
Immunomodulatory oligonucleotides inhibit neutrophil migration by ...
11/2/2012
1
Successfully implement theAdvanced Clinical Parameters to benefit the patient, the lab and the Accountable Care Organization Model
of
The s
and
s
s
Disclosure
Honorarium from Sysmex for this lecture

11/2/2012
2
Introduction
• Holly McDaniel, MD– AP/CP and Cytopathologist
– Clin‐Path Associates (CPA)
– Laboratory Medical Director Banner Estrella Medical Center (BEMC)
– Pathology Specialists of Arizona (PSA)
• Laboratory Sciences of Arizona (LSA)
• Banner Health (BH)
Success!
Banner Health
Largest non profit health care system in the country serving patients across 7 states.
• 22 hospitals
• 6 long term care centers
• Family Clinics
• Home care services
• Medical Equipment services
11/2/2012
3
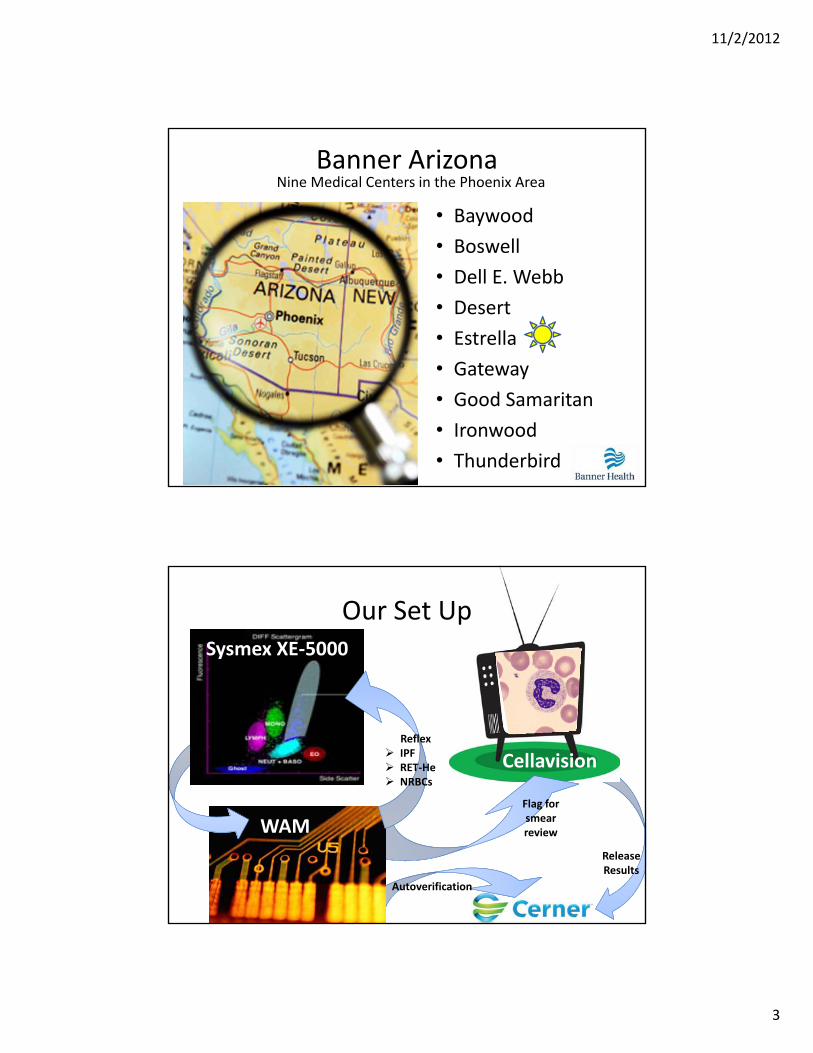
Banner Arizona
• Baywood
• Boswell
• Dell E. Webb
• Desert
• Estrella
• Gateway
• Good Samaritan
• Ironwood
• Thunderbird
Nine Medical Centers in the Phoenix Area
Cellavision
Our Set Up
WAM
Sysmex XE‐5000
Autoverification
Reflex IPF RET‐He NRBCs
Flag for smear review
Release Results
11/2/2012
4
Plan
Reach out
Connect with the BIG Picture
The ABCs of ACPsAdvancedClinicalParameters
Plan: Goals
MAIN GOAL
• Patients: Improved patient care
– IG: Infection, sepsis, response to treatment
– RET‐He: Anemia management, improve transfusion practices, improve EPO utilization
– IPF: Assist with diagnosis of thrombocytopenia, improve transfusion practices, decrease unnecessary bone marrow biopsies
