
The Pulmonary Capillary Bed Various Forms Pulmonary...
9
The Pulmonary Capillary Bed in Various Forms of Pulmonary Hypertension By R. MICHAEL MCCREDIE, M.B., M.R.C.P., M.R.C.P. (EDIN.) IN A PREVIOUS STUDY of the pulmonary capillary bed in mitral valve disease,' the mean value for pulmonary diffusing capacity for carbon monoxide (DL) was found to be significantly lower than normal, in agreement with several other reports.2 7 This was due mainly to impairment of the membrane diffus- ing capacity (DM). Reduction in pulmonary capillary blood volume (V,) was found only in patients with higher pulmonary vascular pressures and resistances. It was suggested that reduction of V. was due to constriction or partial obliteration of the pulmonary cap- illary bed and that this may be an important contributing factor in the elevation of pulmo- nary vascular resistance found in mitral valve disease. This study has now been extended to a larger number of patients with mitral valve disease and other conditions associated with pulmonary hypertension, before and after surgery, to find out (1) if similar changes in the pulmonary capillary bed occurred in aortic valve disease, primary myocardial disease, and idiopathic pulmonary hypertension, (2) if changes in the pulmonary capillary bed were related in any way to functional disability or to the results of cardiac surgery, and (3) if DL, D11, or V, changed after cardiac surgery. Methods Forty-four patients were studied by right and left heart catheterization, using standard proce- dures,8' 9 after premedication with papaveretum, B.P.C. (opium concentration). Steady-state measurements of pulmonary dif- fusing capacity for carbon monoxide (DL), using From the Hallstrom Institute of Cardiology, Royal Prince Alfred Hospital, Camperdown, N.S.W., Sydney, Australia. Work done during tenure as a Senior Research Fellow of the National Heart Foundation of Aus- tralia. 854 an end-tidal sampling method,10 have been described in detail elsewhere.' The diffusing capacity of the alveolar-capillary membrane (Dm,) and the pulmonary capillary blood volume (V,) were derived from measurements of DL at two different levels of alveolar oxygen tension, fol- lowing the methods of Forster, Roughton and associates.11 12 Gas chromatography* was used for the analysis of respired air samples and for the estimation of the carbon monoxide content of arterial blood.13 This method is accurate to within less than ± 2% for both blood and air samples. No premedication was given for the diffusion studies; otherwise they were done under the same conditions as, and within 4 days of, cardiac catheterization. As DL, D.-, and V, in normal subjects have been shown to be related to body surface area,'4 DL and DM, were expressed in milliliters of carbon dioxide per minute per mm Hg per square meter and V, in milliliters per square meter. Pulmonary vascular resistance (PVR) was expressed in "resistance units" also related to body surface area (RU . M2); it was obtained by dividing the gradient from mean pulmonary ar- terial pressure (PPA) to mean left atrial pressure (PLA) in mm Hg by the cardiac index in liters per minute per square meter. The patients were grouped arbitrarily according to the level of PVR which was considered normal when the level was less than 3 RU i m2, moderately raised if 3 to 10 RU im2, severely raised if 10 to 20 RU * M2 and extreme if more than 20 RU * M2. Func- tional disability at the same time of the study was classed I to IV by standard criteria.15 The patients were also grouped according to diagnosis: (1) mitral valve disease, 31 patients, including 18 previously reported on,1 of whom 26 had pure mitral stenosis and five had dominant mitral incompetence; there were 15 males and 16 females, and ages ranged from 20 to 59 years, with a mean of 41 years; (2) aortic valve disease, six male patients, two with pure aortic stenosis and four with dominant incompetence, with ages ranging from 13 to 53 years, with a mean of 33 years; (3) primary myocardial disease, five pa- tients including three with idiopathic hypertrophic *Beckman GC2 Gas Chromatograph, Beckman Instruments, South Pasadena, California. Circulation, Volume XXXIII, June 1966 by guest on June 3, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of The Pulmonary Capillary Bed Various Forms Pulmonary...

The Pulmonary Capillary Bed in VariousForms of Pulmonary Hypertension
By R. MICHAEL MCCREDIE, M.B., M.R.C.P., M.R.C.P. (EDIN.)
