Prevalence and Predictors of Posttraumatic Stress Disorder in Adult Survivors of Childhood Cancer

The Role of Beliefs in the Relationship Between Health Problemsand Posttraumatic Stress in Adolescent and Young Adult CancerSurvivors
Lisa A. Schwartz • Anne E. Kazak •
Branlyn W. DeRosa • Matthew C. Hocking •
Wendy L. Hobbie • Jill P. Ginsberg
Published online: 1 October 2011
� Springer Science+Business Media, LLC 2011
Abstract In addition to the potential for ongoing health
concerns, adolescent and young adult (AYA) childhood
cancer survivors frequently report posttraumatic stress
symptoms (PTSS). The current study examines whether
beliefs about health moderate the relationship between the
number of health problems and PTSS 2 months later in 140
survivors. Beliefs, as measured by scales of the Health
Competence Beliefs Inventory (HCBI), negatively related
to PTSS while health problems positively related to PTSS.
Three scales of the HCBI-health perceptions, satisfaction
with healthcare and cognitive competence—were signifi-
cant moderators. The relationship between health problems
and PTSS was stronger in the presence of less adaptive
beliefs. These beliefs represent potentially malleable
intervention targets for reducing PTSS in childhood cancer
survivors.
Keywords Posttraumatic stress � Cancer � Beliefs �Health problems
Adolescent and young adult (AYA) survivors of childhood
cancer are no longer unusual; one out of every 640 adults
is a survivor of childhood cancer and that number is
increasing (Hewitt, Weiner, & Simone, 2003). Despite
being cured of their original cancer, survivors are vulner-
able to medical (e.g., cardiac and pulmonary disease, en-
docrinopathies, infertility) and psychosocial (e.g., distress,
cognitive problems) sequelae secondary to their disease
and treatment and are at risk for second malignancies.
Approximately 62% of AYA survivors have at least one
chronic health condition (e.g., cardiac or pulmonary dis-
ease, endocrine or growth problems) and these individuals
are eight times more-likely to have a severe or life-
threatening health condition than sibling controls (Oeffin-
ger et al., 2006). Adding further to the vulnerability of this
group is evidence for non-engagement in necessary
healthcare; less than 20% of survivors receive cancer-
related follow-up care that address their risks and necessary
surveillance, and these visits decline during the AYA
period (Nathan et al., 2009).
Because of cumulative cancer-related stressors and events
that may serve as traumatic events (Kazak, Scheider, &
Kassam-Adams, 2009), coupled with increasing cognitive
maturity that facilitates reflection of the cancer experience
and implications, AYA survivors are at risk for developing
posttraumatic stress disorder (PTSD) and frequently report
posttraumatic stress symptoms (PTSS). Up to 35% have a
current or prior diagnosis of PTSD (Hobbie et al., 2000;
Pelcovitz et al., 1998; Rourke et al., 2007; Schwartz &
Drotar, 2006) and up to 50% of AYA survivors experience
PTSS in the form of intrusive, avoidant, and arousal symp-
toms (Brown et al., 2003; Hobbie et al., 2000; Langeveld
et al., 2004). These findings are consistent with current
conceptualizations of PTSD in that physical illness and
associated experiences and fears may be a significant risk
factor for medical traumatic stress and PTSD (Kazak et al.,
2006).
Health problems relate to PTSS in AYA survivors
(Gerhardt et al., 2007; Langeveld et al., 2004; Rourke et al.,
L. A. Schwartz (&) � A. E. Kazak � B. W. DeRosa �M. C. Hocking � W. L. Hobbie � J. P. Ginsberg
The Children’s Hospital of Philadelphia, 34th and Civic Center
Blvd., CHOP North #1484, Philadelphia, PA 19104, USA
e-mail: [email protected]
L. A. Schwartz � A. E. Kazak � J. P. Ginsberg
The University of Pennsylvania School of Medicine,
Philadelphia, PA, USA
123
J Clin Psychol Med Settings (2012) 19:138–146
DOI 10.1007/s10880-011-9264-1

2007; Schwartz & Drotar, 2006). This relationship is not
surprising given the late effects of survivors that increase
with age and often emerge in young adulthood (Oeffinger
et al., 2004). Late effects refer to the sequelae of their
disease or treatment that can include any organ system
(e.g., endocrine, pulmonary, cardiac), cognitive deficits,
and even second cancer diagnoses (Oeffinger et al., 2006).
Further, as AYA survivors become more autonomous in
their health care management, providers may have more
direct conversations with survivors about their late effects
and/or future risk of late effects that may increase survi-
vors’ anxiety. Also, in general, health problems have been
found to relate to PTSS in other populations (Lawler,
Ouimette, & Dahlstedt, 2005; Oeffinger et al., 2006; Oui-
mette et al., 2004; Stein, McQuaid, Pedrelli, Lenox, &
McCahill, 2000).
PTSS have important implications for cancer survivors
in terms of their physical and psychological health. The
increase in distress and anxiety related to PTSS can relate
to health harming behaviors that exacerbate their late
effects, or risk for future late effects or new cancer diag-
noses (Clarke & Eiser, 2007; Lee, Santacroce, & Sadler,
2007). Further, PTSS have been hypothesized to impact
engagement in follow-up care in this population (Rourke
et al., 2007). Finally, PTSS have been shown to relate to
psychological impairment, reduced quality of life, and
difficulty with achievement of developmental tasks of
young adulthood for young adult survivors (Rourke et al.,
2007; Schwartz & Drotar, 2006).
