The Ranting Economist · 2012. 8. 8. · The Ranting Economist 3 2. The government response – The...
17
The Ranting Economist Aid-induced Dutch disease: the causes, effects and what can be done about it 1. Introduction In the 1960’s the Dutch discovered large reserves of natural gas off the coast of the North Sea. These vast reserves promised to bring newfound prosperity to the people of the Netherlands but instead caused long-term damage to their domestic industrial structure. However the Netherlands is not alone. Countries that discover, and export, a variety of natural resources – whether it be gas in the Netherlands, oil in Nigeria or iron ore in Australia 1 – have experienced the same thing: a substantial influx of foreign currency which drives up the value of their real exchange rate thus hurting the competitiveness of their other export industries. This phenomenon is called ‘Dutch disease’ – when the appreciation of the real exchange rate, caused by an inflow of foreign currency, hurts the non-booming export sectors of an economy (Gruen, 2011, p.132). However foreign currency inflows can come in many different forms, unrelated to natural resources. And one of those forms is foreign aid. This raises some potentially alarming questions. Could foreign aid actually cause Dutch disease? Could foreign aid, in and of itself, actually cause harm to the countries we are seeking to help? In this paper I will show that, both theoretically and empirically, foreign aid can indeed cause Dutch disease and that it has done so in the past. So does this mean that foreign aid should be stopped? No. Far from it. I will show that, not only are there a variety of policy options available to governments in managing the effects of aid-induced Dutch disease, but that even on an objective scale the costs of Dutch disease to a country’s economy are likely to be far outweighed by the benefits of foreign aid. These conclusions are, of course, not without controversy, and I will explore these issues in turn. First, however, let us explore the theoretical and empirical evidence of aid-induced Dutch disease and the policy responses available to address it.
Transcript of The Ranting Economist · 2012. 8. 8. · The Ranting Economist 3 2. The government response – The...
-
The Ranting Economist
Aid-induced Dutch disease: the causes, effects and what can
be done about it
1. Introduction
In the 1960’s the Dutch discovered large reserves of natural gas off the coast of the
North Sea. These vast reserves promised to bring newfound prosperity to the people of
the Netherlands but instead caused long-term damage to their domestic industrial
structure. However the Netherlands is not alone. Countries that discover, and export, a
variety of natural resources – whether it be gas in the Netherlands, oil in Nigeria or iron
ore in Australia1 – have experienced the same thing: a substantial influx of foreign
currency which drives up the value of their real exchange rate thus hurting the
competitiveness of their other export industries. This phenomenon is called ‘Dutch
disease’ – when the appreciation of the real exchange rate, caused by an inflow of
foreign currency, hurts the non-booming export sectors of an economy (Gruen, 2011,
p.132). However foreign currency inflows can come in many different forms, unrelated
to natural resources. And one of those forms is foreign aid.
This raises some potentially alarming questions. Could foreign aid actually cause Dutch
disease? Could foreign aid, in and of itself, actually cause harm to the countries we are
seeking to help? In this paper I will show that, both theoretically and empirically,
foreign aid can indeed cause Dutch disease and that it has done so in the past. So does
this mean that foreign aid should be stopped? No. Far from it. I will show that, not only
are there a variety of policy options available to governments in managing the effects of
aid-induced Dutch disease, but that even on an objective scale the costs of Dutch
disease to a country’s economy are likely to be far outweighed by the benefits of foreign
aid.
These conclusions are, of course, not without controversy, and I will explore these
issues in turn. First, however, let us explore the theoretical and empirical evidence of
aid-induced Dutch disease and the policy responses available to address it.