IN A PREVIOUS STUDY of the pulmonarycapillary bed in mitral valve disease,' the
mean value for pulmonary diffusing capacityfor carbon monoxide (DL) was found to besignificantly lower than normal, in agreementwith several other reports.2 7 This was duemainly to impairment of the membrane diffus-ing capacity (DM). Reduction in pulmonarycapillary blood volume (V,) was found onlyin patients with higher pulmonary vascularpressures and resistances. It was suggestedthat reduction of V. was due to constrictionor partial obliteration of the pulmonary cap-
illary bed and that this may be an importantcontributing factor in the elevation of pulmo-nary vascular resistance found in mitral valvedisease.
This study has now been extended to a
larger number of patients with mitral valvedisease and other conditions associated withpulmonary hypertension, before and aftersurgery, to find out (1) if similar changes inthe pulmonary capillary bed occurred in aorticvalve disease, primary myocardial disease, andidiopathic pulmonary hypertension, (2) ifchanges in the pulmonary capillary bed were
related in any way to functional disability or
to the results of cardiac surgery, and (3) ifDL, D11, or V, changed after cardiac surgery.
MethodsForty-four patients were studied by right and
left heart catheterization, using standard proce-
dures,8' 9 after premedication with papaveretum,B.P.C. (opium concentration).
Steady-state measurements of pulmonary dif-fusing capacity for carbon monoxide (DL), using
From the Hallstrom Institute of Cardiology, RoyalPrince Alfred Hospital, Camperdown, N.S.W., Sydney,Australia.Work done during tenure as a Senior Research
Fellow of the National Heart Foundation of Aus-tralia.
854
an end-tidal sampling method,10 have beendescribed in detail elsewhere.' The diffusingcapacity of the alveolar-capillary membrane (Dm,)and the pulmonary capillary blood volume (V,)were derived from measurements of DL at twodifferent levels of alveolar oxygen tension, fol-lowing the methods of Forster, Roughton andassociates.11 12 Gas chromatography* was usedfor the analysis of respired air samples and forthe estimation of the carbon monoxide content ofarterial blood.13 This method is accurate to withinless than ± 2% for both blood and air samples.No premedication was given for the diffusionstudies; otherwise they were done under thesame conditions as, and within 4 days of, cardiaccatheterization.
As DL, D.-, and V, in normal subjects havebeen shown to be related to body surface area,'4DL and DM, were expressed in milliliters ofcarbon dioxide per minute per mm Hg persquare meter and V, in milliliters per squaremeter. Pulmonary vascular resistance (PVR) wasexpressed in "resistance units" also related tobody surface area (RU . M2); it was obtained bydividing the gradient from mean pulmonary ar-terial pressure (PPA) to mean left atrial pressure(PLA) in mm Hg by the cardiac index inliters per minute per square meter. The patientswere grouped arbitrarily according to the level ofPVR which was considered normal when the levelwas less than 3 RU im2, moderately raised if 3 to10 RU im2, severely raised if 10 to 20 RU * M2and extreme if more than 20 RU * M2. Func-tional disability at the same time of the study wasclassed I to IV by standard criteria.15The patients were also grouped according to
diagnosis: (1) mitral valve disease, 31 patients,including 18 previously reported on,1 of whom26 had pure mitral stenosis and five had dominantmitral incompetence; there were 15 males and 16females, and ages ranged from 20 to 59 years,with a mean of 41 years; (2) aortic valve disease,six male patients, two with pure aortic stenosisand four with dominant incompetence, with agesranging from 13 to 53 years, with a mean of 33years; (3) primary myocardial disease, five pa-tients including three with idiopathic hypertrophic
*Beckman GC2 Gas Chromatograph, BeckmanInstruments, South Pasadena, California.
