THE PHYSIOLOGY OF BREATHING DECLARATIONS … · lamas / labas / sabas and copd erj, feb 2004 uplift...
6
the physiology of breathing: Dr. Andrew Fon MBBS FRACP Respiratory and Sleep Medicine Physician PhD Research Fellow Dept. of Thoracic Medicine, ROYAL ADELAIDE HOSPITAL Senior Clinical Lecturer School of Medicine, UNIVERSITY OF ADELAIDE OBSTRUCTIVE LUNG DISORDERS DECLARATIONS THE PHYSIOLOGY OF BREATHING • CME Presentations • Boehringer Ingelheim • PulmonX™ • Astra Zeneca • Mundipharma • PhD Research Grants • University of Adelaide • PulmonX™ • Thoracic Society of Australia and New Zealand • Senior Clinical Lecturer • School of Medicine – University of Adelaide • Access Appointment • Dept of Thoracic Medicine – Royal Adelaide Hospital • The driving pressure for flow is the lung elastic recoil • Resistance is related to properties of the lung and its airways. THE PHYSIOLOGY OF BREATHING WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF EXPIRATORY FLOW? △PRESSURE RESISTANCE FLOW = • Lung volume determines elastic recoil • Determinants of Lung Volume: • Height • Gender • Age • Ethnicity WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF EXPIRATORY PRESSURE? THE PHYSIOLOGY OF BREATHING Emphysema • Elastic recoil pressure has a curvilinear relationship with lung volume • Different disease processes will have different effects on the elastic recoil properties of the lung THE PHYSIOLOGY OF BREATHING WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF EXPIRATORY PRESSURE? Lung Volume Pressure Normal Pulm. Fibrosis THE PHYSIOLOGY OF BREATHING WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF AIRWAY RESISTANCE? • 3 primary factors determine the resistance to flow within a single tube (Hagen-Poiseuille Law) • Radius (cross sectional area) • Length • Viscosity (gas density) • Resistance is DIRECTLY related to the length of the tube and to the viscosity of the gas. • Resistance is INVERSELY proportional to the length of the radius to the 4 th power • Airway calibre is the most important factor
Transcript of THE PHYSIOLOGY OF BREATHING DECLARATIONS … · lamas / labas / sabas and copd erj, feb 2004 uplift...

the physiology of breathing:
Dr. Andrew Fon MBBS FRACP
Respiratory and Sleep Medicine Physician
PhD Research Fellow
Dept. of Thoracic Medicine, ROYAL ADELAIDE HOSPITAL
Senior Clinical Lecturer
School of Medicine, UNIVERSITY OF ADELAIDE
OBSTRUCTIVE LUNG DISORDERS
DECLARATIONS
THE PHYSIOLOGY OF BREATHING
• CME Presentations• Boehringer Ingelheim
• PulmonX™
• Astra Zeneca
• Mundipharma
• PhD Research Grants
• University of Adelaide
• PulmonX™
• Thoracic Society of Australia and New Zealand
• Senior Clinical Lecturer• School of Medicine – University of Adelaide
• Access Appointment
• Dept of Thoracic Medicine – Royal Adelaide Hospital
• The driving pressure for flow is the lung elastic
recoil
• Resistance is related to properties of the lung and
its airways.
THE PHYSIOLOGY OF BREATHING
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS
OF EXPIRATORY FLOW?
△PRESSURE
RESISTANCEFLOW = • Lung volume determines elastic
recoil
• Determinants of Lung Volume:
• Height
• Gender
• Age
• Ethnicity
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS
OF EXPIRATORY PRESSURE?
THE PHYSIOLOGY OF BREATHING
Emphysema
• Elastic recoil pressure has a
curvilinear relationship with
lung volume
• Different disease processes
will have different effects on
the elastic recoil properties
of the lung
THE PHYSIOLOGY OF BREATHING
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS
OF EXPIRATORY PRESSURE?
