
The reporting of adverse clinical incidents ... · The reporting of adverse clinical incidents –...
78
Reporting of adverse clinical incidents ______________________________________________________________ ______________________________________________________________ CASPE Research, October 2001 The reporting of adverse clinical incidents – international views and experience Dr Charles Shaw James Coles CASPE Research 11-13 Cavendish Square London W1G 0AN Tel: 020 7307 2879 Fax: 020 7307 2422 e-mail: [email protected]
Transcript of The reporting of adverse clinical incidents ... · The reporting of adverse clinical incidents –...

Reporting of adverse clinical incidents
______________________________________________________________
______________________________________________________________ CASPE Research, October 2001
The reporting of adverse clinical incidents – international views and experience
Dr Charles Shaw James Coles
CASPE Research 11-13 Cavendish Square
London W1G 0AN Tel: 020 7307 2879 Fax: 020 7307 2422
e-mail: [email protected]

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 1
Contents
Background Page 6
1. Commentaries and Proposals 8
1.1 Australia Taskforce on Quality in Australian Health Care
Australian Patient Safety Foundation (APSF) 1.2 Canada National Safety Council Province of Quebec 1.3 New Zealand
The Cull Report 1.4 UK
‘An Organisation with a Memory’ ‘Building a Safer NHS for Patients’ 1.5 USA American Medical Association (AMA) Institute of Medicine (IoM) National Academy for State Health Policy (NAHSP) Veteran’s Health Administration (VHA) National Summit on Medical Errors and Patient Safety Research
2. Examples of established programmes 22 2.1 Health Care Australia: Wimmera Base Hospital Australian Incident Monitoring System (AIMS) Australian GP sentinel event study
Sweden: National register of medical incidents Switzerland: Anaesthesia-related mortality and incidents
USA: Medication errors and adverse events Medication Error Reporting program (MER) MedMARx MedWatch USA: Emergency Care Research Institute (ECRI)
USA: State-wide incident reporting systems State of Massachusetts State of New York USA: The Joint Commission for the Accreditation of
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 2
Healthcare (JCAHO) 2.2 Other industries
Non-medical industries Aviation Safety Reporting Systems (ASRS) 3. Evidence and practice 31 3.1 Policy 3.1.1 Aims, users and values 3.1.2 Define the words and concepts Terminology 3.1.3 Define a reportable event or situation (strategic) 3.2 Organisation 3.2.1 Clarify scope and authority of all reporting systems Integrating Information sources 3.2.2 Allocate individual and corporate responsibilities Co-ordination Learning centre Evaluation Standards and methodology Role of provider organisations
Role of individuals 3.2.3 Design systems Development process System features Criteria and components of reporting systems 3.2.4 Develop a positive culture
Proposed NHS steps to embed adverse incident reporting locally General attitudes to reporting errors and adverse events Specific factors affecting attitudes to reporting
3.3 Methods of reporting 3.3.1 Case recognition Direct observation Record review Error reporting systems Hospital in-patient data Combined approaches 3.3.2 Reporting procedures Ease of reporting Medium of reporting Minimum data set for reports Type of report 3.3.3 Analysis, taxonomy and aggregation Taxonomy of human error Coding systems for errors

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 3
Severity categories of damage 3.3.4 Feedback and information 3.3.5 System quality (process, outcome) Independent evaluation Evidence of benefit Volume of reports Under-reporting of ADRs Quality of reports 3.4 Resources 3.4.1 Time 3.4.2 Education and training Risk management Undergraduate clinical training Local reporting co-ordinators 3.4.3 Data systems 3.4.4 Funding National costs State costs 4. Research Opportunities 60 Appendices Appendix 1: Non-medical reporting systems Appendix 2: Incident report form – State of Florida
Appendix 3: Reporting codes - New York State, NYPORTS Appendix 4: AHRQ call for research into reporting strategies
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 4
List of Tables Table 1 Cull Report, New Zealand, 2001 – summary of conclusions Table 2 UK NHS – sources and estimates of adverse event data Table 3 Dineen, Walshe – weaknesses of local reporting, NHS Trusts 1999 Table 4 NHS – weaknesses in current reporting systems, 2000 Table 5 NHS – clinical incident reporting methods, England Table 6 NHS – proposals for mandatory reporting, 2000 Table 7 NHS – proposals for voluntary reporting, 2000 Table 8 NHS – Functions of proposed National Patient Safety Agency Table 9 AMA – General principles for Patient Safety Reporting Systems Table 10 IoM recommendations for a national centre for patient safety Table 11 NASHP – barriers to state reporting systems Table 12 NASHP – cost elements of state reporting programmes Table 13 NASHP – Questions for developing reporting systems Table 14 NASHP– Questions for existing reporting systems Table 15 NASHP – scope of mandatory state reporting systems, USA 2000 Table 16 NASHP – Protection of mandatory state reporting, USA 2000 Table 17 NASHP – Critical success factors perceived by states Table 18 VHA – elements of patient safety improvement programme Table 19 Dotseth, USA – Medical anxieties about mandatory reporting Table 20 Wimmera, Australia – messages for reporting systems Table 21 Rosenthal – Comparison of state systems in Florida and New York Table 22 IoM – Characteristics of some state reporting systems Table 23 New York State – action plan to improve reporting systems Table 24 Barach, Small – reporting systems for non-medical events Table 25 Barach, Small – barriers and incentives for reporting: non-medical Table 26 AHRQ – Definitions Table 27 NCPS – Definitions; National Centre for Patient Safety draft handbook,
2000 Table 28 JCAHO - Definition of reportable (“sentinel”) event Table 29 NHS – National mechanisms for reporting adverse situations in the
NHS Table 30 Design criteria for reporting system, transfusion medicine Table 31 Behavioural criteria for reporting systems, non-medical Table 32 Components of reporting system, transfusion medicine Table 33 Components of reporting system, NHS proposal Table 34 Williamson, McKay - Components of reporting system, 1990 Table 35 Northern Region, UK - Voluntary reporting of ADRs Table 36 UK - Factors rarely claimed to discourage ADR reporting, 1993 Table 37 ITU - Factors claimed to discourage error reporting, 1997-99 Table 38 Netherlands – Voluntary reporting of ADRs, 1997 Table 39 Netherlands – Reasons for not reporting ADRs Table 40 USA – Three purposes of mandatory reporting systems Table 41 IoM – Comparison of mandatory and voluntary reporting Table 42 UK – Comparison of event analysis and traditional audit in General
Practice, 1995

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 5
Table 43 Australia - Screening by routine data compared with case records Table 44 USA – Adverse event factors recognisable by routine data screening Table 45 ISMP – Features of reporting process, 2000 Table 46 UK – Issues to be addressed by proposed minimum data set for NHS
reporting Table 47 Florida – reported patient injuries and claims, 1995-99 Table 48 VHA – severity categories Table 49 UK – NHS research questions Table 50 USA – AHRQ research questions List of Figures Figure 1 VHA – report review and analysis flow Figure 2 Proposed national reporting system, UK NHS 2001
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 6
Reporting of Adverse Clinical Incidents
Background International attention has been focused on patient safety largely by the results of a study in New York that was intended to assess the implications of no-fault compensation for medical errors. A similar study was undertaken in Australia, and early results show similar findings in the UK. In the USA and Australia, national centres have been set up to co-ordinate the collection and learning from adverse events and near-misses. A similar structure and procedures are proposed for the UK NHS.
Some marker studies
USA The Harvard Medical Practice Study (HMPS) is the benchmark for estimating the extent of medical injuries occurring in hospitals. Brennan et al reviewed the medical charts of 30,121 patients admitted to 51 acute care hospitals in New York state in 19841. They reported that adverse events (injuries caused by medical management that prolonged admission or produced disability at the time of discharge) occurred in 3.7% of admissions. A subsequent analysis of the same data found that 69% of injuries were caused by errors2. The Institute of Medicine (IoM) estimated in 19993 that between 44 and 98,000 people die each year in the USA as a result of medical errors at a cost of between $17 and $29 billion to society (of which $8.8 billion is direct health care costs). Between 2.9 and 3.7 per cent of hospitalisations involve an adverse event. Their report recommends that “a nationwide mandatory reporting system be established that provides for the collection of standardised information by state governments about adverse events.” These should include ambulatory and institutional care as well as hospitals, and should be supported by a complementary voluntary reporting system.
Australia In a study of the quality of Australian health care, a population based study modelled on HMPS, investigators reviewed the medical records of 14,179 admissions to 28 hospitals in New South Wales and South Australia in 19954. An adverse event occurred in 16.6% of admissions, resulting in permanent disability in 13.7% of patients and death in 4.9%; 51% of adverse events were considered to have been preventable.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 7
UK A retrospective review5 of 1,014 medical and nursing records in two acute hospitals in the Greater London area showed that 110 (10.8%) patients experienced an adverse
event, with an overall rate of adverse events of 11.7% when multiple adverse events were included. About half of these events were judged preventable with ordinary standards of care. A third of adverse events led to moderate or greater disability or
death. These results suggest that adverse events are a serious source of harm to patients and a large drain on NHS resources. Some are major events; others are frequent, minor events that go unnoticed in routine clinical care but together have massive economic consequences. “Medical errors stem more from systematic organisational failures rather than from the isolated failure of individuals” Charles Vincent et al 19986

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 8
1 Commentaries and proposals Worldwide, many organisations and enquiries have expressed views on how adverse events might be reduced. Examples of operational programmes for reporting them are given in Chapter 2.
1.1 Australia
Taskforce on Quality in Australian Health Care Chapter 2 of this 1996 report reviews existing mechanisms of incident surveillance and analysis in hospitals, notes the development of Commonwealth-funded pilot projects in various specialties and recommends a national classification and reporting programme7. This led to the establishment of the Australian Council for Safety and Quality in Health Care in 2001.
Australian Patient Safety Foundation (APSF) The Australian Patient Safety Foundation (APSF)8 is a non-profit, independent organisation based in Adelaide, South Australia. It has developed an incident monitoring system which is used in many healthcare systems within Australia to identify and analyse failures in healthcare delivery, based on the Australian Incident Monitoring Study (AIMS), published in 1997 (see page 22).
1.2 Canada
National Safety Council Canada aims to establish a national patient-safety strategy and oversight council. Representatives from federal and provincial governments, licensing bodies and professional associations like the CMA agreed in September 2001 to launch a 1-year exercise to craft a business plan for a national safety council. They agreed to establish a steering committee and 5 working groups to define a national strategy over the next 6 months. Several priorities were identified; for instance, an information system that is either a single national system, or a series of provincial systems that can communicate with one another and use the same definitions and the same data will be needed. The steering committee will also have to look at regulatory, monitoring and reporting issues
Province of Quebec A recent Quebec ministerial committee report on preventable errors in health services delivery has recommended regulatory changes obligating mandatory reporting of accidents and errors; open disclosure to patients; and improved data gathering about both preventable accidents and the iatrogenic effects of pharmaceuticals.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 9
1.3 New Zealand
The Cull Report In November 2000, the Minister of Health appointed Helen Cull to chair an inquiry into processes concerning adverse medical events and to report in March 2001. A key issue for the Government was to introduce legislation to ensure that agencies such as the Health and Disability Commissioner, the Medical Council of New Zealand, the Medical Practitioners Disciplinary Tribunal and the Accident Compensation Commission (ACC) Medical Misadventures Unit could identify patterns of adverse medical outcomes to ensure speedy response and action on incidents. Another key issue was the adequacy of patient complaint mechanisms. The focus of the Cull Report9 is on complaints, incompetent doctors and the linking of existing reporting systems (eg mortality reviews); it is not primarily about self-reporting and individual clinical incidents, although the key issues may also be found relevant in the UK. Within New Zealand, there are potentially fourteen organisations that can currently undertake an investigation into the same adverse medical event, contemporaneously or cumulatively without reference to each other. This has led to a lengthy process with a multiplicity of agencies processing the same complaints, making the complaint process confusing, cumbersome, difficult to access and costly, both financially and emotionally. Table 1: The Cull Report, New Zealand 2001 - summary of conclusions Principal problems
Multiple Complaint Processes: There is no streamlined approach to complaint mechanisms in New Zealand with multiple agencies undertaking separate investigations into the same incident.
Delays: The time delays in undertaking complaint investigations are frustrating and burdensome.
No disclosure: There has been no agency interaction or co-ordination to enable the disclosure of relevant information.
Difficult Access: The complaint mechanism is difficult for patients to access because of: lack of knowledge, the way the complaint is treated, the failure of agencies to refer patients to the appropriate complaint mechanism.
No Database: There is no centralised database to detect repeated poor practice.
No reporting: There has been no reporting of practitioners who are practising below an acceptable standard by their colleagues or other health professionals.
No powers of suspension prior to charge: There is no power to suspend practitioners prior to a charge being laid and during a process of investigation, even if a potential public risk has been identified.
Insufficient cost recovery: Access by patients to compensation either through ACC or to cost recovery and damages through the Complaints Review Tribunal is unsatisfactory.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 10
Unmet patient needs by ACC: No ACC entitlements can be received until an investigation is complete, sometimes 12 to 15 months after the event. There is no ability to recover personal financial loss or costs through ACC prior to the claim being accepted. This fails to address patient needs at the relevant time.
Immediate solutions
To assist with the timely identification or investigation of adverse medical outcomes, there are some immediate solutions to the current problems. They are:
Mandatory reporting of practitioners whose practice is below acceptable standards. Enabling the Medical Council to have the power to suspend practitioners when the public is at risk, prior to the laying of a charge before the Disciplinary Tribunal.
Protecting disclosure of relevant health information by and to agencies such as ACC, HDC, the Medical Council, and the MPDT in the interests of public health or public safety.
1.4 UK
‘An Organisation with a Memory’10 In addition to the mechanisms listed in Table 2, this report also notes that adverse events can also be reported through local incident report systems, coroner’s offices, periodic Audit Commission studies, whistle-blowing and routine statistics. But these give an incomplete and inconsistent picture as definitions, data capture and their aggregation vary across the NHS. A definition of “Untoward incidents” was proposed (para 4.12) to be those that are:
- serious in that a patient or patients were harmed or could have been harmed
- unexpected - likely to give rise to serious public concern or criticism of the service
involved Table 2: NHS UK - sources and estimates of adverse events data Source Event Annual total Confidential enquiry Suicides, homicides within
12 months of contact with mental health service
1,190
Confidential enquiry Maternal mortality 125 Confidential enquiry Peri-operative deaths 20,000 Confidential enquiry Stillbirths and infant deaths 7,800 Clinical complaints, written Hospital 27,949 Clinical complaints, written Primary care 38,857 NHS litigation authority Clinical negligence claims
settled above local excess 810
Regional report systems Serious untoward incidents 2,500 Medical Devices Agency Adverse incidents (including
87 deaths, 345 serious injuries)
6,610
Medicines Control Agency Reported adverse drug reactions
18,196
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 11
The original (and extant) NHS guidance of 1955 requires reports “as soon as possible” to the hospital secretary (sic), naming the injured and all witnesses, detailing “the full facts” and also the action taken at the time11. Subsequent advice12 extended this to “potential” loss, injury or damage and required that one individual should be designated to follow up reports (which should consist of no more than two forms). The Allitt Inquiry in 199413 and the Kent and Canterbury screening report in 199714 illustrated the lack of systematic communication between the hospital and District and Regional Health Authorities and their successors. Advice to the service was further distilled into Controls Assurance core standards for risk management systems in 1999:
- “incidents including ill-health, are systematically identified, recorded and reported to management in accordance with an agreed policy of positive, non-punitive reporting”
- “all reported incidents are communicated to the relevant external body in accordance with the relevant reporting requirements”
A survey15 of incident reporting in NHS Trusts in 1999 showed wide variations at local level (Table 3). Table 3: Dineen, Walshe - weaknesses of local reporting, NHS Trusts 1999 Systems: one fifth do not have organisation-wide reporting systems Training: less than half provide specific training in risk management or incident reporting Definitions: less than a third provide guidance to staff on what to report Clinical exclusion: a third do not require clinicians to report unexpected operational complications or
unexpected events Pick up rates: rates of reporting vary widely Definitions, procedures and volume of reporting at Regional level also vary widely, the most effective system being attributed to Northern and Yorkshire Regional Office which has operated a system since 1995. The purposes of these Regional systems were summarised as providing:
- an opportunity to make a corrective intervention - information to prevent similar occurrences in future - advice to Ministers of problems - early warning to government and press officers of imminent media reports.
Overall weaknesses in the UK NHS system (Table 4) were attributed in part to the instability of NHS policy (eg purchaser-provider split), the structure (regional offices) and, implicitly, the government in the early 1990s. Existing national reporting procedures for clinical incidents are summarised in Table 5. Table 4: NHS - weaknesses in current reporting systems, 2000 Definitions: no standardised operational definition of “adverse event” which could be easily
understood by all NHS staff Coverage: sophistication and priority among Trusts varies widely but largely excludes
primary care Regional variations: inconsistent approaches to reporting, monitoring and responding
among the eight regions Missed warnings: some serious injuries to patients, and nearly all potential incidents fail to
be detected by regional reporting systems Investigation: inconsistent use of internal and external mechanisms Learning: failure to use corporate experience to learn and teach across the NHS
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 12
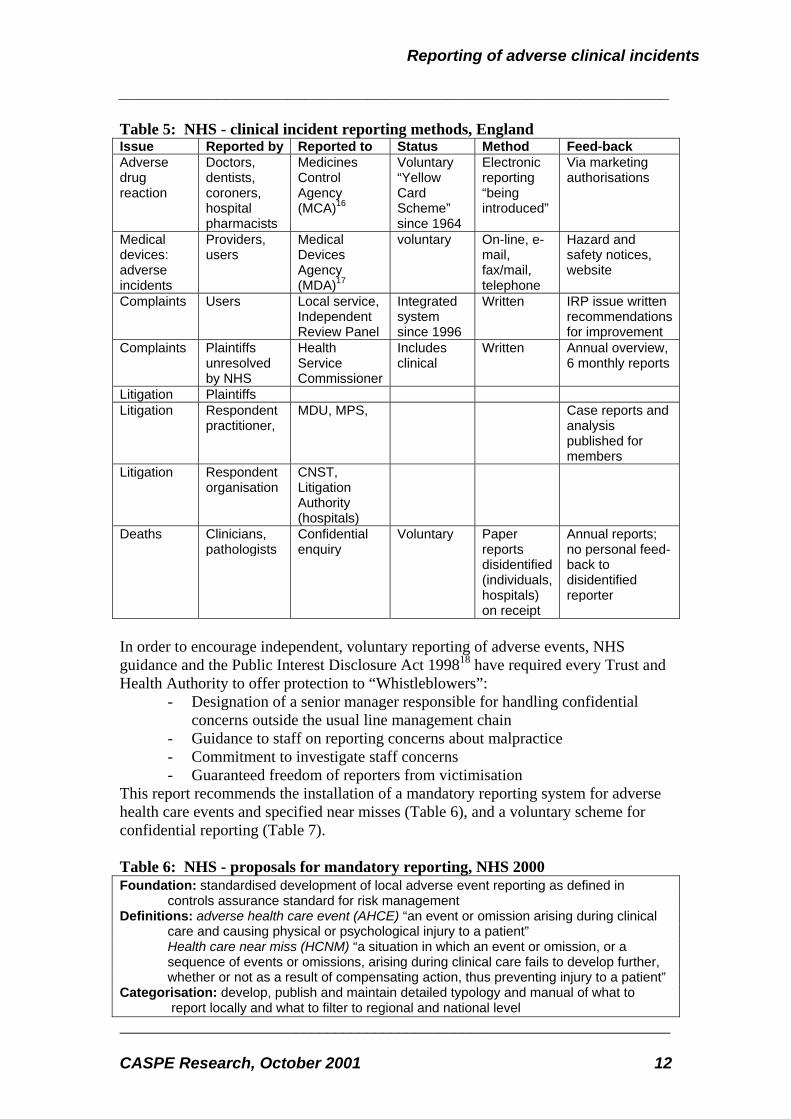
Table 5: NHS - clinical incident reporting methods, England Issue Reported by Reported to Status Method Feed-back Adverse drug reaction
Doctors, dentists, coroners, hospital pharmacists
Medicines Control Agency (MCA)16
Voluntary “Yellow Card Scheme” since 1964
Electronic reporting “being introduced”
Via marketing authorisations
Medical devices: adverse incidents
Providers, users
Medical Devices Agency (MDA)17
voluntary On-line, e-mail, fax/mail, telephone
Hazard and safety notices, website
Complaints Users Local service, Independent Review Panel
Integrated system since 1996
Written IRP issue written recommendations for improvement
Complaints Plaintiffs unresolved by NHS
Health Service Commissioner
Includes clinical
Written Annual overview, 6 monthly reports
Litigation Plaintiffs Litigation Respondent
practitioner, MDU, MPS, Case reports and
analysis published for members
Litigation Respondent organisation
CNST, Litigation Authority (hospitals)
Deaths Clinicians, pathologists
Confidential enquiry
Voluntary Paper reports disidentified (individuals, hospitals) on receipt
Annual reports; no personal feed-back to disidentified reporter
In order to encourage independent, voluntary reporting of adverse events, NHS guidance and the Public Interest Disclosure Act 199818 have required every Trust and Health Authority to offer protection to “Whistleblowers”:
- Designation of a senior manager responsible for handling confidential concerns outside the usual line management chain
- Guidance to staff on reporting concerns about malpractice - Commitment to investigate staff concerns - Guaranteed freedom of reporters from victimisation
This report recommends the installation of a mandatory reporting system for adverse health care events and specified near misses (Table 6), and a voluntary scheme for confidential reporting (Table 7). Table 6: NHS - proposals for mandatory reporting, NHS 2000 Foundation: standardised development of local adverse event reporting as defined in
controls assurance standard for risk management Definitions: adverse health care event (AHCE) “an event or omission arising during clinical
care and causing physical or psychological injury to a patient” Health care near miss (HCNM) “a situation in which an event or omission, or a
sequence of events or omissions, arising during clinical care fails to develop further, whether or not as a result of compensating action, thus preventing injury to a patient”
Categorisation: develop, publish and maintain detailed typology and manual of what to report locally and what to filter to regional and national level