Beliefs play an important role in understanding trau-
matic responses and in intervention (Kazak, McClure et al.,
2004; Luszczynska, Benight, & Cieslak, 2009). In the
pediatric oncology literature, caregiver beliefs about the
likelihood of cancer- and treatment-related suffering,
death, and devastation of the family related to higher levels
of PTSS (Kazak, McClure et al., 2004). Child and ado-
lescent survivor beliefs related to the severity of past life
threat also have been related to PTSS (Barakat et al., 1997;
Stuber et al., 1997). Among AYA survivors, worse per-
ceived severity of medical late effects and higher levels of
perceived current life threat predicted whether or not the
survivor had a diagnosis of PTSD (Rourke et al., 2007).
Thus, beliefs may similarly play a role as potentially
malleable factors to reduce PTSS in AYA cancer survivors.
Because of AYA’s increasing autonomy and awareness
of the health implications of cancer survivorship, adaptive
beliefs about health and health-related competencies may
mitigate PTSS in AYA survivors experiencing health
problems. In order to assess beliefs about health specifi-
cally relevant to AYAs, the Health Competence Beliefs
Inventory (HCBI) (DeRosa et al., 2011) was developed.
Health competence beliefs refer to a multidimensional set
of perceptions about health and well-being, including
beliefs about current and future health concerns, ability to
manage medical issues, and ability to relate to others
(DeRosa et al., 2011). Recent findings from our work
indicate that AYA survivors have less competent health
beliefs than controls (Kazak et al., 2010). As measured by
the HCBI, beliefs about health perceptions, satisfaction
with healthcare, cognitive competence, and autonomy may
influence the relationship between health and PTSS in this
population, and, thus, may be viable targets of intervention.
In other words, beliefs may help us understand under what
conditions health problems and PTSS are linked.
To our knowledge, no studies have examined the role of
beliefs about health and well-being in the relationship
between health problems and PTSS in childhood cancer
survivors or other populations. Thus, using the same
sample of AYA survivors on which the HCBI was vali-
dated, the current study tests how health competence
beliefs interact with health problems to relate to PTSS. It
was hypothesized that the four belief constructs measured
by the HCBI–health perceptions, satisfaction with health-
care, cognitive competence, and autonomy—would mod-
erate the relationship between the number of patient-
reported health problems at a clinic visit and PTSS
2 months later.
Methods
Participants
Participants were 140 AYA survivors of childhood cancer
recruited as part of a larger project examining psycholog-
ical and health outcomes in survivors. Inclusion criteria
included a diagnosis of cancer before age 21, at least
5 years from diagnosis, 2 or more years from the com-
pletion of medical treatment for cancer, English speaking,
and ability to read at the fifth grade level. Survivors of
childhood brain tumors were excluded due to the likelihood
of cognitive deficits limiting their ability to complete the
study. Survivors ranged in age from 16 to 29 years
(M = 20.3, SD = 3.2) and 55.4% of the sample was
female. Cancer diagnoses included leukemias (42.9%),
lymphomas (20.7%), and solid tumors (36.4%). The aver-
age number of years since diagnosis was 11.85 (M = 4.56;
range = 5–24). The sample was predominantly Caucasian
(88.5%) but also included participants who were African–
American (4.3%), Asian (3.6%), Hispanic (2.2%) and more
than one race or unknown (1.4%). Educational attainment
of survivors included current high school student (25.9%),
high school graduate (12.2%), attended some college
(40.3%), or 4 year college graduate or greater (21.6%).
Fifty-one (36.4%) survivors reported being in a committed
J Clin Psychol Med Settings (2012) 19:138–146 139
123

relationship, nine of whom were married. In terms of
family income, 30 survivors reported less than $50,000, 52
survivors reported $50,000 to $99,999, 46 reported
$100,000 or more, and 12 did not report on family income.
The majority (63.6%) reported a personal income of less
than $10,000. Thus, it is suspected that most AYA’s esti-
mated the income of their family of origin.
Procedures
Survivors were recruited consecutively at their annual visit
to a childhood cancer survivorship clinic at a large pedi-
atric medical facility. Informed consent or assent for those
survivors under age 18 was obtained during the clinic visit.
Of 221 approached, 191 (86%) consented to the study, 167
(87% of consented) completed baseline measures during or
following their clinic visit, and 139 (73% of consented)
completed follow-up measures via mail approximately
2 months after the initial appointment. Participants were
compensated $20 and $30 for completing baseline and
follow-up measures, respectively. All study procedures
were approved by the institutional review board.
Measures
Health Problems
The Health Knowledge Inventory (HKI) (Schwartz et al.,
2010) measures self-reported health problems in AYAs
with and without a history of cancer. Clinical expertise
(from both local providers and nationally recognized
experts) and literature reviews on late effects were used to
develop the 35 items (health problems). Participants
endorse whether or not they have 35 categories of health
problems that are potential late effects of cancer treatment.
