
The Role of Shape and Weight in Self-Concept: The Shape...
20
Cognitive Therapy and Research, Vol. 21, No. 1, 1997, pp. 5-24 The Role of Shape and Weight in Self-Concept: The Shape and Weight Based Self-Esteem Inventory 1 Josie Geller, Charlotte Johnston, 2 and Kellianne Madsen University of British Columbia The purpose of this study was to establish the psychometric properties of the Shape and Weight Based Self-Esteem (SAWBS) Inventory, a newly-developed measure of the influence of shape and weight on feelings of self-worth. The results from a nonclinical sample of young women indicated that SAWBS scores were stable over time (N = 24), and correlated moderately with one of two measures of shape and weight schemata (N = 50). In a sample of 84 women, SAWBS scores also correlated moderately with two measures of eating disorder symptomatology, and in regression analyses contributed statistically significant unique variances to both measures of symptomatology, even after the effects of body mass index, depression, and global self-esteem were controlled. Finally, SAWBS scores discriminated between women reporting few or no disturbed eating symptoms and possible/probable eating disorder cases. In sum, the SAWBS Inventory is a reliable and valid measure, and may be a useful tool in the assessment of eating disorders. 1 Support for this research was provided by a Studentship award from the Medical Research Council of Canada to Josie Geller, M.A., clinical psychology doctoral candidate at the University of Bristish Columbia (UBC). Charlotte Johnston, Ph.D., is Associate Professor in the Department of Psychology at UBC. Kellianne Madsen is a Research Assistant in the Department of Psychology at UBC. 2 Address all correspondence, including requests for reprints, to Charlotte Johnston, Department of Psychology, University of British Columbia, Vancouver, BC, Canada V6T 1Z4. KEY WORDS: eating disorders; self-esteem. 5 0147-5916/97/0200-0005$12.50/0 C 1997 Plenum Publishing Corporation
Transcript of The Role of Shape and Weight in Self-Concept: The Shape...

Cognitive Therapy and Research, Vol. 21, No. 1, 1997, pp. 5-24
The Role of Shape and Weight in Self-Concept:The Shape and Weight Based Self-EsteemInventory1
Josie Geller, Charlotte Johnston,2 and Kellianne MadsenUniversity of British Columbia
The purpose of this study was to establish the psychometric properties of theShape and Weight Based Self-Esteem (SAWBS) Inventory, a newly-developedmeasure of the influence of shape and weight on feelings of self-worth. Theresults from a nonclinical sample of young women indicated that SAWBSscores were stable over time (N = 24), and correlated moderately with one oftwo measures of shape and weight schemata (N = 50). In a sample of 84women, SAWBS scores also correlated moderately with two measures of eatingdisorder symptomatology, and in regression analyses contributed statisticallysignificant unique variances to both measures of symptomatology, even afterthe effects of body mass index, depression, and global self-esteem werecontrolled. Finally, SAWBS scores discriminated between women reporting fewor no disturbed eating symptoms and possible/probable eating disorder cases.In sum, the SAWBS Inventory is a reliable and valid measure, and may be auseful tool in the assessment of eating disorders.
1Support for this research was provided by a Studentship award from the Medical ResearchCouncil of Canada to Josie Geller, M.A., clinical psychology doctoral candidate at theUniversity of Bristish Columbia (UBC). Charlotte Johnston, Ph.D., is Associate Professor inthe Department of Psychology at UBC. Kellianne Madsen is a Research Assistant in theDepartment of Psychology at UBC.
2Address all correspondence, including requests for reprints, to Charlotte Johnston,Department of Psychology, University of British Columbia, Vancouver, BC, Canada V6T1Z4.
KEY WORDS: eating disorders; self-esteem.
5
0147-5916/97/0200-0005$12.50/0 C 1997 Plenum Publishing Corporation

Recently, researchers have attempted to understand the eating disorderswithin the context of structural models of the self. Vitousek and Hollon(1990), for instance, proposed that the core psychopathology of the eatingdisorders may be represented in cognitive schemata that unite views of theself with beliefs about shape and weight. Such conceptual models maintainthat shape and weight concerns are not merely salient to eating disorderedindividuals, but rather have a central influence (positive or negative) onfeelings of self-worth. In support of this view, Cooper and Fairburn (1993)recently proposed that overvalued ideas about shape and weight, or theextent to which self-worth is judged in terms of shape and weight, constitutethe "central cognitive substrate" of bulimia (p. 386). This linking of shapeand weight to self-esteem in the eating disorders is also reflected in recentchanges to the Diagnostic and Statistical Manual of Mental Disorders(DSM). In the fourth edition of DSM (DSM-IV), the new criterion "self-evaluation is unduly influenced by shape and weight" (American PsychiatricAssociation, 1994, pp. 545 and 550) has been accorded central status inthe diagnosis of bulimia nervosa, and is one of three possible componentsof a criterion for anorexia nervosa [the other two are "disturbance in theway in which one's body weight or shape is experienced" and "denial ofthe seriousness of the current low body weight" (p. 54)].
Although a number of self-report measures have been developed toaddress the importance of shape and weight concerns to individuals whohave eating disorders (see Ben-Tbvim & Walker, 1991, for a review), manyof these lack specificity, in that they assess multiple dimensions (e.g., evalu-ations, perceptions, and feelings about the body) within a single scale orinstrument. In addition, these measures do not assess the importance ofshape and weight within the context of other dimensions upon which self-esteem is based. The Eating Disorders Examination (EDE; Cooper & Fair-burn, 1987), a structured interview for diagnosing eating disorders, is anotable exception in that it contains two single-item scales that assess theextent to which self-esteem is based on shape and weight, respectively. Un-fortunately, administration of the full interview requires at least 1 hour witha skilled interviewer, and the validity of the two items, taken out of thecontext of the remainder of the interview, has not been established. As aresult, the EDE may not be practical for research or clinical purposes whentime and/or resources are limited. In sum, there is a need for a specific,and easily administrable measure that assesses the extent to which self-es-teem is based on shape and weight. The purpose of the present study wasto develop a measure that met these needs; the Shape and Weight BasedSelf-Esteem (SAWBS) Inventory, and to determine the stability, as well asthe concurrent, discriminant, and predictive validities of SAWBS scores.
6 Geller, Johnston, and Madsen