-
The Ranting Economist
2
2. The theoretical evidence of aid-induced Dutch disease
An economy’s real exchange rate is given by the simple formula below where E is the
economy’s nominal exchange rate, Pn is the price of non-tradable goods2 and Pt is the
price of tradable goods.3
e = E (Pn / Pt)
An appreciation of an economy’s real exchange rate can therefore come through three
channels: an appreciation of the nominal exchange rate, an increase in the price of non-
tradable goods (domestic inflation) or a fall in the price of tradable goods. The problem
with an appreciated real exchange rate is that it makes goods produced at home
relatively more expensive compared to the same goods produced overseas. This
weakens a country’s ability to compete in international markets thus causing a
contraction in the country’s export industries.4
To explain how this comes about, suppose that a country receives a large amount of
foreign currency from abroad – whether it be in the form of foreign aid or payment for
exported natural resources. The country has to make two separate decisions (Berg et al,
2006, p.2):
1. The central bank response. The government can’t spend foreign currency – it
needs to be exchanged for domestic currency. The central bank therefore needs
to decide whether to absorb the foreign currency into the domestic economy (by
exchanging the foreign currency for domestic currency)5 or not absorb the
currency and instead accumulate foreign exchange reserves.
1 For a discussion on whether Australia is suffering from Dutch disease by virtue of its resource boom,
see Gruen (2011). 2 Non-tradable goods are goods that cannot be traded overseas such as haircuts and house cleaning
services. A key point to understand is that there is no substitution between tradable and non-tradable goods. If the price of haircuts increases you cannot import your haircut instead. 3 Tradable goods are goods that are traded internationally, including tradable services like financial and
investment services. 4 Relatively higher non-tradable goods prices can also result in a resource transfer effect where the
economies resources shift away from export industries towards non-tradable goods sectors (discussed below). 5 This translates to a widening of the current account deficit.
-
The Ranting Economist
3
2. The government response – The government has to decide whether to spend
the money (and widen the fiscal deficit) or not. Fundamentally, we are assuming
that if the government spends the money then it does so, at least in part, on non-
tradable goods. If the government spends all the money on tradable goods
(imports) then there is no effect on the real exchange rate.6
The effect of the inflow of foreign currency on the real exchange rate (and, indeed,
whether or not it triggers Dutch disease) depends on the interplay between these two
responses. The corresponding scenarios for the real exchange rate are illustrated in the
matrix below.
SCENARIO 1: Absorb and spend. Under this scenario the central bank absorbs the
foreign currency. The central bank sells the currency in foreign exchange markets in
exchange for local currency which it gives to the government. The effect of this is an
increased demand for local currency which causes an appreciation of the nominal
exchange rate. As per the formula above, this results in an appreciation of the real
exchange rate. Simultaneously, however, the government spends its newfound wealth
on goods and services for its people. This increases aggregate demand which pushes up
the price of non-tradable goods causing domestic inflation.7 As per the formula above,
6 This assumes a small open economy that cannot influence international prices. This is a realistic
assumption for the majority of developing countries which are the recipients of foreign aid. 7 An appreciated exchange rate caused by higher relative prices of non-tradable goods can also result in
what Cordon and Neary (1982) call ‘the resource transfer effect’. Because non-tradable goods receive a higher price compared to tradable goods this results in the economies’ resources being transferred
-
The Ranting Economist
4
this also results in an appreciation of the real exchange rate. This scenario therefore
results in an unambiguous appreciation of the real exchange rate.
SCENARIO 2: Neither absorb nor spend. Under this scenario the central bank does
not absorb the foreign currency and the government does not spend the money. The
effect is that the country accumulates foreign exchange reserves and there is no effect on
the real exchange rate.
SCENARIO 3: Spend but do not absorb. This scenario is the equivalent of fiscal
stimulus (Berg et al, 2006, p.3). The government finances a fiscal expansion by
borrowing from the central bank. Because the central bank has not absorbed the money,
it effectively prints domestic currency for the government to spend. The increase in
government spending increases aggregate demand which, again, causes inflation by
increasing the price of non-tradables. However the expansion in the money supply also
causes inflation. The result is therefore a double-whammy of inflation for the local
economy which causes an appreciation of the real exchange rate.
