
The Power of Family Work: Findings Old and New Recent Outcomes, New Models and Future Prospects...
56
The Power of Family Work: Findings Old and New Recent Outcomes, New Models and Future Prospects Fifth Annual Grampians Mental Health Conference March 1-2, 2005 William R. McFarlane, M.D. Center for Psychiatric Research Portland, Maine University of Vermont
-
Upload
hilary-gray -
Category
Documents
-
view
213 -
download
0
Transcript of The Power of Family Work: Findings Old and New Recent Outcomes, New Models and Future Prospects...

The Power of Family Work: Findings Old and New
Recent Outcomes, New Models and Future Prospects
Fifth Annual Grampians Mental Health ConferenceMarch 1-2, 2005
William R. McFarlane, M.D.
Center for Psychiatric Research Portland, Maine
University of Vermont
Interaction of patient symptoms and family process:
A simple causal model

Effects of EE and medication on relapse in schizophrenia
44.3
57.7
18.4
27.9
0
10
20
30
40
50
60
High EE Low EE
AP Meds
No meds.
Bebbington and Kuipers, 1994

Effects of EE and contact on relapse in schizophrenia
58.8
41.7
18.323.9
0
10
20
30
40
50
60
High EE Low EE
High contact
Low contact
Bebbington and Kuipers, 1994

Effects of genetic risk and family functioning on eventual schizophrenia-spectrum disorders
5.84.8
36.8
5.3
0
5
10
15
20
25
30
35
40
High-risk, spectrum* Low-risk, spectrum**
% of sub-sample
Low OPAS ratings High OPAS ratings
* p < 0.001**p = 0.582
Tienari, et al, BJM, 2004

Positive Outcomes from FPE
• The patient and family work together towards recovery.
• Can be as beneficial in the recovery of schizophrenia and severe mood disorders as medication.

Research with Family Psychoeducation
• This treatment is an elaboration of models developed by Anderson, Falloon, McFarlane, Goldstein and others.
• Outcome studies report a reduction in annual relapse rates for medicated, community-based people of as much as 50% by using a variety of educational, supportive, and behavioral techniques.

Research with Family Psychoeducation
• Functioning in the community improves steadily, especially for employment.
• Family members have less stress, improved coping skills, greater satisfaction with caretaking and fewer physical illnesses over time.

Core Elements of Psychoeducation
• Joining
• Education
• Problem-solving
• Interactional change
• Structural change
• Multi-family contact

Outcomes in family psychoeducation
The evidence for being an evidence-based practice

Relapse outcome, controlled trials, 1980-1997
n Duration of treatment SF SF + MF MF Standard treatment
Falloon (1984) 36 24 17 83
Leff (1985) 19 24 14 78
Tarrier (1989) 44 9 33 59
Leff (1990) 23 24 33 36
Hogarty (1991) 67 24 32 67
Xiong (1994) 63 18 44 64
Zhang (1994) 83 18 15 54
Randolph (1995) 41 12 10 40
McFarlane (1995) 34 48 83 50
McFarlane (1995) 172 24 44 25
Schooler (1997) 313 12/24 29 35
Total 895 19.7 28.0 25.5 28.0 63

Comparison of single and multifamily formats
n Duration of
treatment, months
SF MF
Leff (1990) 23 24 33 36
McFarlane (1995) 34 48 83 50
McFarlane (1995) 172 24 44 25
Total 229 27.6 48.7 29.8

Relapse outcomes in clinical trials
65
41
15
9
0
10
20
30
40
50
60
70
No medication Individual therapy &medication
FPE & medication PEMFG & medication

Hospitalizations before vs.during treatment
1.08
0.27
0
0.2
0.4
0.6
0.8
1
1.2
Mean number of hospitalizations
per year2 yrs priorIn MFG tx

Family Psychoeducation in Schizophrenia
Psychoeducational multiple family group (PEMFG)
vs..
Psychoeducational single family treatment (PESFT)
N = 172

Family Psychoeducation in SchizophreniaProject Sites
Creedmoor Psychiatric CenterQueens, N.Y.
Harlem Hospital CenterNew York City
Hudson River Psychiatric CenterPoughkeepsie, N.Y.
Kings Park Psychiatric CenterIslip, N.Y.
Rochester Psychiatric CenterRochester, N.Y.
South Beach Psychiatric CenterStaten Island & Brooklyn, N.Y