The SAWBS Inventory is an innovative and easy-to-administer meas-ure of the structure of self-esteem, developed to assess the contribution ofshape and weight, in the context of other dimensions, to overall feelingsof self-worth. In the SAWBS Inventory, individuals select and rank orderfrom a list of attributes those that are important to their feelings of self-worth, and then divide a circle into pieces, such that the size of each piecereflects the importance of each attribute to overall feelings of self-worth.The unique design of the SAWBS Inventory allows for the relative contri-bution of shape and weight to overall feelings of self-esteem to be objec-tively assessed, in the context of other dimensions upon which self-esteemis based. As a first step toward the validation of this new instrument, theproperties of the SAWBS Inventory were investigated in a sample of un-dergraduate women. Female undergraduates were considered a suitablepopulation for this study because a range of eating-disordered attitudesand behaviors has been reported in such samples, and risk in such groupshas been judged to be high (e.g., Klemchuk, Hutchinson, & Frank, 1990;Klesges, Beatty, & Berry, 1985; Vanderheyden, Fekken, & Boland, 1988).
With regards to stability of SAWBS scores, given that overvalued ideasabout shape and weight are purported to be relatively enduring over time(Cooper & Fairburn, 1993), it was hypothesized that SAWBS scores as-sessed 1 week apart would be significantly and highly correlated. Althoughone would expect shape- and weight-based self-esteem to be stable overmuch longer periods of time, 1 week was considered to be a minimal test-retest interval for this study, and chosen as a compromise with the practicallimitations of this study.
Three types of concurrent validity of SAWBS scores were investigated.First, shape- and weight-based self-esteem was predicted to be related toindividuals' perceptions of their own shapes and weights. It is importantto note that shape- and weight-based self-esteem is not a measure of posi-tive or negative feelings about the body, but rather of the extent to whichfeelings of self-worth are based on the body. However, given that shape-and weight-based self-esteem is a diagnostic criterion for eating disorders,and individuals who have eating disorders report high body dissatisfaction(e.g., Hsu & Sobkiewicz, 1989), it was hypothesized that higher SAWBSscores would be associated with the tendency to view oneself as more over-weight and one's shape as less attractive.
Next, the relationship between SAWBS scores and eating disordersymptomatology was investigated. Again, because an undue influence ofshape and weight on self-esteem is described as a necessary and uniquefeature of the eating disorders, it was hypothesized that SAWBS scoreswould be positively related to disturbed eating patterns. Furthermore, toexamine whether shape- and weight-based self-esteem accounts for a
The SAWBS Inventory 7

unique aspect of eating disorder symptomatology, independent from globalself-esteem and depression [two constructs that are not eating disorder-specific, but that are frequently associated with eating disorder symptoma-tology (e.g., Hsu, 1982; Kaplan, Busner, & Pollack, 1988)], the relationshipbetween SAWBS scores and eating disorder symptomatology was examinedcontrolling for the effects of depression and global self-esteem.
Finally, given that views of the self are closely tied to cognitive sche-mata (e.g., Markus, 1977), it was hypothesized that shape- and weight-basedself-esteem would be related to the extent to which shape- and weight-basedschemata influence individuals' information processing styles on two meas-ures of cognitive processing. Shape, weight, and food-related schemata havebeen widely investigated in the eating disorders using Stroop (1935) color-naming interference paradigms. A number of studies have shown that, rela-tive to women who do not have eating disorders, women who have eatingdisorders take longer to color-name eating disorder-related target words(e.g., cakes, diet, and hips) than control words (e.g., Cooper, Anastasiades& Fairburn, 1992; Cooper & Fairburn, 1992). However, a number of incon-sistencies in work using the Stroop paradigm have been noted. Ben-Tbvim,Walker, Fok, and Yap (1989) found that when shape and weight words werepresented separately (without food words), color-naming interference wassignificantly reduced, reaching statistical significance only in bulimic, andnot anorexic, subjects. In addition, the occurrence of Stroop effects in sub-clinical populations has been inconsistent, with some authors finding sucheffects (e.g., Green & Rogers, 1993), and others not (e.g., Cooper & Fair-burn, 1992). Finally, the Stroop task has been shown to be susceptible topriming influences, which can significantly affect the sensitivity of this task(e.g., Warren, 1974). Although not yet applied to the eating disorders, asecond, perhaps more promising, methodology for the assessment of cogni-tive schemata involves the false recall of schema-consistent words in falsealarm effect (FAE) paradigms (e.g., Rogers, Rogers, & Kuiper, 1979). Inthis task, participants are presented with a list containing both schema wordsthey have previously seen, as well as new schema-consistent words. The taskis to identify the words that were presented in the previous list only. Theincorrect identification of schema-consistent words has been related to theextent to which the individual is schematic along that dimension (e.g.,Mathews & MacLeod, 1983; Rogers et al., 1979). In sum, Stroop paradigmresearch suggests that women who have eating disorders may selectivelyprocess information related to eating, weight, and shape, and supports theidea that elaborated cognitive schemata representing these categories of in-formation are characteristic of eating disorders. The false alarm effect para-digm is a possible methodology for future cognitive research with the eatingdisorders, and may be an attractive alternative to Stroop paradigm research,
8 Geller, Johnston, and Madsen

given some of the shortcomings that have been identified in this method.In the present study, it was hypothesized that shape- and weight-based self-esteem would be related to the extent to which shape- and weight-basedschemata influence individuals' responding on the Stroop and FAE tasks.
Finally, with regard to predictive validity, the ability of SAWBS scoresto discriminate between women who have an eating disorder and womenwho do not have an eating disorder has implications for the utility of theSAWBS Inventory as a screening instrument. In this study, the ability ofshape- and weight-based self-esteem to discriminate between probable andpossible eating disorder cases, and individuals not expected to have an eatingdisorder were therefore examined. It was hypothesized that SAWBS scoreswould be higher in the group identified as probable and possible cases.
With regard to discriminant validity, because shape- and weight-basedself-esteem is the extent to which feelings of self-worth are based uponshape and weight, and not a measure of actual shape and weight, SAWBSscores were not expected to be correlated with body mass index (BMI). Itwas also hypothesized that SAWBS scores would not be associated withthe tendency to respond in a socially sanctioned manner, or to family so-cioeconomic status.
METHOD
Subjects
One hundred and ten female undergraduate students between theages of 18 and 45 years (M = 21.2, SD = 6.6) participated in a study onwomen's attitudes and self-perceptions in exchange for course credit. Fifty-two (48%) of the women described their ethnic background as Europeanor Anglo Saxon, 33 (31%) as Asian, 5 (5%) as Indo-Canadian, and onewoman (1%) described herself as African. Seventeen (16%) women eitherfailed to respond to this question or gave uncodable responses (e.g., "Ca-nadian"). Most of the women (91%) indicated that they were raised intwo-parent families. Family socioeconomic status ranged from 1 to 5 onthe Hollingshead Four-Factor Index (Hollingshead, 1975), with a mean of2.3 (SD = 1.0), indicating upper middle class.
Measures
Shape and Weight Based Self-Esteem Inventory. In the SAWBS Inven-tory, individuals select from a number of personal attributes those that are
The SAWBS Inventory 9

