The role of ICT in public bad Ruhuha, Rwanda
119
The role of ICT in public bad governance: the case of malaria in Ruhuha, Rwanda Mirthe Boerdijk MSc Thesis International Development Studies August 2018
Transcript of The role of ICT in public bad Ruhuha, Rwanda

TheroleofICTinpublicbadgovernance:thecaseofmalariainRuhuha,RwandaMirtheBoerdijkMScThesisInternationalDevelopmentStudiesAugust2018

August,2018
WageningenUniversity
TheroleofICTinpublicbadgovernance:thecaseofmalariainRuhuha,Rwanda
By
MirtheBoerdijk931217085110
MScThesisInternationalDevelopmentStudiesCourseCode:LAW-80433
Supervisedby:Dr.KatarzynaCieslik,PhD
Secondexaminer:Prof.dr.ArtDewulf

i
Acknowledgements
Thisreportcontainsthethesis‘TheroleofICTinpublicbadgovernance:thecaseofmalariainRuhuha,Rwanda’’.IthasbeenwrittentobringtocompletionthegraduationrequirementsoftheMScprogramInternationalDevelopmentStudiesatWageningenUniversity.Iwasengagedinresearchingandwritingthisthesisintheacademicyear2017/2018.
ForthisthesisIjoinedEVOCA(EnvironmentalVirtualObservatoriesForConnectiveAction),whichisacollaborativeinterdisciplinaryprojectofWageningenUniversityandsevenpartnerinstitutions.Itfocusesonknowledgesharingplatforms(knownasEnvironmentalVirtualObservatories,EVOs)andtheirpotentialtotransformthedevelopmentlandscapeinfivecasestudyareasinruralAfrica.Theresearchproposalandresearchquestionswereformulatedtogetherwithmysupervisor,DrKatarzynaCieslikPhD,tofitintheproject.
Iwouldliketothankmysupervisorforallherguidance,feedback,andsupportduringtheproposalwriting,fieldresearch,dataanalysisandreportwriting.Iwanttothankheraswellfortheopportunitytojointhisprojectandforherenthusiasm.IalsowishtothankprofessorMutesa,DominaAsingizweandMarilynMurindahabiforalltheirhelpduringthefieldresearchinRwanda.WithouttheircooperationIwouldnothavebeenabletoconductthisresearch.Furthermore,IwouldliketothankthesistersatRuhahahealthcenterforschedulingtheinterviewsatthecommunitylevel.Moreover,IwouldliketothankDieudonneBarigoraforhisassistanceandthetranslationsKinyarwanda-Englishduringtheinterviewsatthelocallevelofanalysis.Lastly,Iwanttothanktheintervieweesfortheirtimeandwillingnesstoparticipateinmyresearch.

ii
Abstract
SeveralcountriesinSub-SaharaAfricaarecurrentlyexperiencingaresurgenceofmalaria,amongwhichRwandawitnessedaparticularlysharpincreaseinreportedcasesfromanestimated225,176casesin2011to1,598,055in2014.MyresearchexplorestherolethatICTsmightplayinmalariapreventionandcontrol.ItbuildsonabroadbodyofliteraturethatscrutinizesthepotentialofICTstostrengthenhealthsystemsbyimprovingservicedeliveryandqualityaswellasthroughthegeneralcommunicationfunction.
Inmythesis,IchoseRuhuhasectorinRwandaasastrategicsitetoillustratethemanywaysinwhichICTs–andinparticular,mobilephones–canstrengthenthecapacityofthehealthsystem.Inrecentyears,thegovernmentofRwandahasimplementedanumberofenablingpoliciesandinterventionsinanefforttointegratetechnologyinthehealthsystem.MystudyrevealsthatapartfromthestrategicICT-basedhealthinterventions,mobilephonesalreadyplayacrucialroleinmalariapreventionbyfacilitatingawarenessraising,improvingtheinformationflowswithinandbetweenthestakeholdergroupsandstrengtheningtheimplementationofcommunitylevelmalariapreventionrules.Thiswasdonebyconductinganexploratorystudyconsistingofsemi-structuredinterviewswith32actorsfromthecommunity,district,andnationallevel.
Thecontributionofmystudyistwo-fold.First,mymulti-levelanalysisshedslightontheexistingmeansandrulesconcerningmalariapreventionandcontrolaswellastheirperceivedefficacy.Ifindthatcommunicationandlackofthereofplaysavitalroleininfluencingthestakeholderframingofthedisease.Thisincludesbothface-to-faceandmobilephonebasedcommunication.Second,myfindingsfurtherlookatElinorOstrom’stheoryofcollectiveaction.IarguethatmalariacaninfactbeperceivedasapublicbadandanalyzetheroleofICTsinfacilitatingpeople’scompliancewithOstrom’sdesignprinciples.

iii
TableofcontentACKNOWLEDGEMENTS..................................................................................................................IABSTRACT.........................................................................................................................................IITABLEOFCONTENT.....................................................................................................................IIILISTOFFIGURESANDLISTOFTABLES...................................................................................VLISTOFABBREVIATIONS...........................................................................................................VI1.INTRODUCTION...........................................................................................................................12.LITERATUREREVIEW...............................................................................................................32.1HEALTHSYSTEM.........................................................................................................................................32.2INFORMATIONANDCOMMUNICATIONTECHNOLOGIES(ICTS).........................................................32.3POTENTIALROLEOFICTINHEALTHSYSTEMSOFDEVELOPINGCOUNTRIES.................................42.4RWANDAICTHUB.....................................................................................................................................42.5ICTHEALTHINITIATIVESANDPOLICIESINRWANDA.........................................................................62.6MALARIAPREVENTIONANDCONTROLINRUHUHA,RWANDA..........................................................72.7ICTSFORSUSTAINABLERURALDEVELOPMENT...................................................................................8
3.THEORETICALFRAMEWORK..................................................................................................93.1RELEVANCEANDMAINOBJECTIVEOFTHESTUDY...............................................................................93.2ICTSANDCOLLECTIVEACTION:INTRODUCINGOSTROM’SDESIGNPRINCIPLES............................93.3RESEARCHQUESTIONS............................................................................................................................11
4.METHODOLOGY........................................................................................................................134.1DATACOLLECTION...................................................................................................................................134.1.1Secondarydata................................................................................................................................134.1.2Interviews...........................................................................................................................................13
4.2DATAANALYSIS........................................................................................................................................145.RESULTSANDDISCUSSION....................................................................................................155.1STAKEHOLDERANALYSIS........................................................................................................................155.1.1Communitylevel..............................................................................................................................165.1.2DistrictLevel.....................................................................................................................................195.1.3NationalLevel..................................................................................................................................19
5.2INFORMATIONANDCOMMUNICATION:ACTORS,FLOWSANDCHANNELS......................................225.2.1Informationandcommunicationflowsbetweenactors................................................225.2.2TheroleofICTs................................................................................................................................39
5.3ANALYSISOFACTOR’SPERCEPTIONS....................................................................................................445.3.1Perceptionsofthefutureroleofmobilephones................................................................445.3.2Situationregardingmalaria......................................................................................................465.3.3Knowledgeandmisconceptions...............................................................................................495.3.4Trust.....................................................................................................................................................595.3.5Sharedperspectiveoftheproblem..........................................................................................64
5.4MALARIAGOVERNANCEARRANGEMENTS...........................................................................................755.4.1Preventionandcontrolmeasures............................................................................................755.4.2Malariaasapublicbad................................................................................................................835.4.3Ostrom’sdesignprinciples..........................................................................................................925.4.4TheroleofICTsinthemalariagovernancearrangements.........................................96
6.CONCLUSION..............................................................................................................................987.RECOMMENDATIONS...............................................................................................................99REFERENCES................................................................................................................................100APPENDICES.................................................................................................................................103

iv
APPENDIX1–OVERVIEWOFINTERVIEWEES.........................................................................................103APPENDIX2–TOPICLISTOFTHEINTERVIEWS.....................................................................................1072.1Interviewtopics–community.....................................................................................................1072.2Interviewtopics–actorsinhealth/policylevel................................................................108
APPENDIX3–OVERVIEWOFCODES........................................................................................................109

V
ListoffiguresFigure1:LocationRuhuhasectorintheredcircleFigure2:Ostrom’sDesignPrinciplesFigure3:Informationandcommunicationflowsaboutmalariabetweenactors
ListoftablesTable1:FactorsthatinfluencedrapidICTdevelopmentinRwanda(Mwangi,2006)Table2:MajorinitiativesinhealthinformationtechnologyinRwanda(Frasieretal,2008)Table3:ActorsinRwanda’shealthsystemregardingmalariapreventionandcontrolinRuhuhaTable4:ICTchannelsusedinmalariapreventionandcontrolinRuhuhaacrosslevelsTable5:ExplanationinformationandcommunicationflowsfromcommunitymembersTable6:ExplanationinformationandcommunicationflowsfromcommunityhealthworkersTable7:ExplanationinformationandcommunicationflowsfromthehealthcenterTable8:ExplanationinformationandcommunicationflowsfromthehealthcenterpharmacyTable9:ExplanationinformationandcommunicationflowsfromtheprivatepharmacyTable10:ExplanationinformationandcommunicationflowsfromlocalleadersTable11:ExplanationinformationandcommunicationflowsfromcooperativesTable12:ExplanationinformationandcommunicationflowsfromthedistricthospitalTable13:ExplanationinformationandcommunicationflowstheRwandaBiomedicalCenterTable14:TherolesofmobilephonesinmalariapreventionandcontrolinRuhuhaTable15:ExamplesofperceptionsthatmalariaisaproblemathighlevelTable16:ExamplesofperceptionsthatmalariaexceededlimitscomparedtothepastTable17:ExamplesofperceptionsthatmalariaexceededcomparedtootherregionsinRwandaTable18:ExamplesofperceptionsthatmalariaincreasesduringcertainmonthsTable19:PerceptionsofactorswhothinkthatknowledgeaboutmalariaisnotenoughTable20:ExamplesofactorswhomentionedtheneedforcontinuousteachingTable23:MisconceptionsaboutmalariaTable24:ExamplesofstatementsthatillustratethattherearecommunitymemberswhodonotbelievethatthetabletsstillcuremalariaTable25:WhatproblemswerementionedbywhichactorsTable26:RulesandregulationsregardingmalariapreventionandcontrolinRuhuhaTable27:ExamplesthatthepreventionmeasuresarenotenforcedTable28:ExamplesofquotationsexplainingcooperationbetweenactorsTable29:ExamplesofquotationsontheimportanceoffollowingtherulesandregulationsTable30:Examplesofquotationsabouttryingtobeanexampletoothercommunitymemberswhenitcomestofollowingtherulesandregulations

VI
ListofabbreviationsBti BacillusthuringiensisisraelensisCBHI CommunityBasedHealthInsuranceCMATs CommunityMalariaActionTeamsEVOCA EnvironmentalVirtualObservatoriesForConnectiveActionEVOs EnvironmentalVirtualObservatoriesGoR GovernmentofRwandaHIV HumanimmunodeficiencyvirusHMIS HealthManagementInformationSystemsLLIN Long-lastinginsecticidalnetsICTs InformationcommunicationtechnologiesIRS IndoorresidualsprayingITN Insecticide-treatedmosquitonetsMEPR MalariaEliminationProgramNMCP NationalMalariaControlProgramPMI President’sMalariaInitiativeRBC RwandaBiomedicalCenterRDT RapiddiagnostictestRSSB RwandaSocialSecurityBoardSFH SocietyforFamilyPlanningSIScom CommunityHealthWorkerInformationSystemSMS ShortmessageserviceTB TuberculosisUSAID UnitedStatesAgencyforInternationalDevelopmentUSD UnitedStateddollarWHO WorldHealthOrganization

1
1.Introduction
Malariaisadiseasethatisconsideredendemicin91countries(WHO,2016).Halfoftheworld’spopulationwasatriskofmalariain2016.In2015therewere212millionmalariacasesglobally,ofwhich429.000resultedindeath.Sub-SaharaAfricaistheregionthatcarriestheheaviestmalariaburdenworldwide(ibid).
Malariacontrolinterventionshavebeenwidelydeployedtoreducemalariacaseincidenceandmortalityrates(WHO,2016).Themostcommonlyusedmethodtopreventmosquitobitesareindoorresidualspraying(IRS)andinsecticide-treatedmosquitonets(ITN).Thesetwocorevectorcontrolinterventionsareestimatedtohavereducedmalariaincidenceratesby50%since2000(ibid).Bothofthesemeasures,however,areheavilyreliantonthecapacityandwillingnessoftheaffectedpopulationstocomplywiththepreventionrulesandregulationsintheirdailychoicesandactivities.Despitelargeincreasesinthefinancingofmalariacontrolandeliminationprogramsovertheyears2000to2015malariaremainsathreattopublichealthinmanycountries(WHO,2016).
Althoughmalariainterventionshavebeenwidelyadoptedandmalariaincidencerateshavegloballydecreasedsince,severalcountriesinSub-SaharanAfricaareexperiencingaresurgenceofmalaria(President’sMalariaInitiative,2016).Inparticular,Rwandahasseenanincreaseinreportedmalariacasesfromanestimated225,176casesin2011to1,598,055in2014.Changesinrainfallandtemperature,increasedimportationofmalariacasesfromneighboringcountries,anincreaseofresistanceofmosquitotoinsecticides,anduseofdistributednetsthatshouldhavebeenreplacedmayhavecontributedtothisincrease(ibid).
MyresearchbuildsontheassumptionthatICTsmightplayavitalroleinmalariaprevention,asICTscanstrengthenthehealthcaresystem(ShiferawandZolfo,2012).WhenICTsareusedeffectivelytheyhavealargepotentialtoboostinformationflowsandknowledge,andtoempowercitizens(Chetley,2006).Inparticular,theconnectivefunctionofmobilephonecommunicationmaybeleveragedtotriggercollectiveactionprocessesbothwithinandbetweenstakeholdergroups.Thisisofspecialimportanceformalaria:asavectorbornedisease,malariaistransmittedbyaparasitefromoneinfectedperson(host)toanother.Effectivepreventionandcontrolmeasuresmustthusentailcommunalresponsibilityandcollectivemobilizing(Ostrom2009).
Interestingly,in2015theGovernmentofRwandadevelopedanationalICTstrategyandplan(GoR,2015).ThepolicyaimstoleverageICTsinallsectorstotransformRwandaintoaninformation-richandknowledgebasedeconomyby2020(ibid).TheGovernmentofRwandaisinvolvedinallleadinginitiativesandemergingtechnologies,astheprivatesectorhasnotyetcomeup(Frasieretal.,2008).Inthisrespect,anumberofenablingpoliciesandinterventionshavebeenputinplaceinanefforttointegratetechnologyinthehealthcaresystem(ibid).
MythesisinvestigatestheroleofICTandtheroleofinformationinthemanagementandcontrolofmalariainRuhuhasectorinBugeseradistrict,easternprovinceofRwanda.Thissectoristhelocallevelofanalysisandislocated42kmfromKigali.Becauseofitsgeographicalfeaturessuchasaltitude,

2
ricefieldirrigationschemes,swampsandcrossbordermovements,thisregionisamalariaendemiczone(Ingabireetal,2016b).
Myresultsshowthatmultiplestakeholdergroupsexchangeinformationaboutmalariaaswellasthemeansofitscontrolandpreventionintheireverydaycommunicationboththroughface-to-faceandICTs.SomeadvantagesofICTsarethattheyfacilitateinformationandcommunicationflowsthatarerealtime,lowcost,overlargedistanceandacrossstakeholdergroups.However,thecanalsoincreasethespreadofmisconceptions.Furthermoretheresultsalsoshowthatmobilephonescantoapointfacilitatecollectiveaction.

3
2.Literaturereview
Informationplaysanimportantroleintheeffectivemanagementanddevelopmentofhealthcaresystems(HartshorneandCarstens,1990).Informationinhealthisrequiredforthemanagementofoperations,planning,andcontrol(ibid).HartshorneandCarstens(1990)describethat:
‘Toprovidethenecessaryinformationneedsofusersatdifferentlevelsofmanagementinthehealthcaresystem,astructuredinformationsystemcoupledwithappropriateinformationtechnologyisrequired’’.
Suchinformationtechnologies,orICTs,arerevolutionizinglivesanditsapplicationinhealthcouldbenefithealthsystemsandinformationmanagementproblems(ShiferawandZolfo,2012).Inthischapter,IfirstdefinehealthsystemsandICTsfromthepointofviewofaccesstoexpertinformationandknowledge.Secondly,IreviewtherelevantliteratureandpolicydocumentsfocusingontheroleofICTandmalariapreventionandcontrolinRuhuha,Rwanda.
2.1HealthsystemAccordingtoBloomandStanding(2008)healthsystemscanbeanalyzed
as‘’waysoforganizingaccesstoexpertknowledge’’.Thisconceptcontainspublicandprivateactorsandmodernandtraditionalproviders(Lucas,2008).Rwanda’shealthsystemalsoconsistsofpublicandprivatetraditionalandmodernprovidersofhealthservicesforcommunitymemberstoaccessknowledge.FurthermoreLucas(2008)describes,‘’itfocusesonthewaysinwhichhealthknowledgeisgraspedorwithdrawn,whogainsaccesstoitandtheverydifferentwaysinwhichitcanbeorganized’’(ibid).Appropriateinformationandhealthcaresupportempowershealthcarestaff,isastrategyforachievingsustainableimprovementofhealthsystemsinruralareasandiscosteffective(ShiferawandZolfo,2012).ICTsplayaroleinthisbecausetheyhaveshownpotentialtoimprovehealthcaredeliverysystemstobetterhealthandhealthcoverage,theyenhancequality,theycancreateaccess,andenablequickcommunicationbetweenhealthprofessionalswiththeircolleaguesandpatients.ExamplesofICTsinhealthsystemsincludeeLearningtools,telemedicine1,healthinformationsystemswithdecisionsupport,electronicmedicalrecords,andmobilehealth(ibid).
2.2Informationandcommunicationtechnologies(ICTs)Inthisdigitalera,ICTsareconsideredtohaveasignificantpotentialto
stimulatesustainabledevelopmentandgovernance,improvethehealthandwellbeingofmarginalizedpopulationsandthepoor,andtocontributetopovertyreduction(Chetley,2006;Panir,2011).Nayaketal.(2010)definesICTas“technologiesthatfacilitatecommunicationandtheprocessingandtransmissionofinformationbyelectronicmeans”.ICTsarenowadaysbeingusedineffortstofacilitategreaterplanning,control,andcommunication,whichinturncanchangeorganizationalstructures(Bloomfield,1991).Forexample,inhealthICTscanfacilitatepatientdatacollectionandprocessing,helpscreeningandmonitoring,andimproveinformationdeliveranceandeducation(Frasieretal,2008).ShiferawandZolfo(2012)describethatthecurrenttrendofexpandingpenetrationratesofmobiletechnologyindevelopingcountriesisanopportunity

4
toimplementrelevanttechnologicalapplicationsinhealthsystems.Theygivesomeexamplesbystating:
‘’Forinstance,inUgandatheuseofaVHFradiobytraditionalbirthattendantsfacilitatedearlyreferralandcontributedtoasignificantreductioninmaternalmortality,showingthattheuseofICTtechnologycanpreventavoidablematernaldeath.InSouthAfricaandRwandamobiletechnologyimprovedadherencetoTBandHIVtreatment,respectively’’(ibid).
Thereforejustlikeintheexamplesofmaternalhealth,TB(Tuberculosis)andHIV,inmyresearchICTsareconsideredtopossiblyalsohavearoleinmalariapreventionandcontrolinRwanda.ThenextsectiondiscussesthisfurtherbyexplainingthepotentialroleofICTinhealthsystemsindevelopingcountries.
2.3PotentialroleofICTinhealthsystemsofdevelopingcountriesDigitaltechnologiesandshareddataareexpectedtohavethepotentialto
radicallytransformthehealthcareinfrastructureofdevelopingcountries(Feganetal.,2011;Lucas,2008).Asdescribedearlier,whenICTsareusedeffectivelytheyhavealargepotentialtoboostinformationflowsandknowledge,andtoempowercitizens(Chetley,2006).Althoughstudiesagreeaboutthispotential,thereisnoagreementyetaboutthelikelynatureofthisimpact(Lucas,2008).
Lucas(2008)arguesthatadistinctioncanbemadebetweenICTinnovationswhichreinforcetheexistinghealthsystemsfrominnovationswhichhavethepotentialtochangethemcompletely.Manycurrentinnovationsfallunderthefirstcategory.Forexample,mobilephonenetworkstoenhancehealthreportingproceduresimprovetheprocessorinformationavailablewithinalreadyexistinghealthsystems.Withthesekindsofinnovationsthe‘’lawofunintendedconsequences’’mightplayarole,aschanginghealthreportingprocedureswasnotanobjectiveofthosedesigningthisinnovation(ibid).Innovationsthatfallunderthesecondcategoryandwhicharedevelopedtotransformexistinghealthsystemsarestillinearlyphasesofimplementation,withnotenoughresearchconductedtodeterminetheirrelevance,costeffectivenessandapplicability(Chetley,2006).Thismakesithardforgovernmentsofdevelopingcountriestodecideontheirinvestmentpriorities(ibid).Again,inbothcategories,itisthepromisingabilityofICT,itspowertoquicklydeveloplocal,nationalandglobalnetworksaroundparticularissuesthatmaystimulatearadicalchangeinthewayhealthsystemsareorganized(Lucas,2008).MythesiscomplimentsthisliteraturebyanalyzinghowICTsareusedinthehealthsystemaroundmalariapreventionandcontrolinRuhuha.Asmentionedearlierinthisparagraph,itishardforgovernmentsofdevelopingcountriestodecideontheirinvestmentprioritiesregardingICTs.ThefollowingsectiondescribesRwanda’sattitudetowardsICTinvestmentsandprovidesabackgroundofRwanda’sICTenvironment.
2.4RwandaICThubThegovernmentofRwandaistryingtopositionRwandaasaregionalICT
hubbycreatingaconducivelegalandregulatoryframework,availabilityofgoodinfrastructureandagrowingandinnovativehumanresourcebase(GoR,2015).Beingoneofthemosttechnologicallydeficientcountriestwodecadesago,RwandahasmaderapidprogressinICTdevelopmentincomparisonwithother

5
countriesinSub-SaharaAfrica(Mwangi,2006).AccordingtoMwangi(2006)thisisbecauseofthepolicyenvironment,politicalleadership,emigrantsandrefugeereturnees,andbecauseofnetworkingwithepistemiccommunities(seetable1below).Table1:FactorsthatinfluencedrapidICTdevelopmentinRwanda(Mwangi,2006)Factors ExplanationUnder-contestedpolicyenvironment
-Thecivilwardestroyedpreexistingpoliticalinstitutions,allowingthedevelopmentofICTaspartofthesocialconstructionofthestate,togiveitanewhistoryandidentity.-Rwanda’sdevelopmentframeworkande-governmentinitiativesarepremisedonaneoliberalagenda,whichminimizesfurtheropportunitiesforforeigninterference.-Noorganizedinterest-grouppoliticsthatmighthavecontestedeffortstoestablishthee-governmentsystem.Domesticandnon-stateactorswerefocusingonhumanitarianworkandstatereconstruction.Themainsourceofopposition,Rwandeserefugeesandexiles,lacksavisibleandeffectivefootholddomesticallyorintheinternationalcommunity.
Politicalleadership -BypersonallyengagingwiththevisionofaRwandeseinformationsociety,Kagamewasabletoidentifywithitandassignahighprioritytoitsdevelopment.-Kagamebecamethecountry’sembodimentofthenewRwanda,andhiscommitmenttothevisionhasenabledhimtomobilizesubstantialfinancialresourcesfortheprocess.-TheshiftbyallmembersoftheTransitionalNationalAssemblytoanelectronicconductofHouseandSenatebusinessislikelytospillovertomembers’localofficesandinteractionswithotherpublicagencies,andtherebybroadenandentrenchthesystem.
Emigrantsandrefugeereturnees
-CalledonpowerfulsuccessimagesofSingaporeandSouthKorea-Injectedasubstantial,badlyneededhumanresourceinputintothesystemintheaftermathofthegenocide-Supporteditsdiffusionbecauseofbeinghighlyskilledandsocializedintoe-governmentthroughexposureabroad-Theyprovidedfinancialinvestmentstokick-startthedevelopmentofane-governmentsystem
(International)epistemiccommunities
-RwandaturnedtotheITepistemic(knowledge)community;thatis,globalnetworksofITexpertsthattheyhadengagedwithduringtheircareersabroad,andthroughregionalintergovernmentalorganizations-RwandaalsostartedtappingintoprivateinitiativesthatsupportITdevelopment
ThepotentialroleofICTsanditsusedependoncultural,politicaland
socialfactors(Panir,2011).ICTinterventionsareoftentechnologicallydrivenandsocio-politicalfactorsareoftenignored,causinghealthrelatedICTprojectstofail(ibid).Thefactorsintable1areimportanttogetanunderstandingofthehistoricalpoliticalfactorsthatinfluencedthecurrentcontextofICTuseinRwanda.Firstofall,theunder-contestedpolicyenvironmentandpresidentKagame’spoliticalleadershipenabledthegovernmenttodevelopICTpoliciesallowingthedevelopmentofICTaspartofthesocialconstructionofthestate(Mwangi,2006).Furthermore,emigrantsandrefugeereturneessupportedthedevelopmentofane-governmentsystembyprovidingskills,knowledge,financialinvestmentsandbytappingintotheirglobalnetworksofITexpertsthattheyhadengagedwithduringtheircareersabroad(ibid).AlsoShiferawandZolfo(2012)arguethatthesuccessorfailureofICTinterventionsinhealth

6
systemsindevelopingcountriesdonotonlyrelyontechnologicalfactors,butalsorelyonmultisectorialinvolvementofstakeholders,capacitybuilding,e-governance,effectivehumanresourcemanagement,andonanenablingpolicyenvironment.ThenextsectiondescribestheparticularICTinterventionsinRwanda’shealthsystem.
2.5ICThealthinitiativesandpoliciesinRwandaICTisafastdevelopingindustryinRwanda(Frasieretal.,2008).This
developmentislargelysupportedbytheGovernmentofRwanda,astheprivatemarkethasnotcomeup.Therefore,thegovernmentofRwandaisinvolvedinallleadinginitiativesandemergingtechnologies.Theyhavemadeanefforttotrytointegratetechnologyintothehealthcaresystem.Rwandahasespeciallybeenapioneerinthefieldsofelectronichealthrecordsandnationalreportingsystem.Frasieretal.(2008)identifiedsixmajorinitiativesinhealthinformationtechnologyinRwandain2008,seetable2below.Table2:MajorinitiativesinhealthinformationtechnologyinRwanda(Frasieretal,2008)Initiative ExplanationOpenMRS Anopen-sourceMedicalRecordsSystemthattracks
patient-leveldataTracPlusandTRACnet Monthlymonitoringofinfectiousdiseasesincluding
HIV/AIDS,TB,andMalariaCAMERWA DrugandmedicalsupplymanagementsystemTelemedicine ICTusedtodeliverhealthandhealthcareservices,
informationandeducationtogeographicallyseparateparties
HealthManagementInformationSystems(HMIS)
Systemsthatintegratedatacollectionprocessing,reporting,anduseoftheinformationforprogrammaticdecision-making
E-Learning UseofICTininstructionofA2-levelnursesforpromotiontoA1status
Asmentionedearlier,thegovernmentofRwandadevelopedanational
ICTstrategyandplanin2015(GoR,2015).ThegovernmentofRwandawantstoleverageICTinallsectorstotransformRwandaintoaninformation-richandknowledgebasedeconomyby2020.ThisnationalICTplanincludesthreecommunitydevelopmentprojectsthataredirectlyrelatedtohealth,namely1)CommunityHealthWorkerReportingandInformationSystem,2)HealthInsuranceInformationSystem,and3)Telemedicine,whichis“anapplicationofclinicalmedicinewheremedicalinformationistransferredthroughaudio-visualmediaandothertechnologiesforpurposesofdiagnosingortreatingpatients”(ibid).ThecommunitydevelopmentprojectsaimtoimprovehealthcaredeliverythroughICTbyincreasingICTusage,accessandawarenesswithincommunities,improveaccesstoinformationandthereforeincreaseparticipationthroughICT,andtofacilitatetheprovisionofbasichealthservicestocommunitiesusingICT(ibid).Asexplainedinsection2.3,adistinctioncanbemadebetweenICTinnovationsthatarepartiallyunintendedandthosethatarespecificallydesignedforhealthsystems.TheinitiativesinhealthinformationtechnologyinRwandathatarementionedabovefallunderthesecondcategoryandarespecificallydesignedtoimprovethehealthsystem.Thecontributionofmyresearchisabouttheroleofspecificallydesignedinterventionsandthe

7
partiallyunintendedimpactofmobilephonesonmalariapreventionandcontrolinRuhuha.
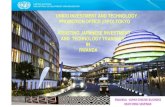
2.6MalariapreventionandcontrolinRuhuha,Rwanda RuhuhasectorinBugeseraDistrictintheeasternprovinceofRwanda(seefigure1below)isamalariaepidemiczone.Thissectoristhelocallevelofanalysisandislocated42kmfromKigali.Thenumberofhouseholdsinthisareaisestimatedat5098with23,893individuallivingin35differentvillages(Ingabireetal,2016b).
Figure1:LocationRuhuhasectorintheredcircle(Rulisaetal,2013)
FourstudiesrelatedtomalariapreventionandcontrolhavebeenconductedinRuhuha,Rwanda.Thefirststudyinvestigatedthepotentialrolesofcommunitystakeholdersinmalariaelimination(Ingabireetal,2014).Long-lastinginsecticidalnets(LLIN),indoorresidualspraying(IRS)andmalariacasetreatmentwithartemisinin-basedcombinationtherapy(ACT)mightreducebutnotleadtotheeliminationofmalaria(Ingabireetal,2015).Therefore,thesecondstudyanalyzedfactorshinderingtheacceptabilityanduseofmalariapreventivemeasures(ibid).Thethirdresearchconductedastakeholderanalysistoexplorepotentialstakeholdersfromnationaltolocalleveltoanalyzewhomtoinvolveforaspecificprojectactivityandthesuitabletimetodoso(Ingabire,2016a).Thelaststudyidentifiedmalariapatternsintheregionanddeterminedbehavioralandenvironmentalaspectsthatcontributetomalariatransmission(Ingabire,2016b).Thismeansthatstudiestoanalyzethepotentialrolesofcommunitymembers,thefactorshinderingtheacceptabilityofpreventivemeasures,stakeholderanalysistoassesswhotoinvolveinspecificprojectactivities,andmalariapatternsandenvironmentalaspectsthatcontributetomalariatransmissionhavebeenconductedalready.

8
MythesiscomplementsthisexistingliteraturewithananalysisoftheroleofICTsandgovernanceprocessesinmalariapreventionandcontrolinRuhuha.MythesisaddsanotherdimensiontotheexistingknowledgebyanalyzingthecommunicationandinformationflowsbetweenactorsandtherolesofICTsinmalariapreventionandcontrolinRuhuha.
2.7ICTsforsustainableruraldevelopmentThemajorityoftheworld’spoor(around75%)liveinruralareas(Panir,
2011).Thesepooraswellashealthprofessionalshavebeenatargetofhealthrelatedmillenniumdevelopmentgoals(ibid).Furthermore,thethirdgoalofthesustainabledevelopmentgoalsdescribes‘’healthylivesandpromotingthewell-beingforallatallagesisessentialtosustainabledevelopment’’(UnitedNations,n.d.).
TheconceptofICThasbecomeinformation-centeredandhastworoles(Panir,2011).Thefirstroleistheprocessofhandlingdataelectronically.Inthisprocess,dataischangedintoinformationordataismovedfromsourcestorecipients.ThesecondroleisturninginformationintoknowledgewhenICTsfacilitateassourcesofoutcome.Thisknowledgecanresultintakingaction,learningorindecision-makingprocesses(ibid).Whenthesetworolesareappropriatelyimplementedtheycanbecomestrongenginesofsocial,economicandpoliticalempowerment(Nayaketal.,2010).ICTscancreateinformationrichsocietiesbystimulatingcommunicationandinformationsharingamongruralandmarginalizedpeople.Thiscansubsequentlyempowerruralcommunitiestobeabletocontributetodevelopmentprocesses.Furthermore,ICTcouldcreatemoretransparentandefficientgovernmentprocessesthatalsoadvanceempowermentandparticipationoflocalcommunities(ibid).
InthisliteraturereviewIarguedthatICTsareexpectedtohavealargepotentialtohaveapositiveimpactoninformationflows,knowledge,andtheempowermentofcitizensinhealthsystemsindevelopingcountries.ThegovernmentofRwandahasimplementedseveralICThealthinitiatives.RuhuhasectorinBugeseraDistrictinRwandaisamalariaepidemiczone.Severalstudiesrelatedtomalariapreventionandcontrolhavebeenconductedinthisarea.MythesiscomplementsthisliteraturewithananalysisoftheroleofICTsininformationandcommunicationflowsandingovernanceprocessesinmalariapreventionandcontrolinRuhuha.Thefollowingchapterprovidesmoreinformationabouttheobjectiveandrelevanceofmythesis.

9
3.Theoreticalframework
3.1RelevanceandmainobjectiveofthestudyIntheliteraturereview,IdefinedhealthsystemsandICTsfromthepoint
ofviewofaccesstoexpertinformationandknowledge.Furthermore,IprovidedbackgroundinformationonICTpoliciesandhealthinitiativesinRwanda,introducingtheresearchsiteRuhuhasector.Iarguedthatmythesisresearchisrelevant,becausetheroleofinformation,andinparticularICTs,inmalariapreventionandcontrolinRwanda’shealthsystemhasnotbeenstudiedextensively.
Inaddition,abroadstreamofliteratureassertsthattheprocessofICTuseisanespeciallycomplexphenomenonindevelopingcountries(WalshamandSahay,2006).ICTsarealargepotentialbenefittoallpublicandprivatesectorsatvariouslevels(ibid).BothNayaketal.(2010)andSahayandWalsham(1995)stresstheneedformulti-levelanalysisoftheinteractionofactorsatvariouslevelsinICTimplementationanduse.BothnationalandlocalpowerrelationsinfluencetheeffectivenessandpotentialofICTuseindevelopingcountries(Nayaketal.,2010).Therefore,politicalawarenessandanalysisofalllevelsarecrucial(ibid).WalshamandSahay(2006)state‘’itisimportanttostudytheinteractionofthesedifferentactorsandtheprocessofICTimplementationanduse”.TheywouldliketocontinuetoseemoreresearchonforexampletheroleofICTsonlarge-scalegovernmentsystems,butalsoresearchrelatedtotheroleofICToncommunitieswouldbeavaluablefocusaccordingtothem(ibid).MythesiscontributestothisdiscussionbyanalyzingtheroleofICTsininformationandcommunicationflowsofactorsandgovernancearrangementsinthehealthsystemregardingmalariapreventionandcontrolinRuhuhaviaamulti-levelanalysis,involvingactorsfromthecommunity,districtandnationallevel.ThisisdonebecausethereisalackofunderstandingabouttheroleofICTsininformationandcommunicationandinthegovernancearrangementsinmalariapreventionandcontrolinRwanda.Forthisreason,amulti-levelanalysisisconductedtoanalyzetheroleofICTsininformationandcommunicationflowsofactorsinvolvedinmalariapreventionandcontrolinRuhuhaandinthesegovernancearrangements.
3.2ICTsandcollectiveaction:introducingOstrom’sdesignprinciplesSeinandHarindranath(2004)statethat‘’ICTessentiallyrelatesto
enhancinganindividual’scapabilitythroughempowermentandknowledge’’.ThisexplanationhasanindividualemphasisandfocusesonICTonlyinfluencingthedevelopmentofindividualcapabilities.Oxoby(2009)criticizesthisviewbyarguingthatindividualsarenotsociallyexcludedanddependonsocialnetworkstomakeupforalackofindividualresources.Thesesocialnetworkscanfacilitatecollectiveaction(Thapaetal.,2012).Gilbert(2006)describesthat‘’Collectiveactionrequiresajointcommitmentwhichbindsgroupmembersthroughasharedandpersistingreasontocommitandobligethemtoactasagreedupon’’.Ibrahim(2006)states‘’Collectivecapabilityisnotmerelythesumofindividualcapabilities’’,but‘’Rather,thesearepropertiesofagroupwhichanindividualalonewouldneitherhavenorbeabletoachieveifhe/shedidnotjoinacollectivity”.Thapaetal.(2012)explainthatICTsdonotonlyenhanceanindividualscapabilitiesbutcanfacilitateinthebuildingofcollectiveactionby

10
increasingflowsofinformation,socialnetworking,participation,transparency,andinteractionsamongcommunitymembersthatfacilitatemaintainingtrust,acceptanceandalignmentnecessaryforsuccessfulcooperation.
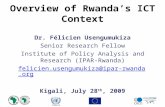
ElinorOstromcontributedtotheunderstandingofcollectiveaction(HoldenandTilahun,2018).In2009shereceivedtheNobelPrizeineconomicsforherworkbyshowingthat‘’whencertainconditionsaremet,groupsofpeoplearecapableofsustainablymanagingcommonresources’’(Wilsonetal,2013).Ostromanalyzedalargenumberofworldwidecasestudiesinwhichgroupsattemptedtomanagecommon-poolresources,suchasfisheries,irrigationsystems,pasturesandforests(Wilsonetal,2013).Byanalyzingthecasestudiessheidentifiedconditionsforsuccessfulcollectiveactiontosecuresustainablemanagementofthesenaturalresources(HoldenandTilahun,2018).Basedontheseconditionssheproposedeightdesignprinciples(seefigure2below).Theseprinciplesweredesignedtounderstandtheimportantconditionsoftheinstitutionalarrangementsthatattainedgoodoutcome,oppositetogroupswhoseeffortsfailed(Wilsonetal,2013).Ostrom(1993)describesthat:
‘‘By‘designprinciple’ismeantacharacteristicthathelpstoaccountforthesuccessoftheseinstitutionsinsustainingthephysicalworksandgainingthecomplianceofgenerationsofuserstotherulesinuse’’.
Figure2:Ostrom’sDesignPrinciples(Wilsonetal.,2013)
Thedesignprincipleswereinitiallycreatedtomanagecommon-poolresourcessuchasfisheries,irrigationsystemsandforests.Wilsonetal.(2013)arguethatbecauseofthetheoreticalgenerality,thedesignprinciplescanbegeneralizedtoberelevantforamuchwiderrangeofapplicationthancommonpoolresourcegroups.Theycanbeusedasapracticalguidetonearlyanygroupwhosemembersmustcooperateandworktogethertoachieveasharedgoal(ibid).
Thecommonsareeverycommoninterestthatcanbesharedbyagroupofpeople.Thedifferencebetweencommongoods(orcommonresources)andpublicgoodsisthatcommongoodsarerivalrousandpublicgoodsarenon-rivalrous.Examplesofpublicgoodsaretheairthatwebreatheorthewaterthat

11
wedrink.Theyarenon-rivalandindividualsarenotexcludablefromthesepublicgoods.Publicbadsarethesymmetryofpublicgoods.Asexplainedearlier,publicgoodsaretheairthatwebreatheorthewaterthatwedrink.Nowexamplesofpublicbadsareairpollutionorwaterpollution.Ifairgetspollutedthisisapublicbad,becauseindividualscannotexcludethemselvesfrombreathingthispollutedairanditisnon-rivalrousasbreathingpollutedairdoesnotdiminishthepollutedairforotherindividuals.Rulesthatarecreatedforpublicbadsaredifferentfromrulesforpublicgoods,asrulesforpublicbadsareaboutavoidingasharedriskwhilerulesforapublicgoodareaboutsharingabenefit.Anotherexampleofapublicgoodispublichealth.Diseasesthreatenhealthasapublicgoodandareapublicbad.Inthisresearch,Iconsiderthediseasemalariaasapublicbad.Justlikewithwaterandairpollution,thereisnorivalandindividualsarenotexcludablefromgettingmalaria.Malariaisadiseasethatistransmittedifaninfectedvectorstingsahumanbeing.Therefore,everyindividualhasaroleinpreventingthespreadofthediseaseandmalariaisapublicbad.Ifanindividualdoesnottakepreventivemeasuresagainstmalariathisisathreattowardsotherpersonseffortstoreducethepublicbadandtoimprovehealth.Thismeansthatindividualsinacommonsdilemmaarecapturedinaninescapableprocessfromwhichtheycannotremovethemselves(Ostrom,1999).ImprovedcommunicationthroughICTsholdsapromisetomoreeffectivelymonitortheapplicationofpreventivemeasuresbyfacilitatingimprovedcommunication,negotiationanddiscussion.ThisiswhyimprovedcommunicationflowsthroughICTscouldplayaroleinimprovingpublicbad(malaria)governance.Difficultiesthatariseincommonsdilemma’sarehowtoassureallindividualshaveasharedperspectiveoftheproblemtheyneedtosolve,howtocreateruleswhichareagreeabletoalmosteveryone,howtomonitortomakesurethatthosebreakingtherulesaresanctioned,andhowtoguaranteethattrustandcooperationarenotthreatened.TocopewiththeseissuesOstrom(1999)arguedthatpolicyanalystsshouldchangetheirviewsfromindependentgovernancesystemsdirectedbyasinglecentertopolycentricgovernancesystemstomanageoranalyzethesecommonsmoreeffectively.
MythesisbuildsonOstrom’stheorybyanalyzingtheroleofICTsinthegovernancearrangementsofactorsthataredealingwithmalariaasapublicbadinRuhuha.FollowingOstrom,Iscrutinizetheexistingrulesforcontainingmalaria(avoidingasharedrisk)andtheroleofcommunicationinestablishingandmaintainingthem.Foreffectivecollectiveaction,differentactorswithinthemalaria-affectedareaofRuhuhahavetocooperateandworktogethertoachieveasharedgoalofbattlingthedisease.Inthenextsection,Ioutlinemyresearchquestions,showinghowfocusingoncommunication,itsusesandmisusesallowsmetoelaborateonOstrom’sdesignprinciplesofeffectivelypreventingapublicbad.
3.3ResearchquestionsTherearethreemainquestionsguidingmyresearchwithseveralsub
questions.ThemainobjectiveofmythesisistoinvestigatetheroleofICTsinthepreventionandcontrolofmalariaasapublicbadinRuhuhasector,Rwanda.Theresearchquestionsarethefollowing:

12
1.WhatarethecommunicationandinformationflowsrelatedtomalariainRwanda’shealthsystem?
• Whathealthsystemsandgovernancenetworksarecurrentlyinplacetomonitorandanalyzemalariaoutbreaks?
• Howistheinformationsharedinthesesystems/networks?Whataretherelationshipsbetweendifferentinstitutionallevels/actors/networks?Howdotheyinteract?Whatistherelationbetweenscalelevels?Howaretheyconnected?Howaremalariacontrolandpreventionstrategiescommunicatedtocommunities?
2.WhatistheroleofICTsinthesesystems/networks?
• WhataretheeffectsoftheemergenceofICTsonhealthsystemsandthegovernancenetworksrelatedtomalariacontrolandprevention?
• TowhatextentdoestheemergenceofICTsinRwandachangetheroleandlegitimacyofactorsinhealthsystemsandgovernancenetworks?
• HowarethenationalICTpoliciesandstrategiesrelatedtolocaloutcomesinICTuseandmalariaprevention?(ArenationalICTpoliciesdeadpiecesofpaperandirrelevantforcesatthelocallevel,orhavethesestrategies,plansandpoliciesincreasinglybeenusedtoimprovepublichealthandmalariaprevention?)
3.Whatisthepotentialofmobile-basedcommunicationtoimprovethecollectivegovernanceofapublicbad(Ostrom,1993)?