In other words, the measure is presented as a symptom
checklist. Participants are provided with a list of health
problems with examples (e.g., heart/blood problems: weak
heart, chest pain, irregular heartbeat, high blood pressure)
and asked to endorse (Yes/no) whether or not they have
each of the 35 potential categories of problems. The
problems include those affecting organ systems referred to
as organic/major (e.g., cardiac, pulmonary, blood disor-
ders) and more general and somatic problems referred to as
constitutional/other (e.g., balance, sleep, growth). There is
no overlap among problems. The total number of problem
endorsements is summed into a total score of health
problems (maximum of 35). Prior analysis from the same
dataset revealed that overall percent agreement of report of
problems between survivors and their providers was 86.8%
(Schwartz et al., 2008).
Health Competence Beliefs
The Health Competence Beliefs Inventory (HCBI)
(DeRosa et al., 2011) was developed using an iterative pro-
cess of inductive and deductive methods. A multi-disci-
plinary team developed items that were pilot tested,
modified, and then subjected to a large validation study with
AYAs who survived cancer and who did not have history of
chronic illness. Factor analysis resulted in a 21-item measure
that assesses health-related beliefs across four factors: (1)
health perceptions (six items; scores ranging 6–24)—current
health and the possibility of future health problems (e.g., My
future health is very uncertain, I am not as healthy as other
people my age); (2) satisfaction with healthcare (five items;
scores ranging 4–20)—engagement with and effectiveness
of healthcare (e.g., My doctors understand my medical his-
tory, I can reach my doctor or nurse by phone or email when I
need to); (3) cognitive competence (five items; scores
ranging 4–20)—perceived cognitive ability, memory (e.g.,
Most people my age are smarter than me, I learn new things
as easily as other people); and (4) Autonomy (five items;
scores ranging 4–20)—independence from their family and
their ability to accomplish their healthcare independently
(e.g., I prefer having my parents with me at doctor’s
appointments, I rely on my parents or siblings more than
other people my age). Participants rate the extent to which
they agree with the statements on a four point scale. Higher
scores indicate beliefs that are more adaptive and that have
been found to relate to positive psychosocial functioning
(DeRosa et al., 2011). Specifically, higher scores on the
subscales indicate positive beliefs about health status, cog-
nitive abilities, and ability to function autonomously, and
greater satisfaction with healthcare. Internal consistencies
for the factors range from .75–.87.
Posttraumatic Stress
The Posttraumatic Stress Checklist-Civilian Version
(PCL-C) (Weathers & Ford, 1996) is a 17-item self-report
questionnaire that assesses five symptoms of arousal
(e.g., having difficulty concentrating), five symptoms of
re-experiencing (e.g., repeated, disturbing memories,
thoughts, or images of a stressful experience), and seven
symptoms of avoidance (e.g., avoiding activities or situa-
tions because they reminded you of a stressful experience)
based on DSM-IV criteria for PTSD. It has been shown to
demonstrate excellent reliability and validity (Ruggiero,
Del Ben, Scotti, & Rabalais, 2003; Smith, Redd, DuHamel,
Vickberg, & Ricketts, 1999; Weathers & Ford, 1996) and
has been used with childhood cancer survivors (Schwartz
& Drotar, 2006). Participants rate the level of distress
associated with each symptom on a five point scale
(1 = not at all; 5 = extremely). Scores range from 17 to
140 J Clin Psychol Med Settings (2012) 19:138–146
123

85. The PCL-C total score is used to measure PTSS and has
excellent internal consistency in this sample (a = .91). A
score of 40 or above indicates significant PTSS (Manne,
DuHamel, Gallelli, Sorgen, & Redd, 1998). The measure
can also be scored to indicate endorsement of DSM-IV
criteria for PTSD (Weathers & Ford, 1996). Specifically, a
score of three or higher on an item indicates endorsement
of that symptom. Subsequently, whether or not a respon-
dent meets criteria for arousal, re-experiencing, and
avoidance clusters can be derived based on symptom
endorsement. The PTSS total score was used as the main
outcome in the current study. Because survivors are likely
to experience general distress at a clinic visit that may
artificially inflate reports of PTSS, and the likelihood that
health problems serve as traumatic stress triggers of cancer
survivors, PTSS was measured 2 months after the clinic
visit.
Data Analysis
Descriptive statistics were calculated to characterize the
sample and the variables of interest in the moderation
model. Bivariate correlations were also used to identify the
relationship between patient-reported number of health
problems (HKI) at baseline and PTSS (PCL-C) 2 months
later.
Following Aiken and West (1991) and Holmbeck (2002)
recommendations for conducting moderation analyses,
regressions were used to identify whether HCBI subscales
moderated the relationship between health problems and
PTSS. In other words, we were interested in identifying
whether or not beliefs interacted with health problems to
affect the relationship between health problems and PTSS.
The independent variables (i.e., HKI total score; four HCBI
subscale scores) were first centered (i.e., sample M sub-
tracted from raw score).
Then, following standard procedures for testing inter-
actions between variables, four interaction terms were
created (i.e., the product of the centered HKI total health
problems score [predictor main effect] and the centered
HCBI subscale score [moderator main effect]) (Aiken &
West, 1991). As described by Aiken and West (1991),
centering the variables before creating interaction terms
reduces multicollinearity between main effects and inter-
action terms and facilitates interpretation of simple slope
post-hoc analysis.
Four regressions were conducted, representing the four
potential moderators of the HCBI subscales. In each
regression, the main effects (centered HKI and HCBI
subscale score) were entered in step one and the associated
interaction term was entered in step two to predict PTSS.
Post-hoc probing of the interaction terms was conducted to
test if the slopes were significantly different from zero.
