles show that snorers with acute myocardial infarction more often died during the night than non-snorers and that smoking, not even habitual smoking was an additional
infarction4.
BRUXISM: A RISK FACTOR FOR SLEEP DISORDERED BREATHING

WWW.SLEEPGS.COM 21
As the above photos imply, SLEEP BRUXISM is a fairly common manifestation of a sleep and breathing problem, in fact, it is referred to as a parasomnia of sleep, an intrusion into normal sleep, like sleep walking and talking etc. In fact, it is cited as the 3rd most frequent parasomnia of sleep. Additionally, often reported by patients who brux are the triumvirate of symptoms
more going on than the need for a free gingival graft or an equilibration, namely: “…subjective sense of choking and blocked breathing during sleep…” “…nocturnal awakenings…”, and “…morning headaches…” 5
If these common clinical complaints are not being reported by your patients, you are either working on a Typodont™ or you
magnitude or prevalence of the problem. At the 2008 American Academy of Sleep Medicine annual meeting in Baltimore, Md, a seminal poster presentation was made by a fellow dentist out of Houston, Texas, Dr. Ron S. Prehn
and his co-author and researcher, Jerald H. Simmons, MD, also of Houston. In my view and that of many who attended as
the culmination of a work well done. The essence of their research was summed up in the poster which you can see below. 6 Wow, does this do for you, what it did
clinician trying to help his TMD patients, this good work, well, to say the very least, rocked my world. This made sense to me and explains why the body will expend so much energy to perform such a seemingly senseless and destructive maneuver . . . getting the jaw forward and/or side to side, helps to stabilize the airway so that we can
why, some bruxers might brux. As you become more aware of the interface between the medical problem of SDB and dental manifestation because of this “compensatory” mechanism, it will begin to clear a lot of things up for you. You will understand that we play a bigger role in the overall health of our patients, so when Mrs. Jones comes in and she you see changes in her health such as elevated blood pressure, and you note that she is now taking SSRIs and alas and alack you
begin to see the erosions and attrition and recession not as an occlusal problem but a manifestation of a survival problem, that of maintaining or regaining an airway. It may be unnecessary to add that the rule is that there are no hard rules and that exceptions are the norm, and certainly stress and anxiety are common risk factors for sleep bruxism too but when you have ruled them out, remember that sleep bruxism and the gaggle of problems and symptoms associated with it, rarely occurs alone and research has shown it can be centrally mediated because our patients are in survival mode when SDB is the reason 5, 7, 7, 8. So when your peri- or post-menopausal happily married grandmother-to-be female patient9 or obese but fat and sassy unstressed male patient comes in for an a recall visit complaining of headaches in the am and “TMJ” and you notice that they are now on beta blockers, please, ask them a simple question: “Do You Snore” and if either one of them says yes, well, you may be on the brink of a breakthrough that may impact his or her life forever.
want to get them in front of a dentist who has some credentials in Dental Sleep Medicine or refer them to a Medical Sleep Specialist. However, there is an excellent screening protocol (among many) which has been shown to be predictive of SDB and it is called the Adjusted Neck Circumference screening for Obstructive Sleep Apnea10 . I am attaching a copy of a handout made from that article. I suggest that you obtain the article and anything written by Ward Flemons, MD. It can be obtained from the New England Journal of Medicine for a fee but it is available all over the Internet for free. There are many resources for growing in your understanding of (Dental) Sleep Medicine. The world we live in, professionally, cannot remain “vanilla” if we are to serve our patients. Sure, you can make a buck living with vanilla while our patients struggle. Hey, make mine “Rocky Road”, the Road Less Traveled. I am up for the challenge, how about you? Sleep apnea should be suspected in patients who are obese, hypertensive, habitual snorers, with excessive daytime sleepiness. In a primary care setting, patients with a “We postulate that Sleep Bruxism (SB) is a compensatory mechanism of the upper
airway to help overcome upper airway obstruction by activation of the clenching muscles which results in bringing the mandible, and therefore the tongue, forward.”
Patient falls asleep.
Mandible falls back bringing the back of the tongue with it.
This triggers a series of events causing a reflexive attempt to open up the airway by increasing masseter tone.
This brings the mandible forward and in many patients improves respirations.
Unfortunately over time this can lead to anterior tooth wear and Symptoms of
1.
2.
3.
5.
Continued on Page 22
DENTAL SLEEP MEDICINE22
high risk of sleep apnea were those who met two of the following three criteria: Snoring
while driving,.
Combinations of clinical variables such as neck circumference or body-mass index, snoring, reports of nocturnal breathing disturbances, and hypertension have been used to predict which patients will have abnormal results on sleep tests. The sensitivity of this approach can be
tends to be low (41 to 63 percent). Neck circumference (measured in centimeters) is adjusted if the patient has hypertension (4 cm is added), is a habitual snorer (3 cm is added), or is reported to choke or gasp most nights (3 cm is added). A low clinical probability corresponds to an adjusted neck circumference of less than 43 cm, an intermediate probability (4 to 8 times as probable as a low probability) to a neck circumference of 43 to 48 cm, and a high probability (20 times as probable) to a neck circumference of more than 48 cm. Together with the consideration of the severity of symptoms, the clinical-probability estimate helps guide management10. To hear and see more of Dr. Tache.You can hear him in one of the seminars www.sleepseminars.com or (see page 31 from old magazine) Dr. Tache has an In
BIBLIOGRAPHY1. Young T, Peppard PE, Gottlieb DJ. Epidemiology of
obstructive sleep apnea: A population health perspective. American journal of respiratory and critical care medicine. 2002;165:1217.
2. Gozal D. Sleep-disordered breathing and school performance in children.
20. 3. Teculescu D, Benamghar L,
Hannhart B, Montaut-Verient B, Michaely JP. Habitual snoring. prevalence and risk factors in a sample of the french male population. Rev
Hallqvist J. Heavy snoring is a risk factor for case fatality and poor short-term prognosis after a first acute myocardial infarction. Sleep. 2008;31:801.
5. Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population*. Chest.
6. Prehn, R.S., Simmons, J.H. Sleep burxism: Poster presentation for the american academy of sleep medicine. 2008;Poster Presentation for the American Academy of Sleep Medicine.
7. Lindberg E, Janson C, Svardsudd K, Gislason T, Hetta J, Boman G. Increased mortality among sleepy snorers: A prospective population based study.
Kato T, et al. Genesis of sleep bruxism: Motor and autonomic-cardiac interactions. Arch Oral Biol.
MW, et al. Subjective and objective sleep quality and aging in the sleep heart health study. J Am Geriatr Soc [Sleep Heart Health Study]. 2008;56:1218.
10. Flemons WW. Obstructive
ANC* = NC + H(4) + S(3) + C/G(3)
(H: Hypertension; S: Snoring; C/G: Choking/Gasping)
Less Than 43Low Probability
43-48Intermediate ProbabilityGreater Than 38
High Probability
* Adjusted Neck Circumference
How likely are you to doze off or fall asleep in the following situations, in contrast to just feeling tired? Use the following scale to choose the most appropriate number for each situation:
0 - Would never doze1 - Slight chance of dozing2 - Moderate chance of dozing3 - High chance of dozing
SITUATION: CHANCE OF DOZING 1. Sitting and reading ___2. Watching television ___3. Sitting, inactive in a public place (i.e. A theater or a meeting) ___4. As a passenger in a car for an hour without a break ___ 5. Lying down in afternoon when circumstances permit ___ 6. Sitting and talking to someone ___ 7. Sitting quietly after lunch without alcohol ___ 8. In a car, while stopped for a
TOTAL EST SCORE: ___
The Epworth Sleepiness Test is a tool, not a diagnosis. However, if your ESS score is: 1-6 Obstructive Sleep Apnea is Less Likely 7-8 Your Score is Average
Obstructive Sleep Apnea is More Likely and You Should Seek the Advice of a Sleep Specialist
EPWORTH SLEEP TEST
Dental Sleep Medicine
By Dr. Dan Taché, DDS
No, Thanks Mister, I’ll Take Vanilla!
Continued from Page 19
WWW.SLEEPGS.COM 23
DENTAL SLEEP MEDICINE
United Sleep Diagnostics, Inc. (USD) is a Joint Commission accred-
(American Academy of Sleep Medicine) accred-ited sleep diagnostic company. USD provides comprehen-sive diagnostic sleep testing and treatment in our state-of-the-art sleep laboratories,
hospital environment. Our service is de-signed to ensure high quality, cost effec-tive sleep services to physicians and their patients. USD also serves as an advisory board member on The Joint Commission.
OUR HISTORY:USD is a direct descendant of Ambulatory Services Of Amer-ica, Inc. (ASA) which was the
channel Polysomnography (Sleep Studies) in the home and bedside CCU in the United States. ASA was founded in 1991 and grew to provide over 6,000 sleep studies per year in both patient homes and in 20 hospital based sleep labs. In 1999, ASA was sold to a publicly traded company.
a new company in South Florida and United Sleep Diagnostics, Inc. was born. Together with
Registered Polysomnographic Technologists and a professional administrative staff, USD has
Feat
ure
dS
leep
Lab
over 25 years experience in providing quality sleep diagnostics and treatment.
SERVICESAll tests performed for the diagnosis of sleep disorders are in accordance with
the parameters outlined in the American Academy of Sleep Medicine as well as Medicare guidelines. (Polysom-nography). A one night nocturnal poly-somnogram (NPSG) allows visually aided
period, by the accepted method of evaluat-ing the EEG, EOG and EMG. In addition,
nose and mouth is determined, respira-tory belts monitor abdominal and thoracic respiratory efforts, continuous non-inva-sive evaluation of arterial blood oxygen saturation, recording of electro-cardiogram (ECG) to diagnose intermittent rhythm abnormalities, recording of body position for nocturnal breathing abnormalities, recording of continuous leg movements and several other parameters. (MSLT). The accepted diagnosis tool for assess-ment of excessive daytime sleepiness
-lepsy. . A second nocturnal polysomnogram (NPSG) is
performed with the aid of Continuous Positive Air Pres-
presence of apnea.OUR FUTURE:
USD is poised to be-come the leading force in sleep in the South Florida Region. USD currently operates full service sleep centers as well as providing complete in-home Polysomnography and CPAP titration throughout the tri-county area. USD has been fortunate to be recognized as a quality provider and has won many managed care contracts as well as working with some
of the top physician groups in South Florida. USD looks forward to expand-ing our sleep centers, partnering with physician groups, hospitals, contracting with new managed care organizations and participating in research grants as well as improving the awareness and education of sleep disorders in the South Florida region. USD is well contracted with all the major carriers. United Sleep Diagnostics now runs 7 Hospital based facilities and 3 free-standing facilities. USD covers Dade, Broward, and Palm Beach Counties.
Director of Marketing and Business Development
United Sleep DiagnosticsComprehensive diagnostic sleep testing and treatment
DENTAL SLEEP MEDICINE24

