
The Quality Payment Program - h1ccp.comh1ccp.com/util/slides/QPP_Powerpoint_For_Dispersal.pdfThe...
53
The Quality Payment Program American Geriatrics Society Webinar November 30, 2016 Alan Lazaroff, MD AGS Board Member Physician Health Partners Denver, CO Paul Rudolf, MD, JD Partner Arnold & Porter LLP Washington, DC
Transcript of The Quality Payment Program - h1ccp.comh1ccp.com/util/slides/QPP_Powerpoint_For_Dispersal.pdfThe...

The Quality Payment ProgramAmerican Geriatrics Society Webinar
November 30, 2016
Alan Lazaroff, MDAGS Board MemberPhysician Health PartnersDenver, CO
Paul Rudolf, MD, JDPartnerArnold & Porter LLPWashington, DC

Webinar Planning Committee and Faculty Disclosures
2
The following webinar planning committee members and webinar faculty have indicated that they (and/or their spouses/partners) have no affiliation with, or financial interest in, any commercial interest that may have direct interest in the subject matter of their presentation(s):
Planning Committee: Michael Malone, MD
Faculty: Alan Lazaroff, MD Paul Rudolf, MD, JD
The following webinar planning committee member has indicated that they have a potential conflict of interest to report: Jen Madsen: Advisor: Lundbeck Pharmaceuticals and Roche Diagnostics.

Medicare and CHIP Access and Reauthorization Act of 2015 (MACRA)
Eliminated the (Un)Sustainable Growth Rate & Created the Quality Payment Program (QPP)

QPP and the Physician Fee Schedule4
MACRA affects only Medicare fee-for-service payments to physicians on the Physician Fee Schedule (PFS) – not payments to physicians by Medicare Advantage plans or PACE
QPP replaces the (un)Sustainable Growth Rate formula Medicare used to pay physicians on the PFS
During the transition to the QPP, Congress set a (small) stable update: +0.5% each year in 2016 - 2018
MACRA’s new payment policies begin Jan. 1, 2019 But those payments are based on performance in CY 2017 Your success in the first year of QPP depends on successfully
participating during 2017 – potentially as soon as January 1!

QPP Has Two Tracks: Both Have Upside & Downside Financial Risk
5
Two tracks to the QPP: Merit-Based Incentive Payment System (MIPS) Alternative Payment Models (APMs) MIPS APMs
UPSIDE Payment adjustments of +4% to +9% for those whose performance meets or exceeds the performance threshold
Additional bonus for highest performers
Medicare pays a bonus of 5% of total Part B billings for the year based upon participation in APMs
Must be a “qualifying participant” in an “Advanced APM”
DOWNSIDE Payment adjustments of -4% to -9% for those whose performance is below the performance threshold
Maximum penalty for failure to report
Advanced APMs must accept downside financial risk or be a Comprehensive Primary Care Plus (CPC+) medical home
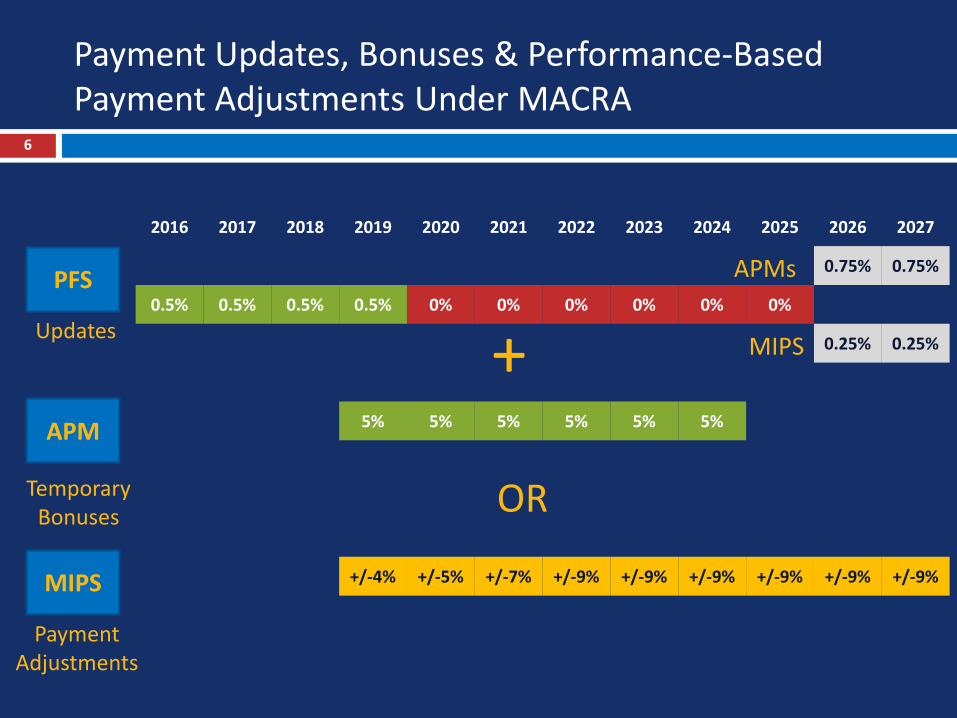
Payment Updates, Bonuses & Performance-Based Payment Adjustments Under MACRA
6
PFS
APM
MIPS
Updates
Temporary Bonuses
Payment Adjustments
2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027
0.75% 0.75%
0.5% 0.5% 0.5% 0.5% 0% 0% 0% 0% 0% 0%
0.25% 0.25%
5% 5% 5% 5% 5% 5%
+/-4% +/-5% +/-7% +/-9% +/-9% +/-9% +/-9% +/-9% +/-9%
+APMs
OR
MIPS