– NRBCs: Better triage of patients from ICU to floor
11/2/2012
5
Plan: Goals
SECONDARY GOALS• Lab– Improve quality• Better tests• WAM:
– Middleware Solutions
– Standardize rules
• Cellavision
– Improve efficiency• Decrease waste time
• Fewer manual differentials
• Autoverification
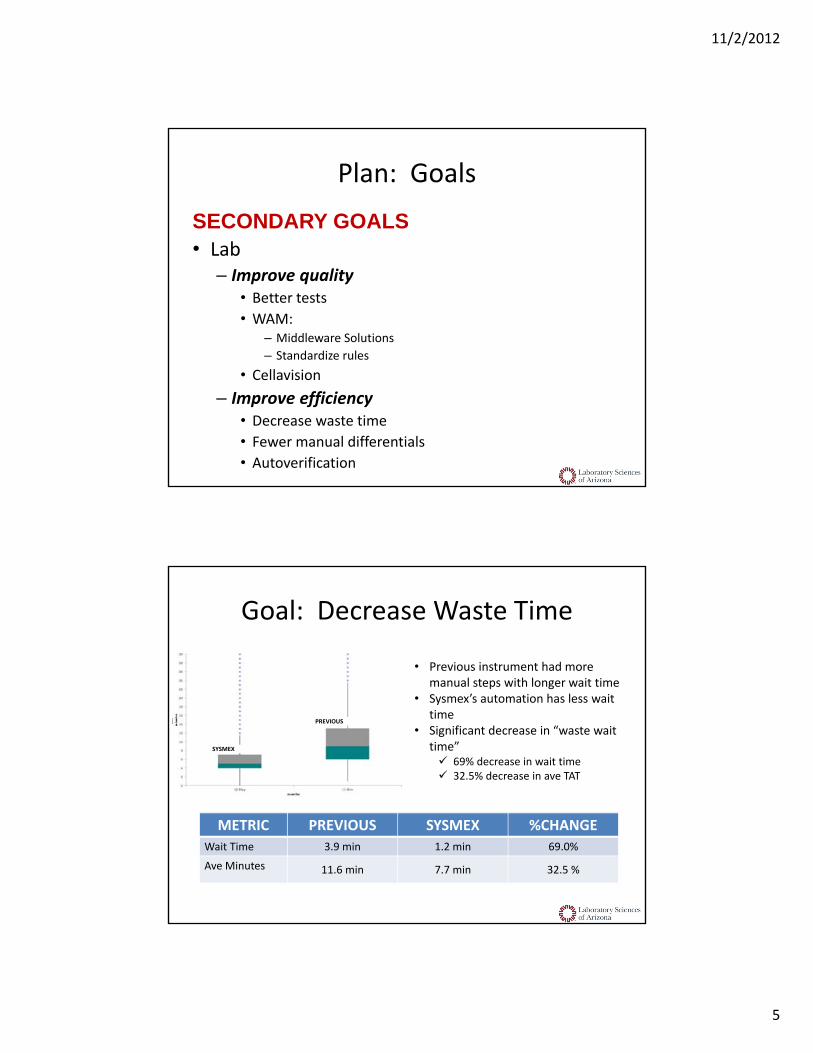
• Previous instrument had more manual steps with longer wait time
• Sysmex’s automation has less wait time
• Significant decrease in “waste wait time” 69% decrease in wait time 32.5% decrease in ave TAT
PREVIOUS
METRIC PREVIOUS SYSMEX %CHANGE
Wait Time 3.9 min 1.2 min 69.0%
Ave Minutes 11.6 min 7.7 min 32.5 %
Goal: Decrease Waste Time
SYSMEX
11/2/2012
6
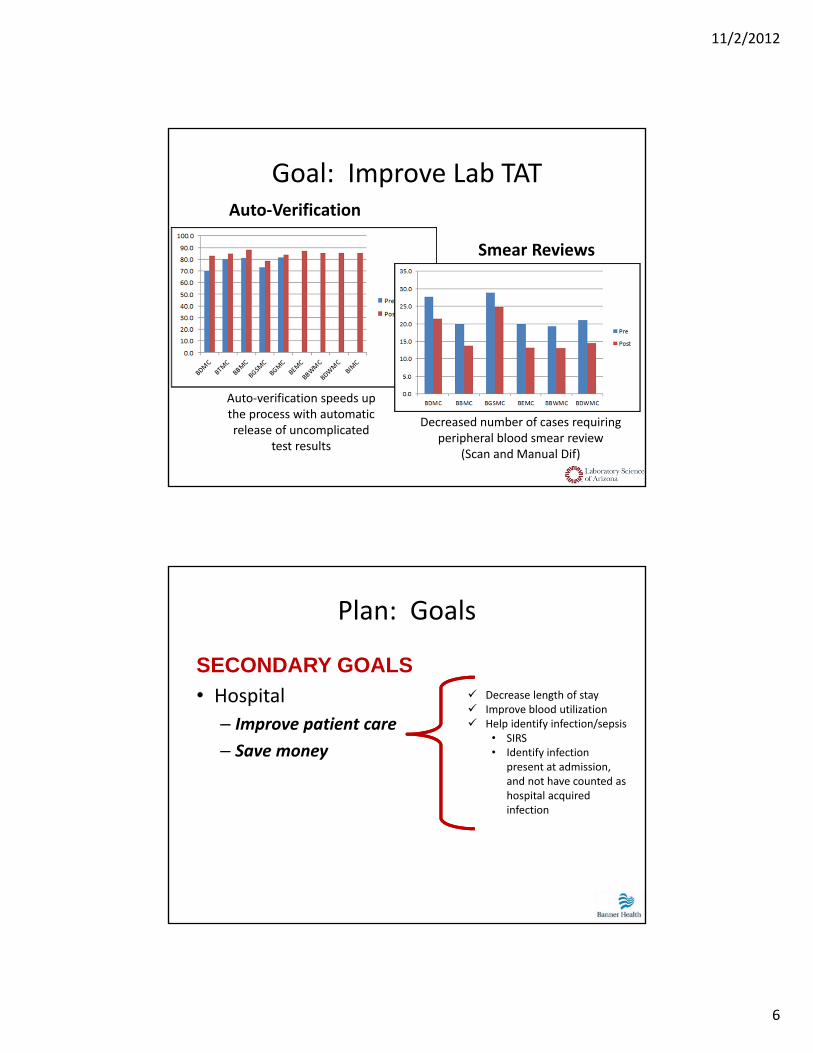
Goal: Improve Lab TAT
Decreased number of cases requiring peripheral blood smear review
(Scan and Manual Dif)
Auto‐verification speeds up the process with automatic release of uncomplicated
test results
Smear Reviews
Auto‐Verification
Plan: Goals
SECONDARY GOALS
• Hospital
– Improve patient care
– Save money
Decrease length of stay Improve blood utilization Help identify infection/sepsis
• SIRS• Identify infection
present at admission, and not have counted as hospital acquired infection
11/2/2012
7
How to reach goals
• Education!
• Questions to consider:
?What are these ***NEW*** tests?
?What do the results mean to my patient?
?What do published studies say?
?What in‐House studies should we do?
?Where should the tests be added to Care Pathways?