WWW.SLEEPGS.COMWWW.DENTALSLEEPMAGAZINE.COM 25

DENTAL SLEEP MEDICINE24

WWW.SLEEPGS.COM 25
DENTAL SLEEP MEDICINEDENTAL SLEEP MEDICINE28

WWW.SLEEPGS.COM 29
INTRODUCTION - Obstructive sleep apnea (OSA) is a common condition characterized by partial closures
(hypopneas) and complete closures (apneas) of the airway while sleeping. These cause blood oxygen saturation levels to decrease markedly resulting in frequent arousals.
OSA is associated with an ever increasing list of both dangerous and inconvenient co-morbidities. A partial list of the clinical and social problems associated with OSA that are demonstrated by medical evidence and well accepted include obesity, vehicular accidents, hypertension, type 2 diabetes, stroke, cardiac complications such as CAD and CVD, recurrent
erectile dysfunction. Perhaps few medical professionals could envision how common OSA would become
described in a prominent medical journal in 1976. It is estimated in the United States that 9% of women and 24% of men between the ages of 30 and 60 have at least mild OSA. Awareness outside the area of sleep medicine has been very slow to develop despite the fact that OSA was described so long ago, evidenced by estimates that less than 25% of the patients with the condition have been diagnosed. The fact that OSA is closely linked to the growing problem of obesity means that the cases of OSA are likely to increase as well. Patients generally present with symptoms of daytime sleepiness, high blood pressure, reports of snoring with arousals, large neck circumference, sleep complaints, and problems with focus or concentration. Most people visit the dentist far more often than their primary care physicians, which puts the dentist in a unique position to empirically diagnose OSA
patients so suspicions can be objectively
dangerous co-morbidities associated with the condition.
DIAGNOSIS - The apnea-hypopnea index (AHI) is equal to the number of apneas and hypopneas per hour. The severity of
of >5 to 10 is termed mild OSA, > 10 to
15 is moderate, and > 15 is described as severe. Selection of appropriate diagnostic tests should consider the estimated pretest probability of the patient having OSA, availability of various diagnostic methods, and local skill to allow for test interpretation. Polysomnography is the universally accepted standard of care in diagnosing OSA. Home Sleep Testing (HST) has recently been approved as an option to qualify a patient for insurance coverage and may be performed
sleep medicine physician.
TREATMENT - Treatment options for OSA fall into three categories, namely surgical intervention, positive airway pressure and oral appliances. The American Academy of Sleep Medicine (AASM), after
a thorough review of the available published peer reviewed medical evidence, declared that oral appliances should be considered the
OSA. The AASM also states that oral appliances are indicated for patients who do not respond to CPAP, are not deemed good candidates for CPAP, or simply fail to use their CPAP. A recent meta-analysis found that oral appliances should not be used as
OSA patients with an AHI >15 or described as severe. Oral appliances are however an excellent alternative therapy for patients that can not tolerate the use of CPAP. The oral appliances lack
therapy but oral devices are sometimes the patient preference which may improve adherence to therapy and therefore improve health outcomes.
described in the medical literature in 1981 Continuous Positive Airway Pressure (CPAP) has been the cornerstone of treatment of patients suffering with obstructive sleep apnea. CPAP is the most effective
treatment for OSA and is the treatment of choice for severe obstructive sleep apnea. Therapeutic effectiveness of CPAP therapy is unfortunately plagued by the high non-compliance rate. CPAP compliance
70% of nights for at least 4 hours and this is the least amount of use it is believed
surgeon general C. Everett Koop MD once
take them!” and the same can be said for
in reversing sleep apnea and the attendant co-morbidities studies indicate between
By James P. Reichmann, MBA American Home Patient, Senior Vice President of Sales and Marketing
Obstructive Sleep Apnea and CPAPDME selection can influence long term therapeutic success.
Continued on Page 48
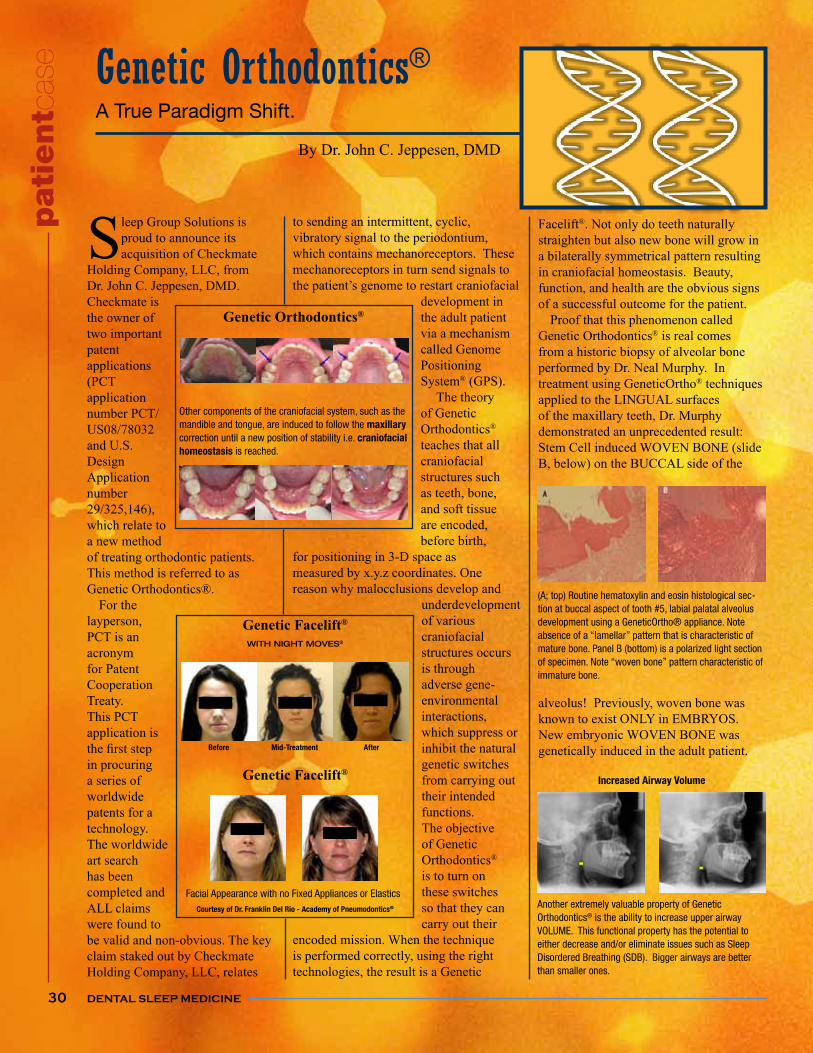
DENTAL SLEEP MEDICINE
Facelift®. Not only do teeth naturally straighten but also new bone will grow in a bilaterally symmetrical pattern resulting in craniofacial homeostasis. Beauty, function, and health are the obvious signs of a successful outcome for the patient. Proof that this phenomenon called Genetic Orthodontics® is real comes from a historic biopsy of alveolar bone performed by Dr. Neal Murphy. In treatment using GeneticOrtho® techniques applied to the LINGUAL surfaces of the maxillary teeth, Dr. Murphy demonstrated an unprecedented result: Stem Cell induced WOVEN BONE (slide B, below) on the BUCCAL side of the
alveolus! Previously, woven bone was known to exist ONLY in EMBRYOS. New embryonic WOVEN BONE was genetically induced in the adult patient.
30
Increased Airway Volume
Another extremely valuable property of Genetic Orthodontics® is the ability to increase upper airway VOLUME. This functional property has the potential to either decrease and/or eliminate issues such as Sleep Disordered Breathing (SDB). Bigger airways are better than smaller ones.
By Dr. John C. Jeppesen, DMD
Genetic Orthodontics®A True Paradigm Shift.
Sleep Group Solutions is proud to announce its acquisition of Checkmate
Holding Company, LLC, from Dr. John C. Jeppesen, DMD. Checkmate is the owner of two important patent applications (PCT application number PCT/US08/78032 and U.S. Design Application number 29/325,146), which relate to a new method of treating orthodontic patients. This method is referred to as Genetic Orthodontics®. For the layperson, PCT is an acronym for Patent Cooperation Treaty. This PCT application is
in procuring a series of worldwide patents for a technology. The worldwide art search has been completed and ALL claims were found to be valid and non-obvious. The key claim staked out by Checkmate Holding Company, LLC, relates
to sending an intermittent, cyclic, vibratory signal to the periodontium, which contains mechanoreceptors. These mechanoreceptors in turn send signals to
development in the adult patient via a mechanism called Genome Positioning System® (GPS). The theory of Genetic Orthodontics® teaches that all craniofacial structures such as teeth, bone, and soft tissue are encoded, before birth,
for positioning in 3-D space as measured by x.y.z coordinates. One reason why malocclusions develop and
underdevelopment of various craniofacial structures occurs is through adverse gene-environmental interactions, which suppress or inhibit the natural genetic switches from carrying out their intended functions. The objective of Genetic Orthodontics® is to turn on these switches so that they can carry out their
encoded mission. When the technique is performed correctly, using the right technologies, the result is a Genetic
pat
ientc
ase
Facial Appearance with no Fixed Appliances or ElasticsCourtesy of Dr. Franklin Del Rio - Academy of Pneumodontics®
®
WITH NIGHT MOVES®
Before
®
Mid-Treatment After
(A; top) Routine hematoxylin and eosin histological sec-tion at buccal aspect of tooth #5, labial palatal alveolus
absence of a “lamellar” pattern that is characteristic of mature bone. Panel B (bottom) is a polarized light section
immature bone.
®
Other components of the craniofacial system, such as the mandible and tongue, are induced to follow the maxillary correction until a new position of stability i.e. craniofacial homeostasis is reached.
DENTAL SLEEP MEDICINE
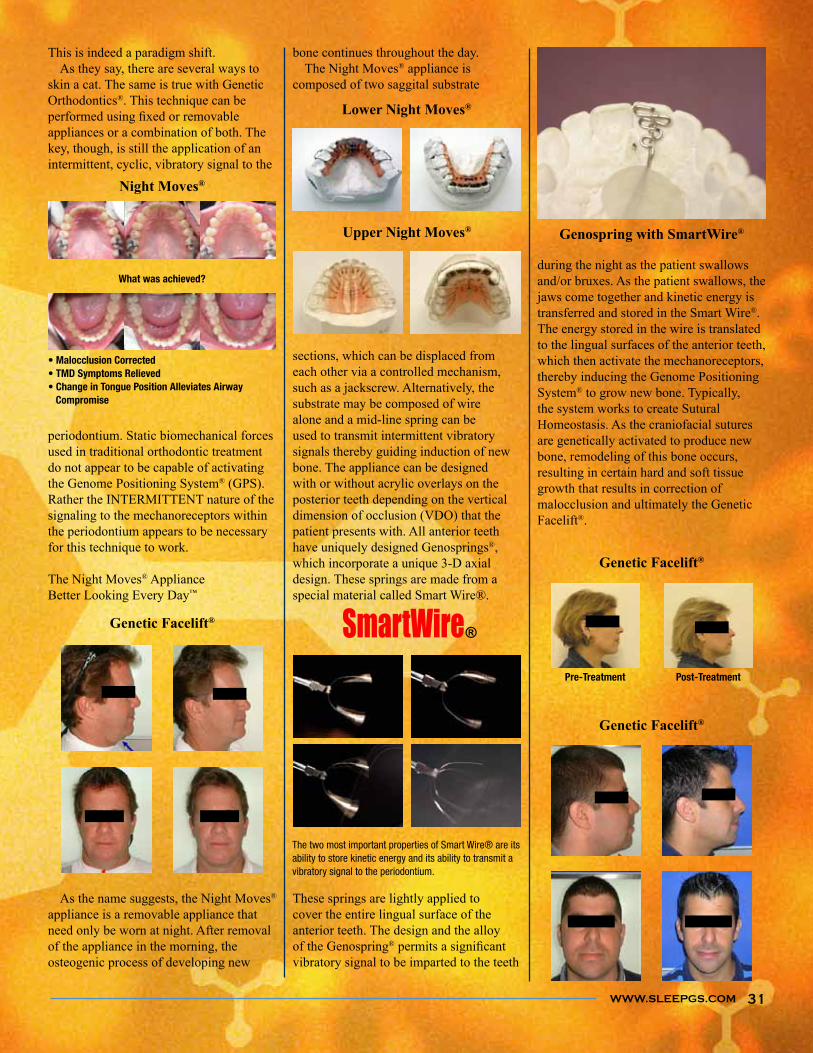
WWW.SLEEPGS.COM
during the night as the patient swallows and/or bruxes. As the patient swallows, the jaws come together and kinetic energy is transferred and stored in the Smart Wire®. The energy stored in the wire is translated to the lingual surfaces of the anterior teeth, which then activate the mechanoreceptors, thereby inducing the Genome Positioning System® to grow new bone. Typically, the system works to create Sutural Homeostasis. As the craniofacial sutures are genetically activated to produce new bone, remodeling of this bone occurs, resulting in certain hard and soft tissue growth that results in correction of malocclusion and ultimately the Genetic Facelift®.
bone continues throughout the day. The Night Moves® appliance is composed of two saggital substrate
sections, which can be displaced from each other via a controlled mechanism, such as a jackscrew. Alternatively, the substrate may be composed of wire alone and a mid-line spring can be used to transmit intermittent vibratory signals thereby guiding induction of new bone. The appliance can be designed with or without acrylic overlays on the posterior teeth depending on the vertical dimension of occlusion (VDO) that the patient presents with. All anterior teeth have uniquely designed Genosprings®, which incorporate a unique 3-D axial design. These springs are made from a special material called Smart Wire®.
These springs are lightly applied to cover the entire lingual surface of the anterior teeth. The design and the alloy of the Genospring®vibratory signal to be imparted to the teeth
This is indeed a paradigm shift. As they say, there are several ways to skin a cat. The same is true with Genetic Orthodontics®. This technique can be
appliances or a combination of both. The key, though, is still the application of an intermittent, cyclic, vibratory signal to the
periodontium. Static biomechanical forces used in traditional orthodontic treatment do not appear to be capable of activating the Genome Positioning System® (GPS). Rather the INTERMITTENT nature of the signaling to the mechanoreceptors within the periodontium appears to be necessary for this technique to work.
The Night Moves® ApplianceBetter Looking Every Day™
As the name suggests, the Night Moves® appliance is a removable appliance that need only be worn at night. After removal of the appliance in the morning, the osteogenic process of developing new
What was achieved?
®
Compromise
31
®
Pre-Treatment Post-Treatment
®
®
®
®
®
The two most important properties of Smart Wire® are its ability to store kinetic energy and its ability to transmit a vibratory signal to the periodontium.
WWW.SLEEPGS.COM