SCENARIO 4: Absorb but do not spend. If the central bank absorbs the foreign
currency without any increase in government spending, then the government has
effectively increased its deposits with the central bank (Berg et al, 2006, p.11). With no
increase in government spending there is no increase in inflation. However the central
banks’ decision to absorb the currency has two effects: (1) the increased demand for the
local currency causes an appreciation of the nominal exchange rate; and (2) the money
supply is effectively contracted since the central bank has withdrawn money from
circulation without any increase in government spending. This causes deflation. The
overall effect on the real exchange rate is therefore ambiguous.
We can now see the theoretical evidence behind aid-induced Dutch disease. The key
problem with foreign aid is that it tends to come in foreign currency.8 In the context of
the real exchange rate, foreign aid is no different than the exporting of natural resources.
Both result in an inflow of foreign currency and both have the potential to cause an
away from the country’s export sectors towards its non-tradable goods sectors. This can cause long-term damage to a country’s international competitiveness which can be difficult to reverse.
-
The Ranting Economist
5
appreciation of the real exchange rate. Whether one of the above four scenarios is
preferable to the others depends on the macroeconomic circumstances of the country in
question. This is discussed in detail in section 4 in regards to the appropriate policy
responses to Dutch disease. First, however, let us consider the empirical evidence of
Dutch disease.
3. The empirical evidence of aid-induced Dutch disease
In this section I will explore the studies which have found evidence of aid-induced
Dutch disease, compare them to the studies that have found no evidence of aid-induced
Dutch disease and then show that much of the contradiction between these studies can
be explained by three key variables.
Empirical studies evidencing Dutch disease
A cross-country study by Rajan and Subramanian (Rajan and Subramanian, 2009)
looked at the effects of foreign aid on manufacturing growth. The study found that aid
inflows have systematically adverse effects on a country’s competitiveness, reflected by
a lower relative growth rate of export industries. Fundamentally, the study found that
the key channel for this reduction in competitiveness was the appreciation of the real
exchange rate which was, in turn, caused by aid inflows (Rajan and Subramanian, 2009,
p.4).9 Specifically, Rajan and Subramanian found that, across aid-recipient countries,
the more aid a country received the smaller was its manufacturing sectors’ share of GDP
(Rajan and Subramanian, 2009, p.1).10
On review of the literature on this topic, Riddell similarly found that ‘...there is
significant country-based and cross-country evidence documenting the occurrence of
Dutch disease in aid-recipient countries’ (Riddell, 2007, p.227). One example is a 2006
study by Berg et al which focused on the experiences of Ethiopia, Ghana, Mozambique,
8 Aid can, of course, come in the form of goods and services which does not involve any currency.
9 Rajan and Subramanian go one step further to suggest that their results help explain the micro-macro
paradox of foreign aid. 10
They found that a one percentage point increase in the aid-to-GDP ratio is associated with a reduced share of manufacturing in total GDP of 0.2 to 0.3 percentage points (Rajan and Subramanian, 2009, p.15).
-
The Ranting Economist
6
Tanzania and Uganda – five countries which all faced a surge in foreign aid around the
same time (2005). The study found that each of these countries faced similar pressures,
all consistent with Dutch disease, although how each them responded differed markedly
(Berg et al, 2006, p.2) (discussed in section 4).
Empirical studies finding no evidence of Dutch disease
For every study that finds evidence of aid-induced Dutch disease there seems to be
another that finds evidence against it. Barder’s 2006 paper with the Centre for Global
Development is one such example. Barder finds that ‘it is unlikely that a long-term,
sustained and predictable increase in aid would, through the impact on the real the
exchange rate, cause more harm than good’(Barder, 2006, p.3). Barder’s analysis finds
that aid to Africa has often been associated with a depreciation of the real exchange
rate, not an appreciation. He finds that, based on cross-country regression analysis, there
is little evidence that increases in aid are in any way correlated with an overvaluation of
the exchange rate (Barder, 2006, p.12). Berg et al similarly finds that, over their sample
of countries in 2006, the real exchange rate remained relatively constant (Berg et al,
2006, p.3).
