The rehabilitation of an edentulous mandible with a CAD/CAM zirconia … · 2020-03-24 · complete...
5
The rehabilitation of an edentulous mandible with a CAD/CAM zirconia framework and heat-pressed lithium disilicate ceramic crowns: A clinical report Youngwook Cho, DMD, MSD, PhD a and Ariel J. Raigrodski, DMD, MS b School of Dentistry, Kyung Hee University, Seoul, Republic of Korea; School of Dentistry, University of Washington, Seattle, Wash This clinical report describes a complete arch, implant-supported prosthesis with a zirconia framework and monolithic lithium disilicate crowns. The design of the computer-aided design/computer-aided manufacturing zirconia framework with cemented crowns with screw access is useful in facilitating retrievability and adequate fit, and may reduce the likelihood of porcelain chipping. (J Prosthet Dent 2014;111:443-447) Dental implants are considered to be a predictable treatment for restor- ing edentulous mandibular arches. 1-3 Computer-aided design/computer-aided manufacturing (CAD/CAM) systems have been used for restoring edentulous arches with implant-supported fixed restorations 4,5 because they facilitate the fit between implants and super- structures better than conventional metal alloy castings. 6,7 Various meth- ods for fabricating these types of res- torations have been reported. Some suggest acrylic resin and denture teeth processed onto a CAD/CAM milled titanium framework, 8 and others re- commend the use of a screw or cement- retained 1-piece zirconia framework with veneering porcelain. 9,10 A zirconia framework is superior to a metal alloy or titanium framework in terms of esthetics and biocom- patibility. 11-14 However, concerns have been reported regarding long-term degradation, aging, and veneering por- celain chipping. 15,16 Even though long- term degradation is known to decrease the flexural strength of zirconia, the fracture of zirconia infrastructures has rarely been reported and is unlikely to cause clinical catastrophic failure. 17 Veneering porcelain chipping has been reported with zirconia-based fixed dental prostheses (FDP). Suggested causes include a lack of compatibility in terms of the coefficient of thermal expansion between the zirconia core and the veneering porcelain, 18-21 a framework design that does not provide proper support for the veneering porcelain, 22 rapid cooling rates, and relatively low fracture toughness and low flexural strength of the veneering porcelain. 23-25 To address these concerns, new layering porcelains with an adequate coefficient of thermal expansion and adequate mechanical properties have been de- veloped. 26,27 However, the veneering porcelain may still chip, and the repair process may become complicated and time consuming. In addition, por- celain chipping is the most frequently reported prosthesis-related technical complication of implant-supported ceramic FDPs. 28-30 To reduce the like- lihood of defects in veneering ceramics, alternative techniques such as mono- lithic zirconia restorations or pressing the veneering porcelain to the zirconia framework have been introduced. 31-33 Another frequent implant-related tech- nical complication is abutment screw loosening. 34 The purpose of this clini- cal report was to describe the use of lithium disilicate monolithic heat- pressed ceramic crowns with holes for abutment screw access that are bonded onto a zirconia framework to restore the edentulous mandible while de- creasing the risk of veneering porcelain fracture and facilitating retrievability. CLINICAL REPORT A 49-year-old man presented to the prosthodontic clinic of Gowoon Guide Dental Hospital with generalized advanced chronic periodontitis and missing teeth in the right posterior mandible and multiple teeth missing in the maxilla (Fig. 1). His chief complaint was difficulty in masticating. His med- ical history was noncontributory, with the exception of controlled hyperten- sion. A clinical evaluation revealed class II to class III mobility (according to the Miller classification) of the man- dibular teeth and gingival swelling with probing depths that exceeded 5 mm. The maxillary remaining teeth were in good condition except for wear due to sleep bruxism. A panoramic radiograph showed an edentulous atrophic poste- rior maxilla with pneumatization and significant alveolar bone resorption in the mandible (Fig. 2). Because of financial concerns, the patient wanted to have the mandible treated first with an implant-supported complete fixed a Private practice; and Affiliate Professor, Department of Prosthodontics, Kyung Hee University. b Professor, Department of Restorative Dentistry, University of Washington, School of Dentistry; Adjunct Professor, Department of Materials Sciences and Engineering University of Washington, College of Engineering. Cho and Raigrodski
Transcript of The rehabilitation of an edentulous mandible with a CAD/CAM zirconia … · 2020-03-24 · complete...