MIPS & APMs Have Many More Similarities7

Advanced APMs for 20178
Comprehensive ESRD Care (CEC) - Two-Sided Risk Comprehensive Primary Care Plus (CPC+) Next Generation ACO Model Shared Savings Program - Track 2 Shared Savings Program - Track 3 Oncology Care Model (OCM) - Two-Sided Risk This list may change. CMS plans to publish a final
list before January 1, 2017.

Understanding Your Choices9
Eligible clinicians must choose a path. Here’s how:
1. Determine if you are in an Advanced APM. CMS has announced the Advanced APMs for 2017; if you are not enrolled in one already, you cannot join until 2018. A list of 2017 Advanced APMs is in Appendix 2. CMS estimates that ~3.5% of geriatricians will be Qualifying Participants
in Advanced APMs in 2017.
2. Determine if you are excluded from MIPS. Two groups of clinicians are excluded from MIPS:A. New In Practice – first year billing MedicareB. Low Volume Threshold – Less than $30,000 OR 100 Medicare patients
seen in a year (from 9/1/2015 to 8/30/2016) CMS estimates that 70% of geriatricians will be in MIPS; remainder are
excluded.
If you are in MIPS, here’s what you need to know:

MIPS: 4 Performance Categories10
Report Quality Measures (Like PQRS)
CMS Calculates Using Claims(Like Value Modifier)
Replaces EHR Incentive Program & Meaningful Use
New Category for Clinical Practice Improvement

Several Reporting Methods Available in 201711
Individuals Groups
• Claims• Registries• EHR Vendors
• No Claims• Registries• EHR Vendors• CMS Website (Groups of 25+)• CAHPS Survey Vendors
• Claims • Claims
• Attestation• Registries• EHR Vendors
• Attestation• Registries• EHR Vendors• CMS Website (Groups of 25+)
• Attestation• Registries• EHR Vendors• Claims
• Attestation• Registries• EHR Vendors• CMS Website (Groups of 25+)

3. Choose Individual or Group Reporting
12
Like PQRS, you may report as an individual, or as part of a group; administrative burden may be lower for groups.
Low-volume threshold criteria of $30,000 Part B allowables or <100 Medicare patients applies to you as an individual: if you meet criteria, you’re excluded from MIPS.
HOWEVER, if you report as a group, the low-volume threshold applies at the level of the group.
If your group reports as a group, and exceeds the $30,000 / 100 patient thresholds, you will be evaluated under MIPS performance categories even though individually you would have been excluded from MIPS.
Your payment adjustment will reflect the group’s performance on the MIPS performance categories.

4. Avoid a MIPS Payment Penalty13
For 2017, CMS established a revised scoring methodology to minimize penalties, which by statute would be -4% for MIPS-eligible clinicians who do not participate: Any MIPS-eligible clinician who reports:
1 quality measure, 1 improvement activity, or required EHRmeasures is eligible to receive a neutral or (small) positive payment adjustment.
Payment penalties will only be assigned if you do nothing!
However, the rules get more complicated in the future.