13
4.Methodology
Thechosenmethodtogetthedataneededwastodoanexploratorystudywithqualitativeresearch.ThisapproachwaschosenbecauseinexistingliteraturethereisnotalotwrittenabouttheroleofICTsandtheroleofinformationinmalariapreventionandcontrol.Forthisreasonanexploratorystudywithqualitativeresearchwaschosenwiththeaimtogainknowledgeandtogiveinsightsintothesetopics.Inordertoanswertheresearchquestionsdifferentstepshadtobetaken.Thischapterdescribesthemethodsfordatacollectionandhowthedatawasanalyzed.
4.1DatacollectionDatawascollectedintwoways,bygatheringsecondarydataandby
conductinginterviews.Bothmethodsareexplainedinmoredetailbelow.
4.1.1SecondarydataFirstofall,secondarydatawasgatheredtryingtoidentifyhealthsystems,
governancenetworks,andfactsrelatedtomalariapreventionandcontrolinRwanda.Thesepolicydocumentsincludedthepresident’smalariainitiativeRwanda,thenationalmalariacontrolprogram,andhealthsectorstrategicplansamongothers.Moreover,literaturewasusedtoexploreanddefinekeytermssuchasICTs,healthsystem,andpublicbad.Furthermore,byanalyzingpreviousstudiesaboutmalariaconductedinRuhuhasectorpotentialstakeholdersthatcouldbeinterviewedwereidentified.
4.1.2InterviewsDuringfieldresearchinRuhuhasectorinRwandaactorsrelatedtothe
managementandcontrolofmalariawereinterviewed(adetailedoverviewoftheintervieweescanbefoundinappendix1).Thiswasdonethroughsemi-structuredinterviews(thetopiclistsoftheinterviewscanbefoundinappendix2).Thesamplingmethodthatwasusedispurposivesampling.FirstactorswereidentifiedbyanalyzingpreviousstudiesaboutmalariainRuhuha.ThesestudiesareconductedbyIngabireetal.(2014,2015,2016a,2016b).Secondly,theselectionofrespondentswasconsultedwithprofessorMutesa(supervisorofthetwoPhDstudentswithintheEVOCA1Rwandacasestudy)bygoingthroughthisdraftedlistofactorsthatcouldpotentiallybeinterviewed,withreferencetotherelevancefortheresearchquestionsandtheoverallfeasibilityofthestudy(timingandavailabilitylimitations).Afterwards,acontractwasmadewithRuhuhahealthcentertofacilitatemyresearch.Theheadofthehealthcenterandthedatamanagerofthehealthcenterweregivenascheduleoftheactorsthatwereidentifiedtobeinterviewed.AccordingtothisscheduleRuhuhahealthcenterstaffarrangedtherequestedactors/participantstobeatthehealthcenterforaninterview.Therefore,thehealthcenterselectedtheparticipantsthat
1EVOCA(EnvironmentalVirtualObservatoriesForConnectiveAction)isacollaborativeinterdisciplinaryprojectofWageningenUniversityandsevenpartnerinstitutions.Itfocusesonknowledgesharingplatforms(knownasEnvironmentalVirtualObservatories,EVOs)andtheirpotentialtotransformthedevelopmentlandscapeinfivecasestudyareasinruralAfrica.

14
participatedinmyresearchsuchasthecommunitymembers,cooperatives,religiousleader,localleader,pharmacists,teacher,communityhealthworkers,amongothers.ForthedistrictandnationallevelcontactsoftheEVOCAprojectwereusedandtheinterviewswerescheduledandaccompaniedbyDominaAsingizweandMarilynMurindahabi(PhDresearcherswithintheEVOCAproject).Theinterviewswereallrecordedbyanelectronicdevice.Duringtheinterviewsaresearchassistant/translatorwashiredtotranslateinterviewsatthecommunitylevel.TheinterviewsatthedistrictandnationallevelwereconductedinEnglish.
4.2DataanalysisAfterfinishingthefieldworktheinterviewsweretranscribed.The
programAtlas.tiwasusedtocodeandanalyzedata.Aninductiveapproachwasusedasacodingtechnique,sothecategoriestocodeemergedfromthedata.Anoverviewofthecodescanbefoundinappendix3.

15
5.Resultsanddiscussion
Thischapterdescribesandanalyzestheresultsoftheresearch.ItstartswithastakeholderanalysisofactorsinvolvedinmalariapreventionandcontrolinRuhuha.Thisisfollowedbyananalysisoftheperceptionsofactorsaboutthefutureroleofmobilephones,thesituationregardingmalaria,knowledgeandmisconceptions,trust,andsharedperspectiveoftheproblem.Thelastsectionanalyzesthemalariagovernancearrangements,thecompliancewithOstrom’sdesignprinciples,andtheroleofICTsinthegovernancearrangements.
5.1StakeholderanalysisThisfirstsectionidentifiesthestakeholdersinvolvedinmalaria
preventionandcontrolinRuhuhaandanalyzestheirroleinmalariapreventionandcontrol.Theactorsthatwereinterviewedduringmyresearchcanbecategorizedincommunity,districtandnationallevel(seetable3).Furthermore,therearetwotypesofactorsonthecommunitylevel.Thefirsttypeofactorsarestakeholdersthatarerelatedtohealth.Thesecondtypeofactorsareotherstakeholderswhoarenotdirectlyrelatedtohealth,butwhoalsoplayaroleinmalariapreventionandcontrolinRuhuha.Table3:ActorsinRwanda’shealthsystemregardingmalariapreventionandcontrolinRuhuha CommunityLevel DistrictLevel NationalLevelActorsthatarehealthrelated
CommunityHealthWorkers
NyamataDistrictHospital
RwandaBiomedicalCenter(RBC)
RuhuhaHealthCenter
NationalHealthInsuranceScheme
Pharmacies CommunityMalariaActionTeams(CMATs)
MalariaEliminationProgram(MEPR)
TraditionalHealers OtheractorsthathavearoleinmalariapreventionandcontrolinRuhuha
Communitymembers
LocalLeaders Religiousleaders Schools Cooperatives
Itwasdefinedintheliteraturereviewthathealthsystemscanbe
analyzedas‘’waysoforganizingaccesstoexpertknowledge’’(BloomandStanding,2008).Asillustratedinthetableabove(table3),theactorsinmalariapreventionandcontrolinRuhuhaincludepublicandprivateactorsandmodernandtraditionalprovidersforcommunitymemberstoaccessknowledge.Nowwillbeanalyzedhowthishealthsystemisorganizedandhowthewaysofaccess

16
toexpertknowledgeisorganizedusingamulti-levelanalysisstartingwiththecommunitylevel,followedbythedistrictlevelandlastlythenationallevel.
5.1.1CommunitylevelAsexplainedabove,therearetwotypesofactorsonthecommunitylevel.
Firsttheroleofthehealthrelatedactorswillbedescribedindifferentsub-sections.Afterwardstheroleoftheactorswhoarenotdirectlyrelatedtohealthbutwhoalsoplayaroleinmalariapreventionwillbedescribed.
CommunityHealthWorkersEveryvillageinRuhuhasub-sectorhastwoorthreecommunityhealth
workers.Thecommunityhealthworkersareelectedbythecommunitymembersinavillage.Therearerulesthatarefollowedwhilerecruitingcommunityhealthworkers.Thoseruleshavecommunityvalues,suchasbeingintegrated,beinghonest,havingonenationality,andknowinghowtoreadandwrite.Thereisnoenddatetothepositionofacommunityhealthworker.Inthepast,communityhealthworkersusedtotreatchildrenunderfiveyearsold.Theyusedtotreatmalnutritionandmalnutritionhasnowimproved.Therefore,theynowtreatthewholecommunitywhenitcomestoillnessesandtheyadviceregardingpregnancies.Communityhealthworkersreceivedtrainingtoadviseandimpartcommunitymembersaboutmalaria,asmalariahasbecomeaprobleminthecommunity.Theycantestcommunitymemberstocheckiftheyaresufferingfrommalariaandgivetabletswherenecessary.Furthermore,whentheyseeaseveremalariapatienttheycantransferthispersontothehealthcenter.Communityhealthworkersalsovisitcommunitymember’shomesonceamonthtoteachpeopledifferentwaysoffightingagainstmalaria.Duringthesevisitstheygivetheservicesthatthepeopleneedandtheycomeintothehousetocheckwhethertherearebednets.Whenevertheyseethatthatthereisnobednetthecommunityhealthworkeradvisesabouthowtopreventmalariaandtheyexplainhowtheycangetbednets.Theprocedureofgettingbednetsstartsduringthevisitsofthecommunityhealthworkerswhowritedownallthepeoplewhodonotpossesbednets.Thenthecommunityhealthworkersgotothehealthcentertoreportthepeoplewhodonothavemosquitonets.Wheneverthebednetsareavailable,themessengers(inchargeofadvertisingandspreadinginformation)informvillagerstopickthemosquitonetsatthehealthcenter.Furthermore,thecommunityhealthworkersmobilizecommunitymemberstogethealthinsuranceintime.
RuhuhaHealthCenterTheroleofRuhuhahealthcenteristoteachandadvisecommunity
membersaboutthecausesofmalaria,preventionmeasures,andtocometothehealthcenterassoonaspossiblewhenevertheysufferfrommalariaorwhentheyidentifysignsofmalaria.Therefore,thehealthcenterteachescommunitymembersmeasuresoffightingagainstmalariaandcurepeopleintimewhoarecomingformedicaltreatment.Furthermore,thehealthcenterstaffgoesintotheareatocheckifthemalariapreventionandcontrolmeasuresarefollowedandusedbycommunitymembers.Theycheckwhethercommunitymembersusemosquitonets,removestagnantwateraroundthehouse,andwhethertheyclosewindowsanddoorsduringevenings.Thenursesofthehealthcenteralsooccasionallyhavedaysatthesectorsofficewheretheytreatcommunity

17
memberswhodonothavemedicalinsurance.Furthermore,thehealthcentersupervisesthecommunityhealthworkers.Nexttotrainingcommunitymemberstheyalsoadviseandtraincommunityhealthworkersaboutmalariapreventionandcontrolmeasures.
PharmaciesThereisapharmacyinRuhuhaatthehealthcenter.Inaddition,thereare
alsoprivatepharmacieswithinvillages.TheprivatepharmaciesarelicensedbytheMinistryofHealth.Theroleofthepharmaciesistoprovidemedicinestothecommunitymembers.Atthehealthcenterpharmacycommunitymemberswhohaveahealthinsurancecangettheirmedicinesforfreeoratlowcostastheyarereimbursedbytheinsurancesdependingontheirsocialcategory.Atthehealthcentercommunitymemberswhodonothaveahealthinsuranceneedtopayforexaminationandconsultationfeesbeforebeingabletobuymedicinesatthehealthcenterpharmacy.Forthisreason,communitymemberswhodonothaveamedicalinsuranceusuallygototheprivatepharmacies.Furthermore,alsocommunitymemberswhohavemoneyandwhodonotwanttowaitinlineatthehealthcenteroftenattendprivatepharmaciesbecauseitisaquickerwaytogetmedicinescomparedtothehealthcenterpharmacy.
MalariaEliminationProgram(MEPR)Themalariaeliminationprogramwasagroupofresearchers,whichwas
madeupoutoffivestudentswhoweredoingtheirPhDfromtheNetherlands.Theywereresearchersbuttheresearchhasended.Theirresearchhadtwointerventions.ThefirstonewastheapplicationofBti(Bacillusthuringiensisisraelensis).Btiisalarvicidingprocessthatkillsmosquitolarvaeinricefields.Thesecondinterventionwastheestablishmentofcommunitymalariaactionteams(CMATs),moreinformationaboutCMATsinthefollowingsub-section.
CommunityMalariaActionTeams(CMATs)Everyvillagehasacommunitymalariaactionteam.Thecommunity
malariaactionteamsexistofthreepeoplewhoareselectedtorepresentotherswithinavillage.Thethreemembersworktogethertofightagainstmalaria.Theseteamsareunderthesocialaffairsadministrationofthesectorsoffice.ThecommunitymalariaactionteamshaveameetingeverySaturday.Duringthesemeetingsthemobilizecommunitymemberstoreachthehealthcenterontimewhentheyaresufferingfrommalaria,tosensitizecommunitymembersabouttheroleofsleepinginmosquitonets,toclosewindowsduringtheevenings,tomobilizecommunitymemberstoacceptfumigatorsintotheirhouses,andtheyteachcommunitymemberstoremovestagnantwaterandbushesaroundtheirhouses.
TraditionalHealersInthepastcommunitymembersusedtogototraditionalhealers
whenevertheyweresufferingfromadisease.Nowadayscommunityhealthworkershavetakenoverthisroleandthemajorityofthecommunitymembersgotothecommunityhealthworkerstogetinformationorforexamination.However,therearestillanumberoftraditionalhealersinRuhuha.Acommunitymembermentionedthatinhisvillagetherearearoundfourpersonsinhisvillagewhohavepermissionfromthegovernmenttoworkasatraditionalhealerand

18
othertraditionalhealerswhohideintheirhouseswithoutbeinglicensedbythegovernment.Thetraditionalhealerthatwasinterviewedisatraditionalhealerandafarmeratthesametime.Heexplainedthatbecomingatraditionalhealerdependsonheritageandancestors.Hehasbeengiventhelegacyfromhisgrandfather.
Accordingtothetraditionalhealer,hisroleistocuretraditionalsicknessesandheadvisescommunitymembersaboutdifferentdiseases.Heexplainedthatthedifferencebetweentraditionalandnon-traditionalsicknessesisthattraditionalsicknessesarerelatedtobewitcheryandpoisonousactivities,whereasnon-traditionalsicknessesareillnessesthatrequirepeopletoreachhealthcenterandhospitals.Thetraditionalhealerexplainedthathedoesnotcuremalaria.Whenpeopleattendhishouseholdfornon-traditionalillnesseslikemalaria,headvisesthemtogotothehealthcenter.However,accordingtocommunitymemberstherearepeoplewhostillbelieveinthetraditionalhealers.Theyexplainedthatthesecommunitymembersattendtraditionalhealersinsteadofgoingtohealthcenterstobetreatedwhensufferingfromanillness.Thetraditionalhealerswillthentellapatientthatheorsheisnotsufferingfromotherdiseasesexceptbewitcheryormagicpower.Afterthatapersonmaydieofmalariawhereastheherbalistsortraditionalhealersaresayingthepersonissufferingfrombewitcheryandthepatientreachesthehealthcentertoolatewhenmalariahasreachedseverestages.
OtheractorsthatarepartofmalariapreventionandcontrolinRuhuhaThefollowingparagraphsdescribetherolesofthenon-healthrelated
actorsinmalariapreventionandcontrolinRuhuha.
CommunitymembersTherearetwogroupsofpeoplewithinvillages,whichareclubandcare.
Bothclubandcareareformalgovernancegroupsmobilizedthroughsectorlevelbythegovernment.Careisnotrelatedtomalariapreventionandcontrol,butitdealswithmoneyandloans.However,withinclubcommunitymembersoftentalkaboutmalaria.Clubexistsofallpeoplewithinavillageandthemeetingisonceaweek.Clubhelpspeopletosolveconflictswithintheirfamiliesandhelpspeopletobeawareofdifferentdiseases.Withinclubtheyadvisepeopleaboutmalariaandotherdiseases.Noclubcancometogetherwithoutacommunityhealthworker,whoisexpectedtoinformpeopleaboutmalariaandthewaysofpreventingmalaria.Furthermore,anotherroleofthecommunitymembersistofollowtherulesandregulationsregardingmalariapreventionandcontrolinRuhuha(moreinformationaboutthisin5.6.1).
LocalleadersLocalleadersareatcelllevelandbeingtheleaderisadailyjob.The
leaderofacellisnotelected,butgetsappointedforanunspecifiedtimeafterpassinganexam.Theroleofaleaderistomobilizecommunitymemberstobeawareofmalaria.Furthermore,theroleofaleaderistoadvocateandmakepeopleonhigherlevelsawareofproblemsthatareexperiencedbycommunitymemberswithinthecell.Whenthereisaproblemrelatedtomalaria,thelocalleadertalkstoleadersofhigherlevelstoinformthemaboutthisproblem.

19
ReligiousleadersTheroleofthereligiousleadersinmalariapreventionandcontrolisto
encouragepeopletopayforhealthinsurance.Peoplefromthesocialadministrationofsectorsometimesaskthechurchtoencouragepeopletogethealthinsurances,becausetheyknowthatpeoplegetitquicklywhenthepriestisannouncingit.Onsuchoccasions,theycangivecommunicationsrelatedtomalariaduringamass.
SchoolsWithinprimaryschoolsmalariaisdiscussedwithindifferentsubjects.
MalariaisdiscussedduringSocialStudies,Kinyarwanda,EnglishandSciences.Accordingtotheprimaryschoolteacher,eachofthebooksofthesesubjectscontainsachaptertalkingaboutmalaria.Theteacherisresponsibleforteachingchildrenhowmalariaattackspeople,howitispreventedandhowtheymayhelpneighborsandfriendshowtofightagainstmalaria.
CooperativesTherearedifferentcooperativeswithinRuhuhaandtworicecooperative
memberswereinterviewed.Theyexplainedthataricecooperativecontainsaround900persons,andwithinthisbiggrouptherearesmallergroupsofaround40persons.Everygrouphasit’sownplace,thisplaceisdividedintosmallerplots,andwithinthoseplotseverypersonhashisorherownplot.Acooperativeismadeupoutofdifferentcategoriesofpersons.Forexample,therearealsocommunityhealthworkerswhoareamemberofacooperativeworkingasafarmer.Withinthecooperativethosecommunityhealthworkershelpthemtounderstandandtofightagainstmalariabyillustratingthemeasuresthatareusedsoastofightagainstit.
5.1.2DistrictLevelAtthedistrictlevelthereisoneactorrelatedtomalariapreventionand
controlinRuhuha,whichistheNyamataDistrictHospital.
NyamataDistrictHospitalTheroleofthedistricthospitalistosupervisethehealthcentersandthe
communityhealthworkers.Thedistricthospitalisinbetweenthecommunitylevelandthenationallevel.Theheadofthedistricthospitalexplainedthattheyashealthprofessionalsconnectthecentralleveltothelocalauthority,becausetheyhavemoreknowledgeaboutmalariacomparedtothehealthprofessionalsatthecommunitylevel.ThedistricthospitalforexampleworkstogetherwithRBCtotrainthehealthprofessionalsfromthehealthcentersandcommunityhealthworkers.Furthermore,thedistricthospitalhasadistrictpharmacythathasamandatetodistributedrugsinruralareastothehealthcenterpharmacies.
5.1.3NationalLevelOnthenationalleveltherearetwomajoractors,whicharetheRwanda
BiomedicalCenter(RBC)andtheNationalHealthInsuranceScheme.
RwandaBiomedicalCenterTheRwandaBiomedicalCenterisundertheMinistryofHealth.Theyhave
amalariadivisionandanationalmalariacontrolprogram.TheRwandabiomedicalcenterhasdifferentrolesregardingmalariapreventionandcontrol.

20
Thefirstroleistoensureprevention,treatmentanddiagnostics.InJanuary/February2017theydistributedbednetscoveringeachhousehold.Afterthedistributionofthesebednetstheydidnotfindadeclineofmalaria.Theydonotknowwhathappened.Furthermore,withintreatmenttheyalsousesprayingthehighburdendistrictasastrategy.Theyidentifiedeighthighburdendistricts,butonlysprayedfiveofthesedistrictsbecausetheydidnothaveenoughresourcestosprayalleight.Themosquitonetsandsprayingofhousestargetindoortransmissions.Fortreatmentanddiagnosticstheyarenowensuringtreatmentanddiagnosticofmalariatargetingallgroupsofage.ThesecondroleisoftheRwandanBiomedicalCenterisbehaviorcommunicationchange.Theyworktogetherwithlocalgovernmenttoensurebehavioralcommunicationchangefortreatmentandpreventionofmalaria.Theselocalgovernmentstakeholderstaketheleadinsensitizationandmobilizationtowardsbehaviorcommunicationchange.Thethirdroleismonitoringandevaluation.Formonitoringandevaluationtheyhavemonthlyreportstomonitorthenumberofmalariacases.ThefourthroleoftheRwandabiomedicalcenterisoperationalresearch.Theyconductoperationalresearchintermsofprevention,casemanagement,andinnovationsfortesting,preventionandtreatment.Thefifthroleismalariacontrol.TheRwandaBiomedicalCenterusedtohaveagoaltoeliminatemalariaby2017.However,nowinthenewstrategicplanfrom2013to2020theyhaveagoaltocontrolmalariaandtoreducethemalariaburden,becausetheyfoundoutthatmalariaeliminationisnoteasyastheyneedtomobilizemoreresources.
NationalHealthInsuranceSchemeTheNationalHealthInsuranceSchemehasdecentralizedservicesto30
administrativedistrictsinRwanda.ThismeansthatateveryadministrativedistrictthereisanRSSB(RwandaSocialSecurityBoard)branchwheremostoftheservicesareprovided.Forthecommunitybasedhealthinsurance,theyhaveanofficeoftwopeopleateveryhealthcenter.Intheseofficesathealthcenterscommunitymembersreceivetheirmembershipcards.Communitymembersalsogotothisofficewhentheywanttobetreated,theyarethengivenamedicalformandtheycanenterthehealthcenter.AccordingtotheintervieweefromtheNationalHealthInsuranceSchemeabove90%oftheRwandanpopulationhavemedicalinsurance.TheNationalHealthInsurancereimburseswhatisnotgivenforfreebythegovernment.Forexample,mosquitonetsandindoorresidualsprayingarenotreimbursedbecausethegovernmentprovidesthesemeasuresforfreetothecommunitymembers.Ifacommunitymemberfallssickthentheconsultation,laboratoryexamination,andmalariadrugsarepaidbytheinsurance.However,themalariadrugsaresubsidizedbythegovernmentanddevelopmentpartners,tomakethemaffordableforinsuranceinstitutionsorforthosewithoutamedicalinsurance.
Insummary,themostimportantactorsrelatedtomalariapreventionandcontrolinRuhuhaarethecommunityhealthworkers,CMATs,pharmacies,healthcenter,districthospital,andtheRwandaBiomedicalCenter.Theseareactorsinvolvedindiagnosing,treatingpatients,andmobilizingawarenessaboutmalariapreventionandcontrolmeasures.Inaddition,thereareotheractorssuchasthelocalleaders,religiousleaders,andschoolswhoplayaroleatraisingawarenessandknowledgeaboutmalariapreventionandcontrolmeasuresin

21
Ruhuha.Furthermore,theNationalHealthInsuranceSchemeistheretoprovideinsurancesandreimbursecostsofconsultation,laboratoryexaminationandmedicinestothosewhohaveinsurance.Moreover,thecommunitymembersmostimportantroleistofollowtherulesandregulationsregardingmalariapreventionandcontrolinRuhuha(moreinformationaboutthisin5.6.1).

22
5.2Informationandcommunication:actors,flowsandchannelsTheprevioussectionintroducedtheactorsinmalariapreventionand
controlinRuhuhaandidentifiedtheirrole.Thissectionanalyzestheinformationandcommunicationflowsbetweentheseactorsandthechannelsusedtosendorreceiveinformation.Firsttheinformationandcommunicationflowsbetweenactorsareanalyzed.AfterwardstheroleofICTsinmalariapreventionandcontrolinRuhuhaisdescribed.
5.2.1InformationandcommunicationflowsbetweenactorsThissub-sectionanalyzestheinformationandcommunicationflows
betweenthestakeholdersrelatedtomalariapreventionandcontrolinRuhuha.FriedmanandMiles(2006)describethatRowley’snetworktheorycanbe
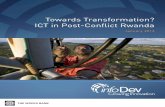
usedtomapstakeholdernetworks.Anetworkmapsinteractionsthatexistinstakeholderenvironments.Networkdensityandcentralityofstakeholdersareusedtoanalyzenetwork.Densityismainlyabouttheinterconnectednessbetweenstakeholders.Thecentralityshowsthepositionofastakeholderinthenetworkrelativelytootheractors.Whendensityincreasesthecommunicationbetweenstakeholdersimprovesanditislikelythatsharedexpectationsandbehaviorincreases.Themorecentralthepositionofastakeholderinanetwork,themorepowerthestakeholderhastoinfluence(ibid).Asdescribedearlier,thestakeholderenvironmentinthecaseofmythesisareactorsinvolvedinthepreventionandcontrolofmalariainRuhuha.Thefollowingmap(figure3)showsanetworkmapoftheinformationandcommunicationflowsaboutmalariabetweentheseactors.Italsoshowshowinformationisshared,eitherface-to-face,bymobilephone,SIScom,HMIS,radioorvideoprojections.
Figure3:Informationandcommunicationflowsaboutmalariabetweenactors
Ascanbeobservedfromfigure3,thecommunitymembershavethehighestdensityandthemostcentralpositioninthenetwork.Thismeansthattheyareinvolvedininformationandcommunicationflowsaboutmalariawiththemajorityofotheractors.Onthecommunitylevel,thehealthcenter,localleaders,andcommunityhealthworkersalsohaveahighnetworkdensity.Asdescribedinthestakeholderanalysis,thedistricthospitalconnectsthecentralleveltothelocalauthority.Thenetworkconfirmsthisbecausethedistricthospitalhasinformationandcommunicationflowstobothnationalandcommunitylevelactors.Inaddition,thedistricthospitalalsohasarelativelyhigh

23
networkdensityandmainlycommunicateswithhealthrelatedactors.Nexttothedistricthospital,thecommunityhealthworkersandthecommunitymembersalsohaveinformationandcommunicationflowsaboutmalariatoandfromactorsfromalllevels.Ascanbeanalyzedfromthenetwork,therearebothhealthandnon-healthrelatedactorswithalownetworkdensity.Thismeansthatthehealthrelatedactorsdonotnecessarilycommunicateorshareinformationaboutmalariawithahigheramountofactorscomparedtonon-healthrelatedactors.Stakeholdersthathavearelativelylownetworkdensityaretraditionalhealers,ricecooperatives,religiousleaders,CMATs,MEPR,privatepharmaciesandthenationalhealthinsurancescheme.AccordingtoFriedmanandMiles(2008),thismeansthatthereislimitedcommunicationandthereforelimitedcooperationwiththeseactorstopreventandcontrolmalaria.However,thenetworkdoesnotillustratedataaboutthefrequencyofcommunicationandquantityandqualityofinformationflowsaboutmalariabetweenactors.Therefore,actorswithalownetworkdensitymightstillhaveanimportantroleandcouldstillbeeffectiveininfluencingperceptionsandbehaviorregardingmalariapreventionandcontrol.Moreaboutthisisanalyzedinsections5.3and5.4.
InformationflowsinmalariapreventionandcontrolinRuhuhaarefacilitatedbyface-to-facecommunication;communicationusingmobilephonestocall,tosendtextmessages,toaccessradio,andtoaccesssocialmedia;reportsusingSIScom;reportsusingHMIS;andcommunicationthroughradioandvideoprojections.Table4givesanoverviewofhowthesecommunicationchannelsareusedacrossthedifferentlevels.Table4:ICTchannelsusedinmalariapreventionandcontrolinRuhuhaacrosslevels Tocommunity Todistrict TonationalFromcommunity
Face-to-face,mobilephone,SIScom
Face-to-face,mobilephone,HMIS
Mobilephone
Fromdistrict Face-to-face,mobilephone
Onlyoneactorincludedondistrictlevel
Face-to-face,mobilephone,HMIS
Fromnational Mobilephone,radio,videoprojections
Face-to-face,mobilephone
Face-to-face,mobilephone
Asillustratedintable5theICTsusedonthecommunitylevelareSIScom
andHMIS,whichareusedtoreportfromthecommunityhealthworkerstothehealthcenterandfromthehealthcentertothedistricthospital.Furthermore,face-to-facecommunicationisusedacrossalllevelsexceptbetweenthecommunityandnationallevel.OtherICTssuchasmobilephone,radioandvideoprojectionsareusedforcommunicationflowsfromthenationaltocommunitylevel,whilefromthecommunitytothenationallevelonlymobilephonesareusedasacommunicationchannel.Regardingthesimilaritiesanddifferencesbetweenhowstakeholderschoosetocommunicate,MEPR,traditionalhealersandricecooperativesonlycommunicateaboutmalariaface-to-facewithotherstakeholders.Allotheractorsalsousemobilephonesnexttoface-to-facecommunicationtoshareorreceiveinformationaboutmalaria.

24
Thefollowingsub-sectionsexplaintheinformationandcommunicationflowsofthenetworkinmoredetail,startingwiththecommunitylevelactors,andthenthedistrictlevelactorfollowedbythenationallevelactors.
5.2.1.1Communitylevel
CommunitymembersThecommunitymembershavethehighestdensityandthemostcentral
positioninthenetworkofinformationandcommunicationflows.Thecommunitymemberscommunicatewithlocalleaders,privatepharmacies,thehealthcenterpharmacy,communityhealthworkers,thehealthcenter,andthenationalhealthinsuranceschemebymobilephoneandface-to-face.Inaddition,theycommunicatetoreligiousleaders,personsfromthemalariaeliminationprogram,andthedistricthospitalface-to-face.Theseinformationandcommunicationflowsareexplainedmoredetailedintable5below.Table5:ExplanationinformationandcommunicationflowsfromcommunitymembersFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whattheinformationisabout
Face-to-faceAmongcommunitymembers
Athomewhenthereisavisitor,withintheneighborhood,withfriends,duringculturalevenings,duringspecialevenings(eveningsforadultstotalkaboutsocietalproblemsandproblemsintheirlives),whensomeoneissufferingfrommalariawithinthehousehold,orwhenapersoninthevillagehasdiedofmalaria.
Mosquitonetsandotherpreventionmeasures,wherethisepidemiccomesfrom,andwhyisitdifferentfromthepreviousone.Furthermore,theyalsodiscussthatthetreatmentdoesnotlastlong,forexampleifIgetmalariaitcomesbackafteronemonthortwoweeksandtheyadviseeachothertogetmoreknowledge.
Localleaders Whenevercommunitymembersaregatheredinmeetingswiththelocalleaderstheytalkaboutmalariaface-to-face.Examplesareduringvillagemeetingsorattheendofthemonthlypublicwork.Attheendofpublicworkthecommunitymemberssittogetherandtheleaderstalkaboutdifferentwaysofpreventingagainstmalaria.
Duringthesemeetingscommunitymembersdiscussandreportproblemssuchasmalaria.
CommunityHealthworkers
Thecommunitymemberscommunicateaboutmalariawithcommunityhealthworkersface-to-faceduringmeetingsandhomevisits.Therearemeetingswherethecommunityhealthworkershaveaspecifictimewhentheytalkaboutmalariatocommunitymembers.
Duringthesemeetingsandhomevisitsthecommunityhealthworkersteachandadvisecommunitymembersabouthowtopreventmalariabyremovingstagnantwaterthatsurroundsthehouse,tosleepinmosquitonetsduringthenight,toclosewindowsduringtheevening,tocutdowntrees,andbycleaningmosquitobreedingsites.Furthermore,thecommunityhealthworkerstellthecommunitymemberstheconsequencesofmalaria,toreachthehealthcenterearlywhentheyseesignsofmalaria,andaboutthepeopleatrisk.Thecommunityhealthworkerstellthemthat

25
especiallyyoungkidsandpregnantwomenarevulnerablegroups,althougheveryoneisatrisk.
Healthcenter Thecommunitymemberscommunicatewiththehealthcenterface-to-facewhentheycomeformedicaltreatmentatthehealthcenter.Beforeconsultationsthenursesgatherthepatientsandtheysittogethertotalkabouthowtheycanpreventmalaria.Furthermore,thehealthcenterstaffoccasionallyalsogoestothevillagestodiagnosecommunitymembersusingrapiddiagnostictest.
Whencommunitymembersaregatheredatthehealthcenterbeforebeingtreatedthehealthcenterstafftalkstothemabouthowtopreventmalaria.Furthermore,wheneverthehealthcenterstafffindsapersonsufferingfrommalariawhenusingrapiddiagnostictestsinthevillagestheyreferthesecommunitymemberstothehealthcenter.
MEPRresearchers
CommunitymembersexplainedthattheMEPRresearchersusedtocomewithfumigationthatwasgiventocommunitymemberswhoarefarmersofrice.
Ontheseoccasionstheywouldtalkaboutthefumigation.Thisfumigationwastopumpintheswampswherericeiscultivatedsoastokillmosquitos.
Religiousleaders
Thecommunitymemberscommunicateaboutmalariaface-to-facewithpriestsduringchurchservices.
Apriestsometimesasksduringmasswhatisnowadaysoccurringandthencommunitymemberstalkaboutmalaria.Duringmasspriestscanalsogiveexamplesofcommunitymemberswhoweresufferingfrommalariabyexplaininghowsuchpersonrecoveredfrommalariabecauseofattendingthehealthcenter.
Districthospital
Whenacommunitymemberistransportedtothedistricthospitaltogettreatedmalariainaseverestage.
Aboutthediagnosisandtreatment.
MobilephoneAmongcommunitymembers
Tocallothercommunitymemberstoaskforhelpwhensufferingfrommalaria.Theyalsoreceiveinformationregardingmalariabyaccessingsocialmediathroughtheirmobilephones.Onecommunitymemberbetween18-35yearsmentionedshereceivesinformationaboutmalariafromsocialmediaplatformssuchasFacebookandWhatsApp
ShementionedtheinformationgotfromFacebook,WhatsApp,andInternetisveryimportantforthemsoastobeawareofmalariaandhowitisprevented.Mostofthetimethisinformationfromsocialmediacontainmessagesthathelppeopletoknowthesignsofmalaria,thecausesofmalariaandthewayofpreventingagainstmalaria.
Localleaders Whenanymosquitobreedingsiteisobservedwithinthevillagecommunitymembersusemobilephonestocalllocalleaders.
Bycallinglocalleadersthecommunitymemberscanindicatethemosquitobreedingsitessothattheycanprovidesupportandorganizecommunityworktocleanthemforexampleduringpublicwork.
Communityhealthworkers
Thecommunitymembersalsousemobilephonestocallcommunityhealthworkerswheneverthereisacaseofmalariawithinthehousehold.Accordingtocommunitymembersallpersonsinavillagehavethephonenumberofacommunityhealthworker,sowheneverthereisamalariacasetheycallthem.
Communitymemberscallcommunityhealthworkerstoaskforhelpandtogetmedicineswhentheysufferfrommalaria.Thereasonforcallingistosavetime.Forexample,thecommunityhealthworkermightbewithoutmedicinessotheycallfirsttocheckandmakeadecisionofreachingthecommunityhealthworkersor

26
healthcenterdependingontheavailabilityoftreatment.
Healthcenter Communitymemberscallthenursesfromthehealthcenterwhentheyaresickandwhentheywanttoaskforinformationoradvice.Thissavestimeinsteadofgoingtothehealthcenter.
Communitymemberscallnursesfromthehealthcentertotellthemsignsofwhattheyaresufferingfromsoastogetadviceonwhattodo.Theyalsocallthehealthcentertoaskforinformation,forexamplewhethertotaketheseconddoseafter10or12hours.
Nationalhealthinsurancescheme
Whentheyneedinformationaboutthehealthinsurance.
Anyquestionrelatedtothehealthinsurance.
RadioRBC Communitymembersreceive
informationthroughtheradio.AccordingtoacommunitymembermostRwandanshaveportableradiosorlistentotheradiousingausemobilephone.Duringaninterviewwithacommunitymemberstheresearchassistanttranslatedanexample:‘Andhehasalsoillustratedanotherroleoftelephonewherebyhehasexplainedthatphoneisnowadayshelpinghimtogettolistentotheradio.Hemayusephonesoastoturnonradio’.Thisexampleshowsthatcommunitymembersusemobilephonestoaccessradio.EveryWednesdayat7amthereisaradioshowwheretheyinviteaguesttotalkaboutmalaria.DuringthisradioshowlistenerscansendfreeSMStextmessagesorcanmakeafreecalltoaskquestions.Accordingtocommunitymemberstherearealsoadvertisementsontheradiothatcommunicateinformationaboutmalaria.
Thequestionsaresendbycommunitymemberstotheradioprogramarewrittendownandareansweredduringtheradioshow.Duringtheinterviewacommunitymembertheresearchassistanttranslated:’Themessagethatistransmittedthroughthisradioprogramisbrief.But,thisprogramtalksaboutthewayofpreventingagainstmalariawherebytheyexplainhowmosquitonetsareused.Explainingthatwheneverproductsthatarespecializedatgivingmosquitosareexpiredwithinmosquitonets,youaddothers.Whenevermosquitonetisexpired,whenevermosquitonetisnotfunctioningwellorhasexpiredyouhavetoreportandgetanewone.Andwhattheytalkaboutalsois,whattheyalsoexplainduringthisradioprogramtheyalsoexplainthewayofremovingthisstagnantwater,cuttingdowntrees,cuttingdownbushes,andhavinghygienicconditionswithinhouseholdssoastofightagainstthismalaria’.Thisstatementshowsthatwhenlisteningtotheradioshowcommunitymembersreceiveinformationaboutmeasureshowtopreventmalaria.Furthermore,theadvertisementsforexamplecommunicateinformationregardingthesymptomsofmalaria,toreachthehealthcenterintimefordiagnosingandtreatment,andhowbednetsshouldbeused.
VideoRBC Onseveraloccasionscommunity
membersreceiveinformationviavideosorplays.Firstofall,onTuesdaysandFridaysthereisanopenmarketinRuhuha.OnthismarkettheMinistryofhealthortheRwandanBiomedicalCenterprojectatelevisionshowwithaprojector
Thesevideosshowpeoplewhohavebeenattackedbymalariacomparedtopeoplewhohavenotbeenattackedbymalariabecauseofpreventionmeasuresthattheyused.