Psychiatric Characteristics of Patients
by therapy modality
VariableAge of onset Mean s.d.Diagnosis Schizophrenia Schizoaffective SchizophreniformPrior hospitalization Mean s.d.Substance abuse No history Positive history
PEMFG PESFT
18.5 19.6 5.5 6.2
81.9% 88.3%13.8% 8.5% 4.3% 3.2%
4.0 5.5 4.5 5.5
61.7% 66.0%38.3% 34.0%
Modality differences: all not significant
Total
19.0 5.8
85.1%11.2% 3.7%
4.85.1
63.8%36.2%

50
60
70
80
90
100
0 100 200 300 400 500 600 700 800
Days at risk
% in
re
mis
sio
n
MFG SFT
Remission to 2 years
N: PEMFG=83; PESFT=92Main effect, all cases: p=.07Main effect, completers: p<.05

0
5
10
0 5 10 15 20 25
Months at risk
# of relapses
MFG SFT Linear (MFG) Linear (SFT)
Risk for relapse over two years
N: MFG=83; SFT=89

850
656
751
875
400
500
600
700
800
900
1000
-5 0 5 10 15 20 25 30
Months
Ch
lorp
rom
azi
ne
eq
uiv
ale
nts
in m
gs
.
MFG SFT MFG SFT
Medication dosages in MFG and SFT

48
38
29
1214
4953
57
0
10
20
30
40
50
60
70
Low a-d/Low CC Low a-d/High CC High a-d/Low CC High a-d/High CC
Cumulative two-year relapse rate (%)
MFG SFT
Anxious depression, critical comments and treatment type:Differential effects on relapse rates

Differential relapse rates by number of prior hospitalizations
19
35
4744
32
44
0
5
10
15
20
25
30
35
40
45
50
0 1 2 or moreNumber of prior hospitalizations
Percent of subsample relapsed in 2 years
MFGSFT


Functioning as an effect of repeated psychotic episodes
0
20
40
60
80
100
120
0 1 2 3 4 5 6Number of episodes
Fu
nct
ion
ing

Other effects in clinical trials
• Improved family-member well-being• Increased patient participation in rehabilitation• Substantially increased employment rates• Decreased psychiatric symptoms, including deficit
syndrome• Improved social functioning• Decreased family medical illnesses and medical
care utilization• Reduced costs of care
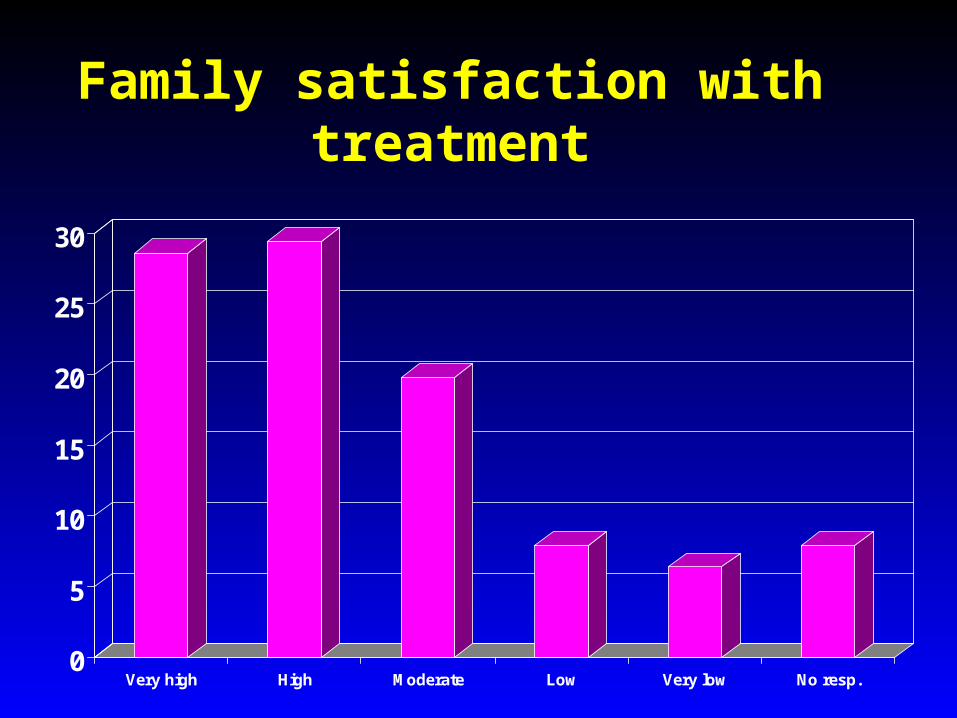
Family satisfaction with treatment
0
5
10
15
20
25
30
Very high High Moderate Low Very low No resp.
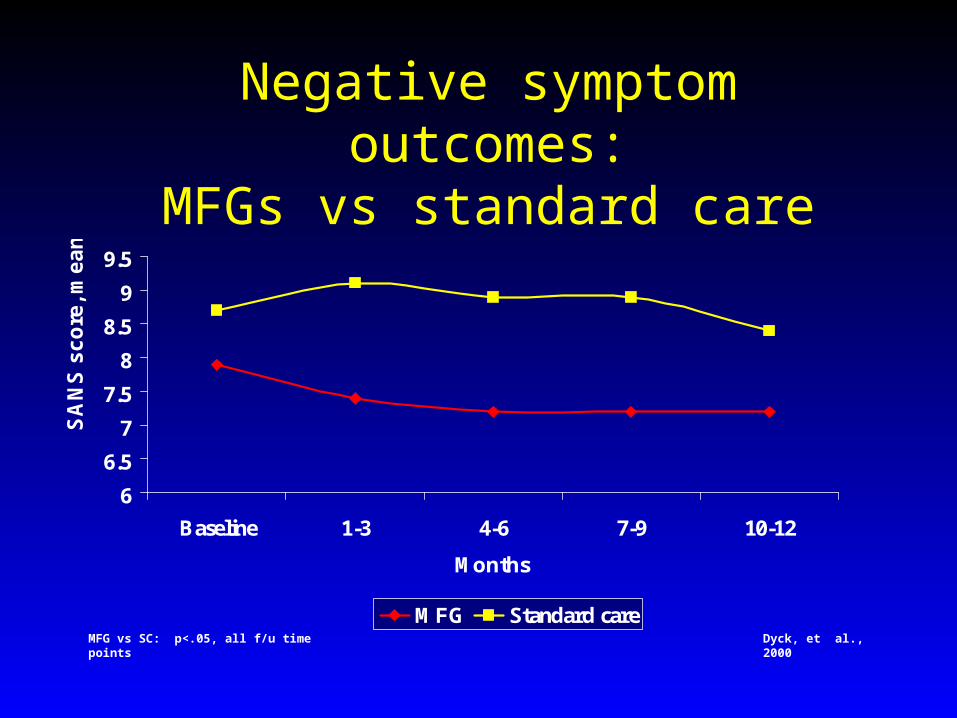
Negative symptom outcomes:MFGs vs standard care
6
6.5
7
7.5
8
8.5
9
9.5
Baseline 1-3 4-6 7-9 10-12
Months
SA
NS
sc
ore
, me
an
MFG Standard careMFG vs SC: p<.05, all f/u time points Dyck, et al., 2000