The
rehabilitation of an edentulousman
fram
disi
repo
Youngwook Cho
aPrivate practice; and Affiliate ProfesbProfessor, Department of RestorativSciences and Engineering University
Cho and Raigrodski
dible with a CAD/CAM zirconia
ework and heat-pressed lithium
licate ceramic crowns: A clinical
rt
, DMD, MSD, PhDa andAriel J. Raigrodski, DMD, MSb
School of Dentistry, Kyung Hee University, Seoul, Republic of Korea;School of Dentistry, University of Washington, Seattle, Wash
This clinical report describes a complete arch, implant-supported prosthesis with a zirconia framework and monolithiclithium disilicate crowns. The design of the computer-aided design/computer-aided manufacturing zirconia framework withcemented crowns with screw access is useful in facilitating retrievability and adequate fit, and may reduce the likelihood ofporcelain chipping. (J Prosthet Dent 2014;111:443-447)
Dental implants are considered tobe a predictable treatment for restor-ing edentulous mandibular arches.1-3
Computer-aided design/computer-aidedmanufacturing (CAD/CAM) systemshave been used for restoring edentulousarches with implant-supported fixedrestorations4,5 because they facilitatethe fit between implants and super-structures better than conventionalmetal alloy castings.6,7 Various meth-ods for fabricating these types of res-torations have been reported. Somesuggest acrylic resin and denture teethprocessed onto a CAD/CAM milledtitanium framework,8 and others re-commend the use of a screw or cement-retained 1-piece zirconia frameworkwith veneering porcelain.9,10
A zirconia framework is superiorto a metal alloy or titanium frameworkin terms of esthetics and biocom-patibility.11-14 However, concerns havebeen reported regarding long-termdegradation, aging, and veneering por-celain chipping.15,16 Even though long-term degradation is known to decreasethe flexural strength of zirconia, thefracture of zirconia infrastructures hasrarely been reported and is unlikely tocause clinical catastrophic failure.17
Veneering porcelain chipping has beenreported with zirconia-based fixed dental
sor, Depae Dentistryof Washin
prostheses (FDP). Suggested causesinclude a lack of compatibility in termsof the coefficient of thermal expansionbetween the zirconia core and theveneering porcelain,18-21 a frameworkdesign that does not provide propersupport for the veneering porcelain,22
rapid cooling rates, and relatively lowfracture toughness and low flexuralstrength of the veneering porcelain.23-25
To address these concerns, new layeringporcelains with an adequate coefficientof thermal expansion and adequatemechanical properties have been de-veloped.26,27 However, the veneeringporcelain may still chip, and the repairprocess may become complicatedand time consuming. In addition, por-celain chipping is the most frequentlyreported prosthesis-related technicalcomplication of implant-supportedceramic FDPs.28-30 To reduce the like-lihood of defects in veneering ceramics,alternative techniques such as mono-lithic zirconia restorations or pressingthe veneering porcelain to the zirconiaframework have been introduced.31-33
Another frequent implant-related tech-nical complication is abutment screwloosening.34 The purpose of this clini-cal report was to describe the useof lithium disilicate monolithic heat-pressed ceramic crowns with holes for
rtment of Prosthodontics, Kyung Hee Universit, University of Washington, School of Dentistrygton, College of Engineering.
abutment screw access that are bondedonto a zirconia framework to restorethe edentulous mandible while de-creasing the risk of veneering porcelainfracture and facilitating retrievability.