27
aboutmalaria,HIVandotherdiseases,andabouttheworkofcommunityhealthworkers.Inaddition,sometimescommunitymembersareshowedvideosatthesectorsoffice.Moreover,therearemeetingsinvillageswhereinactorsperformaplaythatexplainsaboutmalariatoinformcommunitymembers.Lastly,therearealsotheatersontelevisiontoinformcommunitymembersmoreaboutmalaria.
Asillustratedinthetableabove,communitymembersmainlycommunicateface-to-faceandthroughmobilephoneswithcommunitylevelhealthandnon-healthrelatedactors.Moreover,theycommunicateface-to-facewiththedistricthospitalwhenbeingtreatedthere.Inaddition,theycallthenationalhealthinsurancewhentheyhaveanyquestionregardingtheirinsurance.
CommunityHealthWorkersThecommunityhealthworkerscommunicatewithothercommunity
healthworkers,communitymembers,thehealthcenter,thedistricthospital,andRBC.Theseinformationandcommunicationflowsareexplainedinmoredetailintable6below.Table6:ExplanationinformationandcommunicationflowsfromcommunityhealthworkersFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceandmobilephoneCommunitymembers
Theytalkaboutmalariaduringdifferentmeetingswhencommunitymembersaregathered.Theseoccasionsincludemeetingsheldatvillagelevel,afterpublicwork,withinCLUB,duringmeetingsofcooperativesandduringspecialevenings.Furthermore,theytalkaboutmalariawithcommunitymemberswhentheygodownintothevillagestovisithouseholdstocountthenumberofbedsandtocheckifcommunitymembersfollowtherulesandregulations(moreabouttheserulesandregulationsinsection5.6.1).Inaddition,communitymemberscallthemincaseofanemergencyorwhentheyhavequestionsregardingmalaria.
Duringthesemeetingstheymainlytalkaboutdifferentmeasuresoffightingagainstmalariaandhowtousethem,theyexplaindifferentsignsofmalaria,theyalsoencouragecommunitymemberstogetmedicalinsuranceontime,andtheyinformcommunitymembersaboutwhatcausesmalaria.Furthermore,duringaninterviewwithacommunityhealthworkertheresearchassistanttranslated:‘Theyhavetelephonestheyusewithintheirdailywork.Andthesetelephoneshelppeopletoreceiveinformationaboutmalaria.Andallpeoplewithinavillage,allpeople,havetheircontact.Havethecontactofthecommunityhealthworkerssoastocallthemanytimetheymeetanemergency’.
CMATs Thehealthcenterisanindicatorofthesituationregardingmalaria,becausetheynoticewhenmalariaisincreasing.Whenevermalariahasbeenfoundincreasingwithinthehealthcenter,thehealthcentercalls
Afterinformingthemabouttheincreaseofmalaria,thecommunityhealthworkersgoandcommunicatetotheCMATs.ThenafterinformingthemtheCMATsinformthecommunitymembersaboutthenews.Thismeans

28
thelocalleadersandthecommunityhealthworkerstoinformthem.
thatthehealthcentercommunicatestothecommunityhealthworkersandthecommunityhealthworkerscommunicatetotheCMATs.
MobilephoneOthercommunityhealthworkers
Communityhealthworkersuseamobilephonetocallothercommunityhealthworkers.CommunityhealthworkershavefreenetworkpaidbytheMinistryofHealth.Therefore,wheneverapatientreachesacommunityhealthworkerandtherearenomedicines,thiscommunityhealthworkercancallanothercommunityhealthworkertoaskwhetherheorshehasmedicines.
Theresearchassistanttranslatedthatacommunityhealthworkersexplained:’Phonehasplayedagreatroleinbattlingmalaria.Wherebywheneverpatientreachescommunityhealthworkerssoastobesupported,soastobecured.Whenevertherearenomedicalmentsnomedicationsarenotaccessible.Sheorhemaycallimmediatelytheothercolleaguebyaskingwhethertherearemedicalments.Thenmedicalmentsmaybegained,maybegotbyusingphone’.
RapidSMSandSIScomHealthcenter,districthospital,RBC
Thecommunityhealthworkersreportthroughmobilephones.ThetextmessagesthattheyusetoreportarecalledrapidSMS.WhenapatientissufferingfrommalariaandshowingdangeroussignstheyuserapidSMStoreportthem.TheserapidSMSmessagesaresentimmediatelywhenthecaseisthereandaresentfreelytotheMinistryofHealth.Acopyofthemessagesissendtothedistricthospitalandthehealthcenter.Inothernotseverecasesofmalaria,thecommunityhealthworkersuseasystemcalledSIScomtoreport.TheyuseSIScomtoreportthenumberofcasesthattheytreatedweekly.Thisisanotherchannelofgivingreportsusingbookregisters.Theygivethisbookregistertothedatamanagerfromhealthcenters.ThenthedatamanagerofthehealthcenterentersthesereportsintoHMISandtheysendittothecentrallevel.
Duringaninterviewwithacommunityhealthworker,theresearchassistanttranslatedthecontentoftheserapidSMSmessages:‘Themessagethattheysendtoministryofhealth.Themessagesissendbyusingtheircodes.Therearesomecodes.Thereisonelineatministryofhealth.But,aslongastheyfacilitatethosedifferentpersonswhoarenowsufferingfromdifferentsicknesses.Thereisacodethatsheputsatmalaria.Andthereisalsoacodethatsheputsatammonia.Thosecodesarenotthesame.SoastomakethosepeoplefromMinistryofHealthnoticetherealsickness.Soitmeansthattheirmessagecontainsthesicknessthathasbeencured,thesignsofthepatient,themedicalmentsthatweregiventothepatient,andthestageofwhichthepersonifthepersonwastotalsufferer.Wasatagreatlevelofsuffer.Andifthepatientwasatalowerstageofsuffering.Ya.Themessagecontainsthose’.AfterreportingthatthereisapatientbeingtreatedattheirlevelbysendingtherapidSMS,innotmorethanthreedaysthecommunityhealthworkersreceiveatextbackaskingwhetherthepatientisstillsuffering,sotheyreceiveinformationfromtheMinistryofHealthaskingaboutthesituation.
Theexamplesinthetableaboveshowthatmobilephonesplayarolein
savingtimeandtoaskforinformationquickly.Furthermore,theyshowthatcommunitymembershavethephonenumbersofthecommunityhealthworkersandthatmobilephonesplayanimportantroleincaseofemergencies.

29
HealthCenterThestaffofthehealthcentercommunicatesaboutmalariawith
communitymembers,communityhealthworkers,localleadersandthedistricthospital.Theseinformationandcommunicationflowsareexplainedinmoredetailintable7below.
Table7:ExplanationinformationandcommunicationflowsfromthehealthcenterFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceCommunitymembers
Thestaffofthehealthcentertalksface-to-facetocommunitymembersaboutmalariaonseveraloccasions.Firstofall,inthemorningstheygatherpatientsthathavecomeformedicaltreatmenttogivetheminformationregardingdifferentsicknesses.Inaddition,theheadofthehealthcenteralsoexplainedthatbecauseofdecentralizationtheworkersofthehealthcentergodowntolocalareastodiscusssicknesseswithcommunitymembers.Forexample,thenursesofthehealthcenterattendmeetingswithcommunitymembersthatareheldatcell.Furthermore,attheendofthemonthlypublicworkstaffofthehealthcenterinformscommunitymembersaboutmalaria.Thismeansthatwheneverpeoplearegatheredthehealthcentertakestheoccasiontoinformpeopleaboutdifferentdiseases.Furthermore,thehealthcenterstaffalsotalksaboutmalariatocommunitymemberswithinlocalareaswheretheylive.Thehealthcenterworkersalsotalkaboutmalariaintheirfamilieswherebytherearealsopeoplewhoareattackedbymalaria.
Duringthesemeetingstheydonotonlytalkaboutmalaria,theyalsotalkaboutotherdiseases.However,oftentheytalkaboutmalariaasitisatagreatlevelcomparedtootherdiseases.Mostofthetimetheinformationdiscussedisaboutmalariaasmalariahasbecomeepidemicwithinthisregion.Astheyarestaffofthehealthcenter,thepeopleoftenvisitthemtotalkaboutmalaria.Communitymemberscomeandaskthemmoreinformationregardingtomalaria.Theyinformthemastobeawareofmalariaandtellingthemdifferentmeasuresoffightingagainstmalaria.
Face-to-faceandmobilephoneLocalLeaders Thehealthcentercommunicates
withlocalleadersface-to-faceandbymobilephone.Thehealthcentercommunicatestothelocalleadersbymobilephonewhentheywanthelptogathercommunitymembersforameeting,sothatthehealthcentercaninformthemaboutcurrentissuesregardinghealth,includingmalaria.
Thelocalleaderdiscusseswiththehealthcenteraboutthenumberofcommunitymembersthatsufferfrommalariaareattendingthehealthcenter,whytheysufferfrommalaria,whatmaybedonetosolvetheproblem,measuresoffightingagainstmalaria,andwheneverpossibletheytalkaboutadvocacytohigherlevelsofleadership.
Face-to-face,mobilephone,andSIScomCommunityhealthworkers
Thehealthcenterstaffcommunicatestocommunityhealthworkersface-to-faceandbymobilephone.Thecommunityhealth
Duringthesemeetingsthehealthcentersharesinformationaboutmalariathatthecommunityhealthworkersneedtoinformthe

30
workerssometimeshavemeetingsatthehealthcenterwheretheycommunicateface-to-face.Regardingthecommunicationviamobilephone,thehealthcenterusesaphonetocallcommunityhealthworkersincaseofemergencies,forexamplewhensomeoneescapedfromthehealthcenterwhilesufferingfrommalaria.Inaddition,thehealthcenterreceivesreportsfromthecommunityhealthworkersusingbooks(SIScom).
communitymembersabout.Forexample,whentherearerumorsthatthemedicinesathealthcenterarenolongercuringmalaria.Furthermore,thehealthcenterusesaphonetocommunityhealthworkers.Duringtheinterviewwithahealthcenterstaff,anexamplewastranslatedofwhenacommunitymemberquitsthehealthcenterwhilesufferingfrommalaria:’Thenafterquittingtheyareinchargeofreportingthistothehealthcommunityworkersbycallingtellingthemthatthereissomeonewhoisnowescapinghealthcenter.Butbeingtotallysick.Beingtotallyinbadconditions.Sothosecommunityhealthworkerswillinterveneafterhearingthisinformationbyusingphone.Thenthepersonalsoisbackistransportedalsosoastochecktheelement.Thisisthefunctionthatthephoneisnowplaying’.Inaddition,theSIScomreportscontaininformationaboutthenumberofpatientstheytreatedandwhichillnesses.Thehealthcenteralsoreceivesreportsfromthecommunityhealthworkersaboutthehouseholdsthatneedbednets.
Face-to-face,mobilephone,HMISDistricthospital
Thehealthcentercommunicatesandsharesinformationwiththedistricthospitalface-to-face,bymobilephone,andusingHMIS(moreinformationaboutHMISin5.2.2.2).Furthermore,theyuseamobilephonetocallthedistricthospitalincaseofanemergenceorwhenthereisalackofmedicinesatthehealthcenter.Moreover,thedatamanageratthehealthcentersendsthereportsreceivedbythecommunityhealthworkersandcombinesthisinformationwithreportsfromthehealthcenterandsendsthistothedistricthospitalusingHMIS.ThesereportsfromthehealthcentertothedistricthospitalinHMISarereportedweeklyandthesystemusesInternet.Lastly,theheadofthehealthcenterusesamobilephonetoaccesssocialmediatocommunicateinformationaboutmalariatothedistricthospital.
Firstofall,thereportssendviaHMIScontaintheinformationthatisgatheredviaSIScomfromthecommunityhealthworkers.Thisinformationisaboutthenumberofbednetsneeded,theamountofpatientstheytreatedandotherproblemsrelatedtomalaria.Secondly,theresearchassistanttranslatedthattheinformationthattheheadofthehealthcenterandthedistricthospitalshareviasocialmediaisabout:’Itdependsuponcurrentproblem.Shehasgivenanexamplewherebydistricthospitalmayseethatthereisincreasingincreasementthereisoccumentationofmalariawithincertainlocationcertainarea.Thentheymaycallthesehealthcenters.Arehealthcommunityworkersfunctioningwell?Dotheyhavesomemedicaltreatment?Dotheyhavesomemedicaltablets?Dotheyhave,aretheyequippedwithmaterials?Thenthroughthisway,throughWhatsApp,viaWhatsApptheymaysharethisinformation’.

31
Theexamplesinthetableaboveshowthatthehealthcentercommunicatestheinformationthatthecommunityhealthworkersgathertothedistricthospital.Furthermore,theycommunicatetothecommunitymembersandcommunityhealthworkerstospreadinformationaboutmalariasuchasthemalariapreventionmeasures.
HealthcenterpharmacyThehealthcenterpharmacycommunicatesface-to-facewithcommunity
memberswhoaretheirpatients/customersandtothehealthcenter.Furthermore,theyusemobilephonetocommunicatewithcommunitymembers,communityhealthworkersandthedistrictpharmacy.Theseinformationandcommunicationflowsareexplainedinmoredetailintable8below.Table8:ExplanationinformationandcommunicationflowsfromthehealthcenterpharmacyFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceandmobilephoneCommunitymembers
Firstofall,thehealthcenterpharmacycommunicatesface-to-faceaboutmalariaamongtheworkersofthehealthcenterandthepatients(communitymembers)onadailybasis.Furthermore,thehealthcenterpharmacyalsoreceivesphonecallsfromcommunitymembers.
Duringtheinterviewwiththehealthcenterpharmacytheresearchassistanttranslated:‘Telephonesplaysagreatrole.Wherebyapatient,apersonwhohasapatientmaybemotherhasherchildwhoissick.Thismotherwillcallthispharmacistbyaskingmoreinformationandbyaskingmoretellingsregardingtomedicalments,regardingtowhatshemaysoastocureherchild.Thenthispharmacistmaytellhersomemoreinformationbytellingthis:goandlookforsometablets,whicharelikethis,whichareinthiscategory.Thenaftergivingsuchgivingsuchtabletstoyourchildmakeherormakehimreachthishealthcenterassoonaspossible.Thesemedicalmentsareforreducingthepain,thismaybedone’.
MobilephoneDistrictpharmacy
Whenthereisashortageofmedicinesatthehealthcenterpharmacyorwhencommunication/informationsharingisneeded.
Aboutthedistributionofmedicines.
Communityhealthworkers
Thehealthcenterpharmacyalsousesamobilephonetoreceivecallsfromcommunityhealthworkers.
Duringtheinterviewwiththehealthcenterpharmacytheresearchassistanttranslatedanexampleofwhattheytalkaboutduringsuchaphonecall:‘YouhavegivenussomemedicalmentsandIamnowdealingwithacaseofmalariawherebyIamnowgoingtocureachildoffiveyears,howdoIprescribemedicalments.Thenafterbeingcalledshewillexplainthisbygivingexplanationtothesecommunityhealthworkerstoknowthemedicalmentsthatcouldbeprescribedtoapatient’.

32
Ascanbeseeninthetableabove,thehealthcenterpharmacymainlyusesmobilephonetoadvicecommunitymembersandcommunityhealthworkers.Furthermoretheyuseamobilephonetoexchangeinformationaboutthedistributionofmedicines.
PrivatepharmaciesTheprivatepharmaciescommunicateaboutmalariatotheleadersand
nursesofhealthcentersandtocommunitymemberswhoaretheirpatients.Theseinformationandcommunicationflowsareexplainedinmoredetailintable9below.Table9:ExplanationinformationandcommunicationflowsfromtheprivatepharmacyFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceandmobilephoneCommunitymembers
Theprivatepharmacistscommunicatewithcommunitymemberswhentheycometothepharmacytobuymedicinesorwhentheycallthepharmacytoaskforinformationoradvice.
Duringtheinterviewwithaprivatepharmacisttheresearchassistanttranslated:‘Hehasgivenanexamplewherebypatientmaycallhimtellinghimthatheissufferingfrommalaria.Thenalsoasking,whatkindofmedicationcanbetakensoastocuresuchelement.Thenhe,astheprivatepharmacist,mayadvicesuchpersonviaphone’.
Healthcenter Theprivatepharmaciescommunicatewithhealthcentersviamobilephonetoaskthemforinformationaboutthecurrentsituationregardingmalaria.Furthermore,theinterviewedprivatepharmacistmentionedthatthehealthcenteralsoplaysagreatroleinadvisingtheprivatepharmacies,astheworkersathealthcentersaremoretrainedandmorefamiliarandinformedaboutmalariaandotherkindofillnessescomparedtotheprivatepharmacists.Therefore,therearetrainingsatthehealthcenterwherethehealthcentertrainsandadvisesprivatepharmacies.Thismeansthattheprivatepharmacistsalsoreceiveinformationface-to-faceaboutmalariafromthehealthcenter.
Duringtheinterviewwithaprivatepharmacisttheresearchassistanttranslated:‘Heisgivinganexamplewherebyhemaycallheraskingwhethertherearesomenewmedicationsaboutmalaria.Askingwhetherthereareothernewmedicalments.ArethereothernewmedicalmentswhicharenotCoartem.Oraretheresomenewmedicalmentswhichmayfacilitatemesoastocuremypatients.Andhemayalsocallthisleaderofhealthcenteraskingsomeinformationsoastobegivensomeadvice.Askinghowisthelevelofmalaria?Howisthesituationofmalariawithinyourhealthcentercompared.Becauseweseeherethatmalariaisnowincreasing.Isitthesameasyours?Yaaskingthiskindofinformation’.
Thetableaboveshowsthatprivatepharmacistsusemobilephonesto
advisecommunitymembersandtoaskforinformationfromthehealthcenter.Italsoshowsthatthesepublicandprivateactorsonthecommunitylevelshareinformationineffortstofightagainstmalaria.

33
LocalleadersThelocalleadercommunicatesface-to-faceaboutmalariawith
communitymembers,religiousleaders,thehealthcenter,andCMATs.Furthermore,thelocalleadercommunicatesbymobilephonewithcommunityhealthworkers.Theseinformationandcommunicationflowsareexplainedinmoredetailintable10below.
Table10:ExplanationinformationandcommunicationflowsfromlocalleadersFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceCommunitymembers
Thelocalleadertalksaboutmalariaface-to-facewheneveragreatnumberofcommunitymembersgather.
Thewaysofhowtopreventagainstmalaria.
Religiousleaders
Localleaderaskreligiousleaderstoallowthereadingofadvertisementsaboutmalariaduringmass.
Thelocalleaderwritesadvertisementsthatcontaininformationaboutthecauseofmalaria,howitistransmitted,andhowcommunitymemberscanpreventagainstit.
CMATs WhentheCMATsareinthevillagesspreadingawarenessaboutmalariaanditspreventivemeasures.
Themalariapreventivemeasures.
MobilephoneCommunitymembers
Communitymemberscallthelocalleadertoinformhimaboutcurrentnewswithinthearea.
Theycalltodiscussnewsandthesituationregardingmalaria.
Communityhealthworkers
Thelocalleadercommunicateswithcommunityhealthworkerstoaskaboutthesituationregardingmalariabycallingthem.
Duringtheinterviewwithacommunityhealthworkertheresearchassistanttranslated:’Ortheleaderofacellmaycommunicatetothemaskingcurrentinformation.Howarepatientswithinlocalareas.Howareyoutreatingtheirillnesses.Howareyou,areyounowgettingmanytablets.Whataretheproblemsnowareyousufferingfrom.Thoseare,thisistheactivity,thisisthemessagethattheygiveeachotherwhilecalling,whileusingtheirphones’.
Religiousleadersandhealthcenter
Duringtheinterviewwithalocalleadertheresearchassistanttranslated:‘Yestheyworkhandinhand.Eithertheleaderofcell,executivesecretaryofacell,priestorthesetheleaderofthishealthcenter.Nomonthwhichtheycantgooveronemonthwithouttalkingeachother.Theycommunicateeachothertalkingaboutthecurrentproblems.Mostofthetimemalariaandalsosharingideasaboutthemedicalmentsthatarebeinggiving.Theycalloneanother’.
Duringthesephonecallstheytalkaboutthenumberofcommunitymembersthatareattendingthehealthcentersufferingfrommalaria,whydotheysufferfrommalaria,whatistheproblem,whatmaybedonetosolvetheproblem,theydiscussmeasuresoffightingagainstmalaria,andwheneverpossibletheytalkaboutadvocacytohigherlevelsofleadership.
Ascanbeseenfromthetablebelow,thelocalleadersareincontactwiththehealthcenterandcommunityhealthworkerstobeuptodateaboutthe

34
currentsituationregardingmalaria.Thelocalleadersneedtobeuptodateastheyaddressmalariaandthepreventivemeasureswhenevercommunitymembersgatherandbecausethecommunitymalariaactionteamsfallunderthelocalleaders.
CooperativesMembersfromricecooperativescommunicateaboutmalariaface-to-face
withothermembersfromricecooperativesandtheyusetheirmobilephonestocallwithpeopleinotherareasinRwanda.Theseinformationandcommunicationflowsareexplainedinmoredetailintable11below.
Table11:ExplanationinformationandcommunicationflowsfromcooperativesFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceOthermembersofthecooperative.
Withinthericecooperativescommunitymemberstalkaboutmalariaface-to-facetoothermembersofthecooperativeswhiletheyarecultivatingrice.
Forexample,thereisatimeoneoftheirneighborswithinaswampisattackedbymalariaandisnownotcultivatingandtheytalkaboutit.Thetranslatormentionedthatamemberofacooperativeexplained:‘Whattheytalkaboutitisthatmalariahasbecomeanepidemic.Ithasincreaseditsforces.Ithasexceeded,ithasgonebeyondtopasttimes.Pasttimesapersoncouldbeattackedbymalariaoneadayduringfiveyears.Oroncefiveyears,butnowadaysmalariacannotattackmostofthepeoplemonthlyortwiceduringthemonth.Sotheytalkaboutitandtheytrytoillustratetoexplainthatmalariahasgonebeyondtheirimagination’.
MobilephonePeopleinotherareasinRwanda
Amemberofricecooperativementionedthatshesometimescallspersonsfromthesouthprovincetotalktothemaboutmalaria.
Thesepersonsfromthesouthernprovinceimmediatelybecomesurprisedaskingwhysheissufferingfrommalaria.Theytellherthatsheissufferingfrommalariabecausespendsalotoftimeintheswampwhereshecultivatesrice.Thismemberofthecooperativementionedthatshetellsthemthisisnotthereason,becauseherchildrenwhodonotreachtheswamparealsosufferingfrommalaria.Itisinsuchprocesswherethemembersofricecooperativediscussinformationaboutmalariaonphone.
Thetableaboveshowsthatthemembersofacooperativecommunicateaboutmalariaineverydaysituationsandthattheydiscussaboutthecurrentsituationregardingmalaria.
CommunityMalariaActionTeams(CMATs)Thecommunitymalariaactionteamstalkaboutmalariaondifferent
occasionssuchasvillagemeetingsandafterpublicwork.Theysensitize

35
communitymemberstoreachthehealthcenterearlywhenevertheyareattackedbymalaria,toknowtherolesoflayinginmosquitonets,toclosewindowsduringtheevening,andtheyplayagreatroleatinformingpeopletoacceptpersonswhoareinchargeoffumigatingintotheirhouses,andinexplainingcommunitymemberstoremovestagnantwaterandbushesaroundthehouses.Therefore,thecommunitymalariaactionteamscommunicateface-to-faceaboutmalariawithcommunitymembers.
Furthermore,thecommunitymalariaactionteamscommunicateface-to-faceandbymobilephonewithlocalleadersandcommunityhealthworkers.Theyusemobilephonestocommunicatetolocalleaderstoshareinformationaboutmalaria.Furthermore,theyusemobilephonestocallcommunityhealthworkerstobegiveninformationregardingmalaria.Moreover,theyalsocallothermalariaactionteamsinothersectorswherethereisalowerrateofmalariatoaskinformationonwhattheydidtoreducethemalariaburden.
TraditionalHealersThetraditionalhealersreceiveinformationaboutmalariaface-to-face
fromthehealthcenterandfromthedistricthospital.Thetraditionalhealerthatwasinterviewedmentionedtherearetrainingsorganizedbythehealthcenterwheretraditionalhealersareinformedabouthowtofightagainstmalaria.Duringthesetrainingstheyaretaughthowtousemosquitonets,howtoremovestagnantwateraroundthehouse,andaboutothermeasuresthataretheretofightagainstmalaria.Furthermore,theheadofthedistricthospitalmentionedthattheysometimeshavemeetingswiththetraditionalhealers.
ReligiousleadersThereligiousleaderscommunicateface-to-facewiththehealthcenterand
thecommunitymembersaboutmalaria.Apriestgaveanexampleofasituationwhenhetalksaboutmalariawithacommunitymember:
‘YeswhenImeetwiththosepeoplewhosufferfrommalaria.Italkaboutwiththemandaskingthemwhattheyaresufferingandwhatreasonsoftheirsufferings.Andwhytheydidn'tdosomeprotection’.
Thisexampleshowsthatprieststalkaboutmalariawithcommunitymembers.Priestsalsooccasionallytalkaboutmalariaduringmass,forexamplewhencurrentproblemsarebeingdiscussedorwhenpriestsareaskedtoencouragecommunitymemberstobuyhealthinsurances.
MalariaEliminationProgram(MEPR)Themalariaeliminationprogramisnolongeractive.Theresearchproject
anditsinterventionshaveended.Theresearchersusedtocommunicateface-to-facetocommunitymembers,thehealthcenterandricecooperatives.
SchoolsTeachersatprimaryschoolscommunicateaboutmalariaface-to-faceto
theirstudents.Theyareresponsibleforteachingchildrenhowmalariaattackspeople,howitispreventedandhowtheymayhelptheirneighborsandfriendstoknowhowtofightagainstmalaria.Theinformationthatistaughttothestudentsaboutmalariaisfromdifferentbooksofdifferentsubjects,suchasbooksfromsocialstudies,Kinyarwanda,EnglishandScience.Thebooksofthese

36
subjectscontainsomechaptersthatareaboutmalaria.Furthermore,duringtheinterviewwithateachertheresearchassistanttranslated:
‘Theyusemobilephone,theyusemobilephoneseitheramongteachersamongthemselves.Oreitheramongatutorofanyclasscallingcommunityhealthworkersoastocometoschoolwhencommunityhealthworkerlivesnearbytheschool.Theremaybeanincident,therewillbeincidentwhereachildmaybecomesick.Immediatelyafterbecomingsickateacherlooksdifferentmeasuresofhelpingpatient.Thensheorheastheteacherhemaycallorshemaycallsuchcommunityhealthworkersoastocometoschooltohelpachild’.
Thisstatementshowsthatschoolsusemobilephonetoreachcommunityhealthworkerswhenachildissufferingfrommalaria.
5.2.1.2DistrictLevel
DistrictHospitalTheNyamatadistricthospitalcommunicatesaboutmalariawiththe
RwandaBiomedicalCenter,thehealthcenter,healthcenterpharmacy,localleadersandtraditionalhealers.Theseinformationandcommunicationflowsareexplainedinmoredetailintable12below.Table12:ExplanationinformationandcommunicationflowsfromthedistricthospitalFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
Face-to-faceLocalleaders Whentheyobservethatmalariacases
areincreasing.Thedistricthospitalcommunicatesface-to-facewiththeadministrativeandlocalleaderstoensurethatpracticesregardingmalariapreventionandcontrolareinplace,becauselocalleaderscanhelpsensitizethepopulation.
Traditionalhealers
Thedistricthospitalsometimeshasface-to-facemeetingswithtraditionalhealers.
Practicesregardingmalariapreventionandcontrol.
MobilephoneHealthcenterpharmacy
Thedistricthospitalincludesadistrictpharmacy,justlikethehealthcentersatcommunitylevelhavehealthcenterpharmacies.Thedistrictpharmacyreceivesmedicinesfromthenationallevelandisinchargeofdistributingandsendingthosemedicinestothehealthcenters.
Thehealthcenterpharmaciesreporttothedistrictpharmacytoorderfornewstockofmedicines.
RBCorMinisterofHealth
ThedirectorofthedistricthospitalusesemailandWhatsApptocommunicatetotheheadofthemalariadivisionatRBCortheminister.Hestated:‘Uhm,centrallevel..theyhavetheirownWhatsAppgroup.WealsohaveourownWhatsAppgroup.ButifweneedtoshareinformationIcansendinformationthroughWhatsAppgrouptotheheadof
Theheadofthedistricthospitalexplained:‘Highprevalenceofmalaria.Anduhm,wegotherewherethereishighprevalence,butthereisnopeoplearenotsleepingundermosquitonetsforexample.Andtheyneedmosquitonets,wecommunicatewithRBCandsayheretheyneedmosquitonets.Soweneedmoreintervention.Orifcommunityhealthworkersdonothave

37
malariadivisionforexample.Evenminister.IcanwritetoheranemailorWhatsAppgroup’.
whatwecallrapiddiagnostictestordrugswecommunicatewiththem.Yeah.SoforthemtogivethissupportofdrugsorRDT’.
Healthcenter Thedistricthospitalusessocialmediatocommunicateinformationtotheheadofhealthcenters.
WiththehealthcenterandotherhealthprofessionalstheyhaveWhatsAppgroupsinwhichtheyshareinformation.Forexample,whenthereishighprevalenceofmalariainthedistricttheycansendmessagesthroughWhatsAppinforminghealthcentersthattheprevalenceisincreasingandaskingthemtotakemeasures.
HMISHealthcenter Thedistricthospitalreceivesreports
fromthehealthcentersthroughHMIS.Thesereportscontaininformationaboutthenumberofbednetsneeded,theamountofpatientstheytreatedandotherproblemsrelatedtomalaria.
RBC ThedistrictcombinesthereportsfromallhealthcentersandsendsthisthroughHMIStoRBC.
Thesereportscontaininformationaboutthenumberofbednetsneeded,theamountofpatientstheytreatedandotherproblemsrelatedtomalaria.
ThedistricthospitalworkscloselytogetherwiththeRBCmalariadivision.Thedistricthospitalisthelinkbetweenthenationallevelandthecommunitylevel.Thehealthprofessionalsatthedistricthospitalhavemoreknowledgeaboutmalaria,sotheyareinbetweenbothlevelsandworkcloselytogetherwiththem.Thisalsoreflectsintheirinformationandcommunicationflows,becausetheymainlycommunicatetoRBCfromthenationallevelandtothehealthcenterandlocalleadersonthecommunitylevel.Thehealthcenterisresponsibletosupervisethecommunityhealthworkers,whilethelocalleaderssupervisetheCMATs.Subsequently,thecommunityhealthworkersandtheCMATsareresponsibletospreadawarenessandknowledgeaboutmalariainthecommunity.Thereasonthatthedistricthospitaldoesnotcommunicatedirectlywithotheractorsthroughsocialmedia,suchasthecommunityhealthworkersandCMATs,isbecausethemajorityofthemdonotusesocialmediabecausetheydonothavesmartphonesbutsimplephones.
5.2.1.3NationalLevel
RwandaBiomedicalCenter(RBC)TheRwandaBiomedicalCenterhasinformationandcommunication
flowsfromthedistricthospitalandcommunityhealthworkers.Furthermore,theysendinformationtocommunitymembersthroughradioandvideos.Theseinformationandcommunicationflowsareexplainedinmoredetailintable13below.Table13:ExplanationinformationandcommunicationflowstheRwandaBiomedicalCenterFromortowhichactor
Occasionwhentheycommunicateaboutmalaria
Whatthecommunicationisabout
HMISDistricthospital
ThedistricthospitalworkscloselytogetherwiththeRwanda
Thesereportscontaininformationaboutthenumberofbednetsneeded,

38
BiomedicalCentermalariadivision.TheRwandaBiomedicalCenterreceivesreportsfromthedistricthospitalsendthroughHMIS.
theamountofpatientsthecommunityhealthworkersinthewholedistricttreatedandotherproblemsrelatedtomalaria.
MobilephoneCommunityhealthworkers
TheRwandaBiomedicalCenterreceivesrapidSMSmessagesfromcommunityhealthworkersincaseofapatientwhoissufferingfromseveremalaria.
TheseSMSmessagesarecopiedtothedistricthospitalandthehealthcenter,sotheycanreadaswellwhatisoccurringattheground.
RadioandvideoCommunitymembers
TheRwandaBiomedicalCenterusesradioandvideosontelevisiontosendinformationaboutmalariatocommunitymembers.
TheheadofthemalariadivisionoftheRwandaBiomedicalCenterstated:‘Andweusealsomedia.WeusemediathroughradioandalsothroughTV.ForradiowehaveatalkshoweveryWednesdaymorning.From7amto8amwehaveatalkshowonRwandaRadio,ontheradio.ButthecoordinationforalltrainingforallmediaisdonebyRwandaCommunication,UhRwandaHealthCommunicationCenter.ItisanotherdivisionofRBCbutinchargeofthetrainingandcommunitymobilizations,allmedia,andalsotrainings’.
Asisillustratedinthetableabove,RBChasinformationflowsfromandtoalimitedamountofactors.TheymainlyreceiveinformationfromthedistricthospitalthroughHMIS,andfromcommunityhealthworkersthroughSMSmessages.Furthermore,theysendinformationtocommunitymembersthroughradioandvideoprojections.
NationalHealthInsuranceSchemeTheNationalHealthInsuranceSchemecommunicatesface-to-faceto
communitymembers.AttheheadquartersoftheNationalHealthInsuranceSchemeinKigalitheydonotprovideanyservices.However,theyhavedecentralizedservicesinthirtyadministrativedistrictsweretheyhaveanRSSBbranch.Thisiswheremostofthetechnicalservicesareprovidedtocommunitymembers.Furthermore,theyhaveanofficeoftwopeopleateveryhealthcenterforthecommunitybasedhealthinsurance.Thisiswherecommunitymembersreceivetheirmembershipcards.Moreover,whencommunitymembersenterthehealthcenterthisiswheretheygotoreceiveamedicalformwhentheywanttogettreated.
Inaddition,theNationalHealthInsuranceSchemeusesmobilephonesinseveralways.Firstofall,thisyearthenationalhealthinsuranceschemewillstartofferingcommunitymemberstopayfortheirhealthinsuranceusingmobilepaymentsviatheirphones.Furthermore,thenationalhealthinsuranceusestextmessagestoremindcommunitymemberstopayfortheirhealthinsurance.Communitymemberscontributetotheinsuranceonannualbasis.TheyearrunsfromJulytoJuneofthefollowingyear.FromJanuarytoJunetheywanttostartmobilizingcommunitymemberstostartpayingcontributionsviainstallments.TheysendSMSmessagestomobilephonestoremindcommunitymembersto

39
makecontributionsfortheirhealthinsurance.Inthisprocess,theNationalHealthInsuranceSchemedealswithtelephonecommunicationcompaniestosendmessagestoeveryoneregardlessiftheyaretheirinsuredmembers.TherearearoundeightmedicalinsurancesinRwanda,however80%belongstoRSSBsothereforetheyknowthatthemajorityisconcernedbytheirtextmessages,astheydonothavethephonenumbersoftheirmembers.Moreover,theNationalHealthInsuranceSchemeusesphonestoassistoranswerquestionsfromcommunitymembers.Theyhaveashorttelephonenumberoffourdigits4044thatmemberscanfreelycalliftheyhaveanyquestions.Thisistwo-waycommunicationwheretheycanaskanyquestion.
5.2.2TheroleofICTsTheprevioussectionanalyzedthecommunicationandinformationflows
betweenactors.Myresultspointtothevitalroleofcommunitymembers,communityhealthworkers,healthcenter,localleaders,andthedistricthospitalbecauseoftheirhighdensityinthenetworkofinformationandcommunicationflows.Thissub-sectionanalyzestheroleofICTsincommunicationwithinandbetweenstakeholdergroups.Asdescribedearlier,theresultsshowthattheICTsthatareusedinmalariapreventionandcontrolinRuhuhaaremobilephones,HMIS,radios,andvideosprojectedonscreens.Intheliteraturereview(section2.3)adistinctionismadebetweenICTsthatareinventedespeciallyforhealthsystems,andthosewherethelawofunintendedconsequencesplayaroleastheobjectiveofdesigningtheseinnovationswasnotspecificallytoreinforcethehealthsystem.InthecaseofmyresearchHMISfallsunderthefirstcategoryandisanICTspecificallydesignedforthehealthsystem.Contrarily,mobilephones,radios,andvideoprojectionsfallunderthesecondcategoryastheyreinforcethehealthsystem,buttheyarenotICTsspecificallydesignedwiththisobjective.ThemainroleofallICTsusedinmalariapreventionandcontrolinRuhuhaistoshareinformation.Therolesofmobilephones,HMIS,andradiosandvideoprojectionsareexplainedinthesectionsbelow.
5.2.2.1TheroleofmobilephonesMobilephoneshavemanyrolesinmalariapreventionandcontrolin
Ruhuha.Therolesareexplainedintable14belowwithsupportingquotesthatgiveexamples.
Table14:TherolesofmobilephonesinmalariapreventionandcontrolinRuhuhaFunctionofamobilephone
Supportingquote(translatedbyresearchassistantduringinterviews)
Tofacilitateconversationsinwhichmalariaistalkedaboutasatopicingeneralamongcommunitymembers
’Nowadaysapersonmaycallyouaskingyouinformation,askingyounews.Thenyoumayaskherhowareyou?Areyousick?Andmostofthetimeapersonmayrespondtoanothertellinghimortellingherthatsheissick,sheissufferingfrommalaria.Thenyouashisorherfriendmaycallforhelp,maycallforotherpersonssoastohelpher,soastointervene.Butwhenthepersonbeingcalledeachothertheymostofthetimetheyaskeachotheraboutlife’(communitymember).
Tocalltoaskorshareinformationaboutmalariaamongdifferentactors
‘Duringthiscontact.Theleaders.Theytalkaboutthenumberofpeoplethatarenowattendingheresufferingfrommalariabycomparinghowwhyaremostofthepeoplecomingsufferingfrommalaria,whatistheproblem,whatmaybedonesoasto

40
solvetheproblem.Theydiscussmeasuresoffightingagainstmalaria,thenumberofpeoplenowattending,andwheneverpossibletheyhaveadvocacytohigherlevelofleadership’(localleader).
Tocalltoaskforhelpfromneighbors,family,friends,communityhealthworkers,orthehealthcenterstaffincaseofillness
‘Telephoneisimportantforher,aswhensheissufferingfrommalariashemaycallherchildwhoisinKigalicity.Tellinghimthatsheissuffering.(…)Shecallsherboyaskingforhelp.Forexamplebringingabikesoasmakeherreachhospital.Andshemayalsousephonesoastocallaneighborsoastoreachhospitalintime’(communitymember).
Tocalltohelpsavetimeandmoney
‘Telephoneisveryimportanttothem.Wherebyshemaycallanursebeinginbed.Tellingherthatherchildwhohasbeenrecentlybeenattackedbymalariaandwhohasbeenrecentlycuredathospitalatclinicalcenterthatheorsheisalsobeingattacked.Andimmediatelythenursemayreplyhertellinghertogobackwiththechildtothehospital.Thenaphonemayhelphertosavetime,tosavemoney.Wherebyshemayreachhospitalwithoutcallingthenurseandthenursemayreplyhertogobackandtogobackhomesoastoattendhospitallater.Sotelephonesavesthetimeandsavesmoneysoastosolveproblems’(communitymember).
Tocallincaseofanemergence
‘Hereathealthcenterthereisonetelephonethatisusedsoastocallcommunityhealthworkersandtoimpartthemdifferentinformationregardingtodifferentsicknessesasheretheydon’ttreatonesicknessmalaria.Andtheyalsofunctionsthisphoneagreatrolewherebytheremaybeanemergence.Anunexpectedeventwherebythereisonewhoisabouttodie.Andinthisoneneedsemergence.Needsquicksupport.ThistelephonewillfunctiongreatrolewherebytheywillcallathospitalNyamatasoastoinformthatthereisonepersonwhoisgoingwhoneedsemergence,whoneedssupport,quicksupport’(healthcenterstaff).
Tofacilitateingatheringpeopleforameetingaboutmalaria
‘Thenshehasalsogivenanexamplewherebytheymayusephonebycallingthesecellleaders,executivesecretaryofcells.Theseleadersofcells.Thentheytellthem.Couldyouhelpustocallpeoplesoastocomeforthemeetingsoastoimpartthemsomethingimportantabouthealth.Thenthroughthiswayofcallingtheleaderofthecellwillalsointerveneandcallpeopleandtellmessengerstherearenowmessengerswhoarenowindifferentlocalareasspreadinginformationfromleaders.Thenthesemessengerswillgoduringtheeveningorduringthemorningbeforepeoplequittheirhomes,tellingthemthatthereisameeting,thereisameetingthatwilltakeplace.Thenaftercomingtogether,throughthismeetingtheinformationthatispreparedbyhealthcenterwillbespread.Andalso,alsoatthevillagelevelitmaybedonethroughthisway’(headofthehealthcenter).
Toreceiveorsendinformationviasocialmedia
‘TheinformationgotfromFacebook,WhatsApp,internetisveryimportantforthemsoastobeawareofsoastobeawareofmalariaandhowitisprevented.Yes.Andshefollowssuchinformationcollectivelysoastoknowanytimeshemeetmalariasoastoknowtheproblemsheissufferingfrom’(communitymember).