Family influences on work
Modeling
Information
Encouragement
Buffering
Guidance
Adjusting expectations
Ancillary support
Cueing
Personal connections

Rehabilitation effects of multifamily groups
Reducing family confusion and tension
Tuning and ratification of goals
Coordinating efforts of family, team, consumer and employer
Developing informal job leads and contacts
Cheerleading and guidance in early phases of working
Ongoing problem-solving

Work Outcome
Employed at baseline
17.3%
(p=.001)
Employed at 2 years
29.3%
Gain in % employed
PEMFG 16%
PESFT 8%
(n.s.)

Family-aided Assertive Community Treatment (FACT):
A clinical and employment intervention
• Psychoeducational multifamily groups
• Clinical case management using ACT principles and methods
• Integrated, multidisciplinary teams
• Supported employment
• MH Employers’ Consortium
• Cognitive assessments used in job accommodation

Vocational specialists on FACT teams: Principal tasks
–Developing contacts with employers–Case-specific job development–Job assessment –Assessment of patients' cognitive, physical and social capacities
–Setting career goals–Practicing interviews and resumes –Assistance with job interviews–On- or near-job support–Intervening with employers–Close coordination with clinicians

Rehabilitation effects of multifamily groups
Reducing family confusion and tension
Tuning and ratification of goals
Coordinating efforts of family, team, consumer and employer
Developing informal job leads and contacts
Cheerleading and guidance in early phases of working
Ongoing problem-solving

Outcomes in Family-aided Assertive Community
Treatment
FACT vs ACT
William R. McFarlane, M.D.Peter Stastny, M.D.
Susan Deakins, M.D.Robert Dushay, Ph.D.