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 13
Reporting medium: standard reporting software Reporting chain: defined channels and responsibility within and beyond local organisations Scope: all NHS health care delivery including primary care GPs and dentists, mandatory
reporting of deaths in general practice, and care provided to NHS patients in private hospitals and clinics; format and content of reports appropriate to required analysis
Status: mandatory for organisations and individuals Management: run by independent body perceived by health care staff to be neutral Table 7: NHS - proposals for voluntary reporting, NHS 2000 Foundation: direct, confidential (but not anonymous) reporting to regional or national level Publicity: practical information aimed at all NHS staff, contractors and their employees
(including independent sector) Function: follow up near misses, preserving anonymity of reporter whenever wished and
feasible, in exceptional circumstances when mandatory system not applied Probation: evaluation of whether voluntary reporting is either necessary or desirable adjunct
to mandatory system
‘Building a Safer NHS for Patients’19 This response by government to ‘An Organisation with a Memory’ places patient safety in the context of the NHS plan and linked it to other government initiatives. It re-iterated many of the previous messages and describes (page 42) the role of a National Patient Safety Agency (Table 8). Table 8: NHS -Functions of proposed National Patient Safety Agency Set and maintain standards and requirements for reporting, in conjunction with the DoH Collect, collate, categorise and code adverse event information from local NHS
organisations, other bodies providing care to NHS patients, directly from staff, and from patients and carers
Assimilate other safety-related information from existing reporting systems and other sources in the UK and abroad
Analyse information on adverse events and maintenance of a publicly available central repository of de-identified information for learning
Examine and track patterns and trends and act on their findings where risks are identified Provide feed-back to organisations and individuals, including issue of “patient safety
alerts” to improve safety and quality Produce solutions to reduce risk and prevent harm to future patients, and specify national
goals and targets Promote research on patient safety Promote a reporting culture in the NHS Collaborate with relevant bodies both nationally and internationally The Report enlarges on the characteristics of a mandatory reporting system described in ‘An Organisation with a Memory’ (Table 6), adding:
- accessibility: confidential, but open and accessible - values: generally blame-free - scope: simple to use but comprehensive in coverage and data collection
1.5 USA
American Medical Association (AMA) The AMA, similar to organisations in other countries, believes that health professionals and organisations should be encouraged to report and evaluate health
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 14
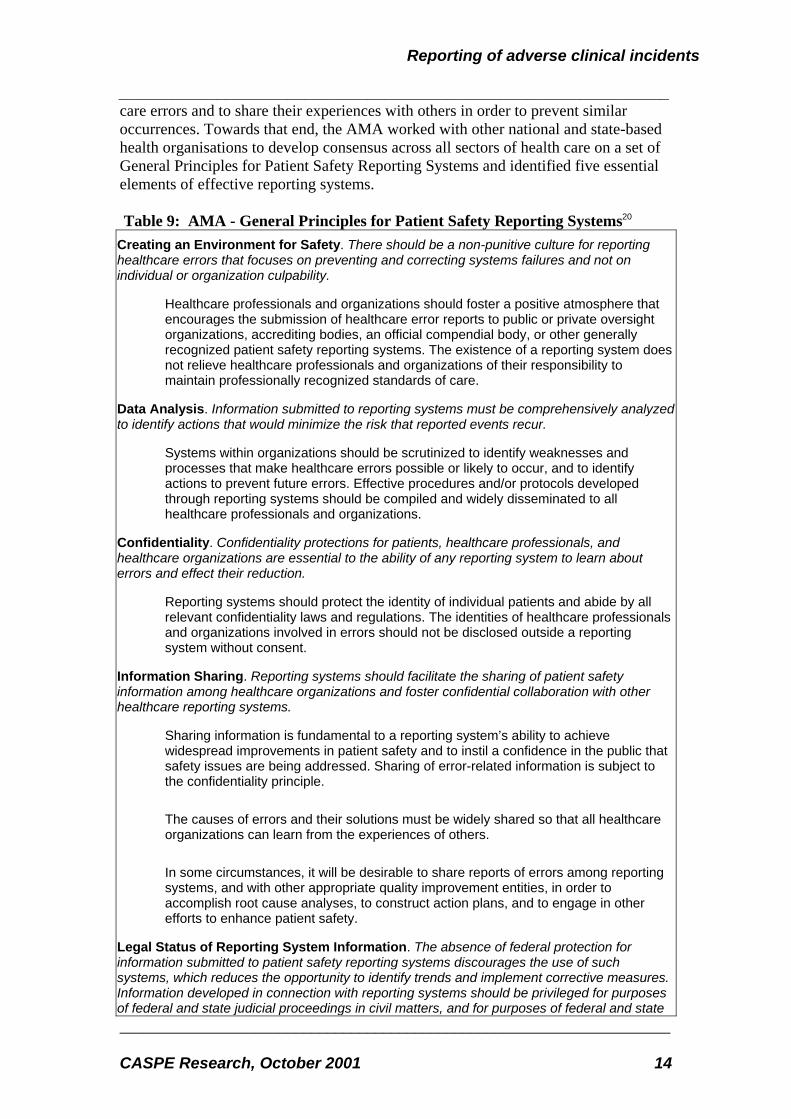
care errors and to share their experiences with others in order to prevent similar occurrences. Towards that end, the AMA worked with other national and state-based health organisations to develop consensus across all sectors of health care on a set of General Principles for Patient Safety Reporting Systems and identified five essential elements of effective reporting systems. Table 9: AMA - General Principles for Patient Safety Reporting Systems20 Creating an Environment for Safety. There should be a non-punitive culture for reporting healthcare errors that focuses on preventing and correcting systems failures and not on individual or organization culpability.
Healthcare professionals and organizations should foster a positive atmosphere that encourages the submission of healthcare error reports to public or private oversight organizations, accrediting bodies, an official compendial body, or other generally recognized patient safety reporting systems. The existence of a reporting system does not relieve healthcare professionals and organizations of their responsibility to maintain professionally recognized standards of care.
Data Analysis. Information submitted to reporting systems must be comprehensively analyzed to identify actions that would minimize the risk that reported events recur.
Systems within organizations should be scrutinized to identify weaknesses and processes that make healthcare errors possible or likely to occur, and to identify actions to prevent future errors. Effective procedures and/or protocols developed through reporting systems should be compiled and widely disseminated to all healthcare professionals and organizations.
Confidentiality. Confidentiality protections for patients, healthcare professionals, and healthcare organizations are essential to the ability of any reporting system to learn about errors and effect their reduction.
Reporting systems should protect the identity of individual patients and abide by all relevant confidentiality laws and regulations. The identities of healthcare professionals and organizations involved in errors should not be disclosed outside a reporting system without consent.
Information Sharing. Reporting systems should facilitate the sharing of patient safety information among healthcare organizations and foster confidential collaboration with other healthcare reporting systems.
Sharing information is fundamental to a reporting system’s ability to achieve widespread improvements in patient safety and to instil a confidence in the public that safety issues are being addressed. Sharing of error-related information is subject to the confidentiality principle.
The causes of errors and their solutions must be widely shared so that all healthcare organizations can learn from the experiences of others.
In some circumstances, it will be desirable to share reports of errors among reporting systems, and with other appropriate quality improvement entities, in order to accomplish root cause analyses, to construct action plans, and to engage in other efforts to enhance patient safety.
Legal Status of Reporting System Information. The absence of federal protection for information submitted to patient safety reporting systems discourages the use of such systems, which reduces the opportunity to identify trends and implement corrective measures. Information developed in connection with reporting systems should be privileged for purposes of federal and state judicial proceedings in civil matters, and for purposes of federal and state

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 15
administrative proceedings, including with respect to discovery, subpoenas, testimony, or any other form of disclosure.
Scope. The privilege for the information prepared for a reporting system should extend to any data, report, memorandum, analysis, statement, or other communication developed for the purposes of the system. This privilege should not interfere with the disclosure of information that is otherwise available, including the right of individuals to access their own medical records. No Waiver. The submission of healthcare error information to a reporting system, or the sharing of information by healthcare organizations or reporting systems with third parties in accordance with these principles, should not be construed as waiving this privilege or any other privilege under federal or state law that exists with respect to the information. Freedom of Information Act. Healthcare error information received by and from reporting systems should be exempt from the Freedom of Information Act and other similar state laws. Such an exemption is necessary to preserve the privilege discussed in this principle. Impact on State Law. A federal law is necessary to assure protection of information submitted to national reporting systems, but the federal protection should not pre-empt state evidentiary laws that provide greater protection than federal law. Providing such information to reporting systems should not constitute a waiver of any state law privilege.
Focusing specifically on product introduction in healthcare, the Association said that “Given the clinical importance of post-marketing surveillance, all healthcare providers (physicians, pharmacists, nurses, dentists, and others) should look upon adverse event reporting as part of their professional responsibility.” The American Medical Association[13] and American Dental Association[14] advocate (respectively) physician and dentist participation in adverse event reporting systems as an obligation.
Institute of Medicine (IoM) Towards a safer health system in the USA, the Institute of Medicine (IoM) recommended3 a nationwide mandatory reporting system for the standardised collection of information by state governments about adverse events that result in death or serious harm, beginning with hospitals but extending into other institutional and ambulatory care. Reportable events were to be narrowly defined for the system in view of the significant costs (including analysis and follow-up) to the health care providers and to the regulatory programmes. Costs could also be minimised by insisting on a standardised report format that would reduce the burden on reporters, and enable data aggregation, interpretation and communication. Recommendations to Congress are summarised in Table 10. Table 10: IoM recommendations for a national centre for patient safety:
Designate the public/private National Forum responsible for developing and maintaining a core set of reporting standards, including a nomenclature and taxonomy for reporting
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 16
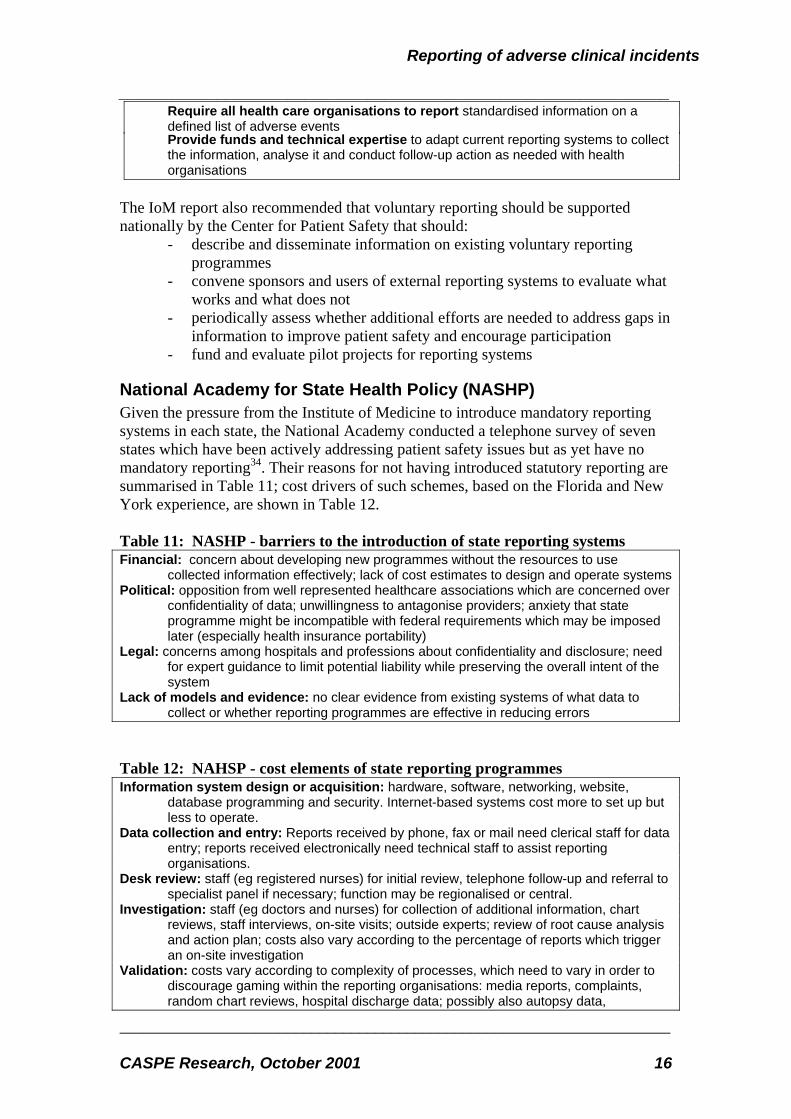
Require all health care organisations to report standardised information on a defined list of adverse events Provide funds and technical expertise to adapt current reporting systems to collect the information, analyse it and conduct follow-up action as needed with health organisations
The IoM report also recommended that voluntary reporting should be supported nationally by the Center for Patient Safety that should:
- describe and disseminate information on existing voluntary reporting programmes
- convene sponsors and users of external reporting systems to evaluate what works and what does not
- periodically assess whether additional efforts are needed to address gaps in information to improve patient safety and encourage participation
- fund and evaluate pilot projects for reporting systems
National Academy for State Health Policy (NASHP) Given the pressure from the Institute of Medicine to introduce mandatory reporting systems in each state, the National Academy conducted a telephone survey of seven states which have been actively addressing patient safety issues but as yet have no mandatory reporting34. Their reasons for not having introduced statutory reporting are summarised in Table 11; cost drivers of such schemes, based on the Florida and New York experience, are shown in Table 12. Table 11: NASHP - barriers to the introduction of state reporting systems Financial: concern about developing new programmes without the resources to use
collected information effectively; lack of cost estimates to design and operate systems Political: opposition from well represented healthcare associations which are concerned over
confidentiality of data; unwillingness to antagonise providers; anxiety that state programme might be incompatible with federal requirements which may be imposed later (especially health insurance portability)
Legal: concerns among hospitals and professions about confidentiality and disclosure; need for expert guidance to limit potential liability while preserving the overall intent of the system
Lack of models and evidence: no clear evidence from existing systems of what data to collect or whether reporting programmes are effective in reducing errors
Table 12: NAHSP - cost elements of state reporting programmes Information system design or acquisition: hardware, software, networking, website,
database programming and security. Internet-based systems cost more to set up but less to operate.
Data collection and entry: Reports received by phone, fax or mail need clerical staff for data entry; reports received electronically need technical staff to assist reporting organisations.
Desk review: staff (eg registered nurses) for initial review, telephone follow-up and referral to specialist panel if necessary; function may be regionalised or central.
Investigation: staff (eg doctors and nurses) for collection of additional information, chart reviews, staff interviews, on-site visits; outside experts; review of root cause analysis and action plan; costs also vary according to the percentage of reports which trigger an on-site investigation
Validation: costs vary according to complexity of processes, which need to vary in order to discourage gaming within the reporting organisations: media reports, complaints, random chart reviews, hospital discharge data; possibly also autopsy data,

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 17
malpractice actions; New York programme contracts validation and analysis function to SUNY School of Public Health
Analysis: costs of synthesising and trending information depend on purpose of programme (eg ad hoc reaction, or corporate learning from event patterns), amount of analysis, and feedback (frequency, breadth and method).
Training, information sharing, education: training for reporting facilities and programme staff; sharing of facility-specific and aggregated results for internal and external audiences; costs vary according to how this is provided (eg in-house or by commercial or voluntary agency) but are most affected by the simplicity and volume of the reporting system. A reporting coordinator is identified and trained within each facility (usually a member of the quality or risk management department).
Administration: overall management and enforcement; panels, advisory councils Another report from the NASHP summarised key questions for state administrations considering (Table 13), or already operating (Table 14), error reporting systems21. Table 13: NAHSP - Questions for developing reporting systems
What is the purpose and intended use of the system? How will you define “reportable” incident; what standards already exist? What specific data will be collected about the incidents/events? What types of facilities will be required to report? Of the reported data what will be confidential, and what will be disclosed, and to whom? What feedback will be provided to those who report? What incentives and sanctions exist to promote reporting?
Table 14: NAHSP - Questions for existing reporting systems
Does the (state) reporting program cross-reference and share information with other programs which may have similar information in order to develop more complete facility profiles? Do the medical facilities that are required to report know and understand what and how to report? Are there educational programmes to ensure that facilities can comply? Does whistleblower protection for reporters need to be developed or modified? How does the program ensure that corrective action plans are implemented? What kind of feedback is provided to reporters?
A five-page survey, based on previous frameworks including the IoM and JCAHO studies22, was sent in February 2000 to licensing and accreditation contacts in all 50 states (and the District of Columbia). This sought descriptions of current activities and any help needed to identify, track, report and respond to medical errors and adverse events23. Specific foci included legislative / regulatory requirements, uniformity / standardisation of data, protection from legal discovery, use of data and technical assistance needs. Eighteen states had mandatory reporting, but three of these were very limited. Of the remaining 15, most emphasis was on acute hospitals and ambulatory centres (Table 15), consistent with the observation that 48% of medical errors relate to surgical treatment. Reporting was protected by a range of means and at varying stages in the reporting chain (Table 16). Six of the 15 states were not sure whether their promises of confidentiality would withstand requests under the Freedom of Information Act. Encouragement for reporting was offered through assurance of confidentiality (60%) and training in reporting (47%), but only 3 states gave any feedback to reporters.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 18
Table 15: NAHSP - Scope of mandatory state reporting systems, USA 2000 Facility Number (of 15) PercentGeneral / acute care hospitals 15 100 Ambulatory care centres 13 87 Psychiatric hospitals 12 80 Outpatient mental health centres 4 27 Home health agencies 4 27 Individual practitioners 2 13 Laboratories 2 13 Pharmacies 0 0 Table 16: NAHSP - Protection of mandatory state reporting, USA 2000 Mechanism Number (of 15) Protected access to case reports 7 State promise of confidentiality 5 Data identified only by provider institution 4 All identification removed 3 Anonymous reporting 1 Table 17 overleaf outlines some Critical Success Factors that this survey identified as being important to those states participating in the survey. Table 17: NAHSP - Critical success factors perceived by states
Veterans Health Administration (VHA) The goals of the Patient Safety Improvement Program are “to prevent injuries to patients, visitors, and personnel, and to manage those injuries that do occur to

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 19
minimize the negative consequences to the injured individuals”. The key building blocks for accomplishing these goals are stated in Table 18. Table 18: VHA - elements of patient safety improvement programme Comprehensive identification and reporting of all adverse events, Sentinel Events,
and close calls (see Table 25). Reviewing adverse events, Sentinel Events, and close calls to identify underlying causes
and system changes needed to reduce the likelihood of recurrence (see paragraph 6). The determination of cause will be aimed at the system issues not directed at use as a punitive tool. The requirements for initiating a review will be determined by the priority scheme as defined by the Safety Assessment Code (Appendix SAC).
Disseminating patient safety alerts and lessons learned regarding effective system modifications throughout VHA (see paragraph 6) in an effective manner.
Prospective analysis of service delivery systems before an adverse event occurs to identify system redesigns that will reduce the likelihood of error.
The VHA emphasise (paragraph 5e) that staff who submit close call and adverse event reports will receive feedback on the actions being taken as a result of their report. It recommended that the feedback should be of a timely nature and come from the risk manager (or other appropriately designated party). Prompt feedback to reporters has been credited in other reporting systems with being one of the cornerstones that establishes trust in the system in that it demonstrates the seriousness and commitment on the part of the system to the importance of the reporting effort. The nature of this feedback can range from a simple acknowledgement that the event is under consideration, to providing information as to the corrective action that is planned or has been accomplished. The VA reporting to the Serious Events Register (SER) is exempt from legal liability; neither the VA nor the doctors (as government employees) can be sued by discovery through the SER. “The bottom line here is for the reporters to be made acutely aware that their effort of reporting was not just a paperwork drill.” VHA Report
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 20
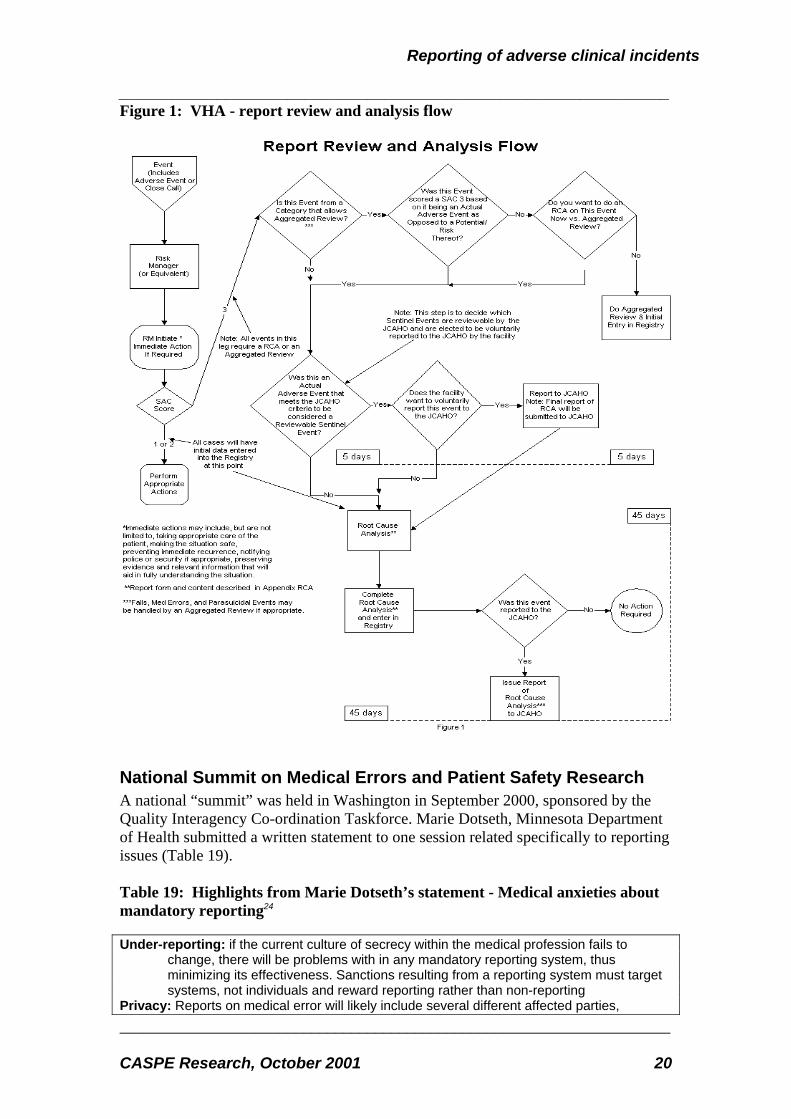
Figure 1: VHA - report review and analysis flow
National Summit on Medical Errors and Patient Safety Research A national “summit” was held in Washington in September 2000, sponsored by the Quality Interagency Co-ordination Taskforce. Marie Dotseth, Minnesota Department of Health submitted a written statement to one session related specifically to reporting issues (Table 19). Table 19: Highlights from Marie Dotseth’s statement - Medical anxieties about mandatory reporting24 Under-reporting: if the current culture of secrecy within the medical profession fails to
change, there will be problems with in any mandatory reporting system, thus minimizing its effectiveness. Sanctions resulting from a reporting system must target systems, not individuals and reward reporting rather than non-reporting
Privacy: Reports on medical error will likely include several different affected parties,

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 21
including the physician or healthcare provider, the patient, the hospital or other place of service, and the payer. Traditionally, information collected by the state or federal government has been accessible under freedom of information laws unless specifically protected. Many advocate the release of at least some portion of reported information to the public. With the variety of interests involved, it is a challenge to develop systems which protect information adequately while still releasing it in some useful form to the general public or providing helpful feedback to payers or providers for quality improvement purposes. Research on this point needs to address the best balance between public and private information within a reporting system in order to maximize the system's effectiveness.
Regulatory and reporting overlap: If and when reporting systems are established by states, it will be important to ensure that these systems are compatible with existing systems and with one another, and will not require multiple reporting in different formats for the federal and state government or for private accrediting organizations. Research needs to address how best to establish systems so providers and care givers are not forced to make duplicate filings to several regulatory oversight agencies or bodies. Consideration of the reporter's time will ensure a far higher level of compliance.
Cost: Setting up a mandatory reporting system will require a significant investment on the part of the state. The state of New York, which established the New York Patient Occurrence Reporting and Tracking System (NYPORTS) reporting system in 1998, reports that their Web-based system is run using existing staff, required an initial investment of $160,000 and needs $20,000 in maintenance per year. This investment is unusually low; most states will face a potential stumbling block in implementing a comprehensive reporting system while staying within tight budget restraints.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 22
2 Examples of established programmes
2.1 Health care
Australia: Wimmera Base Hospital A longitudinal survey25 of adverse in-patient events over eight years of progressive implementation of a risk management programme, screened 49,834 inpatient admissions by retrospective record review from 1991 to 1999 at a rural base hospital in the Wimmera region of Victoria. The latter two years included 20,050 Emergency Department attenders, and noted adverse events detected by critical incident reports (some of which had been sent to the National Patient Safety Foundation in Adelaide) and by reports from general practitioners, patients and coroners. Table 20: Wimmera - messages for reporting systems • Inpatient records screened for 8 outcome criteria (cf 18 in QAHCS, HMPS) • Emergency records screened for 5 outcome criteria • Record screening combined with incident reporting by hospital, GPs and patients • Five times more events were detected by record review than incident reports • Inpatient adverse events reduced from 1.35 to 0.74% over 8 years • Emergency Department events reduced from 3.26 to 0.48% over 2 years
Australian Incident Monitoring System (AIMS) Introduced in 1996, AIMS provides a mechanism for any incident or accident (actual or potential) in healthcare to be reported, using a single standard form. Incidents are then classified on corresponding software, using two unique classification systems developed by the Australian Patient Safety Foundation (APSF). The Foundation derives from an incident monitoring study in anaesthesia (AIMS-Anaesthesia) that began in 1988. In 1993, funding was received from the Australian Commonwealth Government to continue AIMS-Anaesthesia, and to set up pilot studies in other specialty areas. In 1994 the brief was broadened to develop an incident monitoring model that could be used on an institutional basis, rather than being specialty focused. A pilot study was conducted in six tertiary facilities in different Australian States. The current Australian Incident Monitoring System (AIMS) was set up following the national release of results from the Quality in Australian Health Care Study (QAHCS) in 1995. Since that time AIMS has been implemented in several Australian States, as well as individual health units.
Australian GP sentinel event study A 1993-95 study testing incident reporting in Australian general practice was published in 199726 and 199827. An incident was broadly defined as “an unintended event, no matter how seemingly trivial or commonplace, that could have harmed or
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 23
did harm a patient. The study involved 324 GPs who were members of the Australian Sentinel Practice Research Network, and were based in the Wentworth area of Sydney or were participants in the RACGP quality assurance programme. Reports were anonymous and were protected from subpoena under Commonwealth law28. They reported free-text descriptions of incidents and structured responses as to preventability, potential for harm, immediate consequences, predicted long-term outcomes, type of incident, contributing factors, mitigating factors and additional resource use. As the reports were anonymous, response rates could not be calculated but the study showed that:
- 214 of 510 GPs (42%) accepted the invitation to participate; a further 110 volunteered later
- 805 reports were received from 324 participants over 20 months - only 16% of respondents had less than 10 years’ experience, compared to a
national average of 30%
Sweden: National register of medical incidents Every health care provider in Sweden is obliged to report all adverse events (where a patient has been injured) or risk of them to the National Board of Health and Welfare (SoS). Reports are registered and classified in a national database and anonymised information bulletins are regularly circulated to all providers. But reporting levels are low, apparently largely because personnel involved are likely to be reported to the Medical Disciplinary Board (HSAN)29.
Switzerland: Anaesthesia-related mortality and incidents The Department of Anaesthesia at the University of Basle, Switzerland set up an anonymous critical incident reporting system (CIRS ) for anaesthetists in 1996 based on standard Internet technology and mounted on the local network30. It is protected from the Internet with a firewall that satisfies the strong legal requirements of the national data-security act but it can be reached from every networked computer in the hospital. The reporting system is completely electronic; the content of the detailed questionnaire (HTML-form) is automatically inserted into a central database (MS-ACCESS ). This database allows an easy compilation of the data and, with the help of a bulletin board, an anonymous discussion of each case is possible. CIRS is now in its third year and has recorded some 200 cases. Analysing 132 critical incidents showed that in 64% of the cases, human factors such as tiredness, haste, incorrect decision making and reduced situational awareness contributed to the incident. Adding the factor of problems in team performance, namely insufficient communication, increases the rate to 83%. On the other hand, human performance like experience, skills and situational awareness prevented 75% of the cases developing from an incident to an accident. Since the end of 1998, this system has offered a mechanism for a national incident survey in anaesthesiology in Switzerland (CIRS-CH) under the auspices of the national society of anaesthesiology (SGAR). This system, also running on the Internet (http://www.anaesthesie.ch/cirs/), is accessible only after an individual login procedure, so it cannot be accessed from outside. A national board of experts (from different regions of Switzerland and different types of hospital) maintains this system,
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 24
publishes the national results and acts as a facilitator for expert opinion on selected cases. This feedback on individual cases was regarded as most important for national success. It is worth noting that the analysis and comments on the events require at least as much expertise as is involved in their generation. The unprotected international version of CIRS is freely available on the Internet.
USA: Medication errors and adverse events Medication Error Reporting program (MER) This voluntary system for “frontline practitioners” (using telephone, mail, or Internet) was originated by the Institute for Safe Medication Practice in 1975 and is now administered by US Pharmacopoeia31. Information is shared with the FDA and any manufacturers concerned. About 3,000 reports have been received since 1993. MedMARx A voluntary medication error reporting programme, for subscriber hospitals only, was begun in1998; it is administered by US Pharmacopoeia (USP) and guided by the National Co-ordinating Council for Medication Error Reporting and Prevention. It is voluntary, Internet-based and anonymous, so staff can complete a standardised report, and managers can retrieve reports from their own and other participating hospitals. Data are not shared yet either with the FDA or JCAHO. MedWatch The Food and Drug Administration has implemented the MedWatch reporting system for serious adverse events associated with medical products.
USA: Emergency Care Research Institute (ECRI) ECRI32 , a non-profit health services research agency was established following a clinical accident in 1964 arising from an improperly maintained defibrillator. In seeking to address its mission of improving ‘the safety, quality and cost-effectiveness of healthcare’ it has focussed on healthcare technology, healthcare risk and quality management, healthcare environmental management. It collects information on medical devices incidents and hazards and uniformly codes such information using its proprietary Universal Medical Device Nomenclature System. ECRI is a WHO Collaborating Center providing support in the evaluation and dissemination of information about the safety, efficacy and performance of healthcare technology. The organisation offers a range of services to healthcare systems and facilities and has extended its role into management systems, such as credentialling.
USA: State-wide incident reporting systems At the time of the Institute of Medicine (IoM) report (1999), 18 to 23 of 50 states had mandatory reporting, but only 15 complied with the IoM criteria, and these related only to acute and general hospitals. Under-reporting was common, especially in the first years of operation. Several comparisons and analyses have identified wide variations in definitions, processes33, results and costs34 between states (Table 21, Table 22).