DENTAL SLEEP MEDICINE32
not best suited for oral appliance therapy and these individuals should be referred
rewarding to educate our patients on all of their treatment alternatives. As dentists we are used to educating our patients and my experience is that by spending the time to go over all treatment options (not just oral appliances) you build much closer relationships with these patients as well as immeasurably increase your credibility. Often times I will hear comments like “no one has ever taken the time to explain it that way” or “I didn’t know that there were other alternatives”even have the basic understanding of their disorder. Once the alternatives are discussed it may be apparent that an oral device is the appropriate treatment. This situation should never be looked at as negative. Conversely this can be a very positive opportunity to further build relationships with your sleep physicians and ENTs. Also remember there are many, many patients in your dental
practice that have undiagnosed obstructive sleep apnea. Once you have a good screening procedure these patients will need a diagnosis from a physician which is another prime opportunity to nurture your relationships by the appropriate referral. Working with a medical sleep team can be rewarding,
communication and perseverance. With proper training in sleep medicine and an ethical vision of optimal treatment for obstructive sleep apnea patients these
Gy Yatros, D.M.D.Island Dental Spa , Anna Maria Island, FloridaMember of ADSMMember of AGDMember of ADAEmail: [email protected]: www.islanddentalspa.com
As most dentists who are involved in
know, working with your local sleep physicians, ENTs, hospitals and other MDs
experience. If both the sleep dentist and the medical team have the same vision of successful treatment for all Obstructive Sleep Apnea (OSA) patients then a symbiotic relationship will naturally develop among the team members. The most effect will vary depending on the individual, so it is important to develop a protocol with your team members for the different indications for Oral Appliances, CPAP or surgery. Realize that this protocol will be continually dynamic and even possibly different depending on the origin of the patient referral. As you develop closer relationships with your local physicians they may become more educated on indications for oral appliances. Likewise by working with sleep MDs and ENTs you can gain a large amount of knowledge as to which patients are best treated by their particular modality of treatment. In my particular situation these
that two of our referring physician groups
proximity to their sleep facilities. To better serve one particular sleep group we were able to place a dental sleep facility in the sleep lab itself. This has been a wonderful arrangement because I have been able to spend time with my physician team and we can communicate
and treatment goals. The second facility is adjacent to a major hospital with a large educational sleep program. I am presently on the volunteer staff for the university and helping educate the Sleep Fellowship physicians with their training. Similar to location in real estate, the
key to developing these relationships is communication, communication, communication. It is best to take every opportunity that becomes available to communicate with your physicians. From the initial contact to the request for an orthotic PSG, these are all important opportunities
to communicate either by letters, phone or in person. In particular I believe it is of critical importance to contact any physician that you have not worked with in the past if you are going to see a mutual patient. I will usually begin with a phone conversation explaining why I am
seeing their patient and how I believe I may or may not be able to help them. It is then advisable to ask the physician what their treatment goals for the patient might be and to assure them that you will keep them
progress. I usually follow this up with an invitation
meet with them personally to go over the treatment success once our treatment has completed. Keep in mind it is important to be well educated before you begin this process. Once the communication has begun with the physician it is important to never quit. As a dentist I have known specialists that were “gung ho”after a while the communication waned. Resultantly so did my referrals to them. It is important to keep the communicating constant with letters, phone calls, and personal visits either personally or by a member of the dental team. Through constant interaction the physician referral stream will
Lastly it is important to realize that this is a two way street. All patients are
Developing A Sleep Physician TeamWorking with a medical sleep team can be rewarding, educational and profitable. The Key is . . .
By Gy Yatros, DMD

WWW.SLEEPGS.COM 33
Working With The TAP 3 Mandibular Advancement Devices
By Dan Tache DDS, D,ABDSM
Obstructive Sleep Apnea Syndrome (OSAS) is a disorder with high prevalence and it is associated
with substantial morbidity and increased
Gold Standard for the management of OSAS is continuous positive airway
long-term compliance with CPAP therapy has been estimated at between 25-50% of patients.1 Oral appliances (OA) have been shown to be effective in a subset of patients with OSAS who are CPAP-intolerant.2 Typically, these patients who are responsive to OA therapy have mild-moderate supine-dependent sleep apneas OSAS.1, 3
have shown OAs to have a relatively robust compliance rate ranging between 64.1% and 93.7%.4,5 Often, in the course of titration of any of the adjustable MADs, additional advancement is required but the advancement mechanism has been completely advanced. This may be the result NOT of MAD design weakness
the mandible at the time of fabrication of the appliance when cranio-mandibular records are taken. Certainly, this problem is also encountered when patients of record return for their annual OSA recall visit, particularly if there has been weight gain or the patient has begun to take opioid medication at bedtime. This frequently encountered challenge highlights the need for continued vigilance with the OSAS patient not to mention the fact that annual recall of these patients is a requirement of the Practice Parameters for the Treatment of Snoring
and Obstructive Sleep Apnea with Oral
Appliances 2005.2
Effectiveness of MADs requires
order to adequately stabilize the airway.
80% of maximum protrusive range. This may require protrusion ranging between 6 and 8 mm 6 which exceeds the adjustability of most MADs. Many clinicians out of fear of inducing symptoms will elect a more conservative starting point, usually “end to end” only to discover that the device is fully advanced before the airway has been
When a clinician is confronted with this dilemma and has to return the MAD to the lab for alteration, it can mean a considerable problem for the patient was well. Often, the OSA patient has relinquished his or her PAP device and is dependent upon the MAD for controlThe TAP 3 is an excellent device because of its simplicity of design and heartiness of articulating advancement mechanism. It was designed by Dr. Keith Thornton (http://www.airwaylabs.com/) whose intent was to make the process as user and clinician-friendly as possible which would imply
the need for returning the device to the laboratory.
method of moving the advancement mechanism of the TAP 3 MAD when this problem is encountered. I will use a recently treated OSA patient to illustrate the technique.
Alteration of the Advancement Mechanism When You Have More Titration to Accomplish.
This is TV, a 43 y.o. male who was diagnosed with severe obstructive sleep apnea in 1996.
CC: “I am soon to be deployed to Iraq and I used a CPAP but there will not be any electricity where I to be stationed”
PMH: Past history of elevated blood pressure which had been managed with medication Elevated BP has been more recently controlled with management of his OSAS using CPAPDiagnosed in 1998 with obstructive sleep apneaNot currently under the care of a physician for medical problems
HPI: Has been very successfully using CPAP since 1996Most recently, he learned that he was to be deployed to IraqHe is concerned that he may not have access to electricity to run his
CPAP
TV was provided with a TAP3 and we began the titration processThe process had to be accelerated because we had only two weeks to accomplish optimization of the efficacy of his applianceGiven that he had a severe level of disease, advancement was near maximum
Continued on Page 32
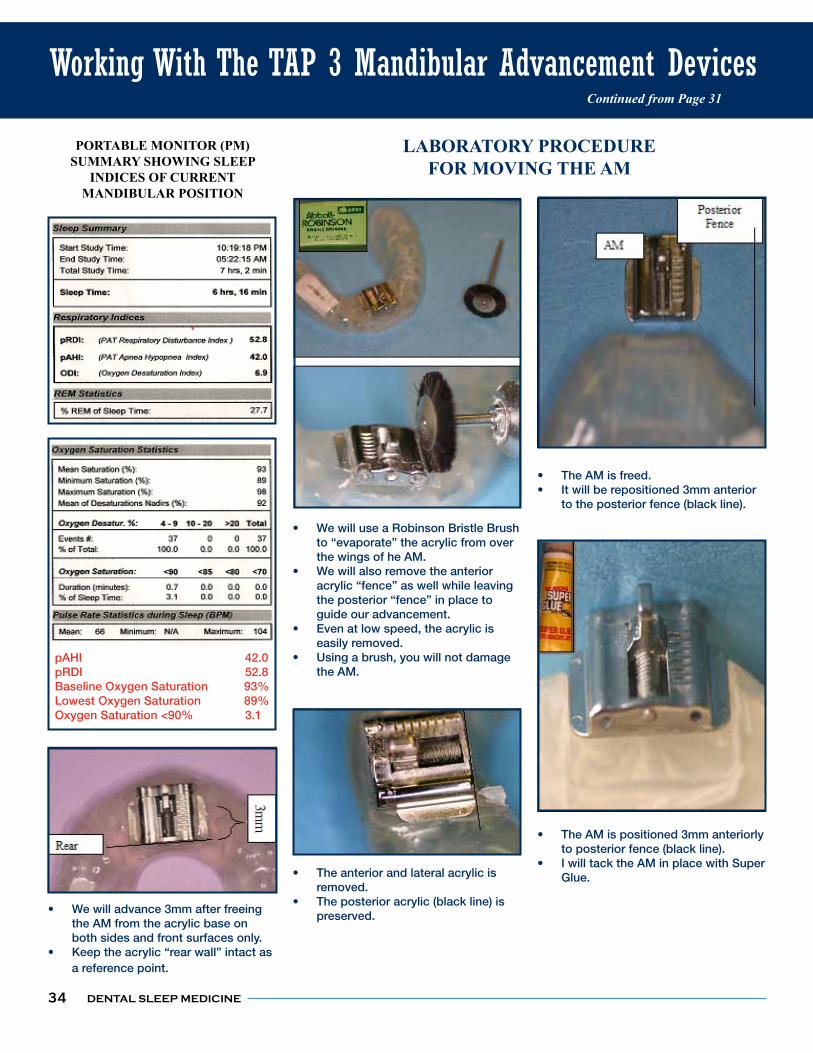
DENTAL SLEEP MEDICINE
LABORATORY PROCEDURE FOR MOVING THE AM
We will use a Robinson Bristle Brush to “evaporate” the acrylic from over the wings of he AM.We will also remove the anterior acrylic “fence” as well while leaving the posterior “fence” in place to guide our advancement.Even at low speed, the acrylic is easily removed.Using a brush, you will not damage the AM.
The anterior and lateral acrylic is removed.The posterior acrylic (black line) is preserved.
The AM is freed.It will be repositioned 3mm anterior to the posterior fence (black line).
The AM is positioned 3mm anteriorly to posterior fence (black line).I will tack the AM in place with Super Glue.
34
PORTABLE MONITOR (PM)
INDICES OF CURRENT MANDIBULAR POSITION
Working With The TAP 3 Mandibular Advancement DevicesContinued from Page 31
pAHI 42.0pRDI 52.8Baseline Oxygen Saturation 93%Lowest Oxygen Saturation 89%Oxygen Saturation <90% 3.1
LABORATORY PROCEDURE FOR MOVING THE AM
We will advance 3mm after freeing the AM from the acrylic base on both sides and front surfaces only.Keep the acrylic “rear wall” intact as a reference point.
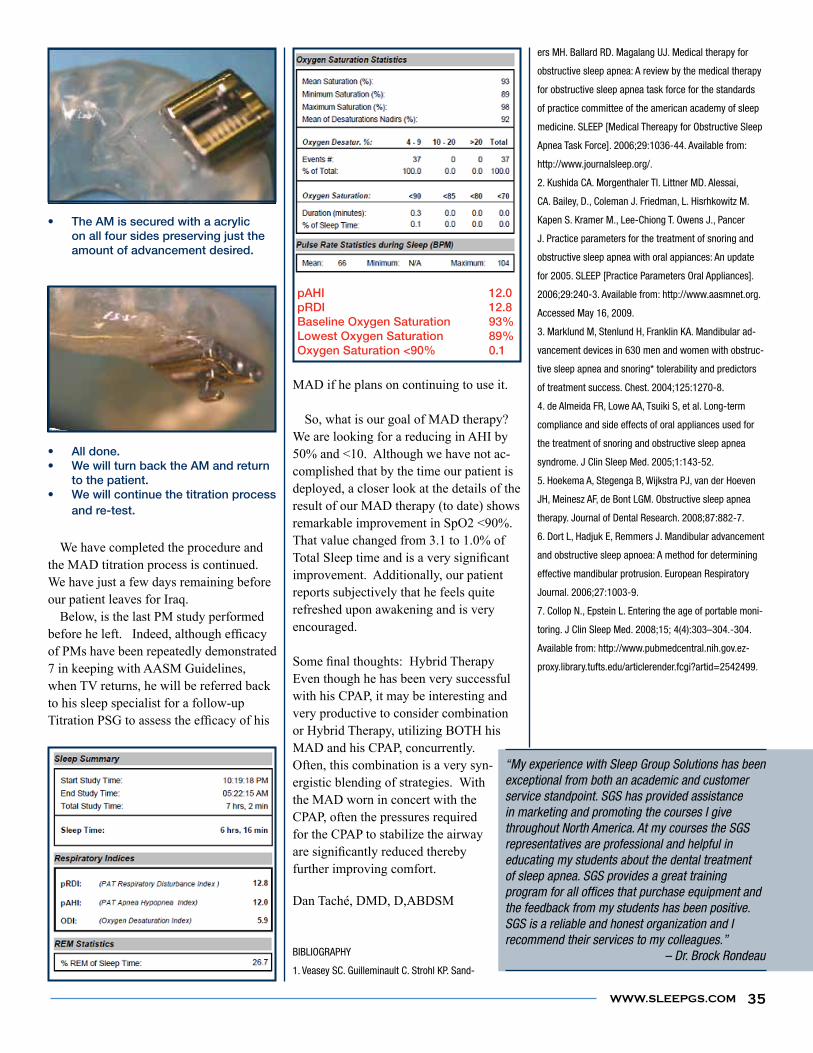
WWW.SLEEPGS.COM
MAD if he plans on continuing to use it. So, what is our goal of MAD therapy? We are looking for a reducing in AHI by 50% and <10. Although we have not ac-complished that by the time our patient is deployed, a closer look at the details of the result of our MAD therapy (to date) shows remarkable improvement in SpO2 <90%. That value changed from 3.1 to 1.0% of
improvement. Additionally, our patient reports subjectively that he feels quite refreshed upon awakening and is very encouraged.
Even though he has been very successful with his CPAP, it may be interesting and very productive to consider combination or Hybrid Therapy, utilizing BOTH his MAD and his CPAP, concurrently. Often, this combination is a very syn-ergistic blending of strategies. With the MAD worn in concert with the CPAP, often the pressures required for the CPAP to stabilize the airway
further improving comfort.
Dan Taché, DMD, D,ABDSM
BIBLIOGRAPHY
1. Veasey SC. Guilleminault C. Strohl KP. Sand-
The AM is secured with a acrylic on all four sides preserving just the amount of advancement desired.
All done.We will turn back the AM and return to the patient.We will continue the titration process and re-test.
35
We have completed the procedure and the MAD titration process is continued.We have just a few days remaining before our patient leaves for Iraq. Below, is the last PM study performed
of PMs have been repeatedly demonstrated 7 in keeping with AASM Guidelines, when TV returns, he will be referred back to his sleep specialist for a follow-up
pAHI 12.0pRDI 12.8Baseline Oxygen Saturation 93%Lowest Oxygen Saturation 89%Oxygen Saturation <90% 0.1
ers MH. Ballard RD. Magalang UJ. Medical therapy for
obstructive sleep apnea: A review by the medical therapy
for obstructive sleep apnea task force for the standards
of practice committee of the american academy of sleep
medicine. SLEEP [Medical Thereapy for Obstructive Sleep
http://www.journalsleep.org/.
2. Kushida CA. Morgenthaler TI. Littner MD. Alessai,
CA. Bailey, D., Coleman J. Friedman, L. Hisrhkowitz M.
Kapen S. Kramer M., Lee-Chiong T. Owens J., Pancer
J. Practice parameters for the treatment of snoring and
obstructive sleep apnea with oral appiances: An update
for 2005. SLEEP [Practice Parameters Oral Appliances].
3. Marklund M, Stenlund H, Franklin KA. Mandibular ad-
vancement devices in 630 men and women with obstruc-
tive sleep apnea and snoring* tolerability and predictors
compliance and side effects of oral appliances used for
the treatment of snoring and obstructive sleep apnea
5. Hoekema A, Stegenga B, Wijkstra PJ, van der Hoeven
JH, Meinesz AF, de Bont LGM. Obstructive sleep apnea
therapy. Journal of Dental Research. 2008;87:882-7.
6. Dort L, Hadjuk E, Remmers J. Mandibular advancement
and obstructive sleep apnoea: A method for determining
effective mandibular protrusion. European Respiratory
-
Available from: http://www.pubmedcentral.nih.gov.ez-
exceptional from both an academic and customer service standpoint. SGS has provided assistance in marketing and promoting the courses I give
representatives are professional and helpful in educating my students about the dental treatment of sleep apnea. SGS provides a great training program for all offices that purchase equipment and the feedback from my students has been positive. SGS is a reliable and honest organization and I recommend their services to my colleagues.” – Dr. Brock Rondeau