CLINICAL REPORT
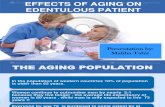
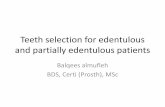
A 49-year-old man presented tothe prosthodontic clinic of GowoonGuide Dental Hospital with generalizedadvanced chronic periodontitis andmissing teeth in the right posteriormandible and multiple teeth missing inthe maxilla (Fig. 1). His chief complaintwas difficulty in masticating. His med-ical history was noncontributory, withthe exception of controlled hyperten-sion. A clinical evaluation revealed classII to class III mobility (according tothe Miller classification) of the man-dibular teeth and gingival swelling withprobing depths that exceeded 5 mm.The maxillary remaining teeth were ingood condition except for wear due tosleep bruxism. A panoramic radiographshowed an edentulous atrophic poste-rior maxilla with pneumatization andsignificant alveolar bone resorptionin the mandible (Fig. 2). Because offinancial concerns, the patient wantedto have the mandible treated first withan implant-supported complete fixed
y.; Adjunct Professor, Department of Materials

1 Preoperative photographs: frontal view. 2 Preoperative panoramic radiograph.
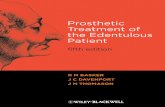
3 Panoramic radiograph after connecting interimabutments to implants.
444 Volume 111 Issue 6
prosthesis and then to have the maxillatreated with a partial removable den-tal prosthesis. An interim mandibularcomplete denture was inserted and re-lined with tissue-conditioning material(Soft-liner; GC Corp) immediately afterextraction of the remaining teeth andwas used for evaluating esthetics,phonetics, and the occlusal verticaldimension. A clear acrylic resin surgicaltemplate (Vertex Rapid Simplified; Ver-tex Dental) was made with a duplicateof the interim denture.
Three months after extraction, 6endosseous dental implants, 10 mmin length and 4.3 mm in diameter(Implantium; Dentium Corp) wereplaced with the 1-stage approach.Because of patient fatigue and reducedtreatment compliance and because ofthe length of surgery, an early loadinginterim denture was planned. After
The Journal of Prosthetic Dentistry
1 week, 6 impression copings (Impres-sion Coping Pick-up; Dentium Corp)were connected to the implantsand used as interim screw-type abut-ments (Fig. 3). The prefabricated fixeddetachable interim prosthesis madeby duplicating the interim completedenture, with access holes for theinterim abutments, was placed andevaluated for proper occlusion andclearance between each access holeand its corresponding interim abut-ment. Successively, autopolymerizedacrylic resin (Jet denture repair resin;Lang Dental Mfg Co) was applied tothe holes, and an interim fixed pros-thesis was placed for 4 months until amaxillary partial removable dentalprosthesis was fabricated.
Subsequently, a definitive man-dibular impression was made witha custom light-polymerized open tray
(Vertex Light Curing Trayplates; VertexDental) and open-tray impression cop-ings (Impression Coping Pick-up; Den-tium Corp). The impression was pouredwith Type IV gypsum material (FujirockEP; GC America Inc) to fabricate thedefinitive cast. Six yellow abutments fordirect milling (Dual Milling abutment;Dentium Corp) with titanium nitridecoating were connected to the implantreplicas on the definitive cast. Thesewere milled with a 2-degree millingbur to fabricate a cement-type zirconiasuperstructure. Subsequently, all theabutments were transferred to the oralcavity, and their positions were con-firmed with an abutment positioningdevice. A centric relation record wasmade with a recording device (GCPattern Resin; GC America Inc), andcasts were mounted in a semiadjustablearticulator (Hanau modular articulator;Whip Mix Corp). An anatomic contourwaxing was made and converted intoan acrylic resin prosthesis (GC Patternresin; GC America Inc) by using puttyindex (Lab Putty; Coltène/Whaledent,Inc). Light-polymerized composite resin(Rigid Transparent þ Blue; Zirkonzhan)was used free hand to correct eachtooth shape. This complete contoursimulation was inserted intraorally toverify the occlusal vertical dimensionand soft-tissue support (Fig. 4). Eachtooth of the simulated restoration wascut back approximately 2.0 mm topermit the fabrication of the definitiverestoration, with the silicone matrix as areference. The acrylic resin framework
Cho and Raigrodski

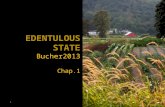
4 Vertical dimension and soft-tissue support evaluation. 5 Scanning of acrylic resin framework.
6 Zirconia framework before final sintering. 7 New centric relation record.
June 2014 445
was scanned (Optical scanner S600;Zirkonzhan), and the CAD/CAM zirco-nia framework was fabricated (Prettau;Zirkonzahn). The intaglio was also cutback for gingival porcelain addition, andthe framework was sintered (Figs. 5, 6).