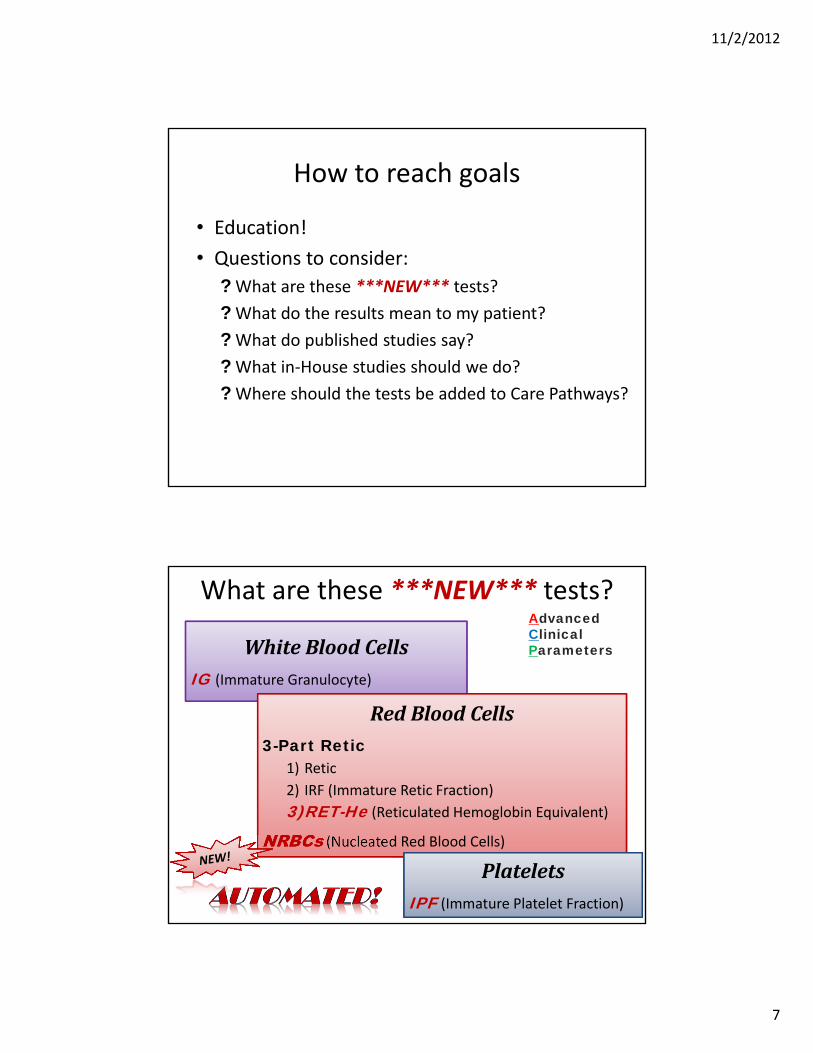
WhiteBloodCellsIG (Immature Granulocyte)
RedBloodCells3-Part Retic
1) Retic
2) IRF (Immature Retic Fraction)
3)RET-He (Reticulated Hemoglobin Equivalent)
NRBCs (Nucleated Red Blood Cells)
PlateletsIPF (Immature Platelet Fraction)
What are these ***NEW*** tests?AdvancedClinicalParameters
11/2/2012
8
Immature Granulocytes
IG
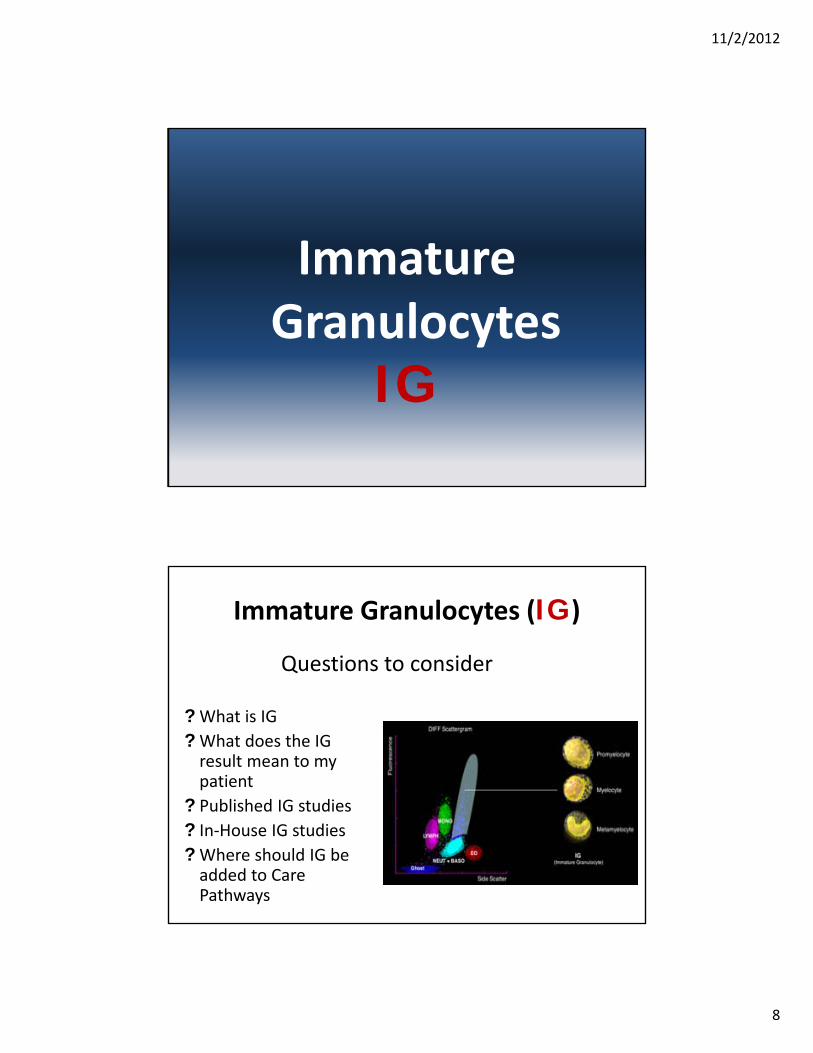
Immature Granulocytes (IG)
?What is IG
?What does the IG result mean to my patient
? Published IG studies
? In‐House IG studies
?Where should IG be added to Care Pathways
Questions to consider
11/2/2012
9
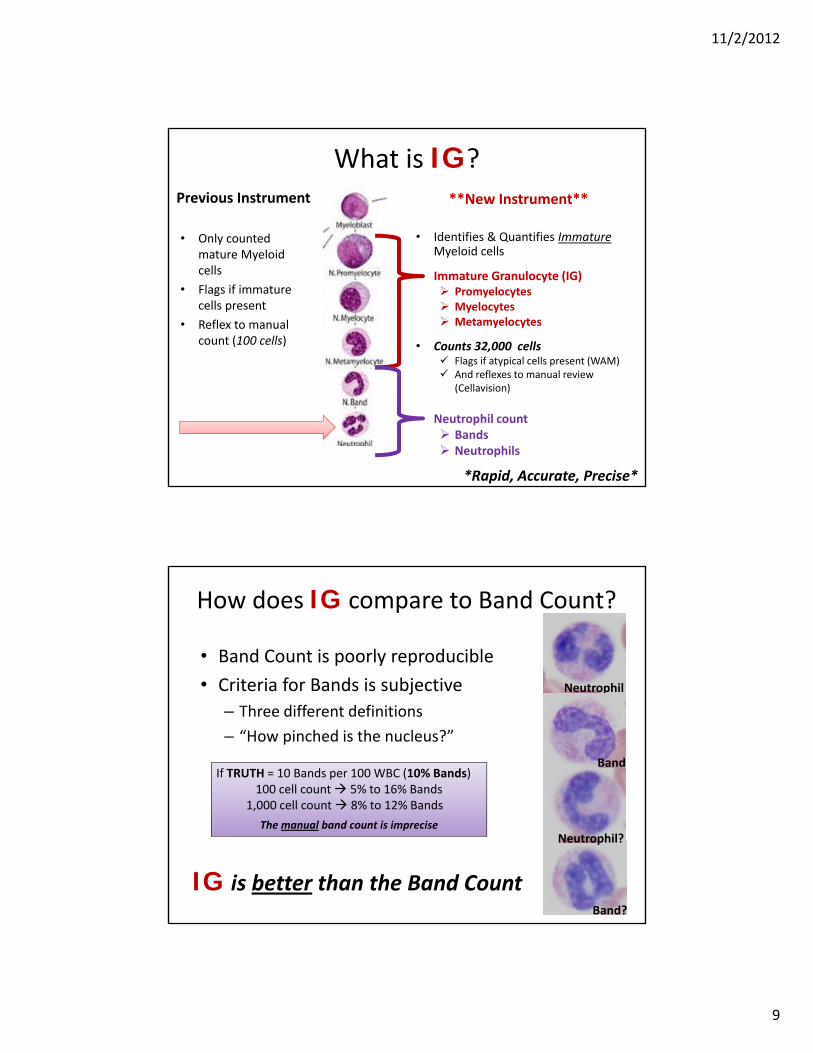
What is IG?Previous Instrument
• Only counted mature Myeloid cells
• Flags if immature cells present
• Reflex to manual count (100 cells)
**New Instrument**
• Identifies & Quantifies ImmatureMyeloid cells
Immature Granulocyte (IG) Promyelocytes Myelocytes Metamyelocytes