This raises the following question: in light of clear theoretical evidence of the potential
for aid-induced Dutch disease, can we explain the contradictions between empirical
studies that do find evidence of aid-induced Dutch disease and empirical studies that do
not?
Reasons for the contradiction
Conflicting cross-country empirical evidence is nothing new when it comes to aid
literature. However if we look specifically at the studies that focus on aid-induced
Dutch disease we can identify three key factors that drive these contradictory findings.
1. Countries can, and do, manage Dutch disease
Put simply, one reason that the effects of Dutch disease are often not detected is because
countries actively implement policies that address the effects of Dutch disease. The
study by Berg et al, for example, found ‘no evidence of aid-related Dutch disease in the
-
The Ranting Economist
7
sample of countries’ but then notes that ‘this is due in large part to the policy decision
[among the sample countries] to accumulate reserves rather than fully absorbing the aid’
(Berg et al, 2006, p.3). Perkins et al similarly concluded that in many countries where
Dutch disease has been found it has been quite effectively managed and therefore
difficult to detect (Perkins et al, 2006, pp.681-683).
2. The micro-macro paradox and statistical limitations
Foreign aid is inherently characterised by a micro-macro paradox – that although the
effects of aid are observable on a micro, country-specific scale they are often difficult to
observe on a global macro scale (Mosley, 2009, p.3). The same issue applies to Dutch
disease. Because of the numerous variables that affect a country’s real exchange rate
and its economy generally, the vast amount of statistical noise makes it difficult to
establish a clear relationship between aid flows and real exchange rate appreciations. To
this end, Adam and Bevan point out that the relationship between enhanced aid flows
and real exchange rates is much less straightforward than the simple models used by
many authors suggest (Adam and Bevan, 2004, p.11). Barder similarly highlights the
difficulty in disentangling the effects of aid on exchange rates and points out the
potential for reverse causality to further cloud the statistical waters – that countries with
poor export performance may attract aid, rather than aid causing poor export
performance (Barder, 2006, p.7).
3. Country specific circumstances
Finally, country-specific circumstances play a significant role in how large an effect aid
will have on a country’s real exchange rate (Perkins et al, 2006, p.228). This is apparent
when you compare the experience of Indonesia to that of Nigeria – something I will do
in the next section.
Overall there are a number of studies that show that there is significant country-based
and cross-country evidence documenting the occurrence of Dutch disease in aid
recipient countries. However the Dutch disease phenomenon is by no means universal –
and there are many reasons why some studies, particularly studies based on cross-
country regressions, may fail to pick up on them (Perkins et al, 2006, pp.681-683). In
-
The Ranting Economist
8
the next section I will consider more of these specific country examples in the context
of how countries can, and have, dealt with the effects of aid-induced Dutch disease.
4. What to do if you catch Dutch disease
The contrasting experiences of Indonesia and Nigeria
As with many countries at the time, Indonesia and Nigeria both experience substantial
oil windfalls during the OPEC oil embargo in 1973 and the Iranian revolution in 1979.
During the first windfall in 1973 the Indonesian government spent around 60% of its
newfound wealth and experienced a real exchange rate appreciation of around 30% –
slightly greater than that experienced by Nigeria (Perkins et al, 2006, p.680). Both
Indonesia and Nigeria therefore began from a similar starting point. However the
government response, central bank response and country-specific circumstances
differed significantly.
Legislative controls in the Indonesian Parliament required the government to balance its
budget year-on-year which acted to restrain government spending (Perkins et al, 2006,
p.680). Furthermore the Indonesian government used its revenues to invest heavily in
agriculture such as irrigation systems, roads, fertilizers and rural credit infrastructure. At
the same time the central bank undertook strict management of the money supply in
order to protect Indonesia’s foreign exchange reserves. The central bank also undertook
to devalue its currency so as to limit the appreciation of the real exchange rate (Perkins
et al, 2006, p.680).