Circulation, Volume XXXIII, June 1966
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

PULMONARY HYPERTENSION
Table 1Estimates of DL, Dm, and V, in Normal Subjects and in Patients with Heart Disease
DL, Dm, c
Diagnosis Number ml CO/min/mm Hg/M2 ml CO/min/mm Hg/M2 MV/rn
Normal subjects 18 15.0 ± 0.59 30 ± 2.45 52 ± 3.51Mitral valve 8.3 0.45 13 0.86 41 3.39
disease 31 (P < 0.001) (P < 0.001) (N.s.)Aortic valve 12.1 + 1.06 21 + 1.55 53 + 9.72
disease 6 (P<0.05) (P<0.001) (N.s.)Primary myocardial 9.2 + 0.89 13 + 1.25 55 + 10.01
disease 5 (P < 0.001) (P < 0.001) (N.s.)Idiopathic pulmonary
hypertension 2 10.5, 9.4 14, 12 44, 61
DL and DM are the diffusing capacities of the lung and of the alveolar-capillary membrane; V. is the pulmo-nary capillary blood volume. Values are mean + 1 standard error; level of significance of difference of means fromnormal values indicated in brackets; N.s., not significant.
subaortic stenosis and two with left ventricularfailure of unknown etiology; there were threemales and two females with ages ranging from 10to 46 years, with a mean of 25 years; and(4) idiopathic pulmonary hypertension, two pa-
tients, both male, aged 31 and 33 years.A control group of 18 normal subjects, whose
data appeared in a previous report,' were usedfor comparison. Included were 15 males andthree females; their ages ranged from 8 to 46years, with a mean of 29 years.
Twenty-seven of these patients underwentcardiac surgery: 22 for mitral valve disease, fourfor aortic valve disease, and one for subaorticobstruction. Four died at operation. The sympto-matic result 3 months or more after operationwas judged to be excellent if the functionaldisability of the patient was class I, good ifclass II, and poor if class III or worse.
In 11 of these patients who underwent mitralvalvotomy, measurements of DL, D.1, and V.were repeated 2 weeks to 8 months after surgery.
Results
Values for DL, Dal, and V, in normal sub-jects and in the diagnostic groups are shownin table 1. Although a few patients had V,above or below the normal range, the means
for each group lay within normal limits, andthere were no differences between the fourgroups. Mean DL and D-q were significantlyreduced in all groups.The relationships of functional disability to
determinations of DL, D-.N, and V, are shownin figure 1. Mean DL was lower than normalat all grades of disability (P <0.001 in all),and significantly more so in class IV patientsCirculation, Volume XXXIII, June 1966
(P < 0.01). Mean D., was also lower thannormal in all grades (P <0.001 in all), butthere were no differences between the fourgrades. Mean V, for patients in classes I, II,and III did not differ significantly from normal
FUNCTIONAL DISABILITY
E
E
0
E
la
?£ 30IEE
d E 20
0
-i 101
usr_S:v
60-
40
20-
Normal Class Class 11 Class III Class IV
Figure 1
Relationships of DL, DM, and Vc to functional classi-
fication. Closed circles and bars represent mean +2
SE for each group.
+ j
.4+
+40-
I. I L __IL-
855
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from
McCREDIE
.C
-r
IE
E
d
C,
15
10
5
30
2C
10
80
60
40
20
PULMONARY VASCULAR RESISTANCE
Group Group 2 Group 3 Group 4
0 3 3 -10 10- 20 '20RUM>
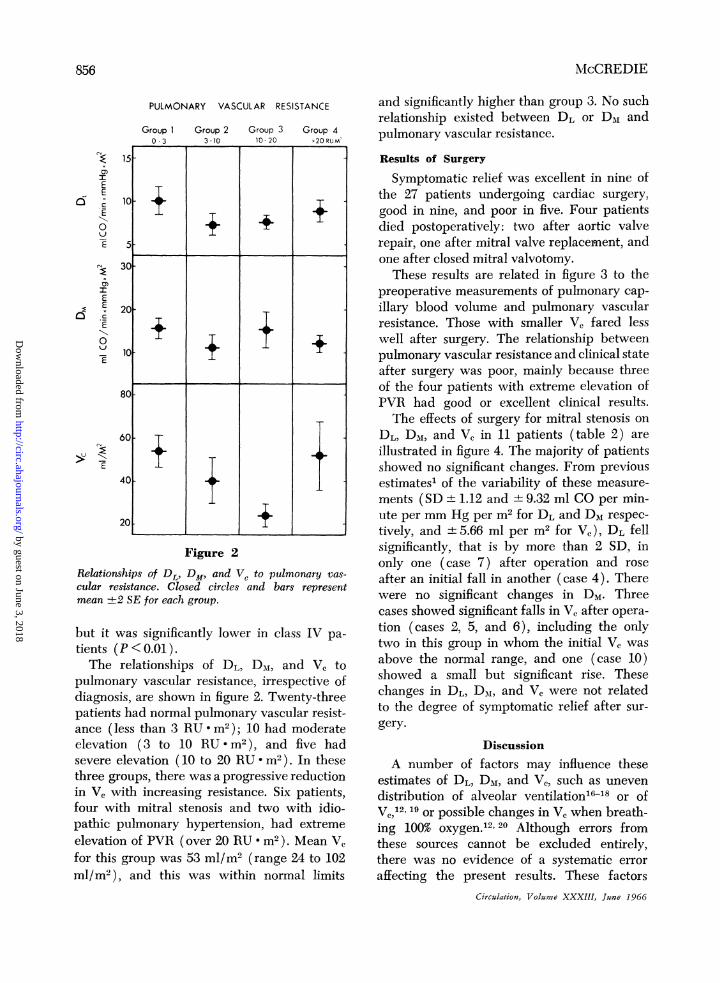
Figure 2
Relationships of DL, DM, and V. to pulmonary vas-
cular resistance. Closed circles and bars representmean ±2 SE for each group.
