The Relative Exposure of the Operating Room Staff to Sevoflurane During Intracerebral Surgery Anesth...
28
The Relative Exposure of the Operating Room Staff to Sevoflurane During In tracerebral Surgery Anesth Analg 2009;109:11 87-92
-
Upload
christal-tyler -
Category
Documents
-
view
222 -
download
3
Transcript of The Relative Exposure of the Operating Room Staff to Sevoflurane During Intracerebral Surgery Anesth...
The Relative Exposure of the Operating Room Staff to Sevoflurane During Intracerebral Surgery
Anesth Analg 2009;109:1187-92
Background Volatile anesthetic on staff
Since 1967 Chronic exposure
Hepatotoxicity and nephrotoxicity Carcinogenesis Immunity Fertility Fetal development
More likely to develop Headache Somatic and mental fatigue attention

Potential environment factors Mask induction Uncuffed tracheal tube Laryngeal mask …… Anesthetic from surgical field to the surg
eon?
Neurosurgery The brain
Blood perfusion Capillary network Fat content
Sevoflurane Rapid accumulation in the brain Blood: gas partition coefficient=0.69
Marked escape from blood when circulation open
Questions?
sevoflurane close to the craniotomy window (the surgeon’s breathing zone) remote site in the OR
a correlation? sevoflurane near surgical site size of the cranitomy window
Methods Induction
propofol 1-2.5mg/kg Maintenance
Fentanly-rocuronium-sevoflurane Intubation
Low pressure cuffed <30mmHg
Monitoring
Fresh gas flow 2L/min Sevoflurane (0.7-2.3 V%) Air
Scavenging system Air circulation 50m3/min

Sample collection (dura opening ~ closure ending) 35 patients
Surgeon’s breathing zone Anesthesiologist’s breathing zone Farthest corner of OR
16 patients …… …… Within 5cm of the tracheal tube