important to how they have felt about themselves in the past 4 weeks. Thelist of personal attributes was generated from previous measures that haveidentified specific dimensions of self-esteem (Harter, 1993; Marsh, 1986,1993; O'Brien, 1980). Several possible personal attributes were initially pi-lot-tested on female graduate students, who provided suggestions regardingthe relevance of the attributes for young women. The final list of attributesincluded intimate or romantic relationships, body shape and weight, com-petence at school/work, personality, friendships, face, personal develop-ment, competence at activities other than school/work, and other(individuals are asked to list an attribute if it is not covered in the precedinglist). After selecting the personal attributes that are important to how theyfeel about themselves, individuals rank-order the attributes in terms of howmuch their opinion of themselves is based on each. Then, they divide acircle into pieces, such that the size of each piece reflects how much theirself-opinion is based on each of the ranked attributes. Thus constructed,the SAWBS Inventory has the advantage of measuring the relative contri-bution of shape and weight attributes to overall self-esteem. The SAWBSscore is the angle of the shape and weight piece of the circle3.
Eating Disorders Inventory (EDI). The EDI (Garner & Olmstead,1984; Garner, Olmstead, & Polivy, 1983) is a 64-item self-report scale de-signed to measure attitudes, personality features, and eating disorder symp-toms thought to be relevant to anorexia nervosa and bulimia nervosa.Subjects are asked to rate each item on a 6-point scale ranging from neverto always. The EDI was constructed to have eight independent subscales(Garner et al., 1983). Some of these assess personality factors thought tobe associated with the eating disorders (i.e., Perfectionism, InterpersonalDistrust), and some assess behaviors that are more directly tied to eatingdisorder symptomatology (i.e., Drive for Thinness, Bulimia). A factor analy-sis in a nonclinical sample revealed that three of the scales (Drive for Thin-ness, Bulimia, and Body Dissatisfaction) loaded on the same factor tappinga general concern with shape, weight, and eating, and this factor was rec-ommended as a screening measure of eating disorder symptoms (Welch,Hall, & Walkey, 1988). Accordingly, in this study, the sum of the Drive forThinness, Body Dissatisfaction, and Bulimia subscales was used to measureseverity of eating disorder symptomatology4. Scores on this composite scalecan range from 0 to 69, with higher scores corresponding to higher levelsof eating disorder symptomatology.
3Copies of the SAWBS Inventory can be obtained from the second author at University ofBritish Columbia, Department of Psychology, 2136 West Mall, Vancouver BC, V6T 1Z4,Canada.
4All analyses were completed with the three EDI scales separately, and an identical patternof results was obtained.
10 Geller, Johnston, and Madsen

Beck Depression Inventory (BDI), The BDI (Beck, Ward, Mendelson,Mock, & Erbaugh, 1961) is a 21-item self-report questionnaire assessingdepressive symptoms. This measure has demonstrated good internal con-sistency, test-retest reliability, and concurrent validity (Beck, Steer, & Gar-bin, 1988). Scores can range from 0 to 63, with higher scores correspondingto more depressed mood.
General Information Sheet. Designed for this study, this form askedeach woman to provide her date of birth, year of study, faculty, major,family situation (two-parent family, one-parent family, step-family, or"other"), parents' occupations and educations, ethnic background, andheight and weight. Parents' occupations and educations were used to de-termine family socioeconomic status (Hollingshead, 1975), and height andweight were used to calculate BMI. Women also rated the extent to whichthey felt they had an attractive shape (on a 7-point scale ranging from notat all attractive to extremely attractive) and rated how they felt about theirweight (on a 7-point scale ranging from extremely overweight to extremelyunderweight). These variables were used to describe the sample and wereexplored as possible correlates of SAWBS scores.
Stroop Task. Two word cards (18 x 25 cm) and one practice card (9x 10 cm) were used. The word cards consisted of 12 stimulus words re-peated five times. The words were printed in block capitals (4 mm inheight) in one of six colors of ink; red, yellow, green, blue, black, or grey.The words were presented in random order in 12 rows of 6. On the shapeand weight card, the words were stomach, shape, buttocks, weight, thighs,hips, fat, obese, flabby, thin, firm, and slim. Each word on the shape andweight card was matched to a control word on the basis of first letter, wordfrequency, and, when possible, word length. The control words were soldier,seven, bribe, welcome, theatre, helm, folk, orchard, fired, thorn, farms, andshoe. The control card was constructed in the same way as the shape andweight card. A practice card was designed for subjects to familiarize them-selves with the ink colors and the color-naming task. This was a smallercard in which the capital letter o was printed in the six colors, in randomorder, in three columns of six.
Instructions for the Stroop informed participants that the task in-volved naming the colors of words each of which was printed in a differentcolored ink. Subjects were shown the practice card, the experimenter iden-tified the six ink colors, and subjects were instructed to name the colorsby placing their finger below each word prior to naming its color. Subjectswere then asked to name the colors of the words printed on the word cardsas quickly as possible, and to correct any mistakes as they occurred. Theexperimenter measured the tune taken to color-name the words on eachof the word cards using a hand-held stop watch. The order of presentation
The SAWBS Inventory 11

of the two word cards was counterbalanced across subjects. The Stroopinterference score is the difference between the time taken to color-namethe shape and weight words and the time taken to color-name the controlwords.
Word Recognition Task. For this task, the 24 words used in the Strooptask (12 shape and weight, and 12 control) were presented on a sheet ofpaper, randomly interspersed with 24 distractor words (also 12 shape andweight, 12 control). Each distractor word was matched to a target word onthe basis of word length, word meaning and structure, and, when possible,first letter and word frequency. The 12 shape and weight distractor wordswere bottom, rotund, pelvis, figure, fat, hard, waist, curves, round, tummy,chubby, and trim. The 12 control distractor words were orange, eleven, held,ranch, salute, sailor, clan, sole, discharged, sliver, bait, and movie. Participantswere instructed to read through the word list and indicate which wordsthey had seen on the previous two cards (target words). The false alarmeffect score was the number of shape and weight distractor words that wereincorrectly identified as target words. FAE scores can range from 0 to 12.
Short Marlowe-Crowne Social Desirability Scale [M-C 1(10)]. The M-C1(10) (Strahan & Gerbasi, 1972) is a 10-item, true-false measure of thetendency to respond in a socially sanctioned manner. The scale has shownmoderate internal consistency and correlates highly with the longer versionof this measure (Strahan & Gerbasi, 1972). Scores on this measure canrange from 0 to 10, with higher scores corresponding to a greater tendencyto respond in a socially sanctioned manner.
Rosenberg Self-Esteem Scale (RSES). The RSES (Rosenberg, 1979) isa self-report questionnaire composed of 10 items that assess global attitudestoward the self. Individuals rate the extent to which statements are descrip-tive of them on a 5-point Likert scale ranging from not at all descriptive ofme to very descriptive of me. The RSES has been shown to have strongconstruct, convergent, and discriminant validity (Rosenberg, 1979; Wylie,1989). It correlates with other measures of self-esteem, as well as with peerratings (Demo, 1985). Scores on the RSES can range from 10 to 50, withhigher scores corresponding to higher levels of self-esteem.
Health Information Questionnaire (HIQ). This measure was designedfor this study to assess the presence and severity of disturbed eating prac-tices. The HIQ is based on DSM-IV eating disorders criteria (APA, 1994)and other self-report surveys developed for assessing eating disorder symp-tomatology (Greenfeld, Quinlan, Harding, Glass, & Bliss, 1987; Kagan &Squires, 1983; Whitaker et al., 1989). It assesses recent weight history, men-strual history, fear of weight gain, worries about eating habits, and presenceand severity of binge eating, perceived lack of control over eating, and sixcompensatory behaviors (excessive exercise, fasting, use of diet pills, use
12 Geller, Johnston, and Madsen