• Counts 32,000 cells Flags if atypical cells present (WAM) And reflexes to manual review
(Cellavision)
Neutrophil count Bands Neutrophils
*Rapid, Accurate, Precise*
How does IG compare to Band Count?
• Band Count is poorly reproducible
• Criteria for Bands is subjective
– Three different definitions
– “How pinched is the nucleus?”
If TRUTH = 10 Bands per 100 WBC (10% Bands)100 cell count 5% to 16% Bands
1,000 cell count 8% to 12% Bands
The manual band count is impreciseNeutrophil?
Neutrophil
Band?
Band
IG is better than the Band Count
11/2/2012
10
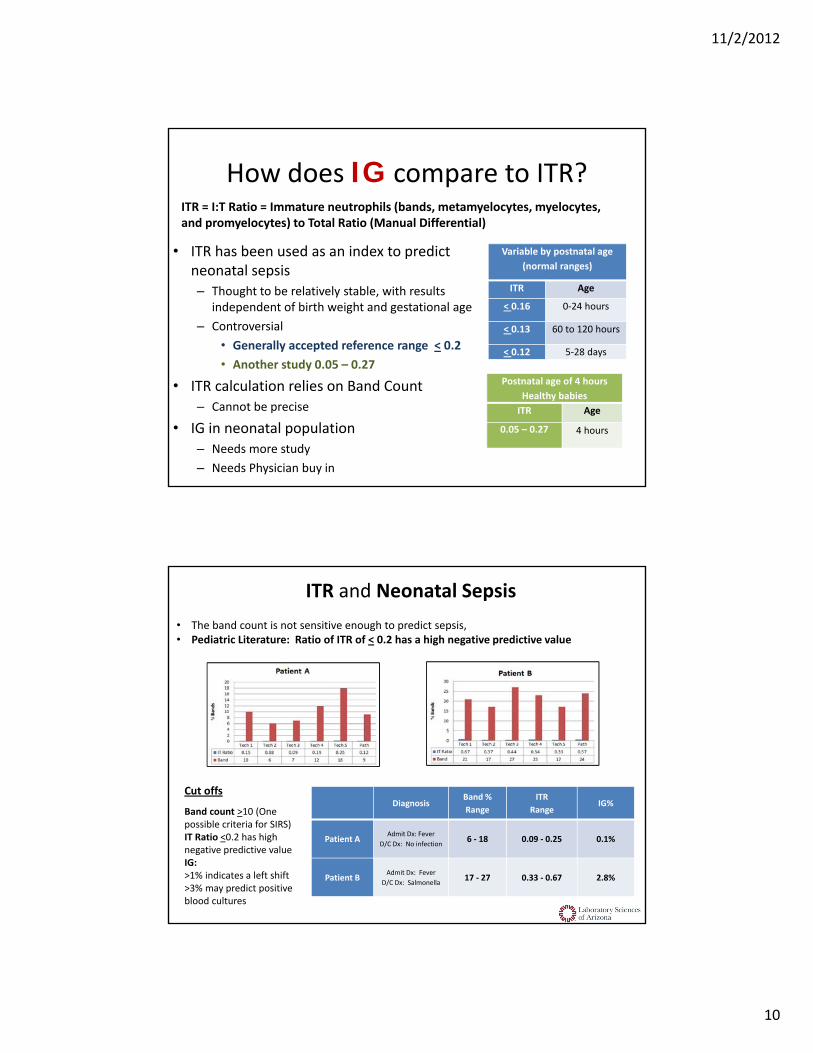
• ITR has been used as an index to predict neonatal sepsis– Thought to be relatively stable, with results
independent of birth weight and gestational age
– Controversial
• Generally accepted reference range < 0.2
• Another study 0.05 – 0.27
• ITR calculation relies on Band Count– Cannot be precise
• IG in neonatal population– Needs more study
– Needs Physician buy in
How does IG compare to ITR?