Through a shrewd and coordinated policy response the Indonesian government was
highly effective at mitigating Dutch disease. By 1983 agricultural output increased by a
third and Indonesia become self-sufficient in rice production. Furthermore by the end of
the boom the real exchange rate had actually depreciated by 8 per cent while non-oil
exports actually increased by 7 per cent (Perkins et al, 2006, p.680) – the polar opposite
to Dutch disease symptoms. However the economic circumstances of Indonesia also
assisted in this regard. The substantial workforce available in the agricultural sector –
around two-thirds of its total workforce – dampened any tendencies for surges in wages
and prices and thus inflation. The Indonesian Government also placed great stress on
-
The Ranting Economist
9
integrating ethnic groups to prevent conflicts over the distribution of oil revenues
(Perkins et al, 2006, p.680).
The Nigerian Dutch disease experience was sadly much more severe. Nigeria’s political
history is characterised by intense competition among ethnic groups and the government
responded to this by spending all of its oil revenues in an effort to appease rival groups.
Public investment rose from 4 to 30 per cent and public sector wages doubled. Much of
the newfound wealth was squandered on wasteful projects (Perkins et al, 2006, p.682).
Furthermore, during this period the central bank maintained its fixed exchange rate
which, in the context of a substantial widening of the fiscal deficit, saw a massive surge
in inflation. This saw the real exchange rate appreciate by three-fold thus killing off
Nigeria’s non-oil exports which saw a staggering 90 per cent fall in production (Perkins
et al, 2006, p.680). For this reason, many economists argue that the oil boom made
Nigeria significantly worse off.
Despite these being in the context of natural resources, the contrasting experiences of
Indonesia and Nigeria highlight the importance of the country-specific circumstances in
how a country is affected by aid-induced Dutch disease. However it also highlights
some of the specific policies that countries should undertake in response to Dutch
disease symptoms. Let us now explore some of these policies further.
Coordinating and targeting fiscal and monetary policy
A country’s response to Dutch disease needs to be effectively coordinated between the
government and the central bank. However the responses of the government and central
bank also need to be independently well targeted.
A coordinated response
The four scenarios I highlighted in section 2 show that the effects of Dutch disease can
be substantially different depending on the interplay between the government’s
response and the response of the central bank. A good example is the ‘spend but don’t
absorb’ scenario. This scenario is problematic given the double-whammy of inflation it
generates. However Berg et al shows that, despite this, ‘spend but don’t absorb’ is
actually a common response among aid-recipient countries and that this is generally
-
The Ranting Economist
10
because of inadequate coordination between the government and central bank (Berg et
al, 2006, p.3).
Fundamentally, the coordinated response which is chosen by a country needs to be
appropriate for the country’s specific circumstances. A country like Zimbabwe, for
example, which has struggled to control inflation, would be unwise to adopt this ‘spend
but don’t absorb’ response. Similarly a country like Somalia, where starvation is
threatening the lives of over a million people, would be unwise to accumulate foreign
reserves instead of spending aid dollars on its people.
A well targeted response
While it is important that the government and central bank coordinate their responses,
their individual responses also need to be well targeted. In the context of the central
bank, this generally means using monetary policy to reverse the effects of the real
exchange rate appreciation. This typically involves a devaluation of the country’s
currency (Riddell, 2007, p.682).11
The central bank similarly needs to show strong
restraint in terms of expanding the money supply. As was the case with Indonesia, this
has significant effects in terms of curbing inflationary pressures that can further
appreciate the real exchange rate (Perkins et al, 2006, p.680).