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 25
Table 21: Rosenthal - Comparison of State systems in Florida and New York Florida New York General and acute hospitals
273 260
Hospital beds 52,000 66,757 Reports (1999) 3,800 17,799 % on-site investigation 20 3 Staff wte 10 12 Method reporting Fax, registered post Internet with secure firewalls,
encrypted data Validation methods Cross-referencing with
discharge data, complaints, media enquiries, autopsy data, chart review, malpractice actions
Cross-referencing with discharge data, complaints, media enquiries
Hospitals fined for failure to report in 2000
7 3
Use, analysis of data • Screened for referral to professional board • facility-specific reports used by surveyors during scheduled on-site surveys
• Longitudinal web-based tracking and comparison with peer, regional and state facilities • Screened by regional council for referral to DOH • DOH issues advisories • facility-specific reports used by surveyors during scheduled on-site surveys • database shared with State University School of Public Health for analysis and production of annual report
Public reports Annual report lists most common injuries and associated operations Aggregated data on website
Hospital specific reporting Measures issued by state university
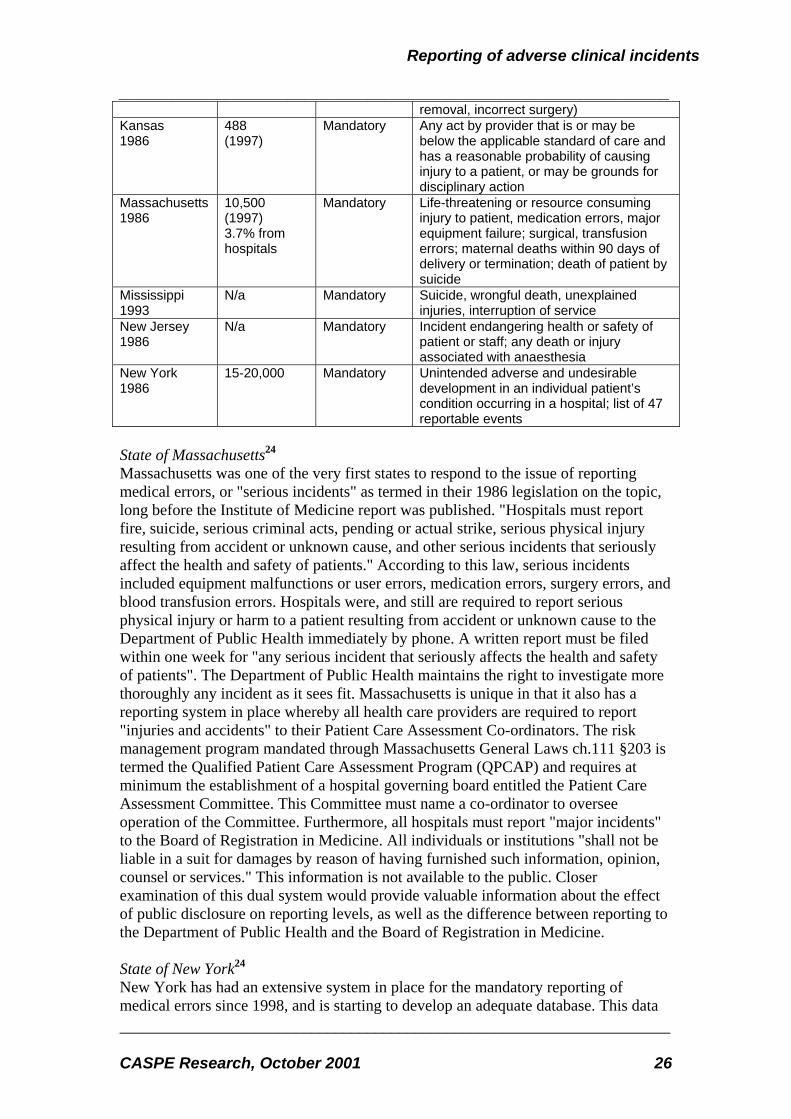
Website www.fdhc.state.fl.us http://www.health.state.ny.us/ Table 22: Institute of Medicine - Characteristics of some State reporting systems State, year begun
Reports/year Status Reportable events
California 1972
4,337 (1998)
Mandatory report within 24 hours
Catastrophes, communicable disease, assaults;
Colorado 1989
1,233 (1998)
Mandatory Unexplained deaths, CNS injuries, life-threatening complications of anaesthesia, transfusion, burns; abuse; equipment failure
Connecticut 1987
14,783 (1996)
Mandatory for nursing homes; voluntary for hospitals
All accidents or incidents that resulted in serious injury, death or disruption of facility services
Florida 1985
Approx 5,000 Mandatory Life-threatening situation, epidemic, serious adverse event (“code 15”) ie wrongful death, brain injury, wrong limb
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 26
removal, incorrect surgery) Kansas 1986
488 (1997)
Mandatory Any act by provider that is or may be below the applicable standard of care and has a reasonable probability of causing injury to a patient, or may be grounds for disciplinary action
Massachusetts 1986
10,500 (1997) 3.7% from hospitals
Mandatory Life-threatening or resource consuming injury to patient, medication errors, major equipment failure; surgical, transfusion errors; maternal deaths within 90 days of delivery or termination; death of patient by suicide
Mississippi 1993
N/a Mandatory Suicide, wrongful death, unexplained injuries, interruption of service
New Jersey 1986
N/a Mandatory Incident endangering health or safety of patient or staff; any death or injury associated with anaesthesia
New York 1986
15-20,000 Mandatory Unintended adverse and undesirable development in an individual patient’s condition occurring in a hospital; list of 47 reportable events
State of Massachusetts24 Massachusetts was one of the very first states to respond to the issue of reporting medical errors, or "serious incidents" as termed in their 1986 legislation on the topic, long before the Institute of Medicine report was published. "Hospitals must report fire, suicide, serious criminal acts, pending or actual strike, serious physical injury resulting from accident or unknown cause, and other serious incidents that seriously affect the health and safety of patients." According to this law, serious incidents included equipment malfunctions or user errors, medication errors, surgery errors, and blood transfusion errors. Hospitals were, and still are required to report serious physical injury or harm to a patient resulting from accident or unknown cause to the Department of Public Health immediately by phone. A written report must be filed within one week for "any serious incident that seriously affects the health and safety of patients". The Department of Public Health maintains the right to investigate more thoroughly any incident as it sees fit. Massachusetts is unique in that it also has a reporting system in place whereby all health care providers are required to report "injuries and accidents" to their Patient Care Assessment Co-ordinators. The risk management program mandated through Massachusetts General Laws ch.111 §203 is termed the Qualified Patient Care Assessment Program (QPCAP) and requires at minimum the establishment of a hospital governing board entitled the Patient Care Assessment Committee. This Committee must name a co-ordinator to oversee operation of the Committee. Furthermore, all hospitals must report "major incidents" to the Board of Registration in Medicine. All individuals or institutions "shall not be liable in a suit for damages by reason of having furnished such information, opinion, counsel or services." This information is not available to the public. Closer examination of this dual system would provide valuable information about the effect of public disclosure on reporting levels, as well as the difference between reporting to the Department of Public Health and the Board of Registration in Medicine. State of New York24 New York has had an extensive system in place for the mandatory reporting of medical errors since 1998, and is starting to develop an adequate database. This data
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 27
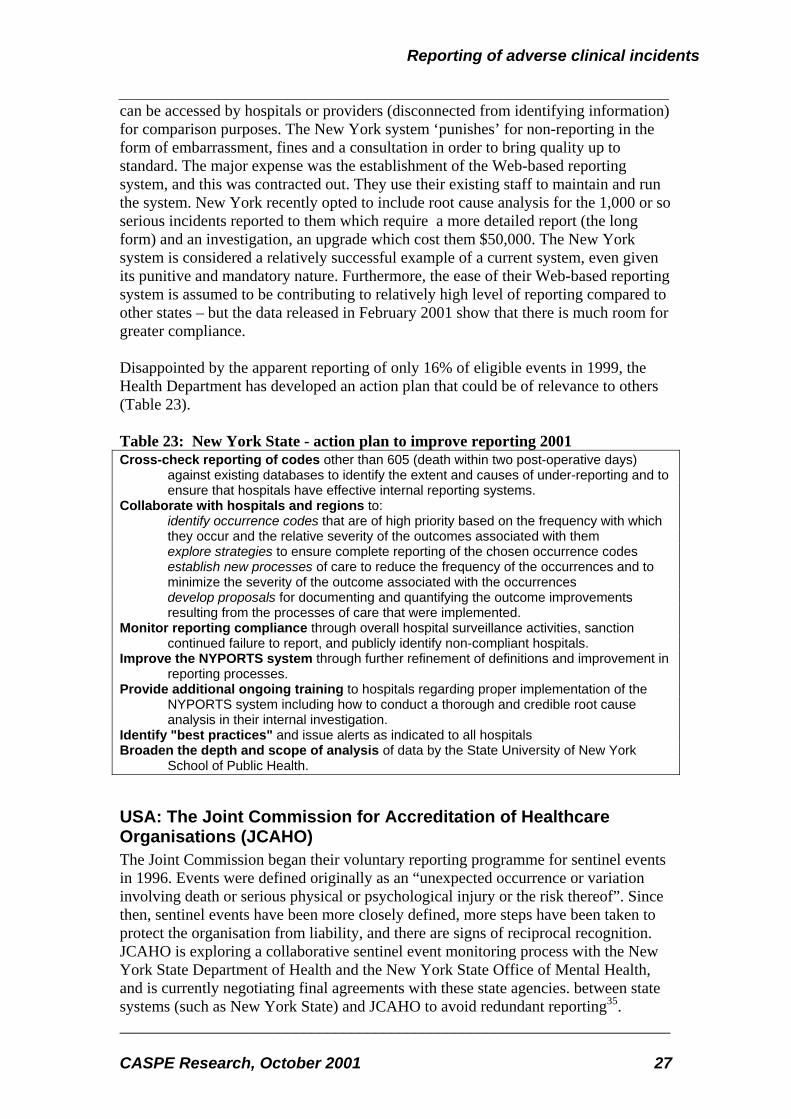
can be accessed by hospitals or providers (disconnected from identifying information) for comparison purposes. The New York system ‘punishes’ for non-reporting in the form of embarrassment, fines and a consultation in order to bring quality up to standard. The major expense was the establishment of the Web-based reporting system, and this was contracted out. They use their existing staff to maintain and run the system. New York recently opted to include root cause analysis for the 1,000 or so serious incidents reported to them which require a more detailed report (the long form) and an investigation, an upgrade which cost them $50,000. The New York system is considered a relatively successful example of a current system, even given its punitive and mandatory nature. Furthermore, the ease of their Web-based reporting system is assumed to be contributing to relatively high level of reporting compared to other states – but the data released in February 2001 show that there is much room for greater compliance. Disappointed by the apparent reporting of only 16% of eligible events in 1999, the Health Department has developed an action plan that could be of relevance to others (Table 23). Table 23: New York State - action plan to improve reporting 2001 Cross-check reporting of codes other than 605 (death within two post-operative days)
against existing databases to identify the extent and causes of under-reporting and to ensure that hospitals have effective internal reporting systems.
Collaborate with hospitals and regions to: identify occurrence codes that are of high priority based on the frequency with which they occur and the relative severity of the outcomes associated with them explore strategies to ensure complete reporting of the chosen occurrence codes establish new processes of care to reduce the frequency of the occurrences and to minimize the severity of the outcome associated with the occurrences develop proposals for documenting and quantifying the outcome improvements resulting from the processes of care that were implemented.
Monitor reporting compliance through overall hospital surveillance activities, sanction continued failure to report, and publicly identify non-compliant hospitals.
Improve the NYPORTS system through further refinement of definitions and improvement in reporting processes.
Provide additional ongoing training to hospitals regarding proper implementation of the NYPORTS system including how to conduct a thorough and credible root cause analysis in their internal investigation.
Identify "best practices" and issue alerts as indicated to all hospitals Broaden the depth and scope of analysis of data by the State University of New York
School of Public Health.
USA: The Joint Commission for Accreditation of Healthcare Organisations (JCAHO) The Joint Commission began their voluntary reporting programme for sentinel events in 1996. Events were defined originally as an “unexpected occurrence or variation involving death or serious physical or psychological injury or the risk thereof”. Since then, sentinel events have been more closely defined, more steps have been taken to protect the organisation from liability, and there are signs of reciprocal recognition. JCAHO is exploring a collaborative sentinel event monitoring process with the New York State Department of Health and the New York State Office of Mental Health, and is currently negotiating final agreements with these state agencies. between state systems (such as New York State) and JCAHO to avoid redundant reporting35.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 28
Largely through this voluntary self-reporting system, the Joint Commission has developed a database of serious adverse events and of the results of organisational analyses of these events. The lessons learnt are shared since 1998 with accredited organisations though the monthly Sentinel Event Alert. President of the Joint Commission, Denis O’Leary argues that mandatory reporting of these occurrences and related analyses would rapidly produce an even richer database, but without the guarantee of confidentiality for the analyses (which does not currently exist) the analyses would probably not be performed with the desired degree of thoroughness36. The Joint Commission has also recently introduced the requirement that each accredited organisation should establish reporting channels for unexpected adverse occurrences, perform an in depth analysis of each such occurrence, implement improvements, and assess the impact of the improvements on internal systems and
processes.
2.2 Other industries
Non-medical industries Schemes for reporting near misses, "close calls," or sentinel ("warning") events have been institutionalised in aviation, nuclear power technology, petrochemical processing, steel production, military operations, and air transportation.
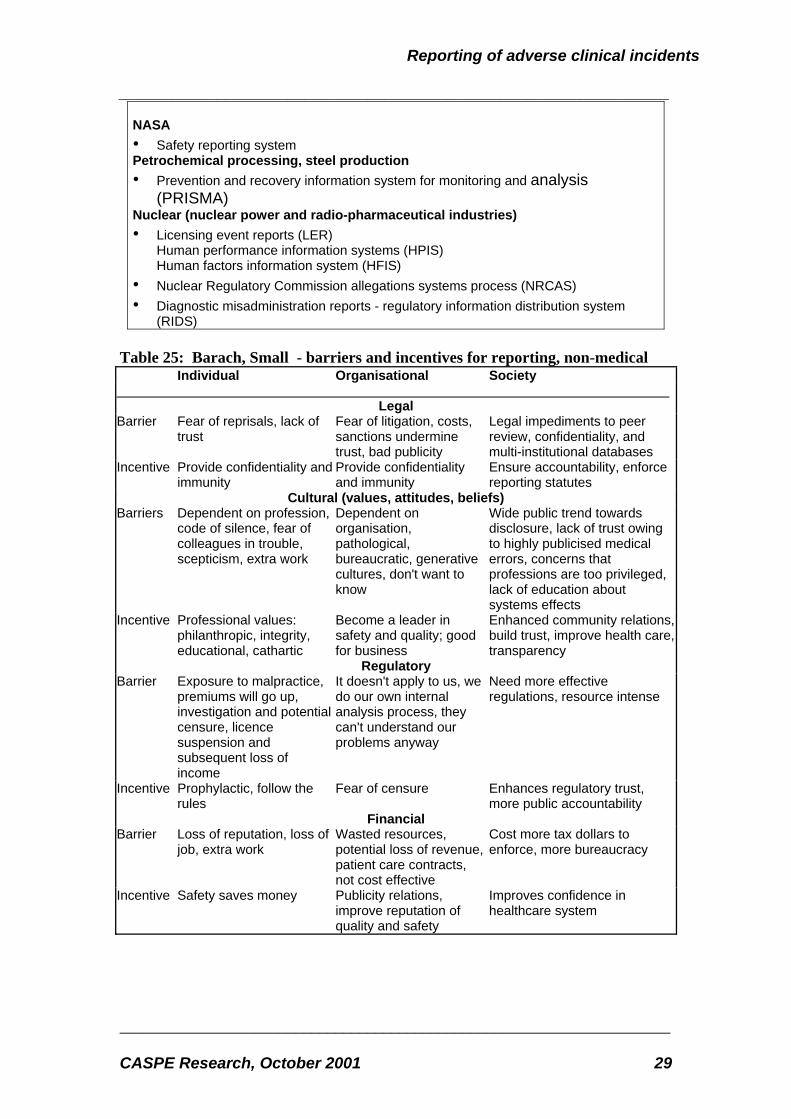
Reason identifies four critical elements of an effective safety culture - that is, a reporting, just, flexible, and learning culture. In order to assess whether this model could be validated in health care, Barach and Small studied incident reporting systems for near misses in non-medical domains37 (Table 23 and Appendix 1). They concluded that “barriers and incentives can be considered in terms of their impact on individuals, organisations, and society. Powerful disincentives to reporting depend on the organisational culture and include extra work, scepticism, lack of trust, fear of reprisals, and lack of effectiveness of present reporting systems. Incentives to reporting included, in addition to confidentiality, that incident reporting systems should be prophylactic (provide some degree of immunity), philanthropic (reporters identify with injured patients and other healthcare providers that could benefit from data), and therapeutic (reporters learn from reporting about adverse events). Incentives for society included accountability, transparency, enhanced community relations, and sustaining trust and confidence in the healthcare system” (Table 25). Table 23: Barach, Small - reporting systems for non-medical events
Aviation • Aviation safety reporting system (ASRS) • Aviation safety airways program (ASAP) • Air Altitude Awareness Program • Canadian aviation safety reporting system (CASRS) • British Airways safety information system (BASIS)
Air safety report (ASR) Confidential human factors reporting program (CHFRP) Special event search and master analysis (SESMA)
• Human factors failure analysis classification system (HFACS)
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 29
NASA • Safety reporting system Petrochemical processing, steel production • Prevention and recovery information system for monitoring and analysis
(PRISMA) Nuclear (nuclear power and radio-pharmaceutical industries) • Licensing event reports (LER)
Human performance information systems (HPIS) Human factors information system (HFIS)
• Nuclear Regulatory Commission allegations systems process (NRCAS) • Diagnostic misadministration reports - regulatory information distribution system
(RIDS) Table 25: Barach, Small - barriers and incentives for reporting, non-medical
Individual Organisational Society
Legal Barrier Fear of reprisals, lack of
trust Fear of litigation, costs, sanctions undermine trust, bad publicity
Legal impediments to peer review, confidentiality, and multi-institutional databases
Incentive Provide confidentiality and immunity
Provide confidentiality and immunity
Ensure accountability, enforce reporting statutes
Cultural (values, attitudes, beliefs) Barriers Dependent on profession,
code of silence, fear of colleagues in trouble, scepticism, extra work
Dependent on organisation, pathological, bureaucratic, generative cultures, don't want to know
Wide public trend towards disclosure, lack of trust owing to highly publicised medical errors, concerns that professions are too privileged, lack of education about systems effects
Incentive Professional values: philanthropic, integrity, educational, cathartic
Become a leader in safety and quality; good for business
Enhanced community relations, build trust, improve health care, transparency
Regulatory Barrier Exposure to malpractice,
premiums will go up, investigation and potential censure, licence suspension and subsequent loss of income
It doesn't apply to us, we do our own internal analysis process, they can't understand our problems anyway
Need more effective regulations, resource intense
Incentive Prophylactic, follow the rules
Fear of censure Enhances regulatory trust, more public accountability
Financial Barrier Loss of reputation, loss of
job, extra work Wasted resources, potential loss of revenue, patient care contracts, not cost effective
Cost more tax dollars to enforce, more bureaucracy
Incentive Safety saves money Publicity relations, improve reputation of quality and safety
Improves confidence in healthcare system