Once sintering was completed, thezirconia framework was veneered withfeldspathic gingival porcelain (CreationZi-F; Creation Willi Geller Intl GmbH).After verifying the fit of the zirconiaframework on the abutments intra-orally, a new centric relation record wasmade (Fig. 7) and used for remounting.A complete-contour waxing was per-formed on each tooth preparationsimulation of the zirconia framework.Subsequently, lithium disilicate mono-lithic crowns (Emax; Ivoclar Vivadent)were heat pressed to fit each abutment(Fig. 8).
The gingival ceramic around eachmargin of the zirconia tooth simulation
Cho and Raigrodski
was etched for 30 seconds with hydro-fluoric acid, and a primer (Z-Primeplus; Bisco Inc) was applied on theabutment margin. The crowns wereetched for 20 seconds with hydrofluoricacid and silanated. Self-etching, self-adhesive resin cement (Unicem; 3MESPE) was used to bond each mono-lithic lithium disilicate crown to thezirconia framework extraorally. Afterconnecting the custom abutments withthe implants in the oral cavity, theCAD/CAM zirconia framework wascemented onto the abutments withprovisional implant cement (ImplantCement; Premier). To ensure the com-plete removal of residual cement, eachabutment screw was loosened andthe restoration was removed; then itwas reseated, and all the abutmentscrews were tightened to 35 Ncm.Finally, the access holes were filled withcotton pellets, interim composite resin
restorative material (Fermit; IvoclarVivadent), and composite resin restor-ative material (Filtek P60; 3M ESPE)(Figs. 9, 10). The occlusion was refined,and the patient expressed his satisfac-tion with the esthetic and functionaloutcomes. The patient was scheduledfor recall at 6-month intervals andpresented with satisfactory oral hygieneand no mechanical complications atthe 9-month follow-up.
DISCUSSION
In this clinical treatment, eachcrown was fabricated from monolithiclithium disilicate and cemented ontothe framework. Lithium disilicate waschosen for esthetics and strength.35
Clinical studies on monolithic lithiumdisilicate crowns and FDPs have shownpromising results in terms of structuralintegrity.36-38 If chipping or fracture of

9 Complete mandibular prosthesis in process of bondingindividual lithium disilicate crowns.
8 Complete contour waxing and monolithic lithium disilicate crowns.
10 Intraoral occlusal view of complete prosthesis.
446 Volume 111 Issue 6
the crowns occurs, then the prosthesisdesign allows the removal and replace-ment of the crown intraorally, orextraorally by removing the restoration.Another prospective complication withcomplete arch implant-supported FDPsis screw loosening or screw fracture.This type of prosthesis enables retriev-ability and screw management becauseeach access hole is maintained as partof the crown.
The Journal of Prosthetic Dentis
Because crowns on this prosthesiscan be easily replaced compared witha monolithic zirconia prosthesis, er-rors such as deficient occlusal con-tacts on an individual crown can becorrected. The possible disadvantageof this prosthesis is the risk of failurein the bond between the zirconiaframework and the veneering gingivalporcelain. Using individual crowns,as with this prosthesis, may also
try
be more costly than conventionalprostheses.
SUMMARY
This technique combines the CAD/CAM fabrication of a zirconia frame-work for precision with heat-pressedmonolithic lithium disilicate crownsfor esthetics and function. This type ofprosthesis may reduce the likelihood of
Cho and Raigrodski

June 2014 447
porcelain fractures and allow ease ofretrievability.
REFERENCES
1. Adell R, Lekholm U, Rockler B, Bränemark PI.A 15-year study of osseointegrated implantsin the treatment of the edentulous jaw. Int JOral Surg 1981;10:387-416.
2. Adell R, Eriksson B, Lekholm U,Brånemark PI, Jemt T. Long-term follow-upstudy of osseointegrated implants in thetreatment of totally edentulous jaws. Int JOral Maxillofac Implants 1990;5:347-59.