DENTAL SLEEP MEDICINE36
Mr. Jones described the past two weeks of his life as having amazing energy, sudden
optimism, a rediscovery of his family, severe head pain gone, and no snoring! Sleep Apnea patient? Not according to his chief complaint, diagnosis and treatment. Yes, only by coincidence. His chief complaint on arrival were his years of constant headaches and many doctors and many but minimally effective strong drugs. He was describing how his lower orthotic freed him of the pain and fog and gave him his family and life back! His snoring comment was interesting, but not
bonus”. No surprise to me was the changes the orthotic had brought into his life, but
1979. The emergence and explosive growth of Obstructive Sleep Apnea (OSA) shares a commonality with dental implants. It started with a few, was not user friendly, had high failure rates and was controversial. There were pioneer gurus, competing systems, mailers assuring the practitioners that a weekend course would make them instant experts. Many of those “week-end warriors” learned through failures and patient disappointment that a little knowledge could be “dangerous”. The ultimate good emerged as many dentists dropped out or got comprehensive training. It started slowly in isolated cells but it soon inspired research, professional and public education and private sector
development until today implants are an
Obstructive Sleep Apnea (OSA) go
DIFFERENT is the OSA Dental evolution is increasingly interfacing Medicine with Dentistry in profound ways
all those involved. My exclusive dental sleep medicine practice started “from scratch” 15+ years ago following 27 wonderful years of general practice. I quickly discovered there were comparatively few guidelines or literature and many diverse opinions. The sleep medicine community was somewhat skeptical and early generation devices shared some common design features that limited their success. I could not
diagnosis, prognosis and treatment that educated the patient from the start through their treatment. I was both humbled and inspired by how a simple oral device could
profoundly improve the lifestyles of the patient and their family. There is no
much can be measured has limitations
and why “professional opinions” and “judgment” span those gaps. The more measuring and experience, the shorter the gap. My outcomes have always been better when I could apply my tools with
as much tape measure involvement as possible and OSA treatment outcomes are no different. It is simply a different metric application. I have developed a
system over some seven years that has had
Its evolution was mostly frustration-
reapplied, etc. It provides a repeatable metric for airway measurement, jaw positioning and recording for start and a target position for optimum airway. It is simple, fast, packaged for quick access and storage, and color-coded for cold
easy for staff to learn and the enhanced patient education almost creates their desire for treatment from the start. It is universally applicable for any device and works with or without Pharyngometry. It can accelerate learning for the beginner and simplify the protocol for the
It is Airway Metrics. The photos are only a sneak preview and speak for themselves. Robert L. Horchover, D.D.S. AIRWAYMETRICS.COM
By Dr. Robert L. Horchover, DDS
OSA Dental evolution is increasingly interfacing medicine with dentistry.
The Emergence And Explosive Growth Of OSA
Pharyngometer Interface.
“I was both humbled and inspired by how a simple oral device could profoundly improve the lifestyles of the patient and their family.”

WWW.SLEEPGS.COM 37
Acoustic Pharyngometry By Jeffrey J. Fredberg, Professor, Harvard School of Public Health
applian
cere
view
Acoustic Pharyngometry has become widely employed to help in the diagnosis and treatment of
obstructive sleep apnea, and to investigate the pathophysiology of the upper airway. But in the beginning, when this technology was
issues were not at all on our radar screen. Instead, in 1973 when
this idea, the goal was to develop an acoustic technology that could be used to probe lung function in infants and young children, the idea being that we needed a lung function test that could be used in the uncooperative subject. We were fortunate to be able to secure generous funding from the NIH, and over the next decade the technology was developed and matured.
At that time the upper airway was simply an obstacle that needed to be traversed in order to probe the deeper
structures of interest, which included larynx, trachea, bronchi, and small airways. But as the technology improved, and as the test became simpler to accomplish, we began to appreciate that the upper airway was not an obstacle,
but rather an important structure in its own right, and one deserving of greater scrutiny. Acoustic Pharyngometry was born. Today Acoustic Pharyngometry is used in children as well as adults to study the size, structure, and collapsibility of the upper airway. It is used as well to titrate mandibular advancement devices for
The Airway Metrics System allows you to quickly determine optimum airway positions
Snore Screener
Manibular PositioningSimulator
the treatment of obstructive sleep apnea, and it is used to study the effect of weight reduction on upper airway patency. The test is fast and noninvasive, it is inexpensive and uses no ionizing radiation.
conveniently in any examination room.
sleep practice. I use it in my consultation appointment, and in variably when they see on the screen what my appliance can potentially do they accept treatment. Then when I start treatment, it helps guide me as far as adjustments. Great for diagnosis, case presentation, and