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 30
Aviation Safety Reporting System (ASRS) The National Transportation Safety Board (US) has an Accident/Incident Database, which applies only to data from mandatory reports on actual aviation accidents since 1967. Since 1976 aviation safety incidents (near misses) are voluntarily reported under the Aviation Safety Reporting System (ASRS), which is funded by the Federal Aviation Administration but administered by the National Aeronautics and Space Administration. The programme was transferred from the FAA to NASA because pilots were reluctant to report incidents (as opposed to accidents) to the regulatory body. The ASRS collects, analyses, and responds to voluntarily submitted aviation incident reports in order to lessen the likelihood of future accidents43. It issues alerts and advisories as required, but without having to refer back to the FAA, and it does not offer specific solutions to reporters as this would interfere with its role as “honest broker”. Some identified problems are thus not resolved, such as with call signs for which no one has yet found a permanent solution. The ASRS keeps a database of incidents, hazards and patterns and circulates a monthly bulletin to 85,000 readers and six-monthly reviews for specialist issues. It receives over 30,000 reports annually and has a budget of about $2 million
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 31
3 Evidence and practice
3.1 Policy
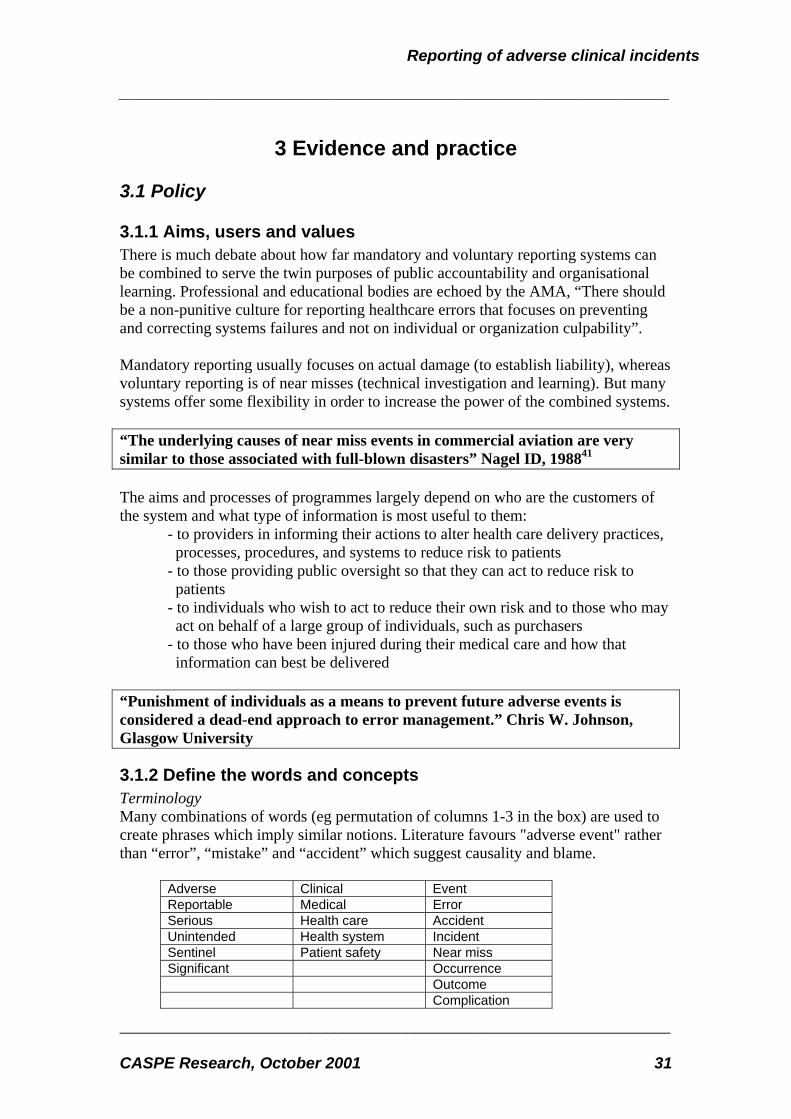
3.1.1 Aims, users and values There is much debate about how far mandatory and voluntary reporting systems can be combined to serve the twin purposes of public accountability and organisational learning. Professional and educational bodies are echoed by the AMA, “There should be a non-punitive culture for reporting healthcare errors that focuses on preventing and correcting systems failures and not on individual or organization culpability”. Mandatory reporting usually focuses on actual damage (to establish liability), whereas voluntary reporting is of near misses (technical investigation and learning). But many systems offer some flexibility in order to increase the power of the combined systems. “The underlying causes of near miss events in commercial aviation are very similar to those associated with full-blown disasters” Nagel ID, 198841 The aims and processes of programmes largely depend on who are the customers of the system and what type of information is most useful to them:
- to providers in informing their actions to alter health care delivery practices, processes, procedures, and systems to reduce risk to patients - to those providing public oversight so that they can act to reduce risk to patients - to individuals who wish to act to reduce their own risk and to those who may act on behalf of a large group of individuals, such as purchasers - to those who have been injured during their medical care and how that information can best be delivered
“Punishment of individuals as a means to prevent future adverse events is considered a dead-end approach to error management.” Chris W. Johnson, Glasgow University
3.1.2 Define the words and concepts Terminology Many combinations of words (eg permutation of columns 1-3 in the box) are used to create phrases which imply similar notions. Literature favours "adverse event" rather than “error”, “mistake” and “accident” which suggest causality and blame.
Adverse Clinical Event Reportable Medical Error Serious Health care Accident Unintended Health system Incident Sentinel Patient safety Near miss Significant Occurrence Outcome Complication
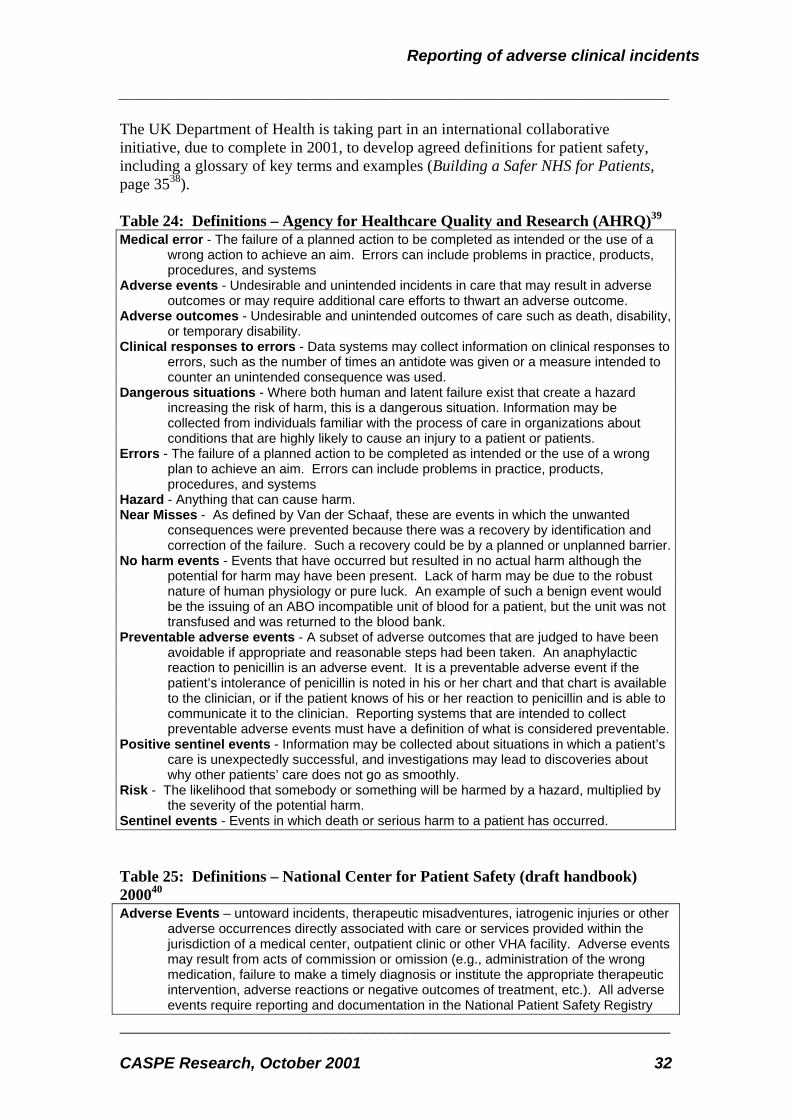
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 32
The UK Department of Health is taking part in an international collaborative initiative, due to complete in 2001, to develop agreed definitions for patient safety, including a glossary of key terms and examples (Building a Safer NHS for Patients, page 3538). Table 24: Definitions – Agency for Healthcare Quality and Research (AHRQ)39 Medical error - The failure of a planned action to be completed as intended or the use of a
wrong action to achieve an aim. Errors can include problems in practice, products, procedures, and systems
Adverse events - Undesirable and unintended incidents in care that may result in adverse outcomes or may require additional care efforts to thwart an adverse outcome.
Adverse outcomes - Undesirable and unintended outcomes of care such as death, disability, or temporary disability.
Clinical responses to errors - Data systems may collect information on clinical responses to errors, such as the number of times an antidote was given or a measure intended to counter an unintended consequence was used.
Dangerous situations - Where both human and latent failure exist that create a hazard increasing the risk of harm, this is a dangerous situation. Information may be collected from individuals familiar with the process of care in organizations about conditions that are highly likely to cause an injury to a patient or patients.
Errors - The failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim. Errors can include problems in practice, products, procedures, and systems
Hazard - Anything that can cause harm. Near Misses - As defined by Van der Schaaf, these are events in which the unwanted
consequences were prevented because there was a recovery by identification and correction of the failure. Such a recovery could be by a planned or unplanned barrier.
No harm events - Events that have occurred but resulted in no actual harm although the potential for harm may have been present. Lack of harm may be due to the robust nature of human physiology or pure luck. An example of such a benign event would be the issuing of an ABO incompatible unit of blood for a patient, but the unit was not transfused and was returned to the blood bank.
Preventable adverse events - A subset of adverse outcomes that are judged to have been avoidable if appropriate and reasonable steps had been taken. An anaphylactic reaction to penicillin is an adverse event. It is a preventable adverse event if the patient’s intolerance of penicillin is noted in his or her chart and that chart is available to the clinician, or if the patient knows of his or her reaction to penicillin and is able to communicate it to the clinician. Reporting systems that are intended to collect preventable adverse events must have a definition of what is considered preventable.
Positive sentinel events - Information may be collected about situations in which a patient’s care is unexpectedly successful, and investigations may lead to discoveries about why other patients’ care does not go as smoothly.
Risk - The likelihood that somebody or something will be harmed by a hazard, multiplied by the severity of the potential harm.
Sentinel events - Events in which death or serious harm to a patient has occurred. Table 25: Definitions – National Center for Patient Safety (draft handbook) 200040 Adverse Events – untoward incidents, therapeutic misadventures, iatrogenic injuries or other
adverse occurrences directly associated with care or services provided within the jurisdiction of a medical center, outpatient clinic or other VHA facility. Adverse events may result from acts of commission or omission (e.g., administration of the wrong medication, failure to make a timely diagnosis or institute the appropriate therapeutic intervention, adverse reactions or negative outcomes of treatment, etc.). All adverse events require reporting and documentation in the National Patient Safety Registry
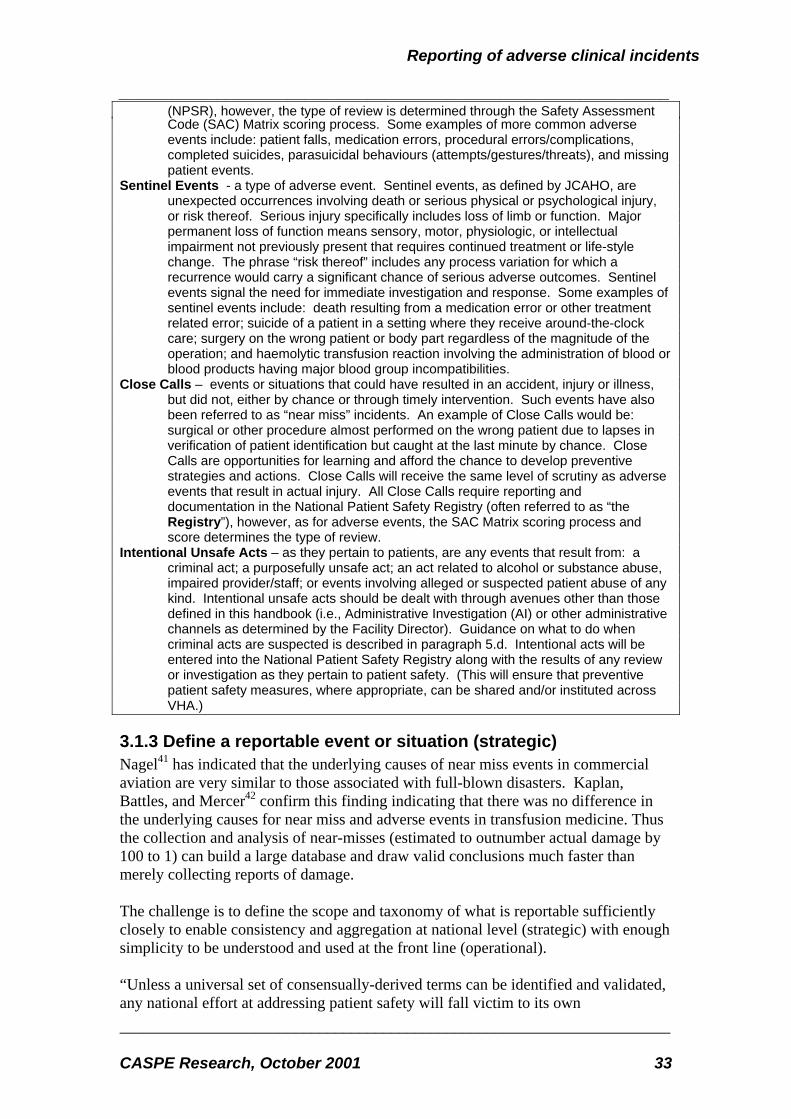
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 33
(NPSR), however, the type of review is determined through the Safety Assessment Code (SAC) Matrix scoring process. Some examples of more common adverse events include: patient falls, medication errors, procedural errors/complications, completed suicides, parasuicidal behaviours (attempts/gestures/threats), and missing patient events.
Sentinel Events - a type of adverse event. Sentinel events, as defined by JCAHO, are unexpected occurrences involving death or serious physical or psychological injury, or risk thereof. Serious injury specifically includes loss of limb or function. Major permanent loss of function means sensory, motor, physiologic, or intellectual impairment not previously present that requires continued treatment or life-style change. The phrase “risk thereof” includes any process variation for which a recurrence would carry a significant chance of serious adverse outcomes. Sentinel events signal the need for immediate investigation and response. Some examples of sentinel events include: death resulting from a medication error or other treatment related error; suicide of a patient in a setting where they receive around-the-clock care; surgery on the wrong patient or body part regardless of the magnitude of the operation; and haemolytic transfusion reaction involving the administration of blood or blood products having major blood group incompatibilities.
Close Calls – events or situations that could have resulted in an accident, injury or illness, but did not, either by chance or through timely intervention. Such events have also been referred to as “near miss” incidents. An example of Close Calls would be: surgical or other procedure almost performed on the wrong patient due to lapses in verification of patient identification but caught at the last minute by chance. Close Calls are opportunities for learning and afford the chance to develop preventive strategies and actions. Close Calls will receive the same level of scrutiny as adverse events that result in actual injury. All Close Calls require reporting and documentation in the National Patient Safety Registry (often referred to as “the Registry”), however, as for adverse events, the SAC Matrix scoring process and score determines the type of review.
Intentional Unsafe Acts – as they pertain to patients, are any events that result from: a criminal act; a purposefully unsafe act; an act related to alcohol or substance abuse, impaired provider/staff; or events involving alleged or suspected patient abuse of any
kind. Intentional unsafe acts should be dealt with through avenues other than those defined in this handbook (i.e., Administrative Investigation (AI) or other administrative channels as determined by the Facility Director). Guidance on what to do when criminal acts are suspected is described in paragraph 5.d. Intentional acts will be entered into the National Patient Safety Registry along with the results of any review or investigation as they pertain to patient safety. (This will ensure that preventive patient safety measures, where appropriate, can be shared and/or instituted across VHA.)
3.1.3 Define a reportable event or situation (strategic) Nagel41 has indicated that the underlying causes of near miss events in commercial aviation are very similar to those associated with full-blown disasters. Kaplan, Battles, and Mercer42 confirm this finding indicating that there was no difference in the underlying causes for near miss and adverse events in transfusion medicine. Thus the collection and analysis of near-misses (estimated to outnumber actual damage by 100 to 1) can build a large database and draw valid conclusions much faster than merely collecting reports of damage. The challenge is to define the scope and taxonomy of what is reportable sufficiently closely to enable consistency and aggregation at national level (strategic) with enough simplicity to be understood and used at the front line (operational). “Unless a universal set of consensually-derived terms can be identified and validated, any national effort at addressing patient safety will fall victim to its own

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 34
inconsistencies. Trending, comparisons, and interpretation can only be done when all information is collected in the same way, using the same criteria, and in a manner that is accessible to and understandable by all the groups who need to participate in the data collection and interpretation process.”43 “Lack of a clear definition has been one of the general challenges in the discussion around medical error to date. In addition, the use of the term “error” has caused some concern within the medical and health care profession, which by and large prefers the term “patient safety”. The lack of a clear definition of medical error has seriously complicated attempts by states, as well as private accrediting bodies such as the Joint Commission on Health Care Accreditation, to gather data on these events.”44 “The lack of a clear definition for reportable events might constitute the single largest challenge to instituting an effective reporting system at the state level.” Marie Dotseth, USA JCAHO defines a “sentinel event” as “any unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof”45 The IoM report defines medical error as “ failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim” based on literature within behavioural sciences. The NASHP report did not give a single definition for “medical error”, nor did any of the 50 states studied, but two defined an “adverse event” and most relied upon listing types of events which should be reported. Vincent suggests that significant medical errors can be defined as resulting in “prolonged hospital admission or in-patient injury”46. This is restrictive but makes enumeration easier by narrowing the field. But restrictive definitions are less appropriate in primary care. Sheikh and Hurwitz define significant clinical error as, “a clinical encounter that results in, or has the potential to result in unintentional and unexpected patient harm”47. This widens the definition and is more applicable to primary care where 70% of doctor-patient encounters take place. Table 28: Definition of reportable (“sentinel”) event – JCAHO48 The following criteria define the subset of sentinel events that are voluntarily reportable, at the facility’s discretion to the Joint Commission. Only those sentinel events that affect recipients of care (patients, clients, and residents) and that meet the following criteria fall into this category: 1. The event has resulted in an unanticipated death or major permanent loss of function, not related to the natural course of the patient's illness or underlying condition, 1,2 or 2. The event is one of the following (even if the outcome was not death or major permanent loss of function): a. Suicide of a patient in a setting where the patient receives around-the-clock care (e.g., hospital, residential treatment center, crisis stabilization center).
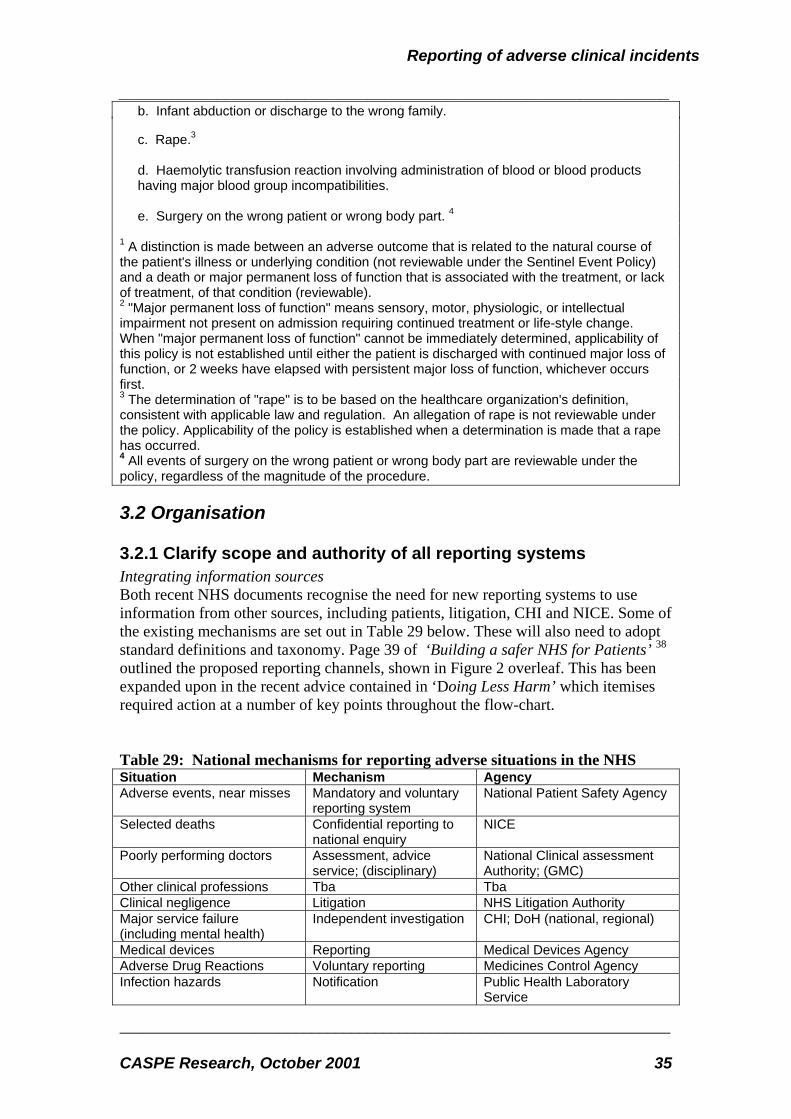
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 35
b. Infant abduction or discharge to the wrong family. c. Rape.3 d. Haemolytic transfusion reaction involving administration of blood or blood products having major blood group incompatibilities. e. Surgery on the wrong patient or wrong body part. 4 1 A distinction is made between an adverse outcome that is related to the natural course of the patient's illness or underlying condition (not reviewable under the Sentinel Event Policy) and a death or major permanent loss of function that is associated with the treatment, or lack of treatment, of that condition (reviewable). 2 "Major permanent loss of function" means sensory, motor, physiologic, or intellectual impairment not present on admission requiring continued treatment or life-style change. When "major permanent loss of function" cannot be immediately determined, applicability of this policy is not established until either the patient is discharged with continued major loss of function, or 2 weeks have elapsed with persistent major loss of function, whichever occurs first. 3 The determination of "rape" is to be based on the healthcare organization's definition, consistent with applicable law and regulation. An allegation of rape is not reviewable under the policy. Applicability of the policy is established when a determination is made that a rape has occurred. 4 All events of surgery on the wrong patient or wrong body part are reviewable under the policy, regardless of the magnitude of the procedure.
3.2 Organisation
3.2.1 Clarify scope and authority of all reporting systems Integrating information sources Both recent NHS documents recognise the need for new reporting systems to use information from other sources, including patients, litigation, CHI and NICE. Some of the existing mechanisms are set out in Table 29 below. These will also need to adopt standard definitions and taxonomy. Page 39 of ‘Building a safer NHS for Patients’ 38 outlined the proposed reporting channels, shown in Figure 2 overleaf. This has been expanded upon in the recent advice contained in ‘Doing Less Harm’ which itemises required action at a number of key points throughout the flow-chart. Table 29: National mechanisms for reporting adverse situations in the NHS Situation Mechanism Agency Adverse events, near misses Mandatory and voluntary
reporting system National Patient Safety Agency
Selected deaths Confidential reporting to national enquiry
NICE
Poorly performing doctors Assessment, advice service; (disciplinary)
National Clinical assessment Authority; (GMC)
Other clinical professions Tba Tba Clinical negligence Litigation NHS Litigation Authority Major service failure (including mental health)
Independent investigation CHI; DoH (national, regional)
Medical devices Reporting Medical Devices Agency Adverse Drug Reactions Voluntary reporting Medicines Control Agency Infection hazards Notification Public Health Laboratory
Service

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 36
Mental health incident Notification Mental Health Act Commission Injuries, diseases, dangerous occurrences
Statutory (1995) reporting Health & Safety Executive
Service failure harming many patients
Public inquiry Secretary of State
Complaints NHS procedure; (appeal) Local NHS; (Ombudsman) Staff concerns national reporting system;
(whistle-blowing) NPSA; (NHS)
Transfusion hazards Reporting to SHOT49 Independent Figure 2: Proposed national reporting system, UK NHS 2001
3.2.2 Allocate individual and corporate responsibilities Co-ordination In the USA, three accreditation/standard setting organisations – AMA, JCAHO, NCQA – have formed a Performance Measures Co-ordinating Council (PMCC) to harmonise measurements of process and outcome, including errors. Also in the USA, the newly-formed National Quality Forum is a public-private partnership set up to develop and implement a national strategy for health care quality measurement and reporting. It emerged from a national review that pointed out the need for government to recognise and integrate the contributions of many non-governmental interests towards quality improvement50. Learning centre The IoM report recommended that Congress should design a mechanism to describe, develop, co-ordinate and disseminate information on existing programmes of
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 37
voluntary reporting. This should involve sponsors and users of external reporting systems (including independent data providers, accreditation programmes and professional bodies) in the evaluation of what works and what does not, and the periodic assessment of whether additional efforts are needed to address gaps in information to improve patient safety and encourage participation. Evaluation The IoM report (page 103) recommended that Congress should identify an independent mechanism to evaluate the reporting systems (page 58), both voluntary and mandatory, equivalent to the Center for Patient Safety. Standards and methodology The IoM report also recommended that Congress identify a national agency to standardise definitions (nomenclature and taxonomy), reporting standards, methods and formats of reporting. This should include the various stakeholders and be supported by relevant expertise, funding and authority. The National Forum for Health Care Quality Measurement and Reporting was proposed for this role. Role of provider organisations There is a need to define what is expected of primary51, community and hospital services. Although, in the USA, state regulators also receive reports from hospitals and ambulatory clinics it is nursing homes that demand the most attention. In Connecticut in 1996, 93% of nearly 15,000 reports were from nursing homes. Role of individuals Identify, train and monitor reporting co-ordinators within each health care facility. The NHS has taken on some of these recommendations. ’Building a safer NHS for patients’ describes a new National Patient Safety Agency (NPSA) designed to: Collect and analyse information on adverse events from local NHS organisations, staff,
patients and carers Assimilate other safety-related information from existing reporting systems and other
sources in the UK and abroad Learn lessons and feed them back into practice, service organisation and delivery Where risks are identified, produce solutions to prevent harm, specify national goals Establish mechanisms to track progress while ‘Organisation with a Memory’ proposes co-ordination with parallel agencies, recommending: Single focus within the NHS Executive be identified as responsible for prioritising and
supporting actions arising from learning from adverse events(page 85) Litigation Authority should have a stronger educational remit with educational bodies
and medical defence organisations to publicise high-risk areas and risk reduction activities among managers and clinicians(page 86)
NICE co-ordinate the development and piloting of standard procedure manuals and safety bulletins relating to specific high-risk procedures
MDA actively seek design solutions to reduce identified hazards