Summary: How to Get Ready for MIPS in 201714
2017 is a transition year; requirements will increase in future and CMS will be less flexible – now is the time to learn!
Get educated! Lots of information at www.qpp.cms.gov
Understand your choices and pick a path for participation
Choose measures. Pick from lists at www.qpp.cms.gov
Review your past years’ Quality and Resource Utilization Reports (QRURs)
Look yourself up on Physician Compare:
https://www.medicare.gov/physiciancompare/search.html

Preparing for MIPS: The Long View15

MIPS Requirements: Quality Performance Category
16
Basic Requirements Weight in 2017
For 50% of patients seen in the year (across ALL payers) (increases to 60% in 2018):• Report 6 quality measures via EHR or registry or web (1 must
be outcome measure) OR
• Report specialty-specific measure set
• In 2017, performance compared to benchmarks will be scored from 3 to 10 points, in deciles
• If clinician submits at least 1 measure: 3 points
• If clinician submits no data: 0 points
• Groups of 16+ will be assessed on all-cause readmissions (from claims) for min. 200 cases
60%

Choose Your Measures from qpp.cms.gov 17
1. Search or Browse
2. Choose 6 or More
3. Download Specs
4. Collect the Data in Your Systems
5. Report to CMS

Quality Measures for Geriatrics18
Top 5 Quality Measures Reported by Geriatricians in 2014
Documentation of Current Medications in the Medical Record
Preventive Care and Screening: Influenza Immunization
Preventive Care and Screening: BMI Screening and Follow-Up Plan
Preventive Care and Screening: Tobacco Use
Diabetes: Hemoglobin A1c Poor Control
• The top 5 most frequently chosen quality measures for geriatricians were very popular with all clinicians.
• All 5 were reported by at least 13.5% of clinicians (influenza) and up to 25.7% (medications).

Process Measures for Geriatrics19
Medication reconciliation post-discharge Advance care plan documented or discussed Proportion receiving chemotherapy in last 14
days of life Proportion not admitted to hospice Plan of care for urinary incontinence in
women 65+ Function and pain assessment for
osteoarthritis Pneumonia vaccination Pain assessment and follow-up Falls plan of care Diabetes: foot exam Functional outcome assessment Use of high-risk medications in elderly Sleep apnea assessment
Dementia: functional status; neuropsychiatric symptom assessment; cognitive assessment; management of neuropsychiatric symptoms; counseling re: safety concerns; caregiver education and support
Parkinson’s: psychiatric symptoms assessment; cognitive impairment assessment; rehabilitative therapy options
Screening: depression and follow up plan; use of PHQ-9 tool; high blood pressure; falls risk; suicide risk; urinary incontinence; elder maltreatment; osteoporosis
Opioids: follow-up evaluation after treatment; documentation of signed opioid treatment agreement; risk of opioid abuse evaluation
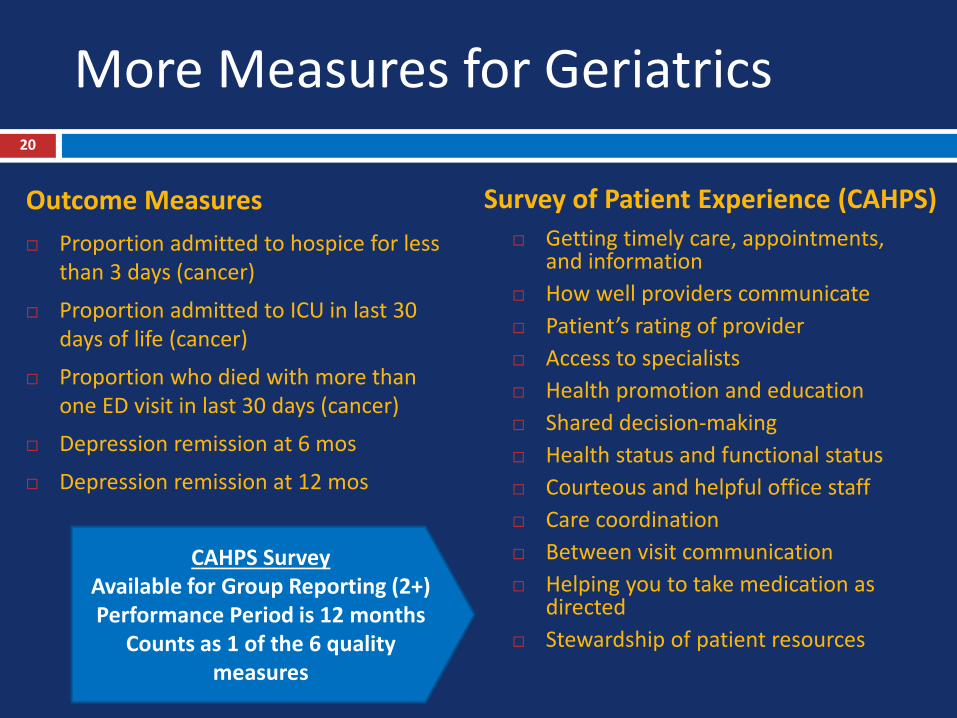
More Measures for Geriatrics20
Outcome Measures Proportion admitted to hospice for less
than 3 days (cancer)
Proportion admitted to ICU in last 30 days of life (cancer)
Proportion who died with more than one ED visit in last 30 days (cancer)
Depression remission at 6 mos
Depression remission at 12 mos
Survey of Patient Experience (CAHPS) Getting timely care, appointments,
and information How well providers communicate Patient’s rating of provider Access to specialists Health promotion and education Shared decision-making Health status and functional status Courteous and helpful office staff Care coordination Between visit communication Helping you to take medication as
directed Stewardship of patient resources
CAHPS SurveyAvailable for Group Reporting (2+)Performance Period is 12 months
Counts as 1 of the 6 quality measures