Lung V
olu
me
Pressure
Normal
Pulm. Fibrosis
THE PHYSIOLOGY OF BREATHING
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS
OF AIRWAY RESISTANCE?
• 3 primary factors determine the resistance to flow within a single tube (Hagen-PoiseuilleLaw)
• Radius (cross sectional area)
• Length
• Viscosity (gas density)
• Resistance is DIRECTLY related to the length of the tube and to the viscosity of the gas.
• Resistance is INVERSELY proportional to the
length of the radius to the 4th power
• Airway calibre is the most important factor

WHICH AIRWAYS CREATE THE MOST RESISTANCE?
THE PHYSIOLOGY OF BREATHING
• Each lung has 1 main bronchi and 1.5-2 million terminal bronchioles
• The TOTAL cross-sectional area at the terminal airways is much greater that that of the intermediate generations.
• COPD is a SMALL AIRWAYS
DISEASE
THE PHYSIOLOGY OF BREATHING
• LUNG VOLUME• Increased lung volume pulls the airways apart
• At TLC airway caliber is at its greatest
• AIRWAY COMPLIANCE• Different disease states will affect the
compliance of the airway
• AIRWAY SMOOTH MUSCLE • Throughout the airways from trachea to
terminal bronchioles
• Intra-luminal Content• Inflammation/secretions may contribute to
narrowing of the airway lumen.
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF
AIRWAY CALIBRE?
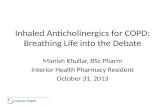
Adapted from 1. Kistemaker LE et al. Trends Pharmacol Sci 2015;36:164–171.
2. Kistemaker LE et al. Life Sci 2012;91:1126–1133. 3. Gosens R et al. Respir Res 2006;7:73.
Vagus nerve
Parasympathetic nerve
Parasympathetic ganglion
Airway
epithelium
Irritants (e.g. cigarette smoke)
Nodose
ganglion
Laryngeal
oesophageal
afferents
C-fibre
A-fibre
Irritantreceptors
C-fibre
receptors
CNS
Airway wall
ACh
ACh
ACh
Muscarinic
receptors
Submucosal
gland
Allergens
Mast cell
“Cholinergic tone”
THE PHYSIOLOGY OF BREATHING
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS OF
AIRWAY CALIBRE?
THE PHYSIOLOGY OF BREATHING
WHAT ARE THE PHYSIOLOGICAL DETERMINANTS
OF GAS EXCHANGE?
In the lung, gas exchange is dependent on 3 principal factors:
1. Delivery of gases to and from the pleural membrane (VENTILATION)
2. The physical properties of the gas exchange membrane. (DIFFUSION)
3. Factors affecting supply of blood (PERFUSION)
IC
• Ventilation is limited by expiratory flow
limitation
• Dynamic hyperinflation (DH) causes:
• Increased end expiratory lung volume
(EELV)
• Decreased Inspiratory Capacity (IC)
• DH increases work of breathing:
• Tidal volumes move up the pressure
volume curve
• Increased thoracic volume increases
intrinsic PEEP.
THE PHYSIOLOGY OF BREATHING
HOW DOES OBSTRUCTIVE DISEASE
AFFECT VENTILATION?
THE PHYSIOLOGY OF BREATHING
HOW DOES OBSTRUCTIVE DISEASE
AFFECT THE GAS TRANSFER MEMBRANE?
Emphysema leads to the
destruction of alveolar walls
and subsequent enlargement
of the inter-alveolar spaces.
Reduced total surface area
available for gas diffusion

EMPHYSEMA AFFECTS PULMONARY VASCULATURE
• Chronic hypoxia and acidosis leads to vascular remodeling
• Destruction of alveoli and associated structures reduce the number of alveolar capillaries
• Disproportionate hyperinflation causes reduced vascular lumen cross-sectional area.