3. Ferrigno N, Laureti M, Fanali S,Grippaudo G. A long-term follow-up study ofnonsubmerge ITI implants in the treatment oftotally edentulous jaws. Part I: ten-year lifetable analysis of a prospective multicenterstudy with 1286 implants. Clin Oral ImplantsRes 2002;13:260-73.
4. Drago C, Saldarriaga RL, Domagala D,Almasri R. Volumetric determination of theamount of misfit in CAD/CAM and castimplant frameworks: a multicenter labora-tory study. Int J Oral Maxillofac Implants2010;25:920-9.
5. Chang PP, Henegbarth EA, Lang LA. Maxil-lary zirconia implant fixed partial denturesopposing an acrylic resin implant fixedcomplete denture: a two-year clinical report.J Prosthet Dent 2007;97:321-30.
6. Al-Fadda SA, Zarb GA, Finer YA. Comparisonof the accuracy of fit of 2 methods forfabricating implant-prosthodontic frame-works. Int J Prosthodont 2007;20:125-31.
7. Drago C, Howell K. Concepts for designingand fabricating metal implant frameworksfor hybrid implant prostheses. J Prosthodont2012;21:413-24.
8. Jemt T, Back T, Petersson A. Precision ofCNC-milled titanium frameworks for implanttreatment in the edentulous jaw. Int J Pros-thodont 1999;12:209-15.
9. Papaspyridakos P, Lal K. Complete archimplant rehabilitation using subtractive rapidprototyping and porcelain fused to zirconiaprosthesis: a clinical report. J Prosthet Dent2008;100:165-72.
10. Hassel AJ, ShahinR, Kreuter A, Rammelsberg P.Rehabilitation of an edentulous mandible withan implant-supported fixed prosthesis using anall-ceramic framework: a case report. Quintes-sence Int 2008;39:421-6.
11. Nakamura K, Kanno T, Milleding P,Ortengren U. Zirconia as a dental implantabutment material: a systematic review. Int JProsthodont 2010;23:299-309.
12. Sailer I, Philipp A, Zembic A, Pjetursson BE,HBE, Hss CH, Zwahlen M. A systematic re-view of the performance of ceramic andmetal implant abutments supporting fixedimplant reconstructions. Clin Oral ImplantsRes 2009;20:4-31.
13. Glauser R, Sailer I, Wohlwend A, Studer S,Schibli M, Scharer P. Experimental zirconiaabutments for implant-supported single-tooth restorations in esthetically demandingregions: 4-year results of a prospective clin-ical study. Int J Prosthodont 2004;17:285-90.
Cho and Raigrodski
14. Jung RE, Sailer I, Hämmerle CH, Attin T,Schmidlin P. In vitro color changes ofsoft tissues caused by restorative materials.Int J Periodontics Restorative Dent2007;27:251-7.
15. Raigrodski AJ, Yu A, Chiche GJ,Hochstedler JL, Mancl LA, Mohamed SE.Clinical efficacy of veneered zirconiumdioxide-based posterior partial fixed dentalprostheses: five-year results. J Prosthet Dent2012;108:214-22.
16. Raigrodski AJ, Hillstead MB, Meng GK,Chung KH. Survival and complications ofzirconia-based fixed dental prostheses: a sys-tematic review. J Prosthet Dent 2012;107:170-7.
17. Flinn BD, deGroot DA, Mancl LA,Raigrodski AJ. Accelerated aging characteris-tics of three yttria-stabilized tetragonal zir-conia polycrystalline dental materials.J Prosthet Dent 2012;108:223-30.
18. Denry I, Kelly JR. State of the art of zirconiafor dental applications. Dent Mater 2008;24:299-307.
19. Fischer J, Stawarczyk B, Trottmann A,Hammerle CH. Impact of thermal propertiesof veneering ceramics on the fracture load oflayered Ce-TZP/A nanocomposite frame-works. Dent Mater 2009;25:326-30.
20. DeHoff PH, Barrett AA, Lee RB, Anusavice KJ.Thermal compatibility of dental ceramicsystems using cylindrical and sphericalgeometries. Dent Mater 2008;24:744-52.
21. Fischer J, Stawarzcyk B, Trottmann A,Hammerle CH. Impact of thermal misfiton shear strength of veneering ceramic/zir-conia composites. Dent Mater 2009;25:419-23.