CMS-Approved CAHPS Survey Vendors (2016)
21
Center for the Study of Serviceswww.cssresearch.orgDataStat, Inc.www.datastat.comDSS Researchwww.dssresearch.comHealthStreamwww.healthstream.comManagement and Technology Consultants, LLChttp://www.mtchealth.com/MetrixMatrix, Inc.www.metrixmatrix.comNational Research Corporationwww.nationalresearch.comNovaetus, Inc.http://www.novaetus.com/
Percy & Company Market Researchhttp://www.percyandcompany.com/Press Ganey Associateswww.pressganey.comProfessional Research Consultants, Inc.www.PRCCustomResearch.comResearch & Marketing Strategies, Inc.www.rmsresults.comSPH Analytics www.sphanalytics.comSullivanLuallin Groupwww.sullivanluallingroup.comThe Jackson Group, a BivarusCompanythejacksongroup.com

Specialty Measure Sets22
Reporting all of the measures in a specialty measure set will satisfy requirements, if the specialty has fewer than 6 measures (true for many sub-specialists).
AGS is developing a list of measures geriatrics professionals will be well positioned to report successfully.
The list will be on our website in 2017.
Allergy / Immunology Plastic Surgery
Anesthesiology Preventive Medicine
Cardiology Neurology
Gastroenterology Mental / Behavioral Health
Dermatology Radiology (diagnostic)
Emergency Medicine Radiology (interventional)
General Practice / Family Medicine
Radiology (radiation oncology)
Internal Medicine Surgery (vascular surgery)
Obstetrics / Gynecology Surgery (general surgery)
Ophthalmology Thoracic Surgery
Orthopedic Surgery Urology
Otolaryngology Oncology (general)
Pathology Oncology (radiation oncology)
Pediatrics Hospitalists
Physical Medicine Rheumatology

Registries23
CMS permits reporting by several types of registries:
Qualified registries
Qualified clinical data registries (QCDRs)
Many specialists have few applicable measures; their specialty societies are creating QCDRs
QCDRs may include measures that are not available outside of the QCDR
CMS has approved over 50 different QCDRs; many have fees and most are not applicable to geriatrics, but a few may be worth closer study

MIPS Requirements: Cost Performance Category
24
Basic Requirements Weight
• CMS will use claims data to measure cost of care
Measures:
• Medicare spending per beneficiary (MPSB) for clinician providing majority of inpatient care from 3 days prior to admission to 30 days post-discharge
• Total per capita cost for Part A and Part B services for clinician providing the most primary care services ($) in year
• CMS will measure compare costs for 10 episodes of care for specific conditions that are risk-adjusted (but not perfectly…)
• CMS working on patient relationship codes to attribute costs to clinicians providing acute / ongoing / supportive care
0%