Variable by postnatal age
(normal ranges)
ITR Age
< 0.16 0‐24 hours
< 0.13 60 to 120 hours
< 0.12 5‐28 days
Postnatal age of 4 hours
Healthy babies
ITR Age
0.05 – 0.27 4 hours
ITR = I:T Ratio = Immature neutrophils (bands, metamyelocytes, myelocytes, and promyelocytes) to Total Ratio (Manual Differential)
DiagnosisBand %
Range
ITR
RangeIG%
Patient AAdmit Dx: Fever
D/C Dx: No infection6 ‐ 18 0.09 ‐ 0.25 0.1%
Patient BAdmit Dx: Fever
D/C Dx: Salmonella 17 ‐ 27 0.33 ‐ 0.67 2.8%
• The band count is not sensitive enough to predict sepsis,• Pediatric Literature: Ratio of ITR of < 0.2 has a high negative predictive value
Cut offs
Band count >10 (One possible criteria for SIRS)IT Ratio <0.2 has high negative predictive value IG: >1% indicates a left shift>3% may predict positive blood cultures
ITR and Neonatal Sepsis
11/2/2012
11
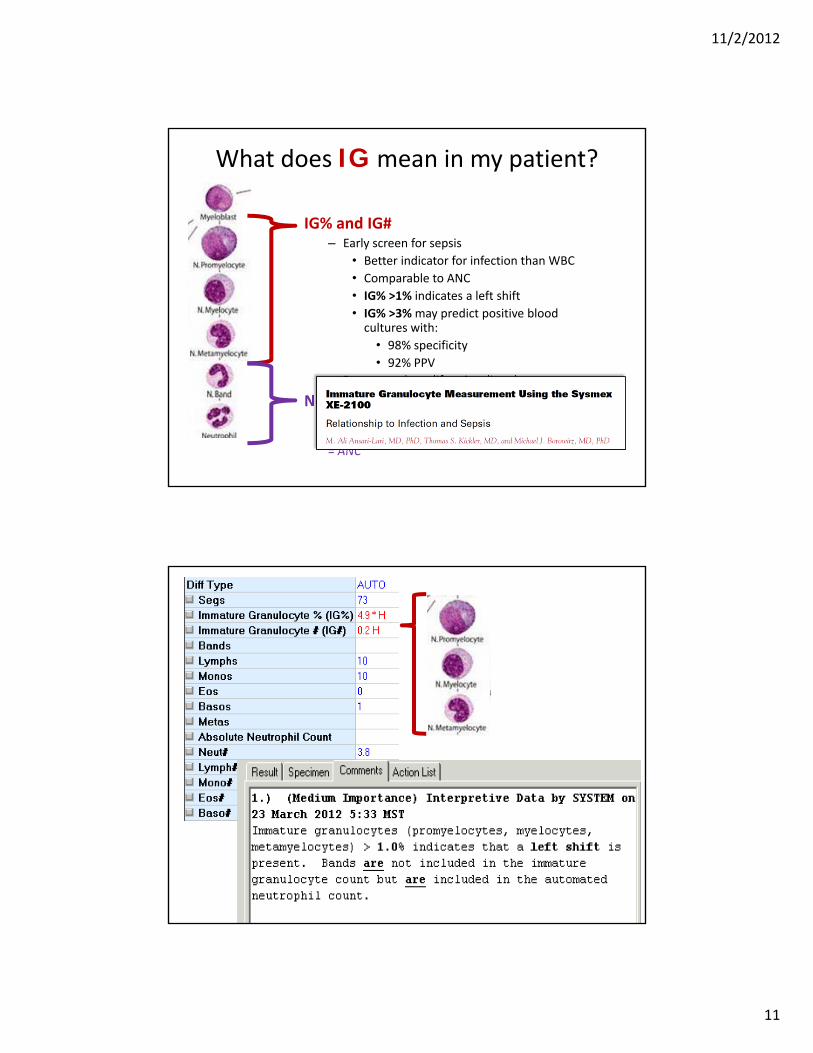
What does IG mean in my patient?
IG% and IG# – Early screen for sepsis
• Better indicator for infection than WBC
• Comparable to ANC
• IG% >1% indicates a left shift
• IG% >3% may predict positive blood cultures with:
• 98% specificity
• 92% PPV
– Detect myeloproliferative disorders
Neutrophil count includes bandsAutomated Neutrophil Count= Manual Absolute Neutrophil Count= ANC
11/2/2012
12
Published IG Studies
In‐House IG Studies
IG to help determine infection/sepsis1. Chart review of patients with Sepsis Alerts
• Patients with sepsis (True Positives)
• Patients without sepsis (True Negatives)
• Compare IG% to determine cut off values
2. Patients with positive blood cultures
• IG and ANC as an indicator for infection/sepsis (SIRS Criteria)
3. What to expect in various disease states, does IG indicate chorioamnionitis?
4. IG versus ITR in pediatric patients.
5. Does IG/ANC/Bands correlate to Procalcitonin?
11/2/2012
13
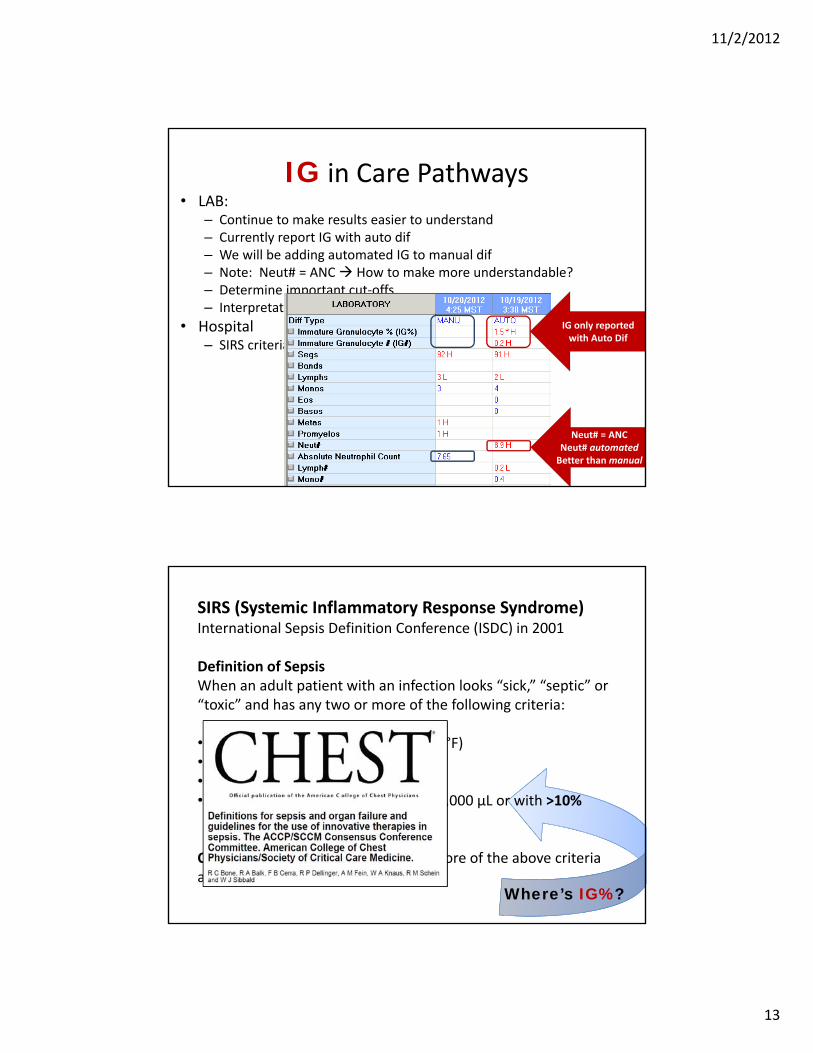
IG in Care Pathways• LAB:
– Continue to make results easier to understand– Currently report IG with auto dif– We will be adding automated IG to manual dif– Note: Neut# = ANC How to make more understandable?– Determine important cut‐offs– Interpretative messages
• Hospital– SIRS criteria
Where’s IG?