In the context of the government, a well targeted response involves spending aid money
on projects and activities that target the supply side and improve the economies’
productivity thus offsetting the losses in competitiveness caused by an appreciated real
exchange rate (Barder, 2006, p.3). Barder found that the governments that were the
most successful in dealing with Dutch disease were those that funnelled funds into
health, education and infrastructure – all of which help boost the productivity, and
hence competitiveness, of the tradables sector (Barder, 2006, pp.2-5).
11 A key reason Nigeria suffered such a significant real exchange rate appreciation compared to
Indonesia is because the latter devalued its nominal exchange rate while the former maintained its fixed exchange rate.
-
The Ranting Economist
11
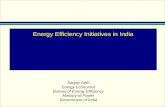
Managing volatile aid flows
Aid flows vary markedly year-on-year and many suggest that this volatility is in fact
getting worse, not better (Hudson and Mosely, 2006). The graph below shows the stark
volatility of international aid from 1996 to 2008 for Burundi, the Central African
Republic, Guinea-Bissau and Haiti.
Source: World Bank (2008)
The volatility and unpredictability of aid exacerbates the effects of Dutch disease. A
country’s ability to respond to the effects of Dutch disease in a targeted and coordinated
way is made all the more difficult when aid flows are volatile and hard to predict. The
text book response of developing countries to aid inflows is often said to be ‘spend and
absorb’. However, in the short- to medium-term, this response is actually quite rare
(Berg et al, 2006, p.2). In the sample of countries used by Berg et al only a minority of
countries actually did this with the majority of countries instead accumulating foreign
exchange reserves so as to better manage volatile aid flows. Ethiopia and Ghana, for
example, accumulated foreign reserves to bolster the exchange rate peg against the
dollar and manage volatile aid flows, respectively (Berg et al, 2006, p.2).
-
The Ranting Economist
12
These issues highlight two key points. First, the volatility and predictability of aid needs
to be addressed, in line with the fundamental principles of the Paris Declaration12
. And
second, to the extent that these issues are not addressed, countries need to be permitted,
and indeed encouraged, to manage their aid flows effectively. If aid flows are
excessively volatile, then recipient countries should build foreign reserves and use those
reserves to smooth spending and absorption (Berg et al, 2006, p.3). However this can be
politically difficult as donors demand that their aid dollars be used when and where they
dictate – not to mention the risk that aid will not be provided if countries are seen to be
accumulating reserves instead of abiding by their donors wishes. Put simply, fungibility
is not necessarily a bad thing (Pettersson, 2004). By allowing aid to be more fungible (at
least in the short-to-medium run) donors are giving countries the slack required to better
manage their economies.
5. Dutch disease in perspective
So far I have explored the causes, consequences, evidence and remedies for Dutch
disease but have not yet explored whether, in weighing up the costs and benefits of
foreign aid, Dutch disease is actually a problem.
To properly understand the Dutch disease phenomenon we need to understand that it is
inherently a trade-off problem. The most effective way of avoiding aid-induced Dutch
disease is to simply neither absorb nor spend the aid in the first place. However by
neither spending nor absorbing foreign aid the country forgoes the very reason aid was
given in the first place – the benefits of enhanced welfare of its citizens. Whether Dutch
disease is a problem will therefore depend on the relative magnitude of these two effects
(Barder, 2006, p.9).
So which, then, is larger? Do the benefits of foreign aid outweigh the costs of Dutch
disease or is it the other way around? A number of studies find that, in general, even on
pessimistic assumptions the additional consumption and investment which is financed
by aid more than outweighs any likely adverse effects of Dutch disease (Barder, 2006,
p.1). However although these studies are insightful, realistically the answer is likely to