22. Rosentritt M, Steiger D, Behr M, Handel G,Kolbeck C. Influence of substructure designand spacer settings on the in vitro perfor-mance of molar zirconia crowns. J Dent2009;37:978-83.
23. Manicone PF, Rossi Iommetti P, Raffaelli L.An overview of zirconia ceramics: basicproperties and clinical applications. J Dent2007;35:819-26.
24. Fischer J, Stawarczyk B, Hammerle CH. Flex-ural strength of veneering ceramics for zir-conia. J Dent 2008;36:316-21.
25. Tan JP, Sederstrom D, Polansky JR,McLaren EA, White SN. The use of slowheating and slow cooling regimens tostrengthen porcelain fused to zirconia.J Prosthet Dent 2012;107:163-9.
26. Ansong R, Flinn B, Chung KH, Mancl L,Ishibe M, Raigrodski AJ. Fracture toughnessof heat-pressed and layered ceramics.J Prosthet Dent 2013;109:234-40.
27. Christensen RP, Ploeger BJ. A clinical com-parison of zirconia, metal and alumina fixed-prosthesis frameworks veneered with layeredor pressed ceramic: a three-year report. J AmDent Assoc 2010;1:1317-29.
28. Vigolo P, Mutinelli S. Evaluation ofzirconium-oxide-based ceramic single-unitposterior fixed dental prostheses (FDPs)generated with two CAD/CAM systemscompared to porcelain-fused-to-metal sin-gle-unit posterior FDPs: a 5-year clinicalprospective study. J Prosthodont 2012;21:265-9.
29. Hatta M, Shinya A, Yokoyama D, Gomi H,Vallittu PK, Shinya A. The effect of surfacetreatment on bond strength of layering por-celain and hybrid composite bonded to zir-conium dioxide ceramics. J Prosthodont Res2011;55:146-53.
30. Pjetursson BE, Brägger U, Lang NP,Zwahlen M. Comparison of survival andcomplication rates of tooth-supported fixeddental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs).Clin Oral Implants Res 2007;18(suppl 3):97-113.
31. Rojas-Vizcaya. Full zirconia fixed detachableimplant-retained restorations manufacturedfrom monolithic zirconia: clinical report aftertwo years in service. J Prosthodont 2011;20:570-6.
32. Ishibe M, Raigrodski AJ, Flinn BD,Chung KH, Spiekerman C, Winter RR. Shearbond strengths of pressed and layeredveneering ceramics to high-noble alloy andzirconia cores. J Prosthet Dent 2011;106:29-37.
33. Rosentritt M, Preis V, Behr M, Hahnel S,Handel G, Kolbeck C. Two-body wearof dental porcelain and substructure oxideceramics. Clin Oral Investig 2012;16:935-43.
34. Papaspyridakos P, Chen CJ, Chuang SK,Weber HP, Gallucci GO. A systematic reviewof biologic and technical complications withfixed implant rehabilitations for edentulouspatients. Int J Oral Maxillofac Implants2012;27:102-10.
35. Raigrodski AJ. Contemporary materials andtechnologies for all-ceramic fixed partialdentures: a review of the literature. J ProsthetDent 2004;92:557-62.
36. Fasbinder DJ, Dennison JB, Heys D, Neiva G.A clinical evaluation of chairsidelithium disilicate CAD/CAM crowns: atwo-year report. J Am Dent Assoc 2010;141:10-4.
37. Reich S, Fischer S, Sobotta B, Klapper HU,Gozdowski S. A preliminary study on theshort-term efficacy of chairside computer-aided design/computer-assistedmanufacturing-generated posterior lithiumdisilicate crowns. Int J Prosthodont 2010;23:214-6.
38. Kern M, Sasse M, Wolfart S. Ten-yearoutcome of three-unit fixed dental prosthesesmade from monolithic lithium disilicateceramic. J Am Dent Assoc 2012;143:234-40.
Corresponding author:Dr Youngwook ChoWashington Dental Clinic830-3 Bi-jeon 2-dongPyeongtaek-si, Gyeonggi-doKOREAE-mail: [email protected]
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.