DENTAL SLEEP MEDICINEDENTAL SLEEP MEDICINE38
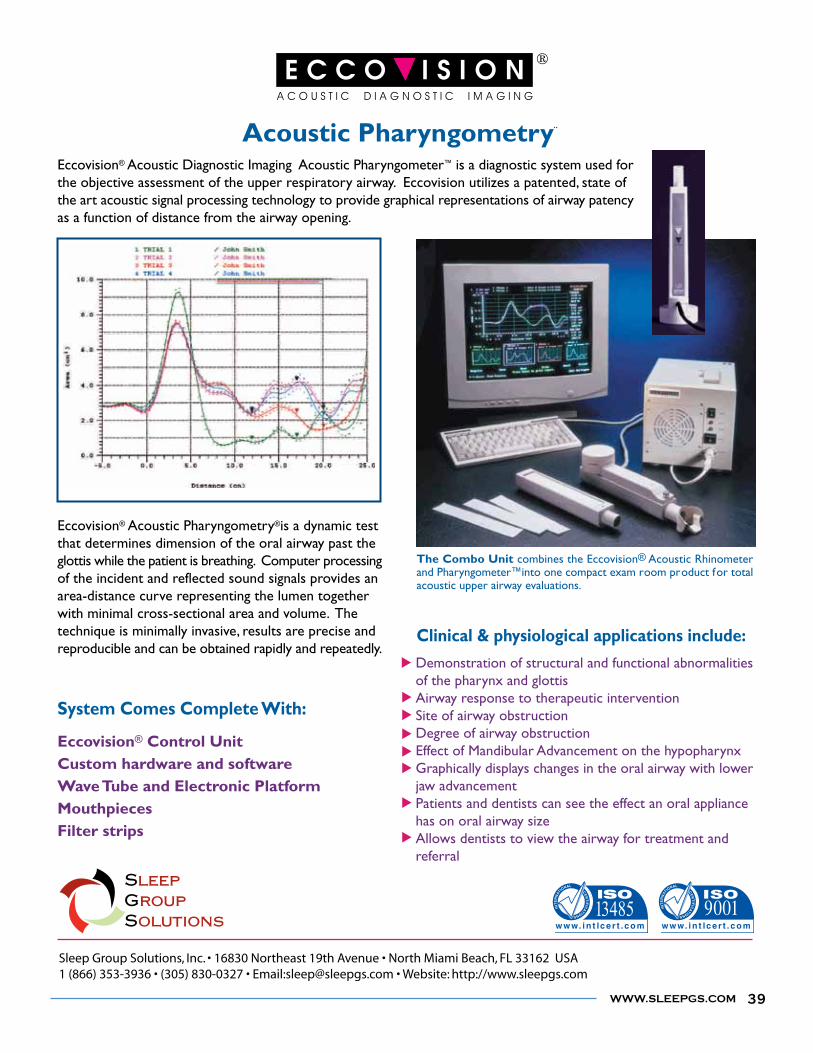
WWW.SLEEPGS.COM 39

DENTAL SLEEP MEDICINE40

WWW.SLEEPGS.COM
IDEAL FOR USE AS A TEMPORARY APPLIANCE
immediately without waiting for lab fabrication. This makes it an ideal temporary appliance to use when patients
need to undergo dental work or if they've lost or damaged their existing appliance. The strong fabrication of the
NORAD will last your patients for months, which makes this appliance the most versatile temporary appliance on
the market.
SLEEP GROUP SOLUTIONS PRESENTS
CHAIR SIDE
FABRICATION
AS EASY AS
1-2-3!
THE NORADBOIL AND BITE APPLIANCE
5MM 7MM
41
applian
cere
view
DENTAL SLEEP MEDICINE42
Sleeping Down Under
by Dr. Lisa Matriste, BDSc Hons (Uni of Queensland), AACNEM
Inspite of its relatively small population (22 million), Australia boasts its fair share of iconic legends in dramatic
quite impressive including actors Hugh Jackman, Russell Crowe and Nicole Kidman. The Aussie rockband AC DC endures equally with the “Grease” starlet Olivia Newton John. Greg Norman still
form and Geoff Ogilvy is currently ranked #4 on the PGA circuit. Our tennis stars include Rod Laver who won the Grand Slam and more recent winners of the US Open have been Pat Rafter and Lleyton Hewitt. Last year the Aussie Olympic Swimming Dream Team managed to steal some records from Michael Phelps. Lauren Jackson who plays for the Seattle Storms has been described as one of the greatest basketballers of all times. In the business world, Frank Lowry who immigrated to Melbourne, Australia, comes in at #174 by Forbes Richest Billionaire list for having founded the
the owner of the most shopping centres in the world. He was instrumental in the rebuilding of the World Trade Centre after 9/11. Of course #109 ranked Forbes Billionaire, Rupert Murdoch, deserves a mention. The Australian born media
of USA newspapers and television.
CNN. There have been many Australians who have been awarded the prestigious Nobel Prize for their contribution to major
one of the leading Nobel Prize winning
Some examples are Howard Walter Florey who is often overlooked for his collaborative role with Alexander Fleming in the discovery of Penicillin and its curative effect of many infectious diseases (Nobel Prize for Medicine 1945)
Barry Marshall and Robin Warren (Nobel Prize for Medicine 2005) who used antibiotics to cure infections of Helicobacter Pylori causing gastric and duodenal ulcers. This discovery has led to
gastric cancer especially in Japan. So, it is with much pride that I draw to your attention to the Aussie Legends in Sleep Medicine. The obvious BIG 4 being Colin Sullivan who invented the CPAP machine and continues a teaching and research career at the University of Sydney. Dr Murray Johns is another pioneer who developed the Epworth Sleepiness Scale in 1990 which is now a
general level of sleepiness in daily life. He was also involved in the development
of diagnostic sleep equipment with Compumedics. For more than 30 years, Dr Johns remains a
sleep medicine, now focusing on
that for an oxymoron?) Prof Peter Cistulli who is based
at the University of Sydney, received the Pierre Robin Award from the AADSM in 2006. Whilst being a Respiratory and Sleep Physician, his research has focused on the orofacial aspects of OSA pathophysiology and
The Aussie legends of sleep medicine!
WWW.SLEEPGS.COM 43
evaluating oral appliances for reducing the symptoms of OSA. More recently he is investigating the effectiveness of orthodontic rapid maxillary expansion for the treatment of obstructive sleep apnoea syndrome. Prof Cistulli remains a champion of dental sleep medicine as his research validates that oral appliances are indeed a valid therapeutic option to CPAP especially for mild and moderate OSA sufferers.
appliances, SomnoDent was designed by an Australian orthodontist, Dr Richard Palmisano. SomnoMed was formed in 2004 to commercialize the mandibular advancement splint and within 5 years has established global marketing and distribution channels for its patented, pretty pink device.
for dentists incorporating dental sleep medicine into their clinical practices. Australian memberships in representative organizations are increasing each year. For example there are now 62 dentists registered with the Australian Sleep Association and of these 17 have joined the AADSM. Unfortunately, the learning
is not very structured and is only regulated in one State which obliges dentists who wish to use oral appliances for their patients, to follow the Guidelines of the AADSM. It remains to be seen whether this policy of the Dental Board of Victoria will be abandoned or introduced nationally when the National Professional Register is formed. All the current Regulatory Health State Boards will be merged into one administrative entity under the Health Insurance Commission. Furthermore, there is no recognized specialty of Dental/Oral Sleep Medicine even if one was to complete the 2-3 year Masters programme of Science of Sleep Medicine offered at the University of Sydney under Prof Colin Sullivan. There have been some visits from our learned American colleagues, Drs Ed Spiegal, Jamieson Spencer and Steve Olmos to teach Aussie dentists about Dental Sleep Medicine. The soon-to-be released internet courses of Dr. Brock Rondeau will provide another educational option on this subject. On the home front, lecturers Dr. Derek Mahoney (Orthodontist) and Dr. Harry Ball have
also conducted courses on Snoring and OSA. Dentists in Australia have quite a range of MAS appliances to utilize with the most popular options being: SomnoDent, Silent Nite, Silencer, Tap II/III, Oasys, EMA and the only registered Australian designed appliance – MDSA. Last year saw the inaugural Australian “Oral Sleep Medicine” course in Adelaide. This initiative is a collaboration of the University of Adelaide Dental School, the Australian Sleep Association and the Australian Dental Association. These organizations have made an annual commitment to provide continuous, non-commercial educational courses for dentists providing both introductory
venue for the “Visions of the Night” Sleep Conference is in Melbourne (October 8-10). It will be springtime downunder where the air is warm and the US dollar is worth a fortune! So make the trip, book QANTAS. Remember to pack the Melatonin. Come and sleep under the Southern Cross (our famous stellar constellation) and wake up refreshed.
PERSONAL & PROFESSIONAL INSIGHTS
Submitting to family pressures, Lisa reluctantly commenced her dental studies at the University of Queensland, Brisbane, Australia in 1982. Graduating with Honours in Bachelor of Dental Science in 1986, Lisa travelled to North Queensland
with the Queensland Government Department of Health completing two years in the School Dental Service. Enjoying coastal living, Lisa then moved
dental practice at the tender age of 25years. She has always worked full-time in spite of her raising three children with the last twelve years being as a sole parent.
ago and has been developing her new dental company which is evolving into a HOLISTIC WELLNESS CENTRE, incorporating dentistry, beauty and laser clinics and a detox spa. There coexists a vision to develop a teaching institute and Foundation. Motivated by the premature deaths of
her parents - her mother dying of cancer and her father suffering a fatal heart attack, Lisa has focussed her career on integrating dental medicine into the day-to-day care of her patients. She describes her practice as being holistic or integrative as well as environmentally responsible. Lisa continually is developing clinical protocols where she as a dentist can offer
bill” methods. Lisa embraces the technological advances in dentistry such as lasers, ozone, photodynamic therapy,
for neuromuscular/TMJ analysis, digital radiography and computer networks plus screens all dental materials to ensure only biocompatible products are used thus making DENTIQUE a mercury and
North America several times a year where she updates her knowledge and skills in toxicology, nutrition and environmental medicine, craniofacial pain, dentofacial orthopaedics, orthodontics and sleep medicine. Having survived twenty plus years in the profession, Lisa genuinely confesses that “Mother did know best” and is more enthusiastic about her career now than she ever was, because Dentistry is the medium by which she heals people and can transform their lives.
MEMBERSHIPS
TOXICOLOGY
TOXICOLOGY

DENTAL SLEEP MEDICINE44
Internet-Based Dental EducationA vast array of global experts showcasing their collective acumen making this type of specific dental information available in a timely manner.
Dental knowledge today, as with most everything, is no longer expanding along a linear curve -
but rather exponentially. Innovative new products, as well as constantly evolving
face to face in a more timely manner.
clinician scans a plethora of Journals and advertising driven dental tabloids, attends ongoing study clubs, academy, and institute meetings (many sponsored by dental companies), and then all too often comes away with new ideas, concepts, and philosophies but little real education on the actual “how to” of any technique or the intricacies in the use of new products. As traditional dental education, even rapid-turn-around print media, struggles to meet this demand, dental education is forced to meet this challenge by combining traditional learning methods with new internet-based technologies. While conventional print media and meetings remain effective at apprizing them of a concept, an internet based site with streaming video would allow a dentist, who may have learned of a new process, to review it in depth on their computer in their own time or literally before doing a particular procedure. New products and technologies have become exceedingly
by Dr. Maurice Salama
technique sensitive. Information on these products and technologies, whether it is the sequences and timing of dentin bonding, subtleties of a suturing technique system or the nuances of a innovative grafting process, can all be similarly available to a clinician anywhere in the world, at any time, on an internet-based teaching site. Developing internet based educational sites are all too often industry sponsored but, sites such as DentalXP available at www.dentalxp.com bring together a vast array of global experts showcasing their collective acumen and
information available in a timely manner. As a multi-disciplinary, cross-disciplinary
non-corporate based site, it is a veritable resource for both new and old information
technology is evident in being able to
easily. The format is similarly particularly
versatile ranging from presentations, using digital images similar to PowerPoint or Keynote, animations to elucidate on the
video to show a sequential aspect of literally any process. Combine all this with downloadable
detailed instructions and information on associated instrumentation or products, and DentalXP becomes a one stop readily available site for any procedure technique, technology, or product. Today DentalXP is becoming an essential supportive adjunct to peer reviewed journals of unbiased educational material. Today, DentalXP has over 16,000 members in over 160 countries
around the world and growing rapidly. The heightened interest from these registrants have led DentalXP.com to initiate Hands-On-Training (HOT) programs beginning this year. Combining on-line dental education with HOT modules is the future of dental education.
WWW.SLEEPGS.COM 45
Biography
Maurice Albert Salama, DMD
Dr. Maurice A. Salama completed his undergraduate studies at the State University of New York at Binghamton in 1985, where he received his B.S. in Biology. Dr. Salama received his D.M.D. from the University of Pennsylvania School of Dental Medicine where he later also received his dual-specialty certification in Orthodontics and Periodontics, as well as implant training at the Brånemark Center at Penn. He is currently on the Faculty of the University of Pennsylvania and the Medical College of Georgia as Clinical Assistant Professor of Periodontics, and is visiting Professor of Periodontics at Nova Southeastern University in Florida.
Dr. Salama has completed an ADA accredited hospital based General Practice Residency at Maimonides Medical Center in New York City. He has had the opportunity to further
broaden his clinical horizons through externships at Hadassah Hospital, Hebrew University in Jerusalem and Beth Israel Hospital in New York City, in 1988 and has been a contributor to the dental literature. His very unique background includes specialized training in Orthodontics, Periodontal Surgery, and Implant Dentistry.
Dr. Salama is a partner in the Atlanta Esthetic Dental Practice known as “Team Atlanta”. His partners include Dr. David Garber, Dr. Ronald Goldstein and his brother, Dr. Henry Salama. This group has an international reputation for interdisciplinary care, dental education and has published hundreds of articles and several text books.
Dr. Salama is a featured Xpert content provider and member of the Scientific Committee of the leading web-based dental education site www.DentalXP.com.
Dr. Salama served as the Dental
Expert for Channel 5 Fox TV in Atlanta. He is an active member in the American Association of Orthodontists, the American Academy of Periodontics, the Academy of Osseointegration, the American Academy of Esthetic Dentistry, and the American Academy of Implant Dentistry. Recently, Dr. Salama has been a speaker at programs for the Academy of Osseointegration, the American Association of Orthodontists, the American Academy of Periodontology, the American Academy of Esthetic Dentistry, the Interdisciplinary Care Conference presented by five Academies, the American Academy of Cosmetic Dentistry, Alpha Omega International, and the Chicago Dental Society.
In private practice at: Goldstein, Garber, & Salama, LLC600 Galleria Parkway, suite 800Atlanta, GA 30339www.goldsteingarber.com
WWW.SLEEPGS.COM

DENTAL SLEEP MEDICINE46
We all know that boil and bite appliances currently on the market are great
for certain patients, but we also know that they can sometimes be frustrating to use. A little over a year ago I set out to develop a new type of non-custom appliance. After months of development, prototypes, and trials, I developed what I believe to be an excellent non-custom oral appliance. I have named it the “Silent Sleep.”
In creating the Silent Sleep I tried to develop a pre-fabricated, customizable appliance that:
vinyl polysiloxane denture reline material (GC Soft Reline). This makes the appliance much easier
appliances. In addition, unlike boil and bite appliances, the Silent
many times as needed. The Silent
Sleep is also unique in that it uses only the posterior teeth for support and retention. As such, the appliance allows for excellent
bulky than other non-custom appliances. The Silent Sleep is easy to use, inexpensive, comfortable and effective. Whether you have been treating patients with sleep disordered breathing for years, or you are just getting started, the Silent Sleep will allow you
increase the number of patients that you are able to help. The Silent Sleep is not intended to be a replacement for custom appliances, but rather another tool to help you in the treatment of patients with snoring and sleep apnea. I believe that the Silent Sleep will become an invaluable addition to your armamentarium of custom appliances, CPAP/oral appliance combination appliances, and other treatments that you are providing to your
sleep disordered breathing patients. It is my hope that use of the Silent Sleep
patients that you are able to help in your
as you improve the health of your patients, improve the
of your practice as well. For further information, please contact me directly via email at [email protected], or contact McMullin Labs at 1-888-872-8538 for sales inquiries. We
stages of FDA approval and will soon offer the Silent Sleep to U.S. dentists. To ensure that you are among
to offer the Silent Sleep, please contact
McMullin Labs to place an order today.
Jamison R. Spencer, DMD, MSDiplomate, American Academy of Craniofacial PainDiplomate, American Academy of Dental Sleep Medicine
Introducing The Silent Sleep Trial Oral Appliance For Snoring And Sleep Apnea
By Dr. Jamison R. Spencer, DMD, MS
An invaluable addition to appliances and treatment for sleep disordered patients.
custom made appliance is fabricated.
uncertain about oral appliance therapy.
lab for patients who are found during the CPAP titration to be CPAP intolerant.
made appliances when treating patients who have been diagnosed by their physician as “primary snorers” and have no insurance coverage, or otherwise have limited financial resources.
protective appliance in veneer cases.
undergoing orthodontic therapy.
Possible uses for: THE SILENT SLEEP
applian
cere
view