60%
0%
15%
25%
2017
Quality
Cost
Improvement Activities
Advancing Care Information
Weights for Composite Performance Score:Cost Measure Increasingly Important in Future
50%
10%
15%
25%
2018
30%
30%
15%
25%
2019
CMS re-weighted the cost category to zero in 2017 and 10% in 2018…
…But weight will increase to 30% in 2018, and CMS lacks authority to re-weight
25
25

MIPS Requirements: Improvement Activities Performance Category
26
Basic Requirements Weight in 2017
• For 2017, reporting ONE improvement activity will avoid a payment penalty in 2019
• Clinicians must perform practice improvement activities for a continuous 90-day period during the year
• In future years, clinicians must report on up to 4 improvement activities
• Activities are weighted medium (10 points) or high (20 points); a total of 40 points needed to receive full credit
• Clinicians participating in an accredited patient-centered medical home receive 40 points for doing so
• Clinicians participating in a MIPS APM (that is, an APM that is not “advanced”) receive 20 points for doing so and may submit additional improvement activities to reach 40 points
15%

CMS Selected 93 Improvement Activities in 9 Subcategories
27
weekend hours, telehealth
SOPs for transitional care mgt
Maintenance of Certification IVregistries, feedback reports
see new Medicaid patientspatient portal, group visits
humanitarian / disaster relief
depression / suicide screening
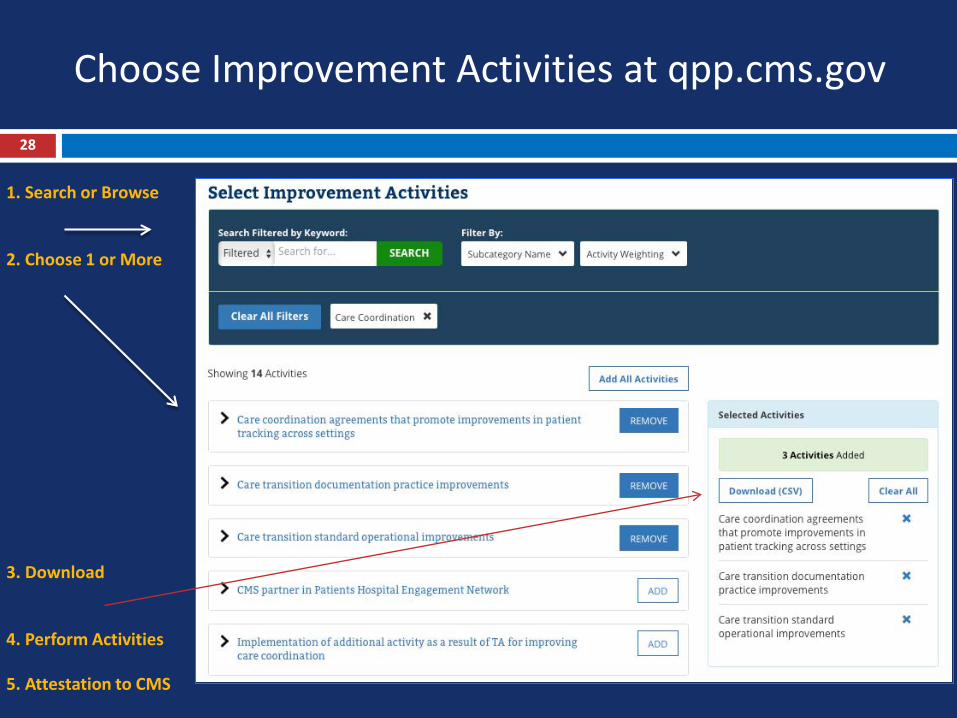
Choose Improvement Activities at qpp.cms.gov
28
1. Search or Browse
2. Choose 1 or More
3. Download
4. Perform Activities
5. Attestation to CMS

Medicare EHR Incentive Program and Attesting to Meaningful Use (MU)
29
Recent History: EHR Incentive Programs paid bonuses to demonstrate meaningful use (MU) of certified EHR technology (CEHRT)
Failing to demonstrate MU now carries payment penalty of -3%.
Beginning on a voluntary basis in 2017 and required beginning in 2018, most providers will attest to Stage 3 objectives and measures.
The EHR Incentive Program sunsets Dec. 31, 2018.