41
Toaccessradiofromwhichcommunitymembersreceiveinformationaboutmalaria
‘Andhehasalsoillustratedanotherroleoftelephonewherebyhehasexplainedthatphoneisnowadayshelpinghimtogettolistentotheradio.Hemayusephonesoastoturnonradio’(communitymember).
Tosendmoneyincaseacommunitymemberneedsmoneyfortransporttothehealthcenterorfortreatment
‘Ofcoursenowpeoplearefamiliarwithusingmobilephones.Especiallywhenitcomestosendingmessages.AndmoreoftennowitisabigchallengetoexchangemoneyifyouarelivinghereinKigaliandtosendmoneytoyourfamilymemberslivinginremoteareas.Butnowaspeoplearesendingmoneytotheirparentsortotheirrelativesusingmobilephonesitbecame,itbecameatoolthateveryhouseholdatleasteveryhouseholdthatinhouseholdeveninruralareasyoucanfindthateveryonehasitsmobileset,butatleastineveryhousehold,eveninpoorhousehold.Becausethepooresthouseholdtheyaretheonesthatneedthosemobilephones,becausehavingthosemobilesetanyonecansendyoumoneythroughthemobilephone’(nationalhealthinsurancescheme).
Toreportsevereincidentsofmalariafromcommunityhealthworkerstothenationallevel,withcopiestothedistricthospitalandthehealthcenter
‘ThemessagethattheysendtoMinistryofHealth.Themessagesissendbyusingtheircodes.Therearesomecodes.Thereisonelineatministryofhealth.But,aslongastheyfacilitatethosedifferentpersonswhoarenowsufferingfromdifferentsicknesses.Thereisacodethatsheputsatmalaria.Andthereisalsoacodethatsheputsatammonia.Thosecodesarenotthesame.SoastomakethosepeoplefromMinistryofHealthnoticetherealsickness.Soitmeansthattheirmessagecontainsthesicknessthathasbeencured,thesignsofthepatient,themedicalmentsthatweregiventothepatient,andthestageofwhichthepersonifthepersonwastotalsufferer’(communityhealthworker).
Tocalltothedistrictorotherhealthcentersincasethereisalackofmedicinesatthehealthcenterpharmacy
’Andshehasgivenanexamplewherebytheremaybeaproblemwheretherearenomedicalmentsforthosecommunityhealthworkers.Thosecommunityhealthworkersarenowlosingmedicalments.Theymayreportthattheyareincaseoflosingmedicalmedicalments.Thenhereafternoticingthattheymayalsolookfordifferentplacesthentheyseealsothattheydonothavethosemedicalments.Theyquickly,theyimmediatelyreporttothedistrict.Ortheyquicklycalldifferenthealthcenters,whicharelocatedwithinthisregionsoastoknowwherethosemedicalmentsareaccessible.Thentheyimmediatelyfacilitatetheirhealthworkerssoastogetthosemedicalments’(healthcenterpharmacy).
Topayforhealthinsurance
‘Forourcasewhatwearegoingtouse,whatwearegoingtodowithmobilephonesistopaytheircontributions.Sotheywillbefromthisfinancialyeartheywillbeabletomaketheircontributionusingmobilepayment’(nationalhealthinsurancescheme).
Tosendandreceivereminderstopayforhealthinsurance
‘Soastheycontributeonannualbasis.AndtheyearrunsfromJulytoJuneofthefollowingyear.ThenfromJanuarytoJunewemobilizethemtostartcontributingmaybeininstallment.Sothemessagethatwesendthroughmobilephoneistoremindthemmakingcontributionforinsurance’(nationalhealthinsurancescheme).

42
Asillustratedintable14,actorsmainlyusemobilephonestoshareinformationquicklyacrossdistances.TheresultsshowthatmobilephoneshelpinmalariapreventionandcontrolinRuhuhaforseveralreasons:1)Byusingmobilephonestoshareandreceiveinformationactorsdonothavetomeeteachotherphysically,whichwouldcostmoneyfortransportandmoretime.2)Whensickitcanbedifficulttomove,socommunitymembersusetheirmobilephonetocallforhelpfromfamily,neighbors,friends,orcommunityhealthworkerswhenbeingsickorincaseofanemergence.3)Mobilephoneshelpingettingcommunitymembersinformedaboutmalariapreventionandcontrolmeasures,forexamplebyaccessingradioorsocialmediathroughmobilephones.Theyalsohelpinremindingcommunitymemberstobuyhealthinsuranceintime.4)Byfacilitatingcommunitymemberstousemobilemoney,phoneshelpintransferringmoneyfortransport,treatment,orhealthinsurancequicklyandacrossdistances.5)Mobilephonesalsohelpinmonitoringandevaluationofseveremalariacasesbyallowingquickreportingofpatientsacrossalllevels.
5.2.2.2TheroleofHMISThehealthcenterandthedistricthospitaluseHMIS(RwandaHealth
InformationManagementSystem)toreporttotheRwandaBiomedicalCenter.HMISisanICTthatisused(nexttoSIScom)formonitoringandevaluationbytheRwandaBiomedicalCenter.TheheadoftheRwandaBiomedicalCenterstated:
‘Anotherstrategyismonitoringandevaluation.Monitoringandevaluationweareusingtwosystems.Theonesystemismonitoringofpatientsandcasestreatedatcommunitylevel.ThesystemisnamedSIScom.ThesecondoneathealthfacilitieswereusingRwandaHealthInformationManagementSystemHMIS.Weareusingthetwosystemsformonitoringofmalariacasesandthereportisdoingeverymonth.Thefirstweekofeverymonth’.
Ascanbereadinthestatement,reportingthroughHMISisdonemonthly.ThecommunityhealthworkersreporttothehealthcenterthroughSIScom,usingpaperreports.ThedatamanageratthehealthcenterthenreportsallthedatafromdifferentcommunityhealthworkersfromSIScomintoHMIS.Thedatamanagerentersthisdatausingacomputerorlaptop.AfterthisinformationisenteredintoHMISitissendtothedistricthospital.Thereisalsoadatamanageratthedistricthospitalthatsupervisesthedatamanagersatthehealthcenterstoensureaccuratedataandtomakesuretheysendthedataontime.ThedatamanageratthedistricthospitalreportsthedatareceivedfromthehealthcentersinthedistricttoHMIS.AftersendingthisreportthecentrallevelcanaccesstheinformationandusestheinformationthatisreportedthroughHMISformonitoringandevaluationpurposes.TheroleofHMISinmalariapreventionandcontrolinRuhuhaismainlythereportingfromcommunityleveltodistrictandnationallevel.
5.2.2.3TheroleofradioandvideoprojectionsTheroleofradioandvideoprojectionsismainlytoinformcommunity
membersandtomakecommunitymembersawareofmalaria.ThesechannelsareusedbytheRwandaBiomedicalCentertobroadcastinformationandadvertisementsaboutmalaria.Theadvertisementsandshowsonradiomainlycommunicateinformationaboutmalariapreventionmeasures,symptomsof

43
malaria,andtoreachthehealthcenterintimefordiagnosingandtreatment.Inaninterviewwithacommunitymemberthetranslatormentioned:
‘Butagaintheyreceivetheinformationfromtheradio.Mostofthetimestheycanbelikearadioshowaboutmalariaoradvertisementaboutmalaria.Andmostlyrelatedtomalariasymptoms,whentheyashowfromacertain,akidhasamalaria,heorsheisvomiting,sotheymentionthosesymptomsandthentheycanimmediatelyshownowthisismalaria,thenheorshehastogotothehealthcenterortheclinicfordiagnosingandtreatment.Sotheymostlylistentothatfromtheradio’.
Thisquotationgivesanexampleofthecontentoftheinformationthatcommunitymembersreceivethroughradio.TheWednesdaymorningradioshowthatwasdescribedearlierisintheformofadialoguewherecommunitymemberscanaskquestionsbysendingtextmessages.Furthermore,theroleofthevideoprojectionsthataredisplayedatthemarketandatsectorsofficeisalsotosensitizecommunitymembersabouthowtopreventthemselvesagainstmalaria. Tosummarizethissection,informationflowsinmalariapreventionandcontrolinRuhuhaarefacilitatedbyface-to-facecommunication;communicationusingmobilephonestocall,tosendtextmessages,toaccessradio,andtoaccesssocialmedia;byreportsusingSIScom;byreportsusingHMIS;andbycommunicationthroughradioandvideoprojections.Variousactorsamongwhichcommunitymembersexchangeinformationaboutmalariaaswellasthemeansofitscontrolandpreventionintheireverydaycommunicationbybothface-to-facecommunicationandthroughICTs.ThismeansthatapartfromthestrategicICTbasedhealthinterventionssuchasHMIS,mobilephonesalreadyplayacrucialroleinmalariapreventionbyfacilitatingawarenessraisingandbyimprovinginformationflowswithinandbetweenstakeholdergroups.TheadvantagesofICTsarethattheyallowinformationandcommunicationflowsrealtime,acrossdistances,atlowcosts,andacrossdifferentstakeholdergroups.However,increasedspreadofinformationcouldalsomeanincreasedspreadofmisconceptionsandinformationthatisnottrustworthy.Thereforethenextsectionwillanalyzeactor’sperceptionsaboutthesituationregardingmalaria,includingknowledge,misconceptionsandtrust.

44
5.3Analysisofactor’sperceptionsThissectionofmyanalysisfocusesonthestakeholders’perceptions
regardingmalaria,mobilephonesandtheirpotentialroleinpublichealth.Perceptions,orframing,arecrucialfortheanalysisofinformationnetworkschannels,astheyrevealhowindividualsandgroupsmakesense,organize,andcommunicateaboutreality(Venot2016).
Thefirstsub-sectionprovidesanoverviewoftheperceptionsofactorsonthefuturerolesofmobilephones.Afterthat,IanalyzewhatactorsthinkaboutthesituationregardingmalariainRuhuha,includingperceptionsonknowledgeandmisconceptions.Moreover,Iinvestigatehowthedifferentactorsassignlegitimacytotheinformationtheyreceive,focusingontheroleoftrust.Thelastsub-sectionanalyzestowhatextenttheseperceptionsaresharedbymultiplestakeholdergroups.
5.3.1PerceptionsofthefutureroleofmobilephonesAstable14illustrates,mobilephoneshaveseveralrolesinmalaria
preventionandcontrolinRuhuha.Mobilephonesarealreadyusedineverydaycommunicationtoexchangeinformationaboutmalaria.Duringtheinterviewsactorswereaskediftheythinkthatmobilephonesmightplayalargerroleinmalariapreventionandcontrolinthefuture.Differentstakeholdersgaveexamplesofwhattheyperceivedasfuturerolesofmobilephones,whicharetoexaminepatients,toteachcommunitymembersaboutpreventionmeasures,toaccesspastdataaboutmalaria,toidentifymosquitospecies,andabiggerroleofsocialmediatocommunicateinformationregardingmalaria.Theseperceptionsaboutthefuturerolesareexplainedinmoredetailbelow.
ToexaminepatientsSeveralcommunitymembersandthetraditionalhealerthoughtthatin
thefuturemobilephoneswillbeusedtoexaminepatients.Theyexplainedthattheyheardinformationaboutthisontheradio.Thetranslatorstatedanexampleacommunitymembergave:
‘Abouttheroleoftelephonewithinfuture.Hehasunderstoodnews.Heunderstoodnewsfromradio.RadioRwanda.Sayingthatthereisatimewhenpeoplewillbeexaminedusingphone.Medicalexaminationswillbecarriedoutbyusingphone.Andafterbeingdiagnosedtherewillbealsosomemedicalmentsbyusingphone.Yaheunderstoodsuchinformation’.
Thisisexampleofoneoftheactorswhothinksthatinthefuturecommunitymemberswillbeabletohavemedicalexaminationbytheuseofaphonefromanylocation.Furthermore,theythinkphoneswillplayaroleinfacilitatingmedicaltreatment.
ToteachcommunitymembersaboutpreventionmeasuresAstaffmemberofthehealthcentersharedthathethinksthatinthe
futuretheremightbemobileapplicationsthatteachcommunitymembersmalariapreventionmeasures.Thetranslatorstatedthathementioned:
‘Yaheisnowsayingthathedoesnotreallyseetheimportanceoftelephones,theimportanceoftelephoneswithinfuture.Thatwillexceedtheimportanceoftoday.Exceptthetimewhenthosetelephoneswillhavesomeprograms,software’s.Wherebythose

45
software’smaybeteachingpeopledifferentwaysofpreventingagainstmalaria.Andthosesoftware’swillalsoplayagreatroleathelpingpeopletoknowdifferent,forexampleheisgivinganexamplewherebytelephonewillbepossessing,willbewithaprogramofhelpingpeopleonhowtousemosquitonet.Thistelephonewillplayagreatrolewithinsuchcase’.
Thisstatementshowsaperceptionthatinthefuturemobileapplicationscouldbeusedtoteachcommunitymembersmalariapreventionandcontrolmeasuresandhowtousethem.Thestaffmemberofthehealthcenteraddedthatthiscouldonlybeusefulifcommunitymembersownsmartphonesthatcanallowthemtousetheseapplicationsontheirmobilephones,otherwisetheyareonlyavailabletocommunitymemberswhocanaffordexpensivemobilephones.
ToaccesspastdataaboutmalariaTheintervieweefromthecommunitymalariaactionteamsexplainedthat
hethinksthatinthefutureitwillbepossibletoaccesspastdataaboutmalariathroughmobilephones.Thetranslatormentionedthathestated:
‘Whatheisnowexplainingisthattheywillusephoneswithinfuture.Tohelpthemtorecallthepastinformationaboutmalaria.Wherebytheywillbeenablingeachothertalkingaboutdifferentpercentageswithinacertainyear.Acertainpastyear.Thesephonesmayplayagreatrolesoastoknowthepast,historywithinmedicalsituation.Thenafterrecalling,afterrememberingthepasteventsaboutmalariatheremaybeimprovementortheremaybesomethingwhichcouldbedonesoastofightagainstit.Therewillbesomethingthatmaybedonesoastofightagainstmalariaaccordingtophones’.
Thisexampleshowsthataccordingtothisactor,inthefuturemobilephonescouldbeusedtoaccesspastdataaboutmalariaincidentsbyusingphones.Hethinksthatthiscouldbeusefultoimprovestrategiesonhowtofightagainstmalaria.
ToidentifymosquitospeciesTheheadofthemalariadivisionoftheRwandaBiomedicalCenter
explainedthatthedayaftertheinterviewtherewasademonstrationaboutanewinnovationregardingmalaria.Therewasademonstrationabouthowyoucanidentifymosquitosbyanalyzingvibrationsofthewingsthroughamobilephoneapplication.Heexplained:
‘Thatmeanswithmobilephone,communitymembersshouldidentifydirectlyaspecies.Usingvibrationofwings.Yourecordvibrationofwingsandeachspecie,hetoldmethat,howcanIsay.Microbone...Uhmwaves(…)WewouldliketoworkwithRuhuhaandotherlocalgovernmentagencieshownowweshouldintroducenewtechnologyinhealthsectorsincludingmalaria.Sothatinthefutureweidentifyworkingwithmobilephone’.
ThisstatementshowsthattheRwandanBiomedicalCenterwouldliketoworkwithlocalgovernmentactorsinRuhuhatointroducenewtechnologyinthehealthsector,sothatinthefuturetheroleofmobilephoneswillincrease.

46
BiggerroleofsocialmediatocommunicateinformationregardingmalariaLastly,theheadofthedistricthospitalgaveanexampleonhowsocial
mediamightplayabiggerroleinthefuture.Hestated:‘Whenforexampleifyouneedtotakesomemeasuresagainstmalaria,weusemobilephonestocommunicatewithuhhealthcentersorrepresentativesofthesecommunityhealthworkers.Sowecommunicatethem,theycomeafewtogether,orwemakesomecommunicationstosocialmedia,uhmonhowtopreventmalariaorhowtocombatmalaria’.
Thisquotationisanexampleofhowtheheadofthedistricthospitalthinksthatmobilephonesandsocialcouldplayalargerroleincommunicationwithcommunitylevelactorsregardingmalariapreventionandcontrolinthefuture. Thissub-sectiongaveexamplesofperceptionsofthepotentialfutureroleofmobilephonesinmalariapreventionandcontrol.Theactorsmainlygaveexamplesofhowtheroleofmobilephonescouldincreaseinthefutureonthecommunitylevelbyexaminingpatients,teachingcommunitymembersaboutmalariapreventionandcontrolmeasures,forhealthrelatedactorstoaccesspastdataaboutmalariaonmobilephonesinordertodeterminestrategies,toidentifymosquitospecies,andmoreinformationandcommunicationflowsregardingmalariaviasocialmediatocommunitylevelactors.
5.3.2SituationregardingmalariaTheprevioussectionsexplainedtheactor’sperceptionsaboutthe
potentialfutureroleofmobilephonesinmalariapreventionandcontrol.ThissectionanalyzeswhatactorsthinkaboutthesituationregardingmalariainRuhuha.ActorswereaskedwhattheythinkaboutthesituationrightnowregardingmalariainRuhuha.Themainthemesthatwerementionedarethatmalariaisaproblemathighlevel,thatmalariaexceededlimitscomparedtothepast,thatmalariaexceededitslimitscomparedtootherregionsinRwanda,andthatthereisanincreaseofmalariaduringcertainmonths.Theseperceptionsareexplainedbelowillustratedwithviewsfromdifferentactors.
AproblemathighlevelIntervieweesgenerallyexpressedmalariaisnowbeingaproblemathigh
levelinRuhuha.Table15illustratesthiswithexamplesfromdifferentactors.Table15:ExamplesofperceptionsthatmalariaisaproblemathighlevelExamples Quotations(translatedbyresearchassistantduringinterviews)Malariaatgreatlevelcomparedtootherdiseases
’Malariaisnowatagreatlevelcomparedtootherelements,comparedtootherillnesses.Andcomparedtootherpatientswhocomefortreatmentsufferingfromotherelements.Malariaisatthetoplevelofproblemwithinthisarea’(headofthehealthcenter).
ManypatientsofmalariainRuhuha
‘Ihaveconsideredthatthereismanypatientsofmalaria.Mainlymalaria.Thereissomepeoplewhosufferfromdifferentseasons,maybefourtimesperyear.Sothatthereismainlymanymalariainthisregion’(religiousleader).
Malariaisexceedingasinoneinthreehouseholdsyoucanfindsomeonesufferingfrommalaria
‘Malariahassurpasseditslimit.Youcan’tquittwohouseswithouthearingsuchinformationaboutmalaria.Threehousesareenoughsoastohearthatthereisonewhoissufferingfrommalaria.Threehomesareenough.Somalariaisnowexceeding’(communitymember).
Attackedbymalaria ’Sheissayingon13Novemberthisyearshewasattackedbymalaria,

47
twiceamonth andinthesamemonthon27ththisNovemberthislastyearshewasalsoattackedbymalaria.Andithasbeenmarkedthatmalariahasexceeded’(communitymember).
Malariaisanepidemic ’Becauseitseemsnowmalariaisanepidemic.Youcangointoonehouseholdandyoufindlikethreeorfourpatientssufferingfrommalaria’(communitymember).
Whenapersoninahouseholdisattackedbymalaria,othermembersofthehouseholdsalsogetmalaria
’Somepeoplearecuredforalongtimeandtheydon’tcomebacksoastogetthosemedicaltreatmentfrommalaria.Andotherscan’tspendtwoweeks,oneweekwithoutbeingbacksoastobecuredhereathealthcenter.Soitmeansthatmalariahasexceeded.Andhehasalsogivenanexamplewherebynohousehold,whenmalariahascomeandhasenteredhousehold,itcan’tgoawaywithoutmovingaroundallpersonsinhousehold.Allpersons,oneiscuredtoday,theotheroneisgettingsufferingfrommalariatomorrow.Thepeoplereplaceeachotherwithinhouseholduntilallareattacked.Yathatishowmalariaisnowcirculating’(staffmemberofthehealthcenter).
Theexamplesinthetableaboveshowthatdifferentactorsperceive
malariaasaproblemathighlevel.Ingeneralallactorshadthisperceptionandthesearesomeexamples.Therewasnoactorwhoexpressedthatmalariaisnotaproblemathighlevel.
MalariaexceededlimitscomparedtothepastDifferentactorsexplainedthatduringthisyearmalariahasshown
exceededlimitscomparedtootheryears.Table16illustratesexamplesofactorsthatmentionedthatmalariaexceededlimitscomparedtothepast.Table16:ExamplesofperceptionsthatmalariaexceededlimitscomparedtothepastExamples Quotations(translatedbyresearchassistantduringinterviews)Therewereyearswithoutmalaria,butnowadaysatgreatlevel
‘Malariaisatahighlevelwithincommunity,nowadays.Hehasgivenanexamplebysayingthattherewasatime,therewereyears,whenmalariawasnotaccessible.Butnowadaysmalariaisnowatgreatlevel.Hehasgivenanexamplethattodayhehashelpedpeople,fivepatientsofmalaria’(communityhealthworker).
Malariamorecommonnowcomparedtopastyears
‘Malariahasexceeded,hasadvancedcomparedtosomepastyears.HehasgivenanexamplewherebyhewascomparingNovember,uhmSeptember,October,NovemberandDecemberandJanuary.Thosemonthswereaccustomedtohavelittlemalaria.Butnow,ithaschanged.Malariaisexceedingandnowadaystheyarereceiving180patientsaday,then160patientsarethosepatientsofmalaria’(staffmemberfromthehealthcenter).
Malariahasexceededcomparedtopastyears
’Nowadaysmalariahasgonebeyond.Hasexceededcomparedtosomepastyears.Malariahasnowbecomelikeanepidemic.Andespeciallywithinthislocation,withinthisdistrict.Malariahasexceededitslimits’(privatepharmacist).
Malariahasincreased ’Malariahasnowincreasedcomparedtothelasttimes.Comparedtothepasttimes.Asnowadaysyoumaytakemedicalmentsortabletswhicharespecializedtocuringmalaria.Butafteronlytwoweeksoroneweekyousufferfrommalariaagain.Thatiswhytheyarenowsayingthatmalariahasexceededitslimits.Andithasbeenconstantlikeapandemic’(communitymember).
Inpastyearssomeonecouldsufferfrommalariathreetimesayear,butnowadaysthreetimesamonth
’Rightnowmalariahasexceeded,hasincreased.Comparedtoyears.Hehascompared2017and2016wherebyheillustratedthatduring2016apersoncouldbeattackedbymalariathreetimesayear.Butduring2017apersoncouldbeattackedbymalariathreeortwotimesmonth.Yaamonth’(memberofcooperative).

48
Alltheexamplesinthetableaboveshowthatactorsperceivethatmalariahasincreasedcomparedtothepast.Thisisperceivedbyhealthandnon-healthrelatedactorsatthecommunitylevel.TherewasnoactorwhoperceivedthatmalariadecreasedinRuhuhacomparedtothelastyears.
MalariaexceededlimitscomparedtootherregionsinRwandaCommunitymemberswereamazedandsurprisedbymalariaand
explainedthatmalariahasexceededitslimitscomparedtootherregionsinRwanda.AccordingtothemincomparisonwithotherregionsinRwanda,BugeseraDistrictishigheratbeingattackedbymalaria.Someexamplesaregivenintable17below.Table17:ExamplesofperceptionsthatmalariaexceededcomparedtootherregionsinRwandaExamples Quotations(translatedbyresearchassistantduringinterviews)AmountofcommunitymemberssufferingfrommalariaishigherinBugeseraDistrictcomparedtootherregionsinRwanda
’HehasmentioneddifferentareasofRwanda.Bygivingexamplesoffarsouthernprovincewherebymalariaisnotseen.AndsomeofthenorthernpartofRwandawherebymalariaisnotseen.HehascomparedmalariafromthoseareaswithmalariafromBugeseradistrict,wherehehasillustratedthatwithinourareamalariahasexceeded’(communitymember).
DifferenceinmalariafromBugeseraandSouthernprovince
’HeisnowcomparingmalariafromBugeseratomalariafromsouthernprovince.Heisnowshowingthatthereisadifference.Malariawithinthisarea,Bugesera,istotallydifferentfromsuchmalariainsouthernprovince.Andhedoesn’tknowwhythereisadifferencebetweenmaybethesemalaria's.Becauseheisnowthinkingmaybemalariafromsouthernprovinceisshorterthanmalariafromthislocationbecausesouthernprovinceisaplaceofcoldness’(communitymember).
MalariaisfoundinregionsinRwandawithgreathotness,suchasBugeseraandMutara
‘MalariaismostlyfoundwithinthoseregionsofRwandawherebythatisgreathotness.ShehasexplainedthisEasternprovince.MostlyBugeseraandMutarathosearetheregionsthatarelocatedinEasternProvinceinRwandaisknowntobehot.AndshehasalsoexplainedsomedistrictsinSouthernProvinceandsomeinNorthernProvincewherebycoldplacesarenotknownatmalaria’(MEPR).
Thesequotationsshowthatdifferentactorsperceivethatmalariain
BugeserahasexceededitslimitscomparedtootherregionsinRwanda.ThiswasalsomentionedduringtheinterviewwithRBC,astheyidentifiedBugeseraasoneoftheeighthighmalariaburdendistrictsinRwanda.
IncreaseofmalariaduringcertainmonthsAnotherperceptionthatIidentifiedaboutthesituationregardingmalaria
inRuhuhaisthatdifferentactorsmentionedthatthereisanincreaseofmalariaduringcertainmonths.Table18containsexamplesofstakeholderswhomentionedthis.
Table18:ExamplesofperceptionsthatmalariaincreasesduringcertainmonthsExamples Quotations(translatedbyresearchassistantduringinterviews)Nowadaysmalariaepidemic,butinOctoberandNovembermoremalariathaninDecemberandJanuary
’Sonowadaysmalariaisseenasanepidemicwhencomparedtotheprevioustime.Butwhencomparinglikemonthtomonth.InOctoberandNovembermanycaseswhereseeninthehealthcenter.Therewasalongcuetillevening.ButtheseDecemberandJanuarytheystarteddecreasing’(communitymember).
Highprevalenceinthe ’InRuhuhasinceAugust,October,November,Decemberwehavehada

49
pastmonthsbutnow(January)itisdecreasingalittlebit
highprevalenceofmalaria.Butnowitisdecreasingalittlebit’(headofthedistricthospital).
Nowadaysmalariaisperiodic.Highernumberofmalariapatientsduringrainseasoncomparedtodryseason
‘Nowadaysmalariaisperiodic.Thatmeansitcomesaccordingtotheseasonoftheyear.Shehasgivenanexamplethathereathealthcenterduringrainreason,mostofthepeoplewhoarenowcomingforhelphereathealthcenterformedicalcarearethesufferersformalaria.Andshehasalsogivenanexamplewithinsummer,withinsunnyseason,thereisnobignumberofmalariapatients’(communitymember).
Duringrainseasontherearemoremalariapatientscomparedtodryseason
’Malariaisnowexceeding,isnotimproving.Atagreatlevel,becauseofthisrainyseason.Thismonthisexpectedtohavesmallrain.Butnowadaysithaschanged.Maybeclimatehaschanged.Thismonthisnotcharacterizedbymuchrain.Thenitmeansthathehasexplainedthatmalariahasexceededastherainisnowraining’(CMAT).
However,acommunitymembermentionedthatevenduringdryseasonmalariaattackedatahighlevellastyear(2017)
’Shehasmentioneddifferentmonthsaccordingtotheincreasementofmalaria.ShehasexplainedJulyandJuneandaugustlastyear,malariawasattackingmostoftheregionandthepeopleweresufferingfromit.Andshewondersherself.Shewondersherselfbysayingthatwhyismalariaattacking,weareaccustomedtosufferingfrommalariaduringrainseasons,butduringsummeroflastyearmalariaattackedus.AndshehasmentionedNovemberandDecemberwherebymalariahasdecreasedcomparedtothosethreemonthsshementioned.Andshehasexplainedtoobysayingmalariahasdecreasedinsomemonths.Inthosetwomonthsago’(communitymember).
Ahealthcenterstaffexplainedthatduringrainseason90%ofthepatientsthataretreatedatthehealthcenteraresufferingfrommalaria
’Malaria,nowadays,hassteppedforward.Shehasexplainedthisbygivingsomeperiodssomeseasonsofhere.Shehasexplainedthatduringsummerduringdryseason,duringdryseasonisatalowlevel.Itisnotseenbecausemosquitosarenotabletomultiplyandwithindifferentareas.Whereasshehasalsoexplainedthatwithinrainseasonmalariahasisatagreatlevel.Shehasexplainedthisbygivingpercentages.Wherebyshehasexplainedthatthosepatientsthatarenowadaysbeingtreatedhereathealthcenter,over90%arenowbeingseensufferingfrommalaria’(healthcenterstaff).
Thequotationsinthistableaboveillustratethattheperceptionofactors
isthatmalariaincreasesduringcertainmonthsoftheyear. Fromtheanalysisofperceptionsinthissectionaboutthesituationregardingmalariacanbeconcludedthatmalariaisperceivedagrowingproblem.
5.3.3KnowledgeandmisconceptionsIntheprevioussub-sectionIanalyzedthatmalariaisperceivedagrowing
problem.Theawarenessaboutmalariaasaproblemishigh.AllactorsperceivemalariaasaprobleminRuhuha.Duringtheinterviewsactorswerealsoaskedwhethertheythinkthereis(enough)knowledgeinthecommunityorregionaboutmalaria.Inaddition,theywereaskediftherearemisconceptionsregardingmalaria.Thefirstpartofthissub-sectionexplainstheperceptionsofactorswhothoughtknowledgeaboutmalariaisnotenoughinRuhuha.Secondly,theperceptionsofactorswhothoughtknowledgeaboutmalariainRuhuhaisenoughareanalyzed.Inthelastparttheperceptionsregardingmisconceptionsaboutmalariaaredescribed.

50
5.3.3.1KnowledgeisnotenoughTheactorswhothoughtknowledgeinmalariaisnotenoughgavevarious
reasons,whichareillustratedintable19.Thetableprovidesargumentsgivenbyintervieweeswhoexplainedthatknowledgeaboutmalariaisnotenough.Table19:PerceptionsofactorswhothinkthatknowledgeaboutmalariaisnotenoughArgumentknowledgeisnotenough MentionedbythefollowingactorsCommunitymembersknowsomepreventivemeasures,butdonothavemoreknowledgeaboutmalaria
Threecommunitymembers
Communitymembersknowsomesignsofmalaria,buttheydonotknowmuchaboutmalaria.Theyseeitastheysufferfromit
Onecommunitymember,onecommunitymemberwithouthealthinsurance
Communitymembersdonotfinishtheprescribeddoseoftabletsbecauseofsharingthemwithothers
Onecommunitymember,healthcenterpharmacy
Knowledgeisnotenoughandmorecontinuoustrainingsandteachingisneeded
Onecommunitymember,CMAT,MEPR,traditionalhealer,communitymemberwithouthealthinsurance,districthospital,religiousleader,headofthehealthcenter
Therearecommunitymemberswithlowerunderstandingwhodonotreachthehealthcenterintimewhensufferingfrommalaria
Healthcenterstaff,districthospital
Somepeopleareaware,butothercommunitymembersarestillconfusingmalariawithpoisonousactivitiesorarenotawareofitssignsandattendtraditionalhealers
Twocommunitymembers,healthcenterpharmacy,districthospital
Understandingofmalariahasimprovedbecauseoftrainings,buttheknowledgeaboutmalariaisnotenoughandmoretrainingsandknowledgeisneededtototallyremovemalaria.
CMAT,healthcenterpharmacy
Therearepeoplewhohavemisunderstandingsabouttherulesandregulations.Thereisaneedtochangesuchunderstandings
Communitymemberwithouthealthinsurance
Communitymemberswonderwhytheydonotneedtobeinmosquitonetsduringthedayandwhytheyshouldremoveplantationsaroundtheirhomes
Onecommunitymember
Thereisawarenessaboutmalariaascommunitymembersseethatmalariaissteppingforward,butmoreexplanationisneededascommunitymembersareaskingthemselveswhymalariaisincreasingcomparedtopasttimes
Memberofcooperative
Thereisnotenoughknowledgeascommunitymembersarenotabletoproducetheirownmedicines
Memberofcooperative
Thereisknowledgeaboutmalariaasitisatopicduringthemeetings,howeverthereisalsolowerunderstandingandpeoplewhodonothavemuchknowledgeaboutmalaria
Schoolteacher
Lackofawarenessthatapersoncanstillgetattackedbyamosquitowhiletakingmalariatablets
Healthcenterstaff
Intermsofsymptoms,diagnosticandtreatmenttheknowledgeishigh,buttheknowledgeaboutpreventionandecologyofvectorsisstillverylow
RBC
Ascanbeanalyzedfromthetableaboveisthatthemajorityofactors
thoughtthatknowledgeaboutmalariaisnotenoughinRuhuha.Themainperceptionsaboutwhyknowledgeisnotenougharethattherearestillcommunitymemberswhodonotreachthehealthcenterintime,thatthe

51
communitymembersneedcontinuousteaching,thatthereisnoawarenessthatapersoncanstillgetattackedbyamosquitowhiletakingmalariatablets,thatthereisnotenoughknowledgeaboutprevention,andthatmoreknowledgeisneededaboutmalariaingeneral.Thesereasonsareexplainedinmoredetailbelow.Afewotherimportantperceptionsfromthetableabovesuchasthatcommunitymemberssharetabletswithothersandthebeliefinpoisonousactivitiesandbewitcheryaredescribedinmoredetailinsection5.3.5aboutsharedperspectiveoftheproblem.
TherearecommunitymemberswhodonotreachthehealthcenterintimeThehealthcenterstaffandthedistricthospitalaretwohealthrelated
actorswhodealwithtreatingcommunitymembers.Theybothmentionedthatknowledgeaboutmalariaisnotenoughbecausetherearestillcommunitymemberswhodonotreachthehealthcenterintime.Duringtheinterviewwithastaffmemberofthehealthcenterthetranslatorexplainedthathesaidthefollowing:
‘Somepeopledie.Therearesomepeoplewhohavelowerunderstandingaboutmalaria.Andthosepeopletheyspendtwoormaybealongtimebeingthereathomesufferingfromtheelement.Sufferingfromthesickness.Sufferingfrommalaria.Thenafterspendingalongtimethereandnoticingthattheyareabouttodie.Theycometothehospitalortheycometothehealthcentersoastobetreated.Thenafterreachinghere,aftermakingsomeexaminationstheyuseblood,theyusewhat,afteracertainperiodtheydie.Becauseofcominghereathospitalontimewhichisnotappropriate.Delaying,theirdelaymakethemdie’.
Theheadofthedistricthospitalalsomentionedthattheknowledgeisnotenoughandthattheyneedtosensitizepeopleaboutmalaria.Hestated:
‘Forsomepeoplesomepersonstheyhavebelieves,theystillhavebelievesthatwhentheyaresick,theydon’ttrustthatitismalaria.Itmaybeotherthings,otherdisease,sotheygolookfortraditionalhealersandsometimestheygotohealthcenterstoolate.Sometimeswehavesomedeathduetomalaria’.
Thisstatementalsoillustratesthattherearecommunitymemberswhoreachthehealthcentertoolate.Thisexamplealsoshowstheirperceivedeffectofthebeliefintraditionalhealers,whichisthatitmakescommunitymembersreachthehealthcentertoolate.
NeedforcontinuousteachingAscanbeseenintable19thereareanumberofactorswhomentioned
knowledgeisnotenoughbecausethereisaneedforcontinuousteaching.Someexamplesofactorswhomentionedthisaregivenintable20below.Table20:ExamplesofactorswhomentionedtheneedforcontinuousteachingActor Supportingquotation(translatedbyresearchassistantduring
interviews)MEPR ’Noonewhocangoandtestifyandconfirmsthatknowledgeisenough.Every
timeweneedtolearn.Everytimeweneedtolearn.Aswealwaysneedtolearn,wealwaysalsoneedtobethought.Thatmeansthatneedthepeopleneedalwaystobethought.Itisalongprocess.Ya,itisnotastillprocess.Itislongandmovingprocess.Itisaperpetualprocess’.

52
Traditionalhealer
‘Thepeopledonotunderstandthingsatthesamelevel.Theyhavedifferentunderstandings.Itmeansthattheyneedtobethoughteverytime.Theyneedperpetualteaching’.
Communitymemberwithouthealthinsurance
‘Theknowledgeisnotenough.AllRwandansneedbeingthought,needendlessteaching.Theyneedtobethoughtforeversoastobeawareofthisillness’.
Religiousleader ‘No,notenough.Wehavetomaybegivesomeinformationeverytime.Butitisnotsufficient’.‘Everyonehasinformationaboutmalaria,butthereisalsosomeignorance.Sothatjusthavetogiveinformationeverytime’.
Thequotationsinthetableabovearesomeexamplesofanumberof
actorswhothinkthatthereisnotenoughknowledgeaboutmalariaandthatthereisaneedforcontinuousteaching.
NoawarenessmalariamayattackwhiletakingtabletsThehealthcenterpharmacistexplainedthattheknowledgeisnotenough
becausethereisnoawarenessthatmalariamayattackwhiletakingtablets.Thetranslatorexplainedthatshementioned:‘Peoplearenotawareofthatmalariamaybemayattackthemwhiletakingthesetablets.Ya.Itmeansthattheyarenotawareofit’.Thisexampleshowsthatthehealthcenterpharmacythinksthatthereisnotenoughawarenessthatmalariamayattackapersonagainwhiletakingtabletstocuremalaria.
NotenoughknowledgeaboutpreventionTheheadofthemalariadivisionoftheRwandaBiomedicalCenter
mentionedthatthereisnotenoughknowledgeaboutthepreventionofmalaria.Hestated:
‘Ok,therearedifferentreportsandpublicationsdone.Theknowledgeisveryhighintermsofdiagnosticandtreatmentofmalariaandsymptoms.Butknowledgeisstilllowintermsofprevention.Thegooduseofbednets.Evenofspraying.Andalsoothermethodsforprevention.Becausetherearedifferentmethodsforpreventionagainstmalaria.Buttheknowledgeisveryhighintermsofskillsintermsofhowtoknow,symptomsofmalaria,howtotreatmalaria,andsofort.Diagnosticofmalaria,butintermsofpreventionknowledgeisstilllow.Butecologyofmosquitos,knowledgeonmosquitosofthebreedingsites,mosquitolarvae,isstillverylowintermsofecologyofvectors.Knowledgestillveryverylow’.
ThisstatementshowsthattheknowledgeaboutmalariaisperceivedaslowbytheRwandaBiomedicalCenter.Theprivatepharmacistalsomentionedthattheknowledgeisnotenoughbyexplainingthattherearecommunitymemberswhoarenotusingpreventionmeasures.Thetranslatormentionedthathestated:
‘Theunderstandingsofthepeoplearenowatabadarenowwithinabadconditionduetodifferentreasons.Asexplainedthatthepeoplearenotusingmosquitonetsproperly.Theydonotusemosquitonet.Andtheydon’t,somepeopledon’thavesuchcleanliness,suchhygienicconditions’.
Thesequotationsillustratethattheseactorsthinkthattheknowledgeaboutmalariapreventionandpreventionmeasuresisnotenough.