Data analysis
Chromatography ppm (one part per million) mean+ SD P<0.05
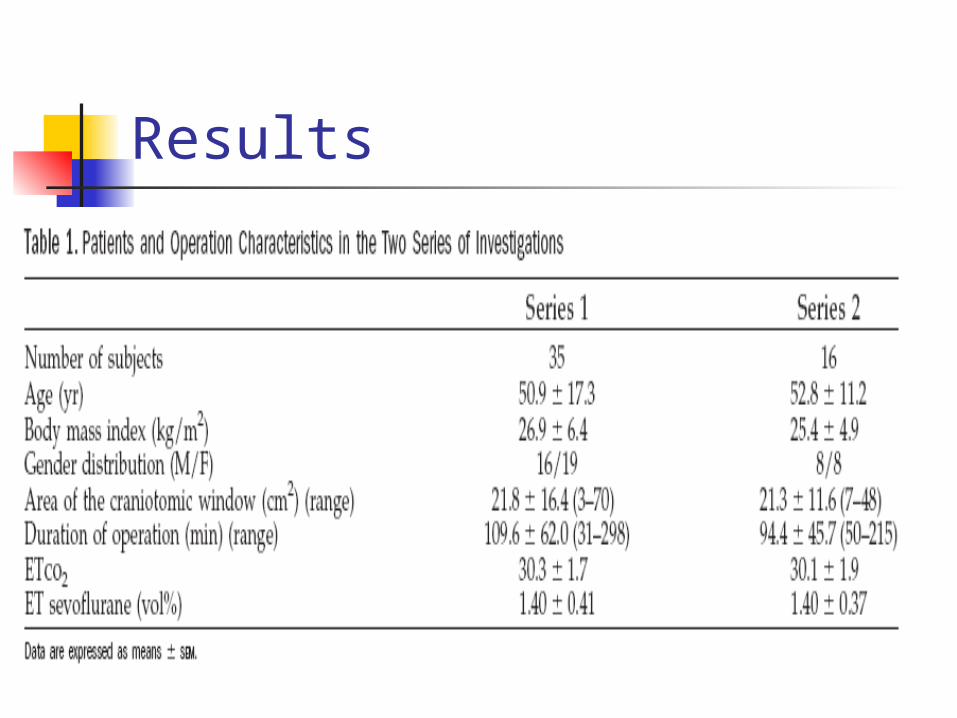
Results
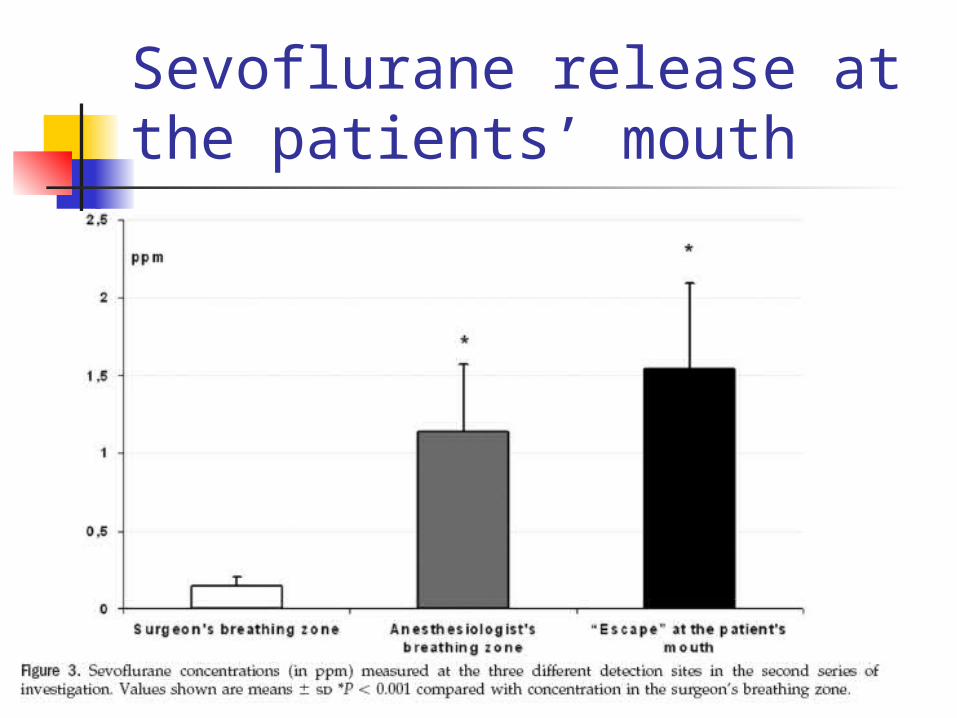
Sevoflurane release at the patients’ mouth
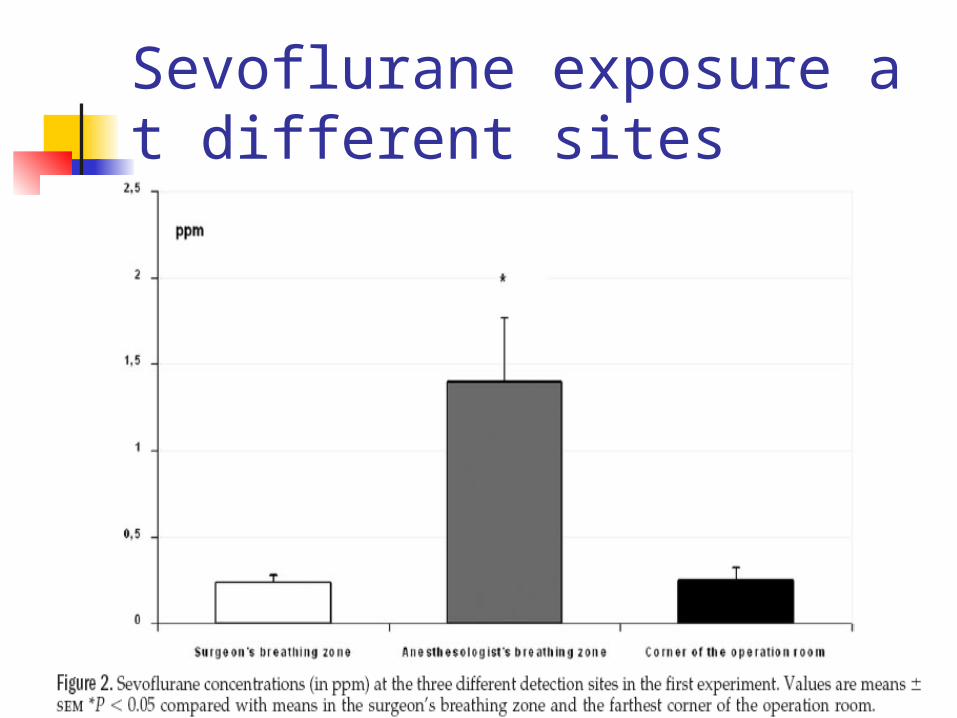
Sevoflurane exposure at different sites
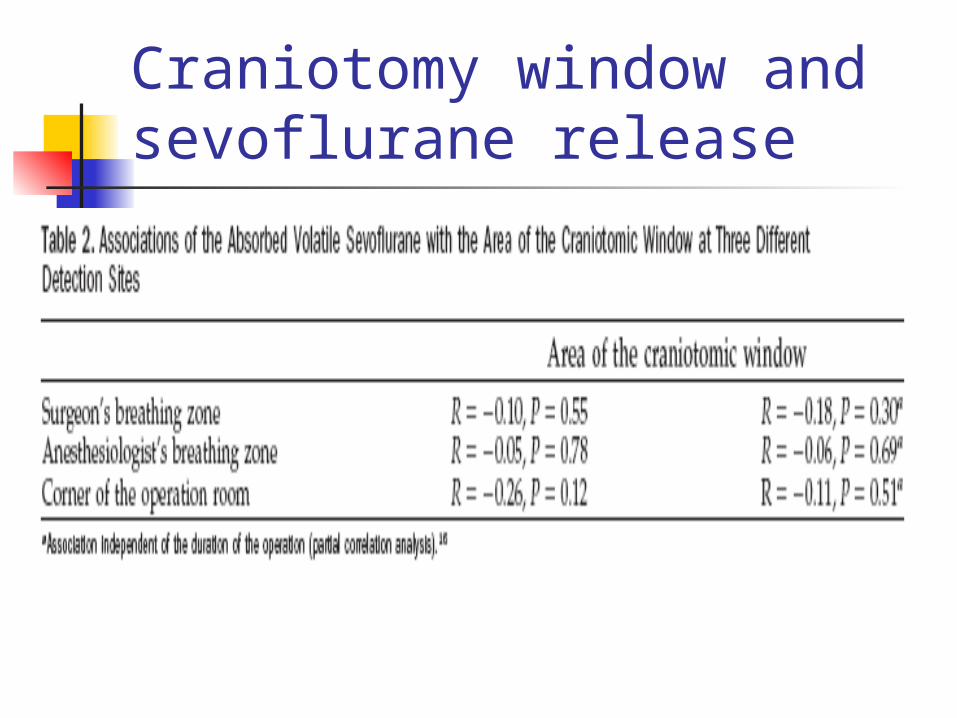
Craniotomy window and sevoflurane release