but it was significantly lower in class IV pa-
tients (P< 0.01).The relationships of DL, Dm, and V, to
pulmonary vascular resistance, irrespective ofdiagnosis, are shown in figure 2. Twenty-threepatients had normal pulmonary vascular resist-ance (less than 3 RU M2); 10 had moderateelevation (3 to 10 RU * m2 ), and five hadsevere elevation (10 to 20 RU m2). In thesethree groups, there was a progressive reductionin V, with increasing resistance. Six patients,four with mitral stenosis and two with idio-pathic pulmonary hypertension, had extreme
elevation of PVR (over 20 RU M2). Mean V,for this group was 53 ml/m2 (range 24 to 102ml/m2 ), and this was within normal limits
and significantly higher than group 3. No suchrelationship existed between DL or DM andpulmonary vascular resistance.
Results of Surgery
Symptomatic relief was excellent in nine ofthe 27 patients undergoing cardiac surgery,good in nine, and poor in five. Four patientsdied postoperatively: two after aortic valverepair, one after mitral valve replacement, andone after closed mitral valvotomy.These results are related in figure 3 to the
preoperative measurements of pulmonary cap-
illary blood volume and pulmonary vascularresistance. Those with smaller V, fared lesswell after surgery. The relationship betweenpulmonary vascular resistance and clinical stateafter surgery was poor, mainly because threeof the four patients with extreme elevation ofPVR had good or excellent clinical results.The effects of surgery for mitral stenosis on
DL, DM, and V, in 11 patients (table 2) are
illustrated in figure 4. The majority of patientsshowed no significant changes. From previousestimates1 of the variability of these measure-
ments (SD 1.12 and + 9.32 ml CO per min-ute per mm Hg per m2 for DL and Dm respec-
tively, and + 5.66 ml per m2 for V½), DL fellsignificantly, that is by more than 2 SD, inonly one (case 7) after operation and rose
after an initial fall in another (case 4). Therewere no significant changes in DM. Threecases showed significant falls in V, after opera-tion (cases 2, 5, and 6), including the onlytwo in this group in whom the initial V, was
above the normal range, and one (case 10)showed a small but significant rise. Thesechanges in DL, Dm1, and V, were not relatedto the degree of symptomatic relief after sur-
gery.
Discussion
A number of factors may influence theseestimates of DL, DM, and Vc, such as uneven
distribution of alveolar ventilation 168 or ofVe,12,19 or possible changes in V, when breath-ing 100% oxygen.12 20 Although errors fromthese sources cannot be excluded entirely,there was no evidence of a systematic error
affecting the present results. These factorsCirculation, Volume XXXIII, Juane 1966
Ii + ±
II
I _ +
856
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

PULMONARY HYPERTENSION
Pre-op
vc2ml /M
100-
8
60-
40-
20-
A
rre -opPVRRU.M2
40-
30-
20
10
BFigure 3
Results of surgery in 27 patients related to preoperative measurements: (A) Pulmonarycapillary blood volume (V,); (B) Pulmonary vascular resistance (PVR). Each dot representsone patient; the four marked with crosses are patients with extreme elevation of PVR(> 20 RU * m2) all in group 4 of figure 2 (see text). Solid and broken lines represent mean
-+-2 SE for each group.
have been discussed previously in detail inrelation to the pulmonary capillary bed inmitral valve disease.'