That is, post-hoc probing tested whether or not the rela-
tionship between health problems and PTSS was significant
for both high and low levels of health competence beliefs.
In order to do so, it was necessary to create two new
conditional moderator variables of high and low values for
each HCBI subscale variable that emerged as a significant
interaction term in the original regressions. This was done
by creating variables that represented high values of the
moderator variables (each respondents’ score ?1 SD of the
mean of the variable) and low values of the moderator
variable (each respondents’ score -1 SD of the mean of
the variable). Holmbeck (2002) noted, the ±SD is a con-
vention that can be replaced with other theoretically
meaningful high or low values. As described by Holmbeck
(2002), the interaction terms of the HKI score by the high
or low values of the HCBI scales were then computed.
Next, two separate regressions tested the effect of the
interaction term on PTSS after controlling for the main
effects of HKI and HCBI high or low scores. To plot the
regression lines, an equation was employed which included
terms for the two main effects and the interaction, along
with the corresponding unstandardized regression coeffi-
cients and the y-intercept.
Results
Descriptive and Bivariate Results
Survivors reported a range of health problems, from 0 to 17,
with an average of 5.7 (SD = 3.9). Posttraumatic stress
symptoms, measured 2 months later using the PCL-C, ran-
ged from 17 to 84, with an average of 26.2 (SD = 10.9).
Seventeen survivors (12.1%) had a score of over 40, indi-
cating significant PTSS. In terms of meeting criteria for
symptom clusters based on symptom endorsement, 33
(23.6%) met criteria for re-experiencing, 20 (14.3%) met
criteria for avoidance, 28 (20.0%) met criteria for arousal,
and 14 (10.0%) met criteria for all PTSD symptoms clusters.
As expected, health problems and PTSS were significantly
correlated (r = .44, p \ .001). This strong relationship held
when examining the correlation of PTSS with the separate
problem categories of organic/major (r = .31, p \ .001)
and constitutional/other (r = .48, p \ .001). Posttraumatic
stress symptoms were not correlated with age, age at diag-
nosis, or time off treatment. Scores on HCBI were: health
perceptions (M = 18.0, SD = 4.1, range = 7–24), cogni-
tive competence (M = 15.2, SD = 2.9, range = 6–20),
autonomy (M = 14.0, SD = 2.9, range = 7–20), and sat-
isfaction with health care (M = 17.4, SD = 2.2, range =
12–20).
J Clin Psychol Med Settings (2012) 19:138–146 141
123

Regression and Moderation Results
As shown in Table 1, health problems significantly and
positively related to PTSS in all regressions. Health
Competence Beliefs Inventory health perceptions, cogni-
tive competence, and satisfaction with healthcare also were
significantly and negatively related to PTSS.
The interaction terms for HKI by HCBI (subscales of
health perceptions, cognitive competence, satisfaction with
care) were significant in all regressions except for the one
testing the moderating effect of autonomy (Table 1). Post-
hoc regressions confirmed the significance of the interac-
tion terms as represented by high and low values of the
HCBI scales. In other words, results confirmed that health
perceptions, cognitive competence, and satisfaction with
care (HCBI subscales) influenced the relationship between
health problems (HKI) and PTSS (PCLC) 2 months later.
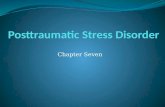
Figures 1, 2, and 3 show the regression slopes representing
the levels of PTSS that correspond to high and low values
of the health competence beliefs (straight and dotted lines)
and high and low values of reported health problems (left
and right side of x axis). As shown in the figures, the
relationship of health problems and PTSS (as indicated by
highest values of PTSS in the graph) was stronger in the
presence of less adaptive beliefs related to health percep-
tions (Fig. 1), cognitive competence (Fig. 2), and satis-
faction with healthcare (Fig. 3). In other words, having low
health competence beliefs (health perceptions, cognitive
competence, satisfaction with healthcare) increases the
likelihood that high health problems relate to PTSS.
Table 1 Regression analyses
for health problems and health
beliefs predicting PTSS
Regression b df R2 D R2 F p-value
Health perceptions (HP)
Step 1: Main effects 2 .21 .21 17.74 .00
HKI health problems total .31 .00
HCBI–HP -.22 .02
Step 2: Interaction 1 .24 .03 13.94 .00
HKI health problems total .28 .00
HCBI–HP -.19 .04
Health problems 9 HP -.14 .02
Satisfaction with healthcare (SHC)
Step 1: Main effects 2 .23 .23 15.59 .00
HKI health problems total .39 .00
HCBI–SHC -.29 .00
Step 2: Interaction 1 .29 .06 17.67 .00
HKI health problems total .39 .00
HCBI–SHC -.18 .02
Health problems 9 SHC -.25 .00
Cognitive competence (CC)
Step 1: Main effects 2 .27 .27 23.92 .00
HKI health problems total .29 .00
HCBI–CC -.33 .00
Step 2: Interaction 1 .29 .03 18.06 .00
HKI health problems total .25 .00
HCBI–CC -.29 .00
Health problems 9 CC –.17 .03
Autonomy (AU)
Step 1: Main effects 2 .18 .18 13.92 .00
HKI health problems total .42 .00
HCBI–AU .01 .93
Step 2: Interaction 1 .18 .01 9.73 .00
HKI health problems total .42 .00
HCBI–AU .00 .99
Health problems 9 AU .09 .26
142 J Clin Psychol Med Settings (2012) 19:138–146
123

Discussion
This study demonstrated that beliefs affect the nature of the
relationship between health problems and traumatic stress
outcomes in a sample of AYA cancer survivors. Survivors
with more health problems reported increased PTSS, a
finding consistent with previous research in pediatric can-
cer (Gerhardt et al., 2007; Langeveld et al., 2003; Rourke
et al., 2007; Schwartz & Drotar, 2006) and other popula-
tions (Englehard, can de Hout, Weerts, Hox, & can
Doornen, 2009; Lawler et al., 2005; Ouimette et al., 2004;
Stein et al., 2000). The relationship between health prob-
lems and PTSS is complicated and dynamic; it is likely that
PTSS exacerbates health problems and vice versa. How-
ever, the literature supporting increased rates of PTSD/
PTSS in cancer survivors, especially those with late effects,
supports the likelihood that health problems precede PTSS
in cancer survivors (Hobbie et al., 2000; Pelcovitz et al.,
1998; Rourke et al., 2007; Schwartz & Drotar, 2006). The
novelty of the data reported in this paper is that beliefs
about health competence moderated this relationship.