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 38
3.2.3 Design system Development process Since 1985, a mandatory incident reporting system has been in place in New York State. This was initially a paper reporting system; later, an email-based system was developed. Neither of these systems allowed feedback to the hospitals which limited the use of the data for quality improvement. NYPORTS was created to simplify reporting, streamline the coding, co-ordinate with other reporting systems to reduce duplication, and allow hospitals to obtain feedback on their own reporting patterns and compare themselves with other facilities in the region and the State. The development of the electronic internet-based system began in 1995, utilizing a state-wide workgroup of industry experts and a consumer representative. The workgroup included a practising surgeon, a practising anaesthesiologist, facility medical directors, internal medicine practitioners, nursing, quality assurance, and risk management professionals. The chair was the chief quality officer at an academic medical center. The health department participated on the group and provided the necessary support to carry out development and implementation activities. The state-wide hospital association and its regional affiliates also participated in development and implementation in support of the group’s activities. The resulting system was based on objective criteria and information and provides hospitals with clear definitions of what must be reported. It was extensively field tested and refined and was implemented across the state in April 1998. The new system made it easier for hospitals to report adverse incidents, as required by law, and to obtain comparative data. During the development of the system, there were three in-depth field tests. For each phase of testing, feedback and input from facilities involved was incorporated, further improving the system. System features
Data collection: Continuous/intermittent v. generic/specialty The IoM considered that a single national, generic mandatory reporting system would not be feasible in the USA. They recommended that Congress should instead (page 105) encourage and support voluntary reporting schemes (generic and specialist), and make better use of their findings by linkage and development eg universal national systems, mini-systems eg medication errors, and rotational sampling of particular reporting mechanisms. The NHS plans to introduce a single overall system for analysing and disseminating lessons from adverse health care events and near misses (‘Organisation with a Memory’ page 83, recommendation 4).
Active v. passive systems Many systems are considered “passive” in that they rely on a report being submitted by someone who has observed the event. “Active” systems work with participating health care organisations to collect complete data on an issue being tracked to determine rates of an adverse event. They use routine data to screen for reportable events and re-enforce the reporting process. See 3.3.1 Case recognition.
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 39
Department-based v. chain-based reporting Most systems for reporting and analysing medical incidents are based on and restricted to single, discrete, often uni-disciplinary hospital departments. Patients, and patient-related products such as blood or medications, flow through a series of departments within and external to the hospital during their treatment. Experience in the Netherlands, analysed at the University of Eindhoven suggested that 15-30% of the causes of incidents in a single department may be imported from others, located earlier in the “chain”52.
Data-driven v. action-driven reporting Arthur and Wynn warn against early concentration on gathering large volumes of data rather than the capacity to convert them into practical analysis and effective action. “As a system matures, its associated data usually becomes cumbersome, particularly if clarification processes are needed. It is at this point that the focus shifts to some form of risk based data handling model, however basic. We suggest that risk based modelling approaches should be used from the outset53.
“Does one begin with a simple expedient system to capture errors and deal with the complexity problems of the data later, or does one begin with a complex system and refine through controlled validation?” John Arthur, Henry Wynn, Warwick University
Data-driven: Incidents may simply lead to a data collection exercise. No directed action per se occurs, but strategic level planning is greatly informed. Ideally this approach should address a concrete issue i.e. potential users are clearly identified and designed into the information form. The use of strategic level data can sometimes be to compare centres or units under study on ‘raw contours’. This kind of broad-brush, multipurpose, data-collection has an important advantage in inclusiveness. It potentially captures the full nature of the process, if there is time to make use of the data. It is essentially a data mining approach: collect large volumes of data for several reasons and use part of it to assess or detect incidents. Examples abound: such as credit analysis by banks, trying to detect telephone fraud from telephone use data, detecting computer hacking from computer-use data or tracing cause of failure in automobiles from warranty data. Action-driven: In this case the aim is only to collect data specifically related to the error reduction actions to be taken as part of the intelligent monitoring highlighted above. Feedback is an essential element in this type of system. Typically this model has discrete well-defined user groups.
Criteria and components of reporting systems A prototype reporting system designed for transfusion medicine may serve as a model in other medical domains54. Three blood centres and three transfusion services collaborated with experts from aviation safety, nuclear power, cognitive psychology, industrial engineering, artificial intelligence, education and training. Using the Delphi and nominal group techniques to establish ideal design parameters and functions, they defined four key requirements for the reporting system (Table 30), which can be compared with conclusions reached by Barach and Small in relation to non-medical
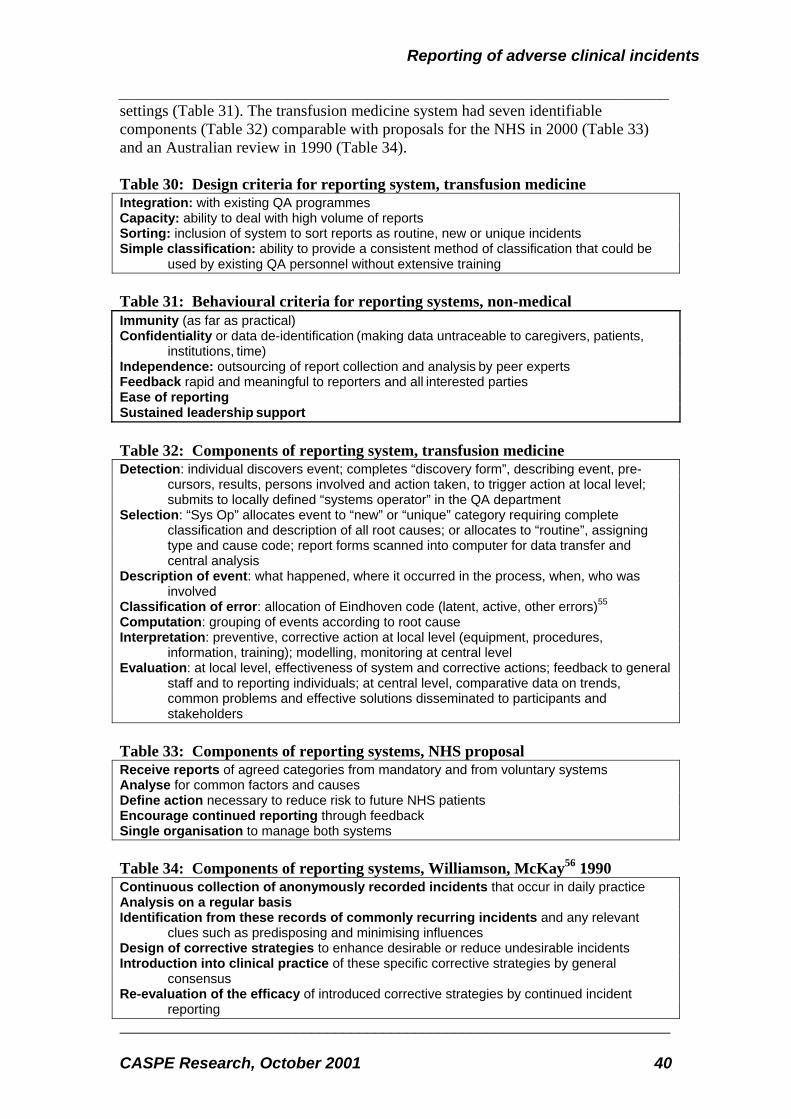
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 40
settings (Table 31). The transfusion medicine system had seven identifiable components (Table 32) comparable with proposals for the NHS in 2000 (Table 33) and an Australian review in 1990 (Table 34). Table 30: Design criteria for reporting system, transfusion medicine Integration: with existing QA programmes Capacity: ability to deal with high volume of reports Sorting: inclusion of system to sort reports as routine, new or unique incidents Simple classification: ability to provide a consistent method of classification that could be
used by existing QA personnel without extensive training Table 31: Behavioural criteria for reporting systems, non-medical Immunity (as far as practical) Confidentiality or data de-identification (making data untraceable to caregivers, patients,
institutions, time) Independence: outsourcing of report collection and analysis by peer experts Feedback rapid and meaningful to reporters and all interested parties Ease of reporting Sustained leadership support Table 32: Components of reporting system, transfusion medicine Detection: individual discovers event; completes “discovery form”, describing event, pre-
cursors, results, persons involved and action taken, to trigger action at local level; submits to locally defined “systems operator” in the QA department
Selection: “Sys Op” allocates event to “new” or “unique” category requiring complete classification and description of all root causes; or allocates to “routine”, assigning type and cause code; report forms scanned into computer for data transfer and central analysis
Description of event: what happened, where it occurred in the process, when, who was involved
Classification of error: allocation of Eindhoven code (latent, active, other errors)55 Computation: grouping of events according to root cause Interpretation: preventive, corrective action at local level (equipment, procedures,
information, training); modelling, monitoring at central level Evaluation: at local level, effectiveness of system and corrective actions; feedback to general
staff and to reporting individuals; at central level, comparative data on trends, common problems and effective solutions disseminated to participants and stakeholders
Table 33: Components of reporting systems, NHS proposal Receive reports of agreed categories from mandatory and from voluntary systems Analyse for common factors and causes Define action necessary to reduce risk to future NHS patients Encourage continued reporting through feedback Single organisation to manage both systems Table 34: Components of reporting systems, Williamson, McKay56 1990 Continuous collection of anonymously recorded incidents that occur in daily practice Analysis on a regular basis Identification from these records of commonly recurring incidents and any relevant
clues such as predisposing and minimising influences Design of corrective strategies to enhance desirable or reduce undesirable incidents Introduction into clinical practice of these specific corrective strategies by general
consensus Re-evaluation of the efficacy of introduced corrective strategies by continued incident
reporting
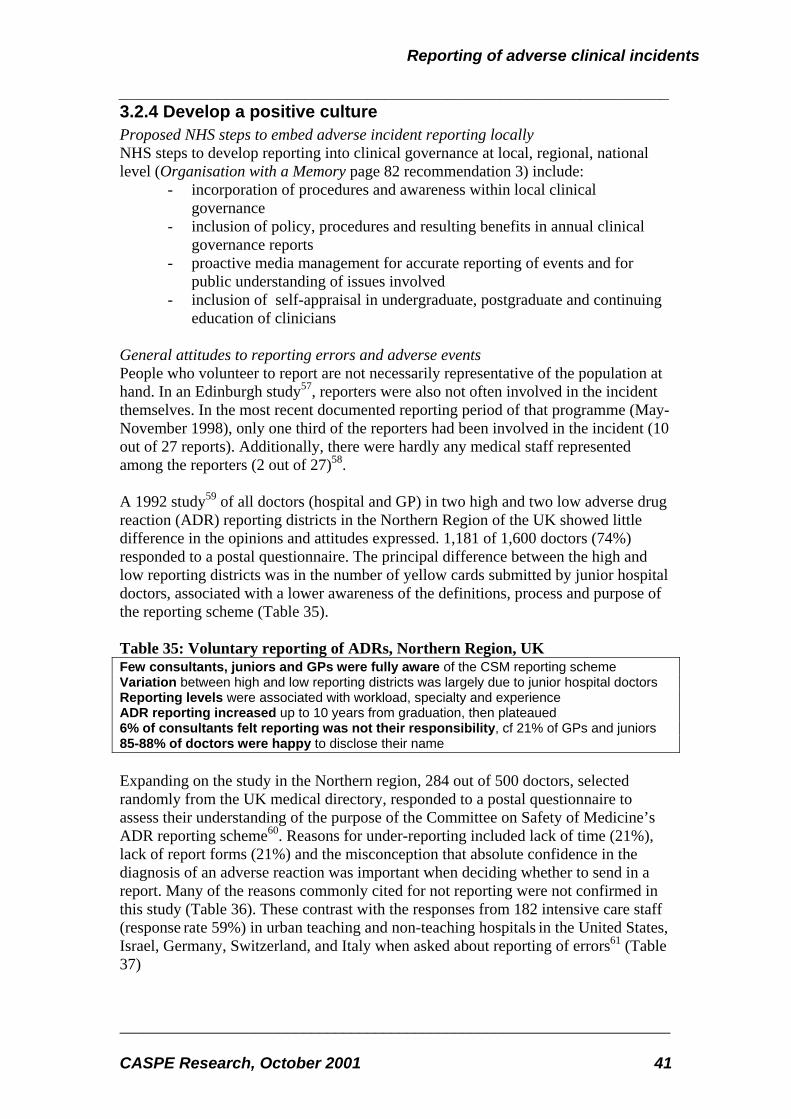
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 41
3.2.4 Develop a positive culture Proposed NHS steps to embed adverse incident reporting locally NHS steps to develop reporting into clinical governance at local, regional, national level (Organisation with a Memory page 82 recommendation 3) include:
- incorporation of procedures and awareness within local clinical governance
- inclusion of policy, procedures and resulting benefits in annual clinical governance reports
- proactive media management for accurate reporting of events and for public understanding of issues involved
- inclusion of self-appraisal in undergraduate, postgraduate and continuing education of clinicians
General attitudes to reporting errors and adverse events People who volunteer to report are not necessarily representative of the population at hand. In an Edinburgh study57, reporters were also not often involved in the incident themselves. In the most recent documented reporting period of that programme (May-November 1998), only one third of the reporters had been involved in the incident (10 out of 27 reports). Additionally, there were hardly any medical staff represented among the reporters (2 out of 27)58. A 1992 study59 of all doctors (hospital and GP) in two high and two low adverse drug reaction (ADR) reporting districts in the Northern Region of the UK showed little difference in the opinions and attitudes expressed. 1,181 of 1,600 doctors (74%) responded to a postal questionnaire. The principal difference between the high and low reporting districts was in the number of yellow cards submitted by junior hospital doctors, associated with a lower awareness of the definitions, process and purpose of the reporting scheme (Table 35). Table 35: Voluntary reporting of ADRs, Northern Region, UK Few consultants, juniors and GPs were fully aware of the CSM reporting scheme Variation between high and low reporting districts was largely due to junior hospital doctors Reporting levels were associated with workload, specialty and experience ADR reporting increased up to 10 years from graduation, then plateaued 6% of consultants felt reporting was not their responsibility, cf 21% of GPs and juniors 85-88% of doctors were happy to disclose their name Expanding on the study in the Northern region, 284 out of 500 doctors, selected randomly from the UK medical directory, responded to a postal questionnaire to assess their understanding of the purpose of the Committee on Safety of Medicine’s ADR reporting scheme60. Reasons for under-reporting included lack of time (21%), lack of report forms (21%) and the misconception that absolute confidence in the diagnosis of an adverse reaction was important when deciding whether to send in a report. Many of the reasons commonly cited for not reporting were not confirmed in this study (Table 36). These contrast with the responses from 182 intensive care staff (response rate 59%) in urban teaching and non-teaching hospitals in the United States, Israel, Germany, Switzerland, and Italy when asked about reporting of errors61 (Table 37)

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 42
Table 36: Factors rarely claimed to discourage ADR reporting, UK 1993 Doctor’s anxiety n=284 Percent “yes” Dislike reporting confidential information 3 Unsure how to report ADR 3 May appear foolish 8 May be exposed to legal liability 1 Reluctant to admit may have caused patient harm 5 Would rather collect and publish personally 1 Believe that only safe drugs are marketed 5 Table 37: Factors claimed to discourage error reporting, ITU, various countries, 1997-99 ITU staff anxiety n=182 Percent “yes” Personal reputation 76 Threat of malpractice suits 71 High expectations of the patients' family or society 68 Possible disciplinary actions by licensing boards 64 Threat to job security 63 Expectations of other team members 61 A study of 10% of all Dutch general practitioners and specialists in 1997 showed that underreporting of adverse drug reactions might partly be explained by lack of knowledge and by misconceptions about the process62. Although 98% of doctors had diagnosed an ADR in their patients, the likelihood of their reporting it (Table 38), and their reasons for not doing so (Table 39), varied between specialty. The commonest reasons for not reporting were similar for all three groups (uncertainty about the reaction itself, or it being too trivial or well-known) but surgeons were significantly less aware of the need to report, of the national system, or how to use it. In all three groups, only a quarter of doctors were familiar with the criteria for a reportable event – even though the reporting form and instructions are printed inside the Dutch equivalent of the British National Formulary (BNF). Based on responses of the 1,357 doctors to 16 hypothetical ADRs, there was no significant association of reporting patterns with age, sex or time since specialisation. Table 38: Voluntary reporting of ADRs, Netherlands 1997 GPs Surgeons Physicians % ever diagnosed but not reported an ADR 86 72 81 % ever reported an ADR 64 38 68 % ever reported to National Centre 51 15 41 % ever reported to pharmaceutical industry 34 31 55 Table 39: Reasons for not reporting ADRs, by specialty, Netherlands 1997
% GPs Surgeon Physician Uncertain association 78 61 66 Too trivial to report 70 81 70 Too well known to report 93 91 93 Unaware of existence of national ADR reporting system 7 16 7 Unaware of the need to report ADRs 18 26 16 Did not know how to report ADRs 20 37 22 Too bureaucratic 38 40 31 Not enough time 42 38 31 Fear of legal discovery 2 3 3

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 43
Four years before the survey of ADR reporting, Dutch GPs had stated that they would welcome reporting of general errors to a national committee. A survey of 600 GPs showed that 83% of respondents agreed that a national committee should be formed to receive error reports, and 89% said that they would submit reports to this standing committee of investigation63. In ‘Building a Safer NHS for Patients’, the UK Department of Health (page 40) reiterates the reasons stated by Dutch GPs for not reporting (Table 39), and adds:
- the patient recovers from the adverse event and the urgency goes out of the situation
- fear of point-scoring by colleagues, retribution by line management, disciplinary action or litigation
- an assumption that someone else will make the report - no evidence of timely feedback and/or corrective action being taken as a
result of making report Specific factors affecting attitudes to reporting Participation by individuals and organisations is affected by many factors, but all programmes studied by the IoM were perceived to suffer from underreporting, whether voluntary or mandatory. A general message from literature review is to ensure that participation of organisations in reporting systems is rewarded by the NHS (eg strategic HAs, CNST, controls assurance) and by independent bodies (eg Royal Colleges, accreditation programmes). “Much of the effort of ethicists and other advisers has been to encourage doctors to admit error without necessarily admitting liability” Vivienne Nathanson, UK 1999. Involvement of regulatory body Voluntary systems such as the Aviation Safety Reporting System (ASRS) avoid reporting to the regulatory body (the Federal Aviation Administration) but transfer the function of analysis and communication to a separate but technically authoritative body (NASA). However, there is no clear evidence in the USA that participation in or overall impact of mandatory systems is any greater than that of voluntary ones. Confidentiality “Protections for patients, healthcare professionals, and healthcare organizations are essential to the ability of any reporting system to learn about errors and effect their reduction” (AMA). Many USA states reported varying attitudes and legislation on whether individual events or institutions should be identified publicly; they were faced with having to balance the concerns of health care organisations to encourage participation in the programme and the importance of making information available to protect and inform consumers. It should be noted that New York State Public Health Law Section 2805-m Confidentiality prevents disclosure of incident reports under the Freedom of Information Law. “The greatest impediment to clinicians is having to give name and address; in Australia this was resolved by including in reporting forms a dark yellow area for “optional details”. The UK doctors are a “wounded population” needing maximum
“Much of the effort of ethicists and other advisers has been to encourage doctors to admit error without necessarily admitting liability” Vivienne Nathanson, UK 1999.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 44
protection. Accountability should be separated from the reporting structure, as in the USA where near-misses in aviation were successfully transferred from the FAA to NASA. In Australia the reporting system is protected from legal discovery, but it will not be in the UK; this argues for data to be disidentified before it leaves a hospital and for a stand-alone system which will be more secure. Using experience from around the world, various methods for obtaining information eg anonymous hot-lines should be piloted by the NPSA in NHS trusts to test their local utility.”80. An option for anonymous reporting may enable vital information, otherwise withheld, to reach the NPSA without compromising personal or public rights.64 Various means have been used to provide confidentiality to reporters65:
- Code of practice: voluntary “firewall”, imposed by the health care organisation, filters release of identity on basis of need to know – but may be challenged legally by subpoena
- Anonymous reporting: protects reporter but may reduce effectiveness of system for two reasons: it relies solely on initial information which cannot be amplified by reporters, and reporters may deliberately withhold key information which they consider might identify them.
- De-identification: removal of identifiers of individuals or institutions is a primary protection, but may lose related data such as type of centre, number of beds, and location. During 20 years of operation of the Aviation Safety Reporting System (ASRS) there has been no breach of identity of the reporter; de-identification usually occurs within 72 hours of the initial receipt of the report.
Litigation “Information developed in connection with reporting systems should be privileged for purposes of federal and state judicial proceedings in civil matters, and for purposes of federal and state administrative proceedings, including with respect to discovery, subpoenas, testimony, or any other form of disclosure.” (AMA) “Congress should pass legislation to extend peer review protection to data related to patient safety and quality improvement that are collected and analysed by health care organizations for internal use or shared with others solely for purposes of improving safety and quality” - Recommendation 6.1, IoM chapter 5 “protecting voluntary reporting systems from legal discovery”. The IoM report identifies three components of a reporting system from which plaintiffs can seek information:
- the original reporter - the recipients of the information who receive, investigate and analyse
reports - the reported data itself, residing in the data bank.
Legal protections are the only way to protect all three sources, but other methods can render the reporter unidentifiable or the data not useful to a plaintiff eg by de-identification. Existing laws in several US states protect data only as long as it remains within the individual institution; once transmitted elsewhere it may be subject to the freedom of information required by “sunshine laws”.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 45
Confidence In order to participate willingly, personnel must have confidence in the effectiveness of reporting and in resulting improvements. Clarity Clarity (of standards, definitions and tools) and ease of the processes and documents help reporters know what is expected to be reported, when and how. Inducement Payment has increased reporting, but the volume drops when payments cease 66 Training Education of staff is essential for them to understand what is reportable and how to do it. Health care organisations that are trained and educated in event recognition are more likely to report events. Feedback In USA, the Federal Drug Administration report that active feedback encourages submission of further reports by assuring reporters that the time taken to file reports is worthwhile67. “Belief by reporters that the information is actually used assures them that the time taken to file reports is worthwhile. Reporters need to perceive a benefit from reporting.” Chapter 5: Institute of Medicine, 2000 Consistent reinforcement A study of adverse incident reporting in an ICU in Australia suggested that there was no direct relation between report frequency and admission rate, and that high rates of reporting compliance were dependent on continual reinforcement of the project to staff, especially when staff rotate or during holiday periods68. Variations in reporting rates relate to the timing of heavy workload, to holiday periods and to staff rotations. The same study noted that 42% of events were recognised during routine checks or hand-overs prior to the occurrence of actual harm to the patient. “(Re-enforcement)… is a logistic problem when new staff commence eg at the beginning of new nursing courses, resident medical officer rotations and vacation periods such as Christmas/New Year when academic and quality assurance programs tend to be suspended.” GK Hart et al, Australia 1994
3.3 Methods of reporting
3.3.1 Case recognition Wilson et al, authors of the report on the Australian QAHCS study, comment that the ideal system for recording adverse events would be valid, reliable and cost effective, but that, in reality, the tools and methods are not available that would allow such a system to be implemented on a routine basis69. Therefore they recommend that