of diuretics or water pills, vomiting, and use of laxatives). The responsescales were designed to assess DSM-IV threshold criteria, as well as sub-threshold levels of severity for binge eating and all relevant compensatorybehaviors. The HIQ yields a total disturbed eating score ranging from 0to 69, with higher scores corresponding to more eating disorder sympto-matology.
Procedure
Fifty of the women completed, in the following order, the SAWBSInventory, the Stroop color-naming task followed by the word-recognitiontask, the EDI, the BDI, and a General Information Sheet. Although itwas anticipated that completing the SAWBS Inventory prior to performingthe Stroop task might prime participants for shape and weight words, thisorder was nevertheless considered more desirable than having SAWBS In-ventory responses biased by prior presentation of the Stroop, or indeedof any other measure. Therefore, because it was our goal to minimize biasin responses to the SAWBS Inventory, possible compromise to the sensi-tivity of the Stroop task was tolerated. Based on an a priori decision thata sample of 20 would be sufficient to test the stability of the SAWBSInventory, women were invited to return for retest 1 week later until thisnumber was reached. Forty women were asked back in order to get asample of 24 (60%) to agree to return. These 24 women completed theSAWBS Inventory a second time, as well as the additional questionnairepacket described below.
Sixty other women participated on only one occasion and did notcomplete the Stroop or word recognition task. These women completed aquestionnaire packet that included, in the following order, a General In-formation Sheet, the SAWBS Inventory, the BDI, the EDI, the M-C 1(10),the RSES, and the HIQ. As part of a larger study, these subjects also com-pleted five other measures assessing health-related perceptions, beliefs, andbehaviors. Two of these measures were placed at the end of the question-naire packet and therefore did not influence responses to the other ques-tionnaires. The other three measures were completed after the SAWBSInventory. In summary, a sample of 50 women completed the SAWBS In-ventory, the cognitive tasks, BDI, and EDI. Twenty-four provided test-re-test data for the SAWBS. Eighty-four women completed the SAWBS, EDI,BDI, social desirability measure, and the HIQ (24 of these women com-pleted these measures as part of the SAWBS retest).
The SAWBS Inventoiy 13