53
KnowledgeistherebutmoreknowledgeisneededThereareseveralactorswhothoughtthereisknowledgeinthe
communityaboutmalaria,butnotenough.Anumberofexamplesareillustratedintable21below.
Table21:ExamplesofactorswhomentionedtheneedformoreknowledgeActor Supportingquotation(translatedbyresearchassistantduring
interviews)Schoolteacher ’Theyhaveknowledgeaboutmalaria.Theyhaveenoughknowledgeabout
malaria,asmalariaisthetopicduringthemeetingswheretheyattend.Andisalso,malariaistalkedaboutindifferentfamilies.Itmeanstheyknowit.Butthereisaproblemoflowerunderstanding.Asthepeoplehavedifferentunderstandings,lowerunderstandings.Therearesomewhodonotposses,whodonothavemuchknowledgeaboutmalaria’.
Healthcenterpharmacist
‘Itisnotgreatknowledge,theydon’thavemuchbuttheyhavesomeknowledgeabout’.
Headofthehealthcenter
‘Peopleareinformedaboutmalaria.Theyarenowinformedaboutdifferentpointsaboutmalariawherebytheyknowthecauseofmalaria.Andtheyalsothepeopletheyknowthewayofpreventingagainstthiskindofelement.Andalsopeopleareinformedaboutthewaytopreventit,thewaythattheymaytreatitandthewaythattheytakethistabletstakenfromhereathealthcenters.Peoplearereallyinformedaboutthis’,butthat:‘Theknowledgeofthepeopleaboutmalariaisatagreatlevel.Butasthisisaproblem.Itrequiresdailyteaching.Itrequiresdailyadvises.Peopleneedbeingtalked,beingeducatedaboutthiskindofillnesses’.
Communitymemberfromcooperative
‘Theyareawareofmalaria,little.But,thereistheyarenowadaysaskingthemselves.Whyismalariaexceeding?Whyismalariaprogressing?Whyisitadvancingcomparedtothepasttimes.Itmeansthattheyneedfurtherexplanation.Peoplearenowwonderingsoastobeexplainedmoreaboutmalaria.Becausetheyseethatmalariahassteppedforward’.
Thequotationinthetableaboveillustratethatseveralactorsthinkthat
thereisknowledgeaboutmalaria,butthatmoreknowledgeisneeded.Thisissomehowsimilartotheactorswhomentionedthatthereisaneedforcontinuousteachingasexplainedearlierinthissection.
5.3.3.2KnowledgeisenoughOtheractorsmentionedthattheythoughtthereis(enough)knowledge
aboutmalariawithinthecommunityorinRuhuha.Theseperceptionsareillustratedintable22.Table22:PerceptionsofactorswhothinkthatknowledgeisenoughArgumentknowledgeisenough MentionedbythefollowingactorsCommunitymembersareadvisedbycommunityhealthworkersandresearcherssendbyhigherlevels
Onecommunitymember
Knowledgewaslow,butisnowincreasingbecauseofthehighmalariaprevalence
Twocommunitymember
Knowledgeisthere,buttheproblemisputtingintopracticetheknowledgethatisbeingthoughtandadvisedbydifferentactors
Onecommunitymember,localleader
Increasinginformationaboutmalariareducedtraditionalwaysoffightingagainstmalaria
Onecommunitymember
Theyaretotallyawareofmalariaandknowledgeisenough
Onecommunitymember,localleader,traditionalhealer
Knowledgeisenough,butcommunitymembersare Communityhealthworker

54
wonderinghowtouprootmalariacompletelyandtheywonderiftheyshouldstillgotoworkinswampsasthatiswheremosquitosareKnowledgeisthere,buttheproblemisthatmosquitonetsarenotavailable
Communityhealthworker
Communitymembershaveknowledgeaboutmalariaaswhentheyaretoldtobuyinsurancecards,theyimmediatelyunderstanditsimportanceandthesituationthattheyarenowadaysphasingmalaria
CMAT
Knowledgeisenough,butthereisaneedforadvocacysoastobesupportedtofightmalaria
Traditionalhealer
Knowledgeaboutmalariaisenough,thecauses,symptoms,treatmentareallknown.Theproblemisthatpreventivemeasuresarenotapplied100%astheyshouldbeandthereisignorance
NationalHealthInsuranceScheme,privatepharmacy
Asillustratedinthetableabove,therearefeweractorswhothinkmalaria
isenoughcomparedtothosewhothinkthatthereisalackofknowledge.Stakeholderswhothoughtthatthereisenoughknowledgeaboutmalariamainlymentionedthatbecauseofadvisefromcommunityhealthworkersandtheincreaseofmalariacommunitymembershavegainedknowledgeaboutit.Otheractorsthinkthatthereisknowledgeaboutmalaria,butthatcommunitymembersdonotapplythepreventionmeasures.Theseperceptionsareexplainedinmoredetailbelow.
CommunityhasknowledgeaboutmalariaDifferentintervieweesmentionedthatthecommunityhasknowledge
aboutmalaria.Duringtheinterviewwithacommunitymemberwithouthealthinsurancethetranslatormentionedthatheexplained:
‘Thepeoplehaveknowledgeaboutmalaria.Hehasexplainedthisbygivinganexamplewherebytheyattenddifferentmeetingswithintheirvillage.Duringthesemeetings,duringthismeetingthatisorganizedatvillagelevel.Theytalkaboutdifferentinformationregardingmalaria.Hehasmentionedsomesignsthattheymostlytalkaboutwithinthemeeting.Hehasillustratedmuchfever,havingpainwithinbodyandhavingpainwithinbodyinallaspirationswherebonesattachtoothers.Andvomiting,beingdiscouraged,being,havingfewlittleforcebecauseofbeingattackedbythisillness’.
Thisexampleshowsthatitisperceivedthatcommunitymembershaveknowledgeaboutmalaria.Alsoaccordingtooneofthehealthcenterstaffcommunitymembershaveknowledgeaboutmalaria.Thetranslatormentionedthatheexplained:
‘Thereisenoughknowledgeinthecommunityregardingtomalaria.Becauseheisoneofthestaffofthehealthcenter.Heisnowsayingthatmanypeoplecomeheresoastomedicaltreatment.Andaftermakingadiagnosis.Aftermakinganexaminationandgivinghimorhersomemedicalmentssayingthatsheorheisnotsufferingfrommalaria.Asthepeopleareaccustomed.Areawareofthesigns,thedifferentsymptomsofmalaria,theymaytellyou,whoareyou?Doyouknowwhatyouaredoing?IreallyknowthatIamsufferingfrommalaria,whyareyougivingmethesetabletswhyIreallyknowthat

55
IhavecomefromhomeknowingthatIknowthatIamsufferingfrommalaria.Ireallyknowthesigns.Whyareyousayingothers.(…).Itmeansthepeoplereallyknowit’.
Thesestatementsareexamplesofactorswhothinkthatthecommunityisinformedaboutmalariaandthattheknowledgeisenough.
ThereisknowledgebutcommunitymembersdonotapplymeasuresThenationalhealthinsurancerepresentativeexplainedthatcommunity
membershaveknowledgeaboutmalaria,howeverthattheydonotapplythepreventionmeasures.Hestated:
’Knowledge?Ya.Whatwerealizedisthatinthecommunitythereisnoproblemaboutknowledgeaboutmalaria.Theyknowthecausesofmalaria,theyknowthesymptomofmalaria,theyknowthetreatmentofmalaria.Soeverythingisknown,whenyoucomparetothepast.Inthepastmanypeoplehadwronginformationaboutmalaria,aboutcauses,aboutsymptoms.Butnow,whenyouseethattheknowledge,itisabove90%theyknowexactlywhatarethecausesofmalaria,whatarethepreventivemeasures,buttheproblemistheapplicationofthosepreventivemeasures.Theyknowthepreventivemeasures,buttheyarenotapplied100%astheyshouldbe.Buttheyknowthem.Theyknowthatmosquitobednetareveryeffective,theyknowthattheyhavetocleanthesurroundingsoftheirhomes,theyknoweverything.Butwhenitcomestoapplythosepreventivemeasuresitbecomesaproblem’.
Thisexampleshowsthatthereisknowledgeaboutmalariainthecommunity,butthatthereareactorswhothinkthatthecommunitymembersdonotapplythepreventionmeasureswell.
5.3.3.3MisconceptionsAccordingtotheperceptionofactorsthereareseveralmisconceptions
thatstillexistwithinthecommunityorregion.Themisconceptionsaboutmalariathatareidentifiedduringtheinterviewsareillustratedintable23.Thetableshowsthemisconceptionsthatwerementionedbywhichactorsduringtheinterviews.Table23:MisconceptionsaboutmalariaMisconceptions MentionedbyBewitcheryandpoisonousactivities,attendingtraditionalhealers
Fivecommunitymembers,schoolteacher,localleader,communitymemberwithouthealthinsurance,districthospital
Eatingsorghumandmaizesticks Twocommunitymembers,cooperativeEatingsugarcanes Threecommunitymembers,RBC,religious
leader(butthinksthatthiswas10yearsago)Drizzleandnewlyharvestedbeans PrivatepharmacyMedicinesatthehealthcenterdonotcuremalaria
Threecommunitymembers,cooperative,staffofthehealthcenter,healthcenterpharmacy
Unbalanceddietandfoodthatisnotwellprepared
Headofthehealthcenter
Nomisconceptionsaboutmalaria Ruhuhahealthcenterstaff,communityhealthworker,traditionalhealer

56
Asillustratedinthetableabove,notallactorsthinkthattherearemisconceptionsaboutmalariainRuhuha.However,misconceptionswerementionedbybothhealthandnon-healthrelatedactorsandbystakeholdersfromalllevels.Themisconceptionsthatareidentifiedareexplainedinmoredetailedbelow.
BewitcheryandpoisonousactivitiesMostactorscriticizedthetraditionalhealersandthecommunity
memberswhostillvisitthem.Forexample,thetranslatorexplainedthatacommunitymembermentioned:
‘Therearesomepeoplewhogoformedicaltreatmenttotraditionalhealers.Andhavingunderstoodthattherearesomesignsofmalariasomepeoplethinkthattheyhavebeenbewitched.Theyhavebeengivensuchapoison.Thentheygotosuchtraditionalhealers.Inrealofcominghereathealthcenter’.
Thehealthcenterpharmacyalsogaveanexampleofcommunitymembersbelievinginbewitcheryandpoisonousactivities,thetranslatorstatedthatshementioned:
‘Therearesomepeoplewhoareunawareofmalaria.Shehasgivenanexamplewherebymothermayseethatherchildissufferingfromsicknessthatshedoesnotreallyknow.Thenafterseeingthatthechildisnowbeingparalyzed,achildisnottalkingisnotmoving,nothingasmovementthatistakingplace.Thenshemaytakeconclusionthatsheisgoingtoreach,thatsheisgoingtogototraditionalhealer.Thiscasethisconditionoftraditionalmedicines,thiscaseofattendingthosetraditionalhealersmaytakeplaceinthiscondition.-Interviewer:Andwhydotheygotothetraditionalhealerinsteadofthehealthcenter?-Translator:Becauseofnotbeinginformedaboutthesignsofsuchsicknesses’.
However,thetraditionalhealermentionedthattherearenomisconceptionsaboutmalaria.Thetranslatorstatedthatthementioned:
‘Peoplehaveknowledgeaboutmalariaastheyimmediatelyhospitalsorhealthcenterswhenevertheyareattacked.Andthereisalsosomepost..thoseclinics.Everycellhasitsclinic.Thisisaplacewherethosepatientssufferingfrommalariaarereachedassoastogettabletsandothermedicalmentsaboutmalaria.Thismeansthatpeoplereallyknowaboutmalaria.Whenevertheycomesoas.Whenevertheygotothosehealthcenters,theygohavingmindthattheyaresufferingfrommalaria.Asalsotheyhavebeentrained,peoplearemostofthetimebeingtrainedaboutmalaria,sohethinksthattheyknowit’.
Theseexamplesshowthatthereareactorswhothinkthattherearecommunitymemberswhobelieveinbewitcheryandpoisonousactivitiesandgototraditionalhealerswhensickinsteadofgoingtothehealthcenter.However,thetraditionalhealerthatwasinterviewedthinksthatthereisenoughknowledgeaboutmalaria.

57
EatingmaizesticksAnothermisconceptionthatwasmentionedduringtheinterviewsisthat
malariamaybecausedbyeatingmaizesticks.Thetranslatormentionedthatamemberofthericecooperativeexplained:
‘Shehasgivenanexamplewherebyshewasthinkingthatmalariamaybecausedbymaizesticks.Mostofmaizesticks.Inheradolescenceshegrowshegrewupthinkingthatmalariawascausedbymaizesticks.Anduntilnoweventoughshehasbeentrained,shehasbeeninformedaboutmalaria.Butisatthefirstpositionattellingherchildrentonoteatthosemaizesticks.Becauseshethinksalsothattheremaybesomethingbadregardingtomalaria.Andshealsosheisinformedaboutmalariaasshegrowuphavingsuch,itislikeaculture,shehasexplainedthatitislikeaculture.Shegrowupunderstandingpeopletalking,understandingpeopletalkingaboutthatmalariaiscausebymaizesticks,soshethinksthatalsothereissomethinghiddenbehind’.
Thisexampleshowsthateatingmaizesticksisanotherperceivedmisconception.
EatingsugarcanesActorssuchastheRwandaBiomedicalCentermentionedthatanother
misconceptionisthatpeoplebelievethateatingsugarcanescausesmalaria.Afteraskingwhythismisconceptionisexistshesaid:
‘Youknow,howcanIsay.Butthisismyinsight.Hm.Itdependsoneducationofpeople.Ithinkitislinkedtothelevelofeducationofpeople.Andalsowelfare.Welfareandalsolevelofeducationofpeople’.
ThisexampleshowsthattheintervieweefromtheRwandaBiomedicalCenterthinksthatmisconceptionsaretherebecauseoflowlevelofeducation.
DrizzleandnewlyharvestedbeansTheprivatepharmacistgavetwootherexamplesofmisconceptions,
whicharesmallrainandeatingnewlyharvestedbeans.Thetranslatorstatedthatheexplained:
‘Therearesomepeoplewhohavemisunderstandingsaboutmalaria.Hehasgivendifferentexampleswherebyhehasexplainedsmallrain.Therearesomepeoplewhoarenowadayswhoarebelievingthatthisrainthatisnotsufficient.Afterbeingcaughtbythissmallrain,theremaybemalaria.Becauseofbeingcaughtbysuchsmallrain.Andalsonewlyharvestedbeans.Somepeoplearenowbelievingthatnewlyharvestedbeansareattheleavesofmalaria.Thesebeansthatarenownewlyharvested.Whicharenowcookedwithouthavingwithoutbeingputatthesun,performingdifferent’.
Thisquotationshowsthatthereareperceivedmisconceptionsthatmalariaiscausedbydrizzleandbyeatingnewlyharvestedbeans.
MedicinesatthehealthcenterdonotcuremalariaAnothermisconceptionthatwasfrequentlymentionedisthatthereare
communitymemberswhodonotbelievethatthetabletsatthehealthcenterstillcuremalaria.Table24givesexamplesofstatementsthatillustratethattherearecommunitymemberswhodonotbelievethatthetabletsstillcuremalaria.

58
Table24:ExamplesofstatementsthatillustratethattherearecommunitymemberswhodonotbelievethatthetabletsstillcuremalariaActor Supportingquotation(translatedbyresearchassistantduringinterviews)Healthcenterstaff
’Peoplethinkdifferenttomalaria.Therearesomepeoplewhoarenowthinkingthatthemedicalmentsthattheyarenowbeinggivenhereathealthcenterhavebecomelikebeans’.‘Theydon’tconsiderthosemedicalmentsasrealmedicalments.Theyconsiderthoseseeds.Andtheysaythosemedicalmentsfromhealthcenterarenolongercuringus.Soitmeansthereisnoneedofgoingtherebecausetheirmedicalmentsaresomehowunabletocureelements’.
Communitymembers
’Aresomemedicalmentsdecreasestheircapacityofcuringmalaria?Howaremedicalmentsnowbeing,howaremedicalmentsnowcuringmalaria?Maybemedicalmentsarebeingexpired,becausemalariahasexceededitslimits.Thepeoplearewonderingthemselveswhethermedicalmentshaveexpired’.‘Thenheproposedthattheymaygetothertreatmentothertabletsothermedicalmentswhicharechanged,whicharenewlychanged.Becausethesemedicalmentsthattheyaretakingnowadaysarenotsufficient,arenotabletocuremalaria.Theyneedimprovement,theyneedinnovationwithinmedicalmentproduction’.’Inadditiontothatpeoplearenowadaysmumblingaboutmalaria.Theyaretalkingaboutdifferentviews,sayingthatmalariaisnowdrugresistant.Whatdoesthegovernmenthelpussoastogetmedicalmentsformalaria?Malariahasbecomedrugresistantanditneedsnewmedicalments.Medicalmentsthatarenowadaysbeingusedarenotablearenotgoodatcuringmalaria.Soweneedsupportfromthegovernmentorfromthenursessoastosupportustogetnewmedicalments.Becausethemedicalmentsthatarenowadaysbeingusedisnotappropriate’.
Thetableaboveshowsthattherearecommunitymemberswhowonder
whetherthemedicinesarestillcuringmalaria.Othersmentionedtheneedfornewmedicinestocuremalaria,astheybelievethatmalariahasbecomedrugresistant.Thequotationsinthetableillustratethatseveralactorsthinkthatmedicinesnolongercuremalaria.
UnbalanceddietandfoodthatisnotwellpreparedInaddition,anothermisconceptionmentionedbytheheadofthehealth
centeristhatsomepeoplebelievethatmalariaiscausedbyunbalanceddietandfoodthatisnotwellprepared.Duringtheinterviewwithhertheresearchassistanttranslated:
‘Theunderstandingsofthepeople,themisconceptionsofthepeoplearedifferentaccordingtotheirlevelofbeingataccordingtothelevelofunderstanding.Ignorancewithincommunity.Therearesomepeoplewhoareignorantaboutthiskindofmalaria.Andtherearealsosomepeoplewhothinkthattheymaygetthiskindofillnessfromunbalanceddiet.Thisfoodthatiswellprepared.Throughconsumption,theremaytheymaygetmalaria.Itmeansthatsomepeoplethinkdifferentlyaboutthiskindofsickness’.
Thisquotationexplainsthattheheadofthehealthcenterthinksthattherearecommunitymemberswhobelievethatmalariaiscausedbyunbalanceddietandfoodthatisnotwellprepared.
Themostimportantfindingsinthissub-sectionarethatthemajorityofactorsperceivetheknowledgeaboutmalarianottobeenoughinRuhuha.Accordingtotheseactorsthereisaneedforcontinuousteachingtoincreaseknowledge.Otheractorsexplainedthatknowledgeisthere,butthatthe

59
preventivemeasuresarenotappliedenough.Furthermore,accordingtoanumberofactorstherearestillsomemisconceptionsaboutmalaria.FormyresearchthesefindingsmeanthattherecouldalsobedisadvantagestoICTs,astheyinthiscasecanfacilitatethespreadofmisconceptions.Furthermore,thefindingsdescribedabovealsomeanthattherearegapsintheinformationflowsasmanystakeholdersmentionedthattheythinkthatknowledgeaboutmalariaisnotenoughinRuhuha.However,earlierwasalsoidentifiedthatcommunitymembersperceivemalariaasagrowingproblemwithinthecommunityandthatawarenessishigh.Asactorsfrombothhealthandnon-healthrelatedactorsfromalllevelsmentionedthattherearemisconceptionsandthatknowledgeaboutmalariaisnotenough,thefollowingsectionwillanalyzehowthedifferentactorsascribelegitimacytotheinformationtheyreceive,focusingontheroleoftrust.
5.3.4TrustTheprevioussectionexplainedwhetheractorsthoughtthereis(enough)
knowledgeaboutmalariaandwhethertherearemisconceptionsaboutmalaria.Thissectionidentifieswhetherthereistrustamongactorstoseehowknowledgeisgraspedorwithdrawn.Firsttheactorsthataretrustedwillbedescribed,followedbytheactorsthatarenottrusted.
5.3.4.1ActorsthataretrustedWhenaskedaboutwhomtheytrustmostwhengettingreliable
informationaboutmalaria,thecommunitymembersmainlymentionedtheytrustinthecommunityhealthworkersandthenursesorstaffofthehealthcenter.Furthermore,theyalsomentionedtheybelieveinlocalleadersandreligiousleadersastheysharethesameinformationcomparedtothecommunityhealthworkersandthehealthcenter.Thereasonsaredescribedinmoredetailbelow.
CommunityhealthworkersarepartofthecommunityThecommunitymembersbelieveincommunityhealthworkers,because
thecommunitymembersselectthecommunityhealthworkersatlocallevelthemselves.Communitymembermentionedthattheytrustcommunityhealthworkers,becausetheyarepartofthecommunity.Duringaninterviewwithacommunitymembertheresearchassistanttranslated:
’Youknowwhytheymostlybelieveinthiscommunityhealthworkers.Theyarenotmosteducatedbecausemosthaveprimaryeducationbutatprimarylevel,butbecausetheyareinthosevillages.Theyknoweachhousehold.Theyarenotoutsidefromthevillages.Sotheybelieveaslongastheyarepartofustheyarewithineithermyneighbor,ormyrelative,ormyfriendsotheybelievewhatevertheinformationtheyget,theyarecorrect’.
Thisexampleshowsthatcommunitymembersbelieveinthecommunityhealthworkersastheyarepartofthecommunity.Anothercommunitymemberalsomentionedthisandthetranslatorstated:
‘Theybelieveinthosecommunityhealthworkersbecausewheneverapersonissufferingfromanydisease.Sheorhecallsthecommunityhealthworkerforsupport.Mostofthetimeshealthcommunityworkersaretogetherwiththepersonsaretogetherwiththepatientsinlocalareas.Sotheybelieveinthemandtheyconsiderthemas

60
nurses.Andtheyconsidersuchactivity.Shehasgivenanexamplewherebyhealthvillage,healthcommunityworkers,maytellsuchpersonstoremovetoputoffthecloths.Andimmediatelyheorshewouldputoff,becauseofbelievinginthem.Theyarecommunityhealthworkersaretotallybelievedinlocalareas’.
Furthermore,anothercommunitymembermentionedthatcommunityhealthworkersarebelievedbecausetheycheckinformationthattheyreceivedfromothercommunicationchannelswiththecommunityhealthworkers.Thetranslatorstatedthatanothercommunitymembermentioned:
‘Theybelieveinallpersonsbutthosepersonsarenotatthesamelevel.Communityhealthworkersaretotallybelieved.Andotherpersonsarenottotallybelieved.Becausewheneverapersonseesorhearsinformationfromtheradio.Sheorheimmediatelygotothecommunityhealthworkertoaskhaveyouunderstoodwhatisbeingadvertisedonradio?Haveyouseenwhathasbeenspreadattv?HaveyouwatchedTV?Theygothereathealthcommunityworkers,soastoaskmore.Believingthatthosecommunityhealthworkersaretotallyinformed’.
Theseexamplesshowthatcommunityhealthworkersaretrustedbycommunitymembers,becausetheyarepartofthecommunity.
NurseshavestudiedandareliterateThecommunitymembersbelieveininformationfromnursesbecause
theythinkthatnurseshavestudiedandthattheyarespecialized.Theresearchassistanttranslatedanexampleduringaninterviewwithacommunitymember:
‘Theymosttrustthosenurse,becausetheythinktheyareliterate,theyhavespecializedwithinsuchspecificationandtheyarealsogoodatworkingtheirduty.Sotheythinkbecauseofbeingliterate.Becauseofhavingknowledge,becauseofstudyingtheybelievethatnursesaremostlyrelied’.
Furthermore,anothercommunitymembermentionedthattheytrustnursesbecausetheyrelyonthem.Theresearchassistanttranslatedbystating:
‘Andtheyalsobelieveinthosenursesbecausethepeoplethinkthatnurseshavetheirlivesintheirhands.Soitmeansthatthenursestakecareoftheirlives,takecareofthelivesofthepeople’.
Theseexamplesillustratethatcommunitymemberstrustnursesastheyareliterateandbecausetheyhavestudiedtotakecareoftheirlives.
LocalleadersandreligiousleaderssourcesaretrustedInaddition,communitymembersmentionedtheybelieveinlocalleaders
andchurchrepresentatives.Theresearchassistanttranslatedduringaninterviewwithacommunitymember:‘Theybelieveinthoselocalleaders.Theybelievealsointhosecommunityhealthworkers.Inthosechurchesrepresentatives,likepriests’.Anothercommunitymembergaveanexampleonwhytheytrustlocalleaders,theresearchassistanttranslated:
‘Itmeans,shehasgivenanexamplethatthosechiefofvillage,thechiefsofvillagesarealsoreliable,becausesuchinformationthatthechiefsofvillagestellthemismostofthetimegottenfromthisplace.Ismostofthetimegottenfromhigherlevel,sotheirinformationisreliable’.

61
Thisexampleshowsthatlocalleadersaretrustedbecausetheirsourceofinformationseemsreliable.Furthermore,thecommunitymembersbelieveintheinformationthattheygetfromleaders,becausetheinformationissimilartoinformationthattheyreceivefromotherchannels.Duringaninterviewwithacommunitymemberthetranslatorstated:
‘Mostofthetimetheybelievein,theytrust,communityhealthworkersandnurses.Buteventhoughtheybelieveinthose,theyalsobelieveinthoseleaders.Becausewhentheycomeforameetingandtalkaboutmalaria.Thereisalinkbetweenthisinformationfromleadersandlinkbetween,thereissimilarity.Thereisnodifferencebetweenthisinformationfromdifferentareas,fromdifferentspeakers.Thereisnodifference’.
Therefore,thesequotationsshowthatcommunitymemberstrustlocalleadersandreligiousleaderswhenitcomestogettingreliableinformationaboutmalaria,becausetheirsourcesaretrustedandbecausetheinformationissimilartotheadvisereceivedfromotheractors.
WhatsAppistrustedbecauseliteratepersonsshareinformationRegardingthesocialmediachannels,communitymemberssaidtobelieve
WhatsAppmorethanFacebook.Thetranslatorstatedthatacommunitymembermentioned:
‘Shereallytrusts,shereallybelievesinWhatsAppinformation.BecauseWhatsAppisaplacewhereliteratepeople.Doctors,leaders,aregatheredsoastosharetheinformation.Sosheisnowsayingthatshedoesnotthinkthatthoseliteratepeopledoctorsleadersmaypostinformationthatisnotreliable.ShebelievesinWhatsApp’.
ThisstatementshowsthataccordingtothiscommunitymemberWhatsAppistrusted,becauseliteratepersonsshareinformationthroughWhatsApp.
5.3.4.2ActorsthatarenottrustedWhencommunitymemberswereaskedwhomtheydonottrustwhenit
comestospreadingreliableinformationaboutmalariatheymentionedtraditionalhealers,illiteratepersons,neighbors,privatepharmacies,andFacebook.Thereasonswhytheymentionedthattheydonotbelieveintheseactorsareexplainedintheparagraphsbelow.
TraditionalhealersdonotprescribetabletsorexaminepatientsThecommunitymembersdonotbelieveintraditionalhealers.Duringan
interviewwithacommunitymemberthetranslatorstated:’Whenthepeoplecomehereathealthcentertheyaregivensometabletsastoreducefever.Thensuchtabletsarenotseenthereattraditionalhealers.Andinadditiontothisisthatthosetraditionalhealersdonotexaminethepeople.Whereashereathealthcenterpeopleareexaminedandcontrolledsoastotestifytheexamsfromsuchexamination.Thoseherbalistdonotexaminethepeople,sothatiswhytheydonotbelieveinthem’.
Thisexampleshowsthatthiscommunitymemberdoesnotbelieveintraditionalhealers,becausetraditionalhealersdonotexaminepatientsbeforesubscribingorsellingtablets.

62
TraditionalhealerslieforsurvivalmeansDifferentactorsperceivedtraditionalhealerstotelluntrueinformation
forbusinesspurposes.Thetranslatorstatedthatacommunitymembermentioned:
’Thosetraditionalhealersspreadrumorssoastogetsurvivalmeans.Theydon’t,mostofthetimetheydon’ttalktheydon’ttellthetruth.Theywanttogainsomethingsoastosurvive.So,mostofthetimetheydon’ttellthepeoplethetruthasitis’.
Furthermore,theheadofthedistricthospitalalsomentionedtraditionalhealerswhenaskediftherearepeoplespreadinginformationaboutmalariathatisnotreliable.Hestated:
‘Fortunatelytheyarenotverymany,theyarenotmany.Butalthoughtherearesomefew,fewpersons.Notablythistraditionalhealers.Becausesomeofthemtheyneedmoney.Theydobusiness.Sotheymisleadpeopletellingthemthatisnotmalaria,itisanotherdiseasethattheycantreat.Ya.Buttheyarenotmany’.
Thesequotationsillustratethatsomeactorsthinkthattraditionalhealersmisleadcommunitymembersforsurvivalmeans.
CommunitymembersdonotbelieveinilliteratepersonsFurthermore,communitymembersmentionedthattheydonotbelievein
illiteratepeople.Theresearchassistanttranslatedthatacommunitymembermentioned:
‘Yeahbecausetheycan’ttrustwhattheyarespeaking.Theytrustinliteratepeople,arevillageadvisorsandthosewhoarehereathealthcenters.Theybelieveinthose,theybelieveinvillageadvisorsandthosethatareathealthcenterotherthanpeoplewhoarespreadingrumorsinruralareasandbeingilliterate’.
Thisstatementillustratesthatcommunitymembersdonotbelieveinilliteratepersons,becausetheythinkthattheyspreadrumors.
CommunitymembersdonotbelieveinuntrainedpersonsMoreover,communitymembersexplainednottotrustallinformation
fromneighborsorpeoplewhoareatthesamelevelasthem.Duringaninterviewwithacommunitymemberthetranslatorstated:
‘Webelievealsointhembutthepeoplewhowedon’tbelieveinarethosewhomareatthesamelevel.Forexamplemyneighbor.Hecomesandtalkstometotellmeaboutmalaria.IwillbecautiousIwillbeattentiveatwhatheorsheisspeaking.Becausetheremaybelies.Theremayberumors.Andhehasmentionedthatthosewhoarenotbelievedarethosepeoplewhoareatthesamelevellikelocalpeoples’.
Thisexampleshowsthatcommunitymembersarecarefulwithtrustinginformationaboutmalariareceivingfromneighbors.Anothercommunitymemberalsomentionedthatneighborsarenottrustedwhenitcomestospreadinginformationaboutmalaria,theresearchassistanttranslated:
‘SoifIgodirecttotheneighborssometimestheneighborwillthinkwhoareyoutalkingtome.Areyouatrainedcommunityhealthworker.Doyouhaveanyroleinthevillage?Butwhenthecommunityhealthworker,iseasyforhim’.

63
Thesequotationsillustratethatcommunitymembersdonotbelieveininformationfromuntrainedpersons.
FacebookisnottrustedbecauseanyonecanpostinformationAcommunitymemberexplainedthatshedoesnottrustallthe
informationfromFacebook.Theresearchassistanttranslated:’Amongthosesocialmediasthatsheread,mostofthetimeshedoesn’treallybelieveinFacebook.ShehasmentionedwhyshehasnotbelievedinFacebook,becauseFacebookincludesthosepersonsfromdifferentfaroffareas.Andamongthosepersons,becauseFacebookdoesnotrequireusingsmartphonesandthosephoneswhichareexpensive.SoitmeansthatFacebookischeaperthanWhatsApp.Thenduetothefactthatthoseparticipants,thoseusersofFacebookarealsodifferentorarealsolowertocomparedto,socially,arelowersocially.Donotpossesmuchmoney,socially.Donothaveacapacityofusingthosesmartphones.Thepeopleamongthoseusersaresometimesofthefaroffareasincludingstreetchildren,includingrobbersandsoon.SotheymayposttheinformationwhichisnottrueatFacebook.Itisinsuchcase,itissuchreason,thatshedoesnotreallybelieveinFacebookbecauseFacebookincludesthosepersonsfromfaroffareas.Yawhocannotbetrusted’.
ThisexampleshowsthatthiscommunitymemberthinksthatFacebookcannotbetrustedwhenitcomestogettinginformationaboutmalaria,becauseanypersoncanpostinformationonFacebook.
PrivatepharmaciesdonotperformexaminationsandcanbeuntrainedInaddition,acommunitymemberexplainedhedoesnottrustsmall
privatepharmacies.Theresearchassistanttranslatedthathementioned:‘Theydon’tbelieveinthosepharmaciesinthoselittlepharmaciesbecausemostofthemrecruitpeoplethatarenotspecialized.Recruitpeoplewhoarespecializedwithinotherareas.Sobecauseofsuch,duetosuchtheydon’tbelieveinthoselittlepharmacies’.
Thiscommunitymemberdoesnotbelieveinsmallprivatepharmacies,becausethestaffcanbeuntrained.Anothercommunitymemberalsomentionedhedoesnotbelieveinprivatepharmacies.Theresearchassistanttranslated:
‘Hehasexplainedthathedoesn’tbelieveinthosepharmacies.Hehasexplainedthatthosepharmaciesaremostofthetimefightingfortheirprivateprofit.Hehasexplainedthatalsothattheseprivatepharmacies,wheneverpersonisenteringsoastotakesuchmedicaltreatmentwithinpharmacy.Theyunderstand,theyfirstlyunderstandsignsandtryandstartprescribingmedicalments.Beforeperformingexaminations.Theywrite,theyprescribemedicalments.Itmeansthattheywritemedicalmentsinsteadofperformingthoseexaminations,patientexaminations.Theydon’tperformpatientexaminations.Theyonlywritemedicalmentsthattheyunderstandthatsuchpatientisinneed.Theydon’tcarryouttheexaminations.Sotheydon’tbelieveinthisinformationgotfrompharmacy,becausetheythinkthattheydon’tperformexaminationsasherecomparedtothishealthcenters’.

64
Thisexampleshowsthatthiscommunitymemberthinksthattheinformationfromprivatepharmaciescannotbetrusted,becauseprivatepharmaciessellmedicineswithoutperforminganyexaminations. Themostimportantfindingsinthissub-sectionarethatcommunitymemberstruststakeholderswhenitcomestospreadingreliableinformationaboutmalariawhentheythinkthattheseactorshavestudied,areliterate,orwhentheinformationissimilartotheactorsthattheytrust.Furthermore,communitymembersdonottrustsourcesofinformationwhentheactorsdonotexaminepatientsorprescribemedicines,areilliterate,untrained,orbecauseanypersoncanpostinformationonFacebook.FormyresearchthesefindingsmeanthatICTsbothhaveadvantagesanddisadvantages.Communitymemberscanmoreeasilyreachtrustedactorstoaskforinformationoradvise.Moreover,ICTsalsofacilitatethespreadofinformationaboutmalariafromthetrustedactorstothecommunitymembers.However,notalltheinformationthatissharedthroughICTsistrustworthy.
5.3.5SharedperspectiveoftheproblemThepreviouslyidentifiedactorshavetocooperateandworktogetherto
achieveasharedgoalofbattlingmalaria.Therefore,thissectionanalyzeswhetheractorshaveasharedperspectiveoftheproblemthatneedstobesolved.Furthermore,itanalyzestowhatextenttheseperceptionsaresharedbymultiplestakeholdergroups.ProblemsregardingmalariapreventionandcontrolinRuhuhathatwerementionedduringtheinterviewsareillustratedintable25.
Table25:WhatproblemswerementionedbywhichactorsProblems Mentionedbythefollowingactors StakeholdergroupsLackofmosquitonetswhicharenotavailableandmosquitonetswhichareexpired
Fivecommunitymembers,cooperative,healthcenterstaff,communityhealthworkers,CMAT,nationalhealthinsurance,headofthehealthcenter
-Communitymembers-Healthrelatedcommunitylevelactors
Tablets Fivecommunitymembers,cooperative,healthcenterstaff,communityhealthworker,healthcenterpharmacy,privatepharmacy
-Communitymembersandcooperative-Healthrelatedcommunitylevelactors
Notusingpreventivemeasuresproperly
Twocommunitymembers,communitymemberswithouthealthinsurance,healthcenterstaff,communityhealthworker,nationalhealthinsurancescheme,districthospital,privatepharmacy,headofthehealthcenter
-Communitymembers-Healthrelatedactorsfromalllevels
Poverty Twocommunitymembers,healthcenterstaff,communitymemberwithouthealthinsurance,districthospital,privatepharmacy,headofthehealthcenter
-Communitymembers-Healthrelatedactorsfromcommunityanddistrictlevel
Fumigationnotbeingcarriedout
Twocommunitymembers,healthcenterstaff,CMAT,RBC,nationalhealthinsurancescheme
-Communitymembers-Healthrelatedactorsfromcommunityandnationallevel
Beliefinbewitcheryandpoisonousactivities
Communitymember,healthcenterpharmacy,localleader,districthospital
-Variousactorsfromcommunityanddistrictlevel
Bedbugs Communitymember,MEPR,districthospital,headofthehealthcenter
-Communitymembers-Healthrelatedactorsfromcommunityand

65
districtlevelRemovingplantationsaroundthehousewhiletheyareimportant
Twocommunitymembers -Communitymembers
Lackoftimelyresponseand(financial)resources
RBC,districthospital -Healthrelatedactorsfromnationalanddistrictlevel
Waterscarcity Healthcenterpharmacy -Healthrelatedcommunitylevelactor
Ascanbeanalyzedfromthetable,theproblemsaremainlymentionedby
healthrelatedactorsandbycommunitymembers.Problemsrelatedtotheavailabilityofmosquitonets,tablets,useofpreventivemeasures,povertyandfumigationaremostfrequentlymentioned.Moreover,problemsrelatedtotheavailabilityofmosquitonets,tablets,removingplantations,andwaterscarcityareonlymentionedbycommunitylevelactors.Furthermore,problemsrelatedtothelackoftimelyresponseand(financial)resourcesareonlymentionedbydistrictandnationallevelactors.Theproblemsinthetableaboveareperceptionsbyactorsandareexplainedinmoredetailbelow.
MosquitobednetsFurthermore,communitylevelactorsdescribedthatthereisalackof
availablemosquitonets.Thereareanumberofpeoplewhodonotsleepinbednets.Thenetscannotbeboughtanywhere.Thecommunitymembersexplainedthattheyarewaitingforthehealthcentertogetmosquitonets.Communitymembersarewonderinghowtheycangetmosquitonets.Onecommunitymembergaveanexamplethatithasbeentwoyearssincethegovernmentdistributedbednetsandcampaigned.Hesaidthatnowadaystheycannotevenfindwheretobuythem,butthathewouldbewillingtospendsomemoneytobuybednetsinsteadofwaitingtogetthemforfreefromthegovernment.TheRuhuhahealthcenterstaffmentionedthelackofbednetsasaproblemaswell.Duringthisinterviewthetranslatorstated:
‘Thesefumigants,theseproductsthatare,thesefumigationsinmosquitonetsisnotaccessible.Heiswonderingwhatcanwedo?Whatcanwedotopreventthosepeoplesufferfrommalariawhiletheysleepinthosehouseswithouthavingmosquitonets.Andwehavenocapacityofgivingthemmosquitonets.Whatwedohereiscuringthosepeoplewhohavebeenattackedorattacked,givingthemmedicalments.Butthematerials,thewayofgettingmaterials,thesupportofmaterials,thisexceedsourimagination’.
AnotherstaffmemberoftheRuhuhahealthcenteralsoexplainedtheproblemofbednetsnotbeingavailable.Theresearchassistanttranslated:
‘Whatisattherootofthisproblem,theincreasementoftheincreasingofthemalariaisthatpeoplearenowdonothavemosquitonets.Therearemosquitonetsthattheyusedtohave,buttheyarenowoldandtheyarenotfunctioning.Eventhegovernmentknowstheproblem.Buttheproblemhasnotyetgiventhosemosquitonetssoastohelpthem.Thosemosquitonetshelpthosenursesbecausewhenthereisavailability,whenthereisaccessibilityofmosquitonetspeoplearenotsufferingfrommalaria.Itmeans

66
thatpeoplearenowstillsufferingfrommalariabecauseoftheirdiscusofthosemosquitonetsthatarenownotbeingavailable’.
Furthermore,acommunityhealthworkerexplainedthatbednetsarenotproducedinRwanda.Thetranslatorstatedthathementioned:
‘Mosquitonetsarefromabroad.Arefromforeigncountries.WherebyshehasemphasizedthatRwandahasnocapacityofproducingthosenets.Sothosenetsarefromoutside.Ya.Andaftergettingthosematerialsfromoutsidethecountry,Rwandaisinchargeofgivingthesematerialstopeoplesoastosupportthemtofightagainstmalaria’.
InadditiontheCMATrepresentativeexplainedthatthebednetsthatarecurrentlyusedareoldandthattheyhaveexpired.Theresearchassistanttranslated:
‘Wheneverpeoplefollowtherulesthatareregulatedsoastofightagainstmalaria,malariawillberemoved.Butexceptthetimewhenthesematerialsthatareusedtoprevent.Likemosquitonets,thosematerialsthatareusedtofightagainstmalaria.Wherethosematerialsarenotuptodate.Areold.Becausenowadayssomepeoplehavethosematerialsthatareold.Likemosquitonetswhichareold.Thismeansthattheywillnotfightagainstmalariabecausethematerialswhichistheretosupportthemisnotfunctioning’.
TheRwandanBiomedicalCenter,whoisinchargeofdistributingbednets,stated:
‘CurrentlyweareusingbednetsandlastyearinJanuary/Februarywedistributedthebednetsandcoveringthehouseholdbyhousehold.Butunfortunatelywehavenotfoundadeclineofmalariaafterthedistributionofbetnets.Wedon'tknowwhathappened.Resistancetoorinsecticideusedfortreatmentofbednet,wedon'tknow’.
ThisstatementillustratedthattheRwandaBiomedicalCenterdoesnotknowwhymalariadidnotdeclineafterthedistributionofbednets.TheheadofRuhuhahealthcenterexplainedthisinformationgapbetweenRBCandwhatishappeningonthegroundthatmalariaisnotdecreasing.Theresearchassistantstatedthatsheexplained:
’Governmentexpectthatmosquitonetshastobeexpiredintwoyears.Itmeansthatmosquitonetsisgivenonceeverytwoyears.Thenafterspending,becauseofthepovertyofthepeople.Andbecauseoftheconditionstheylivein,sheexplainedthisbygivinganexamplewherebysomepeoplearelivinginmudhouses.Wherebythereisnocementinthehouses,thereisnofloorandthehousesaresomehowinappropriate.Thenhavingthislifeconditions,thislifeconditionsthatisdifficultalsoisatthebaseofcausingthisproblemoflackingmosquitonets.Becausewheneverthispersonwholivesinthismuddyhouse,wheneverheisgiventhismosquitonets.Andwheneverthismosquitonetisgoingtobeestablished,isgoingtobeput,isgoingtobesetwithintheirhouseathisorherbed.Thereisnomattressthere,thereisnobedthere,therearesomegrassestherewherebysheorheorshespreadsthismat.Thenputtingtheremosquitonetisdifficultbecauseofsuchlifeconditions.Andwithin