RELAPSE OUTCOMEFACT vs. ACT
FACT (n=36) ACT (n=35)
8 (22%) 14 (40%)
Ln 8.58" Pos 0.75"

Employment outcome: FACT vs. ACT only
15.4% 15.4%
7.7% 7.7%3.7%
22.2%
37.0%
18.5%
0%
10%
20%
30%
40%
Baseline 12 mos. Gainedemploymt.
Lostemploymt.
% e
mp
loye
d, a
ny
job
ACTFACT

Washtenaw County, hospital rates ACT vs. MFG+ACT
0%5%
10%15%20%25%30%35%40%
Annual rate of hospitlaization
5-01 to 3-03
ACT
MFG & ACT

Selection Bias for the MFG?
0%
10%20%
30%40%
50%60%70%
80%
MFG Clients Non-MFG ACT
Annualized Hospitalization Rates
Future MFG clts, preACT 5-99 to 5-01
Future MFG clts, withACT only 5-99 to 5-01
MFG + ACT 5-01 to 5-03
Pre ACT hosp of Non-MFG 5-99 to 5-01
Non-MFG ACT 5-99 to5-01
Non-MFG ACT 5-01 to5-03

WCSTS ACT Employment/School
0%
10%
20%
30%
40%
50%
60%
70%
80%
Employment or School March '03
ACT
ACT + MFPE

Mental Health Employers Mental Health Employers ConsortiumConsortium
Employment OutcomesEmployment Outcomes
An Employment Intervention
Demonstration Project

Total Receiving Service137
Gender
Male 75 (54.7%)
Female 62
Condition
Employers Consortium 67
Community employers 70
Sample Description

0
10
20
30
40
50
60
70
80
Months in Program
Percent Employed(n = 116)
Schizophrenia
Mood Disorders
Other Disorders
Employment rate in FACT combined with supported employment, by diagnosis
67%
41%
19%
Evidence-based benefits for participants
• Promotes understanding of illness• Promotes development of skills• Reduces family burden• Reduces relapse and rehospitalization • Encourages community re-integration, especially
work and earnings• Promotes socialization and the formation of
friendships in the group setting

Practitioners have found...
• Renewed interest in work
• Increased job satisfaction
• Improved ability to help families and consumers deal with issues in early stages
• Families and consumers take more control of recovery and feel more empowered

Who can benefit from FPE?
• Individuals with schizophrenia who are newly diagnosed or chronically ill
• Adolescents and young adults with pre-psychotic symptoms
• There is growing evidence that the following people can also benefit:
- individuals with mood disorders
- consumers with OCD or borderline
personality disorder


Cost-benefit ratios of PMFGs
Treatment Hospital Costs Treatment Net /pt./yr. costs
Usual/prior $6156 $0 $6156
Family PE $1539 $300 $1839
$ saved per pt./yr. $4317

Family psychoeducation and multifamily groups:
Basic techniques

Stages of a psychoeducational multifamily group
Joining
Family and patient separately3-6 weeks
Educa-tional
workshop
Families only1 day
Ongoing MFGFamilies and
patients 1-4 years
Therapeutic processes in multifamily groups
• Stigma reversal
• Social network construction
• Communication improvement
• Crisis prevention
• Treatment adherence
• Anxiety and arousal reduction

Phases and Interventions in Family Psychoeducation
Year One: Relapse Prevention
Engaging individual families
Multifamily educational workshop
Implementing family guidelines
Reducing stigma and shame
Lowering expectations
Controlling rate of recovery
Reducing intensity and exasperation


Phases and Interventions in Family Psychoeducation
Year Two: Rehabilitation
Gradually increasing responsibilities
Moving one step at a time--the internal yardstick
Monitoring encouragement from family members
Establishing inter-family relationships
Cross-parenting
Focusing family interests outside family
Restoring family's natural social network

Structure of SessionsMultifamily groups (MFGs) and single-family treatment
(SFT)
MFG SFT1. Socializing with families and consumers 15 m. 10 m.
2. A Go-around, reviewing-- 20 m. 15 m.
a. The week's events b. Relevant biosocial information c. Applicable guidelines
3. Selection of a single problem 5 m. 5 m.
4. Formal Problem-solving 45 m. 25 m.
a. Problem definition b. Generation of possible solutions c. Weighing pros and cons of each d. Selection of preferred solution e. Delineation of tasks and implementation
5. Socializing with families and consumers 5 m. 5 m. Total: 90 m. 60 m.
Better outcomes in family psychoeducation
• Over 16 controlled clinical trials, comparing to standard outpatient treatment, have shown:– Much lower relapse rates and rehospitalization
• Up to 75% reduction of rates in controls; minimally 50%
– Increased employment• At least twice the number of consumers employed, and up to four times
greater--over 50%employed after two years--when combined with supported employment
– Reduced negative symptoms, in multifamily groups
– Improved family relationships and reduced friction and family burden
– Reduced medical illness • Doctor visits for family members decreased by over 50% in one year, in
multifamily groups

Summary


