14 Geller, Johnston, and Madsen
RESULTS
Description of Sample
In the 84 women who completed the larger questionnaire package,EDI Drive for Thinness, Bulimia, and Body Dissatisfation mean subscalescores were within the nonclinical range, and were similar to values re-ported in other university samples (e.g., Klemchuk et al., 1990; Vanderhey-den et al., 1988). However, also similar to previous research (e.g., Klemchuket al., 1990), a wide range of eating disorder symptoms was reported, anda clinical-level pathology was evident in some women. For instance, on theHIQ, 20% of the women stated that they felt afraid to eat for fear of weightgain "often" or "all the time," and 12% indicated that they binge-ate twoor more times a week. The percentage of women who reported that theyhad fasted, used diuretics, vomited, or used laxatives at least once permonth in order to get rid of unwanted calories was 7%, 1%, 6%, and 5%,respectively.
Using the HIQ items that assessed specific DSM-IV (APA, 1994)eating disorder criteria, three individuals from the sample met the behav-ioral criteria for bulimia nervosa (i.e., the occurrence of both binge-eatingepisodes and compensatory behaviors two or more times per week), andwere identified as probable cases. An additional seven participants met cri-teria for one behavioral category (e.g., binge eating), but were subthresholdon one or more other categories (e.g., used self-induced vomiting, but onlyonce per week). These individuals were identified as possible cases. BMIscores in this sample ranged from 17.0 to 40.5, with a mean of 21.7 (SD= 3.1), which is within the range associated with the lowest risk of illnessfor most people (Health and Welfare Canada, 1988). Table I providesmeans and standard deviations on the HIQ, as well as of participants' Per-ceived Weight and Shape, BMI, EDI composite, BDI, and RSES scores.
Properties of the SAWBS Inventory
In dividing the self-esteem circle, the 110 women in this study usedbetween two and eight pieces (attributes), with a mean of 5.5 pieces. TheSAWBS score, or the angle of the shape and weight piece, ranged from 0to 230°, with a mean angle of 58°. Looking at the rankings of shape andweight compared with other attributes, 9 (11.9%) of the 84 women rankedshape and weight most important to their feelings of self-worth, 16 (19.0%)ranked shape and weight second, 19 (22.6%) third, 8 (9.5%) fourth, 8(9.5%) fifth, 6 (7.1%) sixth, 4 (4.8%) seventh, and 14 (16.7%) women did
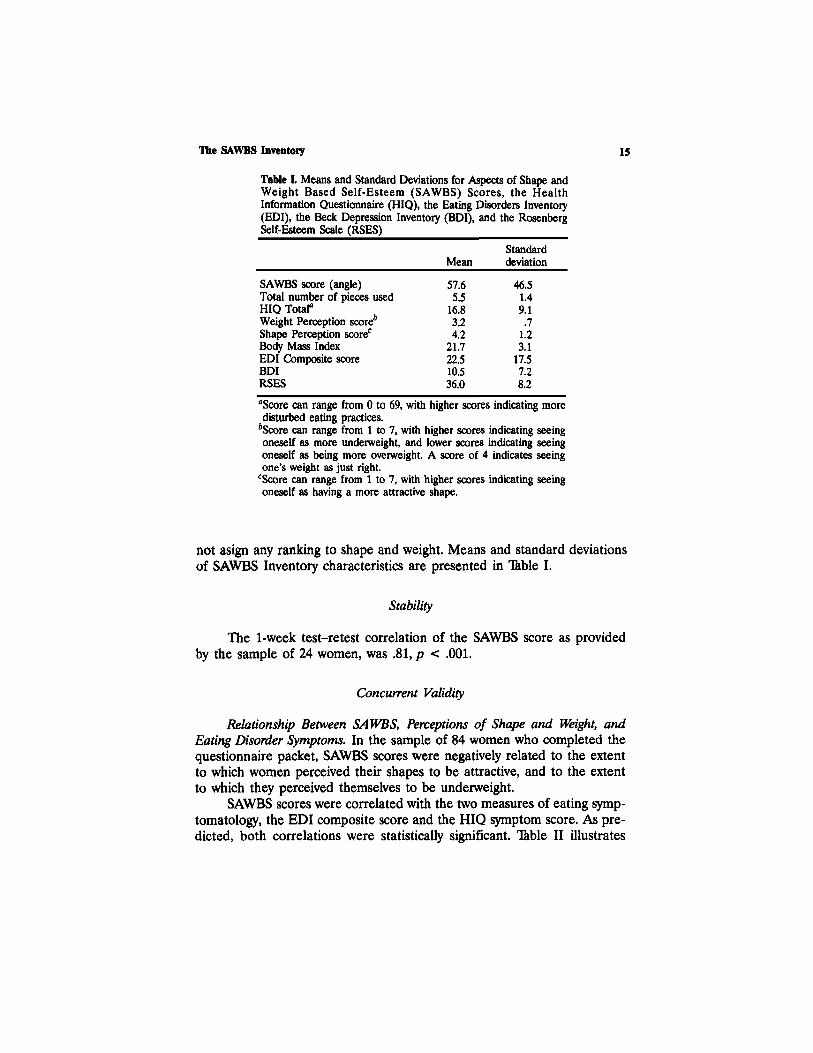
Table L Means and Standard Deviations for Aspects of Shape andWeight Based Self-Esteem (SAWBS) Scores, the HealthInformation Questionnaire (HIQ), the Eating Disorders Inventory(EDI), the Beck Depression Inventory (BDI), and the RosenbergSelf-Esteem Scale (RSES)
SAWBS score (angle)Total number of pieces usedHIQ Totala
Weight Perception score*Shape Perception scorec
Body Mass IndexEDI Composite scoreBDIRSES
Mean
57.65.5
16.83.24.2
21.722.510.536.0
Standarddeviation
46.51.49.1.7
1.23.1
17.57.28.2
aScore can range from 0 to 69, with higher scores indicating moredisturbed eating practices.
bScore can range from 1 to 7, with higher scores indicating seeingoneself as more underweight, and lower scores indicating seeingoneself as being more overweight. A score of 4 indicates seeingone's weight as just right.
cScore can range from 1 to 7, with higher scores indicating seeingoneself as having a more attractive shape.
not asign any ranking to shape and weight. Means and standard deviationsof SAWBS Inventory characteristics are presented in Table I.
Stability
The 1-week test-retest correlation of the SAWBS score as providedby the sample of 24 women, was .81, p < .001.
Concurrent Validity
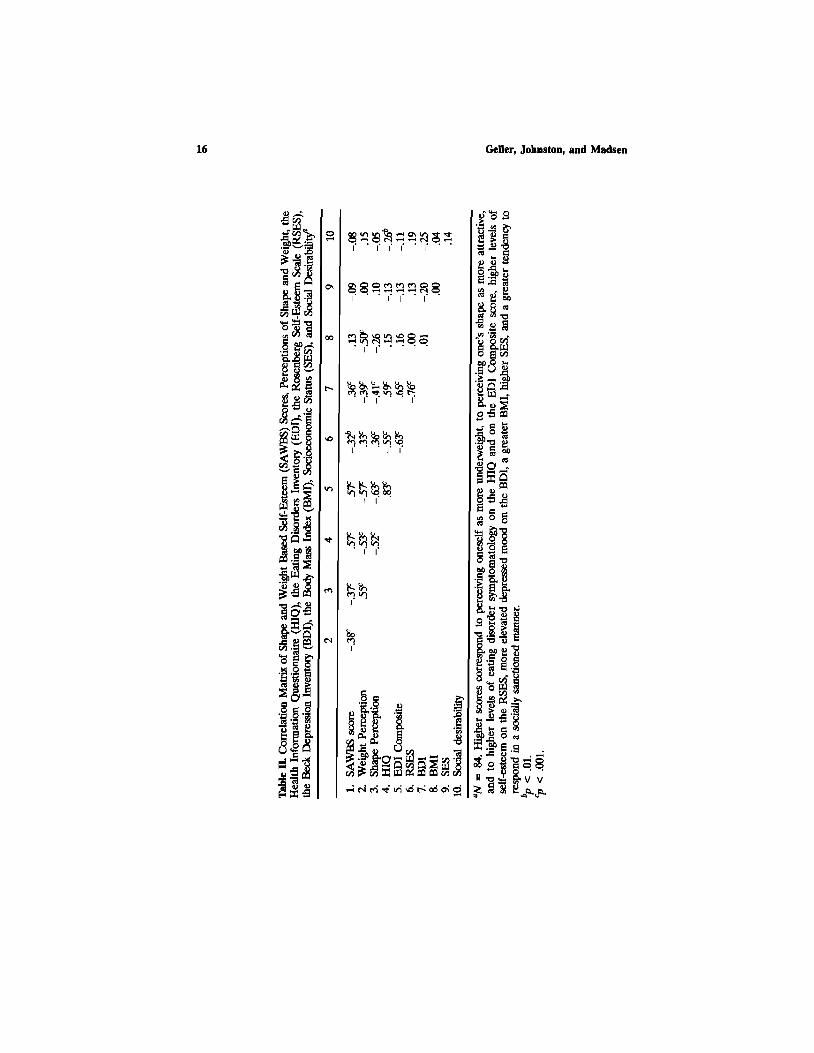
Relationship Between SAWBS, Perceptions of Shape and Weight, andEating Disorder Symptoms. In the sample of 84 women who completed thequestionnaire packet, SAWBS scores were negatively related to the extentto which women perceived their shapes to be attractive, and to the extentto which they perceived themselves to be underweight.
SAWBS scores were correlated with the two measures of eating symp-tomatology, the EDI composite score and the HIQ symptom score. As pre-dicted, both correlations were statistically significant. Table II illustrates
The SAWBS Inventory 15
16 Geller, Johnston, and Madsen