CMS Has Simplified MU Requirements for MIPS
30
CMS has renamed MU as “Advancing Care Information” in MIPS
Allows group data submission and performance to be assessed as a group (vs. individual clinician in EHR Incentive Program).
“Modified Stage 2” and Stage 3 of MU has 10 objectives with all-or-nothing scoring; ACI permits eligible clinicians to receive partial credit on measures.
No longer requires computerized provider order entry (CPOE), Clinical Decision Support (CDS), and clinical quality measures (eCQMs) to streamline reporting.
Permits clinicians to submit data for the first time through Qualified Clinical Data Registries (QCDRs).

MIPS Requirements: Advancing Care Information (EHR) Performance Category
31
Basic Requirements Weight in 2017
• Clinicians must use certified EHRs to report Objectives and Measures
• Clinicians must attest that they will support information exchange and prevent information blocking
• Report 5 required Objectives and Measures for a continuous 90-day period in 2017 to avoid a payment penalty in 2019
Scoring is more complex in future years:• Base Score (50 points)• Performance Score (90 points)
• Bonus for reporting to public health or clinical data registry (5 points) and reporting improvement activities using CEHRT (10 points)
• Total possible score is 155 points, but any score above 100 receives full credit (see Appendix)
25%

Special Rules for Facility-Based Clinicians’ CEHRT
32
Hospital-Based Clinicians Do Not Receive a Score for Advancing Care Information MIPS-eligible clinician who furnishes 75% or more of covered services in
certain sites of service:
PLACE OF SERVICE (POS) 21 (inpatient hospital) POS 22 (on-campus outpatient hospital) POS 23 (emergency room)
Nursing Home-Based Clinicians Do Not Receive This Benefit Nursing home facilities and their medical directors have asked CMS to
create special rules for those who practice in skilled nursing facilities, particularly those that lack interoperable EHRs
Possible area for AGS engagement with CMS

MIPS Performance Categories Combine Into Composite Score
33
Individual or Group Performancein 4 Domains
Individual’s or Group’s CPS Compared With
Performance Threshold
Payment Adjustment Amount
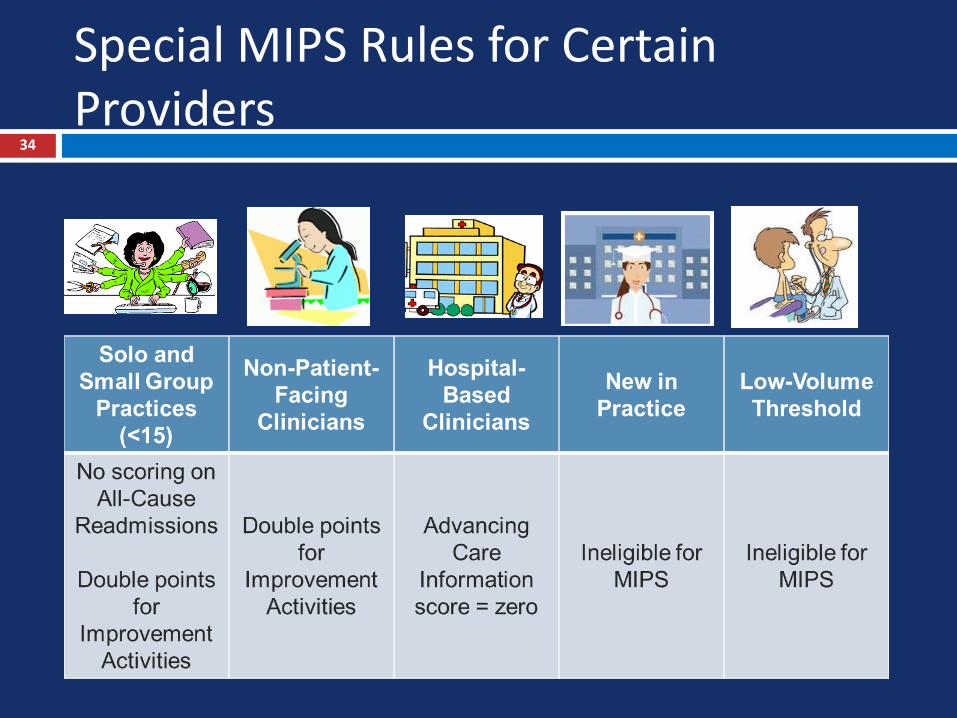
Special MIPS Rules for Certain Providers
34