These findings have potential implications for decreasing
traumatic stress in this population and for supporting the
need to attend to psychological variables, in addition to
medical outcomes, when monitoring this medically vul-
nerable group of AYAs (National Cancer Institute and
Livestrong Young Adult Alliance, 2006).
Three of the four subscales (i.e., health perceptions,
satisfaction with healthcare, and cognitive competence) of
the HCBI were significant moderators of the relationship
between health problems and PTSS. Specifically, survivors
who reported greater current health problems were more
17.51
27.65
21.54
23.61
15
20
25
30
35
-1 SD Mean +1 SD
PTSS
Health Problems
Low HCBI Health Perception
High HCBI Health Perception
Fig. 1 Health problems and PTSS as moderated by health perception
24.01
32.54
20.74
23.12
15
20
25
30
35
-1 SD Mean +1 SD
PTSS
Health Problems
Low HCBI Cognitive Competence
High HCBI Cognitive Competence
Fig. 2 Health problems and PTSS as moderated by cognitive
competence
20.37
34.81
21.98
24.47
15
20
25
30
35
40
-1 SD Mean +1 SD
PTSS
Health Problems
Low HCBI Health Care Satisfaction
High HCBI Health Care Satisfaction
Fig. 3 Health problems and PTSS as moderated by health care
satisfaction
J Clin Psychol Med Settings (2012) 19:138–146 143
123

likely to experience PTSS when they felt more vulnerable
to future health problems, less satisfaction with health care,
and more cognitively competent. The association between
PTSS and survivors’ beliefs about their general health and
vulnerability (health perceptions) is logical. These beliefs
may reflect realistic medical problems related to their
treatment and late effects; thus, a sense of vulnerability
may be appropriate. However, it may be possible to modify
such beliefs to reflect more control and competence in
managing the negative health-related beliefs. This is
important because survivors are expected to engage in
ongoing health monitoring, especially in the presence of
current health problems or significant risks. Avoidance or
arousal associated with PTSS may interfere with adherence
to recommended medical monitoring and treatment. For
example, women treated for Hodgkin’s lymphoma during
childhood are at increased risk for breast cancer (up to 20%
will be diagnosed with breast cancer by age 45), yet 63% of
those in their 20s and 30s have not had a screening
mammogram (Oeffinger et al., 2009). Thus, modifying
health perception beliefs may not only be critical for
reducing PTSS, but for also ultimately facilitating recom-
mended medical follow-up care.
Beliefs about satisfaction with healthcare are similarly
relevant targets of intervention. Survivors who feel dis-
satisfied with their care while experiencing many health
problems may be especially vulnerable to distress and may
subsequently disengage from important medical care and
not adhere to provider recommendations (Bell, Kravitz,
Thom, Krupat, & Azari, 2002). Psychosocial barriers to
accessing care are also prevalent in this population
(National Cancer Institute and Livestrong Young Adult
Alliance, 2006), thus potentially exacerbating lack of
engagement with healthcare for those experiencing PTSS.
Therefore, addressing ways to improve satisfaction with,
and engagement with, health care is a critical target of
intervention.
Survivor beliefs about their cognitive abilities also were
related to greater PTSS in the presence of more health
problems. Like health concerns, cognitive concerns are
often justified given that cognitive late effects are among
the most common consequences of cancer treatments that
involve or impact the central nervous system (Mulhern &
Butler, 2004). Such concerns about memory, attention and
performing cognitively may be associated with psycho-
logical factors (Baker, Taylor, & Hermann, 2009). Thus,
negative beliefs about cognitive competence may be
modifiable to improve one’s self-efficacy and skills to
manage daily tasks and related stress. Cognitive-behavioral
approaches have been integrated successfully in remedia-
tion approaches to address beliefs that affect cognitive
abilities in pediatric cancer survivors (Butler et al., 2008).
These approaches may be modified to reduce the risk of
PTSS in this population.