Table III. Regression Analysis with Body Mass Index (BMI), Beck DepressionInventory (BDI), and Rosenberg Self-Esteem Scale (RSES) Scores asIndependent Predictors of Eating Disorder Inventory (EDI) Composite andHealth Information Questionnaire (HIQ) Total Symptom Scores
Predictor variable
Step 1Body Mass IndexBDI scoreRSES score
Step 2SAWBS scorea
EDI Composite score
b
.10
.30-.28
.34
R2
incremental
.46*
.10b
HIQ Total Symptomscore
b
.10
.25-.22
.37
R2
incremental
.35b
.12b
aSAWBS = Shape and Weight Based Self-Esteem Inventory.bp < .001.
The SAWBS Inventory 17
correlations among SAWBS and Perceived Shape, Perceived Weight, HIQ,and EDI Composite scores.
To determine whether SAWBS scores contributed significantunique variance to eating symptom scores after the effects of BMI, de-pression, and global self-esteem were controlled, two regression analyseswere performed in which the dependent variables were the EDI compos-ite score and the HIQ symptom score, respectively. Table III displaysthe standardized regression coefficients (b) for the full prediction models,and the R2 change for each step when entered into the equations. Thefull models were both statistically significant—for EDI scores, F(4, 79)= 25.61, p <.001, and for the HIQ scores, F(4, 79) = 17.49, p < .001.In both cases, even after the variance accounted for by BMI, depression,and self-esteem was controlled, SAWBS scores accounted for additionalstatistically significant variance in EDI (10%) and HIQ (12%) symptomscores.
Stroop Task. Most (90%) of the 50 women who completed the Strooptask took longer to color-name the words on the shape and weight cardthan they did to color-name the words on the control card. The averageinterference score (shape and weight card time minus control card time)was 5.5s (SD = 4.7). A Mest examining whether Stroop color-naming in-terference was related to the order of presentation of the Stroop cards(shape and weight first vs. control first) was not statistically significant (p= .40).

Contrary to prediction, the correlation between SAWBS and Stroopcolor-naming interference scores was not statistically significant, r(50) =.13, p > .05. However, Stroop scores were related to the number of shapeand weight "hits" in the word recognition task (the correct identificationof shape and weight target words), r(50) = .38, p < .01. Therefore, notunexpectedly, individuals whose color-naming times were most delayed bythe shape and weight card, and who consequently spent more time lookingat the shape and weight words, were able to recall more of those wordsthan did individuals whose color-naming was not as delayed by the shapeand weight target words.
Word Recognition Task. As predicted, the correlation between SAWBSscores and the FAE was positive, and statistically significant, r(50) = .44,p < .001. As expected, SAWBS scores were not associated with the falserecognition of control words, r(50) = .05, p = .36. Because previous lit-erature has shown measures of cognitive schemata to be associated withdepression (e.g., Cooper et al., 1992), and because there was a statisticallysignificant relationship between BDI scores and the FAE in this study [r(50)= .40, p < .01], a multiple-regression analysis was performed to determinewhether SAWBS scores contributed unique variance to FAE scores afterthe effect of depression was controlled. In this analysis, the dependent vari-able was the FAE score, BDI scores were entered as a first predictor, andSAWBS scores were entered second. The overall model was statisticallysignificant, F(2, 47) = 9.37, p < .001. BDI scores accounted for 16% ofthe variance in FAE scores, F(1, 47) = 9.02, p < .01, and SAWBS scoresaccounted for a further 13% of the variance in FAE scores, F(1, 47) =9.37, p < .001. Therefore, the relationship between SAWBS scores andshape and weight false alarms was statistically significant, even after theeffect of depression was controlled. Looking at the relationship betweenthe two measures of cognitive schemata, Stroop interference scores wereunrelated to participants' incorrect identification of shape and weight targetwords in the word recognition task (FAE), r(50) = -.06, p > .05.
Predictive Validity
To further test the relationship between SAWBS scores and eatingdisorder symptomatology in the group of 84 women, the three probableand seven possible eating disorder cases (identified on the basis of theHIQ) were combined into one group. First, the validity of this classificationbased on the HIQ was verified by comparing the cases with the remainderof the sample on the EDI composite score. This t-test was statistically sig-nificant, t(83) = 6.40, p < .001, confirming that individuals identified as
18 Geller, Johnston, and Madsen

probable and possible cases (M = 49.50) scored higher on eating disorderssymptomatology than the remainder of the sample (M = 18.68) as assessedby the EDI Composite score. A t-test comparing SAWBS scores in theprobable and possible eating disorder case group with women with no sus-pected eating disorder was also statistically significant [t(83) = 3.10, p <.01], indicating that SAWBS scores were higher in the probable and possibleeating disorder group (M = 99.70) than in the remainder of the sample(M = 56.19).
Discriminant Validity
Non-Eating Disorder Correlates of SAWBS. In the sample of 84 women,SAWBS scores were not significantly related to the tendency to respondin a socially desirable manner, to socioeconomic status, or to BMI (seeTable II). SAWBS scores were negatively correlated with RSES scores, in-dicating that the more self-esteem was based on shape and weight, thelower were global feelings of self-worth. As noted earlier, the relationshipbetween SAWBS and BDI scores was positive, and statistically significant.That is, the tendency to base one's self-esteem on shape and weight wasrelated to higher depressed mood scores.
DISCUSSION
Growing interest in shape- and weight-based self-esteem has createdthe need for a specific measure of this construct. The purpose of this studywas to establish the psychometric properties of the SAWBS Inventory, anewly developed measure of shape- and weight-based self-esteem that iseasily administered and scored, and requires less than 10 min to complete.Findings from this study, using a nonclinical sample of young women, in-dicated that SAWBS scores were stable over 1 week and correlated mod-erately with a measure of shape and weight schemata, the false alarm effect.SAWBS scores did not correlate significantly with Stroop interference timesusing shape and weight words. Consistent with the idea that a unificationof views of the self with beliefs about shape and weight characterizes theeating disorders, SAWBS scores were moderately correlated with two meas-ures of eating disorder symptomatology. In further support of the view thatindividuals who have eating disorders can be distinguished by the degreeof influence (positive or negative) that shape and weight have on their feel-ings of self-worth, SAWBS scores discriminated between individuals whoreported few or no disturbed eating symptoms and possible and probable
The SAWBS Inventory 19