67
thesegrasses,withintheseleavesofthebananaswherebytheysleep,theremayalsoraisesomeotherinsects,bedbugs.Likebedbugsandsomeotherlikethoseofjiggas.Throughthesebadinsectsthisbadconditionthattheylivein.Theymaysaythatmosquitonetalsoincludeswithintheseisalsoatthebaseofthesebedbugs.Letmeputitasideorburnit.Thentheyburnitwithoutspendingtwoyearsexpected.Thenafterburningthismosquitonetearlier,comparedtothetimethathasexpectedbythegovernmentthemosquitonetisnotavailable.Mostofthepeopleperformthis,thenwithincertainperiod,ashortperiod,nottwoyears,thosemosquitonetsarenotaccessible.Itmeansthattheirlifeconditions,theirpovertyinwhichtheylivealsoisattherootofthesemosquitonetsgivenbythegovernment.Expectingthatthosemosquitonetsmayperpetuatemayhavedurabletimeoftwoyears.Itisimpossiblebecauseofthepovertythatpeoplearenowsufferingfrom’.
ThisquotationshowsthataccordingtotheheadofRuhuhahealthcenterthereasonwhymalariadidnotdeclineafterthedistributionofbednetsisbecauseofpoverty,havingnobedstousemosquitonetsproperly,andbecausecommunitymembersburnthemosquitonetswhentheyfindbedbugs.
TabletsCommunitylevelactorsmentionedseveralproblemsregardingthe
tablets.Firstofallsomeactorsthinkthatthetabletsarenolongerabletocuremalariabecauseofdrugresistance.Communitymembersexplainedthattheythinkthatthemedicinesthattheyarenowadaystakingarenotabletocuremalaria.Thetabletsaresometimeschangedtonewones.Thecommunitymembersexpressedthatthecurrentmedicinesarenotcuringmalaria,becausemalariaattacksapersontwiceaweek.Therefore,theythinktheproblemiswiththetabletsandthattheyneedinnovationwithinmedicalproduction.Thecommunitymembersexplainedmalariahasbecomedrugresistant.Theythinkthatnowisthetimetochangethecurrenttabletsanduseanewdrug.Duringtheinterviewwiththehealthcenterstafftheresearchassistanttranslated:
‘Theydon’tconsiderthosemedicalmentsasrealmedicalments.Theyconsiderthoseseeds.Andtheysaythosemedicalmentsfromhealthcenterarenolongercuringus.Soitmeansthereisnoneedofgoingtherebecausetheirmedicalmentsaresomehowunabletocureelements’.
Thisstatementshowsthatthehealthcenterthinksthatitisaproblemthatthecommunitymembersthinkthatthemedicinesarenolongercuringthem,becauseinthesecasestheywillnotfeeltheneedtocometothehealthcenterforexaminationandtreatment.Othercommunitymembersalsomentionedthattheythinkthatthetabletsatthehealthcenterhaveexpired.
Moreover,actorsalsomentionedthattherearecommunitymemberswhosharetabletswiththeirchildrenathomeorwithneighbors.Theysharetabletsbecausetheyhavenocapacityormeanstoreachthehealthcenter.Thecommunityhealthworkersalsoexplainedthatthesharingoftabletsisaproblem.Thetabletsatthehealthcenteraregivenforfreewhenapersonhasahealthinsurance.Asthetabletsareforfreecommunitymemberssharethetabletswithfamilymembersathome.Whenpeoplegotoaprivatepharmacy

68
theyarechargedforthetablets.Becausetheyarechargedarelativelyhigherpricecommunitymembersdonotsharethosetabletsfromaprivatepharmacywithfamilymembersathome.Therefore,thetabletsatthehealthcenterdonotcuremalariabecausetheyarebeingusedinanimproperwaycomparedtothetabletsboughtfromaprivatepharmacy.Recentlytherehavebeenrumorssayingthatthetabletsgivenathealthcenterarenotabletocuremalaria,whiletabletssoldat3500to6000RwandanFrancbyprivatepharmaciesareabletocurethedisease.Immediatelythehealthcentercalledthecommunityhealthworkerstoshowthemthatthetabletssoldattheprivatepharmaciesarethesamecomparedtotheonesatthehealthcenter.Accordingtothehealthcentertheproblemisthatpeoplegowithintheirlocalareaswiththetabletsfromhealthcenterandstartsharingthetabletswithfamilymembers.Afterwards,theyhavenottakenthenecessaryquantitytocuremalariaasexpected.Thisisthereasonwhyaccordingtothecommunityhealthworkerpeoplearenowspreadingrumorsandinformationregardingthetabletsthatisnottrue.
NotusingpreventivemeasuresproperlyRuhuhahealthcenterstaffmentionedthatoneproblemisthatthepeople
arenotawareofmalaria.Sheexplainedthatapatientmayreceivetabletsformalaria.Whiletakingthesetabletsshemaybestungbyamosquitoathomeagainwhilerecoveringfromthepreviousmalaria.Aftertakingthetabletsthepersonstartsthinkingthatthetabletsdidnotcuremalaria,whileactuallyheorshewasattackedbymalariaagainbeforebeingrecovered.Thenthepeoplecometothehealthcenterandreportthattheywerenotcured.Therefore,thehealthcenterstaffexplainedthattheyarenowadaysdealingwithpeoplewhoarenotawareoffightingagainstmosquitosandusingthepreventivemeasureswhileconsumingtablets.Thesecommunitymembersarenotawarethatmalariamayattackthemwhiletakingtablets.Thiswasalsomentionedduringtheinterviewwiththehealthcenterpharmacy,theresearchassistanttranslated:
‘Somemedicalmentsmaybetakenproperly,thenattheendtheremaybeasting.Themosquitomaystingsuchpatientagain.Thenafterbeingstingtheremaybeproposition,theremaybesomeideasthatpatienthasnotbeencured.Yathisisthecase’.
Thehealthcenterpharmacyalsomentionedthatpeopleconsumethetabletsbadly.Afternotbeingcuredtheystartthinkingthetabletsdonotfunction.Thehealthcenterpharmacistgaveanexample,thetranslatorstated:
‘Themedicalmentsthatareprescribedwithinmalariaareconsumedwithindifferenthours.Therearesomesteps.Thereisfirststepandsecondstep.Firststepisafterapatientispresumedtotakemedicalmentsaftereighthours,butmostofthepeopleunderstandthattheywillconsumemedicalmentsafter12hours,afteraday.Thenafterconsumingthesemedicalmentsbadlytheymaynotbecured’.
TheRwandanBiomedicalCenteralsostatedthattheknowledgeintermsofpreventionisstilllowbymentioning:
‘Theknowledgeisveryhighintermsofdiagnosticandtreatmentofmalariaandsymptoms.Butknowledgeisstilllowintermsofprevention.Thegooduseofbednets.Evenofspraying.Andalsoothermethodsforprevention.Becausetherearedifferentmethods

69
forpreventionagainstmalaria.Buttheknowledgeisveryhighintermsofskillsintermsofhowtoknow,symptomsofmalaria,howtotreatmalaria,andsofort.Diagnosticofmalaria,butintermsofpreventionknowledgeisstilllow.Butecologyofmosquitos,knowledgeonmosquitosofthebreedingsites,mosquitolarvae,isstillverylowintermsofecologyofvectors.Knowledgestillverylow’.
ThiswasalsoconfirmedbytheheadofNyamataDistrictHospitalwhomentioned:
‘Andalsothelackofknowledgeofthepopulation.Aboutthepreventionagainstmalaria.Theydonothaveimportancetothisprevention’.
WhenaskedaboutthecauseoftheincreaseofmalariainRuhuhahesaid:‘Somecausesareduetolackofknowledgeofthepopulation.Theimportanceofsleepingundermosquitonets.Insteadofsleepingundermosquitonets.Theyusethesemosquitonetstofish,forfishing.Anduhmforotheractivities.Andothertheyrefusetosleepundermosquitonetspurposely’.
Theprivatepharmacistalsoexplainedthebaduseofpreventivemeasures.Duringthisinterviewtheresearchassistanttranslated:
‘Theunderstandingsofthepeoplearestillatlowlevel.Someofthemarenowstillsufferingbyarestillmeetingfacingthisproblemofnothavinggoodunderstandings.Wherebyilliteratebothilliterateandliteratepeopledonotusemosquitonets,someofthemdonotusemosquitonetsproperly.Hehasgivenanexamplewherebywifehiswifedoesnotusemosquitonets,whereasshereallyknowstheimportanceandtheroleofmosquitonet.Butthinkingthatthereishotnessandthinkingthatmosquitonetmaycauseotherrelatedproblemsshedoesn’tuseit.Itmeansthatthereislowunderstanding’.
Alltheseexamplesshowtheperspectivesofdifferentactorswhothinkthatmalariapreventionmeasuresarenotappliedproperly.
PovertyWheneverpatientsaresufferingfromseveremalariatheyare
transportedtothedistricthospital,buttherearepatientswhoescapebeforebeingtransportedbecauseofpoverty.Duringaninterviewwithahealthcenterstafftheresearchassistanttranslated:
’Wheneverpatientreacheshereandunderstandsthatheisorsheisgoingtobetransportedtohospitalshestartsthinking,Iamgoingtobetransportedtohospital,Ihavenofamilytocaremewhilebeingthereathospital,noonetobringmefood,noonetobringmeanythingsoastohelpmewhileIamthere,sowhyamIgoingtobetransportedthere.Thenafteranalyzingthissituationsheorheimmediatelyquitsthishealthcenter.Yathisispoverty’.Furthermore,somecommunitymembersalsohavenomoneytobuythe
communityhealthinsurance.Thetreatmentissomehowexpensiveatthehealthcenterwithouthealthinsurance.Forthisreason,thosethatdonothaveahealthinsuranceprefertogotoaprivatepharmacy.Ataprivatepharmacy,ifmedicinesare5000,acommunitymembercansayokformeIhave1000socanyougive

70
methemedicinefor1000.Thisisnotforthewholetreatmentandthiswillnotcuremalaria,sothisisanotherchallenge.Acommunitymemberwithouthealthinsurancementionedthatwheneverthetimeofbuyinginsurancecardscomes,therearesomepeoplewhohavenomeansofbuyingtheinsurancecards.Oneperson’sinsurancecardcosts3000RwandanFranc.Thismeansifafamilyexistsoftenpersons,itmeanstheyneed30000RwandanFranctobuyinsurancecards.Accordingtothiscommunitymemberitisimpossibleforthisfamilytobuytheseinsurancecards.Forthisreason,theybuydrugsataprivatepharmacy.Duringthisinterviewtheresearchassistanttranslatedthathementionedthatwheneverapersonshowsupatthehealthcenterwithoutaninsurancecard:‘Theywillconsiderhimorherassomeoneforeign,thentheywillchargemuchmoney’’.Heexplainedfurtherthatinsteadtheyattendprivatepharmaciesbystating:
‘Hehasexplainedthathedoesn’tbelieveinthosepharmacies.Hehasexplainedthatthosepharmaciesaremostofthetimefightingfortheirprivateprofit.Hehasexplainedthatalsothattheseprivatepharmacies,wheneverpersonisenteringsoastotakesuchmedicaltreatmentwithinpharmacy.Theyunderstand,theyfirstlyunderstandsignsandtryandstartprescribingmedicalments’.
Thisstatementshowsthathedoesnotcompletelytrustprivatepharmacies,howevertheresearchassistantalsotranslatedthattheyattendthembecauseofthefollowing:
‘Buttheyfoundtheysometimesfoundthemselvesinmiserableconditions.Theygotheresoastogetmedicaltreatment.Theygotoprivatepharmaciesnotthinkingthattheremaybebadinformation.Butbecauseoftheirpoverty,theirmiserableconditionstheygothere.Theyhavenothingtodoapartfromgoingthere.Theygotherebecauseoftheirpoverty.Theywanttobeinpeacefulconditionsbutbecauseofmiserableconditions,miserableconditionsdonotallowthemtobeinsuchpeacefulcondition.Sotheygothereforpovertyreasons’.Inaddition,thehealthcenterpharmacyexplainedthatitisaproblemthat
privatepharmaciesdonotgivemanydetailsaboutthemedicationtopatients.Therefore,peoplemaynotgetcuredasplannedbecausetherewasnoeducationattheprivatepharmacy.Aftersomedaysofbeingsickthosepatientsreachthehealthcenterbeingsicker.TheheadofNyamataDistrictHospitalstated:
‘Itisnotagoodpractice.Sowearetryingtodiscouragethisandtosensitizepeopletogointhehealthfacilitytobetested.Iftheyhavemalariatheybegivendrugsthere.Itisnotgoodtogototheprivatepharmacywithoutpassingthroughthehealthfacility’.Moreover,theheadofthehealthcentermentionedthatpovertyis
atthecauseofmalaria,becausepovertydoesnotallowcommunitymemberstoapplysomeofthepreventivemeasures.Duringthisinterviewtheresearchassistanttranslated:
’Sotheconclusionisinshort,povertyisreallythemajorleadingcauseofmalariaincrease.Becauseifpeoplearelivinginsuchconditionthenoneoftherealityisthesebedbugs.Becausebedbugstheyfeedonandtheyreallyfeedonblood.Soiftheyhavethisinfectionofbedbugsandespeciallywiththemosquitonetsbecauseinthenightthebedbugsgoesinthemosquitonetsandthenwhen

71
theyopenittheycomeandstarttofeedonthepeopleinthehouse.Thenpeoplearemore,theyremovequicklythemosquitonetandburnit.Sothatiswhytheydon’thaveanymoremosquitonets.Andthentheyarebecomingmoreoftentogetmalariafromthemosquitos’.
Theseexamplesshowthatanotherperceivedproblembydifferentactorsispoverty.
FumigationAccordingtodifferentactorsmalariaisincreasingduetothefactthatthe
actionoffumigationhasbeensuspended.Communitymembersgaveexampleswherebymalariahaddecreasedtwoyearsagowhentherewhereactivitiesrelatedtofumigationinhousesandswamps,butnowadaysitisnotbeingdone.AlsothememberofaCMATmentionedthatfumigationhasnotbeencarriedoutsince2016.ThetranslatormentionedthattheCMATmentioned:‘Thisfumigationtookplacewithin2016.Fromsuchyeartilltodayithasnotyettakenplace.Itmeansthatthislastyear.2017,theydidn’t.Tilltoday’.Communitymembersmentionedthataftersuspendingthoseproductsforfumigatingthehousesandswampsmalariahasincreasedatagreatnumber.ThestaffofRuhuhahealthcenteralsomentionedthisandtheresearchassistanttranslated:‘Thedecreaseorthislackoffumigationhascausedaproblemwherebymosquitosarenow,malariaisnowspreadingasaresultofusingthisfumigation’.Inaddition,theRwandaBiomedicalCenteralsomentionedthatmalariaincreasedsincefumigationhasstoppedbystating:
’IamnotupdatedaboutmalariainRuhuha.ButIknowthataftersprayingcampaign,wehavenotsprayedRuhuhaduringlastsprayingcampaignofSeptember.NowweareinJanuaryandwesprayedthereinFebruarylastyear,butSeptemberwehavenotsprayedthere.AndMalariaincreasedthere’.
ThepersoninterviewedattheNationalHealthInsuranceSchemewhowaspartoftheMEPRresearchprojectwithaBtiinterventionmentioned:
‘Thenweintroducedtheseapplicationoflarvaecide.Sowediditinjustonecultivationseason.Sothatafterthatcultivationseasonmalariamosquitosreduceddramatically.Butforaperiodaroundsixmonth.AndafterthatitwasabigproblembecausemosquitosstartedagaintoreproduceinmanynumbersthenIthinkwhenIwastherethelasttimeitwasabigchallengebecauseaftertheeffectsofBtithentheproblemofmalariabecameaseriousproblem’.
Theseexamplesillustratethatmultiplestakeholdergroupsperspectivesthelackoffumigationasaproblem.
BeliefinbewitcheryAnotherproblemthatwasmentionedbyseveralactorsisthebeliefin
bewitcheryandpoisonousactivities.Communitymembersexplainedthatwheneverapersonwhoisnotaccustomedtogettingmalariagetsmalariaheorshebecomesmad.Thenpeopleintheruralvillagesstarttalkingthatheorsheisbewitchedandimmediatelymovethispersontotraditionalhealers.Thelocalleadersaidthiscultureisnowuprooted,butgavetheexamplewhichthetranslatortranslated:

72
‘Thereisacasewherebytwoneighbors.Onemaysuspecttheothertobewitchortopoisonhimorher.Thenafterawhile,asthereisapatient,asoneofthemissufferingfromelement.Hesheissufferingfrommalaria.Thenafteracertainperiod.Insteadofcominghereathospital,shegoestotraditionalhealer.Thentraditionalhealerstartsayingyouhaveanopponent.Youhaveapersonwhoisopposingyouinyourvillage.Hehasbewitchedyou.Youhavebeenbewitched,youhavebeenpoisoned.Wherebythistraditionalhealerislyingandthepersonissufferingfrommalaria.Thepersonissufferingfrommalariabuttraditionalhealerissayingthatpersonissufferingfrombewitcheryactivities’.
TheheadofNyamataDistrictHospitalalsomentionedtheproblemofgoingtotraditionalhealersbysaying:
‘Andsometimestheyareill,insteadofgoingtothehealthfacilityorinsteadofgoingtothecommunityhealthworkertheyprefertogotolookfortraditionalhealer’.
Whenaskedaboutthereasonwhypeoplegotothetraditionalhealershementioned:
‘WhatIhaveseen,someofthemdonothavethiscommunitybasedhealthinsurance.Ya.Soiftheydonothavehealthinsurancetheyprefertogotothetraditionalhealerwholiveswiththem,nearbythem’.Thehealthcenterpharmacyalsoexplainedthataftergoingtotraditional
healerstogetcuredpatientstakelongtoreachthehealthcenter.Thenafterspendingalongtimeatthetraditionalhealerstryingtogetcuresinsteadofgoingtothehealthcenter,theyreachthehealthcenterbeingverysick.Inthesesituationsacommunitymemberisoftentakentothedistricthospitaltogetcured.
BedbugsDifferentintervieweesperceivedbedbugsanotherproblemregarding
malariapreventionandcontrol.Whenthecommunitymembersseebedbugsinthebednetstheyfearthembecausetheycauseaswelling.Theyprefertotakethewholebednetandthrowitawayorburnthenetsinsteadofremovingthebedbugs.Therefore,thebedbugsarealsoperceivedasaproblem.Itwasmentionedthatthecommunitymemberseitherneednewbednetsoranythingthatcankillthebedbugs,astheyarecommoninthisarea.
RemovingplantationsaroundthehouseCommunityhealthworkerseducatepeopleaboutthemalariaprevention
measuresincludingtheremovalofmosquitobreedingsites.Onecommunitymembergaveanexamplethatforthelasttwoyearstheyweretaughtnottoplantsorghumandmaizenearthehome,becausethisiswherethemosquitoscanliveandgrow.Anothercommunitymemberwonderedwhethertheyshouldremovebananaandsorghumplantationsnearbytheirhomewhiletheyareplayingagreatroleintheirlives.

73
Timelyresponseandlackof(financial)resourcesTheRwandanBiomedicalCentermentionedthatanotherproblem
regardingmalariapreventionandcontrolinRuhuhaistimelyresponse.Heexplainedthisbysaying:
‘Causeforthefirstweekofeachmonthwehavenewdata.Buttheissuesometimesisresponse.Ourissueisresponse.Weknowthatthereisaproblemthere.Butsometimesifyouwanttosprayitisabigproblemtofindoutmoney.Becauseforonelitter,uhmnoonedosage.Foronesquarepointthereisaroundcurrentlywithoutsubsidyisaround7.34USD.Butyoudon’tknow,tosprayonehouseisaroundprobably20euro.Ifyouwanttosprayonehousefor20eurosisveryexpensive,isveryexpensive.Butwearetargetinghighburdenareas’.
TheheadoftheNyamataDistrictHospitalexplainedanotherproblemregardingmalariapreventionandcontrolinRuhuhawasthelackofRDT(rapiddiagnostictests).Hestated:
‘Othercausesuhmduetolack,theyhadinsomeperiodsastakeoutofRDT,rapiddiagnostictestinthecommunity.Anduhm,somebugsalso.Uuhm,andinordertocombatmalariawehavetocombatitatlocallevelinthevillage.Soifthesecommunityhealthworkersdonothavecommodities,donothavethisRDTordrugs,peoplehavemighthavechancetodieinthecommunity.Orifeveniftheydonotdieinthecommunitytheycometoolateatthehealthfacility.Theycometoolateatthehealthfacility.Theyhaveseveremalaria,becausetheyhavedelayedathome,soitiswhereitisimportanttohavetheseRDTordrugsinthecommunity,sowecantreatmalaria,wecombatitthereatlocallevelinthecommunityinthevillage’.
Thesequotationsillustratethattimelyresponseandlackof(financial)resourcesisanotherproblemperceivedbyactorsfromthedistrictandnationallevel.
WaterscarcityAnotherproblemmentionedbyhealthcenterpharmacystaffisthat
withinBugeseraDistrictthereisscarcityofwater.ThereislesswatercomparedtootherregionsinRwandaandgettingwaterisdifficult.Therefore,whenitrainspeopleputthiswaterwithindifferentmaterialsthinkingthatinsomedaystherewillbeashortageofwater.Withinthisprocessofputtingwaterindifferentmaterialsathomemosquitosareattracted.Mosquitosliveandproduceandpeoplewithinhouseholdsorthosethatcollectwatermaysufferfrommalaria.
Themostimportantfindingsinthissub-sectionarethatthemajorityofproblemswerementionedbycommunitylevelactors.Thedistrictandnationallevelactorsdescribedtimelyresponseandlackoffinancialresourcesasaproblemwhichwasnotmentionedbythecommunitylevelactors.However,thisproblemisrelatedtoissuesdescribedbycommunitylevelactors,suchaslackofmosquitonetsandnofumigation.Otherproblemssuchasthoserelatedtotabletsandbeliefinbewitchery,arerelatedtomisconceptionsonthecommunitylevel.Furthermore,notusingpreventivemeasuresproperly,poverty,andbedbugswerementionedbymultiplestakeholdergroups.Theseproblemsaresomehowrelated,forexamplebecauseofpovertyandbedbugsmosquitonetsarenotusedproperly.RBCmentionedthatthemosquitonetswerelast

74
distributedin2016.Accordingtotheanalysisofthesituationregardingmalaria,andaccordingtoRBCmalariahasincreasedsincethen.Communitylevelactorsexplainedthatmanycommunitymembersdonothavebedstousethemosquitonetsinthewaytheyaresupposedtobeused.Inaddition,itwasmentionedthatsomecommunitymembersusethenetsforfishingandotherpurposes.Moreover,bedbugsareaprobleminRuhuhacausingcommunitymemberstoburnthemosquitonetswhentheyspotbedbugsinthenets.Nowthatmalariahasincreasedcommunitymemberswantmosquitonetsandseetheirimportance,howevertheyarenotavailable.Formyfindingsthismeansthatthereisamiscommunicationorlackofcommunicationbetweenstakeholderlevels,asforexampleRBCmentionedthat‘Butunfortunatelywehavenotfoundadeclineofmalariaafterthedistributionofbetnets.Wedon'tknowwhathappened.Resistancetoorinsecticideusedfortreatmentofbednet,wedon'tknow’,soapparentlytheyarenotawareoftheproblemsrelatedtopovertyandbedbugsidentifiedbycommunitylevelactorsthatexplainwhathappened.
Tosummarizethissection,firstofallactorsperceivedtheexaminationofpatients,teachingcommunitymembersaboutpreventionmeasures,facilitatingaccesstopastdataaboutmalaria,identificationofmosquitospecies,andabiggerroleofsocialmediaincommunicationregardingmalariaasfuturerolesofmobilephones.Furthermore,actorsperceivethesituationregardingmalariainRuhuhaasaproblemathighlevel,exceedinglimitscomparedtothepast,exceedinglimitscomparedtootherregionsinRwanda,andactorsexpressedthatmalariaincreasesduringcertainmonths.Moreover,regardingknowledge,myresultsshowthataccordingtotheperceptionofactorsthereareanumberofmisconceptionsaboutmalariainRuhuha.Thesemisconceptionsincludebewitcheryandpoisonousactivities,eatingmaizesticks,eatingsugarcanes,drizzleandnewlyharvestedbeans,medicinesatthehealthcenterdonotcuremalaria,andunbalanceddietorfoodthatisnotwellprepared.Inaddition,regardingtrustthecommunityhealthworkersandthenursesorstaffatthehealthcenteraremosttrustedwhenitcomestospreadingreliableinformationaboutmalaria.Traditionalhealers,illiteratepersons,neighbors,privatepharmacies,andFacebookaretheleasttrustedwhenitcomestospreadingorreceivingreliableinformationregardingmalaria.Lastly,perceptionsofproblemsregardingmalariapreventionandcontrolthatwerementionedbydifferentactorsarerelatedtofumigation,tablets,bednets,bedbugs,removingplantationsaroundthehouse,beliefinbewitchery,notusingpreventivemeasuresproperly,poverty,waterscarcity,andtimelyresponseandlackof(financial)resources.

75
5.4MalariagovernancearrangementsIntheprevioussectionsIanalyzedtheinformationandcommunication
flowsbetweenactors,theroleofICTsinhealthsysteminRuhuharegardingmalaria,andwiderangeofactors’perceptionsregardingthefutureroleofmobilephones,thesituationregardingmalaria,knowledgeandmisconceptions.IidentifiedthatinformationregardingmalariainRuhuhaissharedviaface-to-facecommunication,SIScomandHMIS,mobilephones,radio,andvideoprojections.MyfindingshaverevealedthatapartfromthestrategicICTbasedhealthinterventionssuchasHMIS,mobilephonesalreadyplayacrucialroleinmalariaprevention,inparticularbyfacilitatingawarenessraisingandbyimprovinginformationflowswithinandbetweenstakeholdergroups.Contrarily,ICTscouldalsofacilitatethespreadofmisconceptions,asactorsfromalllevelsmentionedthatmisconceptionsaboutmalariastillexistinRuhuha.Myanalysispointedtotheroleoftrustinhowdifferentactorsassignlegitimacytotheinformationtheyreceiveaboutmalaria.Thisanalysisshowedthatcommunitymemberstrustinformationfromstakeholderswhohavestudiedhealthandwhoareliterate,opposedtoinformationfromactorswhoareuntrained,illiterate,orwhodonotexaminepatientsorprescribemedicines.Inaddition,therearenostrikinglydifferentviewsontheidentifiedproblemsregardingmalaria.However,differentproblemsdescribedbycommunitylevelactorsrelatedtotheapplicationofpreventionmeasuresaresomehowlinkedtoeachother.Thenationallevelisnotawareoftheseproblemsregardingthepreventivemeasuresdescribedbythecommunitylevelactors,thereforethereisalackofcommunication.
ThissectionanalyzesthemalariagovernancearrangementsandtheroleofICTsinestablishingandarrangingthem.Myinterviewsrevealedasetofrulesandregulationspertainingtomalariapreventionandcontrol.Theserulesandregulationsaremainlysharedbetweenhealthandnon-healthrelatedactorsonthecommunitylevel,howeverthedistrictandnationallevelaretosomeextentinvolvedintherulesaswell.Thisisespeciallyimportantfromthepointofviewofmytheoreticalframing:inherworkElinorOstrompointedtothefactthatdevelopingrulesandapplyingsanctionstorule-breakersisthefirststepineffectiveself-governanceofcommunities.Accordingly,IstartwithpresentinganoverviewofallthemalariapreventionrulesandregulationsobservedinRuhuha,includingthestakeholdersinvolvedintheircompliancemonitoringandthewaysinwhichtherulesareenforced.ThisisfollowedbyadiscussionofmalariaasapublicbadandcollectiveactioninRuhuha.Finally,Ilookatthedifferentlevelsofcompliancewiththerules,followingOstrom’sdesignprinciplesoneffectivegovernance,payingparticularattentiontotheroleofcommunication/ICTs.
5.4.1Preventionandcontrolmeasures
5.4.1.1RulesandregulationsThefollowingtable(table26)showstherulesandregulationsthatare
identifiedfromtheinterviews.TheserulesandregulationsarethepreventionandcontrolmeasuresthatareusedtofightagainstmalariainRuhuha.

76
Table26:RulesandregulationsregardingmalariapreventionandcontrolinRuhuhaRuleorregulation ActorresponsibleTocutdowntreesandbushesaroundthehousewheremalariamosquitosmaylive.
Communitymembersandcommunityhealthworkers
Toremovestagnantwateraroundthehouse. Communitymembersandcommunityhealthworkers
Toreachhealthcenterontimewheneverapersonisshowingsomesignsofmalaria.
Communitymembersandcommunityhealthworkers
Indoorresidualspraying,alsoknownasfumigation. RwandaBiomedicalCenterUsinginsecticides,productsthatarespecializedatkillingsomeinsectsinthehouse.
Communitymembers
Tosleepinmosquitonetsandwheneveramosquitonetisexpiredornotfunctioningwellcommunitymembersareadvisedtoreporttogetanewone.
Communitymembers,communityhealthworkers,andRwandaBiomedicalCenter
Toclosewindowsanddoorsduringtheeveningandnight.Thecommunityhealthworkersalsotoldcommunitymemberstonotspendtheeveningornightoutdoors.
Communitymembersandcommunityhealthworkers
Tonothavebanana,sorghum,ormaizeplantationnearhomes,asthisisthelocationwherefemalemosquitosmayhidethemselves.
Communitymembersandcommunityhealthworkers
Tohavecleanlinessaroundandinhomes.Tobesmart,tohavecleanlinesswhilepreparingfood,cleanbodyandwashedclothes,andtoremovedirtandrubbisharoundtheplace.
Communitymembersandcommunityhealthworkers
Fumigationofswampsofricecooperatives. RicecooperativesResearchersusedtrapsandusedtofumigateswampsasinterventionsofaresearchprojectofthemalariaeliminationprogram.Howeverthoseinterventionsarenolongertakingplace.
ResearchersoftheMalariaEliminationProgram
Thelocalleadermentionedanelectronicdevicethatispluggedsomewhereduringthenightandthiselectronicdeviceplaysaroleinfightingagainstmosquitos.Heexplainedthatthiselectronicdevicefunctionsasamosquitonet.However,nootheractormentionedit.
Communitymembers
Tobuyandprovidehealthinsurances. Communitymembers,NationalHealthInsuranceScheme
Fromtable26canbeidentifiedwhichactorsareresponsibleforwhich
ruleorregulation.Thecommunitymembersarementionedtohavearesponsibilityforallrulesexceptforfumigation.TheRwandaBiomedicalCenterisresponsibletomakesurethatfumigationandmosquitonetsareavailable.Furthermore,fromthetablecanbeseenthatthecommunityhealthworkersalsohavealargeresponsibilityinmakingsurethattherulesandregulationsarefollowed.Moreover,theNationalHealthInsuranceSchemehasaresponsibilitybyprovidinghealthinsurances.Thefollowingsub-sectiondescribestherolesofactorsinensuringthatthemalariapreventionandcontrolmeasuresareinplaceinmoredetail.
5.4.1.2Whoensuresthesepreventionandcontrolmeasuresareinplace?Table26intheprevioussub-sectionshowsthemalariapreventionand
controlmeasuresandwhichactorisresponsibletomakesuretheserulesandregulationsarefollowed.Thissub-sectiondescribesinmoredetailhowthedifferentactorsrelatetotherulesandregulations.

77
CommunitymembersTherulesandregulationsandpreventionmeasuresthatthecommunity
membershavetoperformthemselvesaccordingtotherulesandregulationsare:tocutdowntreesandbushesaroundthehousewheremalariamaylive,toremovestagnantwateraroundthehouse,toreachthehealthcenterontimewheneverapersonisshowingsomesignsofmalaria,tosleepinmosquitonetswhentheyareavailable,toclosewindowsanddoorsduringtheeveningandnight,tonothavebanana,sorghum,ormaizeplantationneartheirhomes,tohavecleanlinessaroundandintheirhomes,andtobuyhealthinsurance.
CommunityhealthworkersThecommunityhealthworkersareinchargeofcheckingwhetherthe
rulesandregulationstopreventagainstmalariaarefollowedbythecommunitymembers.Thecommunityhealthworkersvisithomestocheckifpeoplefollowtherulesandregulations,forexampleiftheyhaveproperhygienicconditionsaroundandintheirhomes.Thecommunityhealthworkersareinchargeofhelpingpeopleinlocalareas.Theycarryoutrapidtestsformalariatoreferpeopletothehealthcenterassoonaspossiblebeforeacommunitymemberbecomesaseveresufferer.Inaddition,thecommunityhealthworkersareinchargeofadvisingthecommunitymembersaboutmalariaandofgivingtabletstothosewhosufferfrommalaria.Furthermore,thecommunityhealthworkersaretheretoinvestigateandgatherinformationwithinlocalareastochecklivelihoodconditions.Theyreportthisinformationtothehealthcenters.Forexample,theyvisithouseholdsandcountandlistallpeoplewhoareinneedofmosquitonets.Afterwardstheyreportthisinformationtothehealthcenter.Thehealthcenterthenreportsthisinformationtothedistricthospital.
HealthcenterThehealthcenterisinchargeofcollectingdatafromlocalareasthrough
communityhealthworkers.Thisdatareportedbythedifferentcommunityhealthworkers(suchastheamountofmosquitonetsneeded)isreportedbythehealthcentertothedistricthospital.Also,wheneverthehealthcenterseesthatthereisaproblemrelatedtomalaria,theyreportthistothedistricthospital.
Moreover,thehealthcentermakesreportsofmedicinesneededandsendsthemtothedistrictpharmacyatthedistricthospital.AfterwardsthehealthcenterpharmacyreceivesmedicinesfromtheMinistryofHealthdistributedthroughthedistricthospital.Afterreceivingthemedicines,thehealthcenterisinchargeofgivingthesemedicinestothecommunityhealthworkers.Thehealthcenterisalsoinchargeofreportingtothedistrictwhenapersonreportshimorherselfatthehealthcenterfourtimesamonth.
DistricthospitalThedistricthospitalworkscloselytogetherwithadministrativeandlocal
leaders,communityhealthworkersandhealthcenterstoensurethatthepracticesregardingmalariapreventionandcontrolareinplace.ThedistricthospitalalsoworkscloselywiththeMinistryofHealthsuchastheRBCdivision.
Thedistricthospitalgathersinformationthatisreportedfromthehealthcentersatlocallevels.TheythenanalyzethisinformationandalsoreporttheinformationtotheMinistryofHealth.AfterwardsatthenationallevelsuchasatRBCtheydecidethematerialstobegivenandtobedistributed.Therefore,as

78
healthprofessionalsthedistricthospitalisthelinkbetweenthecommunitylevelandthenationallevel.Theyhavemoreknowledgeaboutmalariathanthelocalauthoritiesandareinbetweentoworkcloselytogether.Furthermore,thedistricthospitalandthedistrictofficeareinchargeoftrainingnursesatthehealthcenteraboutmalaria.Inaddition,whenevermalariaissevere,communityhealthworkersandleadersfromdifferentlevelsarecalledtothedistrictofficetoattendameetingaboutmalaria.Therefore,thedistrictofficeandhospitalareinchargeoftrainingtherulesandregulationsandpreventionandcontrolmeasuresagainstmalariatoleadersfromsectors,communityhealthworkers,andvillagecommittees.Moreover,thedistrictpharmacyatthedistricthospitalhasthemandatetodistributedrugstosectors.Therearealsoprivatehealthspotsthatrequiredrugsfromthedistrictpharmacy.Lastly,thedistrictaskedthehealthcenterstoreportanycasewherebyapersonreportstothehealthcenterrepeatedly.Inthesecasesthedistricthospitalanalyzeswhethertherearenewspeciesofmalaria.
MinistryofHealth/RwandaBiomedicalCenterTheMinistryofHealthcreatesadvocacytothegovernmenttogetsupport
tofightmalaria.Thegovernmentisinchargeofspreadinginformationtoactorsondifferentlevelsandtomakethemhaveaccesstomaterialstofightagainstmalaria.TheMinistryofHealthadvocatesforsuchresourcestothegovernment.AdvocacyiscarriedoutbytheMinistryofHealthtothegovernmentwheneverthereisaspecialsicknessoralargeamountofpatientssufferingfromacertaindisease.Inthisprocess,forexampleregardingmalariapreventionandcontrol,theMinistryofHealthisresponsibletogivesupportbyprovidingfumigation,bednetsandmedicines.ThedifferentresponsibilitiesoftheMinistryofHealthandRBCregardingmalariapreventionandcontrolarenowexplainedinmoredetail.Firstofall,theRBCdepartmentoftheMinistryofHealthisinchargeofdistributingmosquitonetstothehealthcenters.Beforegivingthesemosquitonetstothehealthcenters,thecommunityhealthworkerscountpeoplewhoareinneedofmosquitonetsindifferentcommunalregions.Aftercollectingthisdatafromlocalareas,thehealthcenterreportsthecommunitymemberswhoneedmosquitonetstothegovernmentatnationallevel.Afterwardsthegovernmentsendsthesemosquitonets.AcommunityhealthworkermentionedthatRwandahasnocapacityofproducingbednetsandthenetsarefromabroad.AfterreceivingthenetsfromabroadtheMinistryofHealthisinchargeofdistributingthenetsinRwanda.RBCmentionedthatthemajorpartnersforbednetsareGlobalfundandUSAIDPMI(President’sMalariaInitiatives).RBCexplainedthatstartingfromthisyear2018,thedistributionofbednetswillnotonlybedonebythegovernmentbutalsobytheprivatesectorthroughSocietyforFamilyPlanning(SFH).Inaddition,fumigationisalsoanactivitythatiscarriedoutbytheMinistryofHealth.TheycurrentlyhavethreepartnersinsprayingwhichareGlobalFund,PMIandthegovernment.Furthermore,theMinistryofHealthwritesbooksthatareusedtofacilitatenursesaroundthecountrytoperformtheirprofessioncorrectly.TheMinistryofHealthisalsoinchargeofdistributingmedicinestodistricthospitals.Fromthedistricthospitalthemedicinesaredistributedtohealthcenters.ThegovernmentofRwandabuysthemedicinesfromwholesalersabroadsuchaswholesalersintheUnitedKingdom.Afterreceivingthesemedicinestheyaresuppliedthroughthepublicnetworkin

79
Rwanda.PrivatepharmaciesinRwandacanalsobuymedicinesfromthesamewholesalerintheUnitedKingdom.Theysellthesameproductswithaprofitmarginandwithoutsubsidy.TheMinistryofHealthisincontactwiththeprivatepharmacistsastheysetregulationstobefollowedbyprivatepharmacies.Firstofall,theycheckwhetherprivatepharmaciesareequippedandeducated.Secondly,theMinistryofHealthlicensesprivatepharmacies.Theygiveoutcertificatestoprivatepharmaciststobeallowedtoengageintheactivityofsellingmedicines.Inaddition,theMinistryofHealthvisittheprivatepharmaciestocheckifthemedicationsthataresoldareonthelistofmedicinesthatareallowedtobesoldtocommunitymembersinRwanda.
OtheractorsFirstofall,theactionscarriedoutbythecommunitymalariaactionteams
arecontrolledandorderedbythepersoninchargeofsocialaffairsatsectorlevel.
Furthermore,thefumigationofswampsofricecooperativesiscarriedoutbythecooperativethemselves.Itisdoneperiodicallywheneverpeoplearegoingtoplantrice.Therearemembersselectedwithinthecooperativetofumigatetheswampbeforeotherscomeforplanting.Thisisdonetopreventmembersofthecooperativefromgettingattackedbymalariawhenworkingintheswamp.
Moreover,theMalariaEliminationProgramhadaninterventionwheretheysprayedswamps,howeverthisinterventionended.
Inaddition,studentsarebeingtaughtaboutmalariainschools.Theteachersalsogivethemexercisesandhomeworktoteachotherpeopleaboutmalaria.
5.4.1.3Aretheyenforced?Duringtheinterviewsactorswereaskedwhetherthemalariaprevention
andcontrolmeasuresareenforcedinanyway.Themajorityofactorsrepliedthattheyarenotenforced,howevertwocommunitymembersmentionedthatthepreventionandcontrolmeasuresaresomehowenforced.
NotenforcedThemajorityofcommunitymembersmentionedthattherulesand
regulationstofightagainstmalariaarenotenforcedinanyway.Someexamplesaregivenintable27.
Table27:ExamplesthatthepreventionmeasuresarenotenforcedActor Supportingquotation(translatedbyresearchassistantduringinterviews)Communitymember
‘Itisnotforced.Theyadvicethem.Thenafterthinkingaboutmalaria,theyonlytaketheirdecision.Theytaketheirdecisionofremovingthoseoftakingofusingthosemeasuresoffightingagainstmalaria.Itisnotforced’.
Communitymember
‘Itisnotenforced.Itisnotenforcedtogetthosemeasuresofpreventingagainstmalaria.But,mostofthepeoplebecauseofthinkingthathavingthosematerialsofhavingthosemeasuresoffightingagainstmalariaisveryimportant,mostofthepeopleneedmosquitonetsandtheyareusuallytalkingaboutmosquitonets,howdowegetmosquitonets.AndmostofthemneedmosquitonetsmostofthetimeandtheysayandIthinkhasitbeenexplained?’.
Communitymember
‘Thecommunityhealthworkersvisitthepeoplemostofthetime.Visiting,suchvisitisnotcarriedoutbyforce.Itisnotcarriedoutforcibly,itiscarriedoutwillingly.Andanytimeacommunityhealthworkerreachesthehouse,thepeoplefromsuchhousewelcomehimorher.Thentheygiveherorhimaservicethatheneedsorsheneeds.