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 46
regular “snapshots” should be taken to identify numerators and denominators, to make recommendations for increased safety and to follow up and analyse their impact. Reporting should be triggered by people directly involved, but there is plenty of evidence that such reporting is more complete if events are also identified internally by indicators, the use of selective ICD10 codes in hospital administration systems eg HES, audits etc. It is also important that while front line staff may trigger the report, the report itself may be completed by others eg risk manager or QA department in order to relieve the clinician of burden and to encourage consistency and completeness. Direct observation Observational studies, although costly, have identified even higher rates of error and injury occurring during medical care than are shown by self-reporting or record review. For example, four trained ethnographers on three general surgical units at a Chicago teaching hospital recorded, over nine months in 1989/90, all "situations in which an inappropriate decision was made when, at the time, an appropriate alternative could have been chosen". They found that 45.8% of patients experienced an adverse event70. Eighteen per cent of these patients had a "serious" adverse event -that is, one that produced at least temporary disability – but only 1.2% of the 1,047 patients made claim for compensation. Similarly, Donchin et al placed an observer at the patient's bedside to observe clinicians in the medical - surgical intensive care unit of a university hospital in Israel. They reported that clinicians made 554 errors over four months, or 1.7 errors per patient per day71. Record review In order to obtain a quantitative estimate of the incidence or prevalence of adverse events medical record review is the only proven methodology69. Although, by their nature, patients’ records do not give contextual information about the clinical environment they do provide reliable measures of individual patient safety which are not as readily available from the higher level clinical indicators and ICD10 codes. Incident reports contain contextual data but the reliability of the numerator is generally poor. The most far-reaching research study so far into adverse events was the Harvard Medical Practice Study (HMPS). This examined a random selection of 30,121 patient records from 51 acute hospitals in New York State and determined that errors occur in 3.7% of cases. This figure is deemed to be low because:
- the study aimed to determine the feasibility of no-fault compensation for medical malpractice and was therefore concerned only with events leading to disability and potential compensation
- it only includes errors that were documented in the patient’s records - to be included in the study, cases had to be agreed as a legitimate legal
claim by two doctors, but in the courts only one doctor’s opinion is needed

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 47
“In order to obtain a quantitative estimate of the incidence or prevalence of adverse events, medical record review is the only proven methodology” Ross Wilson, Australia, 1999 The Quality in Australian Health Care Study, modelled on the Harvard study, surveyed the occurrence of adverse events during inpatient care by retrospective record review, screening 14,210 records from 31 hospitals in New South Wales and Victoria. Though valuable in identifying individual occurrences and resulting disabilities, this method was found to be very labour intensive and unsuitable for regular monitoring of adverse events72. The Wimmera programme25 used 8 (cf 18 in QAHCS and HMPS) criteria for screening inpatient records, and found fewer adverse events. When incident reporting was added, 16% more cases were found. The pilot of the principal UK study of errors also used 18 predefined screening criteria and a team of nurse researchers and physician assessors. Results were used to calculate reliability of the process with respect to causation, disability and preventability of events and to compare with similar studies in the USA and Australia73. Review of ICU records has shown that some adverse events were not recorded74. This reality also limits the power of retrospective observational studies to identify and then gather information on adverse events. Error Reporting systems
Mandatory reporting Most frequently, it is reporting systems whose primary role is to hold providers accountable that are “mandatory”. In the USA, these are operated by state regulatory programmes which have the authority to investigate and issue penalties or fines for wrong-doing. Reporting focuses on errors associated with serious injury or death, and may lead to public exposure. Such systems serve three purposes, as defined in To err is human: building a safer system (chapter 5)75 and shown below in Table 40. Table 40: Three purposes of mandatory reporting systems, USA
• Provide the public with a minimum level of protection by assuring that the most serious errors are reported, investigated and follow up
• Provide an incentive for health organisations to improve patient safety and to avoid the penalties and public exposure
• Require all organisations to invest in patient safety
Voluntary reporting Reporting systems that focus on safety improvement are usually “voluntary”. They concentrate on errors that result in no harm (“near misses”) or minimal harm to patients – but could have major implications. Reports are usually submitted outside the public arena and no penalties or fines are issued around a specific case. Such systems aim to identify and remedy vulnerabilities in systems before the occurrence of harm. They are particularly useful for identifying types of errors that occur too infrequently for an individual health care organisation to detect using their own data, and patterns of errors that point to systematic issues affecting all health care organisations.
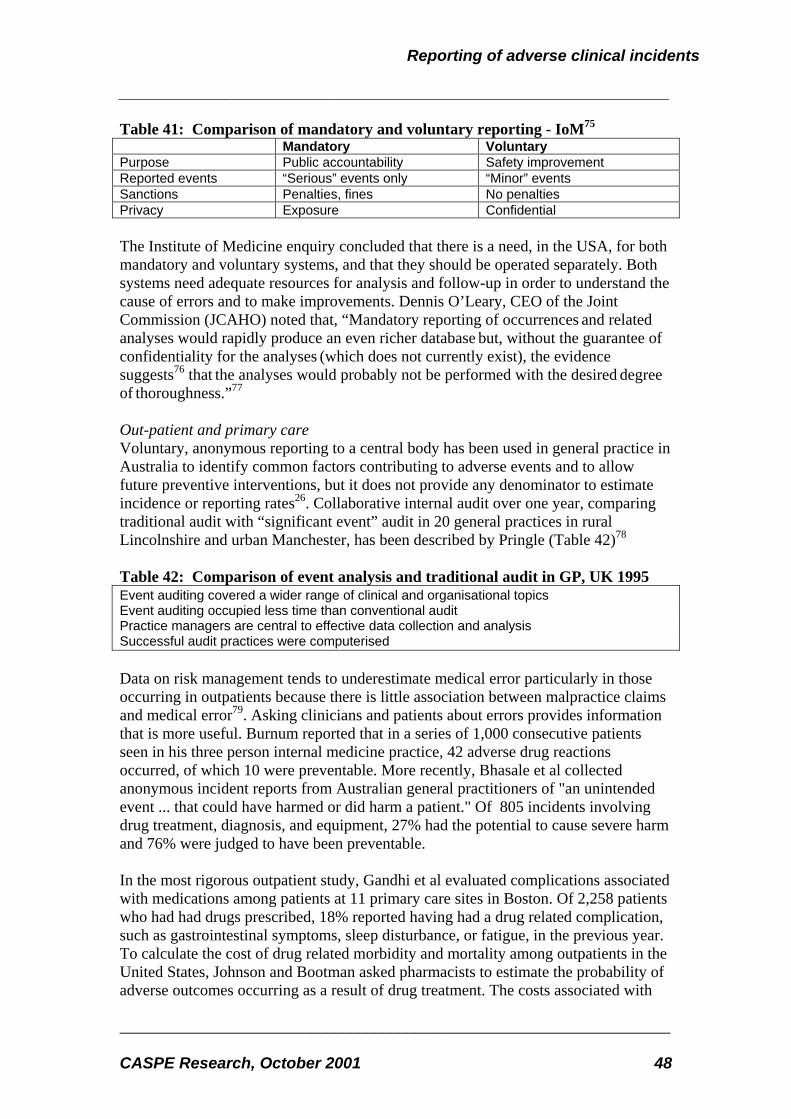
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 48
Table 41: Comparison of mandatory and voluntary reporting - IoM75 Mandatory Voluntary Purpose Public accountability Safety improvement Reported events “Serious” events only “Minor” events Sanctions Penalties, fines No penalties Privacy Exposure Confidential The Institute of Medicine enquiry concluded that there is a need, in the USA, for both mandatory and voluntary systems, and that they should be operated separately. Both systems need adequate resources for analysis and follow-up in order to understand the cause of errors and to make improvements. Dennis O’Leary, CEO of the Joint Commission (JCAHO) noted that, “Mandatory reporting of occurrences and related analyses would rapidly produce an even richer database but, without the guarantee of confidentiality for the analyses (which does not currently exist), the evidence suggests76 that the analyses would probably not be performed with the desired degree of thoroughness.”77
Out-patient and primary care Voluntary, anonymous reporting to a central body has been used in general practice in Australia to identify common factors contributing to adverse events and to allow future preventive interventions, but it does not provide any denominator to estimate incidence or reporting rates26. Collaborative internal audit over one year, comparing traditional audit with “significant event” audit in 20 general practices in rural Lincolnshire and urban Manchester, has been described by Pringle (Table 42)78 Table 42: Comparison of event analysis and traditional audit in GP, UK 1995 Event auditing covered a wider range of clinical and organisational topics Event auditing occupied less time than conventional audit Practice managers are central to effective data collection and analysis Successful audit practices were computerised Data on risk management tends to underestimate medical error particularly in those occurring in outpatients because there is little association between malpractice claims and medical error79. Asking clinicians and patients about errors provides information that is more useful. Burnum reported that in a series of 1,000 consecutive patients seen in his three person internal medicine practice, 42 adverse drug reactions occurred, of which 10 were preventable. More recently, Bhasale et al collected anonymous incident reports from Australian general practitioners of "an unintended event ... that could have harmed or did harm a patient." Of 805 incidents involving drug treatment, diagnosis, and equipment, 27% had the potential to cause severe harm and 76% were judged to have been preventable. In the most rigorous outpatient study, Gandhi et al evaluated complications associated with medications among patients at 11 primary care sites in Boston. Of 2,258 patients who had had drugs prescribed, 18% reported having had a drug related complication, such as gastrointestinal symptoms, sleep disturbance, or fatigue, in the previous year. To calculate the cost of drug related morbidity and mortality among outpatients in the United States, Johnson and Bootman asked pharmacists to estimate the probability of adverse outcomes occurring as a result of drug treatment. The costs associated with

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 49
adverse outcomes were taken from statistical and research reports. The authors calculated that drug related problems accounted for 116 million extra visits to the doctor per year, 76 million additional prescriptions, 17 million emergency department visits, 8 million admissions to hospital, 3 million admissions to long term care facilities, and 199,000 additional deaths. The total cost was estimated to be $76.6bn, rivalling the aggregate cost of caring for patients with diabetes in the US. Hospital in-patient data
Australia Retrospective analysis of the Victorian Inpatient Minimum Database for all 135 public and 112 acute care hospitals in the State was used to describe the nature and frequency of adverse events reported in routine data collection72. Adverse events identified by ICD-9-CM E-codes (870-876; 878-9; 930-49) were collated with Australian national DRG (AN-DRG) codes. This showed an E-code in 5% of the 1,248,021 separations recorded, and a recorded rate of adverse drug events (19%) identical to the Harvard Study (of case records). This suggests that routine in-patient data can provide information on patterns and risks of adverse events, although they cannot identify their seriousness or long-term outcome. The existing ICD E codes are widely under-used for coding adverse events, and need expansion if they are to be used for routine capture of clinical incidents. But only 10-30% of known adverse drug reactions get classified even when an ICD-10 code exists; other sources being tapped in Australia for information on incidents are death certificates and coroners’ reports. 80 Table 43: Screening by routine data compared with case records, Australia VIMD
(data) HMPS
(records) QAHCS
(records) Adverse events as % all separations 5.0 Deaths as % all separations 2.9
(2.7-3.2) 4.9
(3.8-6.0) incl post-discharge
% events attributable to surgery 65.0 48.0 % events attributable to medication 19.0 19.0 % events attributable to misadventure <2.0 % admissions dying due to adverse events 0.14 0.50 0.79
USA In the USA, National Center for Health Statistics (NCHS) data have been proposed to examine questions of patient safety by profiling issues such as in Table 44 81. Table 44: Adverse event factors recognisable by routine data screening, USA
• Complications and adverse events in hospital settings.
• Avoidable hospitalizations, conditions, or procedures.
• Visits to emergency departments or outpatient settings for adverse effects of medication or medical misadventure.
• Under-use of appropriate medications and treatments.
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 50
• Adverse events, such as falls, fractures, or pressure ulcers in nursing-home or home and hospice care settings.
• Deaths due to medical misadventure.
• Characteristics of the health care system that may be related to safety.
• Characteristics of patients experiencing errors
Combined approaches Records plus reporting Aggressive case finding may identify injuries and errors that are not documented in a patient's chart82. Using a computerised model to detect adverse drug events among patients at a hospital in Salt Lake City, Utah, Classen et al found that adverse drug events occurred in 1.7% of admissions83. In comparison, using both chart review and prompted self-reports from clinicians, Bates et al found that adverse drug events occurred among 6.5% of patients and potential adverse drug events occurred among 5.5% of patients admitted to two teaching hospitals in Boston84. Of the adverse drug events 28% were due to errors, making the rate of serious medication errors (that is, preventable adverse drug events plus potential adverse drug events) 7.3%. Both of these studies reported rates that are much higher than the 0.7% rate of adverse drug events identified in the Harvard study's review of medical records. Computer plus reporting During a six-month study of adverse drug events in a 650-bed teaching hospital in Arizona, researchers found that 44% of true-positive alerts identified by a computer system designed to correct errors were unrecognised by the physicians prior to the notification85. A similar study in a teaching hospital showed that non-intercepted serious medication errors decreased by 55% (from 10.7 to 4.86 events per 1000 patient days after the introduction of computerised physician order entry (POE)86. Although these studies were aimed primarily at local error correction, rather than national reporting, they do suggest that the detection of reportable events can be greatly increased when self-reporting is enhanced by surveillance using routine data systems. Patients, GPs, records plus reporting The Wimmera hospital programme25 combined record review with incident reports from staff, from patients and from GPs. GPs were asked to keep a reporting form attached to the notes of each patient for one month after discharge in order to report any adverse event which appeared later. Over two years 0.25 of discharges generated reports, of which 76% were classed as adverse events. Direct observation plus reporting A four-month concurrent incident study of an ICU in a university teaching hospital in Israel gathered data on the nature and causes of 554 human errors reported by medical staff87. Two types of data were collected: errors reported by physicians and nurses immediately after an error discovery; and activity profiles based on 24-hr records of a sample of patients taken by observers with human engineering experience. Errors were rated for severity and classified according to the body system and type of

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 51
medical activity involved. There was an average of 178 activities per patient per day and an estimated number of 1.7 errors per patient per day. For the ICU as a whole, a severe or potentially detrimental error occurred on the average twice a day. Physicians and nurses were about equal contributors to the number of errors, although nurses had many more activities per day. Many of these errors could be attributed to problems of communication between the physicians and nurses. One conclusion of the study was that errors should not be considered as an incurable disease, but rather as preventable phenomena. There is no single best method for capturing information on incidents; a combination of reporting, chart review and discharge data screening is necessary88 Only 10-30% of known adverse drug reactions get classified even when an ICD-10 code exists; other sources being tapped in Australia for information on incidents are death certificates and coroners’ reports.80
3.3.2 Reporting procedure Ease of reporting Ideally, systems would be on-line, highly user friendly and with guaranteed security. Over 35% of Dutch doctors considered that the reporting of adverse drug reactions was time-consuming and bureaucratic, and cited this as a reason for not reporting events. Commenting on the IoM proposals in the United States, Dotseth wrote about standardised formatting, “it will be important to ensure that these systems are compatible with existing systems and with one another, and will not require multiple reporting in different formats for the federal and state government or for private accrediting organizations. Research needs to address how best to establish systems so providers and care givers are not forced to make duplicate filings to several regulatory oversight agencies or bodies.” The new integrated NHS system for reporting to the NPSA will seek to build on rather than duplicate the mechanisms developed locally since 1955, and such as the Clinical Negligence Scheme for Trusts (CNST, voluntary programme) and Controls Assurance project (mandatory, but excludes clinical errors and independent providers). It will also seek to receive reports direct from patients and carers. The Institute for Safe Medication Practices (ISMP) in the USA has summarised key features for effective (voluntary) reporting of errors89(Table 45) Table 45: Features of reporting process - ISMP 2000 Reports initiated by front-line practitioners External reports direct to system or via one identified person in the local organisation Patient names removed from external reports Reporters and institutions remain named until follow-up and analysis completed Manual and electronic forms have standard minimum data fields and taxonomy Narrative descriptions also encouraged Reporting format clear and easy for practitioners to complete

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 52
Medium of reporting “Most NHS trusts already have standardised forms or other mechanisms, including electronic data capture, for recording adverse events and near misses” except in primary care. (Building a Safer NHS page 35) “Exemplar forms…applicable to primary and secondary care and patient or carer reporting will be developed” initially in document form but aiming at electronic use through the NHSnet and/or the Internet. Since several commercial and local software packages are already in use, a minimum reporting standard will be developed, together with enquiry facilities to interface with the national system and the NPSA. Sheikh and Hurwitz propose a national database of errors reported anonymously and confidentially by telephone to trained staff47 as a means of increasing its accessibility. Minimum data set for reports The Department of Health in the UK is developing and piloting a minimum data set to address the issues set out in Table 46. Table 46: Issues to be addressed by proposed minimum data set for NHS reporting • What happened? (event/near miss description, severity of actual or potential harm,
people and equipment involved) • Where did it happen? (location, specialty) • When did it happen? (date and time) • How did it happen? (immediate or proximate cause(s) • Why did it happen? (underlying, or root causes) • What action was taken or proposed? (immediate or longer term) • What impact did the event have? (harm the organisation, the patient, others) • What factors did, or could have, minimised the impact of the event? Hart et al68 noted that the information most often omitted in early reports pertained to the method of detection, incident severity, duration, and action taken. Types of report Florida has three types of “serious patient injury” report:
• the annual report is submitted in March to the risk management unit of the Agency for Health Care Administration by each licensed hospital and ambulatory surgical centre; this summarises all internal records of incidents causing patient injury “occurring in or coming to the attention of the facility for the entire previous calendar year”. This includes an analysis of the individual staff involved, the diagnostic or therapeutic procedures, the type of associated incident, and of pending and closed litigation.
• “Code 15 reports”, to be made within 15 days of occurrence of specific resulting injuries or surgical errors including analysis of causes and what action has been taken to diminish future risk
• “24 hour reports” were mandated by legislation in 1998 as a preliminary notice of patient injuries eg death, spinal or brain damage, wrong side/patient surgery/procedure
The 1998 legislative changes in Florida included narrowing the definition of a reportable adverse incident, and excluding actions related to medical staff on the

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 53
annual report. This may have contributed to the reduction in the number of reports from a peak in 1997 (Table 47). The contents of an incident report form from Florida is shown in Appendix 2. Table 47: Florida - reported patient injuries and claims 1995-99 1995 1996 1997 1998 1999 Annual report 3030 5140 5517 5113 3808 New malpractice claims 680 733 718 783 916 Code 15 reports 570 856 1102 994 720 24 hour reports 0 0 0 110 171
3.3.3 Analysis, taxonomy, aggregation Information submitted to reporting systems must be comprehensively analysed to identify actions that would minimise the risk that reported events recur (AMA). The IoM identified lack of resources and limitations in data as two main obstacles to the use of the information reported to State systems. Many states cited lack of resources as a reason for conducting only a limited analysis of data. Several had constructed, or were planning to construct, a database so that information could be tracked over time but had difficulty getting the resources or expertise to manage it. Additionally, several states indicated that the information they received was inadequate and variable. The need for more standardised formats was noted. The Australian software for incident reporting has been in use for about seven years; it is good at patient level but has been unable to provide aggregate data, benchmarks or cluster analysis until now. The new version being launched simultaneously in the UK, New South Wales and Victoria aims to be able to do this through the Internet, but has not yet been proven.90 Taxonomy of human error Rasmussen’s taxonomy identifies three types of behaviour91
- skill-based behaviour: routine tasks requiring little or no conscious attention during execution
- rule-based behaviour: familiar procedures applied to frequent decision-making situations
- knowledge-based behaviour: problem-solving activities, such as new situations for which no readily available standard solution exists
Reason’s taxonomy separates active, human errors from latent, system errors92 In active, human errors, individuals commit either a slip or a mistake:
- a slip is a skill-based error including omission (knowing what to do but doing nothing) and commission (inadvertently doing the wrong thing)
- a mistake may be knowledge-based or rule-based In system or latent errors, technical design or organisational issues (“organisational pathogens”) precede the error Accidents and adverse events happen when latent errors combine with active, human error.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 54
Coding systems for errors Since 1988, the Australian Patient Safety Foundation has developed classification systems for coding and reporting of incidents and adverse events. Data from the QAHCS was classified into the Generic Occurrence Classification (GOC), and this data compared with the Harvard Medical Practice Study (USA). The GOC+ is a development of the original Generic Occurrence Classification (GOC) structure that underpins the coding of incidents from AIMS and enables categorisation and classification of incidents. The GOC+ allows for quicker and simplified coding of an incident to its essential elements, as well as enhanced reporting from the system. The report coding used by New York State (NYPORTS) is provided in Appendix 3. Severity categories of damage The Safety Assessment Code (SAC) matrix developed by the VHA uses key factors to classify severity in four levels (Table 48). These factors are extent of injury; length of stay; level of care required for remedy, and actual or estimated physical plant costs. These four categories apply to actual adverse events and potential events (close calls). For actual adverse events, severity is assigned according to the patient's actual condition. If the event is a close call, severity is based on the most likely "worst case" systems level scenario. Table 48: VHA - severity categories Catastrophic Major Moderate Minor Patients with actual or potential adverse events
Death, major permanent loss of function not related to the natural course of the patient's illness or underlying condition (ie acts of commission or omission). Suicide (inpatient or outpatient) Rape Hemolytic transfusion reaction Surgery/Procedure on the wrong patient or wrong body part Infant abduction or infant discharge to the wrong family Death or major permanent loss of function sustained in a fall; or associated with an unauthorized departure from an around-the-clock
Permanent lessening of bodily functioning (sensory, motor, physiologic, or intellectual) not related to the natural course of the patient's illness or underlying conditions (i.e., acts of commission or omission). Disfigurement Surgical intervention required Increased length of stay of more than 3 patients Increased level of care for more than 3 patient
Increased length of stay for up to three patients; or Increased level of care for up to three patients.
No increased length of stay or increased level of care

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 55
treatment setting; or the result of an assault or other crime
Visitors Death; or Hospitalization of 3 or more (includes outpatients)
More than 3 visitors requiring evaluation and treatment
Evaluation and treatment for up to three visitors
Evaluated and no treatment required or refused
Staff Death; or Hospitalization of 3 or more
More than 3 lost time or restricted duty injuries or illnesses
Less than three lost time or restricted duty injuries or illnesses
treatment
Equipment or facility
Damage more than $100,000
Damage more than $10,000 but less than $100,000
Damage less than $10,000
3.3.4 Feedback and information Reporting systems should facilitate the sharing of patient safety information among healthcare organisations and foster confidential collaboration with other healthcare reporting systems (AMA). The most valued feedback is immediate, to acknowledge the report and to specify what steps are being taken to respond80.
3.3.5 System quality (process, outcome) Independent evaluation The reporting system should itself be subject to monitoring and evaluation by an identified independent body. This monitoring should include identification of factors that inhibit or encourage reporting, methods of analysing reports, roles of the NHS Executive, health authorities, trusts, and independent organisations in investigating adverse events, follow-up actions taken by the NHS, information disclosed to the public and the use made by purchasers and consumers of the resulting information. Evidence of benefit There is currently no evidence that the mandatory state reporting programmes in New York and Florida have been associated with a reduction in errors; this is largely because they have only recently been used with that intention. Lack of evidence concerning what data to collect, or what system to use, has deterred some states in the USA from introducing any mandatory reporting . “The volume of reports in itself does not indicate the success of a program … Reporting without analysis and follow-up may even be counter-productive in that it weakens support for constructive responses and is viewed as a waste of resources” Institute of Medicine, 2001 Volume of reports The goal of reporting programmes should not be maximising the number of reports per se. It is the analysis and using of the information contained in the reports together with the right tools, expertise and resources that helps to correct errors. Data for 1999,