In each diagnostic group, there was a
significant reduction in mean DL, attributablemainly to reduction in membrane diffusion,as mean V, in each group was within normallimits (table 1). This reduction in Dm1 may
reflect decreased permeability due to fibrosisor thickening of the alveolar walls, as de-scribed by Parker and Weiss21 in mitral valvedisease, and the same changes probably occur
in other conditions with left heart dysfunctionand pulmonary venous congestion. The im-pairment of D.-, found here in two patientswith idiopathic pulmonary hypertension sug-gests some functional involvement, at least, inthis condition also.The relationship of V, to clinical disability
Circulation, Volume XXXIII, June 1966
(fig. 1) is similar to the finding of Palmerand associates6 that V. in mitral stenosiswas reduced in class IV patients. Total diffus-ing capacity of the lungs (DL) was reducedin all, mainly due to reduction in DN1, butwas still further reduced in class IV patientsbecause these patients also have a reduced V,.This combination of reduced Dm, and V,found in the most disabled patients may wellcontribute to their incapacity.The volume of a normally distensible pulmo-
nary capillary bed will increase with rise intransmural pressure until a plateau is reachedcorresponding to maximum distention. Thishas been demonstrated in animal lung prepa-
rations,22 23 and in man.24 Figure 5 presents a
hypothetical pressure-volume curve for a nor-
mal lung, the shape of the normal curve beingbased on data from the isolated dog lung23;
RESULT OF SURGERYExcellent Good Poor Died
x
*-
es --1--
0
0@
x5 0
RESULT OF SURGERYExcellent Good Poor Died
K
I
K
I
S
0 0
I__ ____.--I-- 0
I~~~~~~~~-- -- . a
857
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

Table 2Physical Characteristics and Determinations of DL, DM, and V0 and Hemodynamic Data in 11 Patientswith Mitral Stenosis before and after Mitral Valvotomy
TimeBSA, after
Case Age Sex m2 operation
1 54 F 1.64 Preop.6 mo
2 42 F 1.32 Preop.5 wk
3 30 F 1.41 Preop.8 mo
4 44 M 1.84 Preop.2 wk6 mo
5 36 F 1.76 Preop.2 wk
6 39 M 1.79 Preop.10 wk
7 28 F 1.48 Preop.5 wk
8 34 M 1.85 Preop.3 mo
9 27 M 1.63 Preop.2 wk
10 36 M 1.87 Preop.2 mo
11 53 F 1.54 Preop.7 mo
DL DMml CO/min/mm Hg/m2
5.2 64.7 66.6 86.3 89.9 179.4 167.7 116.6 89.2 177.2 96.5 9
10.1 1210.2 1315.3 2310.7 149.0 187.0 119.9 149.2 139.3 158.6 116.9 136.3 10
Vc C. I. PFX PAX PVR Functionalml m2 L/rmin/m2 mm Hg RU * m2 class
36327751383436353057351027074752929534734472422
1.6 17 9 5 IVIII
2.1 27 14 6 IIIII
1.8 40 24 9 IVI
1.2 81 33 40 IV2.8 39 18 8 II
II2.3 26 21 2 III
I1.6 66 22 28 IV
I3.1 22 18 1 IV
II3.6 26 24 1 III
II1.6 18 15 2 II
I2.1 35 22 6 III
II2.5 75 37 16 IV
III
Abbreviations: BSA is body surface area; DL Dm and V0 as in table 1. C.I. is cardiac index; PPA and Py-J aremean pulmonary arterial and left atrial pressures, and PVR is pulmonary vascular resistance.
the three curves with progressively lower pla-teaus would represent the effects of progres-sive reduction in maximum V,. From such adiagram it can be seen (1) that a substantiallowering of transmural pressure could occurin the more restricted capillary beds withoutany significant change in V0, and (2) that V0must be on or near the steep portion of thecurve for any marked change to occur withlowering of transmural pressure. The resultsshown in figure 4 may be explained on thisbasis. After successful mitral valvotomy, theonly three patients who showed a fall in V0had increased or high normal V0 preoperativelyand were presumably on, or close to, the steeppart of their pressure-volume curve. The factthat all but one of those with low normal orreduced V0 showed no significant change overa period up to 8 months (fig. 4) suggests thatthis reduction in V, is usually irreversible.Neither was there any significant improvement
in DL or D.I in the group over the sameperiod.