IG only reported with Auto Dif
Neut# = ANCNeut# automatedBetter than manual
Where’s IG%?
SIRS (Systemic Inflammatory Response Syndrome)International Sepsis Definition Conference (ISDC) in 2001
Definition of SepsisWhen an adult patient with an infection looks “sick,” “septic” or “toxic” and has any two or more of the following criteria:
• Fever ≥101°F or hypothermia (<96.8°F) • Heart rate >90 beats/minute • Respiration rate >20 breaths/minute • White blood count >12,000 µL or <4,000 μL or with >10% bands
Coding: CMS recognizes any two or more of the above criteria as indicative of sepsis
11/2/2012
14
International Sepsis Forumhttp://internationalsepsisforum.com/
Improving Sepsis Outcomes• Initiative to focus on management of patients with severe sepsis
• International consensus on the latest understanding of key scientific and clinical issues
• Data on patient management to improve outcomes• Findings need to be evaluated and incorporated into existing treatment protocols
• Disseminatie emerging practice guidelines to researchers, intensivists, and other critical care professionals worldwide.
International Sepsis Forumhttp://internationalsepsisforum.com/
We’re talking about themAre they talking about us?

11/2/2012
15
IG in Care Pathways
• LAB:– Report with auto and manual dif
– Determine important cut‐offs
– Interpretative messages
• Hospital– SIRS criteria– Computer alerts for sepsis
– Replace bands– Replace or modify ITR
IG Needs to be added
Immature Platelet Fraction
IPF
11/2/2012
16
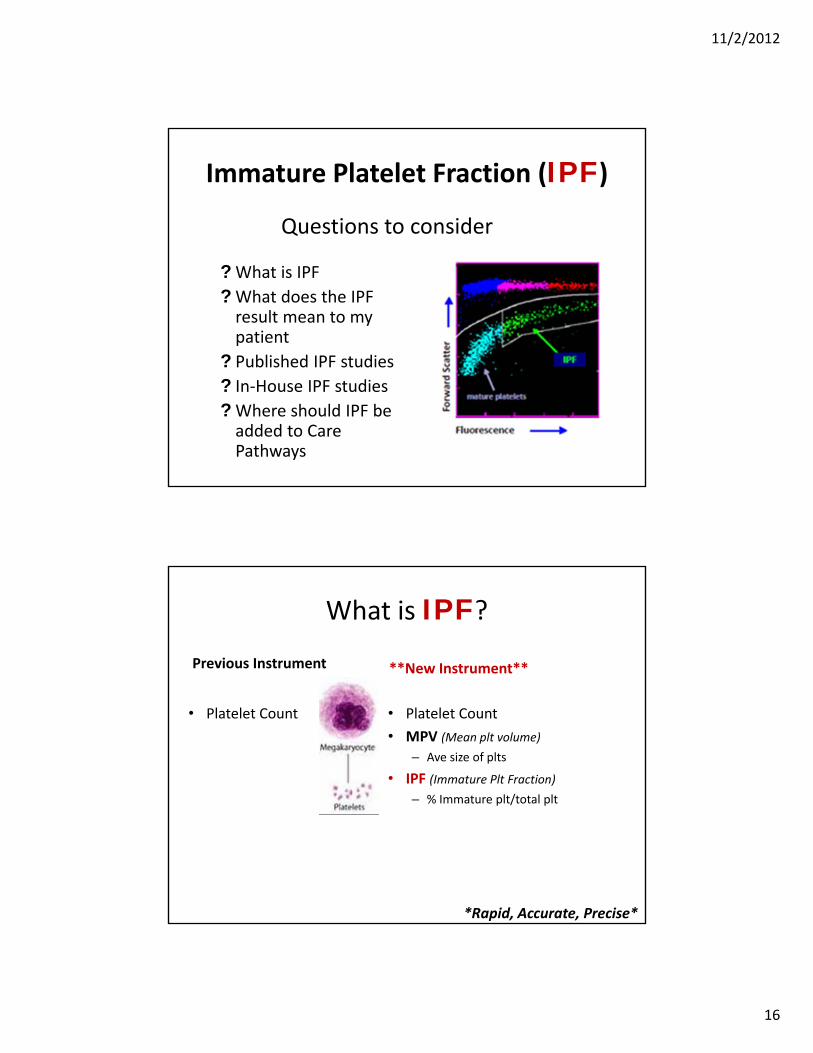
Immature Platelet Fraction (IPF)
Questions to consider
?What is IPF
?What does the IPF result mean to my patient
? Published IPF studies
? In‐House IPF studies
?Where should IPF be added to Care Pathways
What is IPF?Previous Instrument
• Platelet Count • Platelet Count
• MPV (Mean plt volume)
– Ave size of plts
• IPF (Immature Plt Fraction)
– % Immature plt/total plt
**New Instrument**
*Rapid, Accurate, Precise*
11/2/2012
17
What does IPF mean to my Patient?