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 56
the first full year of the Internet-based New York Patient Occurrence Reporting and Tracking System (NYPORTS) system, were released in February 2001. These indicate significant under-reporting against three tests: • wide variations between the seven regions within the state, ranging from 377
reports (New York City) to 1,101 (Finger Lakes) per 100,000 acute care discharges; the state-wide rate was 625 per 100,000
• wide variations between individual hospitals: 25 hospitals reported under 15 cases per 100,000 discharges
• under-reporting of cases identified by separate data systems: in one category analysed by a comparative analysis (patient deaths within 48 hours of surgery) the overall reporting compliance rate was only 16 percent (167 of the 1,030 cases identified by SPARCS state-wide hospital activity database) even after validation of coding. Some of the initial discrepancy (390 cases) between ‘raw’ SPARCS data for this code (1,420 cases) and actual reports was found to be due to differences in definitions (eg of “two days”, of “operating room procedure”). This particular definition seems to be relatively unambiguous and another contributory explanation may be that many hospitals have not yet instituted an effective process for identification and reporting of occurrences.
State officials of the New York State Health Department do not believe it likely that there are significant discrepancies in quality of care from one region to another, but that reporting accuracy and completeness are the most likely causes of the observed regional variations. The regional disparities are almost certainly attributable to under-reporting of patient events – despite the fact that the current system was created in partnership with hospital industry representatives, consumer advocates and representatives of medical specialities and has been mandatory since 1985. The under-reporting noted in this 2001 report appears to represent a systematic failure to report adverse incidents by certain facilities. Hospitals have been warned that, while the Department is ready to assist hospitals in meeting statutory reporting requirements, it also "stands ready to enforce requirements, and will publicly sanction those facilities that fail to promptly and accurately report incidents." Hospitals with reporting rates significantly below that anticipated are listed in the report. “Completeness is not a good measure of a reporting system. Adverse drug reactions which “everybody knows” are under-reported, but there would be no value in more complete reporting of them. Public accountability is not served by over-reporting.”80. “Public accountability is not served by over-reporting.” Bill Runciman, Australia 2001 Under-reporting of ADRs “Another major concern with any spontaneous reporting system is under-reporting of adverse events. It has been estimated that rarely more than 10% of serious ADRs, and 2% to 4% of non-serious reactions, are reported to the British spontaneous reporting program93. A further estimate suggests that the FDA receives by direct report less than 1% of suspected serious ADRs. These examples mean that cases spontaneously reported to surveillance programmes, which comprise the numerator, generally represent only a small proportion of the number that have actually occurred. The

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 57
effect of under-reporting can be somewhat lessened if submitted reports, irrespective of number, are complete and of high quality. After introducing the MERS-TM system of no fault confidential reporting in transfusion medicine, one institution recorded a ten-fold increase in monthly reports54. “An overall increase in the number of events reported is considered a significant sign of success of a near-miss reporting system” van der Schaaf, Netherland 1992 Quality of reports People involved in the administration of reporting systems believe it is better to have good information on fewer cases than poor information on many cases. The perceived value of reports lies in the narrative that describes the event and the circumstances under which it occurred. Inadequate information provides little or no benefit to the reporter or the health system.
3.4 Resources
3.4.1 Time Lack of time, or the perception that it would be wasted time, slowed the uptake of clinical audit and is a stated reason for not reporting adverse drug reactions and peri-operative deaths. “Consideration of the reporter's time will ensure a far higher level of compliance”. Dotseth24
3.4.2 Education and training Risk management ‘Building a Safer NHS for Patients’ (page 41) identifies the need to provide NHS staff with skills to identify, gather information on, record and report events and near misses, undertaken root cause analysis and analyse patterns and trends. This will need: • to be integrated into the training activities of the Modernisation Agency, Clinical
Governance Support Team, Controls Assurance Support Unit and the Litigation Authority.
• to ensure that sufficient staff in each NHS organisation are skilled in the analysis of adverse events
• Intranet, Internet and CD-based learning tools • A dedicated training programme • Reflection in training and education programmes provided by Universities and
other institutions educating students in the health care professions. Undergraduate clinical training Studies on teaching human error and human factor engineering principles to health care personnel and students are limited94. In the United Kingdom, a study was done with 129 nurses to see how their coping mechanisms with errors affected their learning mechanisms95. Pilpel and his colleagues in Israel aimed
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 58
their teaching programme at medical students to "impart a tolerance of error" (quoted by Wu et al96). They posited, but had no outcomes data, that teaching about the inevitability of error and how it can be reduced would lead to acceptance and, subsequently, to candid reporting. They also theorized that the curriculum would help the students realise that their doubts and fears were shared by peers and superiors. As mentioned earlier, the Dutch study of reporting of ADRs by doctors showed widespread ignorance of the criteria, procedure and reasons for voluntary reporting even though these are printed inside the equivalent of the BNF. Local reporting co-ordinators The Australian AIMS programme offers three levels of distance learning packages to train hospital staff in the completion, analysis and coding of reports.
3.4.3 Data systems Some organisations and individuals may routinely report more than others because they have better internal systems (eg for linking events, and recognising patterns, sentinel events or deviations from protocols). Good systems can be used to assist event recognition, to assist report compilation, and to monitor reporting.
3.4.4 Funding National costs The IoM urged Congress to provide funds and technical expertise to adapt current reporting systems to collect the information needed, analyse it and conduct follow-up action with health organisations. A major concern expressed by individual states about mandatory reporting focused on the developing of new programmes when there was a lack of resources to use currently collected information effectively. They also complained of the lack of cost estimates to design and operate such systems. Eight years ago, a computer-based “order entry” system was established at the Brigham and Women’s Hospital in Boston for medications. The set-up costs of $1.4 million and annual maintenance costs of $0.5 million were associated with a 55% reduction in serious medical errors, and a saving of $5-10 million per year (David Bates). Recommendation 4 of the final report of the Australian Taskforce7 recommended the establishment of a national system for reporting adverse events to be run by an independent, non profit organisation called the National Patient Safety Foundation. Operating costs for such a system were estimated to be A$2.03 million per year, to be shared among participating hospitals with more than 75 beds. “Implementation without adequate resources for analysis and follow-up will not be useful” Institute of Medicine, USA, 2000 State costs The state of New York, which established the New York Patient Occurrence Reporting and Tracking System (NYPORTS) in 1998, reports that their Web-based

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 59
system is run using existing staff, required an initial investment of $160,000 and needs $20,000 in maintenance per year. This does not identify from where existing staff have been redeployed. As this investment is unusually low, it is likely that the type of resource investment most states will face might be substantially greater and could be a potential stumbling block in the implementation of a comprehensive reporting system if required to stay within tight budget restraints. However, it will be critical to consider these costs in the context of the cost savings from reporting systems (Dotseth). Costs elements for reporting facilities include staff time and training for co-ordinators and for general staff awareness; for the operation of the programme, they include capital, consumable and staff costs (technical and professional). Systems designed to identify individual occurrences are simpler and cheaper than those designed to extend to achieve overall system improvements. Systems with higher capital investment may be cheaper to operate. “New York made up-front investments to create a web-based technology that, while costly, led to immediate efficiency throughout its operations.” Jill Rosenthal, NAHSP 2001.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 60
4 Research opportunities ‘Current Research on Patient Safety in the United States’ summarises current activity in patient safety and medical error research in the United States, and identifies current and future directions and barriers to conducting this type of research. It includes a searchable database of active research projects identified by the surveyed organisations97. Recommendation 7 of ‘An organisation with a memory’ proposes that a programme of basic research should be commissioned by the Research Council and the NHS R&D programme (Table 49). This agenda was much enlarged in ‘Building a Safer NHS for Patients’ (pages 56-63). Table 49: NHS research questions, UK • Incidence, nature and causation of adverse events • Transferability of knowledge from other fields to health care • Practical approaches to risk minimisation and learning • Use of systems approaches in health care • Use of automated monitoring and evaluation of clinical interventions In the USA, the AHRQ has issued a call for research proposals, summarising the lack of existing evidence about what data should be collected, how it should be aggregated and analysed, how it should be reported to provide useful information to those trying to reduce patient injuries from medical errors, and how it can be protected from unintentional disclosure (Appendix 4). Specific research questions are identified in Table 50 below. Table 50: AHRQ research questions, USA What types of reporting systems are best for collecting the needed information? What types of analyses can turn the reported data into useful information for improving
patient safety (e.g., root cause analyses of single incidents, data sorting for common causes, human factors analyses)?
What reports can be produced, how reports should be formatted and transmitted, and to whom should they be sent to prompt action that will reduce the risk of avoidable harm to patients?
What type of information is most useful in preventing injuries to patients: - to providers in informing their actions to alter health care delivery practices, processes, procedures, and systems to reduce risk to patients? - to those providing public oversight so that they can act to reduce risk to patients? - to individuals who wish to act to reduce their own risk and to those who may act on behalf of a large group of individuals, such as purchasers? - to those who have been injured during their medical care and how can that information best be delivered
What protections are effective in protecting the privacy and confidentiality of the data from unintended disclosure?

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 61
Additional areas of research might focus on the topics described in brief below. Most of these have been drawn from Marie Dotseth’s work at the Minnesota Department of Health and her contribution to the ‘summit’ in Washington in September 2000 (see Table 19) but are equally applicable to the UK and other countries. Costs and benefits An extremely useful piece of information would be cost-benefit research conducted on existing systems to compare the total costs to the state and the private sector with the savings associated with system changes stemming from error reduction and related quality improvements. Effectiveness Dotseth proposed that, before mandatory reporting is considered as the preferred policy option for states attempting to take action on the issue of patient safety, more research must be done to ensure the overall effectiveness of such systems. Studies should also be undertaken on voluntary systems such as the system for the reporting of sentinel events operated by the Joint Commission on the Accreditation of Healthcare Organizations. Mandatory or voluntary Comparisons should be made between mandatory and voluntary reporting systems and research should be pursued to determine how mandatory or voluntary reporting bears on concerns about under-reporting, privacy, cost and regulatory overlap. The Institute of Medicine, with its recommendations for a dual reporting system, provides a framework for beginning to investigate the appropriate balance between voluntary and mandatory reporting. Primary care To date, very little research has focused on errors or adverse events occurring outside hospitals. Comparatively little is known about the prevalence of medical errors outside hospitals. In both the Harvard study and the Australian study 8-9% of adverse events occurred in a doctor's office, 2-3% at home, and 1-2% in nursing homes. Since these studies included only errors that were serious enough to require admission, these figures underestimate the extent of error associated with outpatient care98. Methodological challenges to this type of research include a lack of reliable documentation of medical decisions and inadequate knowledge about the types of errors that are clinically important and most common in ambulatory settings. Optimally, this research needs to be conducted across multiple sites, since findings from such studies are likely to be significantly influenced by particular practice settings.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 62
Appendix 1: Non-medical reporting systems
System
Reg
Mand
Vol
Anon
Conf
Narr
Imm
Threshold
Feedback
Aviation safety reporting systemw12(NASA)
Yes No Yes After filed
Yes Yes Yes Non-accidents Yes (Callback)
Aviation safety airways programw13(AA)
No No yes No Yes Yes No Non-crashes Yes
Airline Pilots Associationw14
(FAA)
No No Yes No Yes Yes No Incidents Yes
BA Air safety reportw20 No Yes No No Yes Yes No Safety related events
Yes (Flywise)
BA Confidential human factors reporting programw15
No No Yes No Yes No but can expand
No Human factor data Yes
BA Special event search and master analysisw16
Yes Yes No Yes Yes N/A Yes Monitors flight data recorders
Yes
Human factors failure analysis classification systemw17(USN)
Yes Yes No No No Yes No Crashes Yes
NASAw18
Yes Yes No No Yes Yes No Safety events Yes
Prevention and recovery information system for monitoring and analysisw19
No No Yes Yes Yes Yes No Accidents and near misses
Yes
Human factors information systemsw20
w21
Yes No Yes No Yes Yes Yes Human factor issues related to nuclear safety
Yes
NRC allegations systems processw22
Yes No Yes No Yes Yes Yes Safety concerns Yes
Diagnostic misadministration reports-regulatory information distribution systemw23(Fed nuclear)
Yes Yes No No, but patient ID is
No Yes ? Misadministration Yes
Key:- Reg Run by regulatory body Anon Anonymous Mand Mandatory Conf Confidential Vol Voluntary Narr Narrative
Imm Immune from discovery
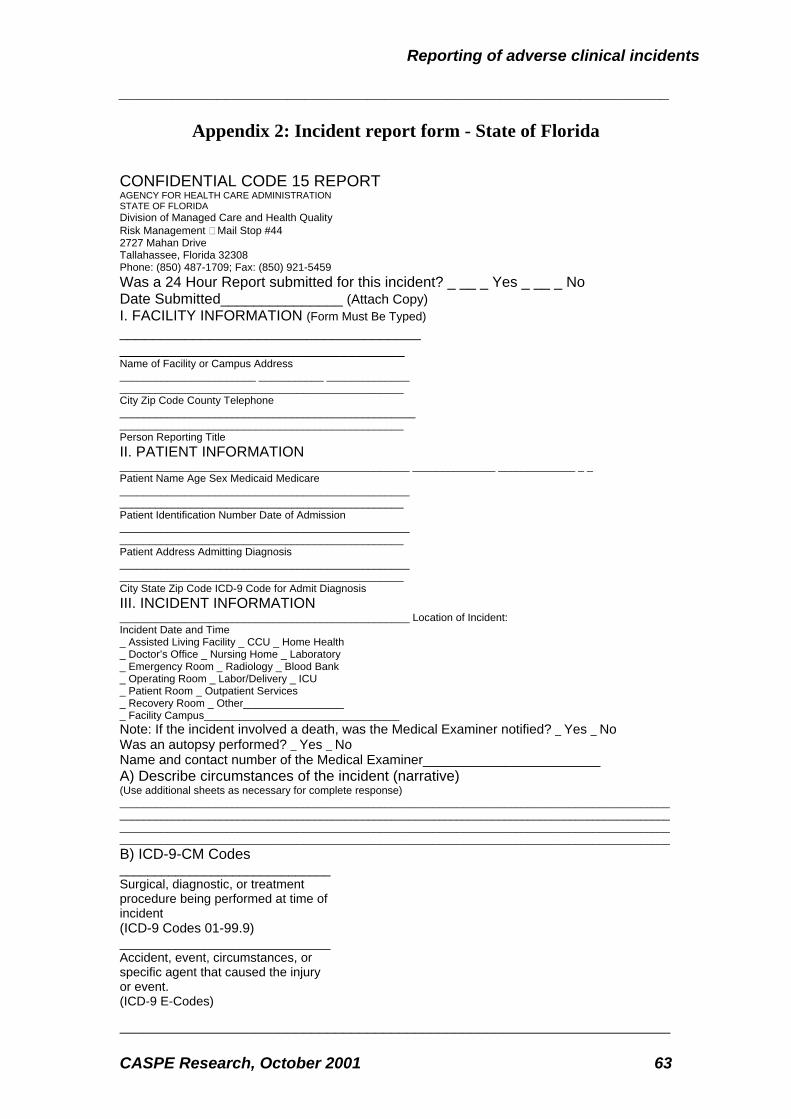
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 63
Appendix 2: Incident report form - State of Florida
CONFIDENTIAL CODE 15 REPORT AGENCY FOR HEALTH CARE ADMINISTRATION STATE OF FLORIDA Division of Managed Care and Health Quality Risk Management Mail Stop #44 2727 Mahan Drive Tallahassee, Florida 32308 Phone: (850) 487-1709; Fax: (850) 921-5459 Was a 24 Hour Report submitted for this incident? _ __ _ Yes _ __ _ No Date Submitted_______________ (Attach Copy) I. FACILITY INFORMATION (Form Must Be Typed) _____________________________________ ___________________________________ Name of Facility or Campus Address _______________________ ___________ ______________ ________________________________________________ City Zip Code County Telephone __________________________________________________ ________________________________________________ Person Reporting Title II. PATIENT INFORMATION _________________________________________________ ______________ _____________ _ _ Patient Name Age Sex Medicaid Medicare _________________________________________________ ________________________________________________ Patient Identification Number Date of Admission _________________________________________________ ________________________________________________ Patient Address Admitting Diagnosis _________________________________________________ ________________________________________________ City State Zip Code ICD-9 Code for Admit Diagnosis III. INCIDENT INFORMATION _________________________________________________ Location of Incident: Incident Date and Time _ Assisted Living Facility _ CCU _ Home Health _ Doctor’s Office _ Nursing Home _ Laboratory _ Emergency Room _ Radiology _ Blood Bank _ Operating Room _ Labor/Delivery _ ICU _ Patient Room _ Outpatient Services _ Recovery Room _ Other_________________ _ Facility Campus_________________________________ Note: If the incident involved a death, was the Medical Examiner notified? _ Yes _ No Was an autopsy performed? _ Yes _ No Name and contact number of the Medical Examiner________________________ A) Describe circumstances of the incident (narrative) (Use additional sheets as necessary for complete response) _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ B) ICD-9-CM Codes ______________________________ Surgical, diagnostic, or treatment procedure being performed at time of incident (ICD-9 Codes 01-99.9) ______________________________ Accident, event, circumstances, or specific agent that caused the injury or event. (ICD-9 E-Codes)

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 64
______________________________ Resulting injury (ICD-9 Codes 800-999.9) C) List any equipment used if directly involved in the incident (Use additional sheets as necessary for complete response) ______________________________________________________________________________ D) Outcome of Incident (Please check) __ Death __ Surgical procedure performed on the wrong patient __ Fetal death __ Wrong surgical procedure performed __ Brain damage __ Surgical procedure unrelated to the patient’s diagnosis __ Spinal damage __ Surgical procedure performed on the wrong site __ Surgical procedure to remove foreign objects remaining from a surgical procedure __ Surgical repair of injuries from a planned surgical procedure E) List license numbers of personnel and the capacity in which they were directly involved with this incident, i.e., ER physician, attending physician, surgeon, etc. (List social security numbers and capacity of unlicensed personnel)
_________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ F) List license numbers of witnesses (List social security numbers and capacity of unlicensed personnel)
_________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ IV. ANALYSIS AND CORRECTIVE ACTION A) Analysis (apparent cause) of this incident (Use additional sheets as necessary for complete response)
_________________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ B) Describe corrective or proactive action(s) taken (Use additional sheets as necessary for complete response)
_________________________________________________________ _________________________________________________________ _________________________________________________________ V. ___________________________________________ _______________ SIGNATURE OF PERSON PREPARING REPORT TITLE DATE From http://www.fdhc.state.fl.us/MCHQ/Health_Facility_Regulation/Risk/documents/Web3_11v02A_Code15form2000.pdf

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 65
Appendix 3: Reporting codes – NYPORTS, New York State
Appendix 4 of report from Commissioner of New York
State Health Department, February 2001
OCCURRENCE INCLUDES EXCLUDES
108. A medication error occurred that resulted in permanent patient harm. 109. A medication error occurred that resulted in a near-death event (e.g., anaphylaxis, cardiac arrest).
Medication Errors: Topical, Injectables, IV, PO
Treatment Medications, Contrasts, Chemotherapy
110. A medication error occurred that resulted in a patient death.
108-110. Any adverse drug reaction that was not the result of a medication error.
Aspiration 201. Aspiration pneumonitis/pneumonia in a non-intubated patient related to conscious sedation.
201. Patients intubated on ventilation, or with known history of chronic aspiration.
301. Necrosis or infection requiring repair (incision and drainage (I&D), debridement, or other surgical intervention), regardless of the location for the repair (e.g., at the bedside, in a treatment room, in the OR).
301. Any infiltration or infection treated exclusively with cold or warm packs, wound irrigation, IV change, and/or medication use (e.g., IV, PO, topical).
302. Volume overload leading to pulmonary edema.
302. Pulmonary edema clearly secondary to acute myocardial infarction. Pulmonary edema occurring in patients with previously known, predisposing conditions such as CHF, cardiac disease, renal failure, renal insufficiency or hemodynamic instability in critically ill patients.
Intravascular Catheter Related
303. Pneumothorax, regardless of size or treatment (including pneumothoraces resulting from a procedure performed through an intravascular catheter, e.g., temporary pacemaker insertion).
303. Non-intravascular catheter related pneumothoraces such as those resulting from lung biopsy, thoracentesis, permanent pacemaker insertion, etc.
401. New, acute pulmonary embolism, confirmed, or suspected and treated.
401. New, acute pulmonary embolism is suspected cause of sudden death but there is no autopsy to confirm. Acute pulmonary embolism present on admission and not associated with previous hospitalization within the past 30 days.
Embolic and Related Disorders
include readmissions within 30 days
402. New documented DVT (deep vein thrombosis)
402. Superficial thrombophlebitis.
Laparoscopic 501. All unplanned conversions to an 501. Diagnostic laparoscopy with