Timeline for MACRA Implementation35
2016CMS RegulationsDevelop New ProcessesPrepare Systems Train Practices
2017Performance Period Measure QualityPerform Improvement ActivitiesUse Interoperable EHR
2018Data Reporting to CMSCalculation of compositescoresComparison to BenchmarksPublic Reporting
2019Medicare Payments Adjusted based on 2017 Performance
1. Get Ready!
2. Practice & Measure Performance
3. Data Reporting & CMS Calculations
4. Payment Period

Transparency of Scoring Calculations36
CMS has made changes to rules to increase transparency
E.g. APM participation “snapshots” 3 times per year
E.g. Claims lookback so clinicians know in advance if they meet MIPS criteria for special exceptions:
Non-patient facing, hospital-based, small practices
But scoring calculation will be a “black box” for most clinicians
Difficult to replicate CMS calculations (don’t try this at home!)

Informal Review Process37
If you believe that the negative payment adjustment is being applied in error, you can submit an informal review request within 60 days of the release date of the feedback reports.
CMS will investigate the merits of your informal review request and issue a decision within 90 days of receipt.
To request an informal review, all requests must be submitted via a web-based tool on the CMS Website.
Physicians are encouraged to access and review their feedback reports and Quality and Resource Use Reports (QRURs) prior to submitting an informal review request.
There is no further opportunity to appeal beyond the informal review; no judicial review.

Key Questions to Ask Your Group38
Are we planning to report as a group? Is our EHR compliant with certification requirements? Have we established processes to record HCPCS codes
for the quality measures we plan to report? What improvement activities are we planning for next
year, and do they fit within QPP rules? How can we use the QPP to improve care for our
patients? How will QPP affect my evaluation within the group
and / or my salary?

Resources for More Information39
Check out the AGS MACRA Toolkit here and find the following: http://www.americangeriatrics.org/health_care_professionals/macra/ The Basics of the Program AGS Updates and Comments on MACRA Links to Key Resources from Various Stakeholders
Check out this page for current updates and how-tos from CMS -https://qpp.cms.gov/
Upcoming Webinars Also, visit Geriatrics Care Online to listen to a recorded version of this
presentation here http://geriatricscareonline.org/ProductStore/webinars/17/ AMA will be hosting an educational webinar on Dec. 6; click here to register
Questions on MACRA or Recommendations for Resources You’d Like to See: Contact [email protected]

40
Thank You!

41
Appendix I: Advancing Care Information
Scoring Details

Advancing Care Information Scoring: Step 142
Base Score = 50 Points“All-or-Nothing”
10 10
10 10 10

Advancing Care Information Scoring: Step 243
Performance Score = up to 90 PointsReport numerators & denominators
Provide Patient Access View, Download and Transmit
Send a Summary of Care
Patient SpecificEducation
Secure Messaging Request / Accept Patient Care Record
Patient-Generated Health Data
Clinical Information Reconciliation
Immunizations
10 10
10 10
10 10
10
10
10

Advancing Care Information Scoring: Step 344
Bonus Score = 5, 10 or 15 PointsReport to one or more registries (max = 5 points)
Report Improvement Activities Using CEHRT (10 points)
Syndromic Surveillance Reporting
Electronic Case Reporting
Public Health Registry Reporting
Clinical Data Registry Reporting
5
Report Improvement Activities Using CEHRT
10

Advancing Care Information: Total Score
45
Total possible score is 155 points 50 points for Base Score 90 points for Performance Score 15 points for Bonus Score
Any score at or above 100 points receives full credit for Advancing Care Information
Failure to use a certified EHR = zero score

Appendix II:
Details on Advanced APMs

Earning APM Bonus Requires Being a Qualified Participant in an Advanced APM
47
“Partial QP”
QP criteria are set in law and increase over time, and will include non-Medicare payers’ APMs in 2019+
Qualifying Participants (QPs)
In 2017 & 2018, QP status requires:Receiving 25% of Medicare payments through the APM ORSeeing 20% of patients in an APM.
“Partial QP” requires receiving 20% of payments or 10% of patients.

Advanced APMs for 201748
Comprehensive ESRD Care (CEC) - Two-Sided Risk Comprehensive Primary Care Plus (CPC+) Next Generation ACO Model Shared Savings Program - Track 2 Shared Savings Program - Track 3 Oncology Care Model (OCM) - Two-Sided Risk This list may change. CMS plans to publish a final
list before January 1, 2017.