If reduction in V, in the presence of highintravascular pressure reflects a decrease incross-sectional area of the capillary bed, itmay contribute an important part of thetotal increase in PVR.' Reduction in V0 alsoappears to be related to poorer symptomaticresults from surgery (fig. 3). But of the sixpatients with extreme elevation of PVR, V,was not reduced in five; the only one in whomit was reduced (24 ml/m2 ) died 1 weekafter mitral valve replacement. Three hadmuch better symptomatic results from mitralvalvotomy than might have been expectedfrom their initial levels of PVR, and theother two had idiopathic pulmonary hyper-tension which may not involve the capillarybed histologically.25-27High or normal V0 in these patients with
extreme elevation of PVR could be relatedCirculation, Volume XXXIII, June 1966
85 McCREDIE
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

PULMONARY HYPERTENSION
opn
DL 15
ml CO/minXmm HgxM2
10
5
DM30
ml CO/minx mm Hg. m2
20
10
vcmt/M2'
100
80
60
40
20
OPERAT ION
4 6 8
OP"l 2 4 6 8
2 4 6 8 Months
Figure 4
Measurements of DL, DM, and V, in 11 patients with mitral stenosis before and aftermitral valvotomy (see table 2). Cross-hatched area represents the normal range.
to the dilatation lesions described by Heathand Edwards.28 Although these dilatationlesions are not structurally capillaries, it ispossible that they take some part in gas
exchange in the lungs29' 30 and, therefore,would be included in the estimate of V,.But it is doubtful that these lesions would besufficiently numerous to account for thepresent results.
If, however, the pulmonary capillary bedis relatively less affected by disease in thesepatients, the increase in pulmonary vascular
Circulation, Volume XXXIII, June 1966
resistance must be almost entirely due toprecapillary obstruction. Recently Aber andCampbell3l compared DL measurements in79 patients with mitral stenosis with resultsof histological examination of lingular biopsiestaken at operation. They found that reductionin DL was associated with intimal changesin small lung vessels and with increasingpulmonary vascular resistance. In four pa-
tients with the highest resistances, however,DL was not reduced, and the histologicalchange was confined to medial thickening
0I I
|
0
I
L
859
:irt---
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCREDIE
vcml /M2
150
Normal
100/
50/ 2i
10 20 30TRANSMURAL PRESSURE mmHg
Figure 5Theoretical pressure-volume curves of the pulmonarycapillary bed in normal lungs and in patients withincreasingly severe pulmonary vascular disease; thegrades (1), (2), and (3) correspond to groups 1, 2and 3 of figure 2.
of the muscular arteries without intimaldamage. If these patients with very highresistance but relatively normal DL (and byinference V.) exist as a distinct group, withvascular changes suggesting muscular c.n-striction rather than intraluminal obstruction,perhaps the patients with high or normalV, despite extreme elevation of resistancebelong to the same group. I do not have anyhistological comparisons, but possibly, in afew patients with mitral stenosis, intense pre-capillary vasoconstriction really does protectthe pulmonary capillary bed.
SummaryPulmonary diffusing capacity for CO (DL),
membrane diffusing capacity (Dm1), and pul-monary capillary blood volume (Vc) weremeasured in 44 patients with various formsand severity of pulmonary vascular disease,and these measurements were compared withhemodynamic data obtained at cardiac cathe-terization, with clinical disability, and, in 27patients, with the results of corrective cardiacsurgery. In 11 of these patients, DL, D-q,
and V, were remeasured up to 8 monthsafter cardiac surgery.