Although pediatric cancer survivors are more likely to
live with their parents than peers and do so longer
(Langeveld et al., 2003), beliefs about autonomy were not
significant moderators of health problems and PTSS. Par-
ents of survivors are more likely to accompany their chil-
dren to healthcare visits than parents of never ill controls
(Ressler, Cash, McNeill, Joy, & Rosoff, 2003). The extent
to which this higher level of parental involvement may be
helpful or constraining for development and wellbeing is
unknown (Banner, Mackie, & Hill, 1996). Given the lack
of support for autonomy as a moderator in this study, these
beliefs seem to be less salient than the other types of beliefs
for understanding PTSS.
The moderating role of beliefs is clinically significant;
modifying beliefs to be more adaptive may mitigate the
association of health problems and PTSS. As shown in
interventions with childhood cancer survivors and their
families, beliefs are important intervention targets that
have led to promising intervention outcomes (Kazak,
Alderfer et al., 2004). Therefore, the HCBI may be useful
for identifying a patient’s maladaptive beliefs to inform
subsequent intervention. Long-term, it may be helpful to
assess health competence beliefs along with PTSS and
health problems as part of the standard of care in survi-
vorship given the prominence of these problems and the
fact that beliefs are amenable to intervention.
Several limitations of this study should be acknowl-
edged. The study focused on survivors of childhood cancer,
and therefore the findings may not generalize to other
populations. However, these findings may be relevant to
other pediatric illness groups that are known to experience
medical trauma (Kazak et al., 2009) and necessitate long-
term medical monitoring. This sample consists of survivors
attending a specialized survivorship clinic and may repre-
sent a group with more medical or psychosocial problems
than others (Ness et al., 2009). Thus, it is unclear if the
findings would generalize to other AYA survivor samples
who may not seek specialized survivorship care or who are
not engaged with the medical system. Replicating the study
in a non-clinic sample may be important given the possi-
bility that those with significant PTSS or maladaptive
beliefs may be less motivated to engage in follow-up care.
Although the range of PTSS varied greatly in the study,
most survivors experienced small to moderate levels of
PTSS. This is consistent with findings that, although most
AYA survivors are psychologically healthy, a small but
significant minority are very distressed (Rourke et al.,
2007; Schwartz & Drotar, 2006). The sample, like many
other childhood cancer survivor samples, is also relatively
homogenous with the majority being non-Hispanic White.
144 J Clin Psychol Med Settings (2012) 19:138–146
123

Finally, the data is based on self-report and lacks method
variance.
While the study would benefit from replication in other
cancer survivor and broader samples, the results highlight
potential targets of intervention for those seeking care in
survivorship clinics. Survivors who report PTSS warrant
further clinical and research attention to identify ways to
reduce their distress and potential related impairment.
Intervention with this small but significant minority of
survivors is important given the potential for PTSS to be
persistent in AYAs (Perkonigg et al., 2005) and to impact
health and related behaviors (Clarke & Eiser, 2007; Lee
et al., 2007). Future research should identify those survi-
vors most at risk based on high endorsement of health
problems and PTSS, coupled with maladaptive health
competence beliefs, and explore related intervention
approaches.
Acknowledgments This research was supported by the National
Cancer Institute (CA106928). The authors thank the study partici-
pants. We also thank Claire Carlson, RN, Sue Ogle, CRNP, and
Maureen Reilly, BSN, RN for assisting with recruitment and access to
patients; and Andrew Gaffney, Emily Knudsen-Strong, Muhammad
Monsour, Ifigenia Mougianis, Sonali Sanyal, Mary Caitlin St. Clair,
Mindy Yang, and Lauren Danzi for serving as research assistants.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing andinterpreting interactions. Newbury Park, CA: Sage.
Baker, G. A., Taylor, J., & Hermann, B. (2009). How can cognitive
status predispose to psychological impairment? Epilepsy andBehavior, 15, S31–S35. doi:10.1016/j.yebeh.2009.03.021.
Banner, L. M., Mackie, E. J., & Hill, J. W. (1996). Family
relationships in survivors of childhood cancer: Resource or
restraint? Patient Education and Counseling, 28, 191–199. doi:
0738-3991(96)00901-9.
Barakat, L. P., Kazak, A. E., Meadows, A. T., Casey, R., Meeske, K.,
& Stuber, M. L. (1997). Families surviving childhood cancer: A
comparison of posttraumatic stress symptoms with families of
healthy children. Journal of Pediatric Psychology, 22, 843–859.
Bell, R. A., Kravitz, R. L., Thom, D., Krupat, E., & Azari, R. (2002).
Unmet expectations for care and the patient–physician relation-
ship. Journal of General Internal Medicine, 17, 817–824. doi:
jgi10319.
Brown, R. T., Madan-Swain, A., & Lambert, R. (2003). Posttraumatic
stress symptoms in adolescent survivors of childhood cancer and
their mothers. Journal of Traumatic Stress, 16, 309–318. doi:
10.1023/A:1024465415620.
Butler, R. W., Copeland, D. R., Fairclough, D. L., Mulhern, R. K.,
Katz, E. R., Kazak, A. E., et al. (2008). A multicenter,
randomized clinical trial of a cognitive remediation program
for childhood survivors of a pediatric malignancy. Journal ofConsulting and Clinical Psychology, 76, 367–378. doi:
10.1037/0022-006X.76.3.367.
Clarke, S. A., & Eiser, C. (2007). Health behaviours in childhood
cancer survivors: A systematic review. European Journal ofCancer, 43, 1373–1384. doi:10.1016/j.ejca.2007.03.002.