eating disorder cases. In addition, SAWBS scores were not related to familysocioeconomic status or to the tendency to respond in a socially sanctionedmanner. Given these characteristics, the SAWBS Inventory shows promiseas a screening instrument to identify individuals at high-risk to develop aneating disorder, and as a tool to measure changes in shape- and weight-based self-esteem in the course of treatment.
The correlation between SAWBS scores and the FAE was consistentwith the hypothesis that shape- and weight-based self-esteem may be as-sociated with a shape and weight schema. In this study, individuals whobased a greater portion of their self-worth on shape and weight were moreapt to confuse novel shape and weight words with ones they had alreadyseen, whereas no such effect occured with neutral control words. As pre-vious research has shown false alarms to increase with the degree to whichthe words refer to important aspects of the self-concept (Rogers et al.,1987), at the very least, these findings suggest that SAWBS scores tappeda salient dimension of beliefs about the self. The fact that SAWBS scoreswere associated with the FAE even after the effects due to depressed moodwere controlled points to the specificity of the SAWBS Inventory in meas-uring a central cognitive dimension of eating disorders (shape- and weight-based self-esteem), independent of depressed mood. This finding is incontrast to previous research (Cooper et al., 1992) in which the associationbetween general eating disorder attitudes and behaviors and a shape,weight, and eating schema assessed using a Stroop paradigm was reducedto nonsignificance when the effect of depression was controlled. A numberof differences between the methodology used in the present study and thatused in the Cooper et al. study may account for this difference in results,including, most importantly, use of the SAWBS Inventory, a specific meas-ure of shape- and weight-based self-esteem instead of the more generalEating Attitudes Test (Garner & Garfinkel, 1979), and use of the FAE toassess cognitive schemata, instead of the Stroop task. Future investigationis clearly warranted to clarify the possible greater specificity of the meas-ures used in the present study.
The failure to detect a relationship between SAWBS and Stroopscores, the second measure of shape and weight schemata used in thisstudy, was contrary to prediction. Follow-up inspection of scores revealedthat this failure was not due to a problem in the score distribution, asStroop interference scores were approximately normally distributed andhad an adequate range (20.5) and variance (SD = 4.7). In addition, asnoted earlier, the significant positive relationship between Stroop scoresand shape and weight hits in the word recognition task suggests that theproblem was not one of inaccuracies in the recording of participants' re-sponse time, as individuals who took longer to color-name shape and weight
20 Geller, Johnston, and Madsen

words correctly identified more of those words in the subsequent word rec-ognition task. Instead, one possible explanation for the lack of relationshipbetween SAWBS and Stroop scores may have been our failure to makecontrol words content consistent. That is, although the control words inthis study were carefully controlled with respect to word frequency andlength, they did not belong to a common content area. Green and Rogers(1993) reported that, when they controlled for this oft-seen methodologicalshortcoming in eating disorder Stroop research, Stroop sensitivity increased.Performance on the Stroop task may also have been affected by partici-pants' awareness of the purpose of the study. As noted earlier, the Stroophas been shown to be susceptible to extraneous influences (e.g., Warren,1974), and it is possible that some individuals guessed that the focus ofthe research pertained to shape and weight. Finally, the inconsistencies re-ported earlier in eating disorder Stroop research (e.g., Cooper & Fairburn,1992; Green & Rogers, 1993) suggest that the Stroop may simply not bea good measure of the construct of interest. Possibly, the FAE task is amore promising measure of eating disorder schemata for future research.
The relationship between SAWBS and eating disorder symptomscores supports the view that shape- and weight-based self-esteem is a cen-tral cognitive feature of the eating disorders. The independent relationshipbetween shape- and weight-based self-esteem and eating disorder sympto-matology was further demonstrated in regression analyses, in which SAWBSscores accounted for unique variance in eating symptom scores, even afterthe effects of depression, global self-esteem, and BMI were controlled. Itis noteworthy that SAWBS scores were also negatively correlated with self-esteem and positively correlated with depression. These findings suggestthat, in addition to being associated with eating disorder symptomatology,basing one's self-worth largely on shape and weight is associated withpoorer global feelings about the self, and a greater likelihood of depression.It was also noteworthy that, while SAWBS scores were not associated withactual weight and shape (as assessed by the BMI), they were associatedwith individuals' perceptions of their shapes and weights.
A limitation of the present research is the self-report nature of theSAWBS Inventory, and the implicit assumption that individuals are able toaccurately report on the extent to which shape and weight affect their self-esteem. Although this limitation cannot be discounted, the fact thatSAWBS scores correlated with the FAE, a measure of low face validity,and were unaffected by social desirability scores, suggests that individualsmay indeed have such awareness, and are able to accurately report on astructural aspect of their self-esteem, independent of their need to presentthemselves in a socially sanctioned manner. A second possible limitationof the SAWBS Inventory is that it is based on a single score. As the SAWBS
The SAWBS Inventory 21

Inventory requires the relative importance of a number of selected attrib-utes to feelings of self-worth to be assessed, this is simply an intrinsic prop-erty of the measure, and unfortunately prevents the calculation of itsinternal consistency. However, it might be argued that participants' priorselection and rank-ordering of attributes increase the validity of the SAWBSscore, in that the final SAWBS score is the culmination of a number ofpreliminary steps. In addition, the ability of the SAWBS Inventory to distilltwo complex constructs (self-esteem and shape and weight concerns) intoa single score is as much a strength of this measure as it is a limitation.
In interpreting our findings regarding the relationship between theSAWBS Inventory and one of our measures of shape and weight schemata(the FAE), we also wish to note that the assessment of schemata is a dif-ficult and controversial area (e.g., Higgins & Bargh, 1987), and alternativeinterpretations are possible. Nevertheless, our data are consistent with ourhypotheses, and we find the schemata to be a useful heuristic in makingsense of our findings.
Perhaps a more serious shortcoming of the present research was theshort test-retest interval of only 1 week. Future research is clearly war-ranted to determine whether SAWBS scores are stable over longer periodsof time. In addition, although use of a female undergraduate sample wasconsidered appropriate as a first step toward the validation of this newinstrument, future research should examine SAWBS scores in women whohave eating disorders, and compare their scores with those from psychiatricand nonpsychiatric control groups. Research in our lab is currently underway to examine SAWBS scores in such clinical samples. Finally, althoughit is tempting to consider the possible causal role of shape- and weight-based self-esteem in the development of eating disorders, the correlationaldesign of this study prevented such causality questions from being ad-dressed. Longitudinal designs offer a necessary and valuable avenue forfuture research.
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders(4th ed). Washington DC: Author.
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the BeckDepression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8,77-100.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory formeasuring depression. Archives of General Psychiatry, 4, 561-571.
Ben-Tovim, D. I., & Walker, M. K. (1991). Women's body attitudes: A review of measurementtechniques. International Journal of Eating Disorders, 10, 155-167.
22 Geller, Johnston, and Madsen