WWW.SLEEPGS.COM 47
save his life with appropriate treatment! Justin is this 18 year old patient
230 pounds and his neck measured 20 inches. Clinically, I have found that any male with a neck circumference greater than 17 inches is susceptible to OSA. I recommend that these patients be scheduled for a consultation appointment with your dental assistant who is knowledgeable in sleep disorder dentistry. You must train someone on your staff to educate these patients regarding the serious health consequences of failure to treat OSA. Our protocol is as follows:
1. TMJ Health Questionnaire2. Epworth Sleepiness Scale3. Rhinometer to check for nasal obstructions
pharyngeal airway when the patient exhales.5. Sample Oral Appliances
The patient is shown samples of two possible oral appliances that are titratable antero-posteriorly as well as vertically. Do not confuse the patient by showing them too many oral appliances. The sleep assistant will educate the patient as to the importance of diagnosing and treating these problems. This appointment lasts approximately thirty minutes, and then I arrive and meet the
the data collected by the assistant and explained it to him:
1. TMJ Health QuestionnaireThis form revealed that he snored at night but he never had a sleep study done at a sleep clinic (hospital), and he was never diagnosed with sleep apnea. 2. Epworth Sleepiness ScaleTotal 15This indicates a serious problem with daytime sleepiness which is one of the main symptoms of OSA.
3. Rhinometer TestThis revealed that there were no nasal obstructions.
4. Pharyngometer TestThis revealed that his airway collapsed to .76 cm2
when he exhaled (normal airway is 2.0 cm2).
Based on his Epworth Sleepiness Scale of 15, the collapsed airway and severe snoring problem, I recommended an appointment for a complete set of records including an evaluation of his nasal, oral and pharyngeal airway. The records appointment involves the following:
1. Sleep Screening QuestionnaireThis form will identify all the problem areas with a history of the signs of OSA including frequent heavy snoring which affects the sleep of others. The patient had been told that he stops breathing when sleeping, gasps for air when waking up and had nighttime choking spells. These forms may be obtained from
These forms further revealed that Justin had a history of asthma, chronic sinus problem, heartburn or sour taste in his mouth at night, insomnia, nighttime sweating, memory loss, and inability to concentrate. This Sleep Screening Questionnaire also revealed that his father had been treated for a sleep disorder and had a history of heart disease, high blood pressure and diabetes. Obviously, Justin who has a BMI of 36 (normal male BMI is 30) is predisposed to cardiovascular disease, type 2 diabetes and already has gastroesphageal reflux (GERD).
2. Pharyngometer TestThe sleep assistant will attempt to find a position where the collapsed airway increases in size when the jaw is put in different positions. Different wax bite registrations are taken in order to find the best position to fabricate the oral appliance. The best registered reading
less than the original reading of .76 cm2. If the airway does not increase in size with the pharyngometer test when the mandible is moved forward, then this usually indicates that the oral appliance may not be successful unless the cause of the airway obstruction is resolved.
3. Oral Examination
enlarged uvula obstructing the airway.
4. Overnight Sleep StudyWe use the Embletta 100 home sleep study as an initial screening device, and also to help titrate the oral appliance before referring them back to the sleep clinic for confirmation that the oral appliance helped reduce the snoring and sleep apnea. The patient is able to sleep in their own bed and the results are available the next day. Justin’s results were:
5. PolysomnogramThe patient is referred to a sleep clinic for a polysomnogram test. The diagnosis of OSA must be made by a sleep specialist. Justin’s test result was:
The diagnosis by the sleep specialist was severe OSA. The sleep specialist recommended another sleep study with the CPAP device. Justin is age 18 and he did not want to wear the CPAP. I had informed him previously that if he had snoring and mild to moderate OSA, I would be willing to fabricate an oral appliance. I recommended the surgical removal of his enlarged tonsils and uvula. Once the severe airway obstructions were eliminated, another sleep study would be done to evaluate the severity of the OSA.
6. E.N.T. Specialist
removal of his enlarged tonsils and enlarged uvula.
7. Overnight Sleep Study (post surgical)After Justin’s tonsils and uvula were removed, the result was: RDI 12 Mild OSA
8. Consultation with ParentDue to the fact that Justin now had mild OSA, still snored slightly, had acid reflux and a family history of heart attacks and diabetes, it was decided to proceed with the oral appliance.
9. Overnight Sleep Study with Oral Appliance The result with the sleep study wearing an oral appliance was:
We were able to lower the RDI from 42 (polysomnogram) to an RDI of 6 by the surgical removal of the enlarged tonsils and uvula, and the oral appliance which moved his lower jaw slightly forward and protected his airway by preventing the mandible from collapsing his airway at night when he slept on his back. If you follow the protocol as I have discussed above, I think you will achieve a high level of success with your oral appliances. I must stress the fact that you need to work closely with your medical colleagues in your area. You need the sleep specialist to do the polysomnogram to diagnose obstructive sleep apnea. If there is an obstruction in the nasal pharyngeal or oropharyngeal airway, you need the cooperation of an E.N.T. specialist to surgically correct the problem. This case was successful because I worked closely with two of my medical colleagues to help my young 18 year old patient. I feel that I prolonged his life expectancy not to mention the fact that by relieving his serious snoring problem (70 decibels), I am certain that will help improve his overall health as well as his love life.
Protocol For Snoring Problems Male Age 18
Continued from Page 11

DENTAL SLEEP MEDICINE48
By Dr. John C. Jeppesen, DMD
Pneumodontics®The Evolution of a new sub-specialty in dentistry.
As a result of my own journey to correct my snoring and sleep apnea problem, I became
absolutely fascinated with the practice of sleep medicine. Besides my wife Brenda, the great inspiration for me was my personal mentor, the late, great Dr. Jim Garry. It was in 1996, after turning 40, that I began my quest to solve my own
began to notice the frequent absence of my wife upon awakening in the morning. The answer as to why this event kept occurring became crystal clear when Brenda played me an audio tape of the sounds I was evidently capable of making at night. After hearing the recording,
was that Brenda had taped a Harley Davidson commercial. Certainly no human could make that much noise. Turning to my then six-year-old son, I asked, “Is this really me?” Without hesitation, my son
I was creating in my household. So for the next year I agreed to sleep out in the living room so that my wife and son could get their well-deserved rest. During that period of time Brenda, an internet neophyte, found a Space Maintainers sponsored course on snoring and insisted that I take the course ASAP. The course was taught by a couple of orthodontists who demonstrated a dual arch, boil
Advancement Device (MAD). Most of the dentists at that meeting had this appliance made for them. I recall being very excited about this area of practice that I literally knew nothing about. But I
do remember a painful look on one
when asked how far to advance the lower jaw. With a mild cringe, the orthodontist said he recommended NOT to advance beyond “end-to-end.” So
for me. I took it home and it seemed to
down the Harley. My wife was now back in my bed when I woke up in the morning. I thought, “Gee, that was easy.” I became
excited that this was a new area of practice I had never considered before. Fast forward about 4 months later
and Brenda informed me that my snoring had returned.
I reviewed the Space Maintainers literature references way in the back of the document entitled “Recommended Reading References.” This is where I found the reference to a couple of documents authored by Dr. Jim Garry. I bought these publications and soon thereafter I signed up for his two-day course in October of 1996. Jim introduced me to the concept of “adjustable” MAD devices.
to another MAD that was at least semi-adjustable. To correct my snoring this time, I had to advance my mandible
beyond edge-to-edge. I noticed a bit of tenderness in my TMJs and teeth, but it
me that the snoring was again mitigated
ADSM (June 2000-Las Vegas) and I was introduced to several different devices. I was excited about the Thornton Adjustable Positioner (TAP®) as it was adjustable down to a quarter millimeter. The other device that fascinated me was the OPAP®. I knew nothing about positive airway pressure in 2000 and bought myself a TAP® kit. I fabricated the TAP® and the adjustability of the device made sense to me. If my snoring returned, I simply turned the advancement knob and I again
was quiet at night. Most importantly, Brenda was happy. When I started my treatment with the TAP® I had a near perfect Class I occlusion. I always took this for granted. I could chew the steaks I loved so much and the MAD was only being used at night, so I thought
that the early morning advancement
temporary when used with the “Leaf Gauges,” was still acceptable. However, after approximately 13-14 months into treatment with the TAP®, I noticed that
maximal intercuspation, i.e., Class I position. To my dismay, I noticed that my occlusion was fairly rapidly progressing from a near perfect Class I relationship to a mild Class III. I began to have trouble chewing my beloved steaks and also
WWW.SLEEPGS.COM 49
noticed that making my “s” sounds during
Nevertheless, I continued using the device. However, as the months rolled on, Brenda would periodically inform me that I needed to advance further to maintain the control of my snoring problem. Not wanting to end up back on the couch and not at all sure that I was ready for CPAP, I continued to advance the TAP® for the next several years. Referring to my original pre-treatment casts (2000) in early 2003, I noticed that I had a permanent advancement of my mandible equal to approximately 6mm. I even made a reverse TAP® as a morning repositioner to help clear prognathia back as far as I could. This approach was clearly not working and now I began to encounter fracture of some posterior teeth as my bite, on most all teeth, was cusp on cusp and edge-to-edge. Also I noticed that I had developed an obvious anterior open bite precluding incisal mastication such that to eat my beloved steak, I had to bite on my premolars. From 2000 to mid-2003 I continued to treat my own patients with MAD. However, now some of my patients were reporting similar permanent advancement issues. Then the straw that broke my
data presented by the esteemed Dr. Alan Lowe (ADSM-Chicago-2003) indicating that at least 70% of Class I occlusions were at risk of becoming Class III occlusions due to the MAD
derived from study of his own Kleerway appliance. To say the least, this really
to “do no harm.” And clearly, I was doing harm, or at least producing unreasonable
made the decision to stop recommending mandibular advancement to as many patients as I could.
Rolling back to 2000, I had also started to treat my patients with moderate to severe OSAS using the OPAP® device. Using this device, I was able to treat very high RDIs successfully. Between 2000 and 2005, I had now surpassed Dr. Richard Moore as the doctor who had made the most OPAP® devices in the world. Along the way I learned a couple of things. One, oral positive airway pressure had its place. It worked particularly well for patients with extreme nasal impatency. Second, I attempted to treat one patient with a history of TMD and advanced her mandible a mere 2mm and she had
of TMD and left my practice never to return again. For some reason, I thought it was in fact necessary to advance mandibles even when using PAP. I
was thoroughly brainwashed into thinking that all sleep apnea dental treatments must include mandibular advancement, regardless of whether the power of positive airway pressure was really doing all the work of correcting OSAS. Regarding OPAP®, I also learned along the way that case selection was extremely important because my rate of positive outcome was 60% to 70% at best. As an anal-retentive dentist, this was not acceptable to me. I needed a new solution. Because I was an inventor before I became
a dentist, solving problems creatively was very natural for me. So again, I proceeded with my journey to create a better, more powerful and consistent solution to treating OSAS patients, which was now all I did in
with teeth or gums, and I certainly was at least a mild neophyte as concerns the treatment of TMD. I never went through
practice was limited to treating a medical condition, sleep-disordered breathing, now usually with CPAP and BiPAP, what was I? I have also always been uncomfortable with the term “Dental Sleep Medicine.”
the physicians who were involved in sleep
Sleep Medicine specialists. I concluded that there was only sleep medicine going on here. But sleep medicine itself includes
a very large number of other esoteric sleep disorders that were not the focus of my practice. My focus was simple. My practice was all about helping patients
when I realized that I really was a Pneumodontist®.
orthodontist, endodontist, periodontist, prosthodontist, and pedodontist, I was
Pneumodontist®of a brand new subspecialty in dentistry which I entitled Pneumodontics®. All I did all day long in my practice now was to treat SDB patients with various forms of positive airway pressure. I also realized that advancing the mandible was not necessary and in fact introduced unreasonable risk to my SDB patients. I also realized that God designed our human
Continued on Page 46
DENTAL SLEEP MEDICINE50
respiratory tracts to preferably breathe nasally. Another exciting development was occurring in the engineering of CPAP machines. I learned of AutoCPAP and C-FLEX (expiratory relief). C-FLEX is the best thing to happen to CPAP since its invention by Sullivan because it makes exhaling against the incoming PAP really easy for most patients. Therefore, this notion that we need to advance mandibles to lower therapeutic pressure was completely false. My SDB practice was built on other
physicians who could not get their patients well began to send me their so-called “CPAP intolerant” or “CPAP failure” patients. I soon learned that these archaic terms, “intolerance” and “failure” were in fact misnomers.
rather these patients were simply not given an opportunity to succeed. There is a difference. In my quest to create a better solution for patients who could not tolerate STANDARD therapy, I had to learn what the major issues were regarding failure of STANDARD therapy. The chief complaints were:
f) Difficulty in tolerating high therapeutic pressures.
The answer was to individualize/customize the pressure-based cases. Realizing that most STANDARD masks were made on manikin heads on mass-production lines in China, it was no wonder that at least 50% of my patients were having CPAP interface problems.
The medical technology industry was using a cookie cutter approach. Cookie cutters are great for making cookies but not really effective in applying this principle to treating humans, where their molds are ALL different. And as they say, the mold is broken (by God) after the human is made. So by approaching each case individually and like a detective,
complaints with STANDARD therapy, it was possible to successfully treat most SDB patients with the gold standard: CPAP therapy. Using this (customizing) approach, I was able to take more than 42 consecutive so-called failures of STANDARD CPAP therapy and make
them CPAP champions. Again, these patients were not intolerant of CPAP nor
not given the opportunity to succeed. CPAP, when utilized correctly, is a very attractive therapy because it is inherently safe, requires no surgery or drugs, and is purely homeopathic as it utilizes room air to create a pneumatic splint. CPAP is, in fact, a very elegant solution if the clinician knows how to make it work for the patient. Inventing, as Thomas Edison once said, is 1% inspiration and 99% perspiration. Inventing requires hard work, attention to detail, and stubborn persistence, with
revisions and constant prototyping. The other very important fact to understand about inventing is that there are NO PERFECT SOLUTIONS. This is particularly true in medicine, as every time we address the chief complaint of the patient successfully, we invariably
exist before. This is an extremely important message to translate to your
expectations. Statistically, in my practice, I can get about 90% of all SDB patients
onto PAP regardless of the size of the patient, the severity of the index, or the type of SDB, i.e., obstructive, central, or complex. When I treat a SDB patient, I need to know two facts to start. First:
Is the type of CPAP machine that they were introduced to appropriate for the patient? Second: Can they utilize a STANDARD interface/mask? Typically, the so-called failure of STANDARD CPAP arrives at my
SINGLE PRESSURE THEORY. Single Pressure Theory (SPT) has
make common sense. SPT is based on a faulty assumption which is that the upper airway dynamics of the
patient remain a constant as if the upper airway is made from a rigid material like PVC. Nothing could be further from the truth. Upper airways are dynamic structures that change continuously throughout the night and vary in their rigidity every single night. Therefore, attempting to treat a patient with a single pressure does not make much common sense. SPT is determined in the sleep lab using a supposed worst case scenario. The single pressure determined in the sleep lab via PSG is, at best, a snapshot in time. The patient is supine and in REM, and during this examination whatever pressure reduces the AHI/RDI on that night in the
Pneumodontics®Continued from Page 45