Qualified Participant Notification49
The QP performance period is January 1 – August 31 CMS will look at three “snapshots” in time -- March 31,
June 30, and August 31 of the QP Performance Period --which are early enough in the year for eligible clinicians to have notice of their status before the end of the MIPS performance period.
Each snapshot may add eligible clinicians to the APM Entity Group or capture new affiliated practitioners
If you are determined to be a QP on any of the snapshots, you will receive the QP bonus -- even if you drop off on later snapshots during the year.

Despite Changes to “Nominal Risk,” 2017 Participation in Advanced APMs < 10%
50
Most eligible clinicians will not have the option of participating in an Advanced APM in 2017, despite modifications to the “nominal financial risk” standard. Revenue standard: In 2017 and 2018, 8% of the average estimated
total Medicare Parts A and B revenues of participating APM Entities OR
Benchmark-based standard: for all QP Performance Periods, 3% of the expected expenditures for which an APM Entity is responsible under the APM design
CMS estimates 70,000 to 120,000 clinicians, or less than 10% those eligible, will receive a bonus payment in 2019, based on expected participation in APMs that meet the criteria to be “advanced” in 2017.

CMS Changing from National Benchmark to Regional Benchmarks for APMs to Improve Risk Adjustment
51

All-Payer APM Revenue Qualifies for Bonus, 2021-2024
52
2019-20 2021-22 2023-24
25% 50% 75%
Medicare Revenue from APMs OR (Medicare + Other Payers) Revenue from APMs
Medicare Revenue from
APMs
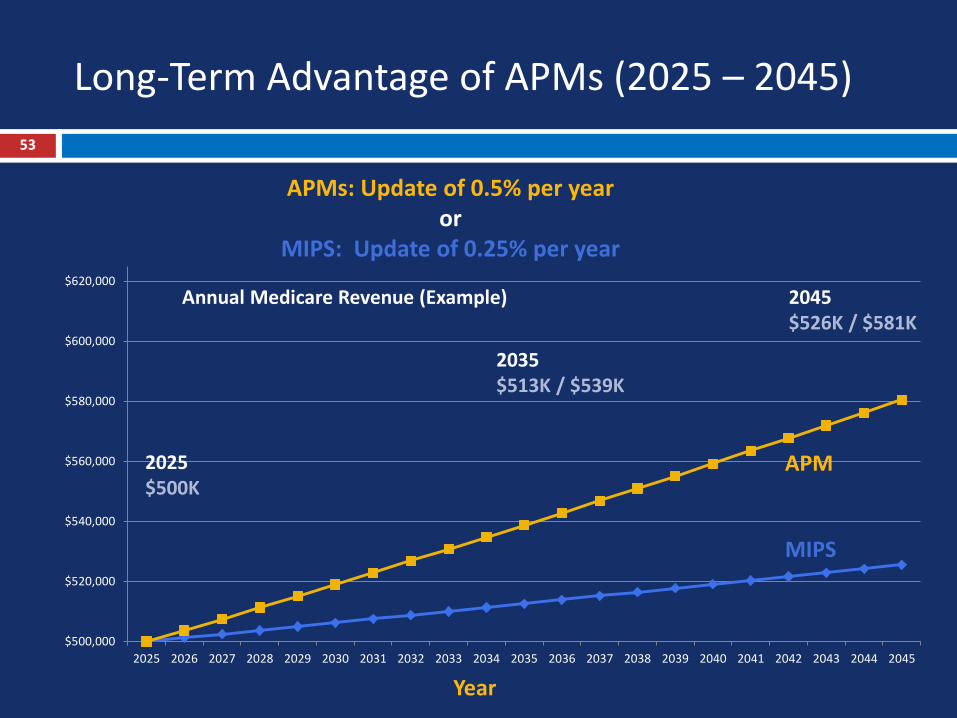
Long-Term Advantage of APMs (2025 – 2045)53
APMs: Update of 0.5% per yearor
MIPS: Update of 0.25% per year
Year
$500,000
$520,000
$540,000
$560,000
$580,000
$600,000
$620,000
2025 2026 2027 2028 2029 2030 2031 2032 2033 2034 2035 2036 2037 2038 2039 2040 2041 2042 2043 2044 2045
Annual Medicare Revenue (Example) 2045$526K / $581K
2025$500K
2035$513K / $539K
APM
MIPS


