As a function of tumor type
Type Concentration(ppm)
n
Meningiomas 0.28+0.20 17
gliomatous 0.19+0.19 20
metastatic 0.20+0.07 9
others 0.19+0.09 5
Others
The ventilation system is good. Different concentrations at different sites For extended surgery
Low concentration Nonsignificant correlation with sevoflurane
OR door opening airflow air clearance
Conclusion Release of sevoflurane from the brain
through the craniotomy window dose not pose an additional environment risk for the neurosurgeon.
We should focus on improving the working condition for anesthesiologists.
We should further explore reasons for sevoflurane escape adequate countermeasures

Effect of Volatile Anesthetics on Oxidative Stress Due to Occupational Exposure
Method 30 anesthesia and surgery personnel
inhalation anesthetics for 3 years 30 healthy volunteers
no exposure at any time Result
antioxidant activity and trace element levels Conclusion
Antioxidant defense system was affected by free radical injury in those exposed to inhalation anesthetics chronically.
So minimizing occupational exposure to volatile anesthetics Operating room personnel should also take antioxidant supple
ments. World Journal of Surgery, 2005,29(4):540-542

Who is exposed? Anesthesiologists Dentists Nurse anesthetists Operating-room nurses Operating-room technicians Other operating-room personnel Recovery-room nurses Other recovery-room personnel Surgeons
What are the health effects? High concentration
Headache Irritability Fatigue Nausea Drowsiness Difficulties with judgement and coordina
tion Liver and kidney disease
Low concentration chronically miscarriages genetic damage cancer miscarriages in spouses birth defects in offspring
Where most likely to be exposed?
no automatic ventilation or scavenging systems
systems are in poor condition recovery rooms where gases exhaled
by recovering patients are not properly vented or scavenged

When leaks breathing circuit disconnection of the system gas seeps over the lip of mask or from en
dotracheal coupling During dental operations During induction of anesthesia
How to reduce? Inspect the anesthetic delivery system befo
re each use as part of the daily machine checklist.
Make sure the scavenging equipment is properly connected.
Start the gas flow after the laryngeal mask or endotracheal tube is installed.
Fill vaporizers under a ceiling-mounted hood with an active evacuation system.
Fill vaporizers before or after the anesthetic procedure.
Make sure that uncuffed endotracheal tubes create a completely sealed airway.
Use the lowest anesthetic gas flow rates possible Do not deliver anesthesia by open drop (drippin
g liquid, volatile anesthetic onto gauze). If a mask is used, make sure it fits the patient wel
l. Eliminate residual gases through the scavenging
system as much as possible before disconnecting a patient from a breathing system.
Turn the gas off before turning off the breathing system.