DeRosa, B. W., Kazak, A. E., Doshi, K., Schwartz, L. A., Ginsberg,
J., Mao, J. J., et al. (2011). Development and validation of the
Health Competence Beliefs Inventory in young adults with and
without a history of childhood cancer. Annals of BehavioralMedicine, 41, 48–58. doi:10.1007/s12160-010-9228-y.
Englehard, I. M., can den Hout, M. A., Weerts, J., Hox, J. J., & can
Doornen, L. J. P. (2009). A prospective study of the relation between
posttraumatic stress and physical health symptoms. InternationalJournal of Clinical and Health Psychology, 9, 365–372.
Gerhardt, C. A., Yopp, J. M., Leininger, L., Valerius, K. S., Correll,
J., Vannatta, K., et al. (2007). Brief report: Post-traumatic stress
during emerging adulthood in survivors of pediatric cancer.
Journal of Pediatric Psychology, 32, 1018–1023. doi:10.1093/
jpepsy/jsm038.
Hewitt, M., Weiner, S. L., & Simone, J. V. (2003). Childhood cancersurvivorship: Improving care and quality of life. Washington
DC: National Academies Press.
Hobbie, W. L., Stuber, M., Meeske, K., Wissler, K., Rourke, M. T.,
Ruccione, K., et al. (2000). Symptoms of posttraumatic stress in
young adult survivors of childhood cancer. Journal of ClinicalOncology, 18, 4060–4066.
Holmbeck, G. N. (2002). Post-hoc probing of significant moderational
and mediational effects in studies of pediatric populations.
Journal of Pediatric Psychology, 27, 87–96.
Kazak, A. E., Alderfer, M. A., Streisand, R., Simms, S., Rourke, M.
T., Barakat, L. P., et al. (2004). Treatment of posttraumatic stress
symptoms in adolescent survivors of childhood cancer and their
families: A randomized clinical trial. Journal of FamilyPsychology, 18, 493–504. doi:10.1037/0893-3200.18.3.493.
Kazak, A. E., DeRosa, B. W., Schwartz, L. A., Hobbie, W., Carlson,
C., Ittenbach, R. F., et al. (2010). Psychological outcomes and
health beliefs in adolescent and young adult survivors of
childhood cancer and controls. Journal of Clinical Oncology,28, 2002–2007. doi:10.1200/JCO.2009.25.9564.
Kazak, A. E., Kassam-Adams, N., Schneider, S., Zelikovsky, N.,
Alderfer, M. A., & Rourke, M. (2006). An integrative model of
pediatric medical traumatic stress. Journal of Pediatric Psy-chology, 31, 343–355.
Kazak, A. E., McClure, K. S., Alderfer, M. A., Hwang, W., Crump, T.
A., Le, L. T., et al. (2004). Cancer-related parental beliefs: The
Family Illness Beliefs Inventory (FIBI). Journal of PediatricPsychology, 29, 531–542. doi:10.1093/jpepsy/jsh055.
Kazak, A. E., Schneider, S., & Kassam-Adams, N. (2009). Pediatric
medical traumatic stress. In M. Roberts & R. Steele (Eds.),
Handbook of pediatric psychology (4th ed., pp. 205–215). New
York: Guilford.
Langeveld, N. E., Grootenhuis, M. A., Voute, P. A., & de Haan, R. J.
(2004). Posttraumatic stress symptoms in adult survivors of
childhood cancer. Pediatric Blood and Cancer, 42, 604–610.
doi:10.1002/pbc.20024.
Langeveld, N. E., Ubbink, M. C., Last, B. F., Grootenhuis, M. A.,
Voute, P. A., & De Haan, R. J. (2003). Educational achievement,
employment and living situation in long-term young adult
survivors of childhood cancer in the Netherlands. Psycho-Oncology, 12, 213–225. doi:10.1002/pon.628.
Lawler, C., Ouimette, P., & Dahlstedt, D. (2005). Posttraumatic stress
symptoms, coping, and physical health status among university
students seeking health care. Journal of Traumatic Stress, 18,
741–750. doi:10.1002/jts.20082.
Lee, Y.-L., Santacroce, S. J., & Sadler, L. (2007). Predictors of
healthy behaviour in long-term survivors of childhood cancer.
Journal of Clinical Nursing, 16, 285–295. doi:
10.1111/j.1365-2702.2007.01966.x.
Luszczynska, A., Benight, C., & Cieslak, R. (2009). Self-efficacy and
health-related outcomes of collective trauma. European Psy-chologist, 14, 51–62.
Manne, S. L., DuHamel, K., Gallelli, K., Sorgen, K., & Redd, W. H.
(1998). Posttraumatic stress disorder among mothers of pediatric
J Clin Psychol Med Settings (2012) 19:138–146 145
123

cancer survivors: Diagnosis, comorbidity, and utility of the
PTSD checklist as a screening instrument. Journal of PediatricPsychology, 6, 357–366.
Mulhern, R. K., & Butler, R. W. (2004). Neurocognitive sequelae of
childhood cancers and their treatment. Pediatric Rehabilitation,7, 1–16. doi:10.1080/13638490310001655528.
Nathan, P. C., Ford, J. S., Henderson, T. O., Hudson, M. M., Emmons,
K. M., Casillas, J. N., et al. (2009). Health behaviors, medical
care, and interventions to promote healthy living in the
childhood cancer survivor study cohort. Journal of ClinicalOncology, 27, 2363–2373. doi:10.1200/JCO.2008.21.1441.