12 The Paris Declaration on Aid Effectiveness, 2005.
-
The Ranting Economist
13
be much more complicated than this. The benefits of foreign aid is a hotly contested
topic and, as discussed earlier, measuring the costs of Dutch disease (and observing
those costs empirically) is a difficult exercise.13
Realistically, whether the benefits of aid will outweigh the costs of Dutch disease will
likely depend on a whole range of factors. What we can say, however, is that there will
be a point – a value of aid-to-GDP – where the costs of foreign aid will begin to
outweigh the benefits. This is because as we increase the aid-to-GDP ratio the benefits
of aid are diminishing while the costs of aid are rising. As countries receive more and
more foreign aid their economies’ absorptive capacity begins to reach its limits – the
first million dollars of aid is substantially more effective than the one-thousandth (see
Radelet et al, 2005). However for Dutch disease the reverse is true. As countries face
larger and larger inflows of foreign currency their ability to manage those inflows
becomes less and less – a country, for example, can only devalue its exchange rate by so
much. The result is that, beyond a certain point, foreign aid will do more damage than
good.
Luckily, most studies suggest that this point is likely to occur at a very high level of aid-
to-GDP (see Gomanee et al, 2003). However this does not mean that aid-induced Dutch
disease is not a problem. As discussed earlier, if left unchecked and un-managed, the
costs of Dutch disease can quickly escalate thus reducing the net-benefit of aid. By
properly managing the effects of Dutch disease countries can ensure that the benefits of
foreign aid can be maximised.
13 Something I haven’t discussed is the distribution of these costs and benefits. The case of Nigeria
highlights that the beneficiaries of foreign aid tend to be those who are politically relevant (poor rural farmers, for example, received very little of the government’s spending of its oil windfalls). Dutch disease similarly has an uneven distribution with those in export-dependent industries being hurt far more than those that manufacture goods for domestic consumption. This inequality of distribution should be kept in mind when we talk about comparing the costs and benefits of foreign aid.
-
The Ranting Economist
14
6. Conclusion
Aid-induced Dutch disease is a scary thought – and there is no shortage of
commentators who are willing to use that fear to jump to alarmist conclusions that the
whole idea of aid should be abandoned as result.14
However the cooler-headed among
us know that, although aid-induced Dutch-disease can cause serious damage to an
economy, at the end of the day it is simply a risk that has to be managed.
Furthermore there are many ways in which this risk can be managed. Although I’ve
shown (in the context of Indonesia and Nigeria) that a country’s specific
macroeconomic circumstances are important, I have outlined four key ways in which
the effects of Dutch disease can be managed and mitigated. These are:
by ensuring that the central bank and government coordinate their response and
that their response is appropriate for their country’s macroeconomic
circumstances;
by ensuring that government spending is restrained and well targeted to areas
that will improve productivity and international competitiveness;
by ensuring that the central bank shows restraint in expanding the money supply
and uses its policy tools to address a real exchange rate appreciation, such as
through a devaluation of its currency; and
by ensuring that aid-recipients have the policy and political flexibility to manage
volatile and unpredictable aid flows.
Dutch disease is a short-term problem for a long-term benefit. But only by properly
managing the effects of Dutch disease can the full benefits of aid be realised.
14 For example, Dambisa Moyo in Dead Aid uses Dutch disease as evidence of the damage aid causes to
developing countries and uses this in her overall argument that ‘the aid taps should be shut off’ (Moyo, 2009, p.144).
-
The Ranting Economist
15
7. References
Adam, Christopher S; Bevan, David L; Aid and the supply side: Public investment,
export performance and Dutch disease in low income countries, Department of
Economics, University of Oxford, August 2004, Discussion Paper Series. Date visited:
13 October 2011, available at: http://economics.ouls.ox.ac.uk/12117/1/paper201.pdf
Barder, Owen, A policymaker’s guide to Dutch disease, Center for Global
Development, Working Paper Number 91, July 2006. Date visited: 13 October 2011,
available at: http://www.cgdev.org/files/8709_file_WP91.pdf
Berg, Andrew et al, The macroeconomics of managing increased aid inflows:
experience of low-income countries and policy implications, International Monetary
Fund, WIDER Conference on Aid, June 2006. Date visited, 13 October 2011, available
at: http://sarpn.org/documents/d0002059/IMF_Macroeconomics_Jun2006.pdf
Cordon and Neary, Booming Sector and De-Industrialisation in a small open economy,
Economic Journal, December, Vol. 92, No. 368 (1982) pp.825-48. Date visited: 13
October 2011, available at: http://www.jstor.org/stable/2232670
Gomanee, Karuna et al, Searching for aid threshold effects, CREDIT Research Paper
No. 03/15, September 2003. Date visited: 13 October 2011, available at:
http://papers.ssrn.com/sol3/papers.cfm?abstract_id=482461
Gruen, David, The resources boom and structural change in the Australian economy,
Department of the Treasury (Australia), 24 February 2011. Date visited: 13 October