80
Thenacommunityhealthworkermaycomeintothehouseandcheckwhetherthereisabednet.Andwheneversheseesthatorheseesthatthereisnobednet.Heorsheadvisesthepeoplehowthewayofpreventingagainstmalariaandthewaytheymaypassthroughastogetbednets’.
Memberofcooperative
‘Asthepeoplehavebeeninformed,trained,taughtaboutmalaria.Thisactionthisactivity,thismeasuresoffightingagainstmalariaarenotdoneonforce.Peoplearewellinformed,arewelltrained,arewelltaughtaboutthisepidemic,malaria.Theythinkwheneverthereisanactionofmosquitonets.Hehasgivenanexample.Peoplestartsharing,startbeinghappy.Arethosemosquitonetscoming,letusgoforthem,letusgoandtakethem.Mosquitosarenowmakingusdieandarenowcausingusdifferentproblems,soletusgoandtakethem.Theyarehappy,theyarehappy.Theyarenotforcedatgettingmosquitonetsorbeinggiventhesemeasuresoffightingagainstmalaria.Theythinkthisistheirownaction.Tostayinmosquitonetsandtogetthemwhenevertheyareaccessible’.
Healthcenterstaff
‘Itisnotforced.Thepeoplearewillinglywishingthosemosquitonetsmostofthetime.Whenevernursepassesaroundtheroad,passesthroughtheroad.Andmeetingthosepeople.Thosepeopleareinquiringandaskinghimorheraren’ttheresomemosquitonets?Aren’ttheresomemosquitonets?Itismeansthatthepeoplereallyknowtheimportanceofmosquitonets.Andtheyreallyknowthatpossessingorhavingthosemosquitonetsisimportanttothem.Soitmeanstheyarenotforcedsoastogetthosemeasuresoffightingagainstmalaria’.
Headofthehealthcenter
‘Thereisnoforcewithinthesewaysofpreventingagainstmalaria.Thereisnoforce.Peoplearewillingtousethosemosquitonets.Andsheisnowsayingthattheyarenowadaysmakingcensustheyarenowcountingbedswithindifferentlocalareas.Andpeoplearenowwaitingandsomeofthemarenowcomingwhenwillthosemosquitonetscome.Itmeansthattheyarewaitingeagerlythosemosquitonets.Theywanttogetthem.Becausetheyhavespendalongtimesufferingfromthiskindofillness.Theyarewaitingeagerlyandcheerfullythesemosquitonets.Itmeansthatthereisnoforceinthiswayofcontrollingthesewaysofpreventingagainstmalaria’.
Communityhealthworker
‘Noitisnotforced.Asthesecommunityhealthworkersaretogetherwiththesepeopledaytoday.Shehasgivenanexamplewherebytheygivethemmedicalmentsofdifferentelements,differentsicknesses.ShehasgivenanexampleofmedicalmentsofImonia,diarrheaandsoon.Thisfamiliarityforbeingtogetherwiththemdaytoday,thisfamiliarityhelpsthosepeopleandcommunityhealthworkersbecomefriends.Andthepeoplelovethosecommunityhealthworkersbecausetheyreallyknowthatthehealthcommunityworkersaretogetherwiththem,arealwaystogetherwiththem’.
Thequotationsinthetableaboveshowthattheseactorsfeelthatthe
rulesandregulationstofightagainstmalariainRuhuhaarenotforced.Thecommunitymembersexpressedthattherulesandregulationssuchasbednetsareimportanttothem,butnotenforceduponthem.Aswasanalyzedearlier,communityhealthworkersaretrustedbycommunitymembers.Moreover,theyalsohavealargeroleincompliancemonitoring.Thequotationofthecommunityhealthworkerinthetableabovealsoexplainedthatcommunitymembersdonotexperiencethattherulesandregulationsareenforcedbecausetheytrustthecommunityhealthworkersandbecausetheyarepartofthecommunity.
EnforcedAlthoughallotheractorsmentionedthatthepreventionandcontrol
measuresarenotenforced,therearetwocommunitymemberswhomentionedthatthemeasuresaresomehowenforcedinsomesituations.Duringtheinterviewwithoneofthemtheresearchassistanttranslated:
’Inadditiontothat,likewithinneighborhood,becauseinthecommunityhealthworkerstheyhavethisvisit.Iftheyget

81
informationthataparticularhouseholdisnotusingthebednets,theygotheyvisittheysearchforinformationwhetherthehusbandandthewifecannotbeathome.Probablyintheplanation.Butwhenthekidistherethecommunityhealthworkercancome.Youknowmostthetimewiththekidheorshecandiscloseallinformation.Sothecommunityhealthworkercanaskthekid.Doyoueverseeyourparentssleepunderbednets,thekidsaysnoIhaveneverseen.Canyoucomeandseewherethebednetsprobablystoredsomewhere.Inthatcircumstancethecommunityhealthworkergetsinformationandthenheorshecandiscloseinthevillagethatok,certainhouseholddoesn'tusebednets.Sowithintheneighborhoodnowtheystartcriticismwhyareyounotsleepingunderbednets,canyouatleastifyoudon'tusejustgiveittootherswhoarewillinglytouseit.Sowithsuchacriticismofcoursepeoplearestartingtochangetheperceptionthentheycanuseit’.
Thisexampleshowsthatinsomesituations,whenthecommunityhealthworkersfindoutthatcertainhouseholdsarenotusingapreventivemeasure,thecommunityhealthworkerscaninformthevillageorneighborhoodthattherearepeoplewhoarenotusingthem.Inthiswaytheymakecommunitymemberstalkaboutittochangeperceptionsandtoincreasepressureonthesehouseholdstousethepreventivemeasures.Furthermore,thiscommunitymemberalsomentionedthatthecommunityhealthworkersaregoingtoensurethatthebednetsareusedproperlyinthefuturebyforce.Thetranslatorstatedthathealsoexplained:
‘Soheissayingthatnowhethinksthathecancontinuemobilizingforthosewhostillhavemisconceptionaboutmalariaaboutcleaningthismosquitobreadingsite.Andthenwhoeverstillhaveabednetssothattheycansleepunderthem.Buttheyarealsowaitingthehealthcentertogivethemthebednetsbecausetheystillhavefeworeveninsomehouseholdtheydon’thaveany.Sothecommunityhealthworkerspromisedthatoncethenewbednetscometheywillmakesureeverybodyuseit.Thosewhowillnotuseittheywillnotonlylikejustcriticizetheminthemeetingsbutsureprovidelikephysicalconditionsforthemsothattheymakesuretheywillnotuseforotheralternativepurposeslikeconstructingthischickenorfishingorwhateversotheygrantedthattheywilldolikeacloserfollowupforthem.-Interviewer:Sothenitisenforced?-Translator:Yeah.Tomakesuretheyenforcesothattheyarereallyused’.
Thisquotationshowsthatthecommunityhealthworkersplayanimportantroleincompliancemonitoringandmakingsurethatcommunitymembersfollowtherulesandregulations.
Furthermore,anothercommunitymemberalsoexplainedthattherulesandregulationsaresometimesforced.Theresearchassistanttranslatedanexamplethathegaveaboutfumigation:
’Aspeopledonothavethesamelevelofunderstanding.Therearesomepeoplewhounderstandthemeasuresoffightingagainstmalariaeasily.Andthereareotherswhoaresomehowrigid.Whoaresomehowdifficultatunderstandingthewayoffightingagainstmalaria.Hehasgivenanexamplewherebythisfumigationactivity.

82
Thetimewhenitiscarriedout.Therearesomepeoplewhoclosetheirhouses.Andleavetheirhomessoastonotacceptthosepersonsfumigatingthehouses.Thenafterleavingtheplace.Afterquittingtheground.Thegovernmentmaynoticethatandanalyzeitandmayputthereforce.Whydon’tyouunderstandthiswhileitisimportantforyou,whywhat.Andasthetimegoesonthepeoplewhoareneglectingthisactivitythiseventsthatistakingplaceunderstandit.Ya.Butwhenthereapersonthepeopleareunderstandingthegovernmentstopsputtingthereforce.Itmeansthatpeoplewhoarenot,itmeansthatpeoplewhoneglecttotallythisactivityoffightingagainstmalariasometimesbutnotoftensometimesareforcedsoastounderstand’.
Thisexampleillustratesthatinsomesituationstherulesandregulationsaresomehowforceduponcommunitymembersbythegovernmentwhentheydonotfollowthem.Accordingtothiscommunitymemberthegovernmenttriestoputforcebymakingthesecommunitymembersunderstandtheimportanceofinthiscasefumigation.
Formyresearchthesefindingspointouttheimportantroleofcommunicationandtrustincompliancemonitoringoftherulesandregulations.Insection5.2wasidentifiedthatcommunitymemberscommunicatewithcommunityhealthworkersbothface-to-faceandviamobilephonesaboutmalaria.Communitymemberstrustthecommunityhealthworkersandthereforefollowtheiradvice.Furthermore,inthewaysinwhichrulesareenforcedcommunicationplaysanimportantroleaswelltomakecommunitymembersunderstandtheirimportance.
Communitymembersexpressedthatthesituationregardingmalariaexceedsitslimitandthatthepreventivemeasureslikebednetsareimportanttothem.Moreover,accordingtotheinformationillustratedintable27therulesandregulationsarenotforced,asthecommunitymembershaveahighwillingnesstofollowthem.However,inprevioussectionsmisconceptionsaboutmalariawereidentified.Inaddition,themajorityofactorsperceiveknowledgeaboutmalarianottobeenoughinRuhuha.Furthermore,communitymembersandhealthrelatedactorsfromalllevelsmentionedthatpreventivemeasuresarenotusedproperly.Anumberoftherulesandregulationssuchasclosingdoorsandwindowsduringtheevening,toreachthehealthcenterontimeandtohavecleanlinesscaneasilybefollowedbycommunitymembers.However,otherrulesandregulationssuchasbuyinghealthinsurance,removingtreesandplantationsaroundhomes,removingstagnantwaterandsleepinginbedswithmosquitonetsdependoncommunitymembers’financialsituation.Inaddition,mosquitonetsarenotavailableandthegovernmentdoesnothaveenoughfinancialresourcestofumigatehousesinRuhuha.Therefore,thecomplianceoftherulesandregulationsdonotonlydependonknowledgeandawareness,butalsoonotherfactorssuchasacommunitymembers’financialsituationorlackofresourcesandtimelyresponsefromhigherlevelactors.However,asearliersectionsinvestigatedpeople’sperceptionsaboutknowledge,beliefsandproblemsrelatedtomalariainRuhuha,itwasconcludedthatthemajorityofactorsperceiveknowledgenottobeenoughandthatmisconceptionsexist.Also,multiplestakeholdergroupsexpressedthatpreventivemeasuresarenotusedproperly.Evenifthousandsofmosquitonetsaredistributedtheywillnothelp

83
unlessallcommunitymembersusethemefficientlyandconsistently.Forthisreason,non-compliancetotherulesbringsoncollectiveactionproblems.Sincemalariaspreadsinareaswheretherearemanyhosts,onerule-breakerendangerstheentirecommunity.
5.4.2MalariaasapublicbadEarlierinthischaptertherulesandregulationregardingmalaria
preventionandcontrolinRuhuhawereidentified.Theprevioussectionarguedthatnon-compliancetotherulesandregulationsbringsoncollectiveactionproblems.Onerule-breakerendangerstheentirecommunity.Therefore,thereisacollectiveresponsibilityinthepreventionofapublicbad.Allcommunitymembershavetofollowtherulesandregulationstofightmalaria,asindividualsarecapturedinaninescapableprocessfromwhichtheycannotremovethemselves.Duringaninterviewwithoneofthestaffmembersofthehealthcentertheresearchassistanttranslated:
‘Somepeoplearecuredforalongtimeandtheydon’tcomebacksoastogetthosemedicaltreatmentfrommalaria.Andotherscan’tspendtwoweeks,oneweekwithoutbeingbacksoastobecuredhereathealthcenter.Soitmeansthatmalariahasexceeded.Andhehasalsogivenanexamplewherebynohousehold,whenmalariahascomeandhasenteredhousehold,itcan’tgoawaywithoutmovingaroundallpersonsinhousehold.Allpersons,oneiscuredtoday,theotheroneisgettingsufferingfrommalariatomorrow.Thepeoplereplaceeachotherwithinhouseholduntilallareattacked.Yathatishowmalariaisnowcirculating’.
Thisquotationshowsthatwhenonepersoninahouseholdisattackedbymalariatheothermembersofthehouseholdalsogetit.Acommunitymemberalsogaveanexamplefromwhichcanbeunderstoodthatmalariaisapublicbad.Duringthisinterviewtheresearchassistanttranslated:
‘Hehasalsoexplainedthatmalariaiscausedbyfemalemosquito,wherebysuchfemalemosquitoisresponsibleforstingingaperson.Thenafterstingingapersonsuchfemalemosquitomayalsogowithindifferentpersons,spreadingsuchmalaria.Thenthosepersonsmaybeattackedatthesametimebeingstingedbythisbeingstangbythisfemalemosquito’.
Theseexamplesshowthatthereissomesenseamongcommunitymembersthatgettingmalariaisaninescapableprocessfromwhichonepersoncannotremovehimorherself.Allindividualshavearoleinincreasingtheefficacyofthepreventivemeasuresandrulesandregulations.Fightingmalariaasapublicbadisheavilyreliantonthecapacityandwillingnessofthecommunitymemberstocomplywiththerulesandregulationsintheirdailychoicesandactivities.Therefore,thefirstpartwithinthissectionanalyzeshowdifferentactorswithinthemalaria-affectedareaofRuhuhacooperateandworktogethertoachieveasharedgoalofbattlingthedisease.ThesecondpartprovidesexamplesofcollectiveactionproblemsinthefightagainstmalariaasapublicbadinRuhuha.
5.4.2.1CollectiveactionForeffectivecollectiveaction,theactorshavetocooperateandwork
togethertoachieveasharedgoalofbattlingmalaria.Thissub-sectionprovidesexamplesofhowcollectiveactionisusedtofightmalariaasapublicbad.These

84
examplesincludecooperationbetweenactors,followingtherulesandregulations,tryingtobeanexampletoothercommunitymembers,andwillingnesstocontributetothecostsofBti.Theseexamplesareexplainedinmoredetailintheparagraphsbelow.
Cooperationbetweenactors Thereiscooperationbetweenactorstoachieveasharedgoalofbattlingmalaria.Table28presentsexamplesofactorsthatexplainedthatactorsworktogether.Table28:ExamplesofquotationsexplainingcooperationbetweenactorsActor Supportingquotation(translatedbyresearchassistantduringinterviews)CMAT ‘Alltheseteams.Communityhealthworkers.Thesecommunitymalariaactionteam
andalsohealthcenteranddifferentleaderswithinthesector,theyworktogether.Theyworkhandinhand.Andhehasmentionedthatwheneverthishealthcenterisanindicatorofmalaria.Itisanindicatorofmalariabecausethisistheplacewheretheleadersorotherpersonsmaycomeandnoticethatthereismalariathatisincreasing.Becausethisiswheremostofthepeoplesufferingfrommalariaareseen.Soitmeansthathealthcenterisanindicatorofmalaria.Andwhenevermalariahasbeenfoundhasbeenremarkedwithinthishealthcenter.Thishealthcentermaycallthosecommunityhealthworkerssoastoimpartthem.(…).Hereathealthcentertheworkersofthishealthcenterimpartthosecommunityhealthworkersthecurrentnewsaboutmalaria.Thenafterimpartingthemafterinformingthem.Thosecommunityhealthworkersalsogothereinthevillage.Andimmediatelytheyinformthesecommunityactionteamsworkers.Theyinformthem.Thenafterinformingthemthosethreepeoplewithincommunitymalariaactionteams.Theyalsoreachthepeople,immediately.Thentheyinformthepeoplethecurrentnews.Thisisthewayinwhich,thisistheprocessinwhichtheyworktogether’.
Communitymember
‘Butwhenyouobservelikeanymosquitobreedingsitewithinthevillage,notonlyforlikethecompoundorthehomeenvironment,youcancallthevillageleadersothattheycanorganizethecommunityworkthelastSaturdayofthemonth.Andthentheycancleantogetherforthevillage.Soheisleavinganexamplelikelastyearonmalariaday.ThatisinDecember,sotheygatheredtogetherinthewholecellandthentheywerejustcleaningthosemosquitobreedingsiteswherevertheywereinthewholecell’.
MEPR ’Andmostofthepeoplewereaccustomedtoburningthosemosquitonetsbysayingthosemosquitonetsarenowattractingbedbugs.Thenimmediatelytheycouldburnthosematerials.Andsisterstogetherwiththiscommunityofthishealthcentertheytrytomakepeopleunderstandwherethosebedbugscomefrom.Thenafterillustratingthesourceofthosebedbugstheyalsofacilitatethemtounderstandthatwhenthosebedbugsarenotavailable,theirmosquitonetswillnotbeburnedandthemosquitonestwillprotectthemfrombeingattackedbymalaria.Generally,theyadvicethosepeoplethewayofusingmosquitonetsandthewayofhavingtheseproperhygienicconditionsandtheyalsovisitpeople.Havinganambitionoftalkingtothosepeopleaboutmalaria’.
Communitymember
‘Thereisalsoacheckupofcommunityhealthworkerswherebythosepersonscheckwhetherallpeoplesleepinmosquitonets.Itmeansthatmostofthetimethosepersonsreachthegroundsoastocheckwhetherthepeopleareequippedandareimpartedaboutmalaria(…)InadditiontothatthelocalleadersandtheMinistryofHealthallhavestoodupsoastohelppeoplehaveknowledgeaboutmalaria.Andsoastohelppeoplepreventagainstmalariaasmalariahasbecomeaproblemintothecommunity(…)Thosepeoplewhoareinchargeoffumigatingthehouseadvisethehealthyadvisethehealthytofollowtherules.Andtheyalsoadvisethemtoreachclinicalcenterassoonastherearesomesignsthatthereissomethingnegativethatisgoingtooccur’.

85
Thequotationsinthetableaboveshowthatthemultiplestakeholdergroupsofdifferentlevelsworktogethertofightagainstmalaria.Wheneverthereisameetingthatgatherspeopletogethertheyhavetotalkaboutmalariaandgetinformedabouttherulesandregulationsregardingmalaria.Moreover,duringpublicworkthecommunitiescollectivelycleanmosquitobreedingsitesinthevillages.Furthermore,thewayhowthehealthsystemisorganizedwithcommunityhealthworkersalsoenhancesthewayactorsworktogether.Duringaninterviewwithacommunitymembertheresearchassistanttranslated:‘Andmalariahasdecreasedduetothefactthatthevillageadvisorsarethereandtheyarealsoimportantatgivingtreatments’.Inthiscasewithvillageadvisorsthetranslatormeantcommunityhealthworkers.Theresearcherofthemalariaeliminationprogramalsoexplainedtheimportanceofthecommunityhealthworkersbystating:
’Ithinkiftheyareorganized,becauseatacertainperiodpeoplestartedtothinkthatthereisnoprobleminRuhuha,notonlyinRuhuhabutinRwanda.Peoplestartedtoneglectusingmosquitobednet,cleaningaround,orclosingtheirwindowseverynight.Sopeoplestartedtothinkthereisnoproblemaboutmalaria.Thenitbecameagainseriousproblemforthem.Andsomepeoplediedofmalaria.Whentheystarttothinkmalariaisstilltherethentheyalsoresumedtheorganizationofthecommunity,whattheycando.SowhatIthinkisthatlocalleadersandhealthprofessionalshavetocontinueremindingthecommunitythattheyhavetoalwaystakecareoftheirhealthusingthosepreventivemeasures’.
Healsomentionedthatcommunityhealthworkersareveryeffectiveinthecommunitiesbysaying:
‘Becausepeoplerelyonthecommunityhealthworkers.Theyareveryeffectiveinthecommunity.Sowehavethelocalleadersbutinadditiontothoselocalleaderswehavethecommunityhealthworkerswhohavetrainingsonspecificdiseaseslikediarrhea,malaria,orotherdiseases.Sotheyaretrainedonthatsothatwhentheygivereliableinformationandpeoplealsostartedtorelyonthem,becauseoncetheycamebackfromthosetrainingstheystartedtotreatmalaria,soifyougivemedicinesagainstmalariaoragainstotherdiseasesandyourfamilymembersiscuredthenyoustarttothinkthatheistherightpersontorelyon’.
Furthermore,anothercommunitymemberalsogaveanexampleoftheimportanceofcommunityhealthworkers,becausetheyaretrustedbycommunitymembers.Duringthisinterviewtheresearchassistanttranslated:
‘Sowewerewonderingwhetherifacommunityhealthworkercanentereasilyintothehouses.Sotheysaidevenawomanafterlikeoneweekofpregnantsohecandisclosetheinformationtothecommunityhealthworker.Soaslongasthesearetheirfriends,thesearetheirneighborsintothevillages.Sotheyarereallytrustableinthevillagessotheycanthideanyinformation’.
TheexamplesshowthatthereiscooperationbetweenactorsinRuhuhatofightagainstmalariacollectively.Furthermore,theyshowthatcommunityhealthworkershaveacrucialroleinthis.

86
FollowingtherulesandregulationsAnotherexampleofcollectiveactioninfightingmalariainRuhuhaisfollowingtherulesandregulations.Severalactorsmentionedthatcommunitymemberscandosomethingaboutmalariathemselvesbyfollowingtherulesandregulations.Someoftheseexamplesareillustratedintable29.Table29:ExamplesofquotationsontheimportanceoffollowingtherulesandregulationsActor Supportingquotation(translatedbyresearchassistantduringinterviews)Privatepharmacy
‘Hethinksthatcommunitycandosomethingtopreventagainstmalariawherebyitfollowstherulesoffightingagainstmalaria.Hehasexplainedthatwheneverpeoplehavecleanliness.Thisproperhygienicconditionswithinthehousehold.Andusingmosquitonets.Throughthisway,followingtheregulationsandrulesthatareusedforfightingagainstmalaria,malariamaybeuprooted,maybe,maybemaybeputasside,maybecuredatagoodlevel’.
Headofthehealthcenter
‘Peoplemayplayagreatroleatfightingagainstmalariawherebytheyfollowtherules,theregulationsthataregotfromhereathealthcenters.Throughthiswayoffollowingrulesthepeoplemayintervene,mayplayagreatrolewithinremovingorputtingasidethiskindofelement,malaria’.
Communitymember
‘Theyfollowtheregulationsasthoseregulationshelpthemsurvive.Forexampleshehasgivenanexamplewherebyshehasexplainedthatwhenapersonisattackedbymalaria,immediatelyahouseholdhomeissufferingfrompovertybecausesheorhemayspendtwodaysinbedwithoutworking.Sotheythinkfollowingtheregulations,followingtherules,isveryimportanttothemasithelpsthemtosurvive’.
Communitymember
‘Theythinktheyshoulddosomethingaboutmalaria.Whatevercost,whateverway,whatevercostthatmaybespendastofightagainstuprootingmalariamaybedone.Andwhattheydonowadaysisfollowingtherules.Followingtherulesthattheyaregivenfromdifferentpersons,fromdifferentareas,fromdifferentcommunityhealthworkersfromhealthcentersandfromleaders.Whattheydoisfollowingtherulessoastofightagainstmalaria.Butwhatevercoststhatmaybespend,whattheythink,whatevercoststhatmaybespendsoastofightagainstmalariamaybedonesoastosavethemselves’.
Stakeholderssuchastheprivatepharmacyandtheheadofthehealth
centermentionedthattheythinkthecommunitycanuprootmalariawhentheyfollowtherulesandregulations.Furthermoreasillustratedinthetableabove,communitymembersalsoexpressedtheimportanceforthemtofollowtherulesandregulations.
TryingtobeanexampletoothercommunitymembersAnotherexampleofcollectiveactioninfightingagainstmalariainRuhuha
isthatcommunitymembersexplainedhowtheycanbeanexampletoothercommunitymemberstoalsofollowtherulesandregulations.Severalexamplesofquotationsinwhichcommunitymembersexplainthisaregivenintable30.Table30:ExamplesofquotationsabouttryingtobeanexampletoothercommunitymemberswhenitcomestofollowingtherulesandregulationsActor Supportingquotation(translatedbyresearchassistantduringinterviews)Communitymember
‘Buthimselfalsocandosomething,likebeingarolemodel.Ifyouwerecleaningyourhomeandthenyoudon’thaveanymalariacaseinayeartheycanalsoseehow,justobserveandcanshowalsoyourexample,okIhavespendawholeyearmyhomeiscleanwithouthavingamalariacase,whycantyoudothesame’.
Communitymember
’Apartfromherselfshemayhelpherneighborsbyadvisingthem,byimpartingthemdifferentmeasures,differentwaysthatareusedsoastofightagainstmalaria’.
Communitymember
‘Whathedoesso.Inhisopinionwhathemaydosoastofightagainstthisproblemmalaria.Isfollowingtheregulationasorganizedaspreparedthoseleadersandalso

87
helpingneighborswhodon’tunderstandtheroleoffollowingtherules,tounderstandtheroleofmosquitonets,becausetherearesomepeoplewhodon’tunderstandtheroleofmosquitonets.Andtheyconsidermosquitonets.Mostofthetimeheisattheleadingpositionleadingthosepeoplesoastounderstandit’.
Communitymember
‘Whattheymaycarryoutasthecommunitytofightagainstmalariaisremovingthisbadunderstanding.Misunderstandingisaproblemwithincommunity.Wheneverpeoplehaveunderstoodsomethingcollectivelytheywillpracticeit.Butwhenevertheymisunderstandittheywillperformsuchthingbadly.Itmeansthattheyneedtochangetheirunderstanding.Andalsoafterchangingsuchunderstandingtheywillfollowandusethoserulesregulationsthataretheresoastofightagainstmalaria.Throughthisoffollowingtherulesthatareusedtofightagainstmalariatheythinkthattherewillbesomethingimportantwhichtheymaycarryoutsoastofightagainstthisepidemic’.
Communitymember
’Whathethinksaboutthismisunderstandingofthepeopleandthiswayofnotgivingvaluethiswayoffightingagainstmalariatosomepeople.Hethinksthathehastoreach.Hastogotherenearbythem.Hastogoandapproachthosepeoplewhodon’tunderstanditwellandwhodon’tgivevaluetothiswayoffightingagainstmalaria.Andteachthemaboutthiswayoffightingagainstmalaria.Andalsoinadditiontothatthosepeoplearerequiredtoattenddifferentmeetingsthatarebeingdonewithindifferentlocalareas.Thenafterattendingthesemeetingshethinksthatthosepeoplewillgetinformationaboutmalariaandtheirunderstandingwillbechanged’.
Communitymember
‘AfterreceivingtheinformationfromWhatsApporFacebookshetriesimplementingtherulesandthewaysofpreventingit.Shehasgivenanexamplewherebyshemaymeetapersonsufferingfrommalaria.Andshegoestohishomeorherhomeandadvisetogotothehospitalintimesoastobecured.Andsheadditionallyaddedthatwheneversheseesapersonorneighborhavingsomestagnantwaterattheoutside,notcuttingthetrees,busheswhicharearoundthehouse,shemaygoandadvisehimtoadvisetheneighbortoremovetheunwantedbushessoastofightagainstmalaria’.
Asillustratedinthetableabovecommunitymembersexpressedthey
couldbeanexampletoothercommunitymemberstofollowtherulesandregulations.Someofthemmentionedthattheyhelpneighborstoremindthemtofollowtherulesandregulations.Inaddition,anothercommunitymemberexplainedthathethinksthathehastoexplaintherulesandregulationstofightagainstmalariatocommunitymemberswhoarenotawareofthemorwhoignorethem.Duringtheinterviewscommunitymemberswerealsoaskedwhattheydowiththeinformationthattheyreceiveaboutmalaria.Severalcommunitymembersansweredthattheyteachthisinformationtoothersinthecommunity.
WillingnesstocontributetothecostsofBtiAchallengeregardingthefightagainstmalariaasapublicbadinRuhuha
isthefactthatthereisalotofricefarminginRuhuha.Theresearcherofthemalariaeliminationprogramexplainedthisbysaying:
‘Ricefarminghaspositivebenefitsfromricefarming.Ricefarmersbenefitdirectlyfromtheirricefarmingactivities.Butatthesametimetheycreatenegativeimpactonothercommunitymembers,becausetheconditionswherericeiscultivateditsincleanandstagnantwaterwhichisafavorableenvironmentformosquitotoreproduce.Ononesidepositiveimpactforthericefarmersbutnegativeimpactfortheentirecommunity.Thenwehadtothinkabouthowfromtheseeconomicbenefitsfromthefarmers,ifasmallportioncanbeusedtomitigatetheriskcausedbytheiractivities.Thenwecarriedoutwillingnesstopaystudy.Thenattheendwe

88
foundthatthericefarmerswerewillingtocontributeupto25%ofthetotalcostsofBti.Thenafterthatweneedtoinvolvealsoothercommunitymembersandthegovernment.Thenweinvolvedriceconsumers.Soinvolvingthericeconsumersistoseeifriceconsumerswerewillingtopayanadditionalamountabovethecurrentpriceoftherice.SothattheadditionalamountcanbeusedtosupplyBti.Sowearebuildingamodelwherericefarmerscouldcontribute,riceconsumers,thenoncethereisagapthegovernmentcancontribute.Butitisbetterifthegovernmentcantopupinsteadofcomingandpay100%,thiscannotbesustainable.Butifthegovernmenttocontribute10%,15%thiscanbeunderstandable’.
ThisquotationillustratesanexampleofhowcollectiveactioncouldbeusedtofightmalariabycontributionsofricefarmersandriceconsumerstoBtitofumigateswamps.
5.4.2.2CollectiveactionproblemsIntheprevioussub-sectionexamplesweregivenonhowmalariaisfought
collectivelyinRuhuha.However,therearealsocollectiveactionproblemsinRuhuha.Asexplainedearliercollectiveactionproblemsoccurwhenforexamplethereisnon-compliancetotherulesandregulations.Whenoneindividualdoesnotfollowtherulesandregulations,thisisatreattotheentirecommunity.Thissub-sectionprovidesexamplesofcollectiveactionproblemsinbattlingmalariainRuhuha.Theseexamplesarethatfumigationandbednetsarenotavailable,thatmalariaknowsnoboundaries,thatsomecommunitymemberscannotfollowtherulesandregulationsbecauseofpoverty,andthattherearecommunitymemberswhodonotfollowtherulesandregulations.Alltheseexamplesarecollectiveactionproblemsandareexplainedintheparagraphsbelow.
Fumigationandbednetsnotavailable OneofthecollectiveactionproblemsisthatbednetsarenotavailableandthatactivitiesoffumigationarenottakingplaceinRuhuha.Forthesereasonscommunitymemberscannotcomplytotherulestosleepunderbednetsandhousesarenotfumigated.Actorsexplainedthatmalariacannotberemovedbycommunitymembersthemselvesifthesepreventivemeasuresarenotcarriedout.Forexample,duringaninterviewwithacommunitymembertheresearchassistanttranslated:
‘Ashehasmentionedabove,teachinginendlesswayinendlessprocess.Theyarerequiredtogoaheadtocontinueteachingthepeoplesoastobeawareofit.Andwhattheymaycarryoutsoastosupportthepeoplesoastopreventagainstmalariaisthattheyhavetobeawareofthis,Malariawillalwaysbetherewithinthecommunity.Whattheymaycutoutisthattheywillgoaheadinpartingthecommunitysoastoknowmoreaboutmalaria(…)Malariawillnotberemovedtotallytherewithinthecommunity.Unlesstheproblemsthattheyencountersuchastohaveprotectionagainstmalaria,unlessthoseproblemsareunavailable’.
Thisstatementshowsthatthiscommunitymemberthinksthatitisnotpossibletouprootmalariaunlessproblemsrelatedtomalariapreventionmeasuressuchastheavailabilityofbednetsandfumigationarenotthere.Thememberofthe

89
CMATalsoexplainedthatitisnotinthecapacityofcommunitymemberstouprootmalariacompletelywithouthelpfromsupportfromhigherleaders.Theresearchtranslatedthisexamplebysaying:
‘Thereissomethingthatcanbedonewithinthecommunitysoastoremovesoastopreventagainstmalaria.Wherebywheneverthosepeoplearefollowingtheregulationsproperly.Malariawillbediminishedatagreatlevel.Butitwillnotbeuprooted.Becausethereissomealsotherearesomealsosomethingsomethingsthatcanbedoneapartfromtheirmeans.Apartfromtheircapacity.Itmeansthattheymaydosomethingaboutmalariathemselvessoastoremoveit.But,itisnot,malariacannotbetotallyremoved.Interviewer:Whynot?Translator:Becausetheirmeans,theirmeansareallowingthemremovepartofmalaria.Butnotwholepart.Yaitmeansthattheremustbealsosomeotherpeople.Someotherleaders,somesupportfromoutsidewhichwillhelpthemsoastoremoveittotally’.
Thisquotationalsoillustratesthatcommunitymemberscanfollowtherulesandregulations,butthatthisalonewillnotuprootmalariacompletely.Accordingtotheseactorsoutsideassistancefromforexamplehigherlevelsareneededtouprootmalariacompletely,suchasassistancebyhigherlevelstoprovidemosquitonetsandfumigation.Moreover,theheadofthemalariadepartmentofRBCalsomentionedthatmalariaeliminationisnoteasyandstated:
‘Beforewehadagoalforelimination.Upto2017.Nowwiththenewstrategicplanfrom2013upto2020wechangethegoalformalariacontrol.Welikenowtoreducemalariaburdenthanelimination.Becausewefoundthateliminationisnoteasy.Weneedtostrengthenourcapacityandalsotogomobilizemoreresourcesfromhealthsectorsandnon-healthsectors.Becausewefoundisnoteasywork’.
ThisquotationexplainsthatforthenationallevelitisdifficulttomobilizemosquitonetsandfundstofumigateallhighburdenareasinRwanda.Therefore,theychangedtheirobjectivefrommalariaeliminationtoreducingthemalariaburden.Thisexplainswhybednetsandfumigationarenotavailableatthecommunitylevel.Duringaninterviewwithanothercommunitymembertheresearchassistanttranslated:
‘Theyhavetriedalltheirbestsoastofightagainstmalaria.Soastopreventthismalaria.Theyhavefollowedallregulationswhichhavebeenregulated,whichhavebeenorganizedbythegovernmentbythenursestellingthepeopleaboutmalariaprevention.Andwhattheyhavedoneisenoughbuttheproblemthattheyarenowadaysencounteringthattheydonothaveenoughmosquitonets’.
Thiscommunitymemberalsoexplainsthatthecommunitymembersfollowtherulesandregulationsbutthattheproblemthattheyarenowadaysfacingisthatmosquitonetsarenotavailable.Thisisacollectiveactionproblem,becausefumigationandbednetsaretwoveryimportantpreventivemeasurestofightagainstmalaria.

90
Malariaknowsnoboundaries Anothercollectiveactionproblemisthatmalariaknowsnoboundaries.Duringtheinterviewwiththemalariaeliminationprogramtheresearchassistanttranslated:
‘Shethinksthatwheneverpeoplefollowtheseregulationsasorganizedshethinksthatmalariawillbediminishedbutitwillnottotallybeended.Becausesheisnowgivingexamplesbysayingthatmosquitosareelsewherearewithindifferentareas,arethroughoutdifferentareas,sothesemosquitoscannotberemovedwithinallareas.Peoplehavenocapacityofremovingallmosquitosaroundallareas’.
ThisexampleshowsthatpeopleinRuhuhamayfollowtherulesandregulations,butmosquitosarealsoinneighboringareas.Thisisacollectiveactionproblem,becausecommunitymembershavenocapacitytoinfluencemalariapreventionandcontrolinneighboringcommunitiesandcountries.
SomecommunitymemberscannotfollowtherulesbecauseofpovertyPovertyisanothercollectiveactionproblem.Becauseofpovertysome
communitymembersarenotabletocomplytotherulesandregulationsofbuyinginsurancecards.Moreover,communitymembersmightnotsleepinbedsbutontheground,whichmakesitdifficulttousemosquitonets.Inaddition,therearecommunitymemberswhowonderwhethertheyshouldfollowtherulesandregulationsregardingtheremovalofplantationsaroundhouses.Theseplantationsareimportantforcommunitymembers.Acommunitymembergaveanexampleofthisandthetranslatorstated:‘Theyaskthemselveswillwecutdownthosebananaplantationswhiletheyareimportantforus.Whatwillwedo’.Anothercommunitymemberalsowonderedwhytheyneedtoremovetheplantationswhiletheyareimportanttothem.Duringthisinterviewtheresearchassistanttranslated:
‘Theproblemisbecausemostofpeopleinthevillageorinacelltheyattendmeetingswherethesecommunityhealthworkerssharethemalariapreventionandcontrolmeasures,orevenmalariarapidinformation.Butthemainproblemisputtingintopracticethisinformationshared.Heisgivingmoreinformation,theexamples.Likethefirstwhere,rememberabovewetalkedaboutnotplantingthissorghumnearthehome.Butnowadayspeopleyoucanobserveevenhouseholdswhichhavesuchplantationbecausetheysay,okwhyaretheypreventingussuchforplantingsuchasorghum.Whycanttheyletusplantandthenworryaboutmosquitos’.
Thesequotationsshowthatcommunitymembersdonotalwaysfollowtherulesandregulations.Therearecommunitymemberswhochoosetohaveplantationsaroundtheirhomestoproducefoodinsteadofremovingthemtogetridofmosquitobreedingsitesaroundtheirhomes.Thisthreatensthehealthofothercommunitymembersinthecommunityastheseplantationsattractmosquitos.
Communitymemberswhodonotfollowtherulesandregulations Communitymemberswhodonotfollowtherulesandregulationsisanothercollectiveactionproblem.Asdescribedinearliersections,theremightbeseveralreasonsforcommunitymembersnottofollowtherulesandregulations,whichincludelackofknowledge,misconceptions,poverty,andthe

91
unavailabilityofmosquitonetsandfumigation.Intheprevioussub-sectiontheimportanceofcommunityhealthworkersinfightingagainstmalariaandinmakingpeoplefollowtherulesandregulationswasexplained.However,communitymembersalsomentionthatitisachallengethattheythemselvesmayfollowtherules,butneighborsmightnotfollowthem.Duringaninterviewwithacommunitymembertheresearchassistanttranslated:
’Butwhenitcomestotheprevention,Iwaswonderingwhetherthey,becausehesaidthathehaslikesixkids,canyouensureeverybodyinyourhouseholdsleepunderbednets.Sohesaidbeforehegoestosleephehastomakesurethateverybodyisunderbednets.Buttoensurewithinthewholecellissomehowdifficult.Becausefewpeoplemaynotsleepunderbednets.Butheisarguingthatcomparedtotheprevioustimeduetotheincreaseofmobilizationofcommunityhealthworkersatleasttheperceptionhasimproved’.
Thisexampleshowsthatthiscommunitymemberexplainsthathishouseholdcanfollowtherulesandregulations,butthathecannotensurethatallpeoplewithinhiscellsleepinmosquitonets.Anothercommunitymemberalsotalkedaboutneighborsnotfollowingtherulesandregulations.Duringthisinterviewtheresearchtranslatorstated:
’Sohestartedmentioningthathefeelsthattheyaredoingtheirbest.Intermsofputtingintopracticethisinformationbeingreceivedbythecommunityhealthworkers,especiallyusingbednetsandcleaningthehomeenvironment.Byaddingtothatwewerewondering,ifhishomeenvironmentisclean,buttheneighborshasbushesandwaterstagnantwateraround.Ofcoursethemosquitoswillflytohishouse.Sointhatcasehesaidsoforhimitisdifficulttoconvincetheneighbors.Butwhatisthebestishecancommunicatewiththecommunityhealthworkerssothatthecommunityhealthworkercangoandeducatethatneighborwiththosemosquitobreedingsites.Butweemphasizethatalthoughofcoursethecommunityhealthworker,ifnotthere,ofcourseasaneighborhecandosomething.Soheagreedatthattimeofcourseifaneighborisdoingsomethinggoodsootherscanalsotakealookandsay,oknow,atleastithasbeenoneyear,ourneighbordoesn’thaveanymalariacasebecauseofsleepingunderthebednetsorcleaningthehomeenvironment.Whynotus.Ifwehavelikeeachmonthwehaveamalariacasebecauseofthismosquitobreedingsitesaroundus,whycantwecleanthemandshowlikeanexampletoothers.Sohesaysthatoknowwecanalsoprayaroundtothosewhohavemosquitobreedingsitesaroundorprobablywhodon’tusethebednets’.
Thesequotationsshowthatcommunitymembersareawarethatitisacollectiveactionproblemwhenneighborsdonotfollowtherulesandregulations. RegardingtheroleofICTsincollectiveactionandincollectiveactionproblems,theroleofmobilephonesextendsbeyondtargetedinterventionsbecausetheycan(toapoint)facilitatecollectiveactionamongconcernedpopulations.Mobilephonesfacilitateincreasedadherencetotherulesandregulations.Whenrulebreakingoccurs,communicationviamobilephonesallowsformoreeffectivereportingofrule-breakers.Forexample,communitymembersmentionedthatwhentheyobservethataneighborisnotfollowinga