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 66
open procedure because of an injury and/or bleeding during the laparoscopic procedure.
a planned conversion or conversion based on a diagnosis made during the laparoscopic procedure. Conversions due to difficulty in identifying anatomy.
600’s category 601-605. Cardiac related occurrences reported in the cardiac reporting systems. NOTE: Consider the 911-963 codes when applicable. ESRD (End Stage Renal Disease) patients post dialysis treatment. (Include only if occurs while patient is in dialysis area.)
601. Any new central neurological deficit (e.g., TIA, stroke, hypoxic/anoxic encephalopathy).
601. Central neurological deficits due to direct procedures on the central nervous system (e.g., tumor dissection or removal). Transient metabolic encephalopathy.
602. Any new peripheral neurological deficit (e.g., palsy, paresis) with motor weakness.
602. Deficits due to operative or other procedure on a specific nerve (e.g., procedures involving neurofibroma, acoustic neuroma). Sensory symptoms or deficits without motor weakness (e.g., numbness or tingling, alone). NOTE: Deficits due to central neurological insults (such as hemiparesis) are submitted as a 601.
603. Cardiac arrest with successful resuscitation.
603. Intentional arrest during cardiopulmonary procedures. Cardiac arrest with unsuccessful resuscitation (submit as a 605).
604. AMI (Acute Myocardial Infarction) –unrelated to a cardiac procedure.
Perioperative/ Periprocedural Related
within 48 hours regardless of setting of operation or procedure
include readmissions.
605. Death (include ASA class if the procedure involves general anesthesia or conscious sedation).
603-605 Multiple trauma, AAA rupture known at time of surgery.
701. 2nd and/or 3rd degree burns. 701. 1st degree burns. Burns
Falls 751. Falls resulting in x-ray proven fractures, subdural or epidural hematoma, cerebral contusion, traumatic subarachnoid hemorrhage, and/or internal trauma (e.g., hepatic or splenic injury).
702. Falls resulting in soft tissue injuries.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 67
800’s category 801-819. Cardiac related occurrences reported in the cardiac reporting systems. 801-853. Birth related occurrences reported in the perinatal data system.
NOTE: Consider the 911-963 codes, when applicable.
801. Procedure related injury requiring repair, removal of an organ, or other procedural intervention. Any procedural injury to liver or spleen, including injury associated with lysis of adhesions or manipulation of the organ.
801. Procedure related injuries which do not penetrate, perforate or enter a lumen, require only a suture(s) to serosal/muscular layers to repair, or which do not require removal of an organ. Procedure related injuries resulting from intended, direct operation on an organ or other anatomical structure based on disease process or lack of an alternative approach available to address the presenting surgical condition.
803. Hemorrhage or hematoma requiring drainage, evacuation or other procedural intervention.
804. Anastomatic leakage requiring repair.
805. Wound dehiscence requiring repair. 806. Displacement, migration or breakage of an implant, device, graft, or drain, whether repaired, intentionally left in place or removed
806. Occurrences reported in 913 (retained foreign body) or occurrences due to equipment malfunction or defective product reported in 937 or 938.
807. Thrombosed distal bypass graft requiring repair.
807. AV grafts and fistulas used for dialysis.
Procedure Related
regardless of setting
within 30 days of the procedure
include readmissions
808. Post-op wound infection following clean or clean/contaminated case requiring drainage or hospital admission within 30 days. ASA class is required to be noted.
808. Contaminated or dirty case procedure
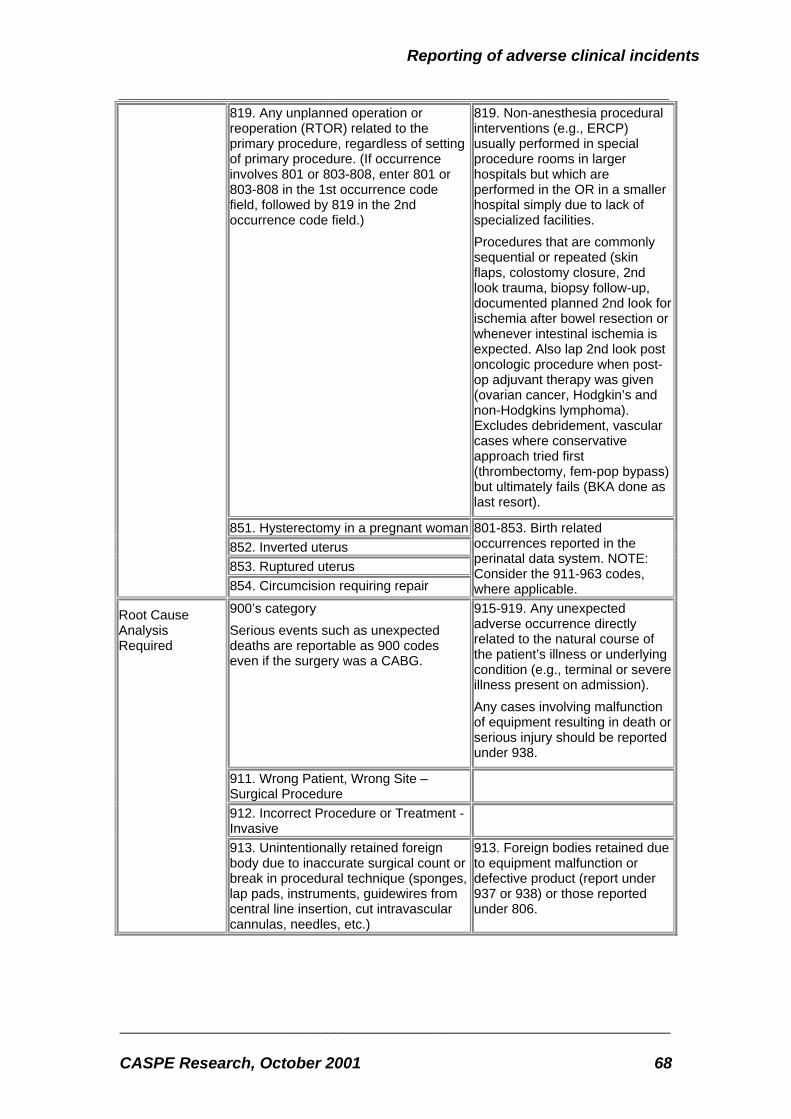
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 68
819. Any unplanned operation or reoperation (RTOR) related to the primary procedure, regardless of setting of primary procedure. (If occurrence involves 801 or 803-808, enter 801 or 803-808 in the 1st occurrence code field, followed by 819 in the 2nd occurrence code field.)
819. Non-anesthesia procedural interventions (e.g., ERCP) usually performed in special procedure rooms in larger hospitals but which are performed in the OR in a smaller hospital simply due to lack of specialized facilities. Procedures that are commonly sequential or repeated (skin flaps, colostomy closure, 2nd look trauma, biopsy follow-up, documented planned 2nd look for ischemia after bowel resection or whenever intestinal ischemia is expected. Also lap 2nd look post oncologic procedure when post-op adjuvant therapy was given (ovarian cancer, Hodgkin’s and non-Hodgkins lymphoma). Excludes debridement, vascular cases where conservative approach tried first (thrombectomy, fem-pop bypass) but ultimately fails (BKA done as last resort).
851. Hysterectomy in a pregnant woman852. Inverted uterus 853. Ruptured uterus
854. Circumcision requiring repair
801-853. Birth related occurrences reported in the perinatal data system. NOTE: Consider the 911-963 codes, where applicable.
900’s category Serious events such as unexpected deaths are reportable as 900 codes even if the surgery was a CABG.
915-919. Any unexpected adverse occurrence directly related to the natural course of the patient’s illness or underlying condition (e.g., terminal or severe illness present on admission). Any cases involving malfunction of equipment resulting in death or serious injury should be reported under 938.
911. Wrong Patient, Wrong Site – Surgical Procedure
912. Incorrect Procedure or Treatment - Invasive
Root Cause Analysis Required
913. Unintentionally retained foreign body due to inaccurate surgical count or break in procedural technique (sponges, lap pads, instruments, guidewires from central line insertion, cut intravascular cannulas, needles, etc.)
913. Foreign bodies retained due to equipment malfunction or defective product (report under 937 or 938) or those reported under 806.
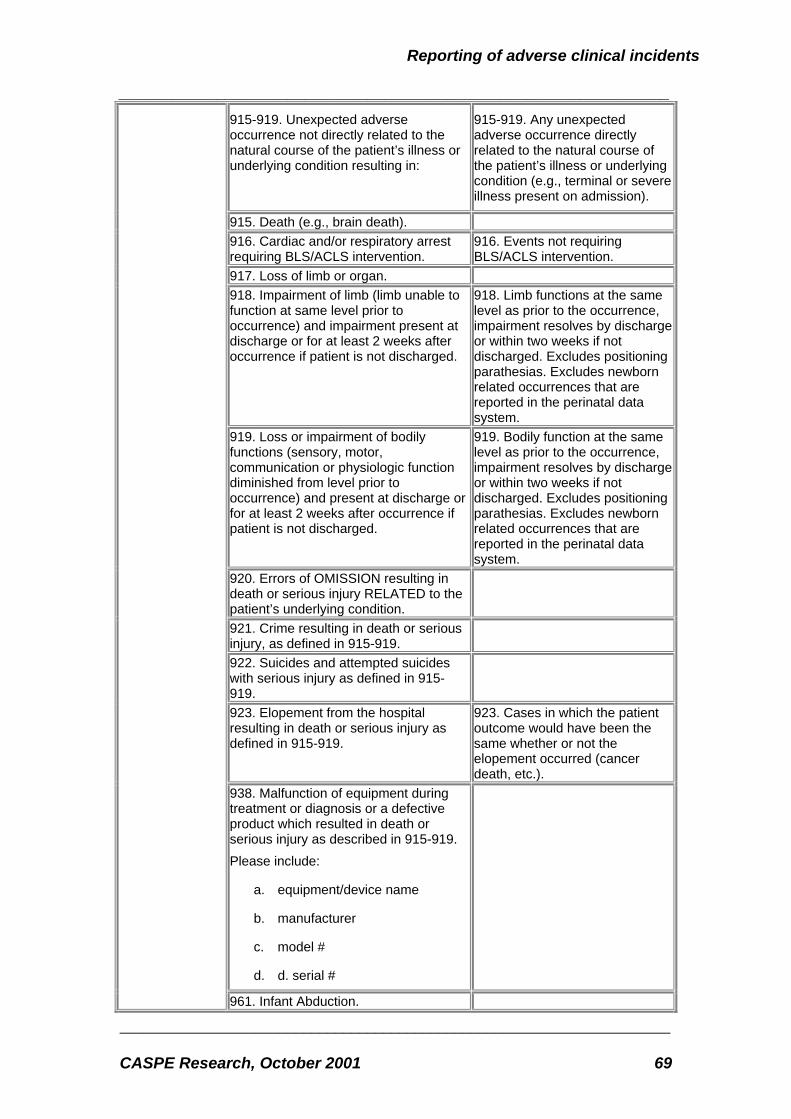
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 69
915-919. Unexpected adverse occurrence not directly related to the natural course of the patient’s illness or underlying condition resulting in:
915-919. Any unexpected adverse occurrence directly related to the natural course of the patient’s illness or underlying condition (e.g., terminal or severe illness present on admission).
915. Death (e.g., brain death). 916. Cardiac and/or respiratory arrest requiring BLS/ACLS intervention.
916. Events not requiring BLS/ACLS intervention.
917. Loss of limb or organ. 918. Impairment of limb (limb unable to function at same level prior to occurrence) and impairment present at discharge or for at least 2 weeks after occurrence if patient is not discharged.
918. Limb functions at the same level as prior to the occurrence, impairment resolves by dischargeor within two weeks if not discharged. Excludes positioning parathesias. Excludes newborn related occurrences that are reported in the perinatal data system.
919. Loss or impairment of bodily functions (sensory, motor, communication or physiologic function diminished from level prior to occurrence) and present at discharge or for at least 2 weeks after occurrence if patient is not discharged.
919. Bodily function at the same level as prior to the occurrence, impairment resolves by discharge or within two weeks if not discharged. Excludes positioning parathesias. Excludes newborn related occurrences that are reported in the perinatal data system.
920. Errors of OMISSION resulting in death or serious injury RELATED to the patient’s underlying condition.
921. Crime resulting in death or serious injury, as defined in 915-919.
922. Suicides and attempted suicides with serious injury as defined in 915-919.
923. Elopement from the hospital resulting in death or serious injury as defined in 915-919.
923. Cases in which the patient outcome would have been the same whether or not the elopement occurred (cancer death, etc.).
938. Malfunction of equipment during treatment or diagnosis or a defective product which resulted in death or serious injury as described in 915-919. Please include:
a. equipment/device name
b. manufacturer
c. model #
d. d. serial #
961. Infant Abduction.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 70
962. Infant discharged to wrong family. 963. Rape by another patient or staff 901. Serious occurrence warranting DOH notification, not covered by codes 911-963.
902. Patients transferred to the hospital from a diagnostic and treatment center.
902. Planned hospital admission from a diagnostic and treatment center.
914. Misadministration of radioactive material (as defined by BERP, Section 16.25, 10NYCRR).
931. Strike by hospital staff. 932. External disaster outside the control of the hospital which affects facility operations.
932. Situations that are related to termination of service should be reported under 933.
933. Termination of any services vital to the continued safe operation of the hospital or to the health and safety of its patients and personnel, including but not limited to the anticipated or actual termination of telephone, electric, gas, fuel, water, heat, air conditioning, rodent or pest control, laundry services, food or contract services.
934. Poisoning occurring within the hospital (water, air, food).
935. Hospital fire disrupting patient care or causing harm to patients or staff.
Submit Short Form Only
Root Cause Analysis Not Required
937. Malfunction of equipment during treatment or diagnosis or a defective product which has a potential for adversely affecting patient or hospital personnel or a resulting in a retained foreign body. Please include:
a. equipment/device name
b. manufacturer
c. model #
d. serial #
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 71
Appendix 4: AHRQ call for research into reporting strategies
The Agency for Healthcare Research and Quality (AHRQ) announces the availability of approximately 13-14 Cooperative Agreements (U18) for up to three years to support large demonstrations in states, health care systems, and/or networks of providers to test reporting strategies and patient safety interventions. By testing a variety of reporting, analysis, and implementation strategies, AHRQ wishes to evaluate what data should be collected, how it should be aggregated and analyzed, how it should be reported to provide useful information to those trying to reduce patient injuries from medical errors, and how it can be protected from unintentional disclosure. AHRQ is particularly interested in research projects that will test systems that publicly disclose information on errors or risks and comparing those systems to ones that are principally designed to enhance providers’ ability to learn to prevent errors. It is also interested in the feasibility of different methods of electronic data collection and analysis that will facilitate the processing and use of large amounts of data. Thus, the focus of this solicitation is the evaluation of error reporting systems that can collect and analyze data to identify risks to patient safety and develop effective methods of providing that information to providers, purchasers, policymakers and the public who can use it to improve safety through interventions like education, use of incentives, reorganization of work, introduction of new tools, the redesign of processes, changes in policies or purchasing strategies, or through their own choice of providers. AHRQ is specifically interested in the following questions: • What information is most useful in preventing injuries to patients? • What types of reporting systems are best for collecting the needed information? • What types of analyses can turn the reported data into useful information for
improving patient safety (e.g., root cause analyses of single incidents, data sorting for common causes, human factors analyses)?
• What reports can be produced, how reports should be formatted and transmitted, and to whom should they be sent to prompt action that will reduce the risk of avoidable harm to patients?
• What type of information is most useful to providers in informing their actions to alter health care delivery practices, processes, procedures, and systems to reduce risk to patients?
• What type of information is most useful to those providing public oversight so that they can act to reduce risk to patients?
• What type of information is most useful to individuals who wish to act to reduce their own risk and to those who may act on behalf of a large group of individuals, such as purchasers?
• What protections are effective in protecting the privacy and confidentiality of the data from unintended disclosure?
• What information is most useful to those who have been injured during their medical care and how can that information best be delivered

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 72
To date, very little research has focused on errors or adverse events occurring outside hospitals, for example, in office practices or ambulatory care clinics. Methodological challenges to this type of research include the lack of reliable ambulatory documentation of medical decisions and inadequate knowledge about the types of errors that are clinically important and most common in ambulatory settings. Optimally, this research needs to be conducted in multiple ambulatory sites, since findings from such studies may be significantly influenced by particular practice settings.

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 73
References
1 Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG, et al. Incidence of adverse events and negligence in hospitalized patients. N Engl J Med 1991;324:370-6 2 Leape LL, Lawthers AG, Brennan TA, Johnson WG. Preventing medical injury. Qual Rev Bull 1993;19:144-9. 3 Kohn LT et al. To err is human: building a safer health system. Washington: National Academy Press, 1999. www.nap.edu/openbook/030906837/html 4 Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The quality in Australian health care study. Med J Aust 1995;163:458-71 5 Vincent C, Neale G, Woloshnowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ 2001; 322: 517-519. 6 Vincent C, Taylor-Adams S, Stanhope N. Framework for analysing risk and safety in medicine. BMJ 1998; 316:1154-7 7 Australian Health Ministers Advisory Council. Final report of the taskforce on quality in Australian Health Care. Canberra: DoH, 1996. www.health.gov.au/pubs/hlthcare/ 8 Australian Patient Safety Foundation. www.apsf.net.au 9 Cull H. Review of processes concerning adverse medical events. Wellington: Ministry of Health, 2001 10 Department of Health. An organisation with a memory. London: HMSO, 2000 11 Ministry of Health. NHS Reporting of accidents in hospitals. HM(55)66. London; MoH, 1955 12 NHS Executive. Risk management in the NHS. London: NHS Executive, 1993 13 NHS Executive. Report of the independent inquiry relating to deaths and injuries on the children’s ward at Grantham and Kesteven General Hospital during the period February to April 1991. EL(94)16. NHS Executive, 1994 14 Wells W (Chairman). Kent and Canterbury screening report. NHS Executive 1997. 15 Dineen M, Walsh K. Incident reporting in the NHS. Health Care Risk Report. March 1999 16 Medicines Control Agency. www.open.gov.uk/mca 17 Medical Devices Agency. http://barn.ccta.gov.uk/mda/mdawebsiteV2.ns4/?Open 18 NHS Executive. The Public Interest Disclosure Act 1998 – Whistleblowing in the NHS. HSC 1999/198. NHS Executive, 1999 19 Department of Health. Building a Safer NHS for Patients. London: DoH, 2001. www.doh.gov.uk/buildsafenhs 20 AMA. www.ama-assn.org/ama/pub/articler/4119-4314.html 21 Rosenthal J, Riley T. Patient safety and medical errors: a road map for state action. Portland: National Academy of State Health Policy, 2001. www.nashp.org 22 JCAHO. Sentinel event reporting www.jcaho.org/sentinel/sentevnt_frm.html 23 Rosenthal J, Riley T, Booth M. State reporting of medical errors and adverse events: results of a 50-state survey. Portland: National Academy for State Health Policy, 2000 24 Dotseth. www.quic.gov/summit/wdotseth1.htm

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 74
25 Wolff AM, Bourke J, Campbell IA, Leembruggen DW. Detecting and reducing hospital adverse events: outcomes of the Wimmera clinical risk management program Med J Aust 2001; 174: 621-625 26 Britt H, Miller GC, Steven ID et al. Collecting data on potentially harmful events: a method for monitoring incidents in general practice. Family Practice 1997;14:101-6 27 Bhasale A, Miller GC, Reid SE, Britt H. Analysing potential harm in Australian general practice: an incident-monitoring study. Med J Aust 1998; 169: 73-6 28 Commonwealth of Australia. Health Insurance Act, 1973 29 Fallberg LH, Calltorp J. Medical mishaps and accidents: the Swedish situation. In Rosenthal MM, Mulcahy L, Lloyd-Bostock S. (eds) Medical mishaps. Buckingham: Open University Press, 1999 30 Critical incident reporting system (CIRS ) for anaesthetists. www.medana.unibas.ch/cirs/ 31 US Pharmacopoeia. http://www.ashp.org/US Pharmacopoeia 32 The Emergency Care Research Institute. www.ecri.org 33 National Academy of State Health. Policymakers report (original). 34 Rosenthal J, Barry A. Cost implications of state medical error reporting programs. Portland: National Academy for State Health Policy, 2001 www.nashp.org 35 JCAHO. Sentinel event reporting www.jcaho.org/ptsafety_frm.html 36 O’Leary D. Accreditation's role in reducing medical errors BMJ 2000;320:727-728 37 Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ 2000;320:759-763 38 Department of Health. Building A Safer NHS For Patients. London: DoH, 2001 39 AHRQ definitions. http://grants.nih.gov/grants/guide/rfa-files/RFA-HS-01-003.html 40 National Center Patient Safety. www.va.gov/ncps/index.html 41 Nagel ID. Human error in aviation operations. In:Weiner EL (ed). Human factors in aviation. San Diego: Academic Press, Inc., 1988. 42 Kaplan HS, Battles JB, van der Schaaf TW, Shea CE, Mercer SQ. Identification and classification of the causes of events in transfusion medicine. Transfusion, 1998; 38: 1071-1081. 43 Testimony of Timothy T. Flaherty, Panel 4: Reporting Issues and Learning Approaches. Written Statement. National Summit on Medical Errors and Patient Safety Research. September 2000. www.quic.gov/summit/mdotseth,htm 44 Dotseth M. Reporting issues and learning approaches. Written Statement. National Summit on Medical Errors and Patient Safety Research. September 2000. www.quic.gov/summit/mdotseth.htm 45 JCAHO. Preventing sentinel events in the environment of care. Oakville Terrace: JCAHO, 2000 46 Vincent C. Risk, safety and the dark side of quality. BMJ 1997; 314:1775-7 47 Sheikh A, Hurwitz B. A national database of medical error. J Roy Soc Med 1999; 92: 554-5 48 JCAHO. Sentinel events. http://www.jcaho.org/ptsafety_frm.html 49 Severe Hazards of Transfusion (SHOT) www.shot.demon.co.uk 50 Kizer KW. The National Quality Forum enters the game. International Journal for Quality in Health Care 2000; 12 (2): 85-87. 51 Andrews LB, Stocking C, Krizek T et al. An alternative strategy for studying adverse events in primary care. Lancet; 349: 309-13
Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 75
52van der Schaaf TW. Learning from errors and recoveries in medical chains www.dcs.gla.ac.uk/johnson/papers/HECS_99/Schaaf.htm 53 Arthur J, Wynn H. Risk Oriented Data Capture: Staged Modelling and Sampling Solutions for Problems with Data Overload in Incident Reporting Systems. Warwick Risk Initiative, University of Warwick , England 54 Battles J, Kaplan HS, vd Schaaf TW, Shea CE. The attributes of medical event reporting systems. Arch Pathol Lab Med 1998; 122: 231-8 55 van der Schaaf TW. Near miss reporting in the chemical process industry. Thesis. Eindhoven: Eindhoven University of Technology, 1992 56 Williamson JW, McKay P. Incident reporting. Med J Australia 1991; 155: 40-43 57 Wright D. Critical Incident Reporting in an Intensive Care Unit: 10 Years' Experience. Intensive Therapy Unit; Western General Hospital, Edinburgh 58 Busse DK, Chris W. Johnson. Identification and Analysis of Incidents in Complex, Medical Environments. Department of Computing Science, University of Glasgow, UK. 59 Bateman DN, Sanders GLS, Rawlins MD. Attitudes to adverse drug reaction reporting in the Northern Region. Br J Clin Pharmac 1992: 34: 421-6 60 Belton KJ, Lewis SC, Payne S, Rawlins MD, Wood S. Attitudinal survey of adverse drug reaction reporting by medical practitioners in the United Kingdom. Br J Clin Pharmac 1995; 39: 223-6 61 Sexton BJ, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ 2000; 320: 745-749 62 Eland IA, Belton KJ, Van Grootheest AC, Meiners AP, Rawlins MD, Stricker BH. Attitudinal survey of voluntary reporting of adverse drug reactions. J Clin Pharmacol. 1999; 48: 623-627. 63 Conradi MH, Schuling J, de Bruijn M, Meyboom de Jong M. Towards a model on prevention of errors in general practice. Int J Risk Safety Medicine. 1994; 6: 47-56 64 Runciman W, Merry A, McCall Smith A. Improving patients’ safety by gathering information. BMJ 2001; 323:298 65 Institute of Medicine. To err is human. Chapter 6: Protecting reporting systems from legal discovery. 66 Feely J, Moriarty S, O’Connor P. Stimulating reporting of adverse drug reaction by using a fee. BMJ 1990; 300: 22-3 67 FDA. Managing the risks from medical product use. 1999 68 Hart GK, Baldwin I, Gutteridge G, Ford J. Adverse incident reporting in intensive care. Anaesth Intens Care 1994; 22: 556-61 69 Wilson RM, Gibberd R, Hamilton J, Harrison B. Safety of health care in Australia: adverse events to hospitalised patients. In Rosenthal MM, Mulcahy L, Lloyd-Bostock S. (eds) Medical mishaps. Buckingham: Open University Press, 1999. 70 Andrews LB, Stocking C, Krizek T, Gottlieb L, Krizek C, Vargish T, et al. An alternative strategy for studying adverse events in medical care. Lancet 1997; 349: 309-13. 71 Donchin Y, Gopher D, Olin M, Badihi Y, Biesky M, Sprung CL, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med 1995; 23: 294-300 72 O’Hara D, Carson NJ. Reporting of adverse events in Hospitals in Victoria, 1994-5. Med J Aust 1997; 166: 460-3

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 76
73 Neale G, Woloshynowych M, Vincent C. Exploring the causes of adverse events in NHS hospital practice. J Roy Soc Med 2001; 94: 322-30 74 Rubins HB, Moskowitz MA. Complications of care in a medical intensive care unit. J Gen Intern Med 1990; 104-9 75 Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington DC: National Academy Press. 1999. ISBN 0-309-06837-1. 76 O'Leary DS. Organisational evaluation and a culture of safety. In: Proceedings of Enhancing Patient Safety and Reducing Errors in Health care. Chicago: National Patient Safety Foundation, 1999 77 O’Leary DS. Accreditation’s role in reducing medical errors. BMJ 2000; 320: 727-728 78 Pringle M, Bradly CP, Carmichael CM et al. Significant event auditing: a study of the feasibility and potential of criteria-based auditing in primary medical care. Occasional paper 70. London: RCGP, 1995 79 Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med 1996;335:1963-7 80 Personal communication. Bill Runciman, President, Australian Patient Safety Foundation 81 Patient Safety Reporting Systems and Research in HHS. Fact Sheet. April 2001. Agency for Healthcare Research and Quality, Rockville, MD. www.ahrq.gov/qual/taskforce/hhsrepor.htm 82 O'Neil AC, Petersen LA, Cook F, Bates DW, Lee TH, Brennan TA, et al. Physician reporting compared with medical-record review to identify adverse medical events. Ann Intern Med 1993; 119: 370-6 83 Classen DC, Pestotnik SL, Evans RS, Burke JP. Computerized surveillance of adverse drug events in hospitalized patients. JAMA 1991;266:2847-51 84 Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events and potential adverse drug events. JAMA 1995;274:29-34 85 Raschke RA, Gollihare B, Wunderlich TA et al. A computer alert system to prevent injury from adverse drug reactions. JAMA 1998; 280: 1317-20 86 Bates DW, Leape LL, Cullen DJ et al. Effect of computerised physician order entry and a team intervention on prevention of serious medication errors. JAMA 1998; 280: 1311-16 87 Donchin Y, Gopher D, Olin M, Badhi Y, Biesky M, Sprung CL, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med 1995; 23: 294-300. 88 Personal communication. Bruce Barraclough, CEO Australian Council for Safety and Quality in Health Care 89 Institute for Safe Medication Practices. Discussion Paper on Adverse Event and Error Reporting in Healthcare. January 24, 2000. www.ismp.org 90 Personal communication. Chris Brook, Director of Acute Services, Health Department, Victoria 91 Rasmussen J. The definition of human error and a taxonomy for technical systems design. In Rasmussen J, Duncan K, Leplat J (eds) New technology and human error. London: Wiley, 1987 92 Reason J. Generic error-modelling system (GEMS): a cognitive framework for locating common human error forms. In Rasmussen J, Duncan K, Leplat J (eds), New technology and human error. London: Wiley, 1987

Reporting of adverse clinical incidents
______________________________________________________________
_____________________________________________________________________ CASPE Research, October 2001 77
93 Rawlins MD. Pharmacovigilance: paradise lost, regained or postponed? The William Withering Lecture 1994. J R Coll Physicians. London: 1995; 29: 41-49. 94 Gosbee JW. Human Factors Engineering is the Basis for a Practical Error-in-Medicine Curriculum. Center for Applied Medical Informatics, Michigan State University 95 Meurier, C.E., C.A. Vincent, and D.G. Parmar, 1997. Learning from Errors in Nursing Practice. Journal of Advanced Nursing 26(1): 111-119. 96Wu, A.W., S. Folkman, S.J. McPhee, and B. Lo, 1991. Do House Officers Learn From Their Mistakes? Journal of the American Medical Association 265: 2089-2094. 97 Cooper JB, Sorensen AV, Anderson SM, Zipperer LA, Blum LN, Blim JF. Current Research on Patient Safety in the United States. Final Report. Health Systems Research, Inc. subcontract # 290-95-2000. National Patient Safety Foundation (www.npsf.org), 2001 98 Weingart SN, Wilson RMcL et al. Epidemiology of medical error. BMJ 2000; 320:774-7.


