WWW.SLEEPGS.COM 51
lab is assumed to be correct for the next night. Hard evidence suggests/proves that no patient should ever be treated using a single pressure. Therapeutic pressure requirements vary from night-to-night for all patients. Correct pneumatic splinting requires delivering just the right pressure at any given moment, i.e., not too much, not too little. I call this the therapeutic window, and again, this therapeutic window changes with every patient from night to night. This is why most of my patients are treated using an AUTOCPAP machine. This AUTOCPAP machine delivers the right amount of pressure minute-to-minute, night-to-night. In fact, because the optimal amount of REM sleep is about 25% of TST (Total Sleep Time), setting a single pressure for this patient will often result in over pressurization 75% of the time. Over pressurization will often create abnormal respiratory events and resultant brain arousals. Automatic (CPAP) algorithms used by single, bi-level S, bi-level ST, and servo-ventilators require correct feedback to the machine for it to work effectively. Correct feedback assumes perfect pneumatics, i.e., control of leaks. Without control of the leaks, the automatic adjusting machines will typically overcorrect/over-ventilate. Therefore, the objective with the interface, be it STANDARD or CUSTOM, is to create excellent pneumatic control of untoward leaks. This is the key.
When a patient cannot tolerate a STANDARD interface or the pneumatics are not excellent, I advance the patient to a custom interface. This could be an OPAP®, but what I utilize most often is trademarked as the JPAP® Obturator. JPAP® is an acronym that stands for Jeppesen Positive Airway Pressure. Hallmark features of the JPAP® Obturator are:
of the mandible in a neutral centric position. This is an orthopedically sound (patented) position that is kind to the TMJs. Typically this neutral centric position will be where TMJ specialists record their
bite registrations to treat TMJ Dysfunction. If the TMJ patient requires a daytime orthotic/splint, this neutral centric position for the JPAP® will be almost identical to the splint position. The only difference would be to make sure the patient has an appropriate vertical dimension of occlusion (VDO) to allow for adequate tongue volume. The method of finding this
neutral centric position is up to the clinician and may include TENS, Energex, Phonetic techniques, etc.
snap-fit to position and hold the maxilla and mandible together, without lateral movement, to prevent mouth venting of PAP.
device sits upon a cylindrical slide which is mounted to the anterior surface of the orthotic positioned at the nasal midline.
proper NASAL ANGULATION.
pressure tubing has RIGID TUBES that are milled with spiral threads to permit precise adjustment to the left and right nares of the patient’s nose.
RIGID SPIRAL THREADED TUBES are SWIVEL PILLOWS®. These swivels are composed of ball and socket joints which permit 360 degree rotation at a 30 degree compound angle. This permits precise angulation into the nares.
AP adjustment closer to the face or further away
from the face depending on the length of the nose itself.
entire PLATFORM permits equalization of the nasal pillow compression for comfort into each nare.
DENTAL SLEEP MEDICINE52
29% and 83% of patients did not adhere to therapy. Fortunately there is an extensive body of evidence that supports three low cost interventions proven to improve acceptance, adherence and compliance. The three proven interventions are heated
and follow up. Lifetime follow up may be one of the most important, yet almost always overlooked, aspects of successful CPAP treatment. Durable medical equipment (DME) dealers are normally the companies that set up patients on CPAP under the direction of a medical professional. Long term follow up with CPAP patients falls into 5 types and over time companies may progress in their follow up regimen. The least effective follow up is termed “set
‘em and forget ‘em”. This is the company
additional contact with the patient that goes un-reimbursed simply adds cost and
sale. The second stage is when the DME, somtimes reluctantly, sells supplies to a walk-in patient. This takes time from the respiratory therapist and costs more than the
next evolution involves outbound calls to patients from a small local branch or single unit DME dealer and then mailing supplies to the patient. Unfortunately the urgent takes precedent over the vital, and COPD patients requiring supplemental oxygen are handled before making proactive follow up calls to CPAP patients. The fourth stage involves centralizing those calls in one location to avoid day to day operational and
evolution of long term or lifetime follow up for CPAP patients is the development of a CPAP compliance call center. The optimal call center should have highly trained CPAP specialists that can assist CPAP patients with all of their equipment and supply needs. Additionally, the CPAP specialists should have a simple CPAP troubleshooting algorithm that allows them to handle simple problems and help maintain CPAP compliance. The call center software
must trigger the quarterly calls to every patient and have ready access to the CPAP supply purchase pattern so that the agent can
supplies necessary to improve the patient
easily be ordered. It is necessary for the DME to have a prescription as well as a copy of the sleep study to bill Medicare and most insurance companies. The sleep study must indicate severe OSA (> 15 AHI or >5 AHI with symptoms) or else third party payers will not cover CPAP therapy. The call center must have availability of a trained respiratory therapist and also be comfortable reporting non-compliance to the treating medical professional. CPAP failure rates can be lowered by selecting a DME supplier who specializes in sleep therapy, performs all three low cost interventions proven to increase compliance, and operates a “state of the art” CPAP call center for a lifetime of health coaching and follow up. Even with the addition of all the evidence based interventions, some severe OSA patients are simply unable to tolerate CPAP therapy. An oral appliance serves as an excellent rescue option for patients that are unable or unwilling to utilize CPAP therapy so they can receive some relief from a condition that carries such devastating co-morbidities.
Continued from Page 27
Obstructive Sleep Apnea and CPAP