2011. Available at: http://www.treasury.gov.au/documents/2130/PDF/06_gruen.pdf.
http://economics.ouls.ox.ac.uk/12117/1/paper201.pdfhttp://www.cgdev.org/files/8709_file_WP91.pdfhttp://sarpn.org/documents/d0002059/IMF_Macroeconomics_Jun2006.pdfhttp://www.jstor.org/stable/2232670http://papers.ssrn.com/sol3/papers.cfm?abstract_id=482461http://www.treasury.gov.au/documents/2130/PDF/06_gruen.pdf
-
The Ranting Economist
16
Mankiw, Gregory N., Macroeconomics, 5th Edition, 2003, Worth Publishers
Mosley, Paul, Aid effectiveness: The micro-macro paradox, IDS Bulletin, Volume 17,
Issue 2, pp22-27, April 1986. Date visited: 13 October 2011, available at:
http://onlinelibrary.wiley.com/doi/10.1111/j.1759-5436.1986.mp17002004.x/abstract.
Moyo, Dambisa, Dead Aid: why aid is not working and how there is a better way for
Africa, Farrar, Straus and Giroux, 2009.
Perkins, Dwight H, Radelet, Steven and Lindauer, David L., Economics of
Development, 6th Edition, 2006, W. W. Norton & Company.
Pettersson, Jan, Foreign sectoral aid fungibility, growth and poverty reduction,
Department of Economics, Stockholm University, 1 June 2004. Date Visited: 13
October 2011, available at: http://www.eea-esem.com/papers/eea-
esem/2004/2604/fungJune04.pdf
Rajan, Raghuram G; Subramanian, Arvind, Aid, Dutch disease, and manufacturing
growth, Journal of Development Economics, December 2009. Date visited: 13 October
2011, available at: http://www.iie.com/publications/papers/subramanian0606.pdf
Riddell, Roger C, Does foreign aid really work?, Oxford University Press, New York
2007.
http://onlinelibrary.wiley.com/doi/10.1111/j.1759-5436.1986.mp17002004.x/abstracthttp://www.eea-esem.com/papers/eea-esem/2004/2604/fungJune04.pdfhttp://www.eea-esem.com/papers/eea-esem/2004/2604/fungJune04.pdfhttp://www.iie.com/publications/papers/subramanian0606.pdf
-
The Ranting Economist
17
Sachs, Jeffrey D, The end of poverty: how we can make it happen in our lifetime,
Penguin Group, 2005
Radelet, Steven; Clemens, Michael, Bhavnani, Rikhil, Aid and Growth: New evidence
shows that aid flows aimed at growth have produced results, International Monetary
Fund: Finance and Development, September 2005, Volume 42, Number 3. Date visited:
13 October 2011, available at:
http://www.imf.org/external/pubs/ft/fandd/2005/09/radelet.htm
Graph source:
Appelbaum, Binyamin, How to rebuild a war-torn nation, image sourced from World
Bank data. Date visited, 13 October 2011, available at:
http://rohitkumarsviews.wordpress.com/2011/04/12/how-to-rebuild-a-war-torn-nation/
http://www.imf.org/external/pubs/ft/fandd/2005/09/radelet.htmhttp://rohitkumarsviews.wordpress.com/2011/04/12/how-to-rebuild-a-war-torn-nation/