• All three changes affect the mixed venous oxygen content
THE PHYSIOLOGY OF BREATHING
ANATOMY AFFECTS PHYSIOLOGY
THE PHYSIOLOGY OF BREATHING
THE PHYSIOLOGY OF BREATHING THE PHYSIOLOGY OF BREATHING
HOW DOES OBSTRUCTIVE LUNG DISEASE AFFECT
NORMAL RESPIRATORY PHYSIOLOGY?
• LUNG MECHANICS AND VENTILATION
• Loss of elastic recoil
• Increase in airways resistance pressure
• Narrow lumens
• Increased compliance
• GAS DIFFUSION
• Reduced alveolar gas exchange surface area
• PULMONARY CAPILLARY
PERFUSION
• Reduced vasculature - increased
dead space ventilation
• Increased pulmonary capillary
pressures
• Hypoxia induced vasoconstriction
• Reduced capillary perfusion
secondary to cor pulmonale
• CARDIAC CHANGES
• Decreased venous return
• Decreased preload
• Decreased stroke volume
PATHOPHYSIOLOGY DRIVES TREATMENT
• Treatment goals are to:
• Minimize disease progression
• Improve quality of life
• Reduce exacerbations
• Improve exercise tolerance
• Maintain lung function
• TREATMENT GOALS ARE
PATIENT FOCUSSED
THE PHYSIOLOGY OF BREATHINGTHE PHYSIOLOGY OF BREATHING
WHAT ARE THE CLINICAL APPLICATIONS?

PHYSIOLOGICAL ADAPTATION
THE PHYSIOLOGY OF BREATHING
PATHOPHYSIOLOGY DRIVES TREATMENT
Vagus nerve
Parasympathetic nerve
Parasympathetic ganglion
Airwayepithelium
Irritants (e.g. cigarette smoke)
Nodoseganglion
Laryngealoesophageal
afferents
C-fibre
Ad-fibre
Irritantreceptors
C-fibrereceptors
CNS
Airway wall
ACh
ACh
ACh
Muscarinicreceptors
Submucosal gland
Allergens
Mast cell
THE PHYSIOLOGY OF BREATHING
PATHOPHYSIOLOGY DRIVES TREATMENT
• Inflammation is different in asthma and COPD requiring a different treatment approach:
COPD AsthmaMast cells,
Eosinophils, Inflammatory
cytokines
Inflammation is responsive
to corticosteroidsinflammation is largely
unresponsiveto corticosteroids
Airway neutrophils,
Macrophages, CD8+ T Cells
10%
THE PHYSIOLOGY OF BREATHING
LAMAs / LABAs / SABAs and COPD
ERJ, Feb 2004
UPLIFT - NEJM, Oct 2008
THE PHYSIOLOGY OF BREATHING
CORTICOSTEROIDS IN COPD
ISOLDE Trial - BMJ, May 2000
TORCH - NEJM, Feb 2007
INSPIRE - AJRCCM, Oct 2007
THE PHYSIOLOGY OF BREATHING
CORTICOSTEROIDS IN COPD
PATHOS - BMJ, May 2013
WISDOM - NEJM, Oct 2014
THE PHYSIOLOGY OF BREATHING
FLAME - NEJM, May 2016

CORTICOSTEROIDS IN COPD
IMPACT - NEJM, Apr 2018
THE PHYSIOLOGY OF BREATHING
• GSK funded project• Only used GSK products
• LABA/LAMA -
Umeclidinium + Vilanterol• LABA/ICS - Fluticasone
Furoate + Vilanterol• LABA/LAMA/ICS -
Vilanterol + Umec + FF
• ~40% of participants were already on triple therapy at enrolment• 70% of participants were taking an ICS• Patients with a history of asthma were included
PATHOPHYSIOLOGY DRIVES TREATMENT
WHO SHOULD BE ON WHAT DEVICE?