WWW.SLEEPGS.COM
Raising the Level of Suspicion
By Dan Tache DDS, D,ABDSM
PSG may lack sufficient sensitivity and that in some cases, there may be a much higher level of OSA.
In epidemiology, the validity of any control of random error, bias, and confounding. These three phenomena are considered alternative explanations when assessing the outcome measure of a study. Random error is the probability that the observed result is due to chance. Bias is a systematic error committed by the investigator during the course of a study, while confounding is not the fault
the inescapable fact that all research is involves free-living human beings.1 It might be helpful to view confounding as a mixing of the effects between the subject(s) being studied and other extraneous factors. The validity of epidemiologic studies also requires that the study be conducted over a particular risk period. 2 The Polysomnogram (PSG) is viewed as the Gold Standard in the objective evaluation of sleep and as such, should be held to the highest standards for validity, much as we expect of epidemiologists when gathering data in the search for central themes or hypotheses in the matter of public health. The PSG does have shortcomings because it is expensive and as a consequence of the cost, the “risk period” during which data collected, is typically only one or two nights. It is widely appreciated that there
of sleep often observed from sleeping in a sleep laboratory vis-à-vis at home. This phenomenon often leads to an
sleep. This “inaccuracy” can be manifest either a classic First Night Effect (FNE)
where there is an exaggeration of sleep
First Night Effect (RFNE) where obtained sleep data represents a better-than-normal sleep than that normally experienced while sleeping at home. The Reverse First Night Effect (RFNE), is characterized by longer rapid eye movement (REM) sleep latency (p < 0.05), increased wakefulness (p < 0.01) and total sleep time (p < 0.02)
0.01).3 The RFNE should be viewed as a potentially more serious confounder than a RFE because the net result is a modest to
severe underestimation of the severity of obstructive sleep apnea. Because of these shortcomings, the PSG
tool in the assessment of insomnia according to American Academy of Sleep Medicine guidelines4 A comparable maladaptive response by both children and adolescents has also been observed.5When a patient who has been diagnosed with obstructive sleep apnea syndrome (OSAS) is deemed to be CPAP-intolerant,
dentist for management of the OSAS with
Mandibular Repositioning Device (MRD). It is generally agreed that such treatment is governed by the Guidelines established by The American Academy of Sleep Medicine (AASM). The American Academy of Sleep Medicine (AASM) has developed evidence-based “Practice Parameters” which provide clinicians with clear recommendations for the evaluation and management of patients with sleep disorders. These parameters are based on
literature. The “Guidelines” which govern the behavior or the Dental Sleep clinician are clearly delineated in the publication: “The Practice Parameters for the Treatment of Snoring and Obstructive Sleep Apnea with Oral Appliances: An Update for 2005” 6. The “Guidelines” are explicit that the PSG should have been obtained prior to the fabrication of an oral device and implicit in that recommendation is that this necessary diagnostic aid is an accurate representation of the level of disease with which the patient presents to us for treatment. Unlike the split-night
study with CPAP-application, when application and titration is completed in one night, the process of MRD Titration to achieve airway stabilization may often take weeks or months to achieve.
mild to moderate OSAS but an honest representation of the time that is often required for the patient to comfortably adapt the necessary 3-dimensional changes
3.1 Diagnosis3.1.1 The presence or absence of OSA must be determined before initiating treatment with oral appliances to identify those patients at risk due to complications of sleep apnea and to provide a baseline to establish the effectiveness of subsequent treatment. Detailed diagnostic criteria for OSA are available and include clinical signs, symptoms and the findings identified by polysomnnography. The severity of sleep related respiratory problems must be established in order to make an appropriate treatment decision. 320 Kushida, CA 2006
53
DENTAL SLEEP MEDICINE
nocturnal mandibular repositioning. The Sleep Dentist will often utilize Unattended Portable Monitors (PM) during the MRD titration progress to ascertain when maximum medical improvement (MMI) has been achieved. Because of the RFNE, this clinician has often observed a relative worsening of the disease level when the PM results are downloaded. Naively, the novice dental clinician who may be unaware of a confounding RFNE might misinterpret the seemingly worsening status of his or her patient as a manifestation
titrated MRD or that the MRD was making the patient worse. If one is unaware of this phenomenon it is altogether possible that the PM will be looked upon as faulty or lacking
never even considering that the problem might lie with the sensitivity of the correctness of the PSG. Retrospective cohort studies have shown that the prevalence of RFNE may
to 43%.” The same study went on to
variability of AHIs and microarousal
that “an important number of subjects presented false-negative results” and that a FNE was found “to be more frequent among severe cases”. 7 The purpose of this article is to raise the level of suspicion that the PSG may
cases, there may be a much higher level of OSAS than was reported from data
lab. It is crucial that the Sleep Dentist be aware of this because it can have a profound effect upon treatment to the extent that the treating clinician may even decide from the onset of treatment that a
MRD alone might not be
the patient will be made aware that a “Hybrid” approach (MRD plus CPAP) will likely be necessary. When it is clear that a RFNE is in effect, it is the exception that the PSG will be repeated due to this inaccuracy and again, probably because of the cost. It is also less common to read in the summary of a PSG report that a First Night Effect (or RFNE) was observed and that it (the PSG) will be or should be repeated,
instead, one will read that there was a
increased wakefulness or decreased
in % REM of Total Sleep time (TST). These intimations by the report sleep specialist of a problem with sensitivity of the diagnostic PSG are not meant to deceive, rather, such an event for the patient whose OSAS will, in most cases, be controlled with CPAP therapy, only means an additional centimeter or two of
can tolerate the treatment but if such error means an additional millimeter or two of
mandibular advancement, this could be
treating with OSAS with a MRD alone. The PSG to this date, is performed with the knowledge that if a problem is
dreary compliance rates reported by many. Consequently, a little problem of underestimation of disease level because of a RFNE such that the diagnosis is perhaps, Upper Airway Resistance Syndrome or mild OSAS when there is in fact, a severe level of OSAS exists is
specialist who considers MRD therapy as an essential part of the strategies for managing OSAS will understand that it is important to get it right because of the limitations of MRD therapy but such individuals are the exception, albeit, that is changing but until that day arrives, it will incumbent upon the dentist, to whom this CPAP-intolerant patient is being referred, that he or she be able to anticipate when a RFNE is in effect. It might even be prudent to offer a PM to the patient BEFORE making any promises or commencing treatment. I hope through “Case Presentation” to illustrate this problem and how to best anticipate when the PSG data might be confounded by a RFNE. Because treatment strategies for MRD therapy may vary considerably with the level of OSAS, it may perhaps be necessary to reassess OSAS levels by performing an unattended PM sleep study BEFORE proceeding with MRD therapy in order to communicate any changes in the potential outcome of MRD therapy to the patient. It is critical
of their probability of success given the adverse medical consequence resultant from failure to effectively manage such a disease.
CASE STUDY
This is a study of a 42 y.o. female, JM,
complaints of “sensitive/chipping teeth” , “TMJ pain” and “fatigue”. Clinical examination of the teeth alone was remarkable because of the severity of the generalized attrition of the teeth on all surfaces with severe cervical erosions present both lingually and facially on
54
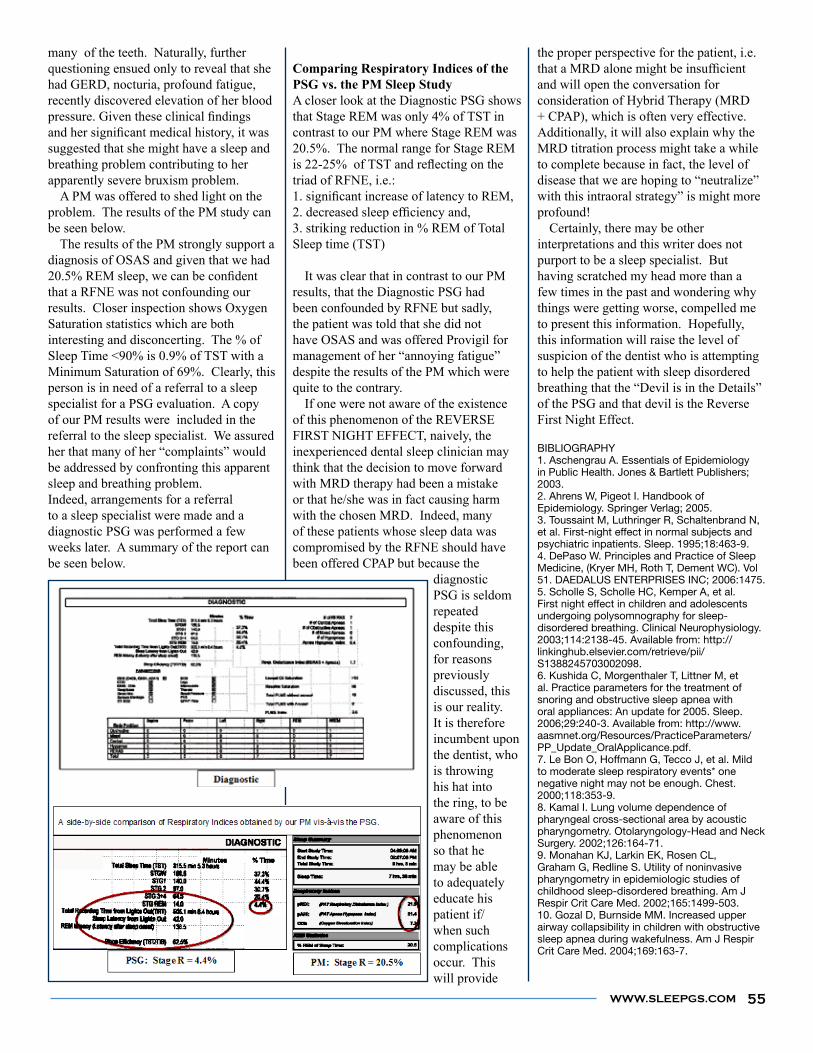
WWW.SLEEPGS.COM
many of the teeth. Naturally, further questioning ensued only to reveal that she had GERD, nocturia, profound fatigue, recently discovered elevation of her blood
suggested that she might have a sleep and breathing problem contributing to her apparently severe bruxism problem. A PM was offered to shed light on the problem. The results of the PM study can be seen below. The results of the PM strongly support a diagnosis of OSAS and given that we had
that a RFNE was not confounding our results. Closer inspection shows Oxygen Saturation statistics which are both interesting and disconcerting. The % of Sleep Time <90% is 0.9% of TST with a Minimum Saturation of 69%. Clearly, this person is in need of a referral to a sleep specialist for a PSG evaluation. A copy of our PM results were included in the referral to the sleep specialist. We assured her that many of her “complaints” would be addressed by confronting this apparent sleep and breathing problem.Indeed, arrangements for a referral to a sleep specialist were made and a diagnostic PSG was performed a few weeks later. A summary of the report can be seen below.
A closer look at the Diagnostic PSG shows that Stage REM was only 4% of TST in contrast to our PM where Stage REM was 20.5%. The normal range for Stage REM
triad of RFNE, i.e.:
3. striking reduction in % REM of Total Sleep time (TST)
It was clear that in contrast to our PM results, that the Diagnostic PSG had been confounded by RFNE but sadly, the patient was told that she did not have OSAS and was offered Provigil for management of her “annoying fatigue” despite the results of the PM which were quite to the contrary. If one were not aware of the existence of this phenomenon of the REVERSE FIRST NIGHT EFFECT, naively, the inexperienced dental sleep clinician may think that the decision to move forward with MRD therapy had been a mistake or that he/she was in fact causing harm with the chosen MRD. Indeed, many of these patients whose sleep data was compromised by the RFNE should have been offered CPAP but because the
diagnostic PSG is seldom repeated despite this confounding, for reasons previously discussed, this is our reality. It is therefore incumbent upon the dentist, who is throwing his hat into the ring, to be aware of this phenomenon so that he may be able to adequately educate his patient if/when such complications occur. This will provide
the proper perspective for the patient, i.e.
and will open the conversation for consideration of Hybrid Therapy (MRD + CPAP), which is often very effective. Additionally, it will also explain why the MRD titration process might take a while to complete because in fact, the level of disease that we are hoping to “neutralize” with this intraoral strategy” is might more profound! Certainly, there may be other interpretations and this writer does not purport to be a sleep specialist. But having scratched my head more than a few times in the past and wondering why things were getting worse, compelled me to present this information. Hopefully, this information will raise the level of suspicion of the dentist who is attempting to help the patient with sleep disordered breathing that the “Devil is in the Details” of the PSG and that devil is the Reverse First Night Effect.
BIBLIOGRAPHY1. Aschengrau A. Essentials of Epidemiology in Public Health. Jones & Bartlett Publishers; 2003. 2. Ahrens W, Pigeot I. Handbook of Epidemiology. Springer Verlag; 2005. 3. Toussaint M, Luthringer R, Schaltenbrand N, et al. First-night effect in normal subjects and psychiatric inpatients. Sleep. 1995;18:463-9. 4. DePaso W. Principles and Practice of Sleep Medicine, (Kryer MH, Roth T, Dement WC). Vol 51. DAEDALUS ENTERPRISES INC; 2006:1475. 5. Scholle S, Scholle HC, Kemper A, et al. First night effect in children and adolescents undergoing polysomnography for sleep-disordered breathing. Clinical Neurophysiology. 2003;114:2138-45. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1388245703002098. 6. Kushida C, Morgenthaler T, Littner M, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: An update for 2005. Sleep. 2006;29:240-3. Available from: http://www.aasmnet.org/Resources/PracticeParameters/PP_Update_OralApplicance.pdf. 7. Le Bon O, Hoffmann G, Tecco J, et al. Mild to moderate sleep respiratory events* one negative night may not be enough. Chest. 2000;118:353-9. 8. Kamal I. Lung volume dependence of pharyngeal cross-sectional area by acoustic pharyngometry. Otolaryngology-Head and Neck Surgery. 2002;126:164-71. 9. Monahan KJ, Larkin EK, Rosen CL, Graham G, Redline S. Utility of noninvasive pharyngometry in epidemiologic studies of childhood sleep-disordered breathing. Am J Respir Crit Care Med. 2002;165:1499-503. 10. Gozal D, Burnside MM. Increased upper airway collapsibility in children with obstructive sleep apnea during wakefulness. Am J Respir Crit Care Med. 2004;169:163-7.
55

DENTAL SLEEP MEDICINE
Sleep apnea is a common disorder in which a person has one or more pauses in breathing or shallow breaths while sleeping. Sleep apnea affects more than 12 million people in the United States. The most common type of sleep apnea is obstructive sleep apnea (OSA). In OSA, the throat muscles relax and block the airway. It is associated with a number of diseases, including the following eye conditions:
In this syndrome, the eyelids can turn inside-out during sleep. The eyes may become
such as irritation, tearing, mucus discharge and blurry vision.
Having sleep apnea seems to increase the risk of developing glaucoma. Glaucoma is the most common cause of irreversible blindness. OSA has been associated with two forms of glaucoma, primary open-angle glaucoma (OAG) and normal-tension glaucoma (NTG).
NAION is a sudden, painless loss of vision in one eye often noticed upon awakening. Certain studies suggest an increased incidence of OSA in patients diagnosed with NAION. Papilledema is characterized as a swelling of the optic nerve in both eyes usually due to increased pressure in the skull. This condition may damage the brain and may cause vision loss. Patients with OSA often have a higher incidence of papilledema. Although it is not understood exactly why OSA may contribute to certain eye conditions, it is important for health care professionals to be aware of the possible associations in order to diagnose them earlier. Patients with obstructive sleep apnea should be asked about possible eye problems and possibly have their eyes examined. Conversely, patients who already have these eye conditions should be evaluated for sleep apnea.
com/od/sportsvision/a/Sleep_Apnea.htm). Used with permission of About, Inc. which can be found online at www.about.com. All rights reserved.
OSA and Eye Vision
By Troy Bedinghaus OD
Awareness of the possible associations in order to diagnose them earlier.
CU
T A
LO
NG
LIN
E A
ND
FA
XC
UT A
LO
NG
LIN
E A
ND
FA
X
56
WWW.SLEEPGS.COM
Dental Sleep Clinics
www.dentalsleepclinics.com
DENTAL SLEEP MEDICINE