↓ Plts + IPF = Production disorder
↓ Plts + IPF = Destruction mechanism or BM Recovery
• Evaluate mechanism causing thrombocytopenia
• IPF recovers ~3 days earlier than platelet count
• Predict platelet count recovery
• Determine need for platelet transfusion
Published IPF Studies
11/2/2012
18
In‐House IPF Studies
• Usefulness of IPF as a differential diagnosis of ITP/TTP
• IPF in transfusion practices• Determine if IPF impacts prophylactic platelet transfusions
• Determine how to include IPF in transfusion protocol
• IPF as an aid to avoid unnecessary bone marrow biopsies
• IPF to determine bone marrow recovery and avoid ordering of HLA typed products
IPF in Care Pathways
• LAB:– What PLT result to trigger reflex IPF testing?
• Started with 30,000• Changed to 50,000
– How to order IPF?• Orderable: Platelet count with IPF• Stand alone platelet count order will reflex to IPF
• Hospital– Evaluation of thrombocytopenia– Assess need for transfusion– Assess bone marrow recovery

11/2/2012
19
Reticulated Hemoglobin Equivalent
RET-He
Reticulated Hemoglobin Equivalent (RET-He)
? What is RET‐He? What does the RET‐He result mean to my patient
? Published RET‐He studies
? In‐House RET‐He studies
? Where should RET‐He be added to Care Pathways
Questions to consider
11/2/2012
20
What is RET-He?
• Retic # & Retic%
**New Instrument**
RETIC‐Comprehensive (3 part Retic)
1. Retic # & Rectic %
2. Immature Retic Fraction (IRF) – Quantitativemeasure of immature
retics
3. RET‐He– Qualitativemeasure of Hb in
reticulocytes
– Same test as Reticulocyte Hemoglobin Content (CHr)
– Not affected by uremia or inflammation
Previous Instrument
*Rapid, Accurate, Precise*
What does RET-He mean in my Patient?
• Same test as Reticulocyte Hemoglobin Content (CHr)
• Qualitativemeasure of Hb in reticulocytes.
• Cellular evaluation of iron status• Help diagnose iron deficiency
• Not affected by uremia or inflammation
• Faster response to treatment than routine iron tests• Monitor response to treatment more closely (3 days)
• Improve EPO usage by identifying non‐responders earlier

11/2/2012
21
Published RET-He Studies
In‐House RET-He Studies
• Economic value of screening for iron deficiency in children
• RBC Transfusion protocol – determine how to add RETIC‐Comprehensive (RET‐He)
• Economic value of screening for ID and IDA, medically treating prior to surgery and avoiding PRBC transfusion– Pre‐Op Anemia elective Ortho surgery
– Pre‐Op anemia screening in Cardiac valve cases
• Hospital patients: Evaluate RET‐He in EPO/Iron treatment– Identify Non‐Responders faster
– Adjust iron or EPO dosage
11/2/2012
22
RET-He in Care Pathways
• LAB:– How to order:
• Part of Reticulocyte Comprehensive Order• Not a stand alone order
– Reflex to RETIC‐Comprehensive (includes RET‐He) if• Hgb < 9.0 and MCV <78 • No Hgb order within 30 days
– How often should it be tested?
– Interpretative messages
• Hospital– Iron/Epo CareSet– Add to anemia algorthm– Pre‐operative work up for elective surgery
Automated Nucleated Red Blood Cells
NRBCs

11/2/2012
23
Automated Nucleated Red Blood Cells (NRBCs)
? What are Automated NRBCs? What does the Automated NRBCs result mean to my patient
? Published Automated NRBCs studies
? In‐House Automated NRBCs studies
? Where should Automated NRBCs be added to Care Pathways
Questions to consider
What are Automated NRBCs?Previous Instrument
• Flag for possible nRBCs
• Reflex to manual review– Manually count
nRBCs
– Manually correct WBC count
• Automated NRBCs– Instrument checks for NRBCs on
every patient
– Up front for ICU, Oncology, babies <30 days old
– Any CBC that flags possible NRBCs will reflex to rerun specimen for automated NRBC evaluation.
– Automatically corrects WBC count
**New Instrument**
*Rapid, Accurate, Precise*
11/2/2012
24
What do NRBCs mean to my Patient?
• One NRBC in an adult is important finding
• Indicates health of patient
• Changes in NRBCs important to follow
– New finding of NRBCs
– Increasing number of NRBCs
– Decreasing number of NRBCs
• Can use to help determine whether to move a patient into or out of the ICU
Published NRBCs Studies
11/2/2012
25
In‐House NRBCs Studies
• To be determined…
NRBCs in Care Pathways
• LAB:– How to order:
• Not a stand alone order• All patients evaluated for NRBCs
– Reflex • Automatically test
– Patient location: ICU, NICU and Oncology – Patient age <30 days– Corrected WBC reported with automated NRBC.
• Instrument flag: NRBC? – Rerun and report Automated NBRC and corrected WBC.
– Interpretative messages• Hospital
– Include in decision for transferring patients from ICU to floor
11/2/2012
26
Reach Out: Who to educate?
• Everyone!
– Lab: Pathologists and techs
– Clinical: Physicians, nursing, pharmacy
– Administration: CEOs, CMOs, CFOs, CNOs, Quality
– Groups: Functional Teams, Clinical Consensus Groups, Strategic Clinical Initiative Teams, Clinical Performance Groups, Discipline Teams
– Informatics: LIS and HIS
Reach Out: How to educate?
• Written material– Articles
– Handouts
– Table toppers
– SBAR
– Laboratory Memo
– Integrate into care pathways and caresets
– Interpretative messages in EMR
– Return On Investment (ROI)
Where’s LAB?
11/2/2012
27
Reach Out: How to educate?
• Talks– Sysmex Clinical Support in‐
house training sessions
– Webinars
– Lectures/In‐services
– Meetings: • Medical Executive
• Departments
• Repeat!
IG %Immature granulocytes (promyelocytes, myelocytes, metamyelocytes) > 1.0% indicates that a left shift is present. BANDS are included in the automated neutrophil count and not in the immature granulocyte count.
IPF %Low PLT + low IPF suggests a bone marrow production disorder.
Low PLT + high IPF suggests peripheral destruction (e.g. ITP, TTP, HIT, DIC, autoimmune) or bone marrow recovery. Trending of serial IPF measurements is recommended when evaluating for bone marrow response.
RET-HeAdults: The RET‐He threshold for defining iron deficiency in adults is < 29 pg. (KDOQI Guideline Changes).
Pediatrics: Less than 27.5 pg is indicative of iron deficiency.