THE PHYSIOLOGY OF BREATHING
CLASS A & B:ICS Free
CLASS C & D:Initiate with LABA/LAMA
Consider ICS
REMEMBER:
• 10-15% of COPD patients
will also have asthma
• FEV1 <50%
AND
• ≥ 2 exacerbations per year
OR ≥ 1 hospitalization
AND
• Blood Eosinophil Count >
300 cells/uL
WISDOM - 2014
STEROID WEANING: HOW AND WHEN
• Insufficient data for a definitive plan.
• Patient counselling regarding rationale for withdrawal of ICS
is essential
• Especially important for patients who have been on ICS long-term
• Optimize bronchodilator therapy first
• Consider more frequent follow up in the short term once
withdrawal is started.
• Review at 1 week / 3 weeks / 6 weeks / 3 months / 6 months
THE PHYSIOLOGY OF BREATHING
• If few/no exacerbations in the past year and low symptom burden:
• Consider abrupt withdrawal of ICS
• If concern regarding withdrawal - 6-12 wk wean across each puffer dose decrease
STEROID WEANING: HOW AND WHEN
THE PHYSIOLOGY OF BREATHING
WISDOM - NEJM 2014
EMPHYSEMA: NO ROOM TO BREATHE
• Three principal factors related to exertional dyspnoea:
• Ventilatory Abnormalities
• Pulmonary Gas Exchange
• Muscle Dysfunction
THE PHYSIOLOGY OF BREATHING

COPD: NO ROOM TO BREATHE
THE PHYSIOLOGY OF BREATHING
PERI-OPERATIVE MORTALITY ~ 5 - 20%
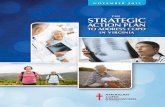
BRONCHOSCOPIC LUNG VOLUME REDUCTION
PRE-ELVR POST-ELVR
ONE-WAY VALVE INSERTION
Damaged, hyperinflated section of the
lungs
Healthy,
squashed
section of the lungs
Healthy section of the lungs
has expanded
Damaged
section of
the lungs has collapsed
THE PHYSIOLOGY OF BREATHING
BRONCHOSCOPIC LUNG VOLUME REDUCTION
Difference EBV vs Control Groups
TRIALSize & Follow-up
period
Lung Function (FEV1%)
MCID = 10%-15%
Exercise Capacity (6MWD)
MCID = 26 m
Quality of Life (SGRQ)
MCID = -4 pts
VENT4
n=122
(post hoc subset)
6 mo24.8% 28 m -8.4 pts
BeLieVeR-HIFi3n=50
3 mo20.9%* 33 m* -5.1 pts
STELVIO2 n=68
6 mo17.8%* 74 m* -14.7 pts
IMPACT1 n=93
3 mo17.0%* 40 m* -9.6 pts*
LIBERATE5 n= 190
12 mo18.0%* 39 m* -7.1 pts
1. Valipour A et al, AJRCCM 2016. 194: 1073–1082;
2. Klooster K. et al. N Engl J Med. 2015; 373: 2325-2336 + Supplementary Appendix;
3. Davey C et al, Lancet. 2015; 386: 1066-1073 + Supplementary appendix;
4. Scuirba F.C. et al. N Engl J Med. 2010; 363(13): 1233-1244/ Herth F. J. et al. Eur. Respir. J. 2012; 39(6): 1334-1342/ Ad hoc analysis on file at Pulmonx
5. Criner, G et al, 2018
THE PHYSIOLOGY OF BREATHING THE PHYSIOLOGY OF BREATHING
SUMMARY• The physiological basis of disease dictates therapy options in
COPD
• COPD causes loss of elastic recoil, increased small airway resistance, and changes to ventilation and perfusion.
• Focus of therapy is to maximize quality of life and minimize exacerbations and loss of function.
• The majority of patients will not be worse off on LABA/LAMA vs LABA/ICS
• ICS are indicated in the appropriate patient - Efforts to minimize steroid exposure is a must.
THE PHYSIOLOGY OF BREATHING
REFERENCES
THANK YOU