In general, the diffusing characteristics andpressure-volume relationships in this largergroup confirmed the previously reportedfindings in mitral valve disease.' DM wasimpaired in almost all cases regardless ofetiology or severity. Most of the 11 patientsrestudied showed no change in DL, DM, orV, up to 8 months after surgery. Reductionin V, correlated well both with clinical dis-ability and with surgical results.Two patients with primary pulmonary
hypertension and three of the four patientswith equally severe pulmonary hypertensiondue to mitral valve disease had high V½relative to pulmonary vascular resistance. Ifthe measurements of V, are not falsely high,then it appears that the capillary bed makesrelatively and absolutely less contribution tothe total rise in pulmonary vascular resist-ance in these patients. This could be ex-plained by intense precapillary vasoconstric-tion in the presence of a relatively normalpulmonary capillary bed.
AcknowledgmentsI am grateful to Dr. A. D. Jose for his helpful
criticism and to Miss T. Guilfoyle for invaluabletechnical assistance.
References1. MCCREDIE, R. M.: Diffusing characteristics and
pressure-volume relationships of the pulmo-nary capillary bed in mitral valve disease. JClin Invest 43: 2279, 1964.
2. RILEY, R. L., JOHNS, C. J., COHEN, G., COHN,J. E., CARROLL, D. G., AND SHEPARD, R. H.:Diffusing capacity of the lungs in patients withmitral stenosis studied post-operatively. J ClinInvest 35: 1008, 1956.
3. MACINTOSH, D. J., SINNOTT, J. C., MILNE, I. G.,AND REID, E. A. S.: Some aspects ofdisordered pulmonary function in mitral steno-sis. Ann Intern Med 49: 1294, 1958.
4. BATES, D. V., VARVIS, C. J., DONEVAN, R. E.,AND CHRISTIE, R. V.: Variations in the pul-monary capillary blood volume and membranediffusion component in health and disease.J Clin Invest 39: 1401, 1960.
5. FLATLEY, F. J., CONSTANTINE, H., MCCREDIE,R. M., AND YU, P. N.: Pulmonary diffusing ca-pacity and pulmonary capillary blood volumein normal subjects and in cardiac patients. AmerHeart J 64: 159, 1962.
Circulation, Volume XXXIII, June 1966
860
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

PULMONARY HYPERTENSION
6. PALMER, W. H., GEE, J. B. L., MILLS, F. C., ANDBATES, D. V.: Disturbances of pulmonaryfunction in mitral valve disease. Canad MedAss J 89: 744, 1963.
7. DALY, W. J., GIAMMONA, S. T., Ross, J. C., ANDFEIGENBAUM, H.: Effects of pulmonary vas-cular congestion on postural changes in the per-fusion and filling of the pulmonary vascularbed. J Clin Invest 43: 68, 1964.
8. COURNAND, R., BALDWIN, J. S., AND HIMMEL-STEIN, A.: Cardiac Catheterization in Congeni-tal Heart Disease. New York, CommonwealthFund, 1949.
9. Ross, J., JR., BRAUNWALD, E., AND MORROW,A. G.: Left heart catheterization by the trans-septal route: A description of the technic andits applications. Circulation 22: 927, 1960.
10. BATES, D. V., BOUCOT, N. G., AND DORMER,A. E.: Pulmonary diffusing capacity in normalsubjects. J Physiol (London) 129: 237, 1955.
11. FORSTER, R. E., ROUGHTON, F. J. W., CANDER,L., BRISCOE, W. A., AND KREUZER, F.: Appar-ent pulmonary diffusing capacity for CO atvarying alveolar 02 tensions. J Appl Physiol11: 277, 1957.
12. ROUGHTON, F. J. W., AND FORSTER, R. E.: Rela-tive importance of diffusion and chemicalreaction rates in determining rate of exchangeof gases in the human lung, with specialreference to true diffusing capacity of pul-monary membrane and volume of blood inthe lung capillaries. J Appl Physiol 11: 290,1957.
13. MCCREDIE, R. M., AND JOSE, A. D.: Analysisof blood carbon monoxide and oxygen by gaschromatography. J Appl Physiol. In press.
14. BUcCI, G., COOK, C. D., AND BARRIE, H.: Studiesof respiratory physiology in children: V. Totallung diffusion, diffusing capacity of pulmonarymembrane and pulmonary capillary bloodvolume in normal subjects 7 to 40 years ofage. J Pediat 58: 820, 1961.