92
certainrule,heorshecallsacommunityhealthworkertoreportthissothatthecommunityhealthworkercancometoadvicetheneighbor.Anotherexamplethatwasgivenbycommunitymembersisthatwhenevertheyobservemosquitobreedingsiteswithinavillagetheycallthelocalleadertoschedulepublicworktocleanthem.Moreover,mobilephonesalsoenabledifferentactorsandstakeholdergroupstoeffectivelycommunicate,negotiateanddiscuss.Formyresearchtheseexamplesmeanthatimprovedcommunicationviamobilephonesfacilitatemoreeffectiveapplicationandmonitoringoftherulesandregulations.
5.4.3Ostrom’sdesignprinciplesTheprevioussub-sectionanalyzedhowcollectiveactionisusedin
Ruhuhatofightagainstmalariaasapublicbad,thecollectiveactionproblems,andtheroleofICTsincollectiveactionandcollectiveactionproblems.ThissectionanalyzesthecompliancewithOstrom’sdesignprinciplesofeffectivelypreventingapublicbad.Asexplainedin3.2Ostrom’sdesignprinciplesweredesignedtounderstandtheimportantconditionsoftheinstitutionalarrangementsthatattainedgoodoutcome,oppositetogroupswhoseeffortsfailed(Wilsonetal,2013).Ostrom(1993)describesthat:
‘’By‘designprinciple’ismeantacharacteristicthathelpstoaccountforthesuccessoftheseinstitutionsinsustainingthephysicalworksandgainingthecomplianceofgenerationsofuserstotherulesinuse’’.Section5.4.1.1identifiedtherulesandregulationsthataretheretofight
againstmalariaasapublicbadinRuhuha.Thedesignprinciplescanbeusedasapracticalguidetonearlyanygroupwhosemembersmustcooperateandworktogethertoachieveasharedgoal(Wilson,2013).Aswasexplainedinsection3.2,ICTscanfacilitateinthebuildingofcollectiveactionbyincreasingflowsofinformation,socialnetworking,participation,transparency,andinteractionsamongcommunitymembersthatfacilitatemaintainingtrust,acceptanceandalignmentnecessaryforsuccessfulcooperation(Thapaetal.,2012).Therefore,thissectionalsoanalyzeswhetherICTshaveaparticularroleinthecompliancewithOstrom’sdesignprinciples.
Thefollowinglistanalyzesthecomplianceofactorsfightingagainst
malariainRuhuhawithOstrom’sdesignprinciplesandtheroleofICTs.1) Clearlydefinedboundaries
Itisimpossibleforactorstodefineboundariesofthehealthsystemandtocloseitofftooutsidersortomosquito’sfromotherareas.WithinRwandamobilephonesandHMISplayaroletoreportincidentstothenationallevel.Thenationallevelusesthisinformationtomonitorwheremalariaincreasesanddecreases.AfteramalariaoutbreakisobservedthenationalanddistrictleveltogetherwithactorsonthecommunitylevelcaninitiateactionswithinRwandatoactupontheseobservationsthataremadeavailablebyICTs.However,RuhuhabordersLakeCyohohaandtheBurundianborderinthesouth.Ingabireetal.(2014)describe‘’LakeCyohohaisamajorcorridorforuncontrolledpopulationmovementsbetweenRwandaandBurundi’’.Therefore,boundariesarenotclearlydefined.TheactorsinvolvedinmalariapreventionandcontrolinRuhuhacannotenforcepeoplewholiveontheothersideofthelakeinBurundito

93
followtheirrulesandregulations,astheydealwithanotherhealthsystem.Forthisreasonthereisnocompliancewiththedesignprincipleclearlydefinedboundaries,astoclearlydefineboundariesthefightagainstmalariawouldneedaregionalapproachthatinthecaseofRwandaalsocoversborderingcountries.
2) ProportionalequivalencebetweenbenefitsandcostsOstrom(1993)states‘’Differentrulesareusedinself-organizingirrigationsystemstomobilizeresourcesforconstruction,formaintenance,andtopaywaterguards’’.Therearedifferentruleshowthehealthsystemisorganizedtomobilizeresourcesformalariapreventionandcontrol.Forexamplethereisthehealthinsurance,whicharepaidbycommunitymembersthemselves.However,afterpayingthelowersocialclassesgetmorereimbursedbythehealthinsurancecomparedtothehighersocialclasses.Furthermore,thegovernmentprovidesbednetsandsubsidizesmedicines.
Inaddition,wetlandsagricultureandricecultivationareacommonpracticeinRuhuha.Theseswampsattractmosquitos.Abenefitcostchallengethatthecommunityisfacingiswhethertheyshouldcontinuegoingintoswampsbecauseofthehighriskofgettingmalaria.Themalariaeliminationprogramdidresearchandfoundthatriceproducersarewillingtopayforthesprayingofswamps.Theyarewillingtopaybecausetheybenefitfromriceproduction,whilethewholecommunityhasabiggerriskofsufferingfrommalariaastheswampsattractmosquitos.Intheexamplesofthesebenefitcostchallengesmobilephonesplayaroletoremindcommunitymemberstopayforhealthinsurance.Moreover,startingthisyearcommunitymemberswillbeabletopayfortheirhealthinsuranceusingmobilemoney.
3) Collective-choicearrangementsOstrom(1993)states:
‘’Theproblemofgainingcompliancetorules,nomatterwhattheirorigin,isfrequentlyassumedawaybytheoristspositioningallknowingandallpowerfulexternalauthoritiesthatenforceagreements.Inthecaseofmanyself-organizingsystems,noexternalauthorityhassufficientpresencetoplayanyroleintheday-to-dayenforcementoftherulesinuse’’.
However,inthecaseofmyresearch,externalauthoritiesthatmakerules‘’thehigherlevel’’areabletoplayaroleintheday-to-dayenforcementoftherules.Theyareabletoinfluencethisbecauseofthewaythehealthsystemisorganizedwithcommunityhealthworkers.ThecommunityhealthworkersreportseverecasesofmalariaviaSMStextmessagestothenationallevel,copiedtothedistricthospitalandthehealthcenter.Furthermore,communityhealthworkersreportweeklytothehealthcenterhowmanypatientsofmalariatheytreated.ThehealthcenterusesHMIStoreportthesecasestothedistricthospital.ThedistricthospitalusesHMISaswelltoreporttothehigherlevel.ForthesereasonsthehigherlevelknowswhatisgoingonregardingmalariainRuhuha.Whentherearemanycasesofmalariatheyworktogetherwiththedistricthospitaltointerfereandtoensurethatthehealthcenter,localleadersand

94
thecommunityhealthworkersraisemoreawarenessabouttherulesandregulationsandthattheyfollowupmorecloselywhethertherulesandregulationsarebeingfollowed.Furthermore,thecommunitymembershavetemptationsnottocomplytherulesandregulations.Thesetemptationsincludehotnesswhilesleepinginbednets,violationofprivacywhenfumigatorsenterthehousewhenspraying,togrowplantationsaroundthehouseforincomeorownfoodconsumption,tosharetabletswhenotherfamilymembersalsosufferfrommalaria,andbedbugs.Wheneverthehealthcenteridentifiesthatcommunitymembersdonotcomplytotherulesforspecificreasonstheytrytogiveexplanationswhenpeoplearegatheredandordercommunityhealthworkerstomakecommunitymembersawareoftheimportanceoffollowingtherulesandregulations.
4) MonitoringOstrom(1993)describes‘’Monitors,whoactivelyauditphysicalconditionsandirrigatorbehavior,areaccountabletotheusersand/oraretheusersthemselves’’.Inthecaseofmyresearchthecommunityhealthworkersaremonitorsandusers.Theymonitorwhethercommunitymembersfollowtherulesandregulationsbyvisitingtheirhomestoassesswhethertheysleepinbednets,havehygienicconditionsinandaroundtheirhomes,andwhethertherearemosquitobreedingsitesorstagnantwateraroundthehouse.ICTsareusedintwowaysregardingmonitoring.Firstthecommunitymembersgaveexamplesthatwhentheyseethattheirneighborsdonotfollowtherulesandregulations(forexamplewhentheyhavestagnantwaterorbushesaroundthehouse)theyuseamobilephonetocallacommunityhealthworkerwhocancometoexplaintherulesandregulationstotheneighbor.Secondly,mobilephonesareusedtoreportseverecasesofmalariatothenationallevel.CommunityhealthworkerssendSMSmessagestothenationallevelincasetheymeetaseverecaseofmalaria.WithinthreedaysthecommunityhealthworkerreceivesaSMStextmessagefromthenationallevelaskingwhetherthemalariapatienthasimproved.
5) GraduatedsanctionsOstrom(1993)states:
‘’Userswhoviolateoperationalrulesarelikelytoreceivegraduatedsanctions(dependingontheseriousnessandcontextoftheoffense)fromotherusers,fromofficialsaccountabletotheseusers,orfromboth’’.
Violationstotherulescanbeprovenwhencommunitymembersforexampledonotallowfumigatorsintheirhomes,whentheydonotsleepinmosquitonets,orwhentherearebushesorstagnantwateraroundhouses.Thecommunityhealthworkers,whoareparticipantsandcommunitymembersthemselves,undertakemonitoring.Inthecaseofmyresearchtherearenoenforcedsanctions.However,thereissocialpressure.Communityhealthworkerscanvisithomeswhentheparentsareawaytotrytogetinformationfromchildren.Afterwards,ifthechildrensaytheydonotseetheirparentssleepinbednets,thecommunityhealthworkersmentioninthevillagemeetingsthatthereare

95
somepeoplewhoarenotusingthebednets.ICTsplayaroleinmonitoring,butdonotplayaroleinsanctioningcommunitymembersfornotfollowingtherulesandregulations.
6) ConflictresolutionmechanismsOstrom(1993)describes:
‘’Ifindividualswhomakeanhonestmistakeorfacepersonalproblemsthatpreventthemfromfollowingarulecannotfindmechanismstomakeuptheirlackofperformanceinanacceptableway,rulescanbeviewedasunfairandconformanceratesdecline’’.
InthecaseofmalariapreventionandcontrolinRuhuhathereareseveralexamplesofthis.
Firstofall,inthecaseofmalariapreventionandcontrolinRuhuha,theruleofsleepinginmosquitonetsisnotfollowedproperly.Manycommunitymemberssleeponmatsonthegroundanddonothavebeds.Thissituationmakesitdifficultforthemtousemosquitonetsproperlyanddeclinesconformanceratestothisrule.Moreover,atthemomenttheresponsibleactorsdonotprovidemosquitonets.Thislackofavailabilityalsodecreasesconformancerates.
Furthermore,becauseofpovertysomecommunitymemberscannotcomplywiththerules.Somehouseholdsdonothaveenoughmoneytobuyhealthinsurancesortablets.Thislackofmoneymightalsomakesomecommunitymemberssharetabletsathomewithotherfamilymemberswhosufferfrommalariaandtheydonotfinishtherequireddozetogetcured.
Inaddition,communitymembersexpressedthattheywerewonderingwhethertheyshouldreallyfollowtherulesofnotplantingbanana,sorghumormaizeplantationsneartheirhomeswhiletheyareimportantforthem.Theseplantationscouldgivethemincomeorfoodtoeat.Communitymemberscouldperceivethisruleasunfairanditwasmentionedthatnowadaystherearemanyhouseholdsthathaveplantationsaroundtheirhomes.ICTsdonotplayaroleinconflictresolutionmechanismsinthecaseofmyresearch.
7) MinimalrecognitionofrightstoorganizeTheactorsinRuhuhaaregivensomerightstoorganizebythegovernment.Forexample,thereisarulethatpeoplewhoshowsignsofmalariashouldreachthehealthcentertogettreated.However,therearealsoprivatepharmaciesthatarelicensedbythegovernmentwherecommunitymemberscanbuymedicineswithoutanyexaminations.Severalactorsmentionedthisasanegativedevelopment.However,thecommunitymembersandallactorsarerecognizedbythenationalgovernmentaslegitimateformoforganization.Nexttothepublicactors,alsothetraditionalhealersandprivatepharmaciesarelicensedbythegovernment.Itisdifficultforcommunitylevelactorstoenforcerulesasfundsforfumigationandbednetsareunavailableatthenationallevel.TheactorsthatareincludedinRuhuha’shealthsystemdohavetherighttoorganizebyauthoritiesfromhigherlevels,buttowhatextentisdifficulttodetermineasthegovernmentsomehowcontrolshowthe

96
healthsystemisorganizedthroughthepublichealthandnon-healthrelatedactorsatthecommunitylevel.ICTsdonotplayaroleintherecognitionofrightstoorganize.
8) NestedenterprisesOstrom(1993)states
‘’Irrigatorscantakeadvantageofmanydifferentscalesoforganization.Small-scaleworkteamsareaneffectivetechniqueforovercomingfreeriding.Everyonemonitorseveryoneelseinsituationswhereshirkingisobvious.Large-scaleenterprisesallowsystemstotakeadvantageofeconomiesofscalewheretheyarerelevantandtoaggregatecapitalforinvestment’’.
Thisisalsothecaseinmyresearch.Everyvillageorcellhastheirownsmallgroupsofcommunityhealthworkers,communitymalariaactionteams,localleaders,andpublicworkonasmallscale.Therearemeetingsonallthesesmalllevels,aswellasmeetingsondifferentlevelssuchasthedistrictbecausemalariaisaregionalproblem.Thereforethiscasealsohasscalesoforganizationfromvillage,cell,district,tothenationallevel.However,RwandaasacountrymightnotevenbebigenoughasascaleformalariapreventionandcontrolinRuhuha,becausetheborderwithBurundiisclose.ICTsplayaroleininformationandcommunicationflowsbetweenactorsondifferentscalesandbetweenactorsofthesamescale.
5.4.4TheroleofICTsinthemalariagovernancearrangementsTheprevioussub-sectiondescribedthatICTsplayaroleinfacilitating
communitylevelstrategiesof‘publicbad’governance.WhenanalyzingthecompliancewithOstrom’sdesignprinciplesitwasidentifiedthatmobilephonesplayaroleinthedesignprinciplescollectivechoicearrangements,monitoring,andnestedenterprises.ThissectiondescribedtheroleofICTsinthemalariagovernancearrangementsinmoredetail.
TheemergenceofICTsinRwandasomehowchangestheroleandlegitimacyofactorsinmalariapreventionandcontrolinRuhuha.Regardingmalariaasapublicbad,ICTsplayaroleineffectivelymanagingcollectiveaction.Firstofall,onthecommunitylevelcommunitymembersusemobilephonestocalllocalleaderstoinformthemaboutmosquitobreedingsitesinvillagesthatneedtobecleanedduringpublicwork.Anotherexampleisthatcommunitymembersusemobilephoneswhentheirneighborsdonotfollowtherulesandregulations.Inthesecasestheycallacommunityhealthworkertocomeandtoexplaintherulesandregulationstotheneighbor.Theadviceofcommunityhealthworkersismorelikelytobefollowedupcomparedtoifacommunitymemberwouldtrytoexplaintherulesandregulationstohisorherneighborbyhimorherself.Moreover,onthenationallevelICTsareenablingthenationalactorstogatherdataformonitoringandevaluation.TheyareusingtheICTsSIScom(CommunityHealthWorkerInformationSystem)andHMIS.Furthermore,ICTsenablequickinformationsharingacrosslevelsandbetweenthestakeholdergroups,whichenhancesquickactionincaseofanincreaseofmalariapatients.
IntermsofwhethernationalICTpoliciesandstrategiesarerelatedtolocaloutcomesinICTuseandmalariaprevention,thenationalICThealth

97
initiativesSIScomandHMISarefunctioningandareusedonthelocallevelandtoreportacrosslevels.Onthenationallevel,theRwandaBiomedicalCenterusesSIScom,rapidSMS,andHMISforreportingandmonitoringpurposes.However,accordingtotheRwandaBiomedicalCenterresponsetothedatagatheredisaproblem.Hestated:
‘Timelyreporting.Causeforthefirstweekofeachmonthwehavenewdata.Buttheissuesometimesisresponse.Ourissueisresponse.Weknowthatthereisaproblemthere.Butsometimesifyouwanttosprayitisabigproblemtofindoutmoney.Becauseforonelitter,uhmnoonedosage.Foronesquarepointthereisaroundcurrentlywithoutsubsidyisaround7.34USD.Butyoudon’tknow,tosprayonehouseisaroundprobably20euro.Ifyouwanttosprayonehousefor20eurosisveryexpensive,isveryexpensive.Butwearetargetinghighburdenareas’.
Thisquotationshowsthatforexampleknowledgeisavailableatthenationallevel.Theyareawarethatthehousesneedtobefumigated,buttherearenofinancialresourcestosupporttheserulesandregulationsregardingmalariapreventionandcontrol.TheRwandaBiomedicalCenteralsohasknowledgethatpreventionmeasuresarenotusedproperly.Recently,therehasbeenaresurgenceofmalariainRuhuha.Therefore,national(ICT/malariaprevention)policiesdidnotresultinalocaloutcomeofmalariaprevention,eliminationorreduction.However,ICTsarealsonotdeadpiecesofpaperthatareirrelevantforcesatthelocallevel.Althoughmalariaincidentshaveincreased,thenationalICThealthstrategiesandpolicieshavebeenimplementedandareusedatthelocallevel.ThecommunityhealthworkersreporttothehealthcenterusingSIScom.Furthermore,thehealthcenterandthedistricthospitalreportusingHMIS.TheseICTsspecificallydesignedforthehealthsystemplayaroletomakedataandknowledgeavailableformonitoringandevaluation,asRBCisawarethatthefollowuponthisdatatopreventmalariaatthecommunitylevelisanissue.

98
6.ConclusionThehealthsystemregardingmalariapreventionandcontrolinRuhuha
consistsofhealthandnon-healthrelatedactorsfromthecommunity,district,andnationallevel.Informationandcommunicationflowsbetweenthesedifferentstakeholdergroupsarefacilitatedbyface-to-facecommunication,SIScom,HMIS,mobilephones,radio,andvideoprojections.Firstofall,SIScomandHMISareinitiativesspecificallydesignedforthehealthsystemandfacilitatethesharingofinformationfromcommunitytothenationallevelformonitoringandevaluationpurposes.Secondly,face-to-facecommunicationandmobilephonesfacilitateinformationandcommunicationflowswithinandbetweenallstakeholdergroups.Lastly,radioandvideoprojectsfacilitateinformationflowsfromthenationaltocommunitylevel.
MalariaisconsideredagrowingprobleminRuhuhaandawarenessishigh.However,themajorityofactorsperceiveknowledgeaboutmalarianotenoughinRuhuha,whileotheractorsexplainedthatknowledgeisenoughbutthepreventivemeasuresarenotappliedproperly.Intheanalysishasbeenidentifiedthatreasonsfornotapplyingthepreventivemeasuresarerelatedtopoverty,misconceptions,andthelackofmosquitonets.Ifacommunitymemberdoesnotapplythepreventivemeasuresproperly,heorsheisarule-breakerandthisendangerstheentirecommunity.Forthisreason,non-compliancetotherulesandregulationsthatareinplacetofightmalariaarecollectiveactionproblems.AccordingtotheanalysisofcompliancewithOstrom’sdesignprinciples,thesecollectiveactionproblemsincludenoclearlydefinedboundaries,lackofgraduatedsanctionsandthelackofconflictresolutionmechanisms.DespitethesecollectiveactionproblemstherearealsoexamplesofhowmultiplestakeholdergroupstrytocollectivelygovernmalariaasapublicbadinRuhuha.Thecommunityhealthworkersplayanimportantroleinthiscollectiveaction.Thecommunityhealthworkersmonitorwhethertherearerule-breakersandgiveadvicewherenecessary.Communitymemberstrusttheadviceandinformationthatisspreadbycommunityhealthworkers,becausetheyarepartofthecommunity.
ICTsplayaroleinthesegovernancearrangementsofactorsthataredealingwithmalariaasapublicbadinRuhuha.Firstofall,theadvantagesofICTsarethattheyfacilitateinformationandcommunicationflowsthatarerealtime,lowcost,overlargedistanceandacrossstakeholdergroups.ApartfromthestrategicICT-basedhealthinterventions,mobilephonesplayacrucialroleinmalariapreventionbyfacilitatingawarenessraising,improvingtheinformationflowswithinandbetweenthestakeholdergroups,andbystrengtheningtheimplementationofcommunitylevelmalariapreventionrulesandregulations.However,stakeholdersalsopointedoutthattherearemisconceptionsaboutmalariainRuhuha.Therefore,notallinformationistrustworthyandmobilephonescouldalsoincreasethespreadofmisconceptions.Despitethisdisadvantage,mobile-basedinformationandcommunicationflowsimprovethecollectivegovernanceofmalariaasapublicbad.

99
7.Recommendations1.MyresultsshowthatthereisnocompliancewithsomeofOstrom’s
designprinciples,whicharenoclearlydefinedboundaries,lackofgraduatedsanctionsandthelackofconflictresolutionmechanisms.Thisanalysiscanbeusedbyactorsfromthevariouslevelstogovernmalariaasapublicbadmoreeffectivelybylookingforpossibilitiestodefineboundaries,graduatedsanctions,andconflictresolutionmechanisms.
2.TheanalysisinmythesisidentifiedthatactorsperceivethatknowledgeaboutmalariaisnotenoughinRuhuhaandthatmisconceptionsexist.Thesefindingscouldbeusefulforthehealthrelatedactorsandlocalleaderstoimprovecommunicationflowsandinformationprovisiontoincreaseknowledgeandtodissolvemisconceptions.Thefindingsofmyresearchshowthatcommunityhealthworkersandhealthcenterstaffaretrustedactorswhenitcomestospreadinginformationaboutmalaria.Therefore,theycouldplayanimportantroleinchangingperceptions.
3.Furthermore,myresearchprovidesinsightsinhowICTsareusedinmalariapreventionandcontrolinRuhuhaacrossandwithindifferentlevelsofthehealthsystem.Actorsfromthevariouslevelsandstakeholdergroupscouldusetheseinsightstoimprovetheirinformationandcommunicationflows.Inaddition,theinsightsofthisanalysiscouldbeusefultoincreasetheeffectivenessanduseofICTinterventionsthatwillbeimplementedinthefuture.

100
ReferencesBloom,G.,&Standing,H.(2008).Futurehealthsystems:Whyfuture?Whynow?SocialScience&Medicine,66,2067-2075.doi:10.1016/j.socscimed.2008.01.032Bloomfield,B.P.(1991).TheRoleofInformationSystemsintheUKNationalHealthService:ActionataDistanceandtheFetishofCalculation.SocialStudiesofScience,21(4),701-734.doi:10.1177/030631291021004004Chetley,A.(2006).Improvinghealth,connectingpeople:TheroleofICTsinthehealthsectorofdevelopingcountries.AFrameworkPaper,vol.7Fegan,G.,Moulsdale,M.,&Todd,J.(2011).Thepotentialofinternet-basedtechnologiesforsharingdataofpublichealthimportance.BulletinoftheWorldHealthOrganization,89:82-82doi:10.2471/BLT.11.085910.Retrievedfromhttp://www.who.int/bulletin/volumes/89/2/11-085910/en/Frasier,H.,May,M.,&Wanchoo,R.(2008).E-HealthRwandaCaseStudy.Retrievedfromhttp://www.ehealth-connection.org/files/resources/Rwanda%20%20Appendices.pdfFriedman.AandMiles.S.(2006).Stakeholders:TheoryandPractice.Oxford:OxfordUniversityPress.Hartshorne,J.,&Carstens,I.(1990).Roleofinformationsystemsinpublichealthservices.MEDLINE,45(4),313-317Holden,S.T.,&Tilahun,M.(2018).TheimportanceofOstrom’sDesignPrinciples:YouthgroupperformanceinnorthernEthiopia.WorldDevelopment,104,10-30.doi:10.1016/j.worlddev.2017.11.010Gilbert,M.(2006).Rationalityincollectiveaction.PhilosophyoftheSocialSciences,36(1),3–17GoR(GovernmentofRwanda).(2015).NationalICTstrategyandplan.Retrievedfromhttp://www.rdb.rw/uploads/tx_sbdownloader/NICI_III.pdfIbrahim,S.S.(2006).Fromindividualtocollectivecapabilities:Thecapabilityapproachasaconceptualframeworkforself–help.JournalofHumanDevelopment,7(3),397–416Ingabire,C.M.,Alaii,J.,Hakizimana,E.,Kateera,F.,Muhimuzi,D.,Nieuwold,I.,…VanDenBorne,B.(2014).Communitymobilizationformalariaelimination:applicationofanopenspacemethodologyinRuhuhasector,Rwanda.MalariaJournal,13(1),167.http://doi.org/10.1186/1475-2875-13-167Ingabire,C.M.,Hakizimana,E.,Kateera,F.,Rulisa,A.,VanDenBorne,B.,Nieuwold,I.,…Alaii,J.(2016B).Usinganinterventionmappingapproachforplanning,implementingandassessingacommunity-ledprojecttowardsmalaria

101
eliminationintheEasternProvinceofRwanda.MalariaJournal,15(1),594.http://doi.org/10.1186/s12936-016-1645-3Ingabire,C.M.,Kateera,F.,Hakizimana,E.,Rulisa,A.,Borne,D.V.B.,Muvunyi,C.,...Alaii,J.(2016A).StakeholderEngagementinCommunity-basedMalariaStudiesinaDefinedSettingintheEasternProvince,Rwanda.MediterraneanJournalofSocialSciences,7(2)Ingabire,C.M.,Rulisa,A.,VanKempen,L.,Muvunyi,C.,Koenraadt,C.J.,VanVugt,M.,...Alaii,J.(2015).Factorsimpedingtheacceptabilityanduseofmalariapreventivemeasures:implicationsformalariaeliminationineasternRwanda.MalarJ,14(1),136.doi:10.1186/s12936-015-0659-6Lucas,H.(2008).Informationandcommunicationstechnologyforfuturehealthsystemsindevelopingcountries.SocialScience&Medicine,66,2122-2132.doi:10.1016/j.socscimed.2008.01.033Mwangi,W.(2006).TheSocialRelationsofe-GovernmentDiffusioninDevelopingCountries:TheCaseofRwanda.TheProceedingsofthe7thAnnualInternationalConferenceonDigitalGovernmentResearch,199-208.Retrievedfrom:https://www.researchgate.net/profile/Jane_Fedorowicz/publication/221585403_Design_principles_for_public_safety_response_mobilization/links/54cf8eec0cf29ca810feb65e.pdf#page=225Nayak,S.,Thorat,S.,&Kalyankar,N.(2010).Reachingtheunreached:ARoleofICTinsustainableRuraldevelopment.(IJCSIS)InternationalJournalofComputerScienceandInformationSecurity,7(1),220-224Ostrom,E.(1999).Copingwithtragediesofthecommons.AnnualReviewofPoliticalScience,2,493-535Ostrom,E.(1993).Designprinciplesinlong-enduringirrigationinstitutions.WaterResourcesResearch,29(7),1907-1912.doi:10.1029/92wr02991Oxoby,R.(2009).Understandingsocialinclusion,socialcohesion,andsocialcapital.InternationalJournalofSocialEconomics,36(12),1133–1152.Panir.(2011).RoleofICTsintheHealthSectorinDevelopingCountries:ACriticalReviewofLiterature.JournalofHealthInformaticsinDevelopingCountries,5(1),197-208President’sMalariaInitiative.(2016).RwandaMalariaOperationalPlanFY2016Rulisa,S.,Kateera,F.,Bizimana,J.P.,Agaba,S.,Dukuzumuremyi,J.,Baas,L.,...Vries,P.J.(2013).MalariaPrevalence,SpatialClusteringandRiskFactorsinaLowEndemicAreaofEasternRwanda:ACrossSectionalStudy.PLoSONE,8(7).doi:10.1371/journal.pone.0069443

102
Sahay,S.,&Walsham,G.(1995).Informationtechnologyindevelopingcountries:Aneedfortheorybuilding.InformationTechnologyforDevelopment,6(3/4),111–124Sein,M.K.,&Harindranath,G.(2004).ConceptualizingtheICTArtifact:TowardUnderstandingtheRoleofICTinNationalDevelopment.TheInformationSociety,20(1),15-24.doi:10.1080/01972240490269942Shiferaw,F.,&Zolfo,M.(2012).Theroleofinformationcommunicationtechnology(ICT)towardsuniversalhealthcoverage:ThefirststepsofatelemedicineprojectinEthiopia.GlobalHealthAction,5(1),15638.doi:10.3402/gha.v5i0.15638Thapa,D.,Sein,M.K.,&Sæbø,Ø.(2012).BuildingcollectivecapabilitiesthroughICTinamountainregionofNepal:Wheresocialcapitalleadstocollectiveaction.InformationTechnologyforDevelopment,18(1),5-22.doi:10.1080/02681102.2011.643205UnitedNations.N.D.SustainableDevelopment,health.Retrievedfromhttps://www.un.org/sustainabledevelopment/health/Venot,J.P.(2016).ASuccessofSomeSort:SocialEnterprisesandDripIrrigationintheDevelopingWorld.WorldDevelopment,79(313),69–81Walsham,G.,&Sahay,S.(2006).Researchoninformationsystemsindevelopingcountries:Currentlandscapeandfutureprospects.InformationTechnologyforDevelopment,12(1),7-24.doi:10.1002/itdj.20020WHO.(2016).Worldmalariareport.Geneva,Switzerland:WorldHealthOrganizationWilson,D.S.,Ostrom,E.,&Cox,M.E.(2013).Generalizingthecoredesignprinciplesfortheefficacyofgroups.JournalofEconomicBehavior&Organization,90.doi:10.1016/j.jebo.2012.12.010

103
Appendices
Appendix1–OverviewofintervieweesNumber Actor Position Amountfor
travelexpensesDate EndTimeof
InterviewDuration
1 Communitymember(above50yearsfemale)
Farmer 2000RWF 08.01.2018 10.03 45:44minutes
2 Communitymember(above50yearsfemale)
Farmer 2000RWF 08.01.2018 10:50 42:46minutes
3 Communitymember(above50yearsmale)
Farmer 2000RWF 08.01.2018 15.13 50:08minutes
4 Communitymember(above50yearsmale)
Farmer 2000RWF 08.01.2018 16.27 01:07:18minutes
5 Communitymember(above35-50yearsfemale)
Farmer 2000RWF 09.01.2018 10:47 01:29:01minutes
6 Communitymember(above35-50yearsfemale)
Farmer 2000RWF 09.01.2018 12:18 01:04:36minutes
7 Communitymember(above35=50yearsmale)
Farmer 2000RWF 09.01.2018 15:10 01:04:02minutes
8 Communitymember(above35-50yearsmale)
Farmer 2000RWF 09.01.2018 16:07 53:44minutes
9 Communitymember(above18-35yearsfemale)
Studentorunemployed
2000RWF 10.01.2018 10:19 01:03:06minutes
10 Communitymember(above18-35yearsfemale)
Studentorunemployed
2000RWF 10.01.2018 11:35 01:08:56minutes
11 Communitymember(above Farmer 2000RWF 10.01.2018 15:25 01:19:04

104
18-35yearsmale) minutes12 Communitymember(above
18-35yearsmale)Farmer 2000RWF 10.01.2018 16:51 01:16:48
minutes13 Cooperativesfemale Farmerofrice
cooperative5000RWF 11.01.2018 10:23 01:34:03
minutes14 Cooperativesmale Farmerofrice
cooperative5000RWF 11.01.2018 11:54 01:10:42
minutes15 Schoolteacher Teacherat
G.S.Butereri5000RWF 11.01.2018 14:55 33:06minutes
16 NonCommunityhealthinsurance(sendtheirchildwhoisastudent)
Studentofprimaryschool
2000RWF 11.01.2018 15:37 26:58minutes
17 StaffofRuhuhaHealthcenter(male)
Ruhuhahealthcenterstaff
5000RWF 12.01.2018 10:10 01:00:57minutes
18 StaffofRuhuhaHealthcenter(female)
Ruhuhahealthcenterstaff
5000RWF 12.01.2018 11:36 01:05:11minutes
19 Communityhealthworker(female)
Communityhealthworker(RuhuhaH.C.)
2000RWF 12.01.2018 15:07 01:09:12minutes
20 Communityhealthworker(male)
Communityhealthworker(RuhuhaH.C.)
2000RWF 12.01.2018 15:51 35:33minutes
21 CMATs CMATS(CommunityMalariaActionTeams)
2000RWF 15.01.2018 10:23 55:20minutes

105
22 Pharmacy Pharmacy–Ruhuhahealthcenter
5000RWF 15.01.2018 11:36 48:37minutes
23 Localleader Localleader 5000RWF 15.01.2018 14:55 52:30minutes24 MEPR Assistantof
MEPR–RuhuhaHealthCenter
5000RWF 15.01.2018 15:51 42:32minutes
25 Traditionalhealer Traditionalhealer
5000RWF 15.01.2018 17:02 40:56minutes
26 NonCommunityhealthinsurance
Non-healthinsuranceperson
2000RWF 16.01.2018 10:26 01:23:03minutes
27 NMCP-RBC Directorofvectorcontrolunit–Rwandabiomedicalcenter
5000RWF 17.01.2018 11:43 40:10minutes
28 NationalHealthinsurancescheme-RSSB
Headofcommunity-basedhealthinsurancedepartmentCBHI-RSSB
5000RWF 22.01.2018 16:06 35:33minutes
29 Nyamatadistricthospital DirectorofNyamatadistricthospital
5000RWF 24.01.2018 09:23 30:46minutes
30 Religiousleader Priest 5000RWF 24.01.2018 11:11 25:08minutes

106
31 Privatepharmacy Privatepharmacy
5000RWF 24.01.2018 12:33 01:08:08minutes
32 HeadofRuhuhahealthcenter
LeaderofRuhuhaHealthCenter
5000RWF 24.01.2018 13:49 01:04:14minutes

107
Appendix2–Topiclistoftheinterviews
2.1Interviewtopics–community
1. Doyouevertalkaboutmalariainyoureverydaylife?(ifnot–whynot?)Onwhatoccasion?Towhom,howface-to-face/phone/other,whatdoyoutalkabout.
2. Doyouthinkthereisknowledgeinyour(community,regionetc.)aboutmalaria?Istheknowledgeenough?Arethereanymisconceptions?Why?Howdotheyspread?
3. Whatmalariaprevention/controlmeasuresdoyouknow(liketraps,nets,
repellant,stayingoutsideafterdark,removingstagnantwatervesselswheremosquitosbreedetc.)?Whatdoyouthinkabouteachofthem?Doyouevertalkaboutthem?Withwhom?
4. Wheredothesemeasurescomefrom?Whoensurethattheseprevention
andcontrolmeasuresareinplace?Isitenforcedinanyway?Why,how,howdoyoufeelaboutit?
5. DoyoureceiveinformationaboutMalaria?E.g.radio,tv,socialmedia,churchservices,advertisements(fromwhom,howandwhatinformation,whatdoyoudowiththeinformation).
6. Whomdoyoutrustthemostwhenitcomestogettingreliable
informationonmalaria?Whomdon’tyoutrust?Why,whynot?
7. Whatisthesituationrightnowinyour(community,region,etc.)regardingmalaria?Whatdoyouthinkaboutit?
8. Doyoufeellikeyoucandosomethingaboutthemalariaissueyourself?How/why/whynot?Howdoesthatmakeyoufeel?
9. Recently,IhaveheardthatanumberofpeopleinRwandaareusing
mobilephonesmoreandmore.Doyoueveruseyourphonetocommunicateorreceiveinformationaboutmalaria?Doyouthinkmobilephonesplayaroleinbattlingmalariainthefuture?How,why,whynot?Canyougivemeexamples?

108
2.2Interviewtopics–actorsinhealth/policylevel
1. Onwhatoccasion(s)doyoutalkaboutmalaria?Towhom,howface-to-face/phone/other,whatdoyoutalkabout.
2. Whatisthesituationrightnowinyour(community,region,etc.)regardingmalaria?Whatdoyouthinkaboutit?
3. Whoensurethatpracticesregardingmalariapreventionandcontrol(like
traps,nets,repellant,stayingoutsideafterdark,removingstagnantwatervesselswheremosquitosbreedetc.)areinplace?Isitenforcedinanyway?Why,how,howdoyoufeelaboutit?
4. Aretheretrainings,programsorawarenessraisingtopreventandcontrol
malaria?Whoensuresthattheseareinplace?Isitenforcedinanyway?Why,how.
5. Doyouthinkthereisknowledgeinthe(community,regionetc.)aboutmalaria?Istheknowledgeenough?Arethereanymisconceptions?Why?Howdotheyspread?
6. Whichactorsdoyoutrustthemostwhenitcomestospreadingreliable
informationonmalaria?Whomdon’tyoutrust?Why,whynot?
7. Doyoufeellikethecommunitycandosomethingaboutthemalariaissuethemselves?How/why/whynot?Howdoesthatmakeyoufeel?
8. Recently,IhaveheardthatanumberofpeopleinRwandaareusing
mobilephonesmoreandmore.Doyouthinkmobilephonesmayplayaroleinbattlingmalaria?How,why,whynot?Canyougivemeexamples?

109
Appendix3–OverviewofcodesCode ExplanationTalkaboutmalaria-occasion,whom Whenintervieweestalkabouttalking
aboutmalariaandtowhomTalkaboutmalaria-what Whatintervieweestalkaboutwhen
theytalkaboutmalariaSituationregardingmalaria Whenintervieweesmentioned
somethingaboutthesituationregardingmalaria
Knowledge-isitthere?enough? Whetherintervieweesthinkthereis(enough)knowledge
Knowledge-misconceptions Whensomethingaboutmisconceptionsismentioned
Preventionandcontrolmeasures-whichonesandinfotheytell
Whenintervieweesmentionedaboutmalariapreventionandcontrolmeasuresandwhattheytalkaboutit
Preventionandcontrolmeasures-whoensurestheyareinplace
Whenintervieweesmentionedwhoensurespreventionandcontrolmeasuresareinplace
Preventionandcontrolmeasures-enforced?
Whenintervieweesmentionorexplainaboutmalariapreventionandcontrolmeasuresbeingenforcedornot
Receivinginformation-fromwhom,how
Whenisbeingmentionedthatthepersonreceivesinformationfromwhomandhow
Receivinginformation-whatinformation
Whenapersonmentionedaboutwhatinformationheorshereceives
Receivinginformation-whatdoyoudowithit
Whenisbeingpersonwhatthepersondoeswiththeinformation
Trust-actorsthataretrusted Whenactorsthataretrustedarementioned
Trust-actorsthatarenottrusted Whenactorsthatarenottrustedarementioned
Cando-feellikecandosomethingyourself?
Whentheintervieweementionsorexplainswhetherheorshefeelsthecommunitymemberscandosomethingaboutthemalariaissuethemselves
Cando-whatshouldbedoneaboutmalaria
Whentheintervieweementionssomethingrelatedtowhatheorshefeelsthatshouldbedoneaboutmalariatosolveitorfutureactions
ICTs-roleofmobilephones Whentheintervieweementionssomethingabouttheroleofamobilephone
ICTs-roleofotherICTs WhentheintervieweementionssomethingabouttheroleofotherICTs

110
ICTs-futurerole WhentheintervieweementionsorexplainsaboutthepossiblefutureroleofmobilephonesorotherICTsinthefuture
Healthinsurance Whensomethingabouthealthinsuranceismentionedbyaninterviewee
Problems-->regardingmalaria Whenanintervieweementionsorexplainsaproblemregardingmalaria
Publicbad-rulesandregulations Whenanintervieweementionssomethingrelatedtorulesandregulationsregardingmalariapreventionandcontrol
Roleofclubandcare Whenanintervieweeexplainstheroleofcluband/orcare
RoleofCMATs WhenanintervieweeexplainsormentionsabouttheroleofCommunityMalariaActionTeams
Roleofcommunityhealthworker Whenanintervieweeexplainsormentionsabouttheroleofcommunityhealthworkers
Roleofcooperative Whenanintervieweeexplainstheroleofcooperatives
Roleofhealthcenter(staff) Whenanintervieweeexplainsormentionsabouttheroleofthehealthcenter
Roleofhealthcenterpharmacy Whenanintervieweeexplainsormentionsabouttheroleofthehealthcenterpharmacy
Roleoflocalleader Whenanintervieweeexplainsormentionsabouttheroleoflocalleader
RoleofMEPR WhenanintervieweeexplainsormentionsabouttheroleoftheMalariaEliminationProgram
RoleofNyamatadistricthospital Whenanintervieweeexplainsormentionsabouttheroleofthedistricthospital
RoleofRBC WhenanintervieweeexplainsormentionsabouttheroleoftheRwandaBiomedicalCenter
Roleofresearchers Whenanintervieweeexplainsormentionsabouttheroleofresearchers
Roleofteacher Whenanintervieweeexplainsormentionsabouttheroleofteachersandschools
Roleofthechurch Whenanintervieweeexplainsormentionsabouttheroleofthechurchandpriestsandotherreligiousleaders

111
Roleoftraditionalhealers Whenanintervieweeexplainsormentionsabouttheroleoftraditionalhealers
Sendinginformationorsharinginformation
Whenanintervieweementionsaboutsendingorsharinginformationwithotheractorsrelatedtomalariapreventionandcontrol
Trainings,programsorawarenessraisings
Whenanintervieweementionsaboutatraining,programorawarenessraising