IPFValues above normal range indicates an increase in RBC cellular response from bone marrow.
Interpretative Messages

11/2/2012
28
• Rapid growth in health care spending
– Now over 17% of GDP
– 30% of health care costs are generated by • Overuse
• Underuse
• Misuse
Connect with the Big Picture
Nace D, Gartland J. Providing accountability: accountable care concepts for providers. http://www.strategiestoperform.com/volume5_issue2/. McKesson/Relay Health white paper. Published 2011. Accessed March 14, 2012.
Connect with the Big Picture
• Most recent trend to – Restrain the growth in US health care spending
– Improve quality of care
– Improve health care outcomes
• Coordinated care systems in which – Providers are incentivized based on outcomes, not number of services
– The Affordable Care Act allows for the establishment of ACOs within Medicare and in the private sector
• How do the Lab and Pathologists fit in this model?
Accountable Care Organization (ACOs)
11/2/2012
29
Pathologists/Lab must share accountability for the larger process
• Extend beyond traditional boundaries
• Engage in activities that improve clinical outcomes
• Special knowledge to contribute– Designing clinical pathways– Informatics and communication tools
– Improve clinical performance
Connect with the Big Picture

11/2/2012
30
Geisinger Health Systems:Role of the pathologist in improving laboratory clinical effectiveness
Banner Health/LSA/PSA
Sharing accountability for patient outcomes and performance of the health care system
Establishing and using a standardized laboratory database for outcomes research and health care improvement
Participating in design of standardized practice algorithms for things such as laboratory test ordering, test interpretation, and therapeutic recommendations
Developing patient health information tools that are designed to improve patient care
Extending laboratory reporting to include improvements in how the data are presented to clinicians as well as clinical recommendations
Montefiore Medical Center: Model of How Pathologists Add Value
Banner Health/LSA/PSA
Working with clinical colleagues to optimize testing protocols
Reducing unnecessary testing in both clinical and anatomic pathology
Applying personalized therapy to help guide treatment
Designing laboratory systems to allow quick data mining by pathologists and clinicians
Administering cost‐effective laboratories
11/2/2012
31
Greater collaboration with other clinicians • Pathologist/Lab leadership
• Collaboration with other physicians and ACO leaders
• Rectify lack of understanding:– Analytic role and expertise of pathologists not appreciated
– Pathologists know most effective applications of laboratory medicine
• Pathologists/Lab easily overlooked during the development of ACOs
• Pathologists/Lab should proactively assert their ability to help the ACO meet its goals
Connect with the Big Picture
How to pay for pathologist contributions?• Traditional fee‐for‐service model not appropriate • Adoption of guidelines may decrease the volume of laboratory tests
• And decrease income derived from fee‐for‐service payments
• Pathologists/Lab add value• Not to specific patients• To the development of systems and guidelines that globally reduce costs and potentially improve patient care
Connect with the Big Picture
11/2/2012
32
What’s Next?• Lab
– Continue education– Continue to evaluate when to reflex tests– Determine best work flow for Lab and Physicians
• Hospital– Continue education– Work on Care Pathways and Order Caresets
• Anemia• Transfusions • Infection/Sepsis
– Studies to determine how to best utilize tests– Report improvements to administration and physicians
• Blood Service Provider– United Blood Services: incorporate RET‐He blood donor testing
• International Sepsis Forum– Need to incorporate IG into SIRS criteria
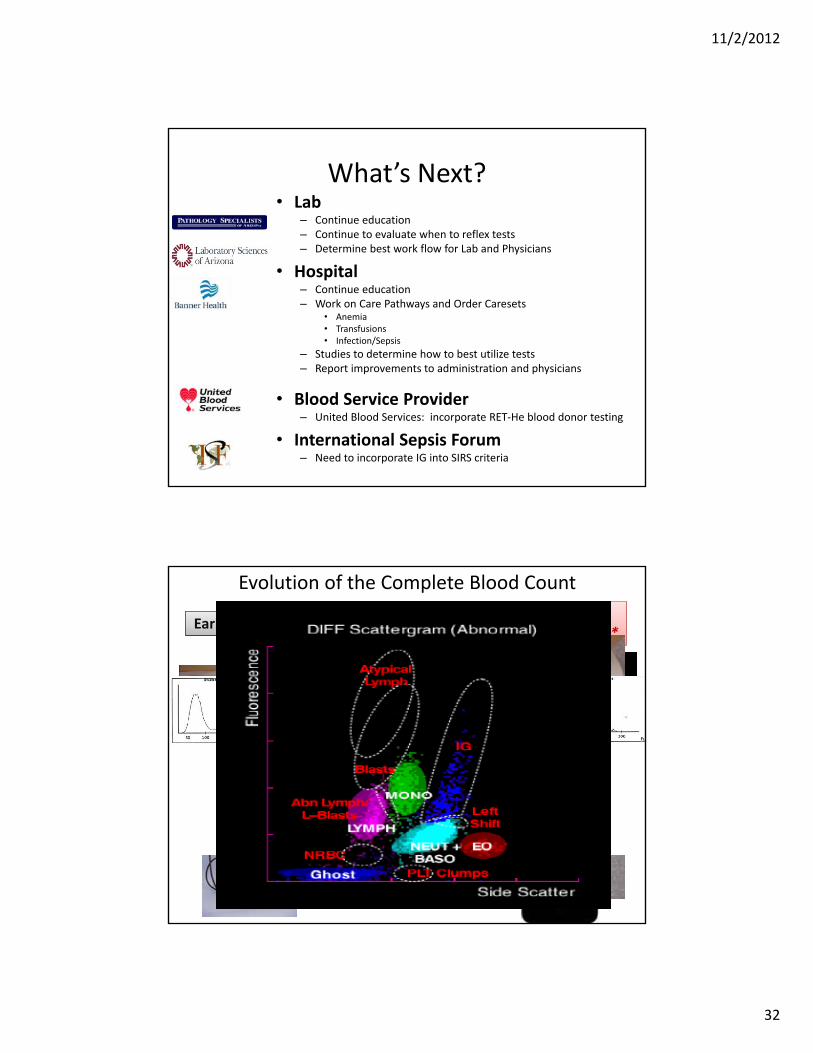
Early TechnologyUpdated
Technology**Cutting Edge
Technology**
Evolution of the Complete Blood Count
11/2/2012
33
Questions?


