15. CRITERIA COMMITTEE OF THE NEW York HEARTASSOCIATION (HAROLD E. B. PARDEE, CHAIR-MAN): Nomenclature and Criteria for Diagno-sis of Diseases of the Heart and Blood Vessels,ed. 3. New York, American Heart Association,1953.
16. FORSTER, R. E.: Exchange of gases betweenalveolar air and pulmonary capillary blood:Pulmonary diffusing capacity. Physiol Rev 37:391, 1957.
17. BuRROWs, B., NIDEN, A. H., MITTMAN, C.,TALLEY, R. C., AND BARCLAY, W. R.: Non-uniform pulmonary diffusion as demonstratedby the carbon monoxide equilibration tech-nique: Experimental results in man. J Clin In-vest 39: 943, 1960.
Circulation, Volume XXXIII, June 1966
18. LEWIS, B. M., HAYFORD-WELSING, E. J., FUROSKO,A., AND REED, L. C., JR.: Effect of unevenventilation on pulmonary diffusing capacity. JAppl Physiol 16: 679, 1961.
19. READ, J., READ, D. J. C., AND PAIN, M. C. F.:Influence of nonuniformity of the lungs onsteady-state measurements of pulmonary dif-fusing capacity for carbon monoxide. ClinSci 29: 107, 1965.
20. LEWIS, B. M., LIN, T.-H., NOE, F. E., ANDKOMISARUK, R.: Measurement of pulmonarycapillary blood volume and pulmonary mem-brane diffusing capacity in normal subjects:The effects of exercise and position. J ClinInvest 37: 1061, 1958.
21. PARKER, F., JR., AND WEISS, S.: Nature andsignificance of the structural changes in thelungs in mitral stenosis. Amer J Path 12: 573,1936.
22. ROSENBERG, E., AND FORSTER, R. E.: Changes indiffusing capacity of isolated cats' lungs withblood pressure and flow. J Appl Physiol 15:883, 1960.
23. BuRROWS, B., AND NIDEN, A. H.: Effect of vascu-lar pressure and blood flow on CO diffusionin the perfused dog lung. J Appl Physiol 18:722, 1963.
24. JOHNSON, R. L., JR., TAYLOR, H. F., ANDLAWSON, W. H.: Maximal diffusing capacityof the lung for carbon monoxide. J Clin Invest44: 349, 1965.
25. SHEPHERD, J. T., EDWARDS, J. E., BURCHELL,H. B., SWAN, H. J. C., AND WOOD, E. H.:Clinical, physiological and pathological con-siderations in patients with idiopathic pul-monary hypertension. Brit Heart J 19: 70,1957.
26. HEATH, D., WHITAKER, W., AND BROWN, J. W.:Idiopathic pulmonary hypertension. Brit HeartJ 19: 83, 1957.
27. EVANS, W., SHORT, D. S., AND BEDFORD, D. E.:Solitary pulmonary hypertension. Brit HeartJ 19: 93, 1957.
28. HEATH, D., AND EDWARDS, J. E.: Pathology ofhypertensive pulmonary vascular disease: De-scription of six grades of structural changes inthe pulmonary arteries with special referenceto congenital cardiac septal defects. Circula-tion 18: 533, 1958.
29. STAUB, N. C.: Gas exchange vessels in the catlung. Fed Proc 20: 107, 1961.
30. SOBOL, B. J., BOTTEX, G., EMIRGIL, C., ANDGISSEN, H.: Gaseous diffusion from alveoli topulmonary vessels of considerable size. Circu-lation Research 13: 71, 1963.
31. ABER, C. P., AND CAMPBELL, J. A.: Significanceof changes in the pulmonary diffusing capa-city in mitral stenosis. Thorax 20: 135, 1965.
861
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

R. MICHAEL MCCREDIEThe Pulmonary Capillary Bed in Various Forms of Pulmonary Hypertension
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1966 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.33.6.854
1966;33:854-861Circulation.
http://circ.ahajournals.org/content/33/6/854located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 3, 2018http://circ.ahajournals.org/
Dow
nloaded from


