National Cancer Institute and Livestrong Young Adult Alliance
(2006). Closing the gap: Research and care imperatives for
adolescents and young adults with cancer No. 06-6067.
Ness, K. K., Leisenring, W., Goodman, P., Kawashima, T., Mertens,
A. C., Oeffinger, K. C., et al. (2009). Assessment of selection
bias in clinic-based populations of childhood cancer survivors: A
report from the childhood cancer survivor study. Pediatric Bloodand Cancer, 52, 379–386. doi:10.1002/pbc.21829.
Oeffinger, K. C., Ford, J. S., Moskowitz, C. S., Diller, L. R., Hudson,
M. M., Chou, J. F., et al. (2009). Breast cancer surveillance
practices among women previously treated with chest radiation
for a childhood cancer. JAMA, 301, 404–414. doi:10.1001/
jama.2008.1039.
Oeffinger, K. C., Mertens, A. C., Hudson, M. M., Gurney, J. G.,
Casillas, J., Chen, H., et al. (2004). Health care of young adult
survivors of childhood cancer: A report from the childhood
cancer survivor study. Annals of Family Medicine, 2, 61–70.
Oeffinger, K. C., Mertens, A. C., Sklar, C. A., Kawashima, T.,
Hudson, M. M., Meadows, A. T., et al. (2006). Chronic health
conditions in adult survivors of childhood cancer. New EnglandJournal of Medicine, 355, 1572–1582.
Ouimette, P., Cronkite, R., Henson, B. R., Prins, A., Gima, K., &
Moos, R. H. (2004). Posttraumatic stress disorder and health
status among female and male medical patients. Journal ofTraumatic Stress, 17, 1–9. doi:10.1023/B:JOTS.0000014670.
68240.38.
Pelcovitz, D., Libov, B. G., Mandel, F., Kaplan, S., Weinblatt, M., &
Septimus, A. (1998). Posttraumatic stress disorder and family
functioning in adolescent cancer. Journal of Traumatic Stress,11, 205–221.
Perkonigg, A., Pfister, H., Stein, M. B., Hofler, M., Lieb, R.,
Maercker, A., et al. (2005). Longitudinal course of posttraumatic
stress disorder and posttraumatic stress disorder symptoms in a
community sample of adolescents and young adults. AmericanJournal of Psychiatry, 162, 1320–1327. doi:10.1176/appi.ajp.
162.7.1320.
Ressler, I. B., Cash, J., McNeill, D., Joy, S., & Rosoff, P. M. (2003).
Continued parental attendance at a clinic for adult survivors of
childhood cancer. Journal of Pediatric Hematology/oncology,25, 868–873.
Rourke, M. T., Hobbie, W. L., Schwartz, L., & Kazak, A. E. (2007).
Posttraumatic stress disorder (PTSD) in young adult survivors of
childhood cancer. Pediatric Blood and Cancer, 49, 177–182.
doi:10.1002/pbc.20942.
Ruggiero, K. J., Del Ben, K., Scotti, J. R., & Rabalais, A. E. (2003).
Psychometric properties of the PTSD Checklist-Civilian Ver-
sion. Journal of Traumatic Stress, 16, 495–502. doi:10.1023/
A:1025714729117.
Schwartz, L. A., Carlson, C. A., Ginsberg, J. P., Hobbie, W. L.,
Ittenbach, R., Mao, J. J., et al. (2008). Perceptions of medicalproblems: Young adult childhood cancer survivors and theirhealthcare providers. Berlin: Paper presented at the Annual
Conference of the International Society for Pediatric Oncology.
Schwartz, L. A., & Drotar, D. (2006). Posttraumatic stress and related
impairment in survivors of childhood cancer in early adulthood
compared to healthy peers. Journal of Pediatric Psychology, 31,
356–366. doi:10.1093/jpepsy/jsj018.
Schwartz, L. A., Mao, J. J., DeRosa, B. W., Ginsberg, J. P., Hobbie,
W. L., Carlson, C. A., et al. (2010). Self-reported health
problems of young adults in clinical settings: survivors of
childhood cancer and healthy controls. Journal of the AmericanBoard of Family Medicine, 23, 306–314. doi:10.3122/jabfm.
2010.03.090215.
Smith, M. Y., Redd, W., DuHamel, K., Vickberg, S. J., & Ricketts, P.
(1999). Validation of the PTSD Checklist-Civilian Version in
survivors of bone marrow transplantation. Journal of TraumaticStress, 12, 485–499. doi:10.1023/A:1024719104351.
Stein, M. B., McQuaid, J. R., Pedrelli, P., Lenox, R., & McCahill, M.
E. (2000). Posttraumatic stress disorder in the primary care
medical setting. General Hospital Psychiatry, 22, 261–269.
Stuber, M. L., Kazak, A. E., Meeske, K., Barakat, L., Guthrie, D.,
Garnier, H., et al. (1997). Predictors of posttraumatic stress
symptoms in childhood cancer survivors. Pediatrics, 100,
958–964.
Weathers, F. W., & Ford, J. (1996). Psychometric review of the PTSD
Checklist. In B. H. Stamm (Ed.), Measurement of stress, trauma,and adaptation (pp. 250–251). Lutherville, MD: Sidran Press.
146 J Clin Psychol Med Settings (2012) 19:138–146
123