
The role of portosystemic shunting in children in the transplant era
7
The Role of Portosystemic Shunting in Children in the Transplant Era By Jorge Reyes, George V. Mazariegos, Javier Bueno, Julio Cerda, Richard B. Towbin, and Sam Kocoshis Pittsburgh, Pennsylvania Purpose: Variceal bleeding in children generally presents in the setting of cirrhosis but may also occur in the absence of liver disease and after successful liver transplantation. The authors reviewed their experience with portosystemic shunt- ing in children to better define its efficacy in sclerotherapy failures, as primary therapy, and its role before and after liver transplantation. Methods: Between 1983 and 1997, 21 children with recurrent variceal bleeding underwent portosystemic shunting at the authors’ institution. Patients were divided into two groups: 13 patients in group I presented with intrinsic liver disease (cirrhosis) as a cause for portal hypertension; eight patients in group II with no liver disease had extrahepatic portal venous thrombosis, five of which occured after successful liver transplantation. The mean age was 8.6 years (range, 3 to 18). Shunt procedures were semielective, and were per- formed successfully in all children without any operative morbidity or mortality. Follow-up ranged from 6 months to 15 years. Results: Shunt procedures included splenorenal (n = 15), splenocaval (n = I), side-to-side splenorenal (n = I), inferior mesenteric vein to renal vein (n = I), mesocaval (n = I), and transcutaneous intrahepatic portosystemic shunt (TIPS; n = 2). All patients in group II are alive and well with no further bleeding or occlusions. Of the 13 patients in group I, three had bleeding postshunt, and three patients went on to require liver transplantation because of worsening liver dis- ease. One child died of liver failure with encephalopathy 4 years after shunting. There were two shunt occlusions. Conclusions: Portosystemic shunting is effective therapy in patients with intrinsic liver disease, with salvage amenable by liver transplantation in the treatment failures. It is defini- tive therapy in patients with extrahepatic venous thrombosis. J Pediatr Surg 34: 117- 123. Copyright o 1999 by W.B. Saunders Company. INDEX WORDS: Portosystemic shunt, distal splenorenal shunt, transcutaneous portosystemic shunt, portal hyperten- sion. B ECAUSE of the previously untreatable nature of end-stage liver disease. most early clinical series that addressed portal hypertension (PHI in children attributed extrahepatic portalvenous obstructions, rather than intrinsic liver disease, as the most common entity precipitating PH in children.‘-’ Over the past four de- cades, however, knowledge regarding the clinical spec- trum of diseases producing PH and its consequences in children has evolved according to the management strategies used to treat the complications of this entity and has thus impacted on the natural history. Irrespective of the etiology of PH, the clinical end results are the same: bleeding from esophageal varices, ascites, and splenomegaly with hypersplenism. Although the major “acute” emphasis in the treatment of PH has been the control of bleeding, many children with intrinsic liver disease continue to lose hepatic functional reserve. Thus. liver transplantation often becomes the only reason- able therapeutic option for the patient with advanced liver disease, either before or after shunt surgery.” The last 20 years have seen improved results with endoscopic sclero- therapy,4-h and the success of liver transplantation as definitive therapy for liver failure has allowed the devel- opment of “temporizing” approaches to the management of PH in children.7 Nonetheless, these therapies carry a Journal of Pediatric Surgery, Vol 34, No 1 (January), 1999: pp 117-123 risk of early and late complications. Also, the current scarcity of donor organs demands the development of guidelines that would distribute them to the most needy patients, perhaps after other effective forms of therapy fail. Portosystemic shunt surgery in children has thus been minimized, not only because of the dramatic evolution of other treatment modalities, but also because of the concern of shunt thrombosis and postshunt encephalopa- thy. To better define the role of portosystemic shunting in children, we analyzed retrospectively our experience in sclerotherapy failures, as primary therapy, and its role before and after liver transplantation. Preserlted (11 the 1’9th A~~uul Meeting of the American Pediatric SurgicalAs.sociation. Hilton Head, South Carolina. Ma! 10-13. 1958. Supported in part bv research yrants from the Veterms Administra- tion and Project Grmt No. DK-29961 ,frotn the National Institutes qf Hecdth. Bethrsdu. MD. Address reprint requests to Jorge Reyes. MD. Children k Hospital qf Pittsburgh. 3705 F$h Ave. Pittsburgh, PA 15213. Copyri& Q 1999 b?; WB. Saut~ders Cornpan~ VO?,-3468/99/3JOI-00-73$03.00/0 117
-
Upload
jorge-reyes -
Category
Documents
-
view
212 -
download
0
Transcript of The role of portosystemic shunting in children in the transplant era

The Role of Portosystemic Shunting in Children in the Transplant Era By Jorge Reyes, George V. Mazariegos, Javier Bueno, Julio Cerda, Richard B. Towbin, and Sam Kocoshis
Pittsburgh, Pennsylvania
Purpose: Variceal bleeding in children generally presents in the setting of cirrhosis but may also occur in the absence of liver disease and after successful liver transplantation. The authors reviewed their experience with portosystemic shunt- ing in children to better define its efficacy in sclerotherapy failures, as primary therapy, and its role before and after liver transplantation.
Methods: Between 1983 and 1997, 21 children with recurrent variceal bleeding underwent portosystemic shunting at the authors’ institution. Patients were divided into two groups: 13 patients in group I presented with intrinsic liver disease (cirrhosis) as a cause for portal hypertension; eight patients in group II with no liver disease had extrahepatic portal venous thrombosis, five of which occured after successful liver transplantation. The mean age was 8.6 years (range, 3 to 18). Shunt procedures were semielective, and were per- formed successfully in all children without any operative morbidity or mortality. Follow-up ranged from 6 months to 15 years.
Results: Shunt procedures included splenorenal (n = 15), splenocaval (n = I), side-to-side splenorenal (n = I), inferior
mesenteric vein to renal vein (n = I), mesocaval (n = I), and transcutaneous intrahepatic portosystemic shunt (TIPS; n = 2). All patients in group II are alive and well with no further bleeding or occlusions. Of the 13 patients in group I, three had bleeding postshunt, and three patients went on to require liver transplantation because of worsening liver dis- ease. One child died of liver failure with encephalopathy 4 years after shunting. There were two shunt occlusions.
Conclusions: Portosystemic shunting is effective therapy in patients with intrinsic liver disease, with salvage amenable by liver transplantation in the treatment failures. It is defini- tive therapy in patients with extrahepatic venous thrombosis. J Pediatr Surg 34: 117- 123. Copyright o 1999 by W.B. Saunders Company.
INDEX WORDS: Portosystemic shunt, distal splenorenal shunt, transcutaneous portosystemic shunt, portal hyperten- sion.
B ECAUSE of the previously untreatable nature of end-stage liver disease. most early clinical series
that addressed portal hypertension (PHI in children attributed extrahepatic portalvenous obstructions, rather than intrinsic liver disease, as the most common entity precipitating PH in children.‘-’ Over the past four de- cades, however, knowledge regarding the clinical spec- trum of diseases producing PH and its consequences in children has evolved according to the management strategies used to treat the complications of this entity and has thus impacted on the natural history.
Irrespective of the etiology of PH, the clinical end results are the same: bleeding from esophageal varices, ascites, and splenomegaly with hypersplenism. Although the major “acute” emphasis in the treatment of PH has been the control of bleeding, many children with intrinsic liver disease continue to lose hepatic functional reserve. Thus. liver transplantation often becomes the only reason- able therapeutic option for the patient with advanced liver disease, either before or after shunt surgery.” The last 20 years have seen improved results with endoscopic sclero- therapy,4-h and the success of liver transplantation as definitive therapy for liver failure has allowed the devel- opment of “temporizing” approaches to the management of PH in children.7 Nonetheless, these therapies carry a
Journal of Pediatric Surgery, Vol 34, No 1 (January), 1999: pp 117-123
risk of early and late complications. Also, the current scarcity of donor organs demands the development of guidelines that would distribute them to the most needy patients, perhaps after other effective forms of therapy fail.
Portosystemic shunt surgery in children has thus been minimized, not only because of the dramatic evolution of other treatment modalities, but also because of the concern of shunt thrombosis and postshunt encephalopa- thy. To better define the role of portosystemic shunting in children, we analyzed retrospectively our experience in sclerotherapy failures, as primary therapy, and its role before and after liver transplantation.
Preserlted (11 the 1’9th A~~uul Meeting of the American Pediatric SurgicalAs.sociation. Hilton Head, South Carolina. Ma! 10-13. 1958.
Supported in part bv research yrants from the Veterms Administra- tion and Project Grmt No. DK-29961 ,frotn the National Institutes qf Hecdth. Bethrsdu. MD.
Address reprint requests to Jorge Reyes. MD. Children k Hospital qf Pittsburgh. 3705 F$h Ave. Pittsburgh, PA 15213.
Copyri& Q 1999 b?; WB. Saut~ders Cornpan~ VO?,-3468/99/3JOI-00-73$03.00/0
117
118 REYES ET AL
MATERIALS AND METHODS
Between 1983 and 1997, inclusive. 21 children suffering recurrent variceal bleeding secondary to portal hypertension underwent portosys- temic shunting at our institution. Their records were reviewed retrospec- tively for etiology of the portal hypertension, indication for shunt procedure, previous method of therapy, diagnostic and medical manage- ment, the type of shunt procedure performed, short- and long-term complications. shunt patency. impact on hypersplenism, and need for further management.
At evaluation all patients had assessment of liver and renal function. complete blood counts, coagulation profile, echocardiogram, and a standard chest x-ray. Medical management of PH included volume resuscitation with blood products and crystalloids, and the use of a splanchnic vascular bed vasoconstrictor, historically limited to vasopres- sin, and since 1994 has been replaced by continuous intravenous infusion of somatostatin. Upper endoscopy is then performed to assess the need for further sclerotherapy and the extent of varices.
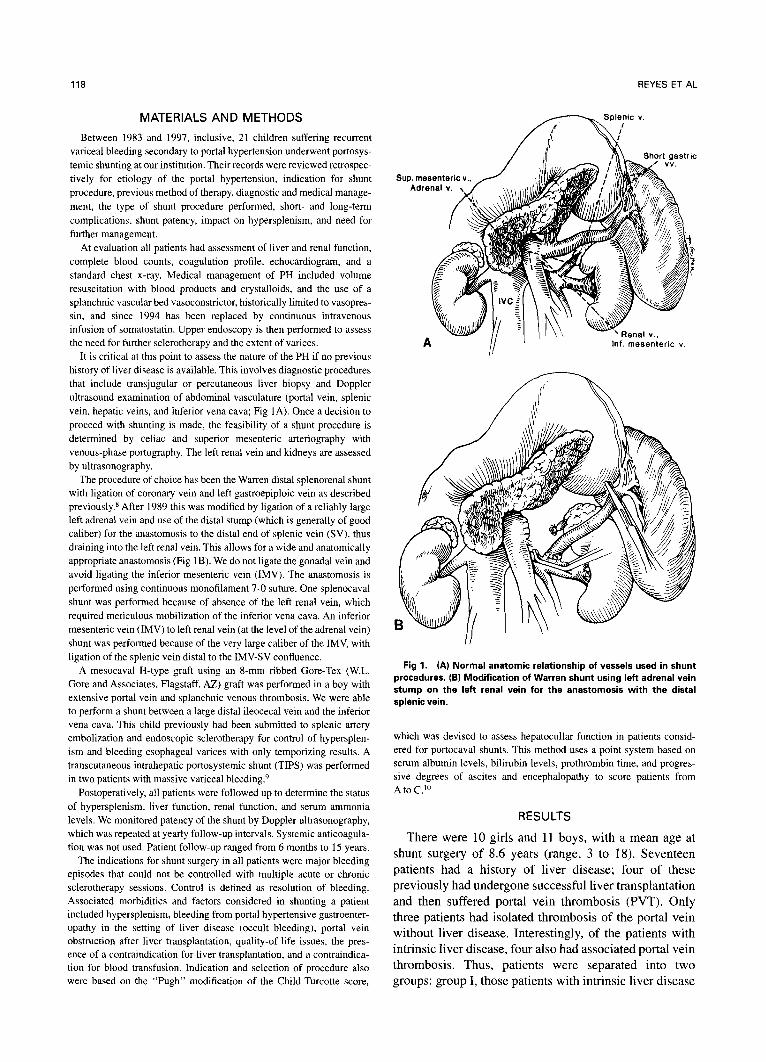
It is critical at this point to assess the nature of the PH if no previous history of liver disease is available. This involves diagnostic procedures that include transjugular or percutaneous liver biopsy and Doppler ultrasound examination of abdominal vasculature (portal vein, splenic vein. hepatic veins, and inferior vena cava; Fig IA). Once a decision to proceed with shunting is made, the feasibility of a shunt procedure is determined by cehac and superior mesenteric arteriography with venous-phase portography. The left renal vein and kidneys are assessed by uhrasonography.
The procedure of choice has been the Warren distal splenorenal shunt with ligation of coronary vein and left gastroepiploic vein as described previously.* After 1989 this was modified by ligation of a reliably large left adrenal vein and use of the distal stump (which is generally of good caliber) for the anastomosis to the distal end of splenic vein (SV). thus draining into the left renal vein. This allows for a wide and anatomically appropriate anastomosis (Fig 1B). We do not ligate the gonadal vein and avoid ligating the inferior mesenteric vein (IMV). The anastomosis is performed using continuous monofilament 7-O suture. One splenocaval shunt was performed because of absence of the left renal vein, which required meticulous mobilization of the inferior vena cava. An inferior mesenteric vein (IMV) to left renal vein (at the level of the adrenal vein) shunt was performed because of the very large caliber of the IMV, with ligation of the splenic vein distal to the IMV-SV confluence.
A mesocaval H-type graft using an 8mm ribbed Gore-Tex (W.L. Gore and Associates. Flagstaff, AZ) graft was performed in a boy with extensive portal vein and splanchnic venous thrombosis. We were able to perform a shunt between a large distal ileocecal vein and the inferior vena cava. This child previously had been submitted to splenic artery embolization and endoscopic sclerotherapy for control of hypersplen- ism and bleeding esophageal varices with only temporizing results. A transcutaneous intrahepatic portosystemic shunt (TIPS) was performed in two patients with massive variceal bleeding.9
Postoperatively, all patients were followed up to determine the status of hypersplenism. liver function, renal function. and serum ammonia levels. We monitored patency of the shunt by Doppler ultrasonography, which was repeated at yearly follow-up intervals. Systemic anticoagula- tion was not used. Patient follow-up ranged from 6 months to 15 years.
The indications for shunt surgery in all patients were major bleeding episodes that could not be controlled with multiple acute or chronic sclerotherapy sessions. Control is defined as resolution of bleeding. Associated morbidities and factors considered in shunting a patient included hypersplenism, bleeding from portal hypertensive gastroenter- opathy in the setting of liver disease (occult bleeding). portal vein obstruction after liver transplantation, quality-of-life issues, the pres- ence of a contraindication for liver transplantation, and a contraindica- tion for blood transfusion. Indication and selection of procedure also were based on the “Pugh” modification of the Child-Turcotte score,
Sup. mesenteric v..
A II ’ hf. mesenteric v
Fig 1. (A) Normal anatomic relationship of vessels used in shunt procedures. 16) Modification of Warren shunt using left adrenal vein stump on the left renal vein for the anastomosis with the distal splenic vein.
which was devised to assess hepatocullar function in patients consid- ered for ponocaval shunts. This method uses a point system based on serum albumin levels, bilirubin levels, prothrombin time. and progres- sive degrees of ascites and encephalopathy to score patients from AtoC.‘O
RESULTS
There were 10 girls and 11 boys, with a mean age at shunt surgery of 8.6 years (range, 3 to 18). Seventeen patients had a history of liver disease; four of these previously had undergone successful liver transplantation and then suffered portal vein thrombosis (PVT). Only three patients had isolated thrombosis of the portal vein without liver disease. Interestingly, of the patients with intrinsic liver disease, four also had associated portal vein thrombosis. Thus, patients were separated into two groups: group I, those patients with intrinsic liver disease

SHUNT SURGERY 119
Table 1. Group I Patients With Intrinsic Liver Disease Precipitating the Portal Hypertension
Patient NO. Diagnow
Child’s Type of SCOE Shunt Complication
Lactulose Requirement
Shunt status
Follow-Up (vr) Outcome
BA
BA
A
A
Splenocaval
Splenorenal*
None
Bleeding postshunt, ulcer
None None
Encephalopathy 4 yr postshunt
None None None
None
Yes
No
Patent
Patent
3 Died of liver failure
5.5 Alive and well 2
3 Cryptogenic
4 Biliary hypoplasia 5 Chronic hepatitis C
Splenorenal*
Splenorenal Splenorenal*
Yes
Yes Yes
Patent 6
Patent 8.8
Patent 7.5
Alive and well Alive and well
Alive, listed for transplant
Alive and well Alive and well Alive and well
Alive and well
A A
A
PNC BA, HIV Schistosomiasis
Congenital hepatic fibrosis
Congenital hepatic fibrosis
Congenital hepatic fibrosis
Cryptogenic cir-
rhosis Postnecrotic cir-
rhosis
Splenorenal” IMV-renal Splenorenal
Splenorenal”
Yes Yes No
No
Patent 7 Patent 8 Patent 9
Occluded 4.5
A A A
A
Splenorenal* None No Patent Alive and well A 6
11 A Splenorenal” None No Occluded, 4mo
Patent
6.3 Alive, OLTX
12 B TIPS Bleeding postshunt Yes 3 Alive. OLTX at 2 wk
13 B TIPS None Yes Patent Alive, OLTX at 1 wk
Abbreviations: BA, biliary atresia; HIV, human immunodeficiency virus; OLTX, orthotopic liver transplant. *Modification placing the distal splenic vein onto the distal stump of the left adrenal vein.
at the time of presentation with PH (n = 13; Table 1); group II, those patients with no evidence of intrinsic liver disease at the time of presentation with PH (extrahepatic venous thrombosis [n = 81; Table 2). There were five patients in group II with a history of successful liver transplantation for end-stage liver disease who subse- quently developed PVT.
The referral to our center was in the context of consideration for liver transplantation in 12 patients, generally those with intrinsic liver disease after failure of chronic sclerotherapy. One of these patients had an esophageal stricture. Three patients with intrinsic liver disease presented continuous “occult” blood loss distal
to the stomach. Four patients were not candidates for liver transplantation: one for medical reasons caused by human immuno-deficiency virus (HIV) infection and three others at the parents request. One of these was severely mentally retarded, and two were Jehovah’s witnesses whose parents did not wish a liver transplant because of the potential need for blood transfusions. The patient with a history of HIV infection was not a candidate for transplantation because of the risk of worsening infection under the required regimen of immu- nosuppression.
Eighteen patients presented with hypersplenism, de- fined by a platelet count of less than 150,000 X 103/mm”
Table 2. Group II Patients With No Intrinsic Liver Disease
Patient Type of Lactulose Shunt NO. Diagnosis Shunt Complication Requirement status Follow-Up Outcome
1 BA, OLTX Side-to-side spleno- Encephalopathy Yes Revision for encepha- 7.5 yr Chronic rejection, renal lopathy relisted
2 Cavernomatous Splenorenal* None No Patent 8.5 yr Alive, well 3 BA, OLTX Splenorenal* None No Patent 8.5 yr Alive, well 4 BA, OLTX Splenorenal” None No Patent 4.9 yr Alive, well 5 Carbomyl phospha- Splenorenal None No Patent 4.8 yr Alive, well
tase deficiency, OLTX
6 Portal vein throm- Mesocaval H-graft None No Patent 3 vr Alive, well bosis
7 Portal vein throm- Splenorenal” None Yes Patent 7mo Alive, well bosis
8 Portal vein throm- Splenorenal” None No Patent 15yr Alive, well bosis post-OLTX
NOTE. Portal hypertension precipitated by extrahepatic venous thrombosis. Abbreviations: BA, biliary atresia; OLTX, orthotopic liver transplantation.
*Modification placing the distal splenic vein onto the distal stump of the left adrenal vein.

120 REYES ET AL
and white blood cell count of less than 5 X 103/mm3. Hypersplenism was reversed permanently in 14 of these patients, with median elevations of platelet count of 58,000 X 103/mm3 (range, 9,000 to 326,000 X 103/mm3), and median elevation of white blood cell count of 2,900 X 103/mm3 (range, 4,400 to 13,100 X 103/mm3). All patients with extrahepatic PH had normal liver pathology results, liver function, and renal function.
For patients in group I, the decision to perform a splenorenal shunt procedure was based on the early nature of their liver dysfunction (Childs A [n = 1 l] in all patients), in association with the recurrent and (in two patients) massive nature of their hemorrhage. Two pa- tients with more advanced liver disease (Childs B) suffering recurrent esophageal bleeding while awaiting donor organ availability received TIPS as a temporizing procedure. Of the five patients with portal vein thrombo- sis after liver transplantation, all had recurrence of bleeding after sclerotherapy. Of the three patients with isolated portal vein thrombosis, all had massive recurrent bleeding postsclerotherapy; however, one patient had sclerotherapy only in the acute initial phase. His bleeding was massive, however, and recurrent at his initial hospi- talization. He was also a college athlete who wished to continue his athletic pursuits. Another patient also had diffuse thrombosis of portal and superior mesenteric veins with varices in the colon and rectosigmoid and had been referred for multivisceral transplantation.
These 21 patients received 21 shunt procedures. The type of shunt used was principally splenorenal as de- scribed previously or modification of the same. One patient from group II (posttransplant) had an initial side-to-side splenorenal shunt and required tying of the distal splenic vein because of encephalopathy. Another patient from group II had splenectomy and gastric devascularization at the time of mesocaval shunt for a previous failed splenic artery embolization. One patient had a splenocaval shunt because the left renal vein was retroaortic, and another patient had an IMV to left renal vein shunt caused by the much larger caliber of this vein for an anastomosis. Semielective shunts were performed in all cases.
Of the patients with intrinsic liver diseases who underwent a splenorenal shunting procedure, only one child has required a subsequent liver transplant 4 months postshunt because of worsening liver function in the face of shunt and native portal vein occlusion. Only one child with PVT postliver transplant has worsening liver allo- graft function from chronic rejection of the liver allograft and is currently relisted for liver transplantation. Shunt patency was confirmed by Doppler ultrasound examina- tion in 19 patients, with occlusion in two children with intrinsic liver disease.
Elevation in serum ammonia level (range, 90 to 125
pmol/L) required lactulose therapy in 10 patients, eight in the early postoperative period (within 1 month). Elevated serum ammonia levels developed in one patient 6 months postshunt. Only two children had clinical evidence of grade I encephalopathy: one patient 4 years after shunting in association with deterioration of liver function, which resolved on lactulose; she is currently actively listed for liver transplant. Another group II patient had an initial side-to-side splenorenal shunt and conversion to a stan- dard distal splenorenal shunt by tying off the distal portion of the splenic vein. This resolved the encephalopa- thy. All patients are neurologically and emotionally normal. Three patients subsequently were able to discon- tinue lactulose therapy. Interestingly, this complication was seen mostly (8 of 10) in patients with a history of intrinsic liver disease (group I).
Two patients with intrinsic liver disease (both Child’s B) who underwent TIPS procedures received liver transplan- tation within 2 weeks of the shunt. They are both well posttransplant. Three patients had recurrence of bleeding after successful shunting, two from varices, and required liver transplantation. One patient with intrinsic liver disease in whom shunt thrombosis and PVT developed required a transplant, and another post-TIPS who had a significant steal thru a coronary vein stopped bleeding postembolization of this vein (thru the TIPS). Another patient with intrinsic liver disease had bleeding from previous recent esophageal ulcer sites, which stopped spontaneously; she has not bled since. Overall patency rate of shunts was 90%; 92% in group I, and 100% in group II. Chylous ascites occurred in two patients and resolved spontaneously in both within 1 month postshunt.
There was only one death 3 years postshunt from progressive liver failure. This child had severe mental retardation and was not a candidate for liver transplanta- tion at the parents request.
DISCUSSION
In this experience, the distribution of pediatric patients with portal hypertension presenting with gastrointestinal hemorrhage is equally distributed among patients with intrinsic liver disease (group I) and those with extrahe- patic portal and splanchnic venous obstruction (group II). The response to shunt therapy also seems to be divided along similar groupings. Shunt surgery was definitive therapy in all group II patients, with no occlusions or rebleeding. Only one child has required lactulose therapy. Shunting allowed continued survival and avoided retrans- plantation in four prior recipients of liver allografts. One child is suffering from chronic rejection and is currently listed for retransplantation. In another child shunting has helped avoid a multivisceral transplant.
Tne results of splenorenal shunting in patients with intrinsic liver disease, although encouraging, were marred

SHUNT SURGERY 121
by a greater requirement for lactulose therapy. Only one of eight patients in this group, however, became clinically encephalopathic 4 years postshunt in association with deterioration of liver function. Another patient died of progressive liver disease, and one more required a liver transplant, also because of progressive liver disease. Thus, long-term outcome is dependent on the evolution of the intrinsic liver disease. Eight patients have been spared liver transplantation and are alive and well 5 to 9 years postshunt.
The success of sclerotherapy in the management of these patients is indisputable,4-6 resulting in an obvious decline of shunt surgery, as expressed by Karrer in his statement referring to “the near extinction of portosys- temic shunt procedures.“7 Currently there is an expand- ing arsenal of “temporizing” measures that have resulted in therapeutic tools that include sclerotherapy, band variceal ligation, peritoneal-venous shunt surgery for the correction of ascites, splenic artery embolization for worsening thrombocytopenia, and TIPS for the control of massive bleeding not responsive to sclerotherapy. It is critical: however, to recognize the limitations of these modalities and their potential for complications.
All patients in this series were referred for uncontrol- lable bleeding, not responsive to standard sclerotherapy protocol, and this should remain the standard approach. This is a particularly important consideration in light of the critical postshunt complications such as occlusion, rebleeding, and elevation of serum ammonia levels that occurred principally in patients with intrinsic liver dis- ease. To a great extent, these complications stem from the severity of liver disease, including the late death from progressive liver failure. Consequently, three patients went on to successful liver transplantation.
In patients with extrahepatic portal vein or splanchnic venous thrombosis, schlerotherapy and band ligation should not be dismissed as therapies because of the known natural history of extrahepatic portal vein obstruc- tion. If bleeding can be controlled and variceal size reduced after a few sessions of sclerotherapy, the risk of rebleeding will diminish progressively over time because of the tendency for development of spontaneous shunts or improved portal flow through collaterals. Unfortunately, variceal size cannot be reduced by “local” therapy in a substantial percentage of these patients. Persistence in performing sclerotherapy or variceal ligation subjects them to significant risk for complication. All of our patients are alive with functioning shunts, having re- quired no further therapy. Because the mortality rate overall was nil, and there were no cases of encephalopa- thy, it seems reasonable to consider shunting the “defini- tive” therapy for this patient population, and to perform shunts in those for whom “local” therapy seems to show no benefit.
In children with intrinsic liver disease and moderate liver dysfunction in whom uncontrollable bleeding devel- ops, a TIPS procedure can control the acute complica- tions of PH. In addition, the intrahepatic shunt can stabilize the child while awaiting donor organ availabil- ity.” The major considerations should be (1) technical issues such as patient size and patency of hepatic and portal veins; (2) potential complications such as bleeding from capsular perforation or extrahepatic portal vein puncture, peritonitis, and hepatic or biliary injury; (3) the development of an uncontrollable rise in serum ammonia levels with encephalopathy. Based on our limited experi- ence, it appears that TIPS is best indicated for someone awaiting urgent transplantation. In patients who do not require this, a surgical shunt should be the procedure of choice because of its operative efficacy.*l-lJ Shunt proce- dures that avoid the hepatic hilus currently are the standard, not only because they avoid complicating a transplant operation, but also because they are effective.15
In a patient without intrinsic liver disease (group II) and extensive portal and splanchnic venous thrombosis it is critical to have an optimum angiographic study of this system in the hope of performing a mesocaval shunt procedure when possible. Because many of these patients manifest portal hypertensive bleeding from the lower gut, this type of shunt procedure addresses this problem.
Children in whom shunting is not feasible may benefit from gastric devascularization and splenectomy.16 In the absence of intrinsic liver disease, these procedures should allow for bleeding-free survival, thus avoiding more complex surgical intervention such as multivisceral trans- plantation.
Our experience with splenic artery embolization has demonstrated temporary effects, with recurrence of throm- bocytopenia within weeks of embolization. We recom- mend embolization only in patients with intrinsic liver disease requiring urgent transplantation, in which TIPS is not feasible. However, with a successful shunt, correction of hypersplenism is permanent. Whether such satisfac- tory results would justify the use of surgical shunts as primary therapy for severe hypersplenism and spleno- megaly addresses the issue of the effect of therapy on quality of life. Although such considerations are impor- tant in the pediatric population, patient selection should be highly individualized.
It is the etiology of the portal hypertension. particularly the presence or absence of intrinsic liver disease that dictates short- and long-term outcome. In patients with a normal liver and extrahepatic obstruction, a shunt proce- dure is definitive therapy, and is accompanied by minimal morbidity. However, in patients with intrinsic liver dis- ease, the severity of bleeding dictates the immediate medical and interventional management to control the hemorrhage. In children with stable liver function, not in

122 REYES ET AL
need of an urgent transplant, a surgical shunt can be patient can await an appropriate offer in a more stable performed with 100% short-term and 92% long-term condition. Elevation in postshunting serum ammonia survival rates. Liver transplantation can be the definitive levels has been manageable with lactulose therapy, and therapy in cases of shunt failure. Donor availability then has a low (two patients, 10%) incidence of correctable ceases to be a critical life-determining issue, and the encephalopathy.
REFERENCES 1. Goh DW, Myers NA: Portal hypertension in children-The
changing spectrum. J Pediatr Surg 29:688-691, 1994 2. Collini FJ, Brener B: Portal hypertension. Collective review. Surg
Gynecol Obstet 170: 177- 192.1990 3. Reyes J, Iwatsuki S: Current management of portal hypertension
with liver transplantation, in Camaron JL, (ed): Advances in Surgery Vo125. St Louis, MO, Mosby-Year Book 1992, pp 353-387
4. Dall’Oglio L, Bagolan P, Ferro F, et al: Endoscopic injection sclerosis of oesophageal varices in children-indications and tech- niques. Endoscopy 16:98-100, 1984
5. Hassal E, Ament ME, Berquist WE: Endoscopic sclerotherapy of esophageal varices in childhood. Gastrointest Endosc 3 1: 130(2 1 A), 1985
6. Donovan TJ, Ward M, Shepherd RW Evaluation of endoscopic sclerotherapy of esophageal varices in children. J Pediatr Gastroenterol Nutr 5:696-700, 1986
7. Karrer FM: Portal hypertension. Semin Pediatr Surg 1:134-144, 1992
8. Warren WD, Zeppa R, Fomon JJ: Selective trans-splenic decom-
pression of gastroesophageal varices by distal splenorenal shunt. Ann Surg 166:437-455, 1967
9. Hackworth CA, Leef JA, Rosenblum JD. et al: Transjugular intrahepatic portosystemic shunt creation in children: Initial clinical experience. Radiology 206: 109-l 14, 1998
10. Pugh RNH, Murray-Lyon IM, Dawson JL, et al: Transsection of the oesophagus for bleeding oesophageal varices. Br J Surg 60:646-649. 1973
1 I. Bismuth H, Franc0 D, Alagille D: Portal diversion for portal hypertension in children. The first ninety patients. Ann Surg 192: 18-24, 1980
12. Bismuth H, Franc0 D: Portal diversion for portal hypertension in early childhood. Ann Surg 183:439-446, 1976
13. Shun A, Delaney DP, Martin HC, et al: Portosystemic shunting for paediatric portal hypertension. J Pediatr Surg 32:489-493. 1997
14. Maksoud JG, Goncalves ME, Porta G, et al: The endoscopic and surgical management of portal hypertension in children: Analysis of 123 cases. J Pediatr Surg 26:178-181, 1991
15. Brems JJ, Hiatt JR, Klein AS, et al: Effect of prior portasystemic shunt on subsequent liver transplantation. Ann Surg 209:51-56. 1988
16. Sugiura M, Futagawa S: A new technique for treating esophageal varices. J Thorac Cardiovasc Surg 66:677-685, 1973
Discussion
From the Floor: Thank you for that nice series and interesting data. I’d like to make a couple of comments and ask you a couple of questions.
Why are you still using angiography to evaluate these children? Today I think the magnetic resonance imaging (MRI) clearly is the best way to look at the venous anatomy of the portal system. Ultrasound examination, even Doppler ultrasonography, is not as accurate, and of course arteriography is invasive, and we have found that the MRI gives beautiful pictures both preshunt and postshunt to evaluate the portal venous anatomy.
My second question is, what is the denominator on your patients? How many of the outcomes are successful on sclerotherapy. I think most of us have found that the majority of our patients are doing very well with sclero- therapy and somatostatin and it is only the rare occasion where we have to resort to a shunt. We have now done about 20 proximal central splenorenal shunts in a group of patients like this over a period of about 25 years.
My third question is, what about that spleen? A number of these children have huge spleens. They are very uncomfortable. It becomes a major problem in terms of their physical activity, such sports participation. And when you do the shunt, whether it is a Warren, a central splenorenal, or any other portosystemic shunt, as you
showed in your data, only about two thirds of them reverse their hypersplenism in terms of their platelet count. You have one-third that still have a problem and still have a very big spleen that is uncomfortable. So what do you do with that group of patients?
J. Reyes (response): The splenomegaly actually im- proves. I just had one patient come back and I cannot palpate his spleen anymore. The degree of hypersplenism does not correlate with the size of the spleen. I think that from the standpoint of indications for transplant or the quality of life as an indication for further therapy, I think it is very important in children. And I think if there is a child with a huge spleen who is having difficulty in growing up and carrying on a normal lifestyle, they should be considered for other forms of therapy or further management even with transplantation.
With angiography we haven’t had any serious compli- cations, at least in the last IO years. I have had small experience with the use of that MRA ASA modality for evaluating the vasculature before shunt surgery. As far as ultrasonography is concerned, we use that to assess the initial patency of the vessel when we are evaluating the patient’s etiology of portal hypertension.
J. Reyes (response): That is actually the best question because we do not know. There is no question that

SHUNT SURGERY 123
sclerotherapy is the standard of therapy for these chil- dren. There is no question about that. All these patients did not respond to sclerotherapy. I think the important thing is to realize that when you refer a patient with uncontrollable bleeding who has not responded to sclero- therapy, and somebody is knocking on your door telling you that they want this patient to undergo transplant, that is when you have to consider, the status of this patient. Can this patient be treated in another way. not necessarily with liver transplant? The issue here is not when should we more aggressively do shunts, but does this patient really need a transplant, can we treat this patient with shunt surgery and avoid a transplant procedure indeti- nitely, or can this patient be spared liver transplant for 5 or 6 or 10 years.
Fror~ the Floor: Don’t you think that if a patient is having trouble after a successful shunt operation with a big spleen that it is less invasive to take out the spleen than to do a liver transplant?
J. Rcyes (re,yyonse): Yes. It is important to note that liver transplantation is not for everybody. I would be lying if I said that if I never did another liver transplant in my lift I would be happy, but we don’t like doing transplants unless it is really indicated, not only for this indication but even for the hemangioendotheliomas that were presented by my colleague before.
PL. Click (Buff&, NY): I would like to congratulate you on a great presentation. You didn’t seem to stratify your patients for age or size, and if you look in the literature there are some contraindications to doing distal splenorenal shunts for small children. You have encour- aged me to go ahead and perform this on small babies, and they have been successful. Is that not an important consideration any longer-the body weight, the size of the vessels, or the age of the baby at the time of considering a distal splenorenal shunt?
J. Reyes (response): It should not be an important consideration at this point in time given our present techniques of vascular anastomoses. Perhaps that ques- tion is a question that I would use even to support the fact that imaging by angiography versus MRI would give you a better picture as to the suitability of these vessels. However, because I have limited experience with hlR1 I won’t do that comparison. I think the publications by Dr Bismuth from France about 5 or 6 years ago really supported the aggressive use of shunt surgery even in the small babies because of his high patency rate and high success rate. At this point I think that would be reassur- ing, and this experience is reassuring, but because the patient population is still limited, age stratification would not have yielded us any significant information.
R. Gnndhi (Saddle River; NJ): I have followed up with about 20 patients with portal hypertension and have found out that if the sclerotherapy fails you can use esophageal banding. I also found out that some of the recurrent bleeders may have gastroesophageal reflux. 1 have two patients of 20 who have severe gastroesopha- geal reflux, one needed surgery and the other needed medications for reflux. I wanted to get your feeling whether you are doing banding on the failed sclero- therapy patients, are you following up with recurrent bleeders to see whether they have severe reflux?
J. Reyes (response): I think banding is becoming more popular now particularly in our center, and I think that option should remain open. I think the experience with banding versus injection sclerotherapy should be better from the standpoint of postoperative complications. How- ever, here the issue is not postoperative complications; the issue is efficacy. Are you getting control of bleeding, and is this life-threatening bleeding, or have you had multiple life-threatening bleeding episodes?


