The SAWBS Inventory 23
Ben-Tovim, D. I., Walker, M. K., Fok, D., & Yap, E. (1989). An adaptation of the Strooptest for measuring shape and food concerns in eating disorders: A quantitative measureof psychopathology? International Journal of Eating Disorders, 8, 681-687.
Cooper, M. J., Anastasiades, P., & Fairburn, C. G. (1992). Selective processing of eating-,shape-, and weight-related words in persons with bulimia nervosa. Journal of AbnormalPsychology, 101, 352-355.
Cooper, P. J., & Fairburn, C. G. (1987). The eating disorder examination: A semi-structuredinterview for the assessment of the specific psychopathology of the eating disorders.International Journal of Eating Disorders, 6, 1-8.
Cooper, M. J., & Fairburn, C. G. (1992). Selective processing of eating, weight and shaperelated words in patients with eating disorders and dieters. British Journal of ClinicalPsychology, 31, 363-365.
Cooper, P. J., & Fairburn, C. G. (1993). Confusion over the core psychopathology of bulimianervosa. International Journal of Eating Disorders, 13, 385-389.
Demo, D. H. (1985). The measurement of self-esteem: Refining our methods. Journal ofPersonality and Social Psychology, 48, 1490-1502.
Fairburn, C. G., & Gamer, D. M. (1988). Diagnostic criteria for anorexia nervosa and bulimianervosa: The importance of attitudes to shape and weight. In D. M. Garner & P. E.Garfinkel (Eds.). Diagnostic issues in anorexia nervosa and bulimia nervosa (pp. 36-55).New York: Brunner/Mazel, pp. 36-55.
Garner, D. M., & Garfinkel, P. E. (1979). The Eating Attitudes Test: An index of thesymptoms of anorexia nervosa. Psychological Medicine, 9, 273-279.
Garner, D. M., & Olmstead, M. P. (1984). The eating disorder inventory manual. Odessa, FL:Psychological Assessment Resources.
Gamer, D. M., Olmstead, M. P., & Polivy, J. (1983). Development and validation of amultidimensional eating disorder inventory for anorexia nervosa and bulimia. InternationalJournal of Eating Disorders, 2, 15-33.
Green, M. W., & Rogers, P. J. (1993). Selective attention to food and body shape words indieters and restrained nondieters. International Journal of Eating Disorders, 14, 515-517.
Greenfeld, D., Quinlan, D. M., Harding, P., Glass, E., & Bliss, A. (1987). Eating behavior inan adolescent population. International Journal of Eating Disorders, 6, 99-111.
Harter, S. (1993). Visions of self: Beyond the me in the mirror. In J. Jacobs (Ed.). NebraskaSymposium on Motivation: Vol. 40. Perspectives on Motivation (pp. 99-144). Lincoln:University of Nebraska Press.
Health and Welfare Canada. (1988). Promoting healthy weights: A discussion paper. Ottawa,Ontario: Author (Health Sciences and Promotion Branch).
Higgins, T. E., & Bargh, J. A. (1987). Social cognition and social perception. Annual Reviewof Psychology, 38, 369-425.
Hollingshead, A. B. (1975). Four-Factor Index of Social Status. New Haven, CT: Author.Hsu, L. K. (1982). Is there a disturbance of body image in anorexia nervosa? Journal of Nervous
and Mental Disease, 170, 305-307.Hsu, L. K., & Sobkiewicz, T. A. (1989). Body image disturbance: Time to abandon the concept
for eating disorders? International Journal of Eating Disorders, 10, 15-30.Kagan, D. M., & Squires, R. L. S. (1983). Dieting, compulsive eating, and feelings of failure
among adolescents. International Journal of Eating Disorders, 3, 15-26.Kaplan, S. L., Busner, J., & Pollack, S. (1988). Perceived weight, actual weight, and depressive
symptoms in a general adolescent sample. International Journal of Eating Disorders, 7,107-113.
Kelly, G. A. (1955). The psychology of personal constructs. New York: Norton.Klemchuk, H. P., Hutchinson, C. B., & Frank, R. I. (1990). Body dissatisfaction and
eating-related problems on the college campus: Usefulness of the the eating disordersinventory with a nonclinical population. Journal of Counseling Psychology, 37, 297-305.
Klesges, R. C., Beatty, W. W., & Berry, S. L. (1985). Some behavioral, attitudinal, andperceptual correlates of obesity in a university population. International Journal of EatingDisorders, 4, 237-245.

Markus, H. (1977). Self-scemata and processing information about the self. Journal ofPersonality and Social Psychology, 35, 63-78.
Marsh, H. W. (1986). Global self-esteem: Its relation to specific facets of self-concept andtheir importance. Journal of Personality and Social Psychology, 51, 1224-1236.
Marsh, H. W. (1993). Relations between global and specific domains of the self: Theimportance of individual importance, certainty, and ideals. Journal of Personality andSocial Psychology, 65, 975-992.
Mathews, A., & MacLeod, C. (1985). Selective processing of threat cues in anxiety states.Behavioral Research Therapy, 23, 563-569.
O'Brien, E. J. (1980). The Self-Report Inventory: Development and validation of amultidimensional measure of the self-concept and sources of self-esteem. Unpublisheddoctoral dissertation, University of Massachusetts at Amherst.
Rogers, T. B., Rogers, P. J., & Kuiper, N, A. (1979). Evidence for the self as a cognitiveprototype: The "false alarms effect." Personality and Social Psychology Bulletin, 5, 53-56.
Rosenberg, M. (1979). Conceiving the self. New York: Basic Books.Strahan, R., & Gerbasi, K. C. (1972). Short, homogeneous versions of the Marlow-Crowne
Social Desirability Scale. Journal of Clinical Psychology, 28, 191-193.Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of Experimental
Psychology, 18, 643-662.Vanderheyden, D. A., Fekken, G. C, & Boland, F. J. (1988). Critical variables associated
with bingeing and bulimia in a university population: A factor analytic study. InternationalJournal of Eating Disorders, 3, 321-329.
Vitousek, K. B., & Hollon, S. D. (1990). The investigation of schematic content and processingin eating disorders. Cognitive Therapy and Research, 14, 191-214.
Warren, R. E. (1974). Association, directionality, and stimulus encoding. Journal ofExperimental Psychology, 102, 151-158.
Welch, G., Hall, A., & Walkey, F. (1988). The factor structure of the Eating DisordersInventory. Journal of Clinical Psychology, 44, 51-56.
Whitaker, A., Davies, M., Shaffer, D., Johnson, J., Abrams, S., Walsh, B. T., & Kalikow, K.(1989). The struggle to be thin: A survey of anorexic and bulimic symptoms in anon-referred adolescent population. Psychological Medicine, 19, 143-163.
Wylie, R. C. (1989). Measures of self-concept. Lincoln: University of Nebraska Press.
24 Geller, Johnston, and